policy: o1 therapeutic engagement & supportive observation · o1/04 june 07 director of nursing...
TRANSCRIPT

West London NHS Trust_______________________________________ _____Page 1 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Policy: O1 Therapeutic Engagement & Supportive Observation
Version: O1/18
Ratified by: Trust Clinical Governance Group
Date ratified: 1st October 2018
Title of originator/author: Deputy Director of Nursing
(West London Forensic services)
Title of responsible Director Director of Nursing & Patient Experience
Date issued: 15th October 2018
Key Stakeholders Director of Nursing and Patient experience
Trust Medical Director
Clinical leads and deputy directors of Nursing
Review date: April 2020
Target audience: All staff trust-wide
Disclosure Status: (B) B: Can be disclosed to patients and the public
EIA / Sustainability
EIA 2018.doc

West London NHS Trust_______________________________________ _____Page 2 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Equality & Diversity Statement The Trust strives to ensure its policies are accessible, appropriate and inclusive for all. Therefore all policies will be required to undergo an Equality Impact Assessment and will only be approved once this process has been completed.
Sustainable Development Statement
The Trust aims to ensure its policies consider and minimise the sustainable development impacts of its activities. All policies are therefore required to undergo a Sustainable Development Impact Assessment to ensure that the financial, environmental and social implications have been considered. Policies will only be approved once this process has been completed

West London NHS Trust_______________________________________ _____Page 3 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
O1 - Enhanced Engagement and Observation Policy Version Control Sheet
Version Date Title of Author
Status Comment
O1/01 April 2001 Observation Policy
O1/02 31/01/05 Policy withdrawn and replaced by new Trust wide Policy
O1/03 07/02/05 Director of Nursing & Facilities
New Trust wide Policy
O1/04 June 07 Director of Nursing & Facilities
Policy reviewed
O1/05 Sept 07 Director of Nursing & Facilities
Revised Policy Issued Substantial revision made to policy in September 2007
O1/06 09.10.07 Director of Nursing & Facilities
Revised policy issued
O1/07 10.10.08 Executive Director of High Secure Services and Nursing
Policy revised. In September 2008 Policy was reviewed. Revised policy issued to account for change to the MHA and role described in section 1.6
O1/08 29.10.08 Executive Director of High Secure Services and Nursing
Policy Revised Minor amendment made to wording in section 4.15.1
O1/09 04.11.08 Head of Standards & Compliance
Policy Revised Added Section 4.16 – Monitoring & Training and Appendix H – Mandatory Training Matrix
O1/09 15.07.09 ED of High Secure Services and Nursing
Addition included as bullet point in section 4.5.3. Note this did not affect version number (stayed same)
O1/10 June 2010
Director of Nursing and Patient Experience
Policy under review
O1/11 01.05.10 Director of Nursing and Patient Experience
Policy Reviewed at Policy Review Group 01/03/10.
Issued as working document on 01/05/10 with consultation ending 28.05.10

West London NHS Trust_______________________________________ _____Page 4 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Version Date Title of Author
Status Comment
O1/12 24.06.10 Director of Nursing and Patient Experience
Policy under consultation Following further review after end of consultation – section 2.5 was noted to be missing. Now included and revised policy re-issued for 2 weeks consultation ending 09/07/10.
O1/13 21.10.10. Director of Nursing and Patient Experience
NB: The CURRENT TRUST Policy that staff should be using for daily work is version O1/11 May 10 which can be found on the Exchange
On 30.07.10 the revised Policy was issued (vO1/13 Jul10) and then retracted for further consultation ending 10.09.10.
Comments from Consultation now incorporated.
To be presented at 21st October
PRG for approval – approved.
O1/14 29.11.10 Director of Nursing and Patient Experience
Revised Enhanced Engagement & Observation Policy Issued
Key Practice Issues accompany this revised enhanced policy
01/15 08.02.11 January 2011 - Addition of Appendix I - The Cassel Enhanced Engagement & Observation Procedure. Present to Policy Review Group 31
st Jan
for approval – approved.
O1/16 05.10.12 Director of Nursing and Patient Experience
Revised Policy issued Approved at July TMT subject to minor amendments, issued October 2012.
O1/17 August 2015
Deputy Director of Nursing (Forensic Services)
Issued Comprehensive review reflecting NICE Guidance 25 and in response to regulation 28 directions
Trust wide consultation ending 28.09.15
Approved PSS Dec 2015
O1/17.1 January 2017
Amended policy issued Text amend to sections 5.7 & 9.2
O1/17.2 December 2017
Amended policy issued Minor text amend to section 8.3 –
Must not use their personal mobile phones
O1/18 October 2018
Deputy Director of Nursing ( West London Forensic Services
Policy review. Ratified and issued
Policy review and Trust-wide consultation July 2018. Ratified at Trust Clinical Governance Group October 2018

West London NHS Trust_______________________________________ _____Page 5 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Contents 1. Therapeutic engagement and supportive observations process table 6 2. Introduction 9 3. Scope 10 4. Definitions 10 5. Duties and responsibilities 12 6. Possible antecedents or warning signs that observation is required 13 7. Implementing Therapeutic engagement and supportive observation 15 8. Undertaking Therapeutic Engagement and Supportive Observation 17 9. Duties of the nurse in charge 18 10. Service user needs 18 11. Reviewing the level of therapeutic engagement and supportive observations 19 12. MDT Review 20 13. Independent Review 20 14. External Review 21 15. Night time 21 16. Service user asleep 21 17. Leave 22 18. Legal status 22 19. Record keeping 22 20. Training for therapeutic engagement & supportive observation 23 21. Monitoring and audit 24
Appendix A (morning) General Engagement and Observation Form 25 Appendix A (afternoon/evening) General Observation Form 26 Appendix A (night) General Observation form 27 Appendix B: Therapeutic Engagement & Supportive Observation Care Plan 28 Appendix C: Therapeutic Engagement & supportive Observation Care Plan 29 Appendix D: Therapeutic Engagement & Supportive Observation Record 30 Appendix E: Therapeutic engagement & supportive observation - Training and competency assessment framework 31 Appendix F: Staff and Service User Information Leaflet 33 Appendix G: Guidance for staff on engagement in challenging situations 34
West London NHS Trust_______________________________________ _____Page 6 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
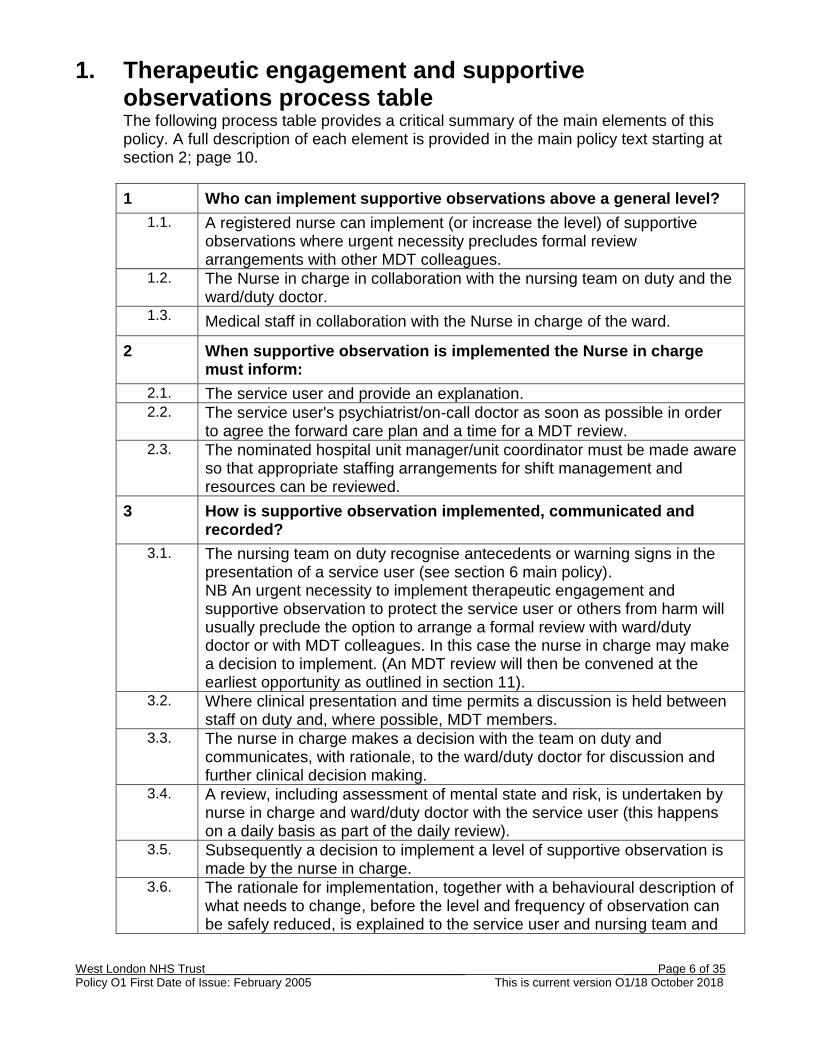
1. Therapeutic engagement and supportive observations process table The following process table provides a critical summary of the main elements of this policy. A full description of each element is provided in the main policy text starting at section 2; page 10.
1 Who can implement supportive observations above a general level?
1.1. A registered nurse can implement (or increase the level) of supportive observations where urgent necessity precludes formal review arrangements with other MDT colleagues.
1.2. The Nurse in charge in collaboration with the nursing team on duty and the ward/duty doctor.
1.3. Medical staff in collaboration with the Nurse in charge of the ward.
2 When supportive observation is implemented the Nurse in charge must inform:
2.1. The service user and provide an explanation. 2.2. The service user's psychiatrist/on-call doctor as soon as possible in order
to agree the forward care plan and a time for a MDT review. 2.3. The nominated hospital unit manager/unit coordinator must be made aware
so that appropriate staffing arrangements for shift management and resources can be reviewed.
3 How is supportive observation implemented, communicated and recorded?
3.1. The nursing team on duty recognise antecedents or warning signs in the presentation of a service user (see section 6 main policy). NB An urgent necessity to implement therapeutic engagement and supportive observation to protect the service user or others from harm will usually preclude the option to arrange a formal review with ward/duty doctor or with MDT colleagues. In this case the nurse in charge may make a decision to implement. (An MDT review will then be convened at the earliest opportunity as outlined in section 11).
3.2. Where clinical presentation and time permits a discussion is held between staff on duty and, where possible, MDT members.
3.3. The nurse in charge makes a decision with the team on duty and communicates, with rationale, to the ward/duty doctor for discussion and further clinical decision making.
3.4. A review, including assessment of mental state and risk, is undertaken by nurse in charge and ward/duty doctor with the service user (this happens on a daily basis as part of the daily review).
3.5. Subsequently a decision to implement a level of supportive observation is made by the nurse in charge.
3.6. The rationale for implementation, together with a behavioural description of what needs to change, before the level and frequency of observation can be safely reduced, is explained to the service user and nursing team and

