precut ercp, fistulotomy, papillotomy, transpancreatic sphincterotomy. miguel chavez rossell
TRANSCRIPT

ERCP: PRECUT “ACCESS”PAPILLOTOMY
NEEDLE-KNIFE SPHINCTEROTOMYFISTULOTOMY, PAPILLOTOMY,
TRANSPANCREATIC SPHINCTEROTOMYUpdate Review
MIGUEL CHAVEZ ROSSELL MDArzobispo Loayza Hospital
Lima - Perú




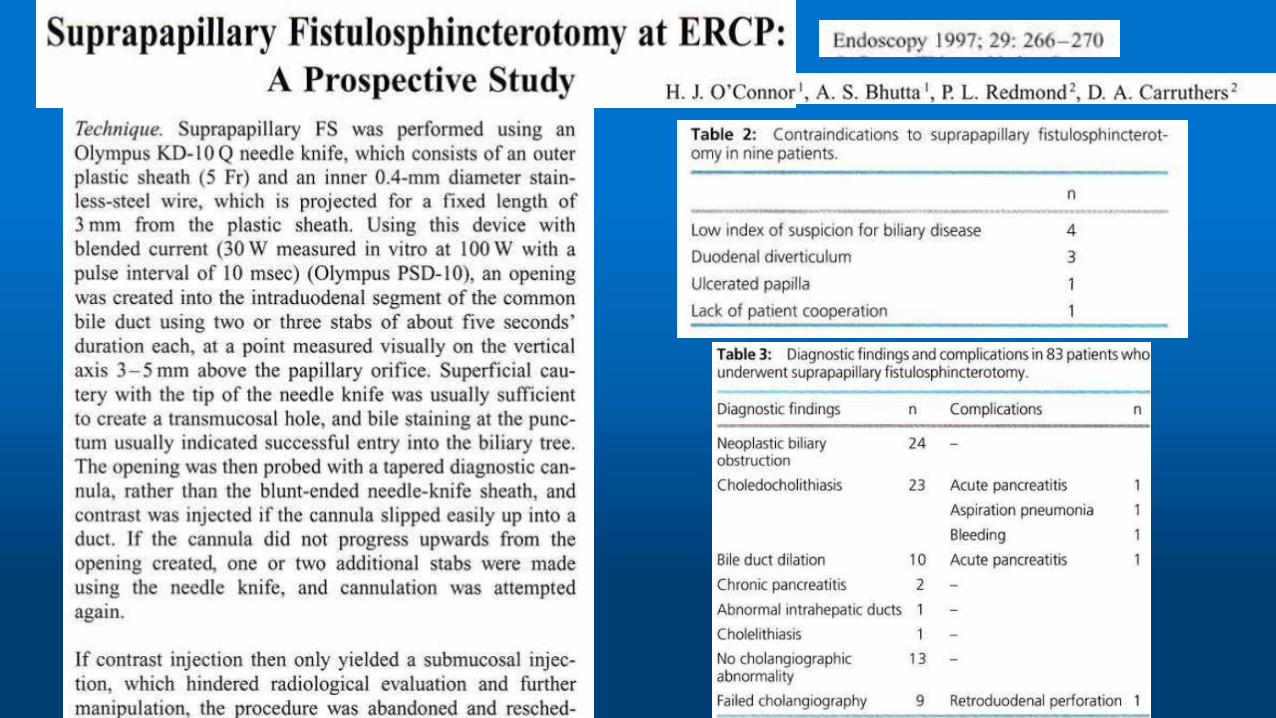














Figure 2. The needle-knife tip is positioned at the junction of
the upper third and lower two thirds of the papillary mound. The
endoscopist is positioned to begin cutting in the downward direction (modified technique).
Figure 3. The needle-knife cut is complete, with the ‘‘safety margin’’ between the cut and the papilla (outlined with a white line).
Early institution of pre-cutting for difficult biliary cannulation:a prospective study comparing conventional vs. a modified technique




Comparison of early pre-cutting vs standard technique forbiliary cannulation in endoscopic retrogradecholangiopancreatography: A personal experience
Kannikar Laohavichitra, Thawatchai Akaraviputh
World J Gastroenterol 2007 July 21; 13(27): 3734-3737
From January 2003 to December 2004
123 procedures (29.6%) with early pre-cutting technique in case of difficult cannulation
If biliary access failed after 10 min or if more than 3 pancreatic injections with contrast were
made (whichever occurred first), the early pre-cutting technique with needle knife catheter (MicroKnife XL, Boston Scientific, Natrick, USA
Endocut mode in the ERBE system
pure cutting mode

