placenta membranacea
TRANSCRIPT

LETTER TO THE EDITOR
Placenta membranacea
Samadh F. Ravangard • Kimberly Henderson •
Kisti Fuller
Received: 25 October 2012 / Accepted: 21 February 2013 / Published online: 7 March 2013
� Springer-Verlag Berlin Heidelberg 2013
Abstract Placenta membranacea is a rare placental dis-
order characterized by the presence of fetal membranes
(complete or partially) covered by chorionic villi. A
35-year-old woman, gravida 1, was admitted for preterm
labor at 24 weeks and 5 days. She subsequently developed
heavy vaginal bleeding and underwent a classical cesarean
delivery for suspected abruption. Postpartum inspection of
the placenta demonstrated a small placenta with tan colored
membranes, and diffusely scattered placental cotyledons.
Histologic examination revealed chorionic villi directly
attached to the fetal membranes on the periphery,consistent
with the diagnosis of a partial placenta membranacea.
Placenta membranacea should be considered in the etiol-
ogy of painless vaginal bleeding in the second and third
trimester. This condition can be associated with other
placental abnormalities, such as placenta previa or accreta.
Perinatal outcome may include stillbirth, preterm delivery,
or neonatal death.
Introduction
First described in 1853 by Dr. Seneca Sargent, placenta
membranacea is a rare placental anomaly that has been
reported to complicate 1:20,000–40,000 births [1, 2]. To
date, there have been 41 previously reported cases in the
literature. This unusual condition is believed to result from
the failure of the trophoblastic shell to differentiate into the
chorion frondosum and chorion laeve at 8–10 weeks of
gestation. This results in membranes that are either com-
pletely or partially covered by chorionic villi [2–6]. The
majority of cases are diagnosed postpartum, however, these
women commonly present with painless vaginal bleeding
and preterm labor in the second or third trimester [2, 3].
Placenta membranacea is a clinically significant and
potentially under-recognized condition that may be asso-
ciated with hemorrhage in the antepartum or postpartum
period, abnormal placental adherence, and pregnancy loss
[2]. Here we present a case of placenta membranacea with
a review of the literature.
Case
A 35-year-old woman, gravida 1, para 0 at 24 weeks and
5 days initially presented with the complaint of uterine
cramping every 4 min, which was associated with vaginal
spotting. Her antenatal course had been otherwise
uncomplicated prior to her admission.
On presentation she was found to be contracting every
5 min, and her cervix was 1 cm dilated and 100 % effaced.
She initially received magnesium sulfate for tocolysis and
betamethasone for fetal lung maturity. However, the
patient continued to contract and was additionally stabi-
lized with indomethacin. Trans-abdominal ultrasound per-
formed on admission, demonstrated a normal appearing
anterior placenta with the fetus in breech position and
estimated weight of 633 g (12 %).
On the morning of hospital day 2, the patient had a
single episode vaginal bleeding with approximately 75 cc
and her cervix was found to have progressed to 3 cm
dilated with bulging membranes. Shortly after, she devel-
oped steady vaginal bleeding. Her bleeding was attributed
S. F. Ravangard (&) � K. Henderson � K. Fuller
Department of Obstetrics and Gynecology, University
of Connecticut Health Center, 263 Farmington Avenue,
Farmington, CT 06030-2947, USA
e-mail: [email protected]
123
Arch Gynecol Obstet (2013) 288:709–712
DOI 10.1007/s00404-013-2778-z
to a placental abruption. As a result of persistent, heavy
vaginal bleeding, the decision was made to proceed with a
primary classical cesarean section. Fetal heart tracing was
reassuring throughout the hospital course. The patient
delivered a viable male infant, weighing 700 g (24 %) with
the APGAR scores of 1, 4, and 7 at 1, 5, and 10 min.