West London NHS Trust_______________________________________ _____Page 7 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
detailed in the clinical record and the service users care plan. 3.7. In addition the nurse in charge must communicate and document to the
nursing team and at every handover; o The level and frequency of the observations o The rationale and any particular needs identified o the name/title of the staff who will be responsible for carrying out
the therapeutic engagement and supportive observation 3.8. The observing nurse makes a record of therapeutic engagement and
supportive observation at the agreed level and frequency in the Therapeutic observation & supportive observation recording form (appendix D).
3.9. At the end of each shift the allocated nurse hands over to the member of staff taking over the next session, involving the service user where possible.
3.10. A review of the therapeutic engagement and supportive observations occurs at a minimum once per day and is clearly documented in the service users progress notes.
3.11. When supportive observation is implemented between the hours of 09:00 and 17:00, Monday to Friday, the Nurse in charge must inform:
a. The service user's Responsible Clinician/on-call doctor as soon as possible.
b. The nominated hospital/unit manager/unit co-ordinator; so that staffing resources can be reviewed.
c. The service user will be given the option for the nurse in charge to inform the nearest relative, friend or carer about the implementation, aims and level of supportive observation.
3.12. If out of hours the nurse in charge must inform; a. The on call consultant psychiatrist. b. The nominated hospital/unit manager/unit co-ordinator so that
staffing resources can be reviewed.
4 Who should review the level of supportive observation?
4.1. Increasing the level of supportive observation (outlined in section1) The nursing team on duty recognises antecedents or warning signs of increased risk in the presentation of a service user. An urgent necessity to implement therapeutic engagement and supportive observation to protect the service user or others from harm will usually preclude the option to arrange a formal review with ward/duty doctor or with MDT colleagues. In this case the nurse in charge may make a decision to implement.
4.2. Follow process described at 3.2 – 3.4 above: a) The rationale for increasing the level of supportive observation together
with a behavioural description of what needs to change before the level of observation can be safely reduced is explained to the service user and nursing team and recorded in the clinical record and the patient care plan.
b) Follow process at 3.7 - 3.12 above 4.3. Reducing level of supportive observation
West London NHS Trust_______________________________________ _____Page 8 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
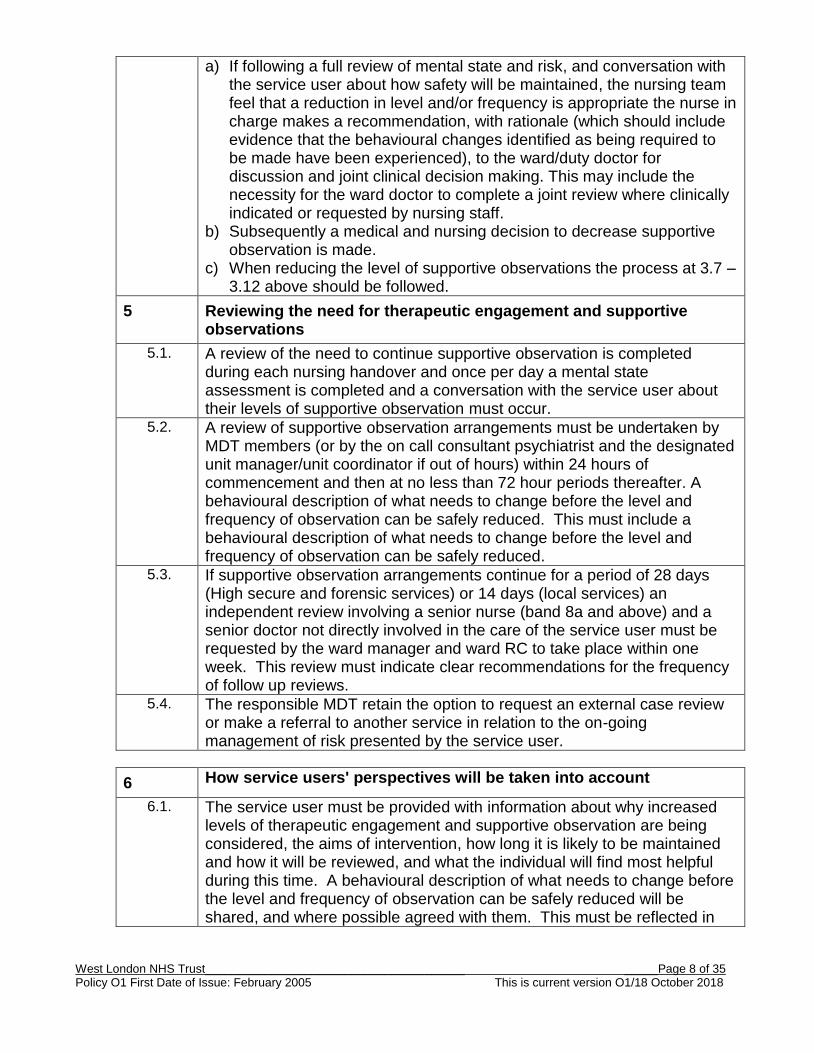
a) If following a full review of mental state and risk, and conversation with the service user about how safety will be maintained, the nursing team feel that a reduction in level and/or frequency is appropriate the nurse in charge makes a recommendation, with rationale (which should include evidence that the behavioural changes identified as being required to be made have been experienced), to the ward/duty doctor for discussion and joint clinical decision making. This may include the necessity for the ward doctor to complete a joint review where clinically indicated or requested by nursing staff.
b) Subsequently a medical and nursing decision to decrease supportive observation is made.
c) When reducing the level of supportive observations the process at 3.7 – 3.12 above should be followed.
5 Reviewing the need for therapeutic engagement and supportive observations
5.1. A review of the need to continue supportive observation is completed during each nursing handover and once per day a mental state assessment is completed and a conversation with the service user about their levels of supportive observation must occur.
5.2. A review of supportive observation arrangements must be undertaken by MDT members (or by the on call consultant psychiatrist and the designated unit manager/unit coordinator if out of hours) within 24 hours of commencement and then at no less than 72 hour periods thereafter. A behavioural description of what needs to change before the level and frequency of observation can be safely reduced. This must include a behavioural description of what needs to change before the level and frequency of observation can be safely reduced.
5.3. If supportive observation arrangements continue for a period of 28 days (High secure and forensic services) or 14 days (local services) an independent review involving a senior nurse (band 8a and above) and a senior doctor not directly involved in the care of the service user must be requested by the ward manager and ward RC to take place within one week. This review must indicate clear recommendations for the frequency of follow up reviews.
5.4. The responsible MDT retain the option to request an external case review or make a referral to another service in relation to the on-going management of risk presented by the service user.
6 How service users' perspectives will be taken into account
6.1. The service user must be provided with information about why increased levels of therapeutic engagement and supportive observation are being considered, the aims of intervention, how long it is likely to be maintained and how it will be reviewed, and what the individual will find most helpful during this time. A behavioural description of what needs to change before the level and frequency of observation can be safely reduced will be shared, and where possible agreed with them. This must be reflected in