Comparison of early pre-cutting vs standard technique forbiliary cannulation in endoscopic retrogradecholangiopancreatography: A personal experience







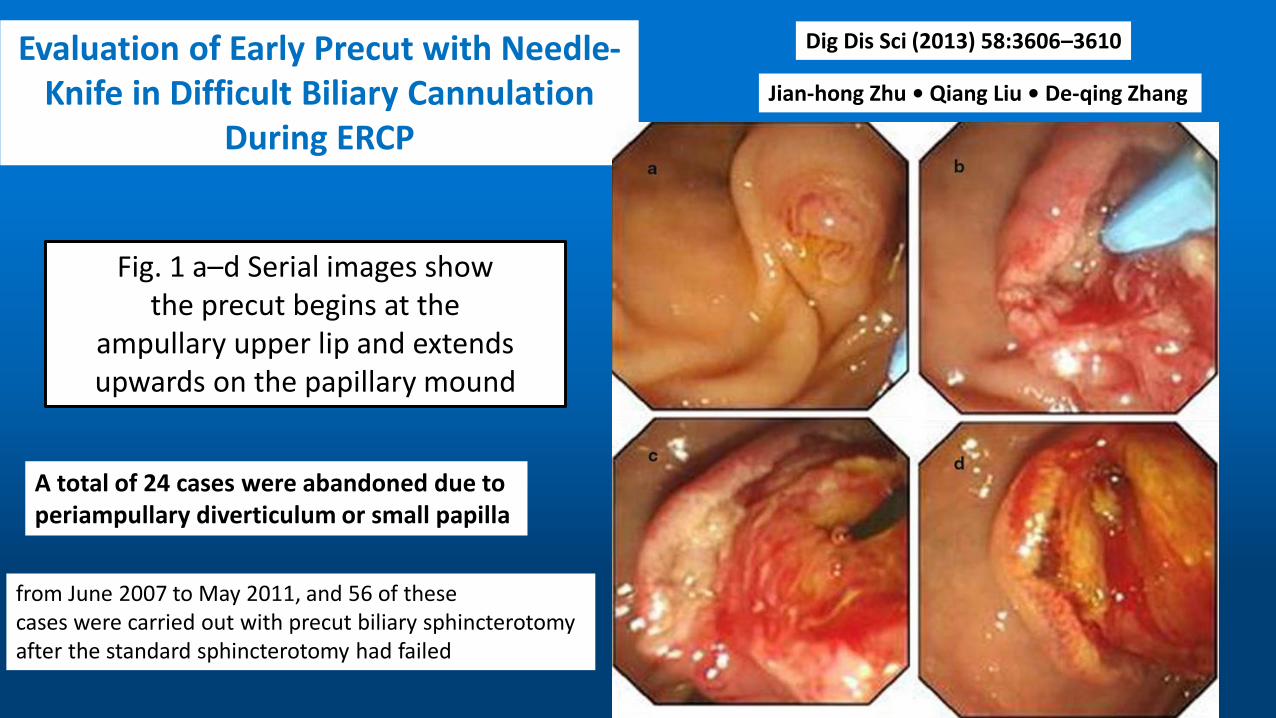
Evaluation of Early Precut with Needle-Knife in Difficult Biliary Cannulation
During ERCP
Dig Dis Sci (2013) 58:3606–3610
Jian-hong Zhu • Qiang Liu • De-qing Zhang
Fig. 1 a–d Serial images showthe precut begins at the
ampullary upper lip and extends upwards on the papillary mound
A total of 24 cases were abandoned due to periampullary diverticulum or small papilla
from June 2007 to May 2011, and 56 of thesecases were carried out with precut biliary sphincterotomyafter the standard sphincterotomy had failed

