placement c student portfolio 2018/19
TRANSCRIPT
Placement C
Student Portfolio
2018/19
Published: November 2018 Review: November 2019

2
Contents Introductory Portfolio Information ................................................................ 3 Peer Assisted Learning (PAL): A Collaborative 2:1 Model for Placement C .......... 5 Pre-Placement C Information ....................................................................... 6 Expectations Agreement ............................................................................. 7 Confidentiality Agreement ........................................................................... 9 Guidance on attendance and absence during Dietetic Practice Placements ....... 11 Guidance on repeat and extended week placements ..................................... 12 Good practice guide to appropriate dress .................................................... 13 Placement C- Summary of Learning outcomes ............................................. 14 ‘Know, Can, Do’ Model .............................................................................. 18 Induction Checklist ................................................................................... 19 Guide to compiling your portfolio ............................................................... 22 Placement C Induction Activity: Catering .................................................... 27 Placement C Activity: Individual Patient Consultations .................................. 29 Summary List of Competent Summative IPC Tools ....................................... 34 Placement C Activity: Service User Involvement .......................................... 35 Placement C Activity: Needs Assessment (NA) of a population/group .............. 38 Placement C Activity: Nutrition and Dietetic Audit ........................................ 43 Placement C Activity: Talk to service user group .......................................... 46 Talk to Service User Group Assessment Tool ............................................... 47 Placement C Activity: Case Presentation ..................................................... 49 Case Presentation Assessment Tool ............................................................ 52 Placement C Activity: Service and Business Management in a Dietetic Team ... 53 Feed Forward Form .................................................................................. 55 Placement C Activity: Independent practice ................................................. 57 C8: Independent Practice Assessment Tool ................................................. 58 Activities mapped to learning outcomes ...................................................... 60 Placement C: Professionalism Checklist ....................................................... 61 Summary of evidence Placement C ............................................................. 64 Observation of Practice Tool ...................................................................... 65 Reflective framework ................................................................................ 66 Review of Placement C ............................................................................. 67 APPENDICES ........................................................................................... 71
Understanding Duty of Care ................................................................... 72 Guidance on use of the Gibbs Reflective Cycle (1988) ................................ 73 DIET-COMMS Formative Communication Assessment Tool.......................... 81 Raising a Concern Algorithm Student Progression Algorithm Fitness to Practice Algorithm

3
Introductory Portfolio Information The following learning outcome framework, activities, tasks and associated assessment tools have been developed in collaboration with all Health Boards in Scotland, NHS Education Scotland and the three Universities in Scotland (Glasgow Caledonian University, Queen Margaret University, and Robert Gordon University) who offer pre-registration Dietetic training. Current students, previous students and service users were also integral to the development process. Furthermore, acknowledgement should be given to other Universities in the UK and beyond who have been willing to share their resources, in particular Kings College London and London Metropolitan University. The framework is aligned to the British Dietetic Association (BDA) Curriculum Framework for the Pre-Registration Education and training of Dietitians, the BDA Model and Process for Nutrition and Dietetic Practice, the Health and Care Professions Council (HCPC) Standards of Education and Training (SETs), and the HCPC Standards of Proficiency for Dietitians. The portfolio has been approved by both the HCPC and BDA and is therefore a compulsory requirement for dietetic student training across Scotland. The placement and portfolio has been developed in a manner that has been cognisant of current drivers across Health and Social Care, the NHS Scotland workforce vision and core values. Consideration has also been given to NHS Education Scotland Post Registration Career Development Framework (for Nurses, Midwives and Allied Health Professionals in Scotland), and the four pillars of practice (Practitioner Level). These pillars reflect the essential requirements for the graduate workforce and therefore have been embedded in the education and training activities in the three placement blocks to support student progression and competence.
NES ‘Four Pillars of Practice’
Key documents https://www.bda.uk.com/careers/education/preregcurriculum https://www.bda.uk.com/professional/practice/process http://www.hpc-uk.org/aboutregistration/standards/sets/ http://www.hpc-uk.org/publications/standards/index.asp?startrow=11&sCategory=&sKeyword= http://www.careerframework.nes.scot.nhs.uk/using-the-framework/pillars-of-practice.aspx
4
Overview of Placement C Placement C is 12 weeks long and is the final of the 3 placements. It occurs late in the academic programme and only after successful completion of placement B.
Students have the opportunity to become competent in translating theory into practice and to demonstrate the range of skills needed to work as a graduate dietitian. To achieve this, students are given the opportunity for experience in a range of settings. Examples of appropriate healthcare settings are hospital wards, hospital outpatient clinics, GP surgeries, health centres, patient’s homes and nursing/residential homes. Students also have the opportunity to visit non-healthcare settings e.g. schools and community groups as well as undertaking health promotion work. Not all students will experience dietetic practice in all settings but all students will be provided with appropriate opportunities to meet the learning outcomes associated with placement C.
Placement C builds on the knowledge, skills and experience obtained in placement B and enables students to become competent practitioners. Students are therefore given the opportunity to develop dietetic interventions for a range of clinical conditions and, in a period of ‘independent practice’ (consolidation) at the end of Placement C, will be working with minimal supervision within their scope of practice.
Placement C has eight learning outcomes associated with it, most of which are based on the various steps in the Nutrition and Dietetic Care Process (NDCP). It is the responsibility of the student to gather evidence to demonstrate that they have met the learning outcomes; this is collated in a portfolio of evidence. Work undertaken throughout the placement will contribute to this ‘live’ portfolio so students must consistently engage with all activities and collate their evidence on an ongoing basis. The first seven learning outcomes must be met by the end of week 10. Successful completion of these learning outcomes permits the student to progress to a period of ‘independent practice’ (consolidation -minimum of 2 weeks) during which they will be assessed on the eighth and final learning outcome.
5
Peer Assisted Learning (PAL): A Collaborative 2:1 Model for Placement C Using PAL on Placement C The term Peer Assisted Learning (PAL) essentially means that you will work in collaboration with at least one other student in order to develop your knowledge and skills. Peer assisted learning has been shown to be a more effective process for learning than an individual based approach. It is seen as a natural progression from problem based learning. You may be working collaboratively on an ad-hoc basis throughout your 12-week C placement with a peer. Some placement providers will use PAL more extensively than others but all providers should include some PAL activities e.g. Needs Assessment, for you to work with another student on should there be more than one student on placement at the time. This method of working will not be new to you as you will have experienced collaborative working either in pairs or teams throughout your time at university and during your A and B placements. You and your peer may have different leaning styles of learning. It is important to find this out early in your placement and share this. You should respect your peers learning style and you may need to adapt your way of working to accommodate this. NB: You should note that your peer may be a student from a different University to your own. You may also be at different stages in your training, for example when a postgraduate and an undergraduate student are paired on placement. Although you may work closely with a peer, you will also meet with a practice educator during your C placement. This will allow you to discuss your learning and seek advice and guidance in areas where peer working has left you unsure about your knowledge or practice. You will be expected to feedback to the facilitator on the PAL activities and also to feedback to your peer where appropriate. Your facilitator should give you feedback individually and in your peer group. You will be assessed against the learning outcomes on an individual basis; your peer will not influence your ability to successfully meet the learning outcomes. PAL will work best when you are prepared to share your knowledge, skills and experiences with your peer(s), and to begin to take responsibility for your own learning.
6
Pre-Placement C Information
Prior to your Practice Placement C, you will be required to supply your Lead Practice Educator with some information about yourself. This will be used in the organisation of your placement, and to support the Practice Educators to better facilitate your learning. In line with GDPR guidelines, the student, personally, will send all pre-placement information to the Lead Practice Educator electronically for further dissemination. However, all documentation will continue to be reviewed by the personal tutor or clinical placement tutor at the University prior to submission. One copy should be sent to the Lead Practice Provider, one copy should be retained by the University for the Students record and one copy should be retained by the Student in this portfolio. February 2018 cohort The pre-placement form will be completed in collaboration with the personal academic tutor. Autumn 2019 cohort The pre-placement information will include:
• a short (2 page) Curriculum Vitae, created by the student in a pre-determined CV template
• Confirmation of food hygiene certificate, and membership of the BDA (or other indemnity insurance arrangements
• a short (1 page) reflective review focussing on knowledge, skills and attributes relating to:
o nutrition/dietetic/professional knowledge required prior to commencement of the relevant placement
o teamwork and communication o time management and organisation
• Other general information e.g. learning style, nutritional analysis software experience, access to car, accommodation plans/ details of location.
• Where required, a separate description of any requested ‘reasonable adjustments’ for consideration by the Lead Practice Educator.

7
Expectations Agreement University tutors and practice placement providers believe that students should be treated as adult learners. This means you will be taking full responsibility for your own learning and it is up to you to provide us with evidence of your progress and your professional qualities at each stage. We will not chase you to hand in work or undertake other tasks. However, please remember that if you regularly fail to complete work within the allotted time, this does not demonstrate commitment or a professional attitude. In addition you must also remember and appreciate that a dietetic department is a working department and the needs of the service must be the priority. In view of this your programme could change at short notice and you should demonstrate flexibility if this happens. What you can expect from us:
• To be treated with respect • To be clear about the aims and tasks of your placement • To be treated fairly and non-judgmentally • That your training is well organised and you are given adequate notice of
tasks where possible • To be clear about what each dietitian expects of you during their the time
that they are facilitating your learning • To be given adequate support • To have confidential matters kept confidential • To be given the opportunity to contribute to the day to day running of the
dietetic department in the practice setting • To receive honest and constructive feedback • To be given every opportunity to demonstrate your skills and abilities • You will have the opportunity to meet with a task facilitator after each task
and receive feedback
What we expect from you: • When working with your peers you should contribute equally to the task
and work submitted • When discussion of a topic is required with your peer around a task / topic,
listen and acknowledge their views and opinions • To treat all members of staff with respect • To let us know if you have a problem with anything that affects your work • To accept feedback and work to address any areas highlighted • To be self-motivated • To inform your supervisor / student training coordinator if tasks or tutorials
have been cancelled and need to be rearranged • To behave appropriately and professionally at all times • To be prepared to reflect on your learning experiences and plan your future
learning
8
• To prepare adequately for tasks, revising notes or reading around a subject if needed
• To ask if you are unsure about something (although this doesn’t mean asking a dietitian something that you could easily look up instead!)
• To use your initiative at every opportunity, for example answering the phone if everyone else in the office is busy
• To be honest and say if you don’t know or understand something • To be punctual to meetings, tutorials etc. • To meet deadlines without prompting and inform the facilitating dietitian in
advance if you are having difficulty • To use any spare time within the placement constructively whether on
campus or in the practice setting • To ensure that you have completed all paperwork required before meetings
and to ensure that all forms are filed in your portfolio • Ensure supervisor / secretary knows where you are at all times • To check that you understand what is expected in terms of your evidence
portfolio • Mobile phones should be switched off during the working hours of your
placement • Appropriate use of emails and internet in line with both the university and
the NHS IT policies
I have read the above, which has been fully discussed with me. I am clear about what is expected of me and I am happy to take full responsibility for my own training. Signed: Name (PRINT): Date:
9
Confidentiality Agreement It is an important professional requirement that you maintain patient confidentiality both when a student and when an HCPC registrant. In view of this, you must agree to maintain confidentiality at all times. In addition to patient confidentiality it is important that you consider the confidentiality of the staff you work with whilst you are on placement, and the confidentiality of other students who are in the placement setting with you. Prior to proceeding to your practice placement you are required to sign a confidentiality agreement to demonstrate that you understand and agree to maintain confidential information regarding patients, staff and other students whilst you are on placement. This agreement extends to disclosing information both verbally and in the written form, which includes social networking fora such as Facebook and Twitter. You may also be asked to sign a confidentiality agreement by your practice placement provider as part of your induction which you should sign in addition to this agreement. You should read the following statement, which is a typical confidentiality agreement for NHS staff: “You must not, either during or after the end of your placement, disclose any confidential information relating to patients (all matters relating to a patient’s diagnosis and treatment are strictly confidential), staff and other students (including details of others student’s performance on placement) to any person or make use of the information unless you are expressly authorised to do so, by the organisation, as a necessary part of your duties. If you disclose or misuse information during the course of your employment, the NHS Board and/or the University will treat such conduct as Gross Misconduct”. In addition, it is not permitted to access your own information. Neither can you access other people’s information unless you have a legitimate reason to do so as part of your practice education programme. Other people include, for example: family members; neighbours; colleagues, or; any high profile patient information. It is not permitted to ask your practice educators, or others who work in the NHS, to access your information on your behalf. Although you do not have a contract of employment whilst on placement, you are required to uphold this statement as a condition of you being offered a placement within the NHS. Any breach of the above statement or additional information may result in the initiation of fitness to practice proceedings. For more information on key documents this information relates to please see the following publications:
• HCPC (2016) Guidance on Conduct and Ethics for Students:
http://www.hcpc-uk.org/publications/brochures/ • HCPC (2016) Standards of Conduct, Performance and Ethics:
http://www.hcpc-uk.org/publications/standards/
10
• NHS Scotland Code of Practice: Protecting Confidentiality: http://www.wdhscp.org.uk/media/1256/revised-code-of-confidentiality-final.pdf
If you agree to this condition please sign the Form of Acceptance. Signed: Name (PRINT): Date:
11
Guidance on attendance and absence during Dietetic Practice Placements Students must normally complete a minimum of 1000 hours on practice placement over the duration of their studies. This is normally achieved through the successful completion of placement A (4 weeks or 150 hours), placement B (12 weeks or 450 hours), and placement C (12 weeks or 450 hours). To satisfy this requirement students are expected to work the full time hours of a dietitian (normally Monday-Friday 9-5pm, or 8.30–4.30pm). Public holidays will be granted in line with departmental policy. Study leave or half days will not be given. Student must attend practice placements in line with the service requirements of the practice educator and, where working hours fall outwith the normal hours of work, the practice educator should provide appropriate notice. Absence Any absence from placement may impact on a student’s ability to fulfil the required 1000 hours of practice-based education. In view of this, it should be noted that due to the short duration of the practice placements, coupled with continued service delivery demands within the NHS, which impinge on the ability to facilitate additional placement days; absences other than those on the grounds of sickness will not normally be sanctioned. Students who have concerns with regards to absence on grounds other than sickness must discuss these with their University Tutor in the first instance and must not approach their Practice Educator. Where absences due to sickness do occur these will normally be dealt with as follows: Placement C: Loss of up to 5 placement days No action needs to be taken if the Practice Educator and University Tutor considers that there is no detrimental effect on the student’s progress, i.e. they have demonstrated competence in all of the learning outcomes for that placement. If this is not the case the lost time must be made up. Loss of more than 5 placement days The student must complete a minimum of 11 weeks; any lost time must be made up to 11 weeks. No action needs to be taken beyond this if the practice educator considers that there is no detrimental effect on student’s progress, i.e. they have demonstrated competence in all the learning outcomes. If this is not the case the rest of the lost time should be made up. If the student requires a prolonged period of absence from their placement, the period of training required will be determined in consultation with the Practice Educator and University Tutor. Notification of absences Students should follow local NHS policy regarding the notification of any absences to Practice Educators and provide medical certification where relevant. The Practice Educator should notify the University Tutor of any absences as a matter of course and record this on the end of placement form.

