platelets
TRANSCRIPT

GOOD MORNING
PLATELETS
DR.A.KUMAR
1-YEAR PG STUDENT
BLOOD

BLOODDEFINITION:
Blood is a fluid connective tissue which transports substances from one part of the body to another.It provides nutrients and hormones to the tissues and removes their waste products
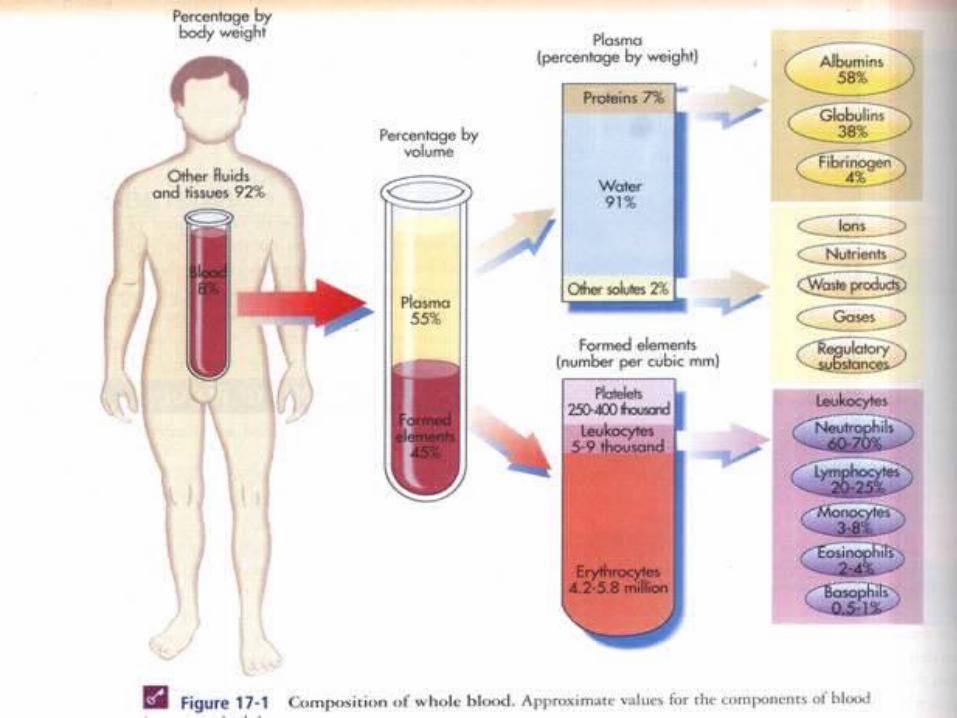

COMPOSITION
1.Red blood cells (erythrocytes)
2.White blood cells (leukocytes)
3.Platelets (thrombocytes)
4.Plasma proteins
SDGDFGFDAA
SDSGGFDFGFHFGHGFA
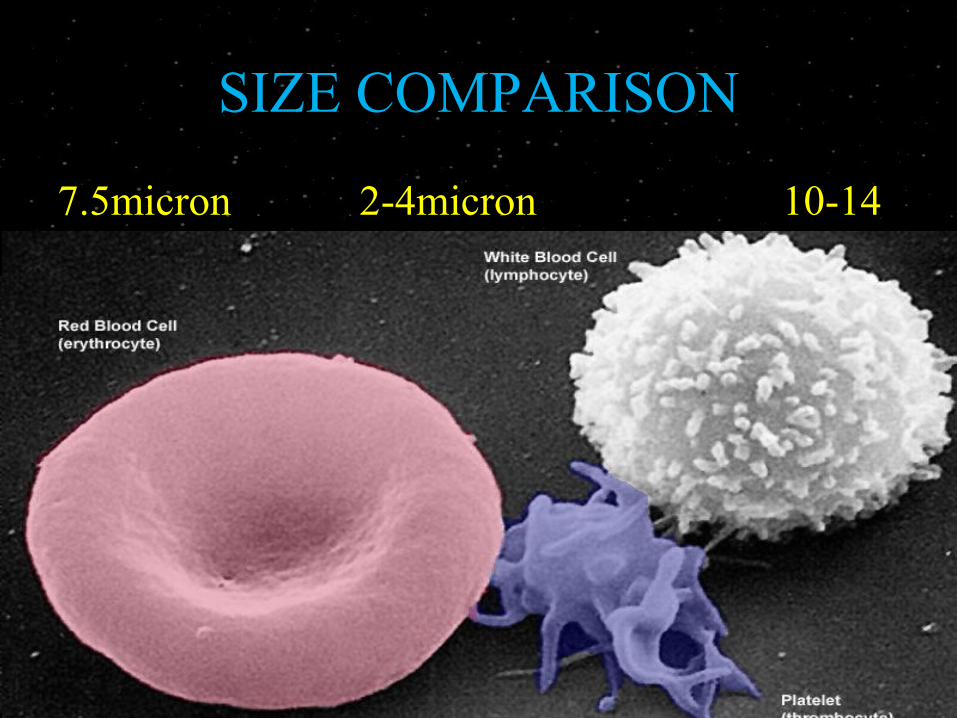
SIZE COMPARISON
7.5micron 2-4micron 10-14