West London NHS Trust_______________________________________ _____Page 9 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
the care plan and a copy shared with them. 6.2. The service user should be given the option for the nurse in charge to
inform the nearest relative, or carer about the implementation, aims and level of supportive observation. Where possible, the handover from one nurse or staff member to another should involve the service user so that they are aware of what is being said about them and have an opportunity to contribute to that handover.
6.3. The service user should be given the option to make a reflective entry in their clinical record during a period of supportive observations and following discontinuation. (This may be a written/verbal statement which is typed into the progress notes verbatim by the allocated nurse with the heading ‘service user reflective entry’).
6.4. Therapeutic engagement and supportive observations is considered to be a restrictive practice and the person’s capacity to consent to this intervention should be fully considered and the least restrictive intervention always used whilst maintaining the person’s safety, and the safety of others.
6.5. The nursing team must fully explore with the individual how privacy and dignity will be best maintained. If the person has a visitor or needs to attend to personal care this should be carefully considered and sensitively planned, recorded in the care plan and progress notes.
2. Introduction 2.1 The primary aim of Therapeutic engagement and supportive observation must be to
engage positively with the service user to reduce risk. This involves a two-way relationship, established between a service user and a staff member, which is meaningful, grounded in trust, and therapeutic in nature. Observation can be a restrictive intervention and therefore the least intrusive level of observation should always be adopted so that the restriction is both appropriate and proportionate to the individual’s clinical presentation
2.2 At times of distress or pronounced ill-health some service users may become a
serious risk of harm to themselves or others. Enhanced observations may be required for management of behavioural disturbance or during periods of distress to prevent harm to self or others. It should be an integral part of the care plan, to ensure the safe and sensitive monitoring of the service user’s behaviour and mental well-being, enabling a rapid response to change, whilst at the same time fostering therapeutic relationships between staff and service user.
2.3 NICE clinical guideline 25 (NICE 2005), ‘The short-term management of
disturbed/violent behaviour in in-patient psychiatric settings and emergency departments’ provides the contemporary evidence underpinning the development of this policy.

West London NHS Trust_______________________________________ _____Page 10 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
This policy addresses the following key issues;
Definitions of the types and levels of therapeutic engagement and supportive observations
Who can implement supportive observation above a general level
How supportive observation is implemented and recorded
Who should review the level of supportive observation
Who can increase or decrease the level of observation
When reviews should take place
How service users' perspectives will be taken into account
3. Scope 3.1 This is a Trust wide policy and applies to all staff working in the Trust’s clinical divisions
who have a responsibility for prescribing and/or undertaking supportive observations (including temporary, permanent, bank and agency staff).
3.2 All patients receiving in-patient care and treatment will be subject to a general level of
observation in each in patient setting. Some service users may require one or more of the other three levels of therapeutic engagement and supportive observations adopted by West London Mental Health NHS Trust. These are;
Intermittent observation,
Continuous observation (within eyesight)
Continuous observation (within arm’s length).
3.3 The responsibility of managers for ensuring that therapeutic engagement and supportive observation is conducted to the appropriate standards is also included within the scope of this policy.
4. Definitions 4.1 The practice of supportive observation can be defined as regarding the service user
attentively whilst minimising the extent to which they feel that they are under surveillance. It requires staff to be caringly vigilant and inquisitive, and have a thorough knowledge of the service users in their care, the service users’ current care plans and their observational requirements. Unusual circumstances and noises must always be investigated.
4.1.1 The staff member undertaking observation should be approachable, listen to and understand the service user’s views and experience, and know when self-disclosure and the therapeutic use of silence are appropriate; they should be able to convey to the service user that they will be valued and supported.
West London NHS Trust_______________________________________ _____Page 11 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
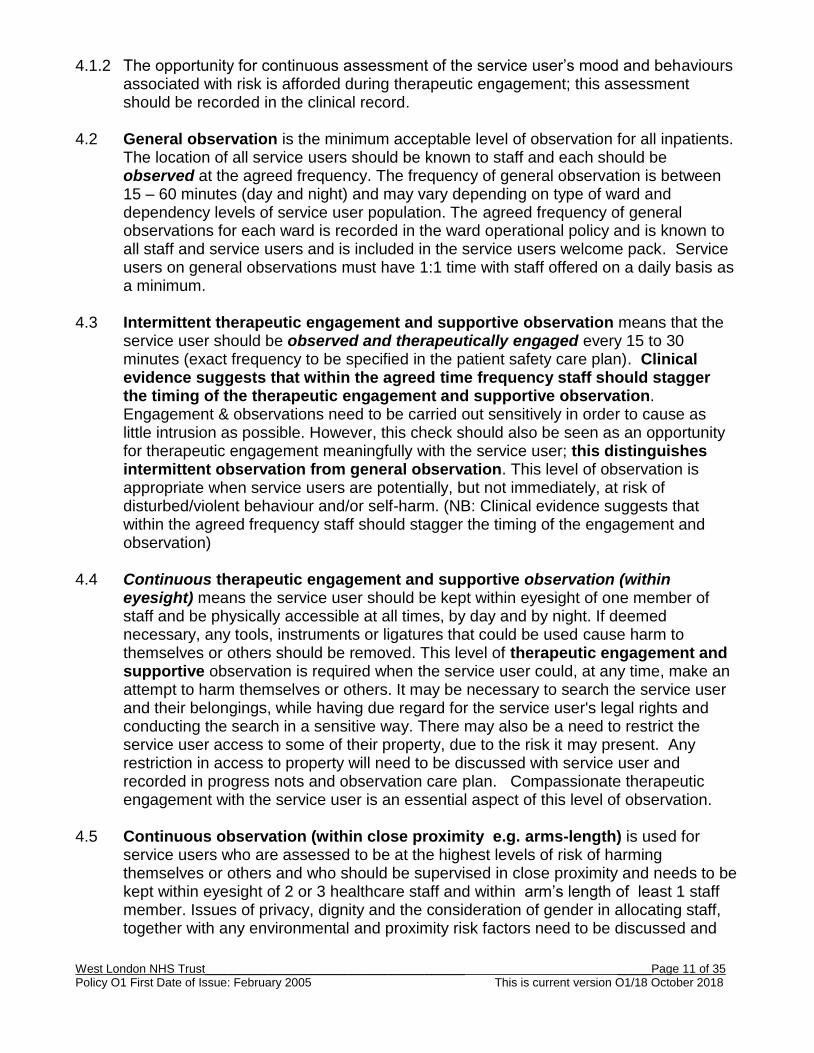
4.1.2 The opportunity for continuous assessment of the service user’s mood and behaviours associated with risk is afforded during therapeutic engagement; this assessment should be recorded in the clinical record.
4.2 General observation is the minimum acceptable level of observation for all inpatients. The location of all service users should be known to staff and each should be observed at the agreed frequency. The frequency of general observation is between 15 – 60 minutes (day and night) and may vary depending on type of ward and dependency levels of service user population. The agreed frequency of general observations for each ward is recorded in the ward operational policy and is known to all staff and service users and is included in the service users welcome pack. Service users on general observations must have 1:1 time with staff offered on a daily basis as a minimum.
4.3 Intermittent therapeutic engagement and supportive observation means that the service user should be observed and therapeutically engaged every 15 to 30 minutes (exact frequency to be specified in the patient safety care plan). Clinical evidence suggests that within the agreed time frequency staff should stagger the timing of the therapeutic engagement and supportive observation. Engagement & observations need to be carried out sensitively in order to cause as little intrusion as possible. However, this check should also be seen as an opportunity for therapeutic engagement meaningfully with the service user; this distinguishes intermittent observation from general observation. This level of observation is appropriate when service users are potentially, but not immediately, at risk of disturbed/violent behaviour and/or self-harm. (NB: Clinical evidence suggests that within the agreed frequency staff should stagger the timing of the engagement and observation)
4.4 Continuous therapeutic engagement and supportive observation (within eyesight) means the service user should be kept within eyesight of one member of staff and be physically accessible at all times, by day and by night. If deemed necessary, any tools, instruments or ligatures that could be used cause harm to themselves or others should be removed. This level of therapeutic engagement and supportive observation is required when the service user could, at any time, make an attempt to harm themselves or others. It may be necessary to search the service user and their belongings, while having due regard for the service user's legal rights and conducting the search in a sensitive way. There may also be a need to restrict the service user access to some of their property, due to the risk it may present. Any restriction in access to property will need to be discussed with service user and recorded in progress nots and observation care plan. Compassionate therapeutic engagement with the service user is an essential aspect of this level of observation.
4.5 Continuous observation (within close proximity e.g. arms-length) is used for service users who are assessed to be at the highest levels of risk of harming themselves or others and who should be supervised in close proximity and needs to be kept within eyesight of 2 or 3 healthcare staff and within arm’s length of least 1 staff member. Issues of privacy, dignity and the consideration of gender in allocating staff, together with any environmental and proximity risk factors need to be discussed and