12
Guidance on repeat and extended week placements In line with the BDA curriculum framework (2013) students must normally complete a minimum of 1000 hours on practice placement. However it is acknowledged that students’ progress at different rates and whilst it is expected that most students will be able to meet the learning outcomes for placements within the suggested time allocation i.e. placement A (150 hours), placement B (450 hours) and placement C (450 hours), provision is made for students to complete additional practice education hours if the placement learning outcomes have not been met. Additional practice education hours will not automatically take place within the same placement setting. Students can only be allocated a maximum of 500 additional hours across the 3 practice placements and the additional hours for each practice placement cannot be more than the original placement length i.e. for placement A only 150 additional hours can be allocated, for placement B and C only 450 additional hours can be allocated. Any additional time taken in placement A reduces the additional time available for placement B and subsequently placement C. Example: If a student requires an additional 50 hours for placement A then only 450 hours additional time can be allocated to any future placements. This takes into consideration the maximum allowance of 500 hours and the maximum additional hours permitted for placement B. If the same student then requires an additional 250 hours for placement B then only 200 hours would be available for placement C (taking into consideration the 50 additional hours for placement A). Placement C To successfully complete placement C, students must pass all learning outcomes by providing evidence of competency. Where a student does not successfully meet all the learning outcomes they will be required to complete additional time to enable them to meet these. The additional time provided to the students will be discussed and agreed by the practice educator and the university tutor. This will take into consideration the rate of student progression and number of learning outcomes not met. The additional hours provided will not be less than 37.5 hours (1 week) and not more than 450 hours (12 weeks). Any additional time utilised during Placement A and Placement B will also be taken into consideration when allocating additional hours to ensure the permitted 500 hours is not exceeded. Placement C Activities Where students have successfully completed the needs assessment and audit during the original 12 week placement (i.e. that these activities were signed to confirm that they were completed and discussed to an acceptable standard to meet the specified learning outcome(s), a student, in exceptional circumstances, may not be required to repeat these activities during the extended placement weeks. This will be determined by the University tutor and Practice Educator. Where these activities were not completed to the required standard during the original 12 week placement, the student will be required to undertake these activities again.
13
Good practice guide to appropriate dress The appearance of students and staff plays an important role in the delivery of person centred, safe, and effective care. Person centred: all students are expected to present a smart and professional image which is likely to inspire public confidence. Uniforms are provided to help achieve this objective. Photo ID badges must be worn and visible unless contraindicated by health and safety requirements. Safe and effective: whilst involved in direct clinical care, dress will be in compliance with the principles relating to the prevention and control of transmission of infection, and health and safety regulations. Personal Protective Equipment (PPE) is provided to help achieve this objective. A good practice guide to appropriate dress is detailed below; however, you should refer to your placement Health Board dress code policy for specific guidance. Please note that dress code policies may be more, or less, restrictive dependent upon the task, setting and service user population/ group.
• Students should wear the uniform provided by their University. • Uniforms must be clean, pressed and laundered. • Uniforms should only be worn in the work environment.
o Uniforms must be transported to and from work in a clean disposable bag.
• Fleeces/cardigans may be worn in the uniform colour but must be removed before patient contact.
• If a disability/medical condition, religious, ethnic or cultural requirement makes it difficult or impossible for a student to comply, the Practice Educator should be contacted for further advice.
• Footwear should be soft soled with closed toes. • No badges other than ID and professional badges to be worn. • Sleeves should be either short, ¾ length or rolled up away from the wrists
prior to hand hygiene. • Fingernails should be kept short and clean. • False nails and nail varnish are not permitted. • Jewellery and piercings may not be permitted or may be limited (refer to
local policy) • Hair must be clean neat and tidy
o Longer hair must be tied or clipped back at all times in clinical areas. • Make up should be kept light; false eyelashes are not permitted. • Perfume/aftershave, if worn, should be subtle in nature.
14
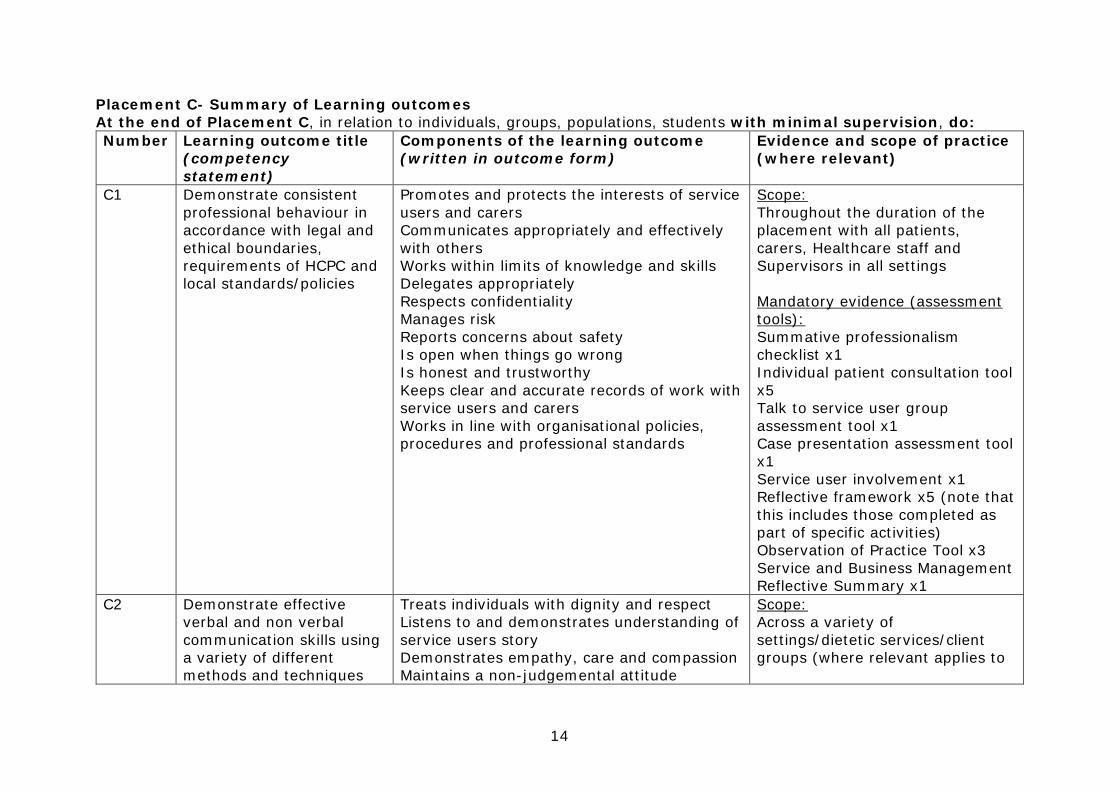
Placement C- Summary of Learning outcomes At the end of Placement C, in relation to individuals, groups, populations, students with minimal supervision, do: Number Learning outcome title
(competency statement)
Components of the learning outcome (written in outcome form)
Evidence and scope of practice (where relevant)
C1 Demonstrate consistent professional behaviour in accordance with legal and ethical boundaries, requirements of HCPC and local standards/policies
Promotes and protects the interests of service users and carers Communicates appropriately and effectively with others Works within limits of knowledge and skills Delegates appropriately Respects confidentiality Manages risk Reports concerns about safety Is open when things go wrong Is honest and trustworthy Keeps clear and accurate records of work with service users and carers Works in line with organisational policies, procedures and professional standards
Scope: Throughout the duration of the placement with all patients, carers, Healthcare staff and Supervisors in all settings Mandatory evidence (assessment tools): Summative professionalism checklist x1 Individual patient consultation tool x5 Talk to service user group assessment tool x1 Case presentation assessment tool x1 Service user involvement x1 Reflective framework x5 (note that this includes those completed as part of specific activities) Observation of Practice Tool x3 Service and Business Management Reflective Summary x1
C2 Demonstrate effective verbal and non verbal communication skills using a variety of different methods and techniques
Treats individuals with dignity and respect Listens to and demonstrates understanding of service users story Demonstrates empathy, care and compassion Maintains a non-judgemental attitude
Scope: Across a variety of settings/dietetic services/client groups (where relevant applies to
15
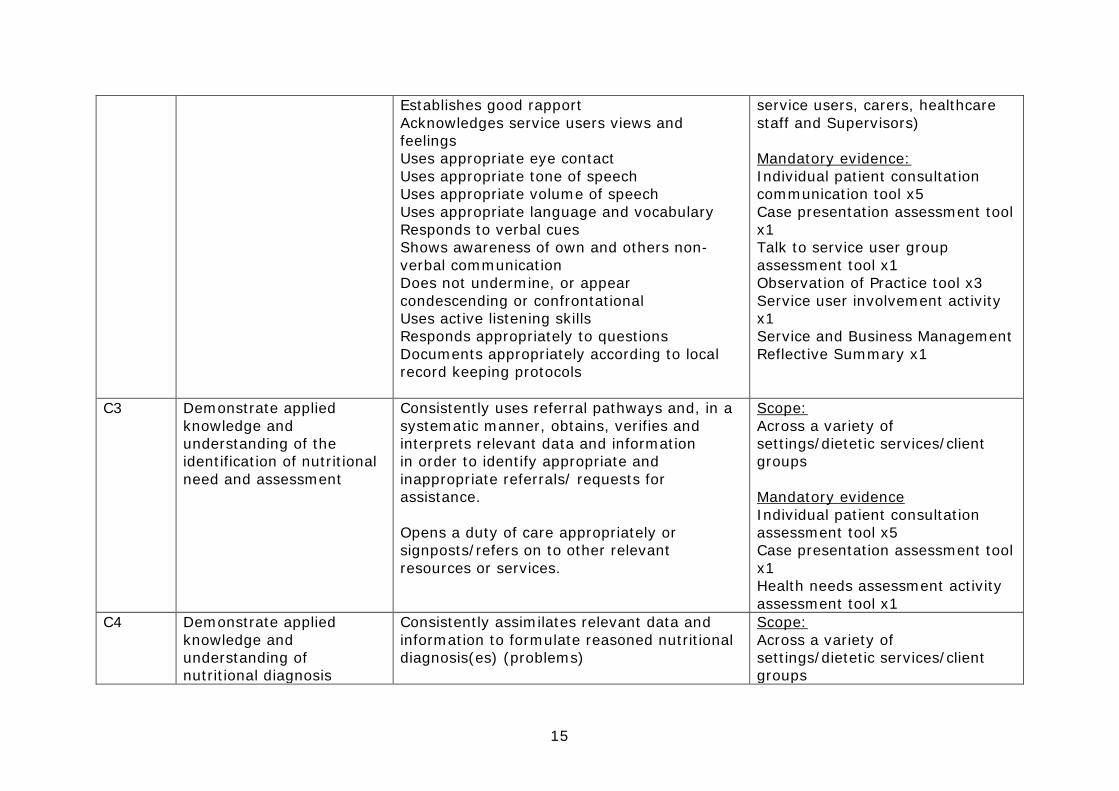
Establishes good rapport Acknowledges service users views and feelings Uses appropriate eye contact Uses appropriate tone of speech Uses appropriate volume of speech Uses appropriate language and vocabulary Responds to verbal cues Shows awareness of own and others non-verbal communication Does not undermine, or appear condescending or confrontational Uses active listening skills Responds appropriately to questions Documents appropriately according to local record keeping protocols
service users, carers, healthcare staff and Supervisors) Mandatory evidence: Individual patient consultation communication tool x5 Case presentation assessment tool x1 Talk to service user group assessment tool x1 Observation of Practice tool x3 Service user involvement activity x1 Service and Business Management Reflective Summary x1
C3 Demonstrate applied knowledge and understanding of the identification of nutritional need and assessment
Consistently uses referral pathways and, in a systematic manner, obtains, verifies and interprets relevant data and information in order to identify appropriate and inappropriate referrals/ requests for assistance. Opens a duty of care appropriately or signposts/refers on to other relevant resources or services.
Scope: Across a variety of settings/dietetic services/client groups Mandatory evidence Individual patient consultation assessment tool x5 Case presentation assessment tool x1 Health needs assessment activity assessment tool x1
C4 Demonstrate applied knowledge and understanding of nutritional diagnosis
Consistently assimilates relevant data and information to formulate reasoned nutritional diagnosis(es) (problems)
Scope: Across a variety of settings/dietetic services/client groups
16
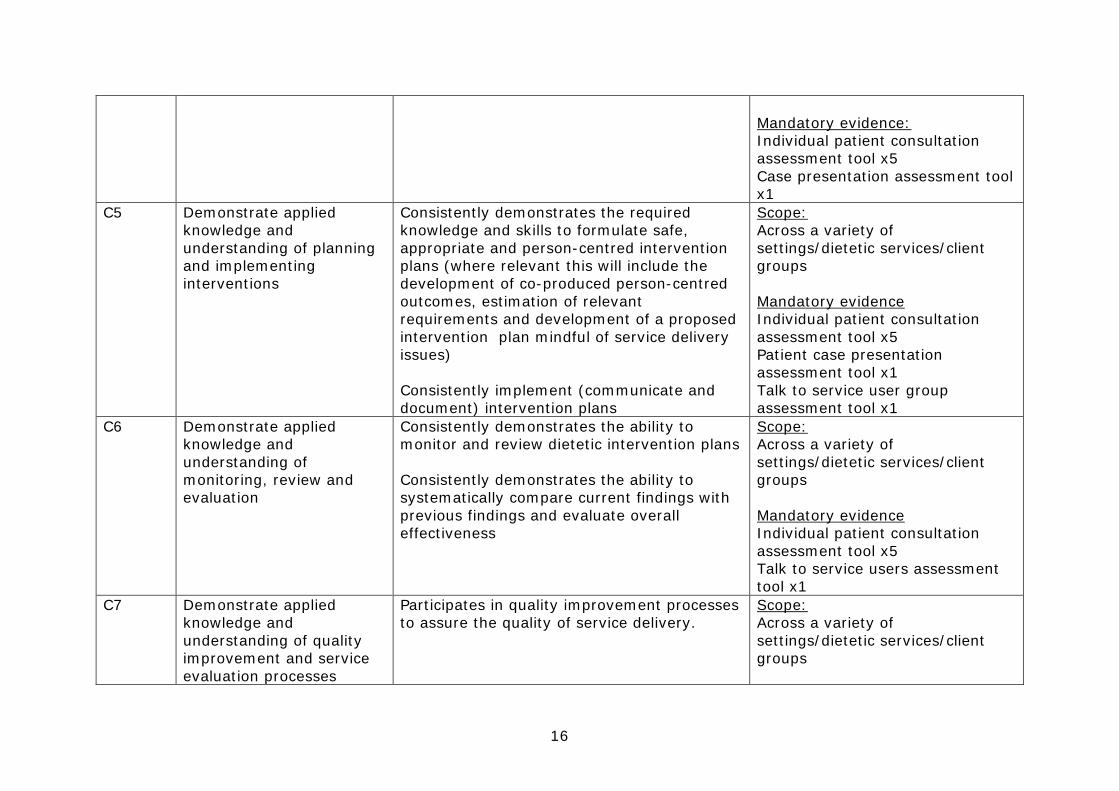
Mandatory evidence: Individual patient consultation assessment tool x5 Case presentation assessment tool x1
C5 Demonstrate applied knowledge and understanding of planning and implementing interventions
Consistently demonstrates the required knowledge and skills to formulate safe, appropriate and person-centred intervention plans (where relevant this will include the development of co-produced person-centred outcomes, estimation of relevant requirements and development of a proposed intervention plan mindful of service delivery issues) Consistently implement (communicate and document) intervention plans
Scope: Across a variety of settings/dietetic services/client groups Mandatory evidence Individual patient consultation assessment tool x5 Patient case presentation assessment tool x1 Talk to service user group assessment tool x1
C6 Demonstrate applied knowledge and understanding of monitoring, review and evaluation
Consistently demonstrates the ability to monitor and review dietetic intervention plans Consistently demonstrates the ability to systematically compare current findings with previous findings and evaluate overall effectiveness
Scope: Across a variety of settings/dietetic services/client groups Mandatory evidence Individual patient consultation assessment tool x5 Talk to service users assessment tool x1
C7 Demonstrate applied knowledge and understanding of quality improvement and service evaluation processes
Participates in quality improvement processes to assure the quality of service delivery.
Scope: Across a variety of settings/dietetic services/client groups
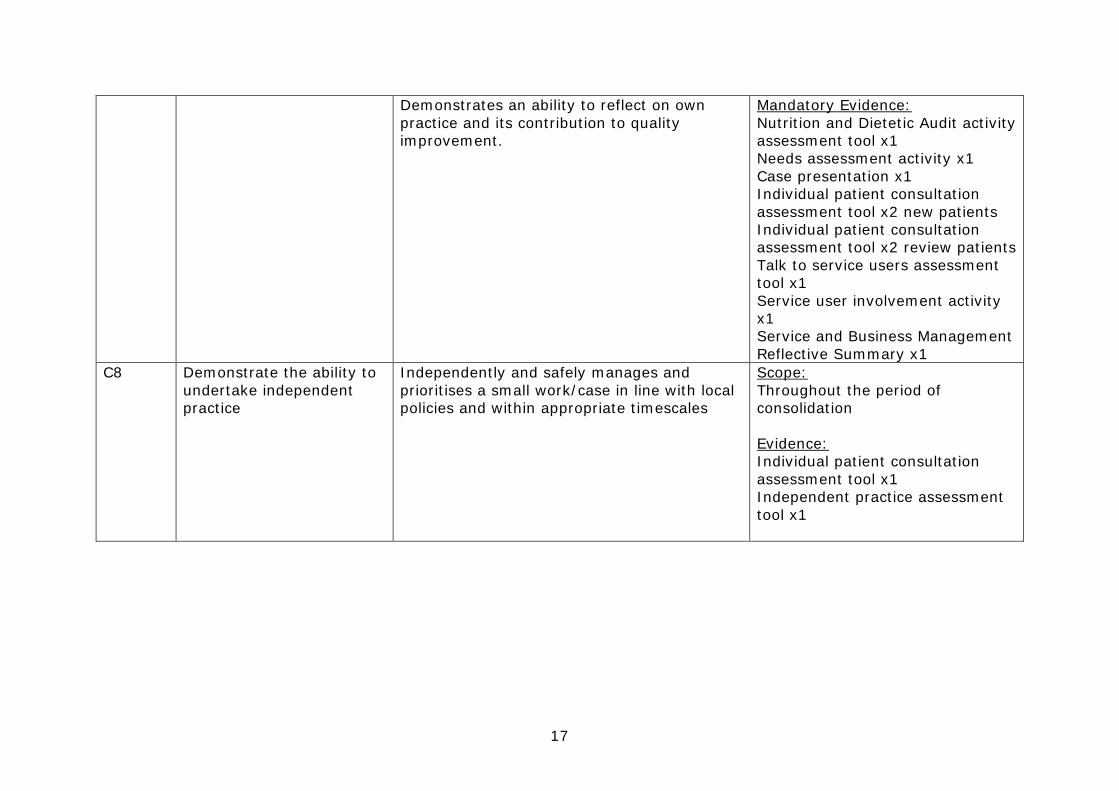
17
Demonstrates an ability to reflect on own practice and its contribution to quality improvement.
Mandatory Evidence: Nutrition and Dietetic Audit activity assessment tool x1 Needs assessment activity x1 Case presentation x1 Individual patient consultation assessment tool x2 new patients Individual patient consultation assessment tool x2 review patients Talk to service users assessment tool x1 Service user involvement activity x1 Service and Business Management Reflective Summary x1
C8 Demonstrate the ability to undertake independent practice
Independently and safely manages and prioritises a small work/case in line with local policies and within appropriate timescales
Scope: Throughout the period of consolidation Evidence: Individual patient consultation assessment tool x1 Independent practice assessment tool x1