INDEX-PLATELETSINTRODUCTION
STRUCTURE & COMPOSITION
1.Cell membrane
2.Microtubule
3.Cytoplasm
FORMATION OF PLATELETS
HEMOSTASIS
1.Vascular Constriction1.Vascular Constriction
2.Formation of Platelet Plug2.Formation of Platelet Plug 3.Blood coagulation
4.Fibrinolysis4.FibrinolysisThrombocytosisThrombocytopeniaHEMOSTATIC FUNCTION TESTS
DENTAL COSIDERATION
INDEX-PLATELETSINTRODUCTION
STRUCTURE & COMPOSITION
1.Cell membrane
2.Microtubule
3.Cytoplasm
FORMATION OF PLATELETS
HEMOSTASIS
1.Vascular Constriction1.Vascular Constriction
2.Formation of Platelet Plug2.Formation of Platelet Plug 3.Blood coagulation
4.Fibrinolysis4.FibrinolysisThrombocytosisThrombocytopeniaHEMOSTATIC FUNCTION TESTS
DENTAL COSIDERATION
INTRODUCTION
small
granulated
Non-nucleated
round or oval
2 – 4 µ in diameter
1,50,000 – 3,50,000/mm³
life span average 8 days
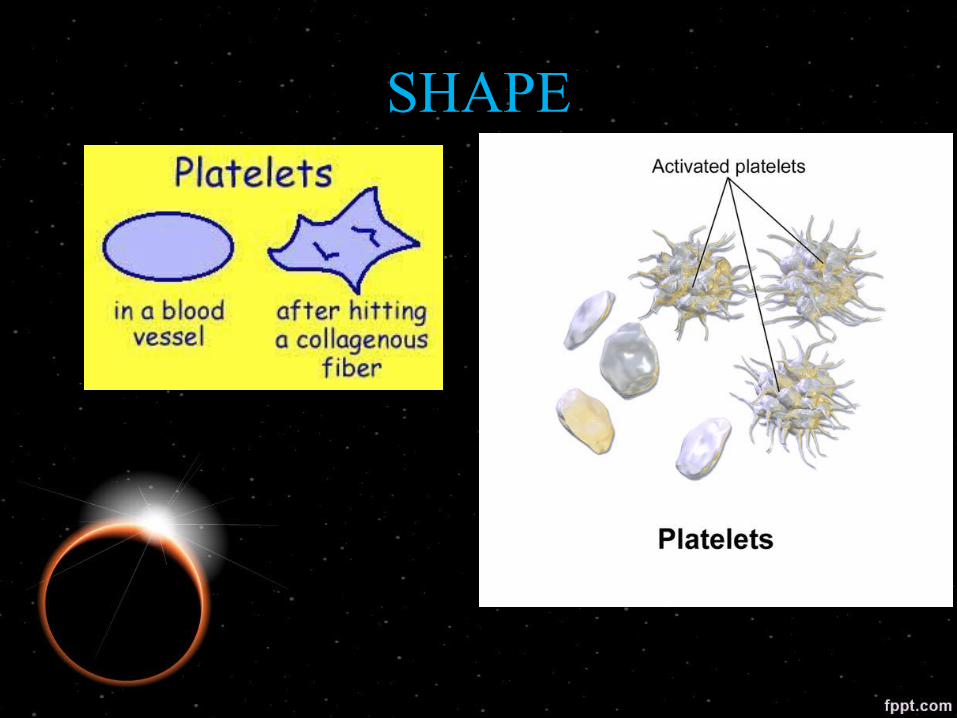
SHAPE
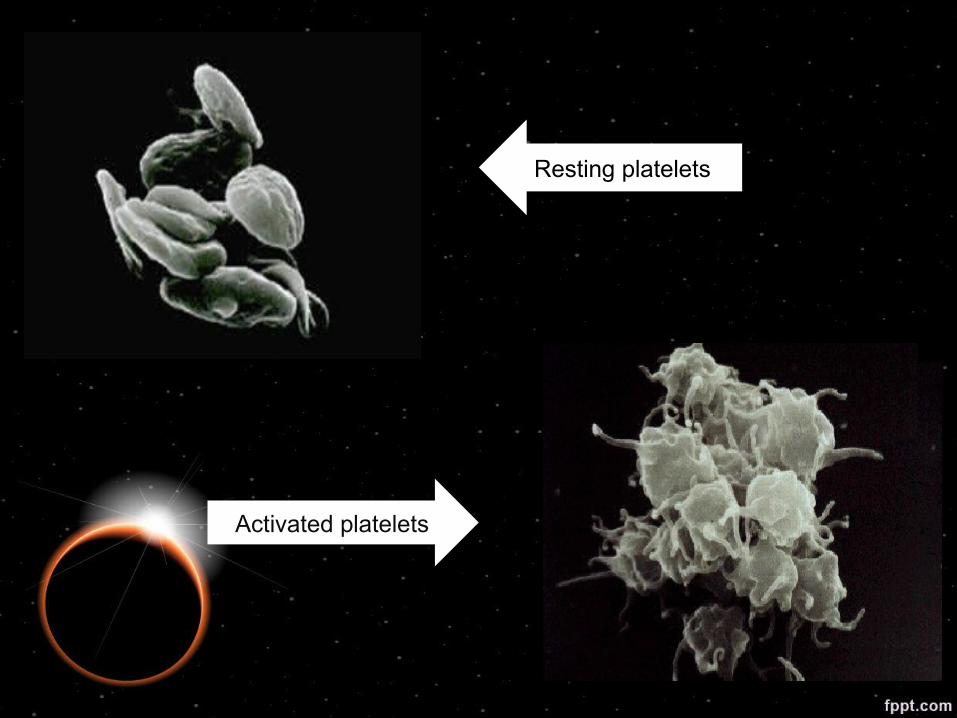
Resting platelets
Activated platelets

Scanning electron micrographs of different stages of platelet adhesion
Resting platelet (left, x10,000);Attached platelet showing shape change and pseudopodia emission (center, x3,000); Spread platelet (right, x3,000). Copyright © 2003-2014 Platelet Research Laboratory
STRUCTURE & COMPOSITION

STRUCTURE
• 1.Cell membrane
• 2.Microtubule
• 3.Cytoplasm

SDGDFGFDAA
SDSGGFDFGFHFGHGFA

1.Cell Membrane It is 6 nm thick and contain
Carbohydrates(glycocalyx),
Proteins (Glycoproteins)
lipids (phospholipids, cholesterol and glycolipids)
Out of all glycoprotein and phospholipids are functionally important

plasma membrane contains
glycoprotein receptors For
Phospholipids Include
• collagen
• vessel von-Willebrand factor
• fibrinogen • platelet factor 3

Glycopropteins• Prevents the adherence of platelets to
normal endothelium.
• Accelerates the adherence of platelets
to collagen and damaged endothelium
in ruptured blood vessels.
• Forms a receptor for ADP and
thrombin.
2.Microtubule
• Made up of tublins (proteins)
• It responsible for the discoid shape of the platelets

INDEX-PLATELETSINTRODUCTION
STRUCTURE & COMPOSITION
1.Cell membrane
2.Microtubule
3.Cytoplasm
FORMATION OF PLATELETS
HEMOSTASIS
1.Vascular Constriction1.Vascular Constriction
2.Formation of Platelet Plug2.Formation of Platelet Plug 3.Blood coagulation
4.Fibrinolysis4.FibrinolysisThrombocytosisThrombocytopeniaHEMOSTATIC FUNCTION TESTS
DENTAL COSIDERATION
SDGDFGFDAA
SDSGGFDFGFHFGHGFA