Fig. 2 a–d The impacted stonespontaneously passes after a
suprapaplillary fistulotomy wasperformed
Evaluation of Early Precut with Needle-Knife in Difficult Biliary
Cannulation During ERCP
Most precuts were performed without pancreatic stent placement, starting from the papillary orifice and proceeding at the 11 o’clock position upward over the papillary mound (Fig. 1). In some clinical situations where there was impacted stone at the ampulla ofVater, a suprapapillary fistulotomy was performed (Fig. 2), the needle was inserted towards 11 o’clock orientation a few millimeters above the papillary orifice, and the cutting was extended downwards towards the orifice. If precut failed, the procedure was abandoned.
Here, there are several points which need to benoted when we are performing duodenum or papillaryprecuts. First, PBS surgery is an injurious form of manipulation, and brings with it a certain level of ignorance. If those responsible for performance do not pay attention, this will increase the risk of complications. Therefore, operators must fully understand and carefully observe the papillary organs and keep looking for formations or tumors.Second, PBS should only be performed by highly trainedand well-experienced endoscopists, while, in addition, it isparticularly to be used only when the operator’s professional intuition plus the patient’s condition means it isrequired. Third, the incision should not be made too largeand the cutting should be gradually opened throughout theprecut process. It is worth pointing out that the blade cutsin one direction only. In the event that a bile duct is cut, thecutting should be immediately stopped. Only after standardtreatment is performed should one elongate the incision
Fourth, operators must be familiar with abdominal anatomy. When the common bile duct is opened, it usuallyappears white. At this point, sphincterotomy can beattempted; if still problematic, the incision can be startedagain at the white orifice, after which one should clearlysee the light pink epithelium. Fifth, during the course ofprecut treatment, blood oozing from the incision couldmake the field of vision murky and affect the cuttingoperation. In this case, one may either spray the affectedarea or wait for the blood to clot. Second cutting must be
avoided at all costs. And sixth, operators should be proficient and capable of responding to unforeseen complications or an emergency during a surgery
Evaluation of Early Precut with Needle-Knife in Difficult Biliary
Cannulation During ERCP

Early precut fistulotomy for biliary access: time to change the paradigm of “the later, the better”?
Needle-knife fistulotomy. NKF was performed by using a needle-knife (Olympus KD-11Q; Olympus Corporation). After making a puncture in the papilla above the orifice, the incision was made upward or downward (depending on the position of the initial puncture), along the axis of the bile duct, while maintaining at least a 3-mm distance from the papillary orifice. The cut was slowly extended until the CBD was exposed, followed by a small incision in the muscle. The CBD was then cannulated directly with the closed needle-knife or with a papillotome(wire guided) if the needle-knife did not slide. Once deep cannulation was achieved, a cholangiogram was obtained by using low-osmolality, nonionic contrast (Ultravist [iopromide]; Bayer Schering Pharma, Berlin, Germany), and the necessary therapeutic maneuvers were performed.
• GASTROINTESTINAL ENDOSCOPY Volume 80, No. 4 : 2014
• Luís Lopes, MD, Mário Dinis-Ribeiro,

GASTROINTESTINAL ENDOSCOPY Volume 80, No. 4 : 2014

Different Strategies for Transpancreatic Septotomyand Needle Knife Infundibulotomy Due to the
Presence of Unintended Pancreatic Cannulation in Difficult Biliary Cannulation
Gut and Liver, Vol. 9, No. 4, July 2015, pp. 534-539
Yoon Jung Lee, Yun Kyung Park, Min Ji Lee, Kyu Taek Lee,
The most widely practiced precut technique is needle knife infundibulotomy, which is valuable if biliary cannulation is not achieved for any duct. The advantage of this technique is that it can minimize the risk of perforation and pancreatitis, due to the predefined upper extent of the cut and untouched pancreatic duct.
needle knife infundibulotomy (NKI)
The papillary configuration was classified as follows: normal, bulging, redundant, impacted stone, papillitis, peripapillary diverticulum, abnormal location or small orifice. The bulging type showed marked swelling of the oral protrusion of papilla. The redundant type showed the longitudinal shape of the papilla and the orifice located in the lower portion of the papilla. Abnormal location signified the deviated axis of papilla from the 11 to 1 o’clock position or an unusual location of the papilla which was leaning toward the third portion of the duodenum.
When the biliary cannulation was not achieved within 5 minutes for any duct, NKI was performed. This technique involves making a puncture into the papilla above the orifice to avoid injuring the pancreatic duct and to minimize the rate of post-ERCP pancreatitis, which is the most serious complication of such procedures, and then cutting in the 11 to 12 o’clock direction along the ridge of the common bile duct using a needle knife papillotome. After a fistula to the bile duct was made, the standard papillotome was repositioned to the biliary duct and the sphincterotomy was extended
Precut sphincterotomy with a needle knife is performed either by a precut papillotomy or by infundibulotomy. In the papillotomy technique, the incision starts from the papillary orifice, whereas in the fistulotomy technique, the incision starts above the papillary orifice.