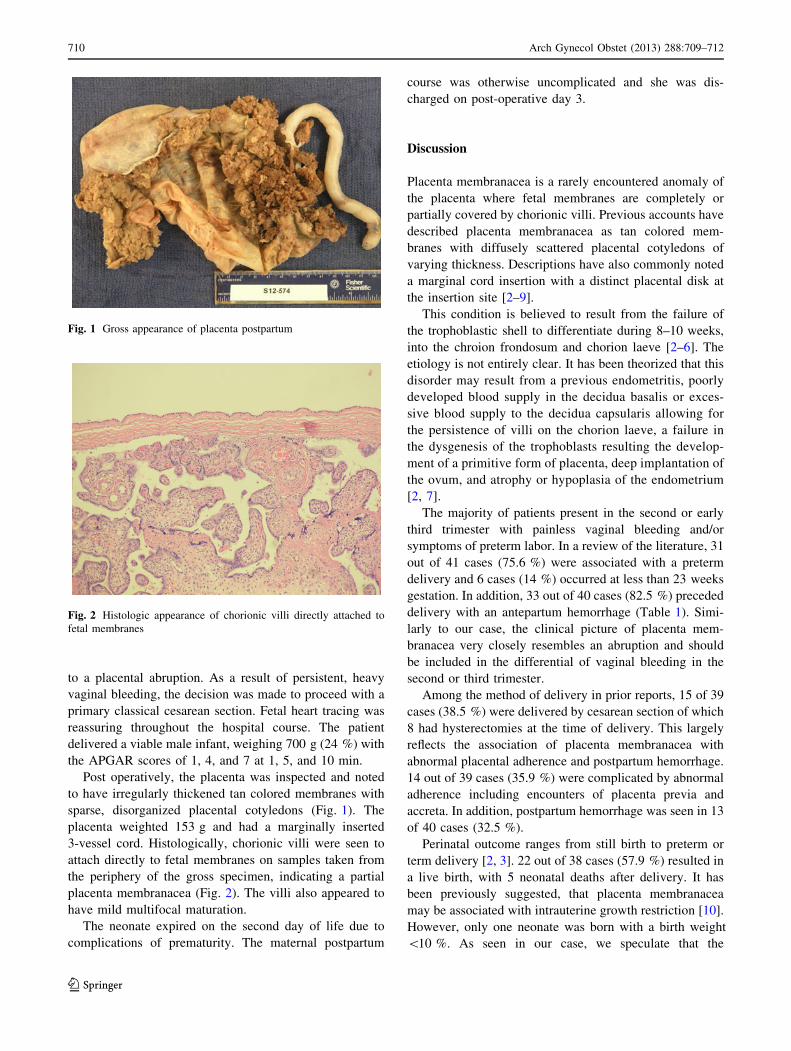
Post operatively, the placenta was inspected and noted
to have irregularly thickened tan colored membranes with
sparse, disorganized placental cotyledons (Fig. 1). The
placenta weighted 153 g and had a marginally inserted
3-vessel cord. Histologically, chorionic villi were seen to
attach directly to fetal membranes on samples taken from
the periphery of the gross specimen, indicating a partial
placenta membranacea (Fig. 2). The villi also appeared to
have mild multifocal maturation.
The neonate expired on the second day of life due to
complications of prematurity. The maternal postpartum
course was otherwise uncomplicated and she was dis-
charged on post-operative day 3.
Discussion
Placenta membranacea is a rarely encountered anomaly of
the placenta where fetal membranes are completely or
partially covered by chorionic villi. Previous accounts have
described placenta membranacea as tan colored mem-
branes with diffusely scattered placental cotyledons of
varying thickness. Descriptions have also commonly noted
a marginal cord insertion with a distinct placental disk at
the insertion site [2–9].
This condition is believed to result from the failure of
the trophoblastic shell to differentiate during 8–10 weeks,
into the chroion frondosum and chorion laeve [2–6]. The
etiology is not entirely clear. It has been theorized that this
disorder may result from a previous endometritis, poorly
developed blood supply in the decidua basalis or exces-
sive blood supply to the decidua capsularis allowing for
the persistence of villi on the chorion laeve, a failure in
the dysgenesis of the trophoblasts resulting the develop-
ment of a primitive form of placenta, deep implantation of
the ovum, and atrophy or hypoplasia of the endometrium
[2, 7].
The majority of patients present in the second or early
third trimester with painless vaginal bleeding and/or
symptoms of preterm labor. In a review of the literature, 31
out of 41 cases (75.6 %) were associated with a preterm
delivery and 6 cases (14 %) occurred at less than 23 weeks
gestation. In addition, 33 out of 40 cases (82.5 %) preceded
delivery with an antepartum hemorrhage (Table 1). Simi-
larly to our case, the clinical picture of placenta mem-
branacea very closely resembles an abruption and should
be included in the differential of vaginal bleeding in the
second or third trimester.
Among the method of delivery in prior reports, 15 of 39
cases (38.5 %) were delivered by cesarean section of which
8 had hysterectomies at the time of delivery. This largely
reflects the association of placenta membranacea with
abnormal placental adherence and postpartum hemorrhage.
14 out of 39 cases (35.9 %) were complicated by abnormal
adherence including encounters of placenta previa and
accreta. In addition, postpartum hemorrhage was seen in 13
of 40 cases (32.5 %).
Perinatal outcome ranges from still birth to preterm or
term delivery [2, 3]. 22 out of 38 cases (57.9 %) resulted in
a live birth, with 5 neonatal deaths after delivery. It has
been previously suggested, that placenta membranacea
may be associated with intrauterine growth restriction [10].