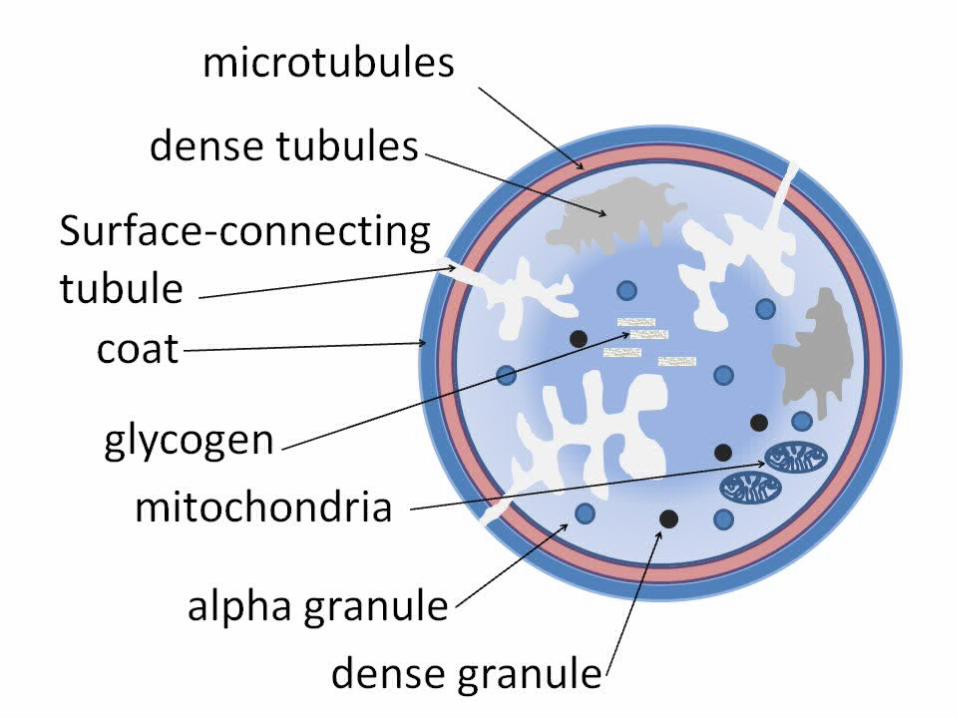
3.Cytoplasm • Contractile proteins• Golgi apparatus• Endoplasmic reticulum• Mitochondria• Lyzosomes• Glycogen granules• Enzymes• Chemical substances• Granules
Contractile proteins
actin myosinthrombosthenin
enable activated platelets to change their shape

Residuals of
Golgi apparatusendoplasmic reticulum
Synthesis of enzymes
Calcium store
Mitochondria and enzyme system for synthesis of ATP and ADP
Lyzosomes containing hydrolytic enzymes.
Glycogen granules for production of energy anaerobically.
Enzyme system that synthesize prostaglandins
from phospholipids of the Platelet membrane.
Chemical substances:
• Calcium ions
• Mg- ions.
• Adenosine triphosphate (ATP)
• Adenosine diphosphate (ADP)

Types of granules
A) Dense granules b) Alpha granules
contain non-protein substances
( ATP, ADP, Ca++ and serotonin)
contain the secreted proteins
• clotting factors
• fibrin stabilizing factor XIII
• platelet derived growth factor
INDEXINTRODUCTION
STRUCTURE & COMPOSITION
1.Cell membrane
2.Microtubule
3.Cytoplasm
FORMATION OF PLATELETS
HEMOSTASIS
1.Vascular Constriction1.Vascular Constriction
2.Formation of Platelet Plug2.Formation of Platelet Plug 3.Blood coagulation
4.Fibrinolysis4.FibrinolysisThrombocytosisThrombocytopeniaHEMOSTATIC FUNCTION TESTS
DENTAL COSIDERATION
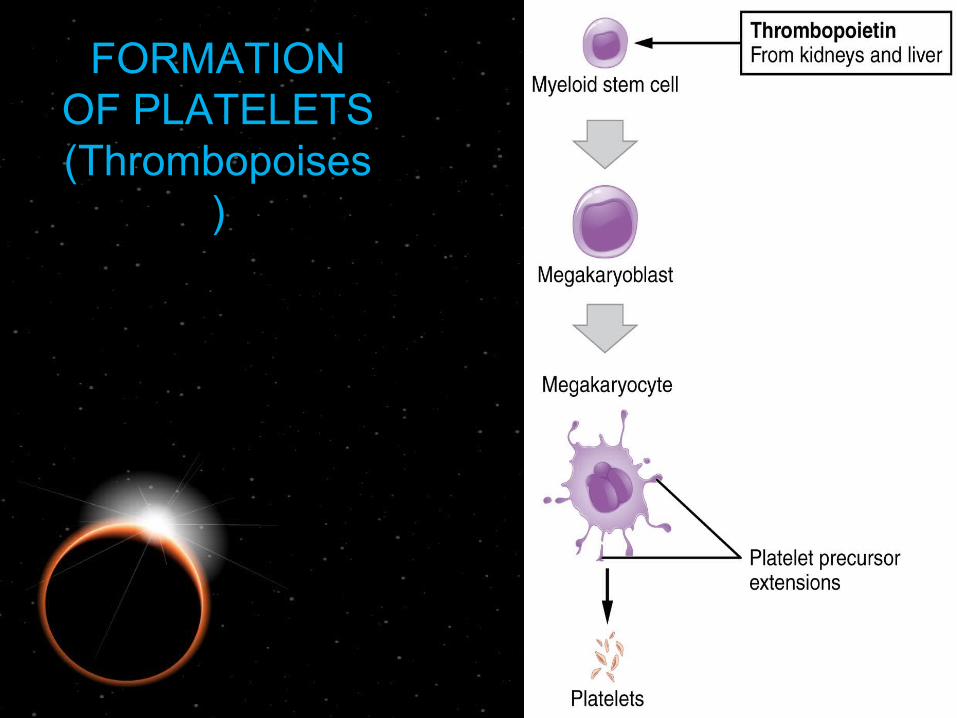
FORMATION OF PLATELETS (Thrombopoises
)

FORMATION OF PLATELETS(Thrombopoises)
• Megakaryoblast :• Large,oval,kidney shaped nucleus
• 20-30 micron diameter
• Megakaryocyte:• Multi lobed (4-16) nucleus• Cell marigin shows pseudopodias• Platelets formed from pseudopodias of the megakaryocyte
• Each megakaryocyte forms upto 4000 platelets
• Formation of platelets from stem cells takes 10 days

RELAX CORNER

INDEXINTRODUCTION
STRUCTURE & COMPOSITION
1.Cell membrane
2.Microtubule
3.Cytoplasm
FORMATION OF PLATELETS
HEMOSTASIS 1.Vascular Constriction1.Vascular Constriction
2.Formation of Platelet Plug2.Formation of Platelet Plug 3.Blood coagulation
4.Fibrinolysis4.FibrinolysisThrombocytosisThrombocytopeniaHEMOSTATIC FUNCTION TESTS
DENTAL COSIDERATION
HEMOSTASIS• DEFINITION - Heme = blood - stasis = to halt
It is the process of forming clots in the wall of damaged blood vessels & preventing blood loss while maintaining blood in a fluid state with in the vascular system.
Stages of HemostasisStages of Hemostasis
FibrinolysisFibrinolysis
Formation of Platelet PlugFormation of Platelet Plug
Blood coagulation
Vascular ConstrictionVascular Constriction
Stages of HemostasisStages of Hemostasis
FibrinolysisFibrinolysis
Formation of Platelet PlugFormation of Platelet Plug
Blood coagulation
Vascular ConstrictionVascular Constriction