West London NHS Trust_______________________________________ _____Page 12 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
incorporated into the care plan. Compassionate therapeutic engagement with the service user is an essential aspect of this level of observation Continues observation must consider the wider aspects of a service user’s physical health care need, and this aspect must be planned, monitored and documented accordingly.
5. Duties and responsibilities 5.1 Chief Executive
The Chief Executive is responsible for ensuring that the Trust has a policy in place for therapeutic engagement and supportive observations and those systems exist for monitoring the effectiveness of its implementation.
5.2 Director of Nursing and Patient Experience The Director of Nursing and Patient Experience is responsible for writing, reviewing and updating the policy and for ensuring it is implemented to the required standards. The Director of Nursing and Patient Experience is responsible for monitoring the quality and usage of therapeutic engagement and supportive observations and for ensuring that the trust provides training for staff in the use of enhanced engagement and observations.
5.3 Deputy Director of Nursing The Deputy Director of Nursing is responsible for providing assurance about the quality of therapeutic engagement and supportive observations and for taking action to improve practice where standards are found to have fallen below those agreed in this policy.
5.4 Service Directors Service Directors have operational responsibility for local compliance with this Policy and will ensure mechanisms in place within each service for:
• Identifying and deploying resources within the clinical division to safely deliver
this Policy. • Ensuring all clinical staff with responsibility for prescribing and carrying out
observation/engagement receive orientation to the content of this Policy • Monitoring the clinical division’s compliance and consistent application of the
Policy • Ensuring that all service users subject to prolonged periods of constant
observations are reviewed after 14 days and then at least once per calendar month by clinicians independent of the patient’s care.
5.4 Responsible Clinician
In collaboration with the primary nurse, the responsible clinician is responsible for evaluating the effectiveness of the use of therapeutic engagement and supportive observations.

West London NHS Trust_______________________________________ _____Page 13 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
5.5 Matrons/Senior Nurses Are accountable to the Service Director for providing assurance that their respective wards’ are compliant with the requirements of the Policy.
5.6 Primary Nurse
The primary nurse is responsible for working in collaboration with the patient to develop a patient safety care plan which includes details of any therapeutic engagement and supportive observation arrangements. In liaison with the responsible clinician, they are responsible for evaluating the effectiveness of those supportive observations.
5.7 Allocated Member of Staff The member of staff allocated to undertake enhanced therapeutic engagement and supportive observation duties is responsible for doing so in accordance with this policy.
5.8 Nurse in Charge of the Ward
The nurse in charge of the ward is responsible for allocating clinicians to undertake therapeutic engagement and supportive observation and the review of these. This includes ensuring that those allocated have the knowledge and skills required to undertake these duties, are sufficiently alert and are free from other duties which could potentially impede their ability to effectively implement therapeutic engagement and supportive observations. The nurse in charge of the ward has a significant role in implementing, reviewing and discontinuing the level of observation for service users. The nurse in charge of the ward will take responsibility to ensure a safe handover of patients at the commencement of duty (see paragraph 9).
5.9 Ward Manager
The Ward Manager is responsible for ensuring members of ward nursing staff have access to and understand this policy, and have opportunities to clarify and discuss its application through discussion with colleagues and via clinical supervision. The ward manager must ensure that staff develop and maintain up to date knowledge and skills relating to therapeutic engagement and supportive observation and that this is evidenced by the completion of a Knowledge and Skills Assessment Records (APPENDIX E). The Ward Manager is responsible for the quality of therapeutic engagement and supportive observation practice within their clinical area; this includes ensuring that there are sufficient staffing levels and that improvement actions are taken following monthly clinical audit.
5.10 Multidisciplinary Care Team Have a responsibility to understand their role in initiating and reviewing supportive observations. They must balance the potentially distressing effect on the individual of increased levels of observation, particularly if these are proposed for many hours or days, against the identified risk of self-injury or behavioural disturbance. Levels of observation and risk should be regularly reviewed by the Multidisciplinary team and a record made of decisions agreed in relation to increasing or decreasing the observation.
West London NHS Trust_______________________________________ _____Page 14 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
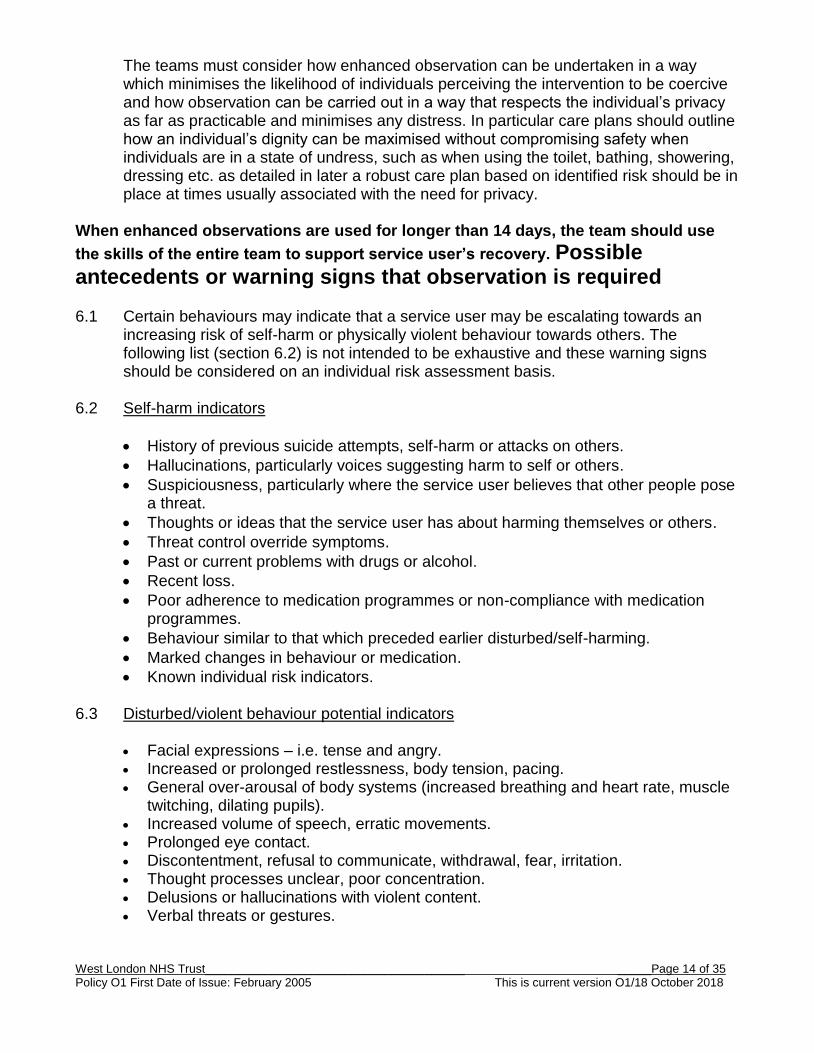
The teams must consider how enhanced observation can be undertaken in a way which minimises the likelihood of individuals perceiving the intervention to be coercive and how observation can be carried out in a way that respects the individual’s privacy as far as practicable and minimises any distress. In particular care plans should outline how an individual’s dignity can be maximised without compromising safety when individuals are in a state of undress, such as when using the toilet, bathing, showering, dressing etc. as detailed in later a robust care plan based on identified risk should be in place at times usually associated with the need for privacy.
When enhanced observations are used for longer than 14 days, the team should use
the skills of the entire team to support service user’s recovery. Possible antecedents or warning signs that observation is required 6.1 Certain behaviours may indicate that a service user may be escalating towards an
increasing risk of self-harm or physically violent behaviour towards others. The following list (section 6.2) is not intended to be exhaustive and these warning signs should be considered on an individual risk assessment basis.
6.2 Self-harm indicators
History of previous suicide attempts, self-harm or attacks on others.
Hallucinations, particularly voices suggesting harm to self or others.
Suspiciousness, particularly where the service user believes that other people pose a threat.
Thoughts or ideas that the service user has about harming themselves or others.
Threat control override symptoms.
Past or current problems with drugs or alcohol.
Recent loss.
Poor adherence to medication programmes or non-compliance with medication programmes.
Behaviour similar to that which preceded earlier disturbed/self-harming.
Marked changes in behaviour or medication.
Known individual risk indicators. 6.3 Disturbed/violent behaviour potential indicators
Facial expressions – i.e. tense and angry. Increased or prolonged restlessness, body tension, pacing. General over-arousal of body systems (increased breathing and heart rate, muscle
twitching, dilating pupils). Increased volume of speech, erratic movements. Prolonged eye contact. Discontentment, refusal to communicate, withdrawal, fear, irritation. Thought processes unclear, poor concentration. Delusions or hallucinations with violent content. Verbal threats or gestures.