However, only one neonate was born with a birth weight
\10 %. As seen in our case, we speculate that the
Fig. 1 Gross appearance of placenta postpartum
Fig. 2 Histologic appearance of chorionic villi directly attached to
fetal membranes
710 Arch Gynecol Obstet (2013) 288:709–712
123

Table 1 Case reports of placenta membranacea
Author(s) (year) Case Gestational ageat delivery
Antepartumhemorrhage
Postpartumhemorrhage
Placentaladherence
Deliverymethod
Livebirth
Birthweight
Percentile Fetal outcome
Sargent [1] 1 6 months ? - - Vag - 909 g 80 %
von Weiss [12] 2 23 weeks ? ? ? Vag ? NA NA Death at 30 min of life
Braun and vonWeiss [13]
3 5–6 months ? ? NA Vag ? NA NA Death described assoon after birth
Reinprecht [14] 4 23 weeks ? ? ? Vag - 370 g 15 %
DeLee [15] 5 Preterm - ? ? Vag ? 2,018 g NA
Viana [16] 6 7 months ? - - Vag - 750 g 15 %
Routh [17] 7 5 months ? - - Vag - NA NA
Kapferer [18] 8 7 months ? ? - Vag - NA NA
Finn [8] 9 27 weeks ? ? - Ces ? 1,446 g 90 % Death at 72 h of life
10 24 weeks ? - - Ces ? 879 g 80 % Death at 1 h of life
Rodriguez-Soriano[19]
11 43 weeks ? ? - Ces ? 4,000 g 95 %
Aguero [20] 12 Term - - - Vag ? NA NA
13 Preterm ? ? ? Vag NA NA NA
14 40 weeks ? NA NA NA NA NA NA
Shanklin [21] 15 30 weeks NA NA NA NA NA NA NA
Janovski andGranowitz [7]
16 20 weeks ? - - Ces* - 120 g NA
Bukovsky et al. [22] 17 42 weeks ? - ? Ces* ? 4,250 g NA
Culp [11] 19 32 weeks ? - - Vag ? 1,700 g 40 %
Pryse-Davies [23] 18 20 weeks ? - - Vag - 378 g NA
Benirschke andDriscoll [24]
20 NA NA ? ? NA* NA NA NA
Wladimiroff et al.[9]
21 26 weeks ? - - Vag - 560 g 10 %
Las Heras et al. [5] 22 40 weeks ? - - Ces ? 3,630 g 75 %
Molloy et al. [10] 23 30 weeks ? - - Ces ? 1,109 g 15 %
Lindner [25] 24 40 weeks ? - ? Ces* ? 2,900 g Na
Hurley andBeischer [6]
25 36 weeks - - - Ces ? 2,630 g 45 %
26 37 weeks ? ? - Vag ? 3,520 g 90 %
27 35 weeks ? ? ? Vag ? 2,235 g 30 %
Greenburg et al. [2] 28 32 weeks - ? ? Ces* ? 1,690 g 25 %
Wilkins et al. [26] 29 24 weeks ? - - Vag - NA NA
30 19 weeks ? - ? Vag - NA NA
31 18 weeks ? - - Vag - NA NA
32 22 weeks ? - - Vag - NA NA
33 17 weeks ? - -- Vag - NA NA
34 17 weeks ? ? ? Vag - NA NA
35 30 weeks ? - - Ces ? NA NA
Dinh [4] 36 37 weeks ? - ? Ces* ? 2945 g NA
Ekoukou et al. [27] 37 38 weeks ? - ? Ces* ? NA NA
Ahmed [3] 38 17 weeks - - - Vag - NA NA
39 37 weeks - - - Vag ? NA NA
40 12 weeks - - - Vag - NA NA
Sparic et al. [28] 41 31 weeks ? - ? Ces* ? 1,800 g NA
Ravangard et al.(present case)
42 24 wk ? - - Ces ? 700 g 25 % Death at 48 h of life
NA not available, Vag vaginal, Ces cesarean
* Hysterectomy at time of delivery
Arch Gynecol Obstet (2013) 288:709–712 711
123

accelerated maturation of villi may allow an abnormal
placenta to compensate and sustain an appropriately grown
fetus for some degree of time.
Antenatal diagnosis of placenta membranacea remains a
clinical challenge. The majority of cases have been diag-
nosed during postpartum examination of the placenta.
However, there have been two reports of antenatal diag-
nosis using ultrasonography [9, 10]. Angiography has also
been reported in the successful diagnosis of one case ret-
rospectively [11]. The ability to detect the distinguishing
placental cotyledons or the placental disk at cord insertion
site with thinning placental tissue distally on ultrasonog-
raphy may raise suspicion of this rare diagnosis [9, 10]. In
our case, we were unable to retrospectively identify any
distinguishing characteristics of placenta membranacea on
ultrasonography.