Vascular ConstrictionVascular Constriction
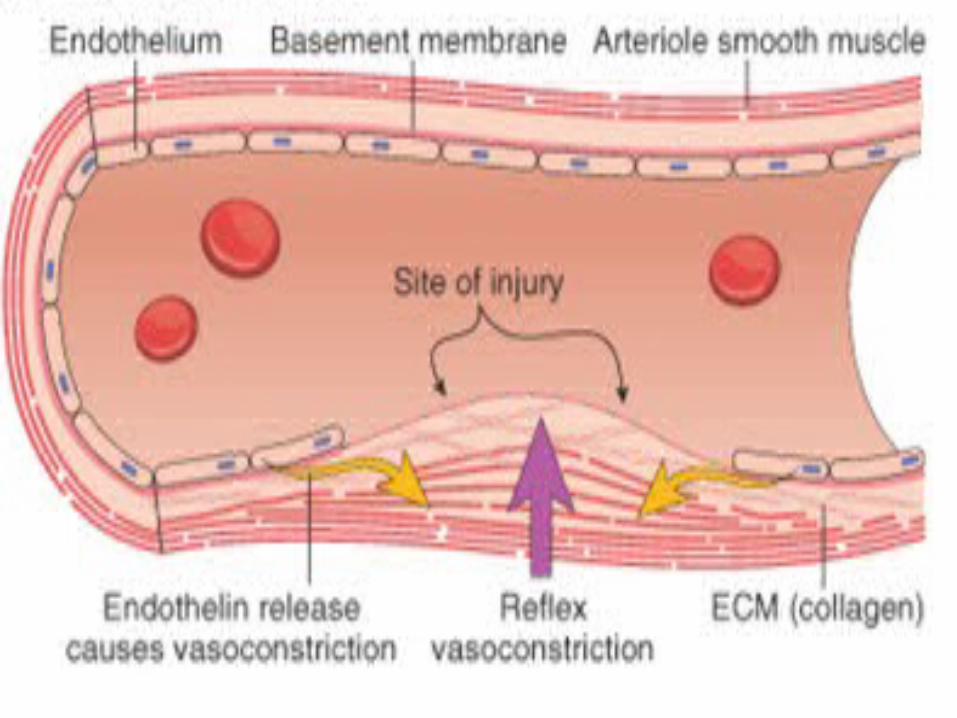
It is the first response to injury.It reduces the amount of blood flow in
damaged areas and limits the amount of blood loss.
These response is triggered by some chemicals released by endothelial cells(endothelin) and platlets (5HT and other vasoconstrictors)

Stages of HemostasisStages of Hemostasis
FibrinolysisFibrinolysis
Formation of Platelet PlugFormation of Platelet Plug
Blood coagulation
Vascular ConstrictionVascular Constriction

Formation of Platelet PlugFormation of Platelet Plug
• Platelet AdhesionPlatelet Adhesion• Platelet ActivationPlatelet Activation• Platelet AggregationPlatelet Aggregation

Platelet AdhesionPlatelet Adhesion
Following Vascular Constriction platlets become Vascular Constriction platlets become stickey and adhere to the collagen matrix in sub stickey and adhere to the collagen matrix in sub endotheliumendothelium
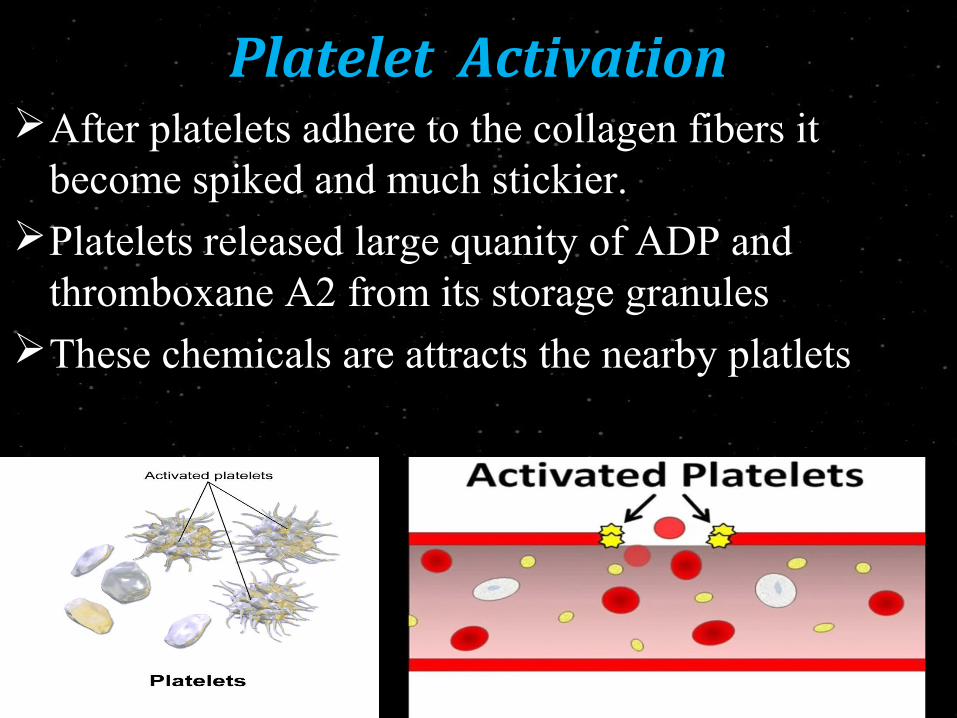
Platelet ActivationPlatelet ActivationAfter platelets adhere to the collagen fibers it
become spiked and much stickier.Platelets released large quanity of ADP and
thromboxane A2 from its storage granulesThese chemicals are attracts the nearby platlets

Platelet AggregationPlatelet Aggregation Large number of activated platlets stick to each other and
forming platelet aggregation or platelet plug. Platelet plug is fairly loose but it successful in blocking the
blood loss That’s why its called temporary haemostatic plug

Stages of HemostasisStages of Hemostasis
FibrinolysisFibrinolysis
Formation of Platelet PlugFormation of Platelet Plug
Blood coagulation
Vascular ConstrictionVascular Constriction
BLOOD COAGULATIONSECONDARY HAEMOSTASIS
DEFINITION:
Blood remains in fluid condition within the blood vessels through out life.but when the blood is shed from the blood vessels or collected in a container,it looses it fluidity within a few minutes and gets converted into jelly-like mass,which is called” clot”.This phenomenon is called coagulation.