West London NHS Trust_______________________________________ _____Page 15 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Behaviour similar to that which preceded earlier disturbed/violent episodes. Reporting anger or violent feelings. Blocking escape routes known individual risk indicators
6.4 Therapeutic engagement and supportive observations may also be considered when
close physical health monitoring is required and/or to monitor the environment. For example, if someone is suspected of possession of illicit drugs, observations may be used instead of a search process, or when supporting someone who is a high risk of falls.
7. Implementing Therapeutic engagement and
supportive observation.
7.1 Increased levels of Therapeutic engagement and supportive observation should only be implemented after positive engagement with the service user, and following unsuccessful interventions to reduce the potential for self-harming and/or disturbed/violent behaviour.
7.2 The least intrusive level of observation that is appropriate and proportionate to the
situation should be adopted so that due sensitivity is given to a service user's dignity and privacy whilst maintaining their safety and the safety of others.
7.3 The nursing team on duty recognise antecedents or warning signs in the presentation
of a service user that indicates an escalating risk of disturbed/violent behaviour and/or self-harm.
N.B. An urgent necessity to implement therapeutic engagement and supportive observation to protect the service user or others from harm will usually preclude the option to arrange a formal review with ward/duty doctor or with MDT colleagues. In this case the Nurse in charge will make the decision to implement Supportive observation.
7.4 Where clinical presentation time permits a discussion is held between staff on duty
and, where possible, MDT members. All decisions about the specific level of Therapeutic engagement and supportive observation should take into account:
The service user's current mental state.
Any prescribed medications and their effects.
The current assessment of risk.
The views of the service user as far as possible. 7.5 The nurse in charge makes a decision with the team on duty and communicates, with
rationale, to the ward/duty doctor for discussion and further clinical decision making.

West London NHS Trust_______________________________________ _____Page 16 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
West London NHS Trust_______________________________________ _____Page 17 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
7.6 A review, including assessment of mental state and risk, is undertaken by nurse in charge and ward/duty doctor with the service user.
7.7 Subsequently a decision to implement Therapeutic engagement and supportive
observation is made by the nurse in charge. 7.8 The rationale for implementation together with a behavioural description of what needs
to change before the level of Therapeutic engagement and supportive observation can be safely reduced is explained to the service user and recorded in the clinical record and the care plan.
7.9 When making decisions about Therapeutic engagement and supportive observation
levels, clear directions should be recorded that specify:
The level and frequency of the observations.
The rationale and any particular needs identified.
The name/title of the persons who will be responsible for carrying out the observation and engagement.
This must be discussed at every Nursing handover or MDT safety huddle. 7.10 The observing nurse makes a record of therapeutic engagement and supportive observation at the agreed level and frequency in the agreed recording form. 7.11 At the end of each period of therapeutic engagement and supportive observation the
allocated nurse hands over to the member of staff taking over the next period, involving the service user where possible/appropriate.
7.12 A review of the therapeutic engagement and supportive observations occurs at a minimum once per day and is clearly documented in the service user’s progress notes. 7.13 When Therapeutic engagement and supportive observation is implemented between
the hours of 09:00 and 17:00, Monday to Friday the Nurse in charge must inform:
1) The service user's Responsible Clinician/on-call doctor as soon as possible. 2) The nominated hospital/unit manager/unit co-ordinator so that staffing resource for
future shifts can be reviewed. 7.14 If out of hours the nurse in charge must inform;
1) The on call consultant psychiatrist 2) The nominated hospital/unit manager/unit co-ordinator so that staffing
arrangements for future shifts can be reviewed.

West London NHS Trust_______________________________________ _____Page 18 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
8. Undertaking Therapeutic Engagement and Supportive Observation
8.1 Supportive observation skills during therapeutic engagement should be used to recognise, prevent and manage disturbed/violent and/or self-harming behaviour (see antecedents and warning signs above).
8.2 Therapeutic engagement and supportive observation should be undertaken by mental
health professional that are competent (see section 19 below) to undertake the role. The Nurse in charge of the ward at the time will ensure supportive observations are undertaken to a high standard.
8.3 Staff undertaking observation:
Must not use their personal mobile phone
Must take an active role in engaging therapeutically with the service user and should be appropriately briefed about the service user's history, background specific risk factors and particular needs; i.e. - physical risks such as risk of falls or risk of choking
Must be familiar with the ward, the ward policy for emergency procedures and potential risks in the environment
Must be competent to vary the level of engagement with the service user as the level of observation changes.
Should be approachable, listen to the service user, know when appropriate communication and the therapeutic use of silence are helpful and be able to convey to the service user that they will be valued and supported (see appendix G for guidance on engagement in challenging situations)
Must make a record of therapeutic engagement and supportive observation at the agreed level and frequency in the Therapeutic observation & supportive observation recording form (appendix D)
8.4 A summary of the observations made during each period of duty is recorded in the
clinical record progress notes by an allocated registered nurse. This should relate to:
The service user's current mental state.
Any prescribed medications and their effects.
The current assessment of risk including any antecedents and warning signs (see above).
The views of the service user as far as possible.
Meaningful engagement statements.
Highlight physical risks, such as risk of falls or risk of choking. 8.5 An individual staff member should not undertake a continuous period of observation
above the general level for longer than two hours.

West London NHS Trust_______________________________________ _____Page 19 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
8.6 Staff members should be aware that service users sometimes find observation provocative, and intrusive, also that it can lead to feelings of isolation and dehumanisation.
8.7 An appropriately trained member of the MDT staff should undertake a 1:1 session with
the individual which will include a suitable mental state review on a shift by shift basis.
9. Duties of the nurse in charge 9.1 At the beginning of a shift of duty the Nurse in Charge will receive a nursing handover of all
patients; this must include a visual/verbal accounting round of all patients. The purpose of the check round is to determine location and safety. The expectation is that the Nurse in Charge will assure themselves by physically seeing the patients and where a patient is in bed / at rest receiving a verbal response or gesture (such as thumbs up) response from a patient.
9.2 There may be some circumstances where the Nurse in Charge considers it to be clinically
inadvisable to wake a patient. In consultation with colleagues, the nurse who has decided not to disturb/wake the patient must undertake as a minimum the following:
9.2.1 A check for respiration (rise and fall of chest) or check of peripheral circulation (Skin colour,
temperature and moisture).
9.2.2 The nurse in charge needs to assure themselves of the patient’s health and safety and documents this accordingly.
10 Service user needs
10.1 The service user should be provided with information (a service user information leaflet
is available at appendix F) about why increased levels of therapeutic engagement and supportive observation are being considered, the aims of the intervention and how long it is likely to be maintained. A behavioural description of what needs to change before the level and frequency of observation can be safely reduced will be shared, and where possible agreed with them. A collaborative risk assessment and patient safety plan should be completed with the service user; this should include information about how it will be reviewed, and what the individual will find most helpful during this time. A copy of the care plan should be provided to the service user, subsequent reviews of the care plan should be completed with the service user.
10.2 The service user may be given the option (following appropriate consultation with the
MDT) for the nurse in charge to inform the nearest relative, friend or carer about the implementation, aims and level of supportive observation.
10.3 Where possible, the handover from one nurse or staff member to another should
involve the service user so that they are aware of what is being said about them and have an opportunity to contribute to that handover.