Different Strategies for TranspancreaticSeptotomy and Needle Knife InfundibulotomyDue to the Presence of Unintended Pancreatic Cannulation in Difficult Biliary Cannulation
In practice, the bulging type of papilla was a good candidate for an infundibulotomy or the modified techniques of needle knife precut. So, future studies should examine the adoption of precut method based on papillary configuration in difficult biliary cannulation.

Different Strategies for TranspancreaticSeptotomy and Needle Knife InfundibulotomyDue to the Presence of Unintended Pancreatic
Cannulation in Difficult Biliary Cannulation






The term difficult biliary Access es poorly defined


Utility of needle-knife fistulotomy as an initial method of biliary cannulation to prevent post-ERCP pancreatitis in a highly selected at-risk group: a single-arm prospective feasibility study
November 2016 Volume 84, Issue 5, Pages 808–813

Figure 1. Needle-knife fistulotomy technique. A, Major duodenal papilla; B, small mucosal incision using a needle-knife papillotome is performed in the 11 to 12 o’clock position on the top of the infundibulum, avoiding touching the orifice; C, sphincter of Oddi muscle of the bile duct is visible after theincision; D, biliary cannulation is achieved by pricking the stigma with a needle-knife.
Seven of the 62 patients were excluded due to periampullarydiverticulum (PAD) type I (n Z 1) or II (n Z 4),stone located at the papilla orifice (n Z 1), and choledochoduodenal fistula (n Z 1). Thus, 55 patients were enrolled in this prospective study, all of whom underwent ERCP and NKF.

Study participantsBetween August 2013 and May 2015, 62 consecutivepatients were diagnosed as having CBD stones and underwent ERCP for stone removal. They had at least one of the following patient-related risk factors for PEP: young age (<60 years), female, or normal CBD diameter (9 mm).All patients were naive for ERCP and had no history ofpancreatitis. A prospective database was created for these62 consecutive patients. Seven of the 62 patients were excluded due to periampullary diverticulum (PAD) type I (n Z 1) or II (n Z 4), stone located at the papilla orifice (n Z 1), and choledochoduodenal fistula (n Z 1). Thus, 55 patients were enrolled in this prospective study, all of whom underwent ERCP and NKF.
The shape of the papilla was classified as hemispherical,papillary, or flat according to the external appearance ofthe major papilla



pancreatitis: a randomized trial
Endoscopy 2016; 48(06): 530-535 Alberto Mariani, Milena Di Leo, Nicola Giardullo



• The best timing of precut in order to limit the incidence of PEP is hard to establish or standardize
• there is still no consensus on the definition of difficult biliary cannulation.
• The time of 5 minutes of cannulation attempts arbitrarily applied in this study provided a reliable basis for assessing the risk of PEP. It amounts to about 10–15 cannulation attempts, a cutoff often associated with a higher risk of
this complication
Fistulotomy was the main approach used for precut. Despite conflicting results on PEP rates for fistulotomy and precut from the orifice technique, fistulotomy significantly reduced the odds of PEP in the subgroup analysis of pooled data of the two RCTs in which it was employed as the only method of precut. In the current study, fistulotomy was used with the aim of protecting the pancreatic orifice from diathermic injury by the cutting wire, except in patients with a small papilla where cutting the roof would be more difficult. The extensive use of fistulotomy in the current study could have avoided trauma in the vicinity of the pancreatic orifice, which would help to explain the lower rate of PEP in the early precut group, as in the repeated cannulation attempts group there is a greater risk of injury to the pancreatic orifice and consequent impairment of pancreatic juice outflow.








CONCLUSIONS
1. The precut is a safe and effective technique to access the biliary tract, in experienced hands.
2. There are several precut techniques. There is no consensus by which is the best. But fistulotomy is theoretically safer to avoid Pancreatitis Post ERCP, because the common channel and the pancreatic duct are completely avoided.
3. The time at which the precut must be done, must be early, but there is no consensus on the definition of “early precut"
4. The precut technique should be included as part of the training of the fellows, so that they can be applied when necessary.
5. The fellows must begin to learn the technique of precut in cases of impacted Ampulla stones or in the very dilated choledochus.

In my practice, I perform Fistulotomy technique. The incision is made from above downward, with a needle knife.The incision begin in the Midportion in the Ampulla of Vater, layer by layer , and it was stopped when pinkish mucosaof the bile duct or bile juice was visible. The risk of pancreatitis is minimum because the pancreatic orifice is untouched