CLOTTING FACTORSFactor I Fibrinogen
Factor II Prothrombin
Factor III Thromboplastin
Factor IV Calcium
Factor V Labile factor, or proaccelerin
Factor VI Non – existent
Factor VII Stable factor or proconvertin
Factor VIII Antihaemophilic factor / globulin A
Factor IX Christmas factor or Antihaemophilic factor B
Factor X Stuart – Prower factor
Factor XI Plasma thromboplastin antecedent or Antihaemophilic factor C
Factor XII Hageman factor or Contact factor
Factor XIII Fibrin stabilizing factor or Laki – Lorand factor

MNEMONICS
Foolish People Try Climbing Long Slopes After Christmas Some People Have Fallen
MECHANISM OF COAGULATION
The process of coagulation involves cascade of reactions
Activation of one factor leads to activation of next clotting factor
This enzyme cascade reaction is also called “WATER FALL SEQUECE”

STEPS IN COAGULATION
Three main steps:
Formation of prothrombin activator
Conversion of prothrombin to thrombin
Conversion of fibrinogen to fibrin

Formation of prothrombin activator
Intrinsic pathway Extrinsic pathway
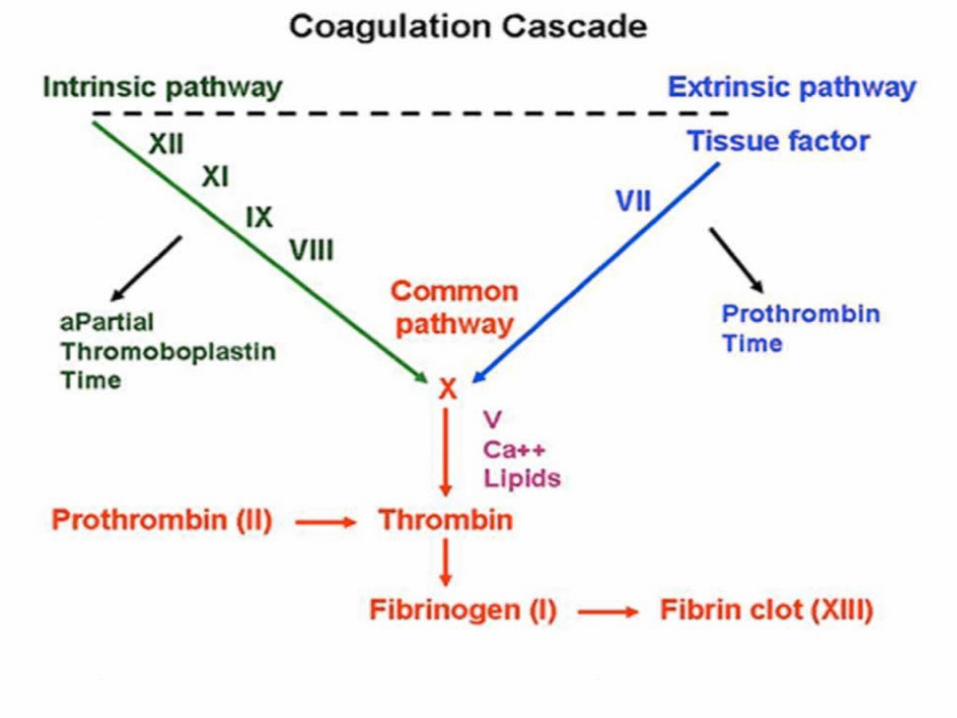
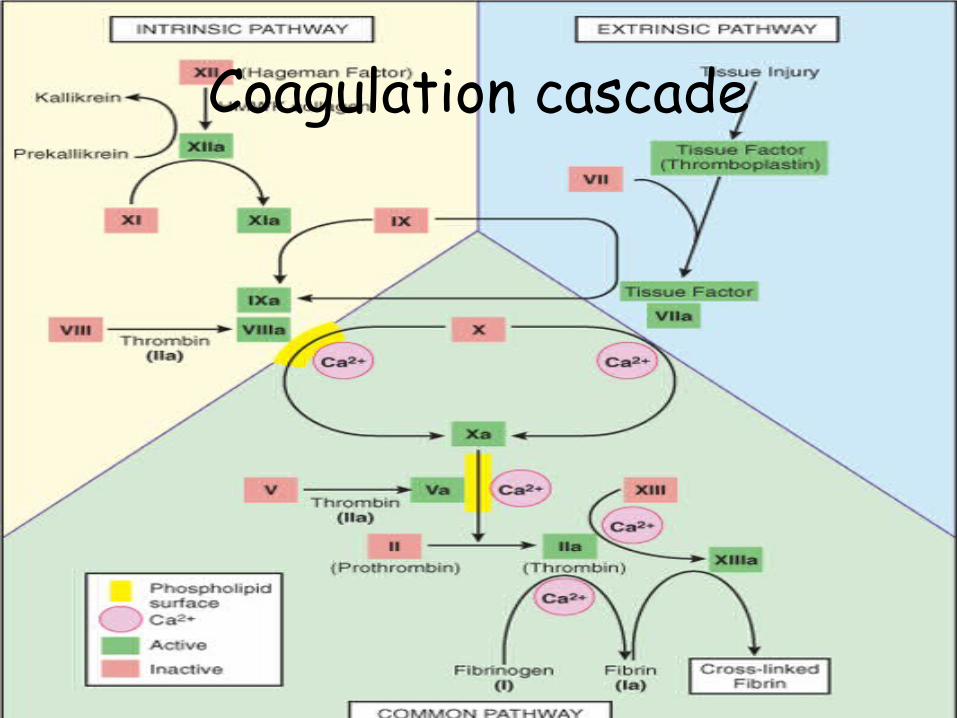
Coagulation cascade

Conversion of prothrombin to thrombin
Prothrombin activator
Prothrombin Thrombin
Ca2+
This process is caused by the prothrombin activator in the precence of ca2+ .
This occurs at the surface of platelets which form the platelet plug at the site of injury.
Conversion of fibrinogen to fibrin
It involves 3 reactionsProteolysisPolymerizationStabilization of fibrin polymers

Soluble fibrinogen
Proteolysis
Fibrin monomer
Polymerization
Fibrin polymer
(Soluble fibrin clot) Stabilization of polymer
Insoluble fibrin clot

In this stage formation of covalent crosslinkages between fibrin threads.
It adds tremendous strength to the fibrin meshwork.
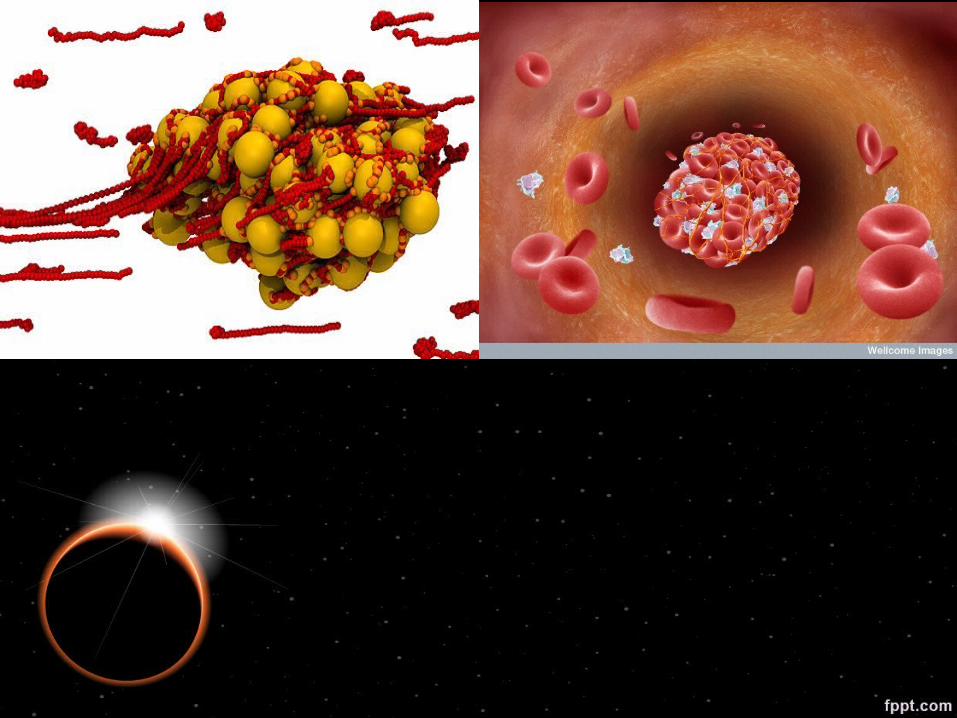
This insoluble fibrin meshwork traps the remaining components of plasma and blood cells to form a solid mass called clot
A