West London NHS Trust_______________________________________ _____Page 20 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
10.4 The service user should be given the option to make a reflective entry in their clinical record during a period of supportive observations and following discontinuation. . (This may be a written/verbal statement which is typed into the progress notes verbatim by the allocated nurse with the heading ‘service user reflective entry’).
10.5 Therapeutic engagement and supportive observations is considered to be a restrictive practice and the person’s capacity to consent to this intervention should be fully considered and the least restrictive intervention always used whilst maintaining the person’s safety and the safety of others.
10.6 The multidisciplinary team should fully explore with the individual how privacy and dignity will be best maintained. If the person has a visitor or needs to attend to personal care this should be carefully considered and sensitively planned.
11 Reviewing the level of therapeutic engagement and supportive observations
11.1 A review of the need to continue Therapeutic engagement and supportive observations is completed during each nursing handover. In addition, where a service user is subject to Continuous observation (within eyesight or within arms-length) the nurse in charge (or another registered nurse) will also have undertaken an assessment to determine mental state and current risk.
11.2 If a change in Therapeutic engagement and supportive observations level and
frequency is indicated by the observing nurse, the registered nurse undertaking the above assessment or during the handover review the following actions will be taken by the Nurse in Charge:
11.3 Increase in level and frequency. 11.3.1The urgent necessity to increase the level and frequency of Therapeutic engagement
and supportive observation to protect the service user or others from harm will usually preclude the option to arrange a formal review with ward/duty doctor or with MDT colleagues. In these circumstances the nurse in charge is responsible for making the decision to implement increased level and frequency of observation.
11.3.2 Where time permits a discussion is held between staff on duty and, where possible,
MDT members. 11.3.3 The nurse in charge communicates a decision, with rationale, to the ward/duty
doctor for discussion and clinical decision making. 11.3.4 A review, including assessment of mental state and risk, is undertaken by nurse in
charge and ward/duty doctor with the service user.

West London NHS Trust_______________________________________ _____Page 21 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
11.3.5 Subsequently a decision to maintain/increase Therapeutic engagement and supportive observation is made by the nurse in charge.
11.3.6The rationale for implementation together with a behavioural description of what needs
to change before the level of Therapeutic engagement and supportive observation can be safely reduced is explained to the service user and nursing team and recorded in the clinical record and the care plan.
11.3.7 In addition, the nurse in charge records and communicates to the service user, nursing
team and colleagues as detailed at 7.8 – 7.14 above. 11.4 Reduction in level and/or frequency:
11.4.1 If following a full review of mental state and risk and conversation with the individual
about how safety will be maintained the nursing team feel that a reduction in level and/or frequency is appropriate the nurse in charge, makes a recommendation, with rationale, to the ward/duty doctor for discussion and joint clinical decision making. This may include the necessity for the ward doctor to complete a joint review where clinically indicated or requested by nursing staff.
11.4.2 In addition, the nurse in charge records and communicates to the service user, nursing
team and colleagues as detailed at 7.8 – 7.14 above.
12 MDT review
12.1 A review of Therapeutic engagement and supportive observation arrangements above the general level should be undertaken by MDT members (or by the on call consultant psychiatrist and the designated unit manager/unit coordinator if out of hours) within 24 hours of commencement. There after a MDT review must occur every 72 hours and be recorded in the patient’s notes.
12.2 The nurse in charge ensures that the review decision together with the rationale for
changing/maintaining level and frequency of Therapeutic engagement and supportive observation is explained to the service user, communicated to staff on duty and recorded in the clinical record and the patient safety care plan.
12.3 There will be occasions where a service user requires high levels of therapeutic
engagement and supportive observations for extended periods of times as part of a planned clinical intervention (this is likely to be connected to long term segregation). In these exceptional cases the Responsible Clinician and Ward manager should agree with the Deputy Director of nursing and Clinical director the appropriate person to undertake a review.
13 Independent review
13.1 If Therapeutic engagement and supportive observation arrangements continue for a period of 28 days in High secure and forensic services (14 days in local services) an

West London NHS Trust_______________________________________ _____Page 22 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
independent review involving a senior nurse (band 7 or above) and senior doctor not directly involved in the care of the service user should be considered by the Clinical team. The independent review outcome is communicated to the ward manager, ward RC and the nurse in charge at the time of the review.
13.1 The nurse in charge ensures that the independent review outcome together with the
rationale for changing/maintaining level and frequency of Therapeutic engagement and supportive observation is explained to the service user, communicated to staff on duty and recorded in the clinical record and the patient safety care plan.
14 External review
14.1 The responsible MDT retain an option to request an external case review or to make a referral for transfer to another appropriate service (internal or external) where the risks presented, for which therapeutic engagement and supportive observations form a part of the management of those risks, persist over an extended period of time without reduction and where the quality of life of the individual service user is compromised due to the environmental and/or resource limits available to continue to safely manage those risks.
15 Night time
15.1 The agreed level and frequency of therapeutic engagement and supportive observations can only be reviewed by following the process identified at 10.3 and 10.4 above; it cannot be reviewed based solely on the time of day.
15.2 Staff engaged in Therapeutic Engagement and Supportive Observation will exercise
sensitivity so that sleep and rest is not unnecessarily disrupted by light or noise.
16 Service user asleep
16.1 A good sleep pattern is important, staff should take steps to ensure that disturbance (Noise, Bright lights and speech volume) are moderated to support a good sleep pattern.
16.2 When a service user is asleep the member of staff carrying out Therapeutic
engagement and supportive observation must monitor their physical state noting changes in body posture and breathing for example, and be alert to changes within the service user bedroom layout that may suggest escalation of risk.
16.3 If the observing member of staff cannot identify movement/breathing they must
immediately seek assistance to prepare to enter the room.

West London NHS Trust_______________________________________ _____Page 23 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
17 Leave
17.1 Except in cases of emergency, patients on therapeutic engagement and supportive observations must only be allowed time outside of the clinical environment within which they are receiving care if a previously agreed risk assessment and patient safety care plan facilitating this is in place.
17.2 The clinical environment within which the service user is receiving care may extend
beyond the inpatient ward to a local off ward therapy setting, for example. Where this is the case the decision to allow access must be part of the above risk assessment process.
17.3 The risk assessment and patient safety care plan must have been agreed by the
Responsible Clinician and the primary nurse/nurse in charge as sufficient to minimise any potentially increased risk arising from the patient being outside the clinical environment within which they are receiving care.
17.4 In certain circumstances (e.g. to attend another hospital) a patient who is subject to
therapeutic engagement and supportive observations may be allowed time outside of their usual care setting. This decision must be part of the risk assessment process and the Responsible Clinician and Primary nurse/nurse in charge must judge that the agreed escorting plan is sufficient to minimise the inherent risk.
18 Legal Status
18.1 While enhanced therapeutic engagement & supportive observations may be unavoidably restrictive, they must never become a form of de-facto detention for informal patients. The necessity for therapeutic engagement and supportive observations engagement can be seen as an indicator for formal detention. If an informal patient is considered to require a period of therapeutic engagement and supportive observations enhanced a review of their legal status by the clinical team should take place immediately and a record made in the notes of the review and outcome. Full capacity to consent to this intervention must be considered - see policy M9 WLMHT mental capacity policy.
19 Record keeping
19.1 There is an absolute obligation on observing staff to accurately record details of the therapeutic engagement and supportive observation to which they are allocated.
19.2 Recording criteria for all types of engagement and observation. 19.2.1 The allocated nurse makes an entry in the clinical notes at least once every shift that is
related to the patient’s behaviour and mental state.

