please!fax to:!207/899/0968!...
TRANSCRIPT
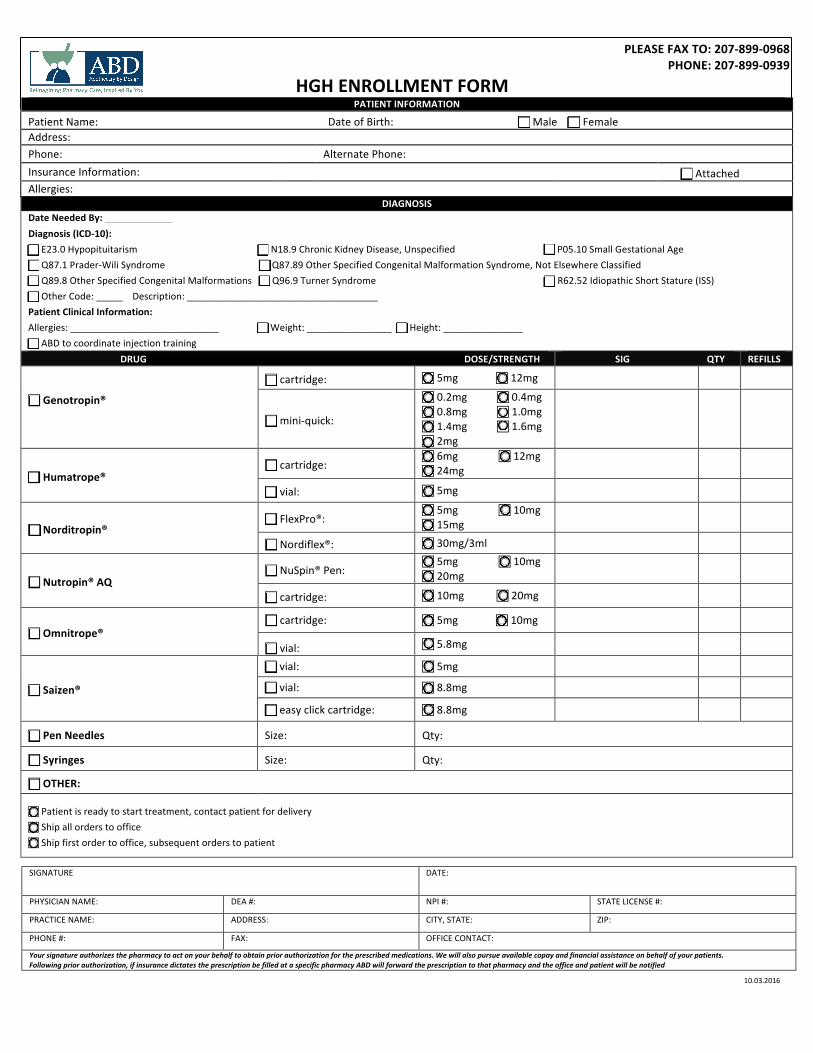
PLEASE FAX TO: 207-‐899-‐0968 PHONE: 207-‐899-‐0939
HGH ENROLLMENT FORM PATIENT INFORMATION
Patient Name: Date of Birth: ! Male ! Female Address: Phone: Alternate Phone: Insurance Information: ! Attached Allergies:
DIAGNOSIS Date Needed By: Diagnosis (ICD-‐10): ! E23.0 Hypopituitarism ! N18.9 Chronic Kidney Disease, Unspecified ! P05.10 Small Gestational Age ! Q87.1 Prader-‐Wili Syndrome ! Q87.89 Other Specified Congenital Malformation Syndrome, Not Elsewhere Classified ! Q89.8 Other Specified Congenital Malformations ! Q96.9 Turner Syndrome ! R62.52 Idiopathic Short Stature (ISS) ! Other Code: _____ Description: ____________________________________ Patient Clinical Information: Allergies: ____________________________ ! Weight: ________________ ! Height: _______________ ! ABD to coordinate injection training DRUG DOSE/STRENGTH SIG QTY REFILLS
! Genotropin®
! cartridge: ! 5mg ! 12mg
! mini-‐quick:
! 0.2mg ! 0.4mg ! 0.8mg ! 1.0mg ! 1.4mg ! 1.6mg ! 2mg
! Humatrope® ! cartridge:
! 6mg ! 12mg ! 24mg
! vial: ! 5mg
! Norditropin® ! FlexPro®:
! 5mg ! 10mg ! 15mg
! Nordiflex®: ! 30mg/3ml
! Nutropin® AQ ! NuSpin® Pen:
! 5mg ! 10mg ! 20mg
! cartridge: ! 10mg ! 20mg
! Omnitrope® ! cartridge: ! 5mg ! 10mg
! vial: ! 5.8mg
! Saizen®
! vial: ! 5mg
! vial: ! 8.8mg
! easy click cartridge: ! 8.8mg
! Pen Needles Size: Qty:
! Syringes Size: Qty:
! OTHER:
! Patient is ready to start treatment, contact patient for delivery ! Ship all orders to office ! Ship first order to office, subsequent orders to patient
SIGNATURE DATE:
PHYSICIAN NAME: DEA #: NPI #: STATE LICENSE #:
PRACTICE NAME: ADDRESS: CITY, STATE: ZIP:
PHONE #: FAX: OFFICE CONTACT:
Your signature authorizes the pharmacy to act on your behalf to obtain prior authorization for the prescribed medications. We will also pursue available copay and financial assistance on behalf of your patients. Following prior authorization, if insurance dictates the prescription be filled at a specific pharmacy ABD will forward the prescription to that pharmacy and the office and patient will be notified
10.03.2016