BLOOD CLOT RETRACTION
Within a few minutes after a clot is formed it begins to contract
Platelets are essential for clot retractionThe contractile proteins
(actin,myosin,thrombosthenin) present in the cytoplasm of platelets causing strong contraction.

Why circulating blood does not clot?
Endothelial surface factor
-smoothness
-layer of glycocalyx
-Negatively chargedVelocity of circulationNatural anticoagulantsActivation of Fibrinolytic systemLiver removes activated clotting factors

Stages of HemostasisStages of Hemostasis
FibrinolysisFibrinolysis
Formation of Platelet PlugFormation of Platelet Plug
Blood coagulation
Vascular ConstrictionVascular Constriction

FIBRINOLYSIS
It is a process that prevents blood clots from growing and becoming problematic.
In fibrinolysis,a fibrin clot,the product of coagulation ,is broken down.
Its main enzyme plasmin cuts the fibrin mesh at various places

As soon as clot develops,another series of events take place locally.
Plasminogen adsorbed on the clot
Plasmin
Breaks down fibrin threads
Fibrin threads are engulfed by reticulo -endothelial system
Fibrinolytic mechanismFibrinolytic mechanism


Factors affecting coagulationFactors affecting coagulation Role of vitamin k – required for the synthesis of prothrombin,
VII,IX and X by the liver. Hence these factors are called vitamin k dependent pro-coagulants.
Role of liver – liver synthesizes pro-coagulants like prothrombin, fibrinogen,factors V,VII IX,X XI.
Role of blood vessels – releases substances like plasminogen activators, tissue factors, von -willebrand factor.
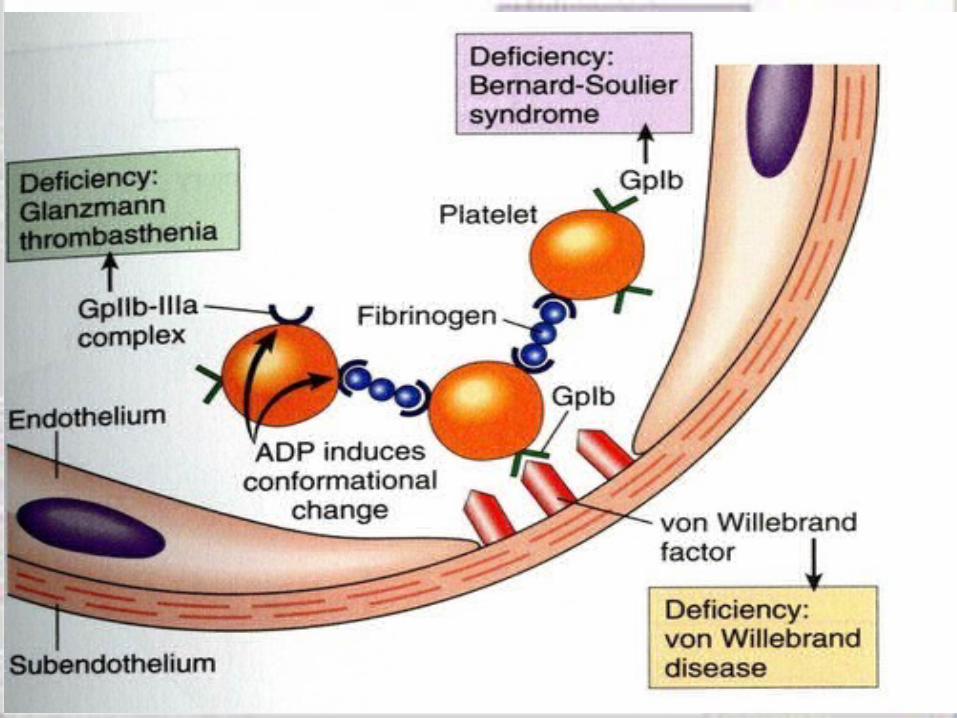
Role of von- willebrand factor – acts as a bridge between denuded vascular endothelium and platelets.
Also acts as a carrier of factor VIII.
Inhibitors of coagulationInhibitors of coagulation


Anticoagulant Coagulant
Eg: Heparin, Antithrombin Eg: FibrinThrombin
Excessive:Hemophilia Excessive:Thrombosis
HEMOSTATIC BALANCE
TEAM GENESIS

INDEXINTRODUCTION
STRUCTURE & COMPOSITION
1.Cell membrane
2.Microtubule
3.Cytoplasm
FORMATION OF PLATELETS
HEMOSTASIS
1.Vascular Constriction1.Vascular Constriction
2.Formation of Platelet Plug2.Formation of Platelet Plug 3.Blood coagulation
4.Fibrinolysis4.Fibrinolysis
ThrombocytosisThrombocytopeniaHEMOSTATIC FUNCTION TESTS
DENTAL COSIDERATION

Thrombocytosis or thrombocythemia is the presence of high platelet count in the blood.(leads to arteriosclerosis and atherosclerosis)
• ReactiveoTumors, inflammation, hemolysis, splenectomy
• AutonomousoMyeloproliferative disorder (PRV, CML)
Thrombocytosis