West London NHS Trust_______________________________________ _____Page 24 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
19.2.2 The nurse(s) completing general observations will record the whereabouts of every service user on the general engagement and observation form (Appendix A) and inform the nurse in charge of any concerns or unplanned absence, which they will record in the patient’s records. The nurse in charge ensures that the general engagement and observation form is completed accurately. The ward manager must ensure the safe storage and easy retrieval of the general engagement and observation forms, which must be kept for a minimum of two years, as a secondary health record (please see Health Records Policy).
19.3 Intermittent and continuous therapeutic Engagement and supportive observation. 19.3.1The Therapeutic engagement and supportive observation initial care plan is completed
(Appendix B) when enhanced engagement and observation is implemented. 19.3.2The Therapeutic engagement and supportive observation amended care plan is
completed (Appendix C) when an enhanced engagement and observation is increased or reduced.
19.3.3The enhanced Therapeutic engagement and supportive observations record is
completed (Appendix D) when enhanced Therapeutic engagement and supportive observation is undertaken and when responsibility is handed over between clinical staff.
19.3.4 All staff on the shift are consulted before the completion of the records and handover to
the new shift.
20 Training for therapeutic engagement & supportive observation
20.1 Staff responsible for carrying out Therapeutic engagement and supportive
observations must receive training so that they are equipped with the skills and confidence to engage with service users. Engaging and observing a patient at risk is a highly skilled activity. Essential components of adequate training include developing knowledge and skills in:
Risk assessment,
Therapeutic engagement and management of care for patients at risk of harming self and others.
Factors associated with self-harm and harm to others.
Indications for therapeutic engagement and supportive observation.
Establishing and maintaining a therapeutic relationship with the service user.
Different intensities of therapeutic engagement and supportive observation.
Attitudes to therapeutic engagement and supportive observation.
Therapeutic opportunities in engagement & supportive observation.
West London NHS Trust_______________________________________ _____Page 25 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Roles and responsibilities of the multi-disciplinary team in relation to therapeutic engagement and supportive observation.
Making the environment safe.
Recording therapeutic engagement and supportive observation.
The use of reviews and audit,
20.2 All staff who provide therapeutic engagement and supportive observation are required to attend a Trust clinical risk workshop, which includes guidance on therapeutic engagement and supportive observation. Attendance is monitored through the Trust performance departments.
20.3 An Additional e-learning module to support therapeutic engagement and supportive
observation practice is available in the nursing home page via the Trust Exchange. This will include an examination of the differences between general observations and the three additional levels of therapeutic engagement and supportive observation used within the Trust.
20.4 A mandatory annual therapeutic engagement and supportive observation practice
assessment process is available. This provides an assurance system for practice competency and will replace the knowledge and Skills Assessment Record. (Appendix E).
21 Monitoring and audit 20.1 Therapeutic engagement and supportive observation is used to support patients in
inpatient settings, the standard of practice related to it must be audited on a regular basis to ensure the interventions remains supportive and is carried out correctly. The appended forms are designed to support the recording and auditing of engagement and observation. These provide key information both in monitoring the frequency of the usage of therapeutic engagement and supportive observation and in incident reviews.
20.2 The Director of Nursing and Patient Experience has responsibility for monitoring the
quality and use of therapeutic engagement and supportive observation. 20.3 Deputy Directors of Nursing have responsibility for ensuring that practice audits occur
within the in- patient clinical environments and that where necessary actions are developed and implemented to improve practice. Deputy Directors of Nursing are responsible for ensuring that unannounced assurance visits are made to inpatient wards to measure the quality of therapeutic engagement and supportive observation practice.
20.4 Ward Managers are responsible for assuring practice and for ensuring actions and
improvements identified from audits and assurance activities are implemented in practice.

West London NHS Trust_______________________________________ _____Page 26 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Appendix A (morning) General Engagement and Observation Form WARD: ___________________ DATE: _____/_____/_____ NB CONTINUE ON ANOTHER SHEET IF YOU HAVE MORE
PATIENTS
L: Location of patient: enter appropriate code SI: Staff initials: the member of staff recording the whereabouts of the patient should write their initials
here
NHS /
Hospital No. Patient Name 07.00 08.00 09.00 10.00 11.00 12.00 13.00 14.00
Surname First Name L SI L SI L SI L SI L SI L SI L SI L SI 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Patient Location Codes Everyone is assumed to be awake unless specified as being asleep, by adding a capital S to the end of the location code, e.g. BeS for being asleep in their bedroom. The most frequent codes are shown in bold.
Art room Ar Day room Da Laundry room La Reception Re Tribunal suite Tr
Association As Dining room Di Leave Le Seclusion room Se Visit room V
AWOL Aw Fresh air facility Fr Meeting room Me Service corridor Sr Washroom W
Bathroom Ba Group room Gr Music room Mu Shower room Sh Others:
Bedroom Be Healthcare suite He Occupational therapy Oc Side room Si
Canteen Ca Interview room In Off ward for activity Of
Corridor Co Kitchen area Ki Phone room Ph Toilet To
NB This sheet can be modified to include more frequent checks, for example, but the codes above must be used and not replaced. This is for continuity across wards.

West London NHS Trust_______________________________________ _____Page 27 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Appendix A: (afternoon/evening) General Observation form: WARD: ___________________ DATE: _____/_____/_____ NB CONTINUE ON ANOTHER SHEET IF YOU HAVE MORE PATIENTS
L: Location of patient: enter appropriate code SI: Staff initials: the member of staff recording the whereabouts of the patient should write their initials
here
NHS /
Hospital No. Patient Name 15.00 16.00 17.00 18.00 19.00 20.00 21.00 22.00
Surname First Name L SI L SI L SI L SI L SI L SI L SI L SI 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Patient Location Codes Everyone is assumed to be awake unless specified as being asleep, by adding a capital S to the end of the location code, e.g. BeS for being asleep in their bedroom. The most frequent codes are shown in bold.
Art room Ar Day room Da Laundry room La Reception Re Tribunal suite Tr
Association As Dining room Di Leave Le Seclusion room Se Visit room V
AWOL Aw Fresh air facility Fr Meeting room Me Service corridor Sr Washroom W
Bathroom Ba Group room Gr Music room Mu Shower room Sh Others:
Bedroom Be Healthcare suite He Occupational therapy Oc Side room Si
Canteen Ca Interview room In Off ward for activity Of
Corridor Co Kitchen area Ki Phone room Ph Toilet To
NB This sheet can be modified to include more frequent checks, for example, but the codes above must be used and not replaced. This is for continuity across wards.

West London NHS Trust_______________________________________ _____Page 28 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Appendix A: (night) General Observation form: WARD: ___________________ DATE: _____/_____/_____ NB CONTINUE ON ANOTHER SHEET IF YOU HAVE MORE PATIENTS
L: Location of patient: enter appropriate code SI: Staff initials: the member of staff recording the whereabouts of the patient should write their initials
here
NHS /
Hospital No. Patient Name 23.00 00.00 01.00 02.00 03.00 04.00 05.00 06.00
Surname First Name L SI L SI L SI L SI L SI L SI L SI L SI 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Patient Location Codes Everyone is assumed to be awake unless specified as being asleep, by adding a capital S to the end of the location code, e.g. BeS for being asleep in their bedroom. The most frequent codes are shown in bold.
Art room Ar Day room Da Laundry room La Reception Re Tribunal suite Tr
Association As Dining room Di Leave Le Seclusion room Se Visit room V
AWOL Aw Fresh air facility Fr Meeting room Me Service corridor Sr Washroom W
Bathroom Ba Group room Gr Music room Mu Shower room Sh Others:
Bedroom Be Healthcare suite He Occupational therapy Oc Side room Si
Canteen Ca Interview room In Off ward for activity Of
Corridor Co Kitchen area Ki Phone room Ph Toilet To
NB This sheet can be modified to include more frequent checks, for example, but the codes above must be used and not replaced. This is for continuity across wards.
West London NHS Trust____________________________________________ _Page 29 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
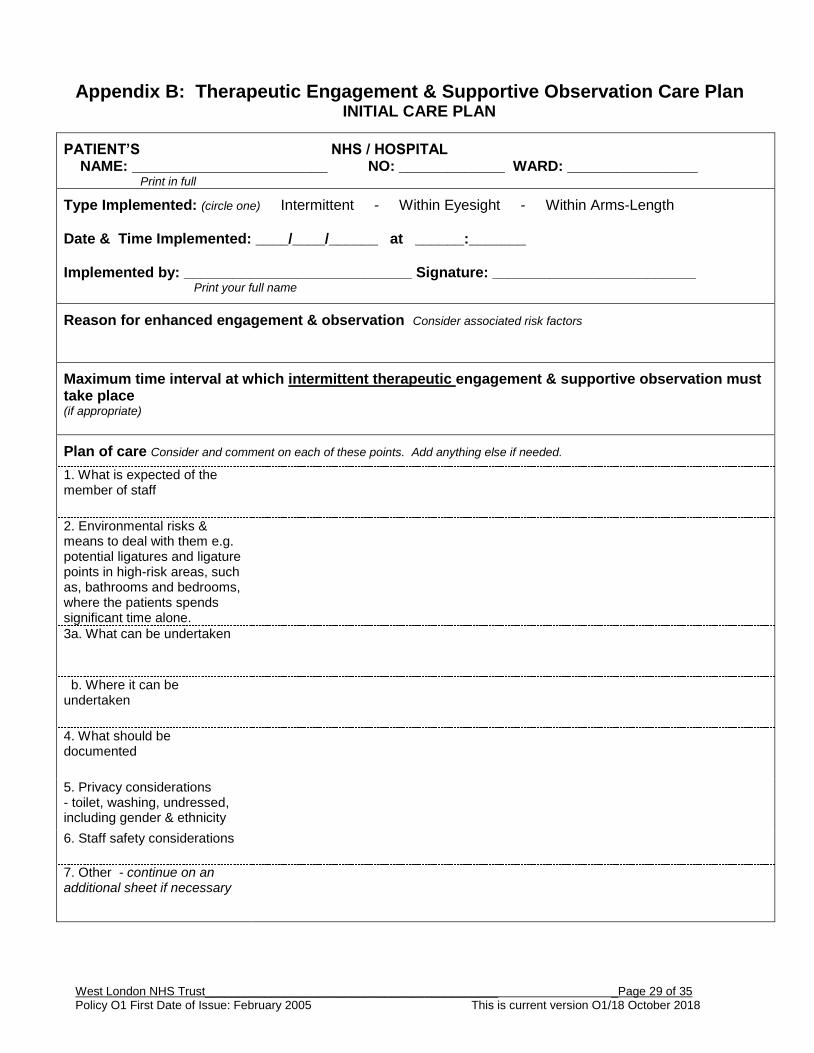
Appendix B: Therapeutic Engagement & Supportive Observation Care Plan INITIAL CARE PLAN
PATIENT’S NHS / HOSPITAL NAME: ________________________ NO: _____________ WARD: ________________ Print in full
Type Implemented: (circle one) Intermittent - Within Eyesight - Within Arms-Length Date & Time Implemented: ____/____/______ at ______:_______ Implemented by: ____________________________ Signature: _________________________ Print your full name
Reason for enhanced engagement & observation Consider associated risk factors
Maximum time interval at which intermittent therapeutic engagement & supportive observation must take place (if appropriate)
Plan of care Consider and comment on each of these points. Add anything else if needed.
1. What is expected of the member of staff
2. Environmental risks & means to deal with them e.g. potential ligatures and ligature points in high-risk areas, such as, bathrooms and bedrooms, where the patients spends significant time alone.
3a. What can be undertaken
b. Where it can be undertaken
4. What should be documented
5. Privacy considerations - toilet, washing, undressed, including gender & ethnicity
6. Staff safety considerations
7. Other - continue on an additional sheet if necessary