18
‘Know, Can, Do’ Model A B C Week 1 2 3 4 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 Professional behaviour
K K C D D D D D D D D D D D D D D D D D D D D D D D D D
Communication K K C D C C C C D D D D D D D D C/D C/D C/D D D D D D D D D D Identification of a nutritional need, and assessment
K K K K K K K C C C C C C C C C C C D D D D D D D D D D
Diagnosis K K K K K K K C C C C C C C C C C C C D D D D D D D D D Intervention K K K K K K K C C C C C C C C C C C C C C C D D D D D D Monitoring and evaluation
K K K K K K K C C C C C C C C C C C C C C C D D D D D D
Quality improvement
K K K K K K K C C C C C C C C C C C C C C C C C D D D D
Definitions: Know = demonstrates with supervision (during observation, questioning or within portfolio evidence) Can = demonstrates with decreasing supervision and support Do = with minimal supervision, and within agreed boundaries
19
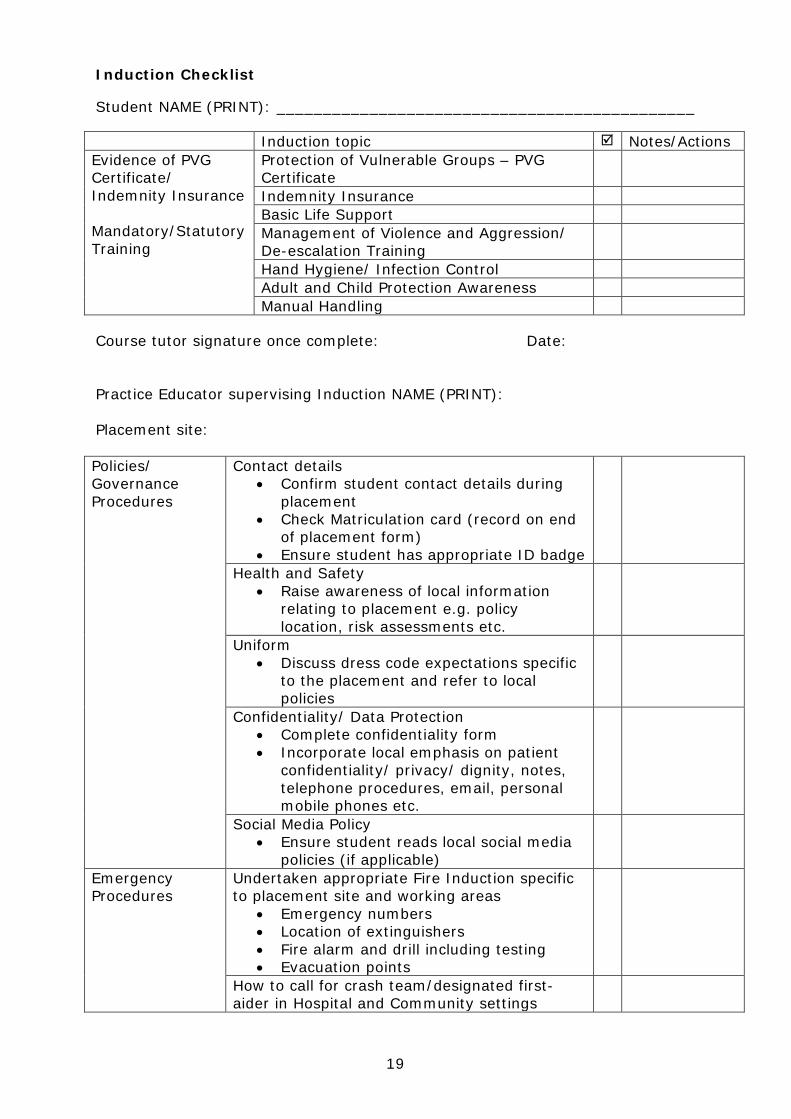
Induction Checklist Student NAME (PRINT): _____________________________________________ Induction topic Notes/Actions Evidence of PVG Certificate/ Indemnity Insurance Mandatory/Statutory Training
Protection of Vulnerable Groups – PVG Certificate
Indemnity Insurance Basic Life Support Management of Violence and Aggression/ De-escalation Training
Hand Hygiene/ Infection Control Adult and Child Protection Awareness Manual Handling
Course tutor signature once complete: Date: Practice Educator supervising Induction NAME (PRINT): Placement site: Policies/ Governance Procedures
Contact details • Confirm student contact details during
placement • Check Matriculation card (record on end
of placement form) • Ensure student has appropriate ID badge
Health and Safety • Raise awareness of local information
relating to placement e.g. policy location, risk assessments etc.
Uniform • Discuss dress code expectations specific
to the placement and refer to local policies
Confidentiality/ Data Protection • Complete confidentiality form • Incorporate local emphasis on patient
confidentiality/ privacy/ dignity, notes, telephone procedures, email, personal mobile phones etc.
Social Media Policy • Ensure student reads local social media
policies (if applicable)
Emergency Procedures
Undertaken appropriate Fire Induction specific to placement site and working areas
• Emergency numbers • Location of extinguishers • Fire alarm and drill including testing • Evacuation points
How to call for crash team/designated first-aider in Hospital and Community settings
20
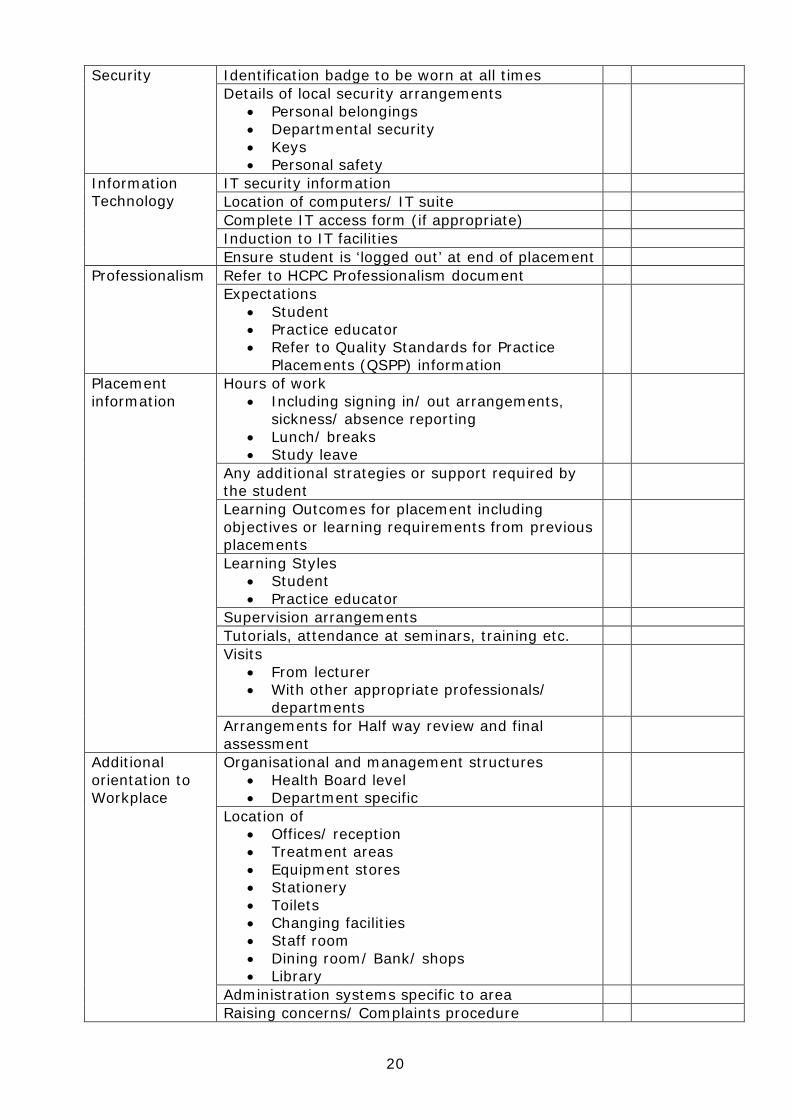
Security Identification badge to be worn at all times Details of local security arrangements
• Personal belongings • Departmental security • Keys • Personal safety
Information Technology
IT security information Location of computers/ IT suite Complete IT access form (if appropriate) Induction to IT facilities Ensure student is ‘logged out’ at end of placement
Professionalism Refer to HCPC Professionalism document Expectations
• Student • Practice educator • Refer to Quality Standards for Practice
Placements (QSPP) information
Placement information
Hours of work • Including signing in/ out arrangements,
sickness/ absence reporting • Lunch/ breaks • Study leave
Any additional strategies or support required by the student
Learning Outcomes for placement including objectives or learning requirements from previous placements
Learning Styles • Student • Practice educator
Supervision arrangements Tutorials, attendance at seminars, training etc. Visits
• From lecturer • With other appropriate professionals/
departments
Arrangements for Half way review and final assessment
Additional orientation to Workplace
Organisational and management structures • Health Board level • Department specific
Location of • Offices/ reception • Treatment areas • Equipment stores • Stationery • Toilets • Changing facilities • Staff room • Dining room/ Bank/ shops • Library
Administration systems specific to area Raising concerns/ Complaints procedure

21
Local Induction Requirements (if relevant)
Placement Evaluation
Advise of placement evaluation procedures
Signed by Supervisor when complete: Date: Signed by Student when complete: Date:

22
Guide to compiling your portfolio This portfolio contains key information about your placement: the expectations placed upon you; details of the tasks and activities that you will undertake; and, copies of the assessment tools that will be used in your assessments. Successfully completing tasks will be evidenced through completed assessment tools that are approved by your Practice Educators, and these have been mapped to each of the learning outcomes. You will therefore have to collect this evidence over the course of your placement in order to demonstrate competence in a range of settings, conditions, with individuals, groups etc. as appropriate to your practice placement. The evidence you collate in this portfolio must be presented well and organised. Your reviewer must be able to find information quickly and easily. Developing these good habits in keeping a portfolio whilst on placement will also benefit your future practice since HCPC require all Registered Dietitians to maintain a continuous, up-to-date and accurate record of their continuing professional development activities. To best achieve this, please take some time to familiarise yourself with the learning outcomes and resources within the pack. Your Practice Educator will design a programme of training that facilitates your ability to demonstrate the learning outcomes. This will involve building your confidence and experience in dealing with individuals, groups and populations through the provision of specialist dietetic services. Your contribution to the care of service users will develop gradually over time and, throughout all of these experiences, you should request assessment and feedback on your performance. You will also develop your practise by demonstrating the ability to reflect on your experiences. Whilst in the early stages of placement, completion of an assessment tool may not result in evidence that you intend to use to demonstrate your competence but will enable you to determine your competence in relation to the ‘Know, Can, Do’ model. The specific activities within this portfolio will all be scheduled at some point within your 12-week placement and your Practice Educator will keep you informed of relevant deadlines. For the majority of time, however, you will be working closely with the dietetic staff in the day-to-day provision of nutritional care to individuals, groups and populations and each of these experiences contribute to your overall assessment. Guide to assessment tools and Evidence This section details which assessment forms are available to record your learning and progress and for which learning outcomes they provide evidence. Some assessment tools are compulsory and relate to specific assessed tasks. Your portfolio of evidence, however, should include more than just the assessment tools; documentary evidence must be included such that an independent observer could assess the information contained within the portfolio. This may be in the form of copies of your presentations, reflective cycles, or other tools, such as the ‘Observation of Practice Tool’. It is important to note that your portfolio must not include any form of information that you did not devise yourself e.g. copies of diet sheets and information sheets given to you by your Practice Educator. Resources not devised by you can be kept
23
in a separate folder for reference. Please note – you can only move to the two week period of ‘Independent Practice’ - C8, if you have achieved competence and have been signed off for learning outcomes C1-C7. Catering This activity is part of your induction to your placement, therefore should be fully completed by the end of week one or midway through week 2. During this activity you will take comprehensive notes of all the tasks you have carried out to enable your Practice Educator to sign you off for this task (within the induction checklist). You will, where possible, complete this as a PAL activity. Individual patient consultation tool (IPC) This form should be used to assess your performance during clinical consultations. It can be used for formative (feedback) or summative assessment. You should aim to do this at least once per week throughout your placement, and asking your Practice Educator or peer to observe your practice. This will help you to get feedback in a formative (informal) way, but will also support your peer in becoming more familiar with the assessment criteria to enhance their own practice. It is your responsibility to ask your peer/ Practice Educator to complete this form. It is likely that you will not present your IPC for summative (formal) assessment until week 7 onwards as you need to demonstrate competence (‘Do’) for all learning outcomes by the end of week 10. The decision as to whether this tool will be used for a summative assessment will be decided by your Practice Educator prior to the consultation (i.e. prospectively) and will be completed by your Practice Educator. You need to collect evidence of consultations with a variety of types of patients in different settings as follows:
• For different client groups e.g. older adults (over 65 years), adults (18-65 years), children (0-16/18 years)
• For different clinical conditions/ dietary treatments (e.g. coeliac disease, diabetes mellitus, food intolerance, nutrition support, weight management)
• In different settings (e.g. inpatient, outpatient, domiciliary visit, care home, day hospital)
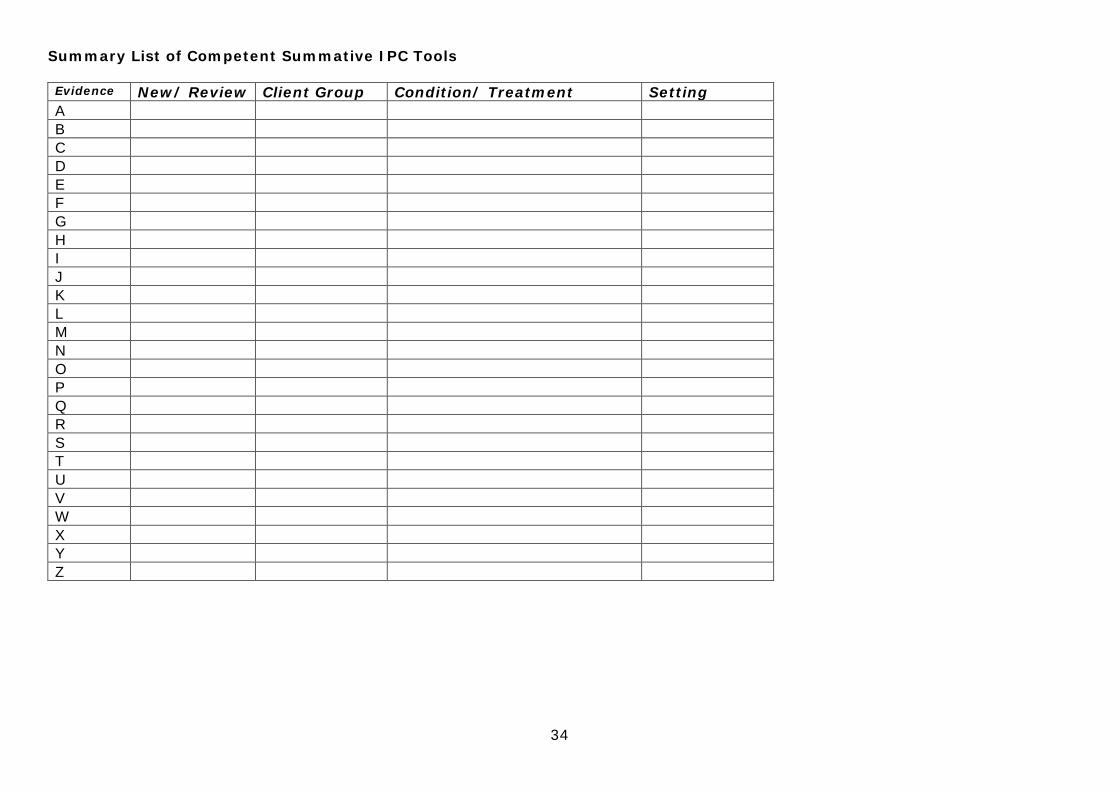
• Both new and review patients Your final portfolio should include only your best evidence, demonstrating competence with a range of patient groups and with different interventions. You are required to submit 5 IPC tools, in total, within your final portfolio and these must all demonstrate competence in each learning outcome, i.e. do not include assessment tools that do not demonstrate all learning outcomes (with the exception of C6 which does not apply in ‘new’ patients). You need to have 4 summative tools completed by the end of week 10 and these should comprise of 2 new patients and 2 review patients. In addition, you need to complete 1 summative IPC tool whilst in your two weeks of independent practice. Where possible, this will be a review patient giving you the opportunity to demonstrate competence in C1-C6 learning outcomes. You must present your evidence (summative assessment forms) in a logical manner. A blank summary sheet is provided within this portfolio to assist you.