INDEXINTRODUCTION
STRUCTURE & COMPOSITION
1.Cell membrane
2.Microtubule
3.Cytoplasm
FORMATION OF PLATELETS
HEMOSTASIS
1.Vascular Constriction1.Vascular Constriction
2.Formation of Platelet Plug2.Formation of Platelet Plug 3.Blood coagulation
4.Fibrinolysis4.FibrinolysisThrombocytosis
ThrombocytopeniaHEMOSTATIC FUNCTION TESTS
DENTAL COSIDERATION
THROMBOCYTOPENIA• Defined as reduced in the platelet count< 150, 000µL
• It characterized by spontaneous bleeding, a prolonged bleeding time,
and a normal PT and PTT.
• The risk of bleeding depends on the level of the platelet count:
Mild thrombocytopenia (platelet <150 000 cells/µL)
Moderate thrombocytopenia (platelet 20 000 - 50 000 cells/µL)
Severe thrombocytopenia (platelet <20 000 cells/µL)
•Thrombocytopenia↓ in platelets production
oBM problem aplastic anemia, acute leukemia, megaloblastic
anemiaoDisorder in distribution
Hyperspleenism: more than 1/3 sequestered in spleen
↑ destruction CLL, SLE Autoimmune Thrombocytopenia Purpura (ITP)
Acute: children with virus (CMV, hepatitis, rubella)
Chronic: adult women with SLEoDisseminated intravascular coagulation (DIC)oVasculitis oDrugs: quinine, sulfa drugs,
Sign and symptoms
• bruising, petechiae, purpura and mucosal bleeding (epistaxis @ gum bleeding)
• major haemorrhage like severe GI bleeding, intracranial bleeding or haematuria.
• normal platelet count may present in platelet dysfunction
INDEXINTRODUCTION
STRUCTURE & COMPOSITION
1.Cell membrane
2.Microtubule
3.Cytoplasm
FORMATION OF PLATELETS
HEMOSTASIS
1.Vascular Constriction1.Vascular Constriction
2.Formation of Platelet Plug2.Formation of Platelet Plug 3.Blood coagulation
4.Fibrinolysis4.FibrinolysisThrombocytosisThrombocytopeniaHEMOSTATIC FUNCTION TESTS
DENTAL COSIDERATION
METHOD OF STUDY• HEMOSTATIC FUNCTION TESTSBleeding timeClotting time (Thrombin time)Prothrombin time
Partial thromboplastin time (PTT)
-

What is the clinical significance of doing BT & CT ?
1. History of frequent, persistent or spontaneous bleeding
2.Before every minor and major surgery
-(e.g. tooth extraction)3.Before taking biopsy
-( bone marrow, liver, kidney etc.)4.Before and during anticoagulant therapy5.Family history of bleeding disorder
80
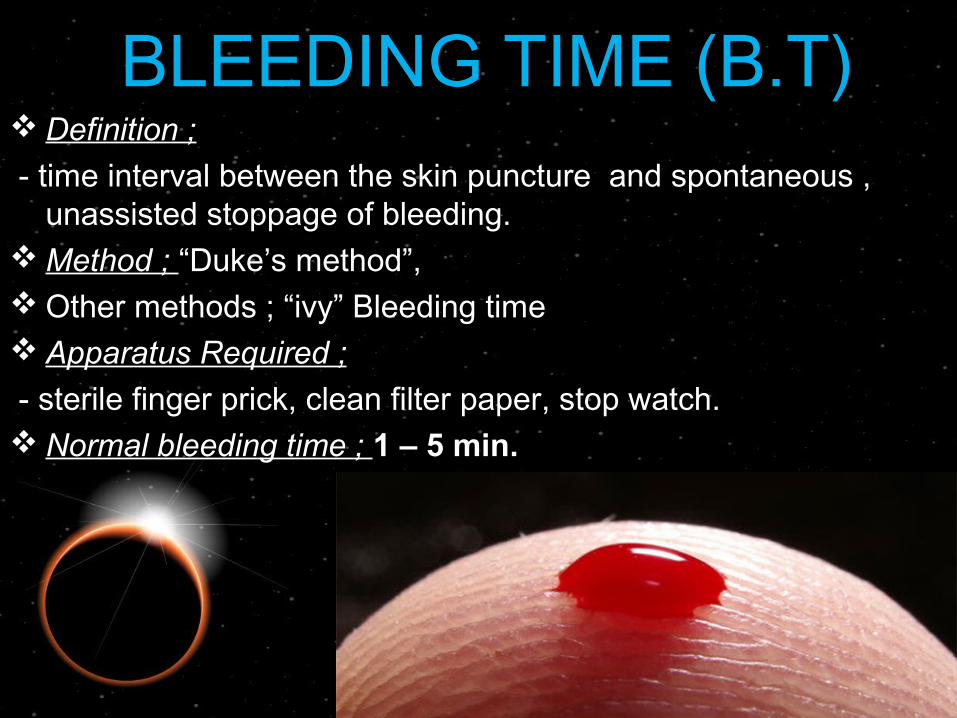
BLEEDING TIME (B.T) Definition ;
- time interval between the skin puncture and spontaneous , unassisted stoppage of bleeding.
Method ; “Duke’s method”, Other methods ; “ivy” Bleeding time Apparatus Required ;
- sterile finger prick, clean filter paper, stop watch. Normal bleeding time ; 1 – 5 min.
81
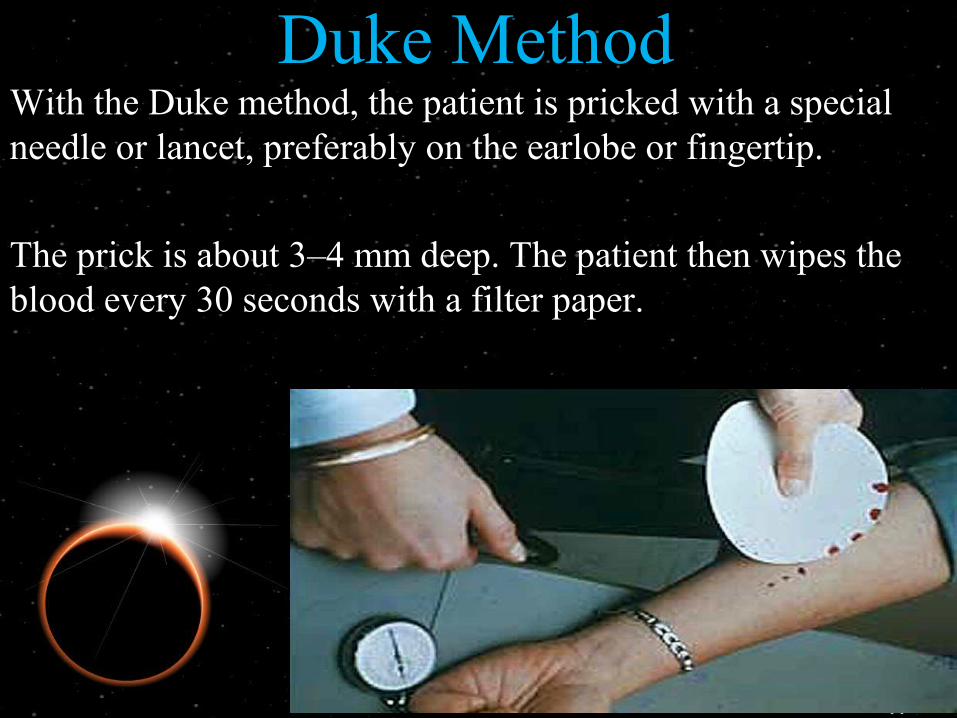
Duke MethodWith the Duke method, the patient is pricked with a special needle or lancet, preferably on the earlobe or fingertip.
The prick is about 3–4 mm deep. The patient then wipes the blood every 30 seconds with a filter paper.
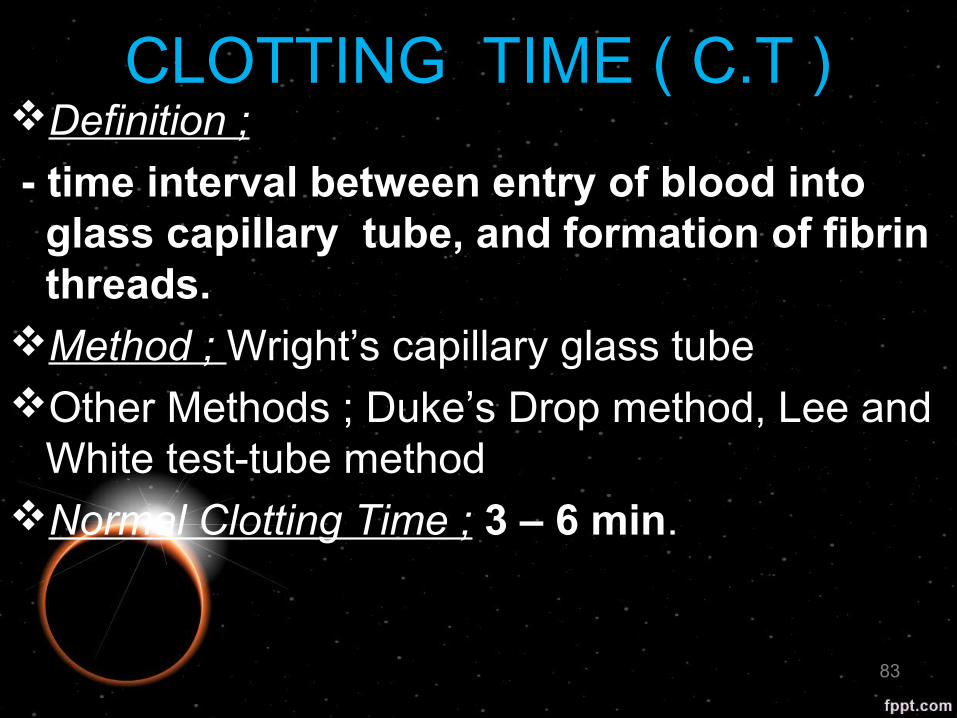
CLOTTING TIME ( C.T )Definition ;
- time interval between entry of blood into glass capillary tube, and formation of fibrin threads.
Method ; Wright’s capillary glass tubeOther Methods ; Duke’s Drop method, Lee and
White test-tube methodNormal Clotting Time ; 3 – 6 min.
83