West London NHS Trust____________________________________________ _Page 30 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Appendix C: Therapeutic Engagement & supportive Observation Care Plan AMENDED CARE PLAN
PATIENT’S NHS / HOSPITAL NAME: ________________________ NO: _____________ WARD: ________________ Print in full
Type Amended to: (circle one) Intermittent - Within Eyesight - Within Arms-Length Date & Time Amended: ____/____/______ at ______:______ Amended by: _____________________________ Signature: __________________________ Print your full name
Amended by: _____________________________ Signature: __________________________ Print your full name
Reason for amendment to engagement & observation Consider updated risk factors
Maximum time interval at which intermittent engagement & observation must take place (if appropriate)
Plan of care Consider and comment on each of these points. Add anything else if needed.
1. What is expected of the member of staff
2. Environmental risks and means to
deal with them e.g. potential ligatures and ligature points in high-risk areas, such as, bathrooms and bedrooms where the patients spends significant time alone
3a. What can be undertaken
b. Where it can be undertaken
4. What should be documented
5. Privacy considerations – toilet, washing, undressed, including gender and ethnicity
6. Staff safety considerations
7. Other - continue on an additional sheet if necessary

West London NHS Trust____________________________________________ _Page 31 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Appendix D: Therapeutic Engagement & Supportive Observation Record
PATIENT’S NHS / HOSPITAL NAME: ________________________ NO: _____________ WARD: ______________ Print in full
TYPE OF Observation: (circle one) Intermittent - Within Eyesight - Within Arms-Length
SUMMARY OF KEY RISKS (observing nurses must read the full patient safety care plan in addition to this summary).
DATE
TIME Taken over/ handed over
ALLOCATED MEMBER OF STAFF
Name: print full name Sig.: Signature
1
NOTE OF ENGAGEMENT UNDERTAKEN AND OBSERVATIONS MADE
To include times when intermittent checks were made; include the patients perspective
____/____/____
______:______
Name:
Sig:
____/____/____
______:______
Name:
Sig:
____/____/____
______:______
Name:
Sig:
____/____/____
______:______
Name:
Sig:
____/____/____
______:______
Name:
Sig:
____/____/____
______:______
Name:
Sig:
____/____/____
______:______
Name:
Sig:
1 To show that you understood the care plan; received a hand-over; and undertook the E&O noted.
West London NHS Trust___________________________________________ __Page 32 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Appendix E - Therapeutic engagement & supportive observation - Training and competency assessment framework
1.0 Policy 1.1 A comprehensive review of existing policy has been undertaken to reflect NICE
Guidance 25 and in response to regulation 28 directions. The revised policy seeks to make explicit the differences between the levels of Therapeutic Engagement and Supportive Observation and the role of healthcare staff in relation to implementation and practice.
1.2 This paper outlines the arrangements for training and competency assessment relating to Therapeutic Engagement and Supportive Observation practice (this replaces the Knowledge and skill assessment record)
2.0 Training and orientation 2.1 Induction (Therapeutic Engagement & Supportive Observations module) 2.2 Orientation to Therapeutic Engagement & Supportive Observations practice during
secondary induction 2.3 Mandatory Clinical risk day (Therapeutic Engagement & Supportive Observations
module) 2.4 Optional Power-Point module summarising key elements via nursing exchange page 3.0 Competency assessment 3.1 Practice observation by line manager/clinical supervisor and discussed in clinical
supervision. 3.2 CSU practice audit arrangements led by deputy Director of Nursing and Head of Nursing.
a) Pass – recorded in individual mandatory training record b) Fail - Notification to line manager highlighting failed elements to assist individual
and line manager to agree a development action plan. c) Re-sit within one month. d) Pass – recorded in individual mandatory training record
e) Fail – capability review by line manager.
4.0 Practice assurance 4.1 Deputy Directors and head of Nursing take lead responsibility for ensuring the training
and competency assessment framework is understood and implemented within areas of responsibility.
4.2 Monthly Therapeutic Engagement & Supportive Observations audits completed for each in patient ward.
4.3 Monthly audits reviewed in Monthly CSU Nursing Governance and patient safety and safeguarding governance meetings.

West London NHS Trust___________________________________________ __Page 33 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
4.4 Ward and area managers have access to live mandatory training data to ensure completion rates for clinical risk training and e-competency assessment.
4.5 Mandatory training attendance data and summary of Therapeutic Engagement & Supportive Observations ward audits to be included in TW & CSU Nursing Governance and CSU & TW SMT performance reports.
4.6 There is a PowerPoint slide deck to be used in Induction and as an e-learning module. Content should also be reflected in mandatory Clinical risk training workshop.

West London NHS Trust___________________________________________ __Page 34 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Appendix F Staff and Service User Information Leaflet

West London NHS Trust___________________________________________ __Page 35 of 35 Policy O1 First Date of Issue: February 2005 This is current version O1/18 October 2018
Appendix G - Guidance for staff on engagement in challenging situations
1. Leave as much personal space as possible.
2. Ensure you appear receptive (to validate the patient) as much as possible
a. Unclenched visible hands (not a threat)
b. Stand at an angle to the patient (not confrontational)
c. A calm demeanour and facial expression (avoiding excessive eye contact)
d. Matching non-verbal and verbal behaviour
3. Actively listen to what the patient says (aim to listen twice as much as you talk)
a. Don’t interrupt, rather listen wherever possible, and demonstrate you are listening.
b. Convey what you have understood from the patient’s verbal/non-verbal behaviour
c. Agree with whatever information you can agree:
Agreeing with the truth (example: 3 attempts at a blood test – yes, she/he has
tried 3 times, do you mind me trying?)
Agreeing in principle (example: yes, everyone deserves respect)
Frightening delusions (example: that must be very scary)
4. Speaking to the patient
a) Let one person do the talking (less confusing)
b) Reassure the patient that your aim is to keep him/her safe
c) Explain to the patient what is happening/what to expect
d) Use short sentences and simple vocabulary, and a calm voice
e) Allow plenty of time and repetitions of the information to enable the patient to
process the information.
5. Agree boundaries
a) Confirm acceptable behaviours
b) Confirm consequences of behaviours, with an emphasis on this being to help the
patient.
6. Offer choices/hope where possible (as an alternative to fight/flight).