24
This will enable you to generate a checklist to ensure sufficient evidence is collected by the end of week 10 and to enable your Practice Educator to cross-reference how the evidence relates to each of the learning outcomes. Having 4 IPC tools (2 new and 2 review) in a range of client groups, conditions and settings will allow your Practice Educator to assess if you have met the competencies to allow you to progress to independent practice. For example:
Evidence New/ Review
Client Group Condition/ Treatment
Setting C1 C2 C3 C4 C5 C6
A Review Older adult Nutrition support OP X X X X X X B Review Adult Enteral feed IP X X X X X X C New Paediatric Nutrition support IP X X X X X D New Adult Low potassium Dialysis
Unit X X X X X
Service user involvement - Involving you: The CARE measure for Student Dietitians tool You will most likely start to use this tool from week 4 or 5 onwards, completing this task by week 9 or 10. In discussion with your Practice Educator, you will ask service users/carers to provide you with feedback on their experience of the health care they received from you. During your placement you should aim to complete 5 CARE measures but, as a minimum, you must complete 3 CARE measures. These can be from a variety of settings e.g. clinic/ home/ ward setting. Once you have obtained the 3-5 completed CARE measures you should reflect on this exercise and put your reflection into your portfolio along with the complete CARE measures. Your reflection should also include how your abilities have progressed since B placement and what you could do to develop further. Needs Assessment This activity will be completed over several days across your placement but will be completed by week 10. You have been given information and checklists to complete this task. At the end of the activity, you will write a summary of the stages on the form provided and you will discuss your findings with your Practice Educator who will sign this off if you meet the acceptable standard. It is worth noting that because you are obtaining factual and up-to-date information relating to a population, this information may well be used to align dietetic services to meet the needs of the population. Once completed and signed off by the Practice Educator, you should put your findings into your portfolio as evidence. Nutrition and Dietetic Audit This activity may be done on consecutive days or across several days. The audit will commence early on in your placement around week 3 or 4 and it should be completed by week 10. The audit will probably be used to ensure that dietetic/nutrition practices are appropriate and you will be advised how you should disseminate your findings. Ideally the chosen area for the audit should have standards available in order for you to audit against. Once you have fully completed the audit and disseminated your findings, you will produce a summary of the activity on the ‘Audit Project Sign off Sheet’ in order for the Practice Educator can sign if you have completed this activity to an acceptable standard. Documentation should then be put into your portfolio as evidence. Talk to service user group Assessment tool
25
This form should be used to assess formal presentations that you deliver. For Placement C you will be required to plan, deliver and evaluate the talk. This may be to a group of patients/ clients or it may be a presentation to other health care professionals. Within your portfolio of evidence, you should also include the plan, talk and evaluation of your presentation. Case presentation Assessment tool With the help of your Practice Educator, you will most likely identify a suitable case study patient/ client/ service user at some point after week 3 or 4 of your placement, and your presentation will take place until around week 8 or 9. You and the service user must complete the case presentation consent form and this should be retained in your portfolio. An appropriate case study is someone who you have seen at least twice and you have been involved with his or her dietetic care. Your case presentation will be assessed by at least two dietitians including the dietitian who is responsible for the service users dietetic care. Once completed all relevant information should be kept in your portfolio. Service and Business Management in a Dietetic Team You will meet with a Dietetic Manager/Team Lead/AHP Lead and discuss elements of service planning/delivery/review in relation to dietetic services so that you have a deeper understanding of their role. You will consider how the management activities relate to safe and effective care of service users. Your reflection on this task should be put into your portfolio. Feed forward form These forms should be completed with your Practice Educator at least every two weeks. Students who require more feedback, for example students who are not yet meeting the ‘Know Can Do’ levels of performance must have this form completed every week. There are elements that should be completed by you (the student) and those which must be completed by the supervisor. Any points raised must be supported by examples/ evidence (which may be a verbal description of events) to ensure that there is clarity. Action points should be agreed and ensure they are SMART (i.e. specific, measureable, achievable, realistic and timely). Any actions should be evaluated to ensure progress is made or to develop further action points as applicable. The feed forward form may also be used as the basis for reviewing your progress more formally at halfway through your placement (alternatively the Review of Placement C form can be used for this). This ‘halfway assessment’ will likely involve a review of your portfolio of evidence collated to date. Independent Practice Assessment Tool You will progress to independent practice (consolidation) once you have demonstrated competency in learning outcomes C1-C7 and you will normally have a minimum of two weeks of independent practice. During this time, you will be given an appropriate caseload for you to manage and your ability to do this whilst continuing to meet all the learning outcomes (C1-C7) will be the basis for you to be signed off as competent for C8. To demonstrate your continued competency, you are also required to complete a summative IPC tool, ideally with a review patient to demonstrate competency in C1-C6 learning outcomes. Your Practice Educator will decide prior to the consultation whether this will be a summative assessment.

26
During this period of independent practice, if you are not continuing to meet any of the learning outcomes an appropriate action plan will be put in place. You will only be signed off as competent for C8 if you have had a successful summative IPC tool completed as well as having managed and prioritised a caseload within appropriate timescales and continue to meet learning outcomes C1-C7. Professionalism checklist This will be completed by the end of week 10 of your placement by your lead supervisor, but may be formatively completed at your halfway assessment. Note that you must continue to meet the professionalism checklist expectations during your period of independent practice. This checklist focuses on you having appropriate communication (verbal and written) consistent professional behaviour in line with the HCPC Guidance on Conduct and Ethics for Students (2016). Observation of Practice Tool These forms can be used to provide additional evidence for a number of learning outcomes but you may find that the tools are most useful to demonstrate evidence of your competence in communication and professionalism. For example, you may undertake visits to departments, spend time with other health and social care professionals, or indeed spend time working with members of the dietetic team who are not directly assessing you e.g. dietetic assistants, administrative staff etc. These experiences and contacts not only allow you to learn about the complex health and social care environment and the implications for dietetic practice, but are valuable in enabling you to demonstrate the learning outcomes with a wide range of people and across environments. You must advise the person, in advance, that you would like them to observe and make comment on your participation, engagement, communication, professionalism, knowledge etc. The form is largely open text so the observer may choose to make as much or as little comment as they wish. This tool may also be useful as a formative feedback tool to support improvement in future so you must be prepared for constructive criticism. Remember that you do not need to include every completed observation of practice tool within your final portfolio; you should be selective in determining which ones are your ‘best evidence’ and enhance areas where you perhaps don’t otherwise have strong documentary evidence. Your final portfolio should include at least 3 ‘observation of practice’ tools.
27
Placement C Induction Activity: Catering It is important that students are familiar with the catering provision for the service they are working in. In view of this students are required to complete the activities below as part of the induction process. The catering activities in both placement B and C and should be completed by the end of week one of the placement and should be signed off as complete on the induction checklist. Where there is no meal provision service in a placement setting this should be noted on the induction checklist. This situation will however be the exception. Where students rotate between sites and where different catering systems exist on each site the students should familiarise themselves with the differences in catering process between the sites but completion of all tasks is not required with each site move. Where students have completed a previous placement in the same Health Board they are not required to complete this activity in the subsequent placements. Where students are completing their C placement and as such have already completed catering activities in placement A and B, it may be that there are similarities in the catering systems between the previous placement and the C placement. In this situation it would be appropriate for the practice educator to discuss the previous catering experiences and to then ask the student to complete only the parts of the catering induction activity which the student may not have experienced in previous placements. This will be at the discretion of the practice educator.
Where possible this activity should be completed as a PAL activity. The purpose of these activities are therefore to familiarise yourselves with: • The catering system that is in place (e.g. production kitchen, cook freeze
service, cook chill service, plated meal service, bulk service etc.) • Timing of meal service/delivery • The preparation and provision of therapeutic diets including the work
undertaken in the diet bay (if applicable) • The meal journey from the perspective of the patients i.e. from completion of
menu to meal production to meal delivery • Any differences between in meal provision (and therapeutic diet adaptations)
across hospital sites e.g. between Acute & Community Hospitals • The system for delivery of oral nutrition supplements to patients in both Acute
and Community hospitals Suggested time allocation: 8 hours (this can be spread over several days) Make notes on each of the following tasks to ensure you are familiar with the catering service and the dietitians role within this. Your notes could form the basis of a student led discussion. To enable you to complete the activity you will be allocated time to spend working in the hospital kitchen, with the diet cooks, in the diet bay and on a ward. Task 1 You should observe and where appropriate participate in the following: -
• Identify the meal delivery system • Observe how the menu analysts liaise with the diet cook (if there is one).
28
• Establish how the diet cooks’ work is generated. • Make notes on the menu i.e. how long the men cycle is, number of choices
at each meal time, provision of hot meals, snack provision, menu coding, choice of portion size etc. and establish how standard recipes are adapted for therapeutic diets.
• Establish which products are used for food enrichment (include quantities per portion) for both Acute and Community Hospitals
• Determine the portion sizes of the meals. • Consider the timing of meal service and any time constraints posed by the
meal service and how these are overcome. • Establish how supplements and tube feeds (if applicable) are delivered to
the wards in both Acute and Community Hospitals • Determine what quality Control measures are in place e.g. use of standard
utensils, temperature of trolleys, checking of trays etc. Task 2 Identify the range of dietetic products used in the hospital and their nutritional contribution to the hospital menu. Task 3 To fully appreciate the meal journey you should follow a patient meal from the point of order i.e. completion of the menu to the point of meal delivery. To do this you should visit a ward to find out how menus are completed and you should follow a meal trolley to a ward and observe meal delivery. In doing this you should note the following:
• Establish how therapeutic diets are ordered at ward level including how many meals in advance meals are ordered
• Follow the meal trolley from the kitchen to a ward • Observe practices when the trolley arrives on the ward (e.g. is the trolley
plugged in? How soon prior to the meal service does the trolley arrive? Is the ward ready for the meal service?)
• Observe meal service – e.g. did the nurses wear aprons and did they use standard utensils? Is a red tray system in place? etc.
• Observe how patients were prepared for mealtimes e.g. were they given an opportunity to wash their hands, visit the bathroom etc.
• Observe where the patients sit to eat their meals • Observe who served the meals to the patients • Observe what fluids were provided at mealtimes • Establish how are patients requiring assistance were identified and whether
assistance was given (this should include all types of assistance e.g. prompting, assistance with opening packages, provision of appropriate cutlery and aids, assistance with feeding etc.
• Observe whether protected mealtimes were in place and whether these were adhered to
• Establish where are supplements were stored on the ward and how these were distributed to patients
• Following the meal establish who cleared the plates away and observe whether left overs were recorded
• For patients who should have food record charts completed observe whether these were completed and by whom
• Establish what provision is made for people who miss a meal • Establish if snacks are available between mealtimes • If possible speak to one patient about their meal time experiences
29
Placement C Activity: Individual Patient Consultations Contributes to learning outcomes: C1; C2; C3; C4; C5; C6; C7 Purpose Throughout Placement C, you will have the opportunity to be involved in one-to-one dietary counselling of service users. This will enable you to further develop your communication skills and demonstrate appropriate knowledge. Guidance Formative assessment: When using the tool retrospectively (i.e. after you have consulted with the patient) this may be completed by your Practice Educator, or PAL partner, and will be used for formative assessment only. You should aim to do this at least once per week throughout your placement so that you become more confident in using the tool, and, by acting on feedback, can progress to getting the tools signed off summatively (this will always be signed off by a Practice Educator). You are responsible for providing the Practice Educator, or PAL, with the assessment tool. Summative assessment: On a regular basis, throughout your placement you should request that your involvement in individual patient consultations be observed by a Practice Educator. You are responsible for providing the Practice Educator with the assessment tool. It is likely that you won’t present your tools for summative assessment until weeks 7-8 as you need to demonstrate ‘Do’ for all learning outcomes by the end of week 10. When presenting this tool to your Practice Educator this will be completed prospectively, i.e. the decision as to whether this will be a summative assessment will be made by the Practice Educator prior to the consultation. The tool will be completed during the patient consultation by the Practice Educator. The competencies should be assessed according to the following criteria: N/A: Not applicable - no opportunity to demonstrate this competency. Not yet met: Competency was relevant but needs more work; it was either not demonstrated or not at the standard required at the end of week 10 yet. Met: Competency was demonstrated at the standard required at the end of week 10 of Placement C. Number of summative tools required You need to have 4 summative IPC tools completed by week 10 and should comprise 2 new patients and 2 review patients. You are also required to complete an IPC tool whilst in your independent practice weeks and this should ideally be a review patient. This will give you the opportunity to demonstrate C1-C6 Learning Outcomes. The patient summary should be completed as follows: Setting: inpatient, outpatient, home visit Patient Group: older adult, south Asian, paediatrics Intervention: nutrition support, IBS, low potassium diet, etc. New/ Follow up: Follow-up patients, only, are suitable for C6 Additional info: carer present, interpreter, etc.

30
Notes for selection for your Portfolio Your final portfolio should include 5 of your best evidence (2 x new patients and 2 x review patients and 1 completed during independent practice), demonstrating competence with a range of settings, patient groups and with different interventions.

31
Individual Patient Consultation Assessment Tool Student: Observing Dietitian: Date: Placement Week:
Patient Summary: Setting New/ Review Patient Group Additional Info. Intervention
Learning outcome and relevant components N/A Not yet
met Met Comments Identification of Nutritional Need and Assessment (C3 or C6) Collects relevant information from records, service user, carer and/or other health and social care professionals, as follows:
• Anthropometry • Biochemistry • Clinical • Dietary • Environmental/ Social
Assesses service user’s general food knowledge and/or cooking skills Identifies service user’s perceived barriers to change Checks understanding of medical condition
Identification of nutrition and dietetic diagnosis (C4 or C6) Correctly interprets assessment information Integrates medical, social and dietary information Generates a PASS statement Correctly identifies and prioritises nutrition and dietetic diagnosis
Care Planning and Implementation (C5 or C6) Develops a dietetic plan prior to consultation Creates suitable physical environment for consultation Considers the knowledge, beliefs and attitudes of the service user Explains how food relates to the condition Provides accurate food and nutrition information Makes reference to a relevant evidence base

32
Learning outcome and relevant components N/A Not yet met Met Comments
Works in partnership with service user to identify possible dietary changes
Explores possible difficulties Develops measureable and specific outcomes, checking understanding and agreement
Selects appropriate resources Concludes consultation appropriately Follow-up arranged as appropriate Professionalism (C1) Adheres to infection control procedures Obtains consent Maintains a non-judgmental attitude Demonstrates sensitivity to confidentiality Recognises and works within scope of practice Works in line with organisational policies, procedures and professional standards
Communication (C2) Greeting, introductions and establishes rapport Establishes background and clarifies reason for consultation Outlines what to expect from consultation Uses appropriate questioning style to elicit relevant information Listens to and demonstrates understanding of the client’s story, using active listening skills
Acknowledges clients view and feelings, using behaviour modification techniques
Uses appropriate non-verbal communication throughout Summarises appropriately throughout consultation Offers written information to reinforce verbal Consultation structured logically Consultation completed in a timely fashion Records relevant quantitative and qualitative information Writes concise, legible, and structured notes in appropriate documents
33
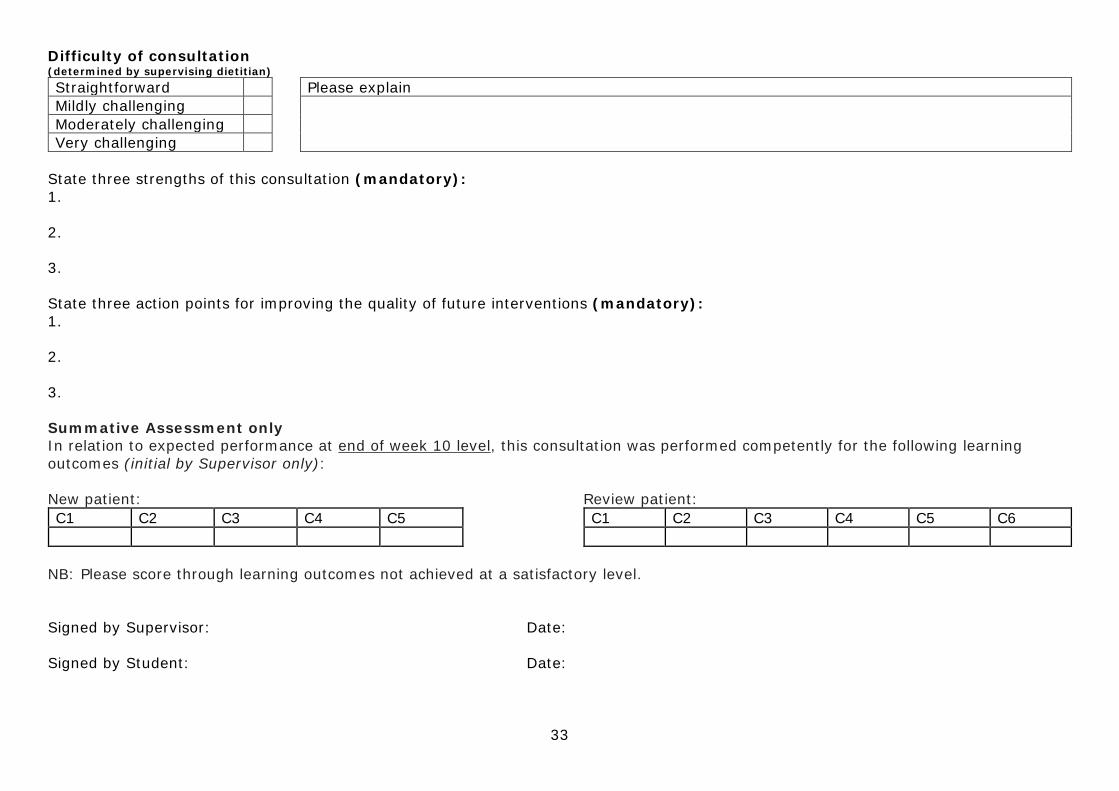
Difficulty of consultation (determined by supervising dietitian) Straightforward Please explain Mildly challenging Moderately challenging Very challenging
State three strengths of this consultation (mandatory): 1. 2. 3. State three action points for improving the quality of future interventions (mandatory): 1. 2. 3. Summative Assessment only In relation to expected performance at end of week 10 level, this consultation was performed competently for the following learning outcomes (initial by Supervisor only): New patient: C1 C2 C3 C4 C5
Review patient: C1 C2 C3 C4 C5 C6
NB: Please score through learning outcomes not achieved at a satisfactory level. Signed by Supervisor: Date: Signed by Student: Date:
34
Summary List of Competent Summative IPC Tools Evidence New/ Review Client Group Condition/ Treatment Setting A B C D E F G H I J K L M N O P Q R S T U V W X Y Z