PROTHROMBIN TIME (P.T)Normal P.T ; 15 – 20 sec.
Clinical Significance ; bleeding tendency occurs below 20% (Normal plasma prothrombin = 30- 40 mg/dl)
Low prothrombin suggest Vit. K def. and liver and biliary diseases.
Prolonged suggests deficiency of factor II, V, VII, and X.
84

Partial thromboplastin time (PTT)
Partial thromboplastin time (PTT) is a blood test that looks at how long it takes for blood to clot. It can help tell if you have bleeding or clotting problems.
The lab specialist will add chemicals to the blood sample and see how many seconds it takes for the blood to clot.
Normal value-25-35 sec
INDEXINTRODUCTION
STRUCTURE & COMPOSITION
1.Cell membrane
2.Microtubule
3.Cytoplasm
FORMATION OF PLATELETS
HEMOSTASIS
1.Vascular Constriction1.Vascular Constriction
2.Formation of Platelet Plug2.Formation of Platelet Plug 3.Blood coagulation
4.Fibrinolysis4.FibrinolysisThrombocytosisThrombocytopeniaHEMOSTATIC FUNCTION TESTS
DENTAL COSIDERATION

DENTAL COSIDERATION
DENTAL COSIDERATION
Assessment
Take accurate, comprehensive histories: personal, medical, dental, and pharmacological. Perform a thorough extra and intraoral examination to identify lesions indicative of a bleeding disorder.
History: History of extraction, personal or family history of blood dyscrasia.
General examination: Look for signs of shock and manage appropriately if present
Specific examination of the mouth
Types of post extraction haemorrhage
Immediate haemorrhage at the time of extractionReactionary haemorrhage, usually two to three
hours post extraction due to wearing off of the vasoconstrictor effect of the local anaesthetic
Secondary haemorrhage may occur at any time within the first week and is always indicative of infection

Management
Identify where the bleeding is coming from.
From soft tissue: The bleeding stops following digital pressure using one finger on each side of the bleeding socket and biting on a rolled up gauze swab moistened with saline or water.
Bleeding from the soft tissues is usually arrested by placing a horizontal mattress suture across the socket.
From the base of the socket, from bone: The bleeding continues following digital pressure and biting on a gauze swab.
Bleeding from the base of the socket, from bone, is usually arrested using a pack such as 'Surgicel' or in some instances soaking ribbon gauze in Whitehead's varnish and packing the socket full.

Bleeding from a vessel; The bleeding is more profound from within the socket or from a nearby vessel
Bleeding from a vessel. Within bone this may be arrested using packs as outlined above. However, if the vessel is within soft tissues there is a need to identify the vessel and either cauterise or ligate the vessel. This may in some instance necessitate a small flap procedure to identify the site of the vessel

Dental management of patients with haemophilia

ENDINTRODUCTION
STRUCTURE & COMPOSITION
1.Cell membrane
2.Microtubule
3.Cytoplasm
FORMATION OF PLATELETS
HEMOSTASIS
1.Vascular Constriction1.Vascular Constriction
2.Formation of Platelet Plug2.Formation of Platelet Plug 3.Blood coagulation
4.Fibrinolysis4.FibrinolysisThrombocytosisThrombocytopeniaHEMOSTATIC FUNCTION TESTS
DENTAL COSIDERATION
RELAX CORNER
THANK U
References-1References-1BOOKS:
1.Textbook of medical physiology- Guyten & hall
2. Textbook of medical physiology-R.B. Chaudhary
3.Text book of human physiology for dental students-Indu khurana

References-2References-2ARTICLES:1.Rafique S1, Fiske J, Palmer G, Daly B. Special care dentistry: part 1. Dental management of patients with inherited bleeding disorders. Dent Update. 2013 Oct;40(8):613-6, 619-22, 625-6 passim.
2.Dental management of medically compromised patient-Little J,Falace D,Miller C,Rhodes N.
3. Bergmeier W, Chauhan A, Wagner D (2008) Glycoprotein Ibalpha and von Willebrand factor in primary platelet adhesion and thrombus formation: lessons from mutant mice. Thromb Haemost 99: 264–270 [PubMed]
References-3References-3WEB-SITES:
1.http://www.britannica.com/EBchecked/topic/720818/blood-disease
2.http://www.patient.co.uk/doctor/bleeding-disorders
3.http://www.healthline.com/health/blood-cell-disorders#Types2
4.http://www.platelet-research.org/1/function_hemo.htm
5.http://www.hopkinsmedicine.org/heart_vascular_institute/index.html