Placenta membranacea is an unusual placental disorder
that is potentially unrecognized. These patients typically
present with vaginal bleeding in the second or third tri-
mester. The majority of pregnancies result in an appro-
priately grown preterm neonate, but outcome can range
from stillbirth to a viable term delivery. Placenta mem-
branacea may be further complicated by postpartum hem-
orrhage and/or abnormal placental adherence. Previous
cases of placenta membranacea have almost entirely been
diagnosed during postpartum placental examination, how-
ever, advances in diagnostic imaging may allow for future
antenatal diagnosis.
Conflict of interest None.
References
1. Sargent S (1854) Case of a foetus within the placenta. Boston
Med Surg J 49:163–164
2. Greenberg JA, Sorem KA, Shifren JL, Riley LE (1991) Placenta
membranacea with placenta increta: a case report and literature
review. Obstet Gynecol 78:512–514
3. Ahmed A (2003) Placenta membranacea: a developmental
anomaly with diverse clinical presentation. Pediatr Dev Path
6:201–202
4. Dinh TV, Bedi DG, Salinas J (1992) Placenta membranacea,
previa and accrete a case report. J Reprod Med 37:97–99
5. Las Heras J, Harding PG, Haust MD (1982) Recurrent bleeding
associated with placenta membranacea partialis: report of a case.
Am J Obtet Gynecol 144:480–482
6. Hurley VA, Beischer NA (1987) Placenta membranacea. Case
reports. Br J Obstet Gynaecol 94:798–802
7. Janovski NA, Granowitz ET (1961) Placenta membranacea.
Obstet Gynecol 18:206–212
8. Finn JL (1954) Placenta membranacea. Obstet Gynecol 3:438–
440
9. Wladimiroff JW, Wallenburg HCS, Putten PVD, Drogendijk AC
(1976) Ultrasonic diagnosis of placenta membranacea. Arch
Gynaekol 221:167–174
10. Molloy CE, McDowell W, Armour T, Crawford W, Berstine R
(1983) Ultrasonic diagnosis of placenta membranacea in utero.
J Ultrasound Med 2:377–379
11. Culp WC, Bryan RN, Morettin LB (1973) Placenta membrana-
cea. Radiology 108:309–310
12. Von Weiss O (1893) Uber placenta membranacea and ihre be-
ziehungen zur placenta praevia. Wien Klin Wochenschr 6:915
13. Braun R, von Weiss O (1894) Berichte aus gynaklog. Gesells-
chaften und krankenhausern. Zentralbl Gynaekol 18:76–79
14. Reinprecht L (1902) Placenta membranacea. Zentralbl Gynaekol
26:73
15. DeLee JB (1902) Placenta membranacea. Am J Obstet 46:530–
531
16. Torpin R (1969) The human placenta: it’s shape, form, origin, and
development. Charles C. Thomas, Springfield, Illinois, pp 88–92
17. Routh A (1908) Placenta diffusa. Proc R Soc Med 1:127–128
18. Kapferer R (1921) Ein fall von placenta difusa. Zentralbl Gy-
naekol 45:661
19. Rodriguez-Soriano JA (1956) Contribucion al studio de la pla-
centa difusa total. An Med (Lima) 42:53–58
20. Aguero O (1957) Anomalias morfologicas de la placenta y su
significado clinic. Caracas, Venezuela, Artegrafia, pp 97–99
21. Shanklin DR (1958) The human placenta: a clinicopathologic
study. Obstet Gynecol 11:129–138
22. Bukovsky I, Hirsch H (1971) Placenta praevia accreta mem-
branacea. Intern Surg 56:422
23. Pryse-Davies J, Dewhurst CJ, Campbell S (1973) Placenta
membranacea. J Obstet Gynaecol Br Commonw 80:1106–1110
24. Benirschke K, Driscoll SG (1974) The pathology of the human
placenta. Springer, New York, pp 109–111
25. Linder E, Zacharlas L, Elkojok M, Kerzabi K (1986) Exceptional
observation of a placenta praevia centralis accrete, increta, percreta,
and membranacea. Acta Univ Palack Olomuc Fac Med 114:225
26. Wilkins BS, Batcup G, Vinall PS (1991) Partial placenta mem-
branacea. Br J Obstet Gynaecol 98:675–679
27. Ekoukou D, Ng Wing Tin L, Nere MB, Bourdet O, Elalaoui Y,
Bazin C (1995) Placenta membranacea. Review of the literature,
a case report. J Gynecol Obstet Biol Reprod (Paris) 24:189–193
28. Sparic R, Kadija S, Tadic J, Dokic M, Milenkovic V (2007)
Intrapartal resection of the bicornuete uterus for placenta mem-
branacea percreta. Srp Arh Celok Lek 135:85–87
712 Arch Gynecol Obstet (2013) 288:709–712
123