35
Placement C Activity: Service User Involvement Contributes to Learning Outcomes: C1; C2; C7 Introduction The NHS actively encourages direct feedback from service users and carers about their experiences of the health care they receive. One particular focus of this is to encourage a culture amongst Healthcare professionals whereby the opinions of patients and carers are actively sought about the inter-relational (communication) aspects of their care. In addition, it is also increasingly recognised that service users and carers should be actively engaged in the education of students. Background to the CARE measure: The Consultation and Relational Empathy (Connecting Assessing Responding Empowering) measure (http://www.caremeasure.org/) is a person-centred process measure. It was developed and researched at the Departments of General Practice in Glasgow University and Edinburgh University and recognises the importance of service user involvement. The CARE Measure is a quick clear and easy to complete patient-completed questionnaire which measures and provides feedback to individuals on empathy in the context of the therapeutic relationship during a one-on-one consultation between a clinician and a patient. Originally developed and rigorously tested for use by GPs, it has since been successfully used by other medical staff, allied health professionals (AHPs) and nurses. Although the data from the CARE measure can be analysed and scores compared to other Practitioners, the CARE measure is being used within Placement B and C as a framework for formative experiential feedback to allow you to complete the summative reflective activity which contributes as evidence for C1 and C2. An adapted ‘student’ version (‘Practitioner’ has been changed to Student) is provided within the portfolio which is suitable for use with adults without significant communication or cognitive difficulties. However a visual CARE measure is also available which is suitable for use with children or adults with communication or cognitive difficulties and can be used instead http://www.caremeasure.org/CAREENG10p.pdf Activity instructions: The focus of this activity is to reflect on the process of obtaining service user feedback within a care environment. Whilst the opinions of service users and carers can be obtained using a variety of methods, a common method is to use a patient reported experience measure (PREM). There are several PREMs in existence, but one such PREM increasingly being used in Scotland is the CARE measure. Therefore the purpose of this activity is to provide you with experience of directly seeking and reflecting on feedback from patients and carers using this particular PREM as a framework. The focus of the activity is the about the process of seeking service user involvement rather than the results obtained. You can, of course, use the information obtain from the care measures as formative feedback for your progress on placement C. With guidance from your supervisor and following patient/carer consultations (either in clinic, home or the ward setting), you or your supervisor should ask,

36
where appropriate, service users/carers, whether they would be willing to complete a ‘student’ CARE measure tool to provide you with some feedback. You should make it clear that they do not have to complete a CARE measure if they do not want to and that this will in no way influence the care that they receive. If they are willing, you or your supervisor should ask that they complete the questionnaire and return it to you, your Supervisor or to another agreed person. Note that service users/carers should not put any personal identifying information on the questionnaire itself. You should aim to collect 5 completed CARE measures over the course of your placement but you must complete a minimum of 3. Once you have collected your completed CARE measures, you should use these to reflect (using the reflective framework provided within the portfolio) on the process of seeking and gaining direct feedback from service users and carers e.g. how difficult or easy was it to do so. You should also reflect on the opinions of service users/carers about your perceived ability to connect, assess, respond and empower them and consider how you could further develop your own skills. When completing this during your C placement you should also take the time to reflect on the progression of your abilities during B versus C.
37
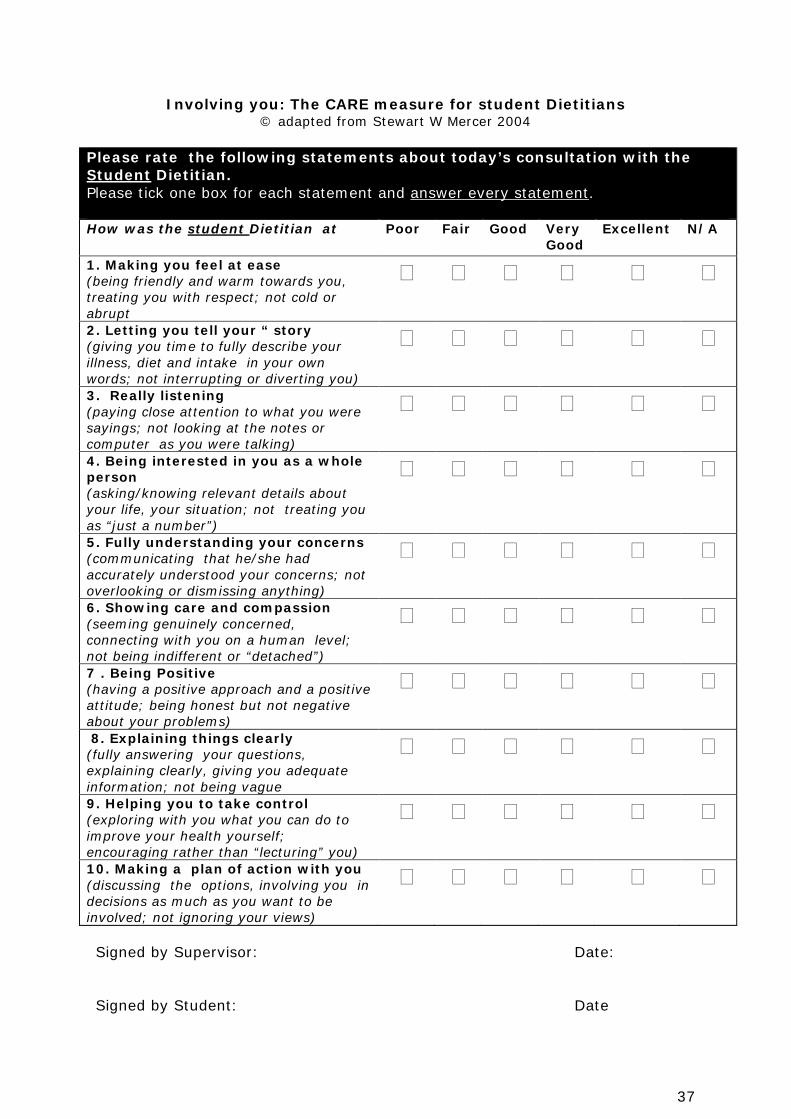
Involving you: The CARE measure for student Dietitians © adapted from Stewart W Mercer 2004
Please rate the following statements about today’s consultation with the Student Dietitian. Please tick one box for each statement and answer every statement. How was the student Dietitian at
Poor Fair Good Very Good
Excellent N/A
1. Making you feel at ease (being friendly and warm towards you, treating you with respect; not cold or abrupt
� � � � � �
2. Letting you tell your “ story (giving you time to fully describe your illness, diet and intake in your own words; not interrupting or diverting you)
� � � � � �
3. Really listening (paying close attention to what you were sayings; not looking at the notes or computer as you were talking)
� � � � � �
4. Being interested in you as a whole person (asking/knowing relevant details about your life, your situation; not treating you as “just a number”)
� � � � � �
5. Fully understanding your concerns (communicating that he/she had accurately understood your concerns; not overlooking or dismissing anything)
� � � � � �
6. Showing care and compassion (seeming genuinely concerned, connecting with you on a human level; not being indifferent or “detached”)
� � � � � �
7 . Being Positive (having a positive approach and a positive attitude; being honest but not negative about your problems)
� � � � � �
8. Explaining things clearly (fully answering your questions, explaining clearly, giving you adequate information; not being vague
� � � � � �
9. Helping you to take control (exploring with you what you can do to improve your health yourself; encouraging rather than “lecturing” you)
� � � � � �
10. Making a plan of action with you (discussing the options, involving you in decisions as much as you want to be involved; not ignoring your views)
� � � � � �
Signed by Supervisor: Date: Signed by Student: Date
38
Placement C Activity: Needs Assessment (NA) of a population/group Contributes to Learning Outcomes: C1; C2; C3; C7; Suggested time allocation: Maximum 1½ - 2 days across the 12 week block. Note that this could be done as ½ days across several weeks and could be done as a PAL activity. Introduction and background Needs assessment (NA) has been defined as a process of measuring the extent and nature of the needs of a particular target population (group) so that services can respond to them (Hooper 1999). It is considered to be an objective and valid method of tailoring health services, as well as an evidence based approach to planning health services (BMJ 1998). The purpose of NA, is to gather information required to bring about change beneficial to the health of a target population/ group and is an important process as the costs of health care continue to rise and at the same time the resources available for healthcare are limited. Although, NAs have more traditionally been undertaken by Public Health professionals looking at a local population/ group, understanding the needs of specific populations are paramount to all healthcare professionals and all Healthcare Professionals and Teams should develop services in line with the identified needs of the ‘populations’ they serve (BMJ 1998). A need is defined as a gap or difference between a current situation and the ideal or desired situation. Most needs assessments are used to identify what the gaps are within a community or population/ group, how to prioritize those gaps, and how to make decisions about which needs can be addressed through a particular intervention. By its nature it focuses on deficiencies (what we need) rather than strengths (what we have already) and thereby fundamentally differs from asset mapping approaches. Assessment of health needs is considered to be more than a process of listening to patients or relying on personal experiences. It is a systematic method of identifying unmet health and healthcare needs of a specific target population/group and making changes to meet these needs (BMJ 1998). Needs assessment can be carried out at various levels:
• International e.g. World Health Organisation • National e.g. Mental health, Dementia, Obesity, Alcohol • Regional e.g. Liver transplantation services, Bariatric surgery services • Health Board e.g. dietetic services, weight management services, GI
services, paediatric services, older adults, low income mothers • Locality e.g. GP practices, social care and voluntary services • Specific populations/groups of service users e.g. diabetes, dialysis,
dementia, coeliac patients, head and neck oncology • Individual e.g. used part of daily individual patient consultations
Needs assessment provides the opportunity to:
39
• Clearly identify and describe the problems of a ‘population’ (group) and the differences from regional, national patterns.
• Learn more about the needs and priorities of a specific ‘population’ of service users/carers
• Highlight areas of unmet need and provide clear objectives to work towards to meet these needs.
• Decide rationally how to use resources to improve a specific ‘populations’ health in the most effective and efficient way.
• Influence policy, interagency collaboration or improvement and research priorities.
There is no easy approach to needs assessment, different topics require different approaches and may involve a combination of qualitative and quantitative methods. However, for the purposes of this activity, the approach described on the following pages, has been adopted. The needs assessment activity With help and guidance from your Practice Supervisor or other relevant staff, you should identify an appropriate ‘population’ (for example, care home, renal, weight management, head and neck oncology, home enteral feeding, coeliac, diabetes, weight management, older adults) to undertake the process of a Nutrition focused needs assessment. Stage 1 Examine and summarise the local routine service/Health Board data/ information available for the identified population/ group to provide you with an understanding of who the population/ group are (e.g. typical age, gender, socio demographics). When doing so, consider the potential nutrition/lifestyle problems they may face as well as the prevalence of such problems. Stage 2 In discussion with the Supervisor of this activity, other relevant members of the multidisciplinary/agency team and by conducting your own research, examine and summarise the locally available services, resources and support that currently exist to address the identified nutrition/lifestyle problems for that population/ group. Stage 3 In trying to proactively seek the views of those the service is provided for, you should undertake a series of conversations (approx. 5-10) with relevant individuals (service users and/or carers and possibly staff depending on the focus of the needs assessment) who currently access/ use the relevant service either via one to one interview, survey or focus group. Aim to explore their expectations of the service, their views on the current service, the resources available and the suggestions they themselves have for changes/improvements (relating to nutrition and lifestyle) e.g. what matters to them? What do they feel they need from the service to manage their own health?
40
Stage 4 From the previous stages consider the following: What are the most appropriate and effective nutrition/lifestyle (clinically and cost effective) proposals/changes that could be implemented by the dietetic service? Identify what would need to be done to implement these, including any resource implications (e.g. staff time, equipment etc.) Stage 5 Focus on one of the nutrition/lifestyle related proposals (identified in stage 4) that could be implemented. Consider the possible positive and negative impacts of implementing the proposal on health and well-being. *Use the additional notes below about the assessment of impact to help you do this. Having considered the possible positive and negative impacts, what (if anything) would need to be amended or other action taken, to maximise the possible positive impacts and minimise the possible negative impacts. Stage 6 Consider how you would monitor and evaluate your chosen proposal should it be implemented (In doing so think back to your Placement B Quality Improvement-service evaluation activity) Finally If you are completing this task with a non-dietetic supervisor, then please complete an observation of practice tool and have this signed by the supervisor as evidence for C1 and C2. Complete the Needs assessment sign off sheet, summarising the 6 stages above. Discuss the process and your findings with the relevant Supervisor of this activity. They will also read and sign your summary and this in turn will be used as evidence for Learning Outcome C1, C2, C3, C7. *Additional notes about the assessment of impact (for use at Stage 5) The assessment of impact is a way to ensure that changes/new proposals do not inadvertently discriminate and where possible promote equality. The key purposes are to promote all aspects of equality, identify whether certain groups may be excluded; identify any possible direct or indirect discrimination; assess whether there is any adverse (negative) impact on particular groups; enhance value for money; act as a method to increase social inclusion. Assessing the likely impact of proposals/plans also makes good common sense, as it is important in developing any proposal/plan to understand how the needs of different groups in the population may differ. Health Boards are legally required to assess any new proposals for equality and diversity impact to ensure that they do not unlawfully discriminate and that they will protect people from discrimination on the basis of ‘protected characteristics’ (see table below for protected characteristics and key points to consider when thinking about impact).
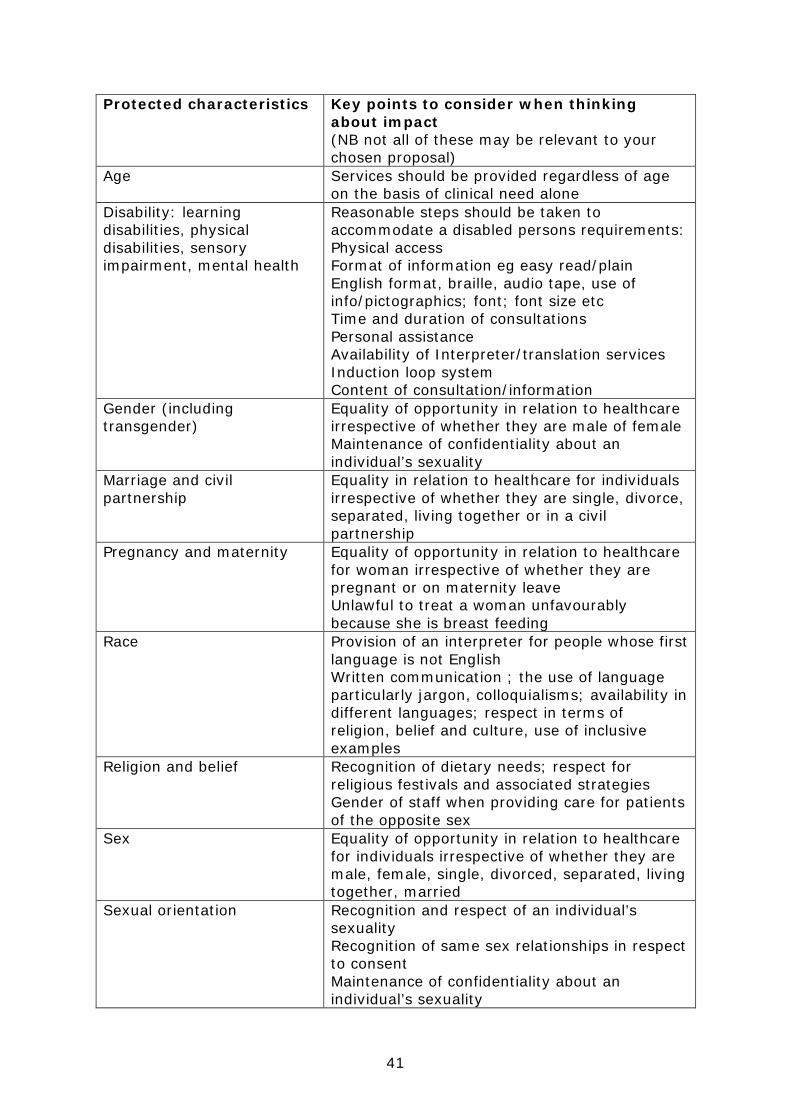
41
Protected characteristics Key points to consider when thinking about impact (NB not all of these may be relevant to your chosen proposal)
Age Services should be provided regardless of age on the basis of clinical need alone
Disability: learning disabilities, physical disabilities, sensory impairment, mental health
Reasonable steps should be taken to accommodate a disabled persons requirements: Physical access Format of information eg easy read/plain English format, braille, audio tape, use of info/pictographics; font; font size etc Time and duration of consultations Personal assistance Availability of Interpreter/translation services Induction loop system Content of consultation/information
Gender (including transgender)
Equality of opportunity in relation to healthcare irrespective of whether they are male of female Maintenance of confidentiality about an individual’s sexuality
Marriage and civil partnership
Equality in relation to healthcare for individuals irrespective of whether they are single, divorce, separated, living together or in a civil partnership
Pregnancy and maternity Equality of opportunity in relation to healthcare for woman irrespective of whether they are pregnant or on maternity leave Unlawful to treat a woman unfavourably because she is breast feeding
Race Provision of an interpreter for people whose first language is not English Written communication ; the use of language particularly jargon, colloquialisms; availability in different languages; respect in terms of religion, belief and culture, use of inclusive examples
Religion and belief Recognition of dietary needs; respect for religious festivals and associated strategies Gender of staff when providing care for patients of the opposite sex
Sex Equality of opportunity in relation to healthcare for individuals irrespective of whether they are male, female, single, divorced, separated, living together, married
Sexual orientation Recognition and respect of an individual’s sexuality Recognition of same sex relationships in respect to consent Maintenance of confidentiality about an individual’s sexuality
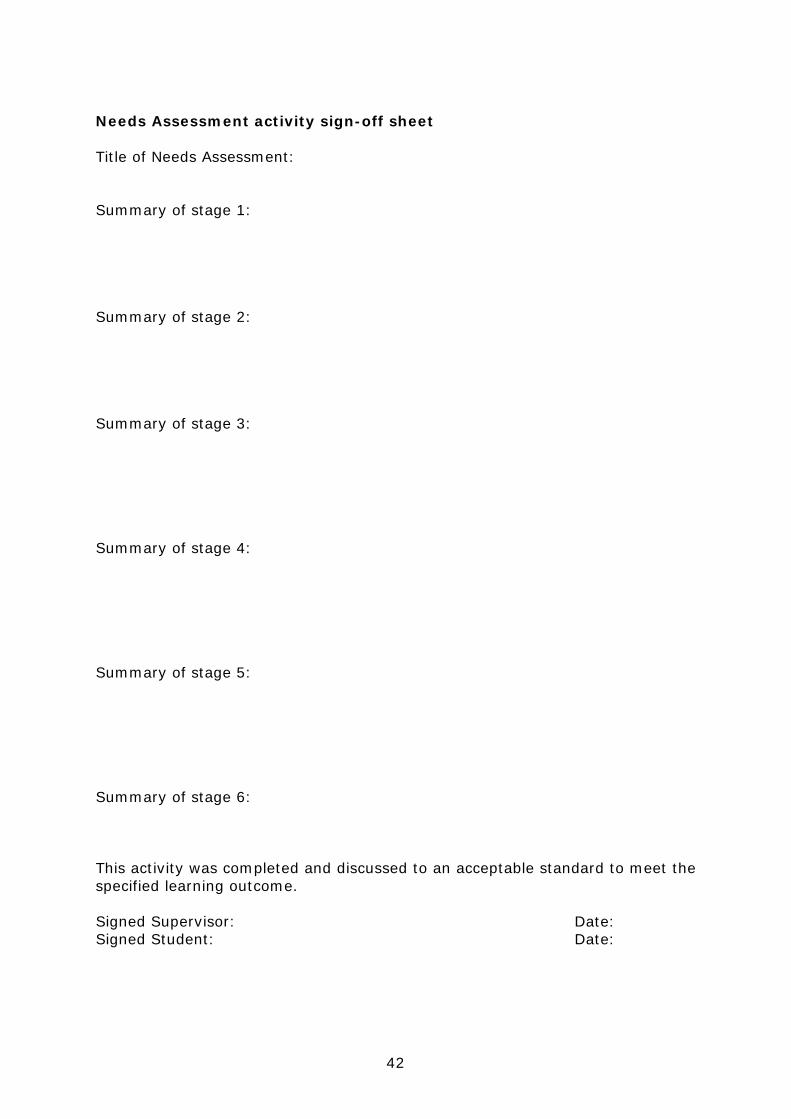
42
Needs Assessment activity sign-off sheet Title of Needs Assessment: Summary of stage 1: Summary of stage 2: Summary of stage 3: Summary of stage 4: Summary of stage 5: Summary of stage 6: This activity was completed and discussed to an acceptable standard to meet the specified learning outcome. Signed Supervisor: Date: Signed Student: Date:
43
Placement C Activity: Nutrition and Dietetic Audit Contributes to Learning Outcomes: C1; C2; C7 Suggested time allocation: Maximum 4-5 days (either as a block of time or across several ½ days). Note that this could also be carried out as a PAL activity. Ensure this is completed successfully by the end of week 10. Purpose This activity allows students to demonstrate knowledge and application of Audit as a quality improvement process. Introduction The audit that you conduct on placement may involve only yourself or perhaps you and another student and may also be conducted over a short, intense time period or a few occasions over several weeks of placement. It is important to think through whether you will need to involve other people in the healthcare team. You will probably be required to present the findings of your audit to the department and so it is important, when designing the audit, to think about how long you will need to analyse the findings and produce a written report and presentation. You may also need to register any audit you undertake with the local R&D department so establish this before you start your audit. What is a Nutrition and Dietetic Audit? Audit is a quality improvement process that was introduced to the NHS by the 1989 White Paper Working for Patients. The current accepted definition as it appears in Principles for Best Practice in Clinical Audit (2002), and endorsed by the National Institute of Clinical Excellence (NICE), is as follows: “… audit is a quality improvement process that seeks to improve patient care and outcomes through systematic review of care against explicit criteria and the implementation of change. Aspects of the structure, process and outcome of care are selected and systematically evaluated against explicit criteria. Where indicated changes are implemented at an individual, team, or service level and further monitoring is used to confirm improvement in healthcare delivery”. In short, an audit is designed to answer the question "Does this service reach a predetermined standard” versus service evaluation, which is designed to answer the question "what standard does this service achieve?" (NHS Research Governance: http://www.apcrc.nhs.uk/governance/is_it_research.htm). Aspects you should consider when undertaking a Nutrition and Dietetic Audit are: Task 1 Undertake background reading and identify a suitable area for audit. To do this read the following document before beginning: http://www.hqip.org.uk/assets/Guidance/HQIP-Clinical-Audit-Simple-Guide-online1.pdf Identify an area of practice that could be subject to audit, or is already a routine area for audit within the service. Ideally you should choose an area that has standards available to enable you to audit against. Task 2
44
Undertake a brief literature review that will provide background information and provide evidence to support the audit. You are not expected to undertake an extensive literature review but your supervisor will be able to provide some guidance as they are likely to be familiar with the topic area. In addition you should critically appraise the literature that you find to ensure that the background to the audit is based on good quality literature. Task 3 Designing the audit Designing a Nutrition and Dietetic Audit usually involves consideration of the following questions: Who will be involved? How will the audit be carried out? Defining the start and end point of the project. Setting an aim for the audit Your audit should have a clearly defined aim Data collection Data collection should be discussed with your supervisor before starting on the audit. Areas to consider include:
• What information you need • The type of information to collect • How the information will be collected (retrospectively from records or
prospectively from patients in a particular setting) including the development of an data collection form
• Whether the data will be valid and reliable • Whether you need to pilot data collection, even if you just spend one or two
hours making sure that your initial ideas are practical • Anonymisation of data
It is also important to consider the sample that you are going to collect data from. What will the sample be e.g. patient records or patients on a ward and how many will you need in the sample? It will be important to consider whether the sample that you choose is representative of the group that you are interested in. Data analysis This part of the audit should consist of being able to use numbers to describe the findings e.g. 10 of 20 patients on a ward had the MUST screening tool fully completed. It is important to think about how you will analyse data before you start collecting it and that will help you to put together a data collection sheet. Audit, at this stage should not involve any statistical tests. Communication (dissemination) of the findings You should be clear how you are going to communicate the findings of the audit and to whom. It might be that you are asked to present the findings to some of the staff in the dietetic department or indeed to staff on a ward. You might also be asked to produce a short report summarising what you have done. Talk to your supervisor and be clear from the start how the findings will be communicated.
45
Nutrition and Dietetic Audit Project Sign off Sheet Title: Source of Project request: Remit given: Conclusions from literature review which should include evidence of critical appraisal: Brief description of audit design: Summary of key findings: Recommendations: Summary of communication (dissemination) activities: This activity was completed to an acceptable standard to meet the specified learning outcomes(s) Signed Dietitian: Date: Signed Student: Date:

46
Placement C Activity: Talk to service user group Contributes to Learning Outcomes: C1, C2, C5, C6, C7 Suggested time allocation: Maximum 1 day Purpose During placement C you will be required to plan, deliver and evaluate at least one presentation/facilitated group session. In most cases, this will be to a group of service users or the general public, and may be clinical or health promotion in nature. However, it is also possible that your audience may be a group health and social care professionals. This activity will enable you to demonstrate the ability to communicate with groups, including relevant content and exhibiting appropriate presentation skills. Task 1 Plan: In C placement, students are required to plan a group talk/ facilitated session. It is this step that is an important distinction between the expectations of a student delivering a talk to a service user group on C placement compared with that on B placement. In some cases, the group session will be part of a regular event however, as a Placement C student, you will not immediately be given access to existing materials. Whilst some arrangements may already have been made for you, as part of the placement programme planning, you will be expected to check all arrangements (room, facilities, timing etc.) You should design the content and any relevant materials that may be needed for the talk. If the talk is part of a previously agreed and standardised event, then you will be provided with the approved materials after you have undertaken your own planning stage. Task 2 Deliver: You will be responsible for the delivery of the group work. You should review the assessment criteria below. Task 3 Evaluate: It will be expected that you will conduct an evaluation of the session with the group, then analyse and produce a short summary of the results. You may be required to develop your own evaluation tool. You are also required to undertake a robust personal reflection of the event (and preparation period). The evaluation results and your personal reflection will enable you to write a short report detailing your conclusions and recommendations for self-improvement and service improvement.
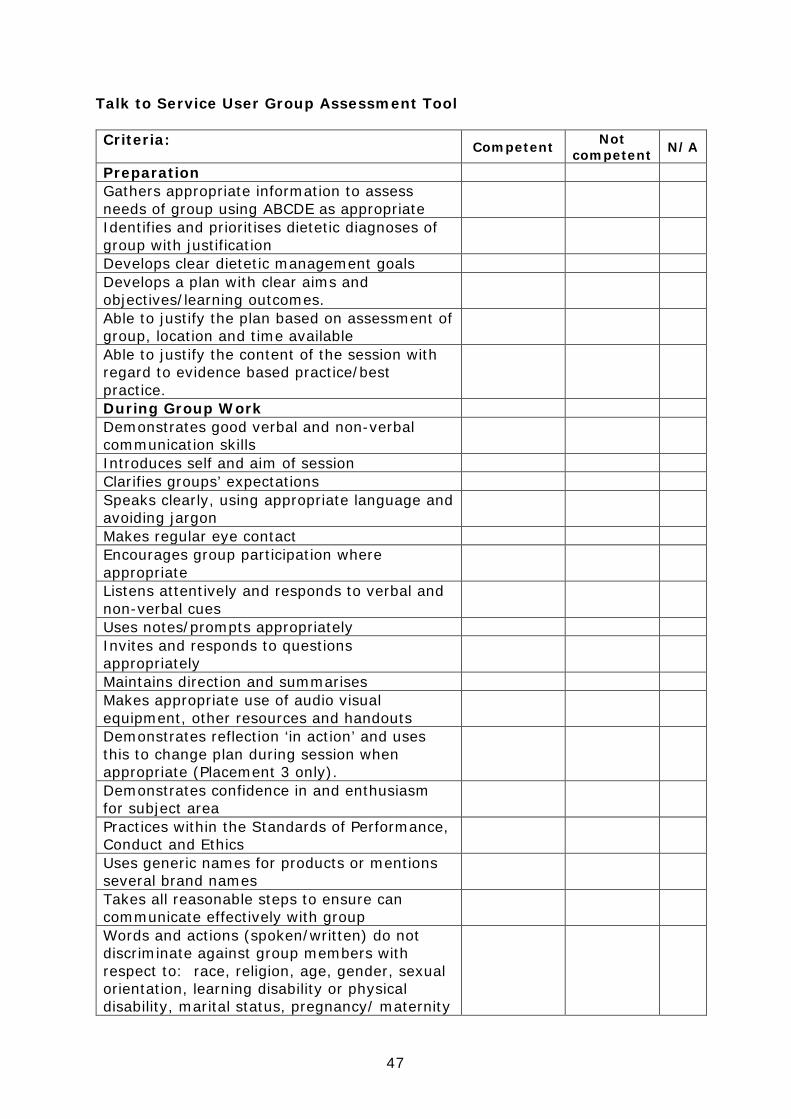
47
Talk to Service User Group Assessment Tool Criteria: Competent Not
competent N/A
Preparation Gathers appropriate information to assess needs of group using ABCDE as appropriate
Identifies and prioritises dietetic diagnoses of group with justification
Develops clear dietetic management goals Develops a plan with clear aims and objectives/learning outcomes.
Able to justify the plan based on assessment of group, location and time available
Able to justify the content of the session with regard to evidence based practice/best practice.
During Group Work Demonstrates good verbal and non-verbal communication skills
Introduces self and aim of session Clarifies groups’ expectations Speaks clearly, using appropriate language and avoiding jargon
Makes regular eye contact Encourages group participation where appropriate
Listens attentively and responds to verbal and non-verbal cues
Uses notes/prompts appropriately Invites and responds to questions appropriately
Maintains direction and summarises Makes appropriate use of audio visual equipment, other resources and handouts
Demonstrates reflection ‘in action’ and uses this to change plan during session when appropriate (Placement 3 only).
Demonstrates confidence in and enthusiasm for subject area
Practices within the Standards of Performance, Conduct and Ethics
Uses generic names for products or mentions several brand names
Takes all reasonable steps to ensure can communicate effectively with group
Words and actions (spoken/written) do not discriminate against group members with respect to: race, religion, age, gender, sexual orientation, learning disability or physical disability, marital status, pregnancy/ maternity
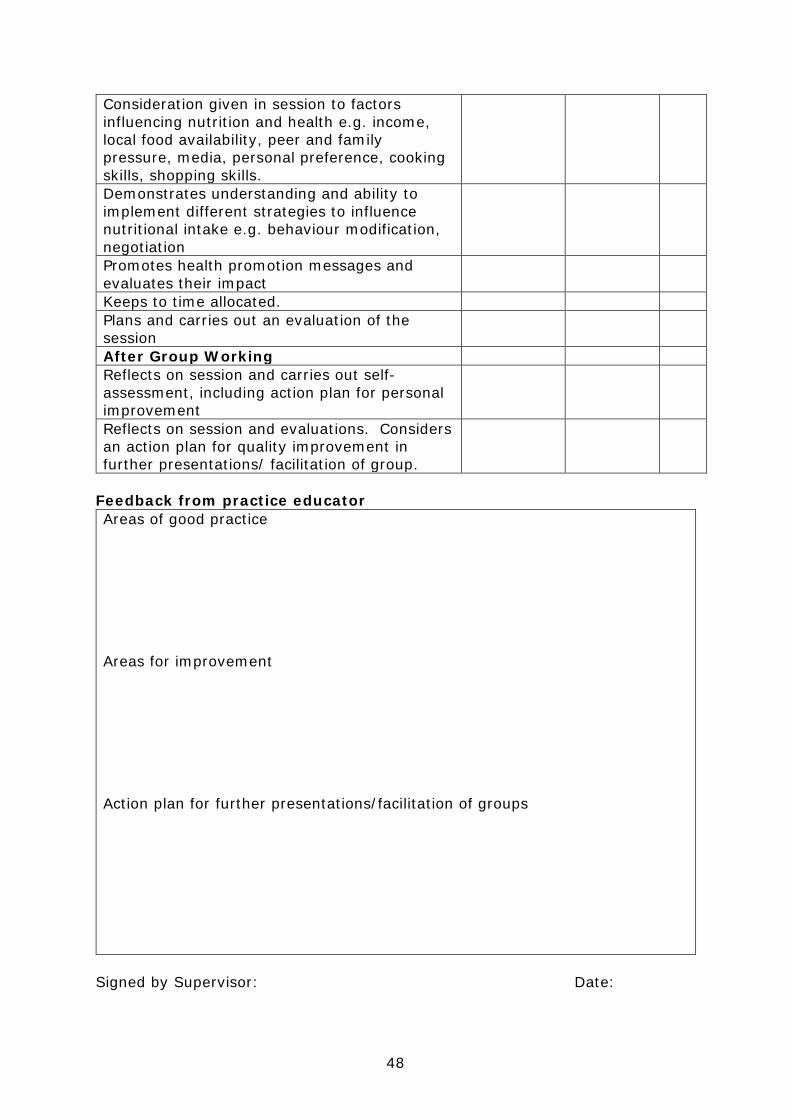
48
Consideration given in session to factors influencing nutrition and health e.g. income, local food availability, peer and family pressure, media, personal preference, cooking skills, shopping skills.
Demonstrates understanding and ability to implement different strategies to influence nutritional intake e.g. behaviour modification, negotiation
Promotes health promotion messages and evaluates their impact
Keeps to time allocated. Plans and carries out an evaluation of the session
After Group Working Reflects on session and carries out self-assessment, including action plan for personal improvement
Reflects on session and evaluations. Considers an action plan for quality improvement in further presentations/ facilitation of group.
Feedback from practice educator Areas of good practice Areas for improvement Action plan for further presentations/facilitation of groups
Signed by Supervisor: Date:
49
Placement C Activity: Case Presentation Contributes to Learning Outcomes: C1, C2, C3, C4, C5, C6, C7 Suggested time: Maximum 1½ days (spread over a number of occasions) Purpose The case presentation will enable you to demonstrate your ability to obtain, assess, interpret and present relevant information. It should also increase your understanding of medical terminology, pathophysiology, prescribed treatments and the patient’s response to treatment. You should use your skills to assemble the relevant data in an informative and understandable way, which may involve the use of graphs, tables and diagrams. Learning Objectives
• To collect, interpret and evaluate relevant details with respect to clinical, nutritional and social history of patient.
• To identify and critically evaluate research literature relevant to patient’s clinical and nutritional treatment.
• To discuss the rationale behind the implementation and any modifications to the nutritional treatment.
• To critically evaluate dietetic practice with reference to current literature, evidence based practice and dietetic services.
Selecting a suitable service user Your Practice Educator will help you in the process of selecting a suitable service user and ensuring the service user has given permission (see consent form below). You should select a service user with whom you are involved in their dietetic care e.g. diet history, anthropometric measurements, nutritional analysis of food intake. This is important because one of the skills that the exercise aims to develop and assess is your ability to respond to the changing situation. It will also ensure that the learning activity is a practical rather than theoretical exercise. You do not need to have been involved in every consultation with the service user over the period of their care, however, you should have participated in at least 2 contacts with the service user or their carer. Timing Once a suitable service user has been identified, one of the supervising dietitians or the student training lead will agree a planned date for the presentation. Throughout the case presentation exercise, you should discuss the service user’s changing situation on a regular basis with the dietitian who is responsible for their care. Confidentiality All information concerning the service user is confidential. To maintain confidentiality, the service user’s name, date of birth/CHI/ward/clinic/address, and the name of the consultant/GP must not be stated. These details should be recorded on a separate sheet of paper and given to the dietitian supervising your case presentation. This is also important if the case presentation is discussed in any forum on your return to university.

50
Information Sources Information on your service user and their treatment may come from various sources including: Documented Sources Dietetic notes, medical notes, nursing notes, care plans,
observation charts, laboratory and other investigation reports.
Individuals Service user (if possible), dietitian treating service user, service user’s relatives/carers, other dietitian’s, other health care professionals involved in service user care.
Reference Sources Books, journals, national/departmental guidelines, websites.
Content Your case presentation should ensure that you cover all of the steps of the nutrition and dietetic care process. You should ensure that your information is evidence-based. This may be through relating to the objective information available about the service user and reference to local policies and procedures but it must also be in relation to the research evidence base; relevant, up-to-date literature should be identified, reviewed and appraised. Assessment of the case presentation You will complete at least one case presentation, lasting 15 minutes with an additional 5 minutes for questions, to a group of dietitians during your placement. Your case presentation will contribute to the assessment of all of the learning outcomes. The case presentation will be assessed by at least 2 dietitians (including the one who was responsible for the service user’s care) using the ‘Case Presentation Assessment Tool’.
51
Case Presentation Consent Form Service User Name: Address: I agree to being the subject of a case presentation to be carried out by …………………………………………………… (Dietetic Student), under the supervision of …………………………………………………… (Dietitian). The aim of the case presentation is that the Dietetic Student will:
• Develop the ability to obtain, assess and present relevant information • Increase awareness of importance of a patient’s medical, cultural, social
and economic circumstances • Increase understanding of medical terminology, disease states, treatments
prescribed and followed and the patient’s response to treatment. I understand that it will be necessary to obtain information from the following sources:
• Myself/my carer • My medical case notes/other clinical information sources • Other healthcare staff involved in my care
I understand that the information in the case presentation will be treated confidentially and that all personal identifiable information will be removed. I understand that the case presentation will be:
• Assessed by the supervising Dietitian and form part of the student’s ongoing assessment
• Summarised by the student in an oral presentation to a small group of Dietitians and fellow dietetic students.
Signed: Date: The completed consent form should be stored within the service user’s dietetic records (and not within the student portfolio).
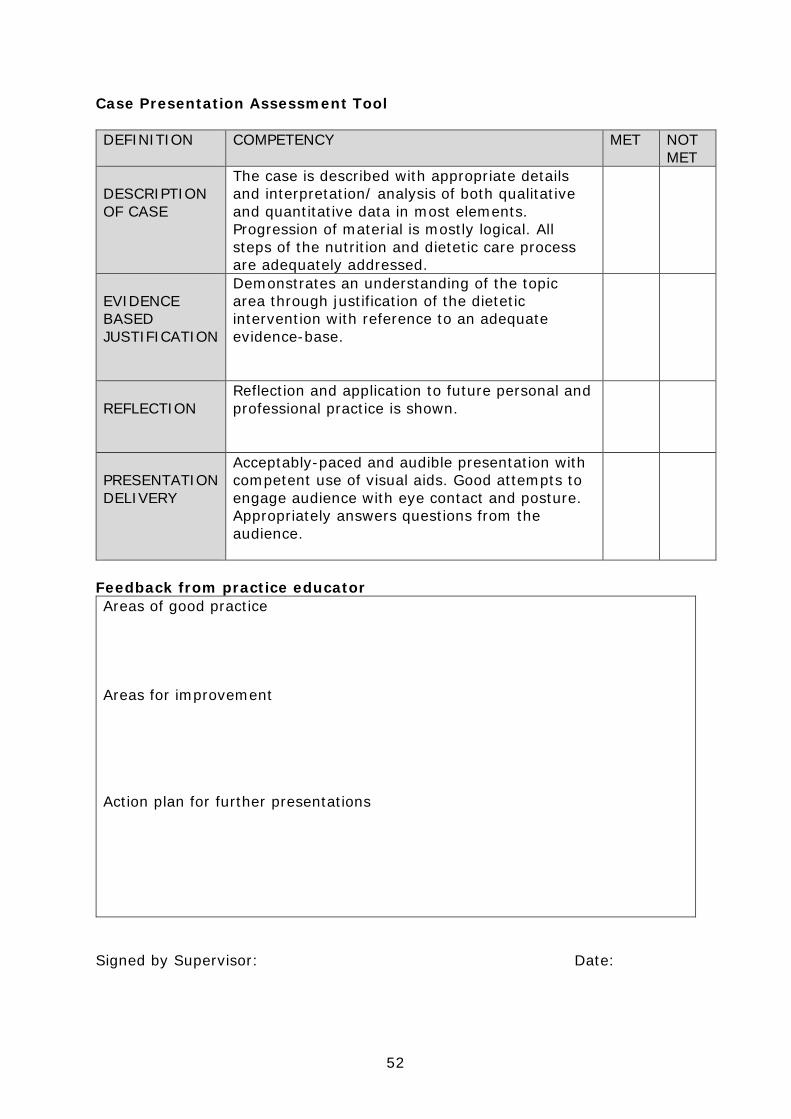
52
Case Presentation Assessment Tool DEFINITION COMPETENCY MET NOT
MET DESCRIPTION OF CASE
The case is described with appropriate details and interpretation/ analysis of both qualitative and quantitative data in most elements. Progression of material is mostly logical. All steps of the nutrition and dietetic care process are adequately addressed.
EVIDENCE BASED JUSTIFICATION
Demonstrates an understanding of the topic area through justification of the dietetic intervention with reference to an adequate evidence-base.
REFLECTION
Reflection and application to future personal and professional practice is shown.
PRESENTATION DELIVERY
Acceptably-paced and audible presentation with competent use of visual aids. Good attempts to engage audience with eye contact and posture. Appropriately answers questions from the audience.
Feedback from practice educator Areas of good practice Areas for improvement Action plan for further presentations
Signed by Supervisor: Date:
53
Placement C Activity: Service and Business Management in a Dietetic Team Contributes to Learning Outcomes: C1, C2, C7 Suggested time allocation: 2 hours, could be done as a PAL/group activity Purpose This activity aims to increase your understanding of the role of the dietetic manager/team leader/AHP lead in relation to the delivery of dietetic services. During your placement you will be given the opportunity to meet with and have a facilitated discussion with a Dietetic manager/lead to enhance your understanding of their role. You will also be given the opportunity to consider the key aspects of managing a service and how this relates to the delivery of safe, effective and patient centred care. Suggested areas for discussion with the Manager/Team Lead/AHP Lead are as follows:
• Their role and responsibilities in service planning, delivery, monitoring and review
• What policy drivers (e.g. Scottish, Health Board, Local) influence Dietetic Service provision and how.
• Their responsibilities in relation to the following activities (the discussion should aim to explore at least 4 of the following areas): • Leadership versus management • Strategic planning • Governance • Financial • Engagement e.g. with other organisations, specialities and departments • Quality • Partnership working • Service development/modernisation • Performance management • Clinical Supervision • Service user feedback and complaints • Health, safety and risk management • Significant adverse events • Safe case load management • Human resource management

54
Reflective summary of Dietetic Service and Business Management Activity Following your discussion, you should write a short reflective summary (approx. 250 words) on what you have learnt. This should be shared with and signed off by the relevant Manager/Team Lead/AHP Lead. The discussion and reflective summary were completed to an acceptable standard to meet the specified learning outcomes. Signed by relevant Manager/Lead: Date: Signed by Student: Date:

55
Feed Forward Form This form should normally be completed at least every 2 weeks. Students who require more feedback, for example students who are not yet meeting the ‘Know, Can, Do’ levels of performance must have this form completed every week. It can also be used at week 6 to formally record performance following a detailed half-way assessment. Alternatively, the Review of Placement C form can be used. At the end of Placement C, in relation to individuals, groups, populations, students should be able to, with minimal supervision, demonstrates competency as follows: Learning outcome Progress identify strengths/areas
for improvement (to be completed by the student)
Total no. competent tools to date
Additional comments about progress and Know/Can/Do stage (to be completed by practice educator)
Action Actions should be specific & measurable (to be completed by the Practice Educator in conjunction with the student)
C1 Consistent professional behaviour in accordance with legal & ethical boundaries, requirements of HCPC and local standards (refer to Professionalism checklist for further information)
K C D (circle as appropriate)
C2 Effective verbal & non-verbal communication skills using a variety of different
56
methods and techniques
K C D (circle as appropriate)
C3 Knowledge and understanding of the identification of nutritional need and assessment
K C D (circle as appropriate)
C4 Knowledge and application of nutritional diagnosis
K C D (circle as appropriate)
C5 Knowledge and application of planning and implementing interventions
K C D (circle as appropriate)
C6 Knowledge and application of monitoring and review
K C D (circle as appropriate)
C7 Knowledge and application of quality improvement and (service) evaluation processes
K C D (circle as appropriate)
Summary:
Signed by Supervisor: Date: Signed by Student: Date:

57
Placement C Activity: Independent practice Contributes to Learning Outcomes: C8 Suggested time allocation: Minimum 2 weeks Purpose Students will progress to independent practice once they have demonstrated competency in learning outcomes C1-C7. Students will normally complete a minimum of 2 weeks of independent practice. Students can progress to independent practice earlier than week 11 if all required assessment tools are complete (see guidance on each assessment tool). Guidance on appropriate caseload and evidence The caseload for independent practice weeks at the end of Placement C will vary within settings and it would be difficult to specify this in terms of wards, patients, clinics etc. Practice Educators should decide on an appropriate caseload for dietetic students in relation to the individual practice setting. An appropriate caseload should reflect the responsibilities of the early stages of a new Graduate Band 5 Dietitian (e.g. once all induction activities are completed). You may wish to include some of the following within the independent practice period to offer a realistic reflection of a new Band 5 role: Out Patient Clinics In patients / Wards Home Visits (where usual risk assessment has been carried out and deemed safe) Nursing Home visits Ward rounds Case conferences Health Promotion work Group work / Group presentations e.g. Cardiac rehabilitation Mock Interview The student caseload should be monitored throughout the independent practice period and adjusted appropriately in relation to the volume of new referrals or patient complexity. To demonstrate your continued competency, you are also required to complete one summative IPC tool during your independent practice weeks, ideally with a review patient to demonstrate competency in C1-C6 learning outcomes. Your Practice Educator will decide prior to the consultation whether this will be a summative assessment.
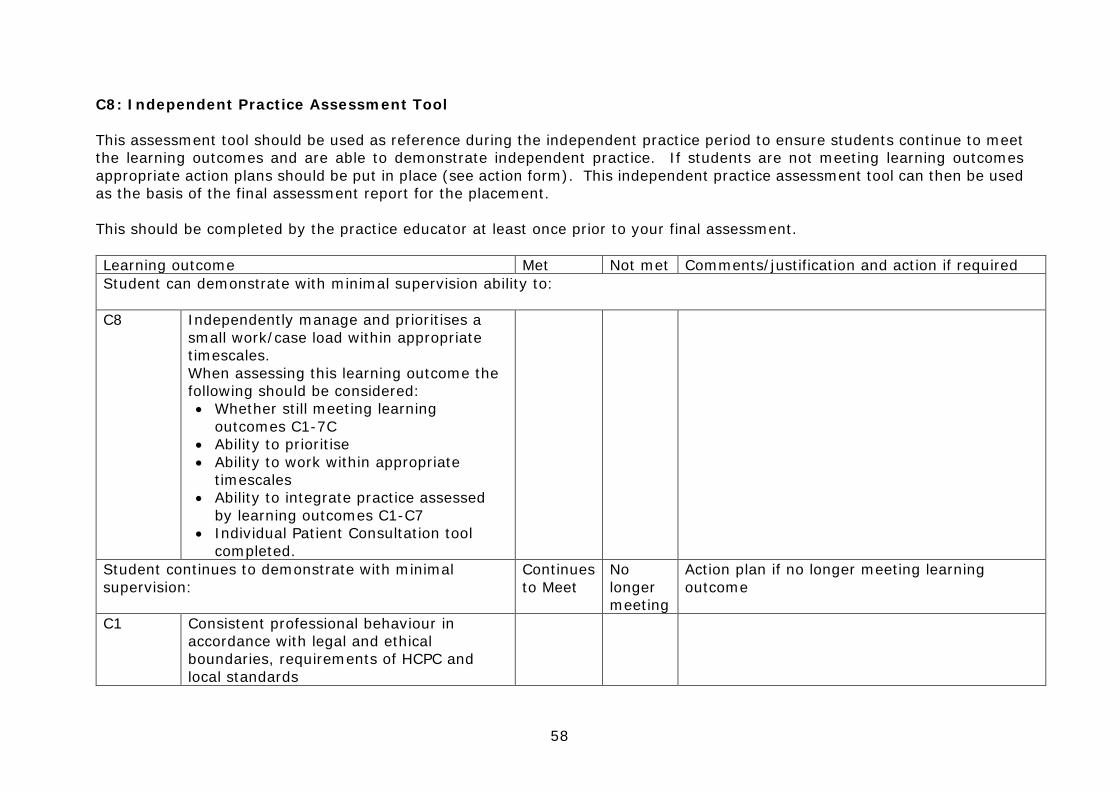
58
C8: Independent Practice Assessment Tool This assessment tool should be used as reference during the independent practice period to ensure students continue to meet the learning outcomes and are able to demonstrate independent practice. If students are not meeting learning outcomes appropriate action plans should be put in place (see action form). This independent practice assessment tool can then be used as the basis of the final assessment report for the placement. This should be completed by the practice educator at least once prior to your final assessment. Learning outcome Met Not met Comments/justification and action if required Student can demonstrate with minimal supervision ability to: C8 Independently manage and prioritises a
small work/case load within appropriate timescales. When assessing this learning outcome the following should be considered: • Whether still meeting learning
outcomes C1-7C • Ability to prioritise • Ability to work within appropriate
timescales • Ability to integrate practice assessed
by learning outcomes C1-C7 • Individual Patient Consultation tool
completed.
Student continues to demonstrate with minimal supervision:
Continues to Meet
No longer meeting
Action plan if no longer meeting learning outcome
C1 Consistent professional behaviour in accordance with legal and ethical boundaries, requirements of HCPC and local standards
59
C2 Effective verbal and non-verbal
communication skills using a variety of different methods and techniques
C3 Knowledge and application of the identification of nutritional need and assessment
C4 Knowledge and application of nutritional diagnosis
C5 Knowledge and application of planning and implementing interventions
C6 Knowledge and application of monitoring and review
C7 Knowledge and application of quality improvement and (service) evaluation processes
For the final assessment any additional comments that would be useful for the student in terms of career progression
Signed by Supervisor: Date: Signed by Student: Date:
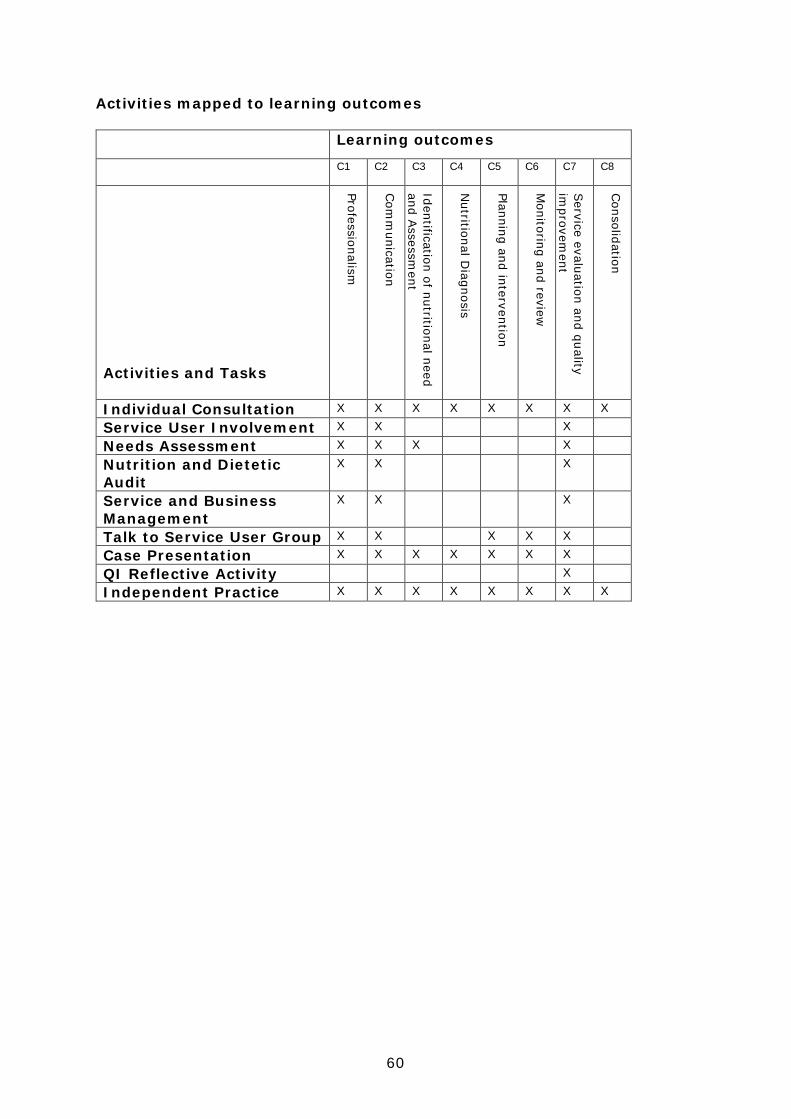
60
Activities mapped to learning outcomes Learning outcomes C1 C2 C3 C4 C5 C6 C7 C8
Activities and Tasks
Professionalism
Com
munication
Identification of nutritional need and A
ssessment
Nutritional D
iagnosis
Planning and intervention
Monitoring and review
Service evaluation and quality
improvem
ent
Consolidation
Individual Consultation X X X X X X X X
Service User Involvement X X X
Needs Assessment X X X X
Nutrition and Dietetic Audit
X X X
Service and Business Management
X X X
Talk to Service User Group X X X X X
Case Presentation X X X X X X X
QI Reflective Activity X
Independent Practice X X X X X X X X
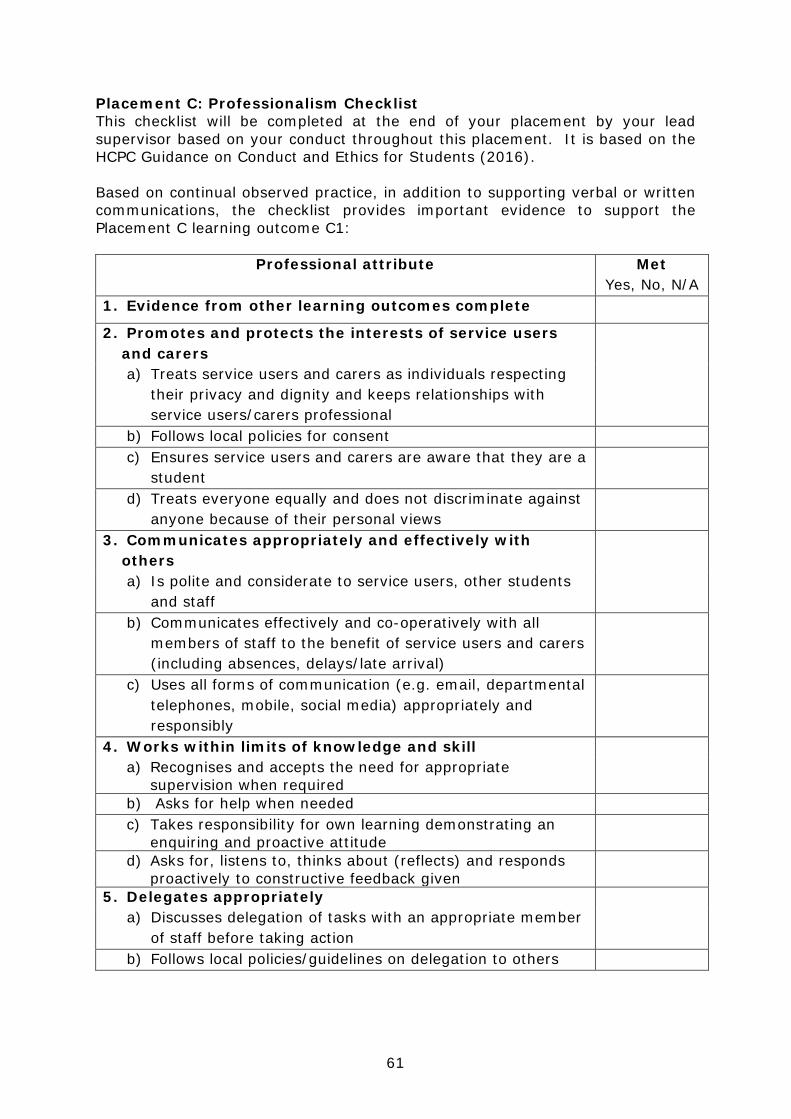
61
Placement C: Professionalism Checklist This checklist will be completed at the end of your placement by your lead supervisor based on your conduct throughout this placement. It is based on the HCPC Guidance on Conduct and Ethics for Students (2016). Based on continual observed practice, in addition to supporting verbal or written communications, the checklist provides important evidence to support the Placement C learning outcome C1:
Professional attribute Met Yes, No, N/A
1. Evidence from other learning outcomes complete
2. Promotes and protects the interests of service users and carers
a) Treats service users and carers as individuals respecting their privacy and dignity and keeps relationships with service users/carers professional
b) Follows local policies for consent c) Ensures service users and carers are aware that they are a
student
d) Treats everyone equally and does not discriminate against anyone because of their personal views
3. Communicates appropriately and effectively with others
a) Is polite and considerate to service users, other students and staff
b) Communicates effectively and co-operatively with all members of staff to the benefit of service users and carers (including absences, delays/late arrival)
c) Uses all forms of communication (e.g. email, departmental telephones, mobile, social media) appropriately and responsibly
4. Works within limits of knowledge and skill a) Recognises and accepts the need for appropriate
supervision when required
b) Asks for help when needed c) Takes responsibility for own learning demonstrating an
enquiring and proactive attitude
d) Asks for, listens to, thinks about (reflects) and responds proactively to constructive feedback given
5. Delegates appropriately a) Discusses delegation of tasks with an appropriate member
of staff before taking action
b) Follows local policies/guidelines on delegation to others
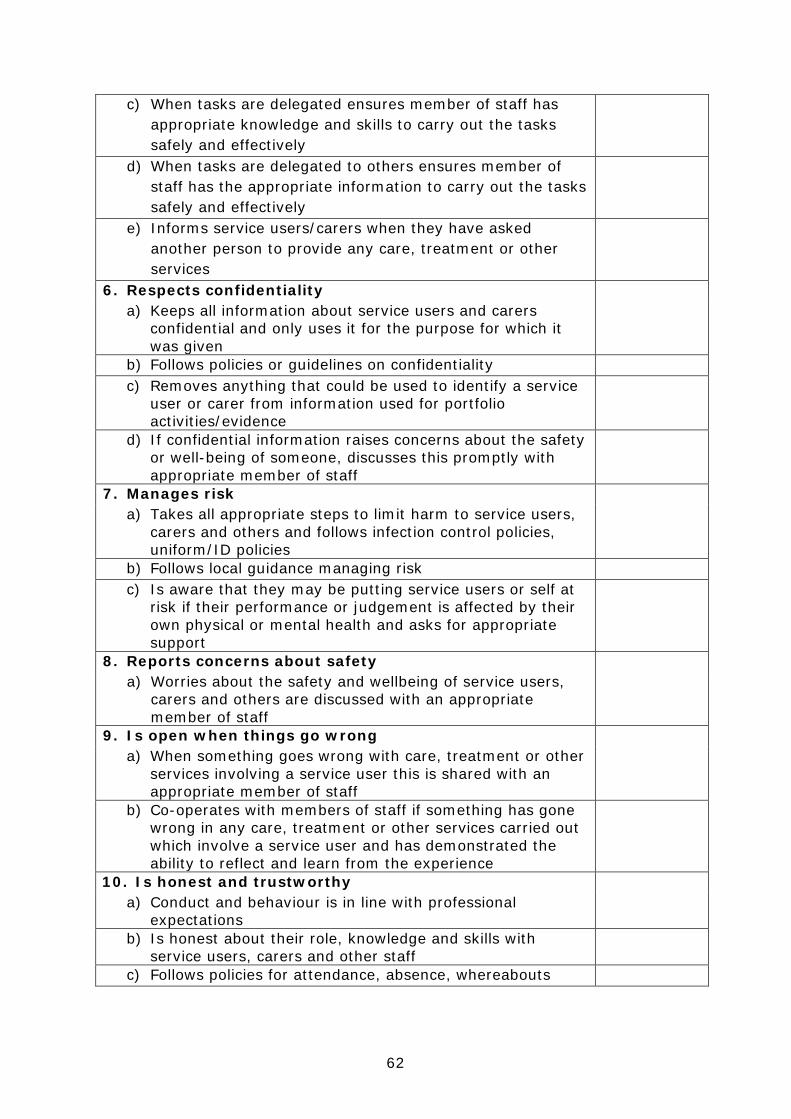
62
c) When tasks are delegated ensures member of staff has appropriate knowledge and skills to carry out the tasks safely and effectively
d) When tasks are delegated to others ensures member of staff has the appropriate information to carry out the tasks safely and effectively
e) Informs service users/carers when they have asked another person to provide any care, treatment or other services
6. Respects confidentiality a) Keeps all information about service users and carers
confidential and only uses it for the purpose for which it was given
b) Follows policies or guidelines on confidentiality c) Removes anything that could be used to identify a service
user or carer from information used for portfolio activities/evidence
d) If confidential information raises concerns about the safety or well-being of someone, discusses this promptly with appropriate member of staff
7. Manages risk a) Takes all appropriate steps to limit harm to service users,
carers and others and follows infection control policies, uniform/ID policies
b) Follows local guidance managing risk c) Is aware that they may be putting service users or self at
risk if their performance or judgement is affected by their own physical or mental health and asks for appropriate support
8. Reports concerns about safety a) Worries about the safety and wellbeing of service users,
carers and others are discussed with an appropriate member of staff
9. Is open when things go wrong a) When something goes wrong with care, treatment or other
services involving a service user this is shared with an appropriate member of staff
b) Co-operates with members of staff if something has gone wrong in any care, treatment or other services carried out which involve a service user and has demonstrated the ability to reflect and learn from the experience
10. Is honest and trustworthy a) Conduct and behaviour is in line with professional
expectations
b) Is honest about their role, knowledge and skills with service users, carers and other staff
c) Follows policies for attendance, absence, whereabouts

63
d) Activities and assessment records have been completed accurately and truthfully and work by others has not been passed off as own
e) Shares important information about conduct, competence and health
11. Keeps records clear and accurate records of work with service users and carers that reflects record keeping policies
Signed by Supervisor: Date: Signed by Student: Date:
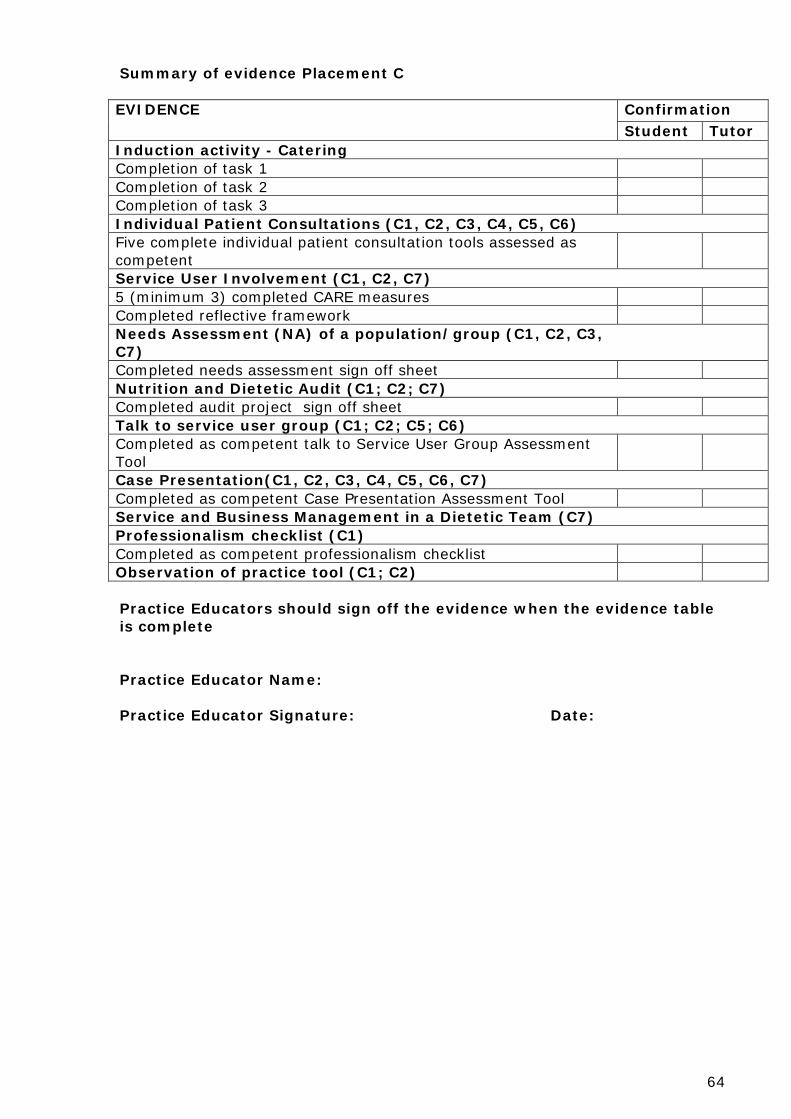
64
Summary of evidence Placement C EVIDENCE Confirmation Student Tutor Induction activity - Catering Completion of task 1 Completion of task 2 Completion of task 3 Individual Patient Consultations (C1, C2, C3, C4, C5, C6) Five complete individual patient consultation tools assessed as competent
Service User Involvement (C1, C2, C7) 5 (minimum 3) completed CARE measures Completed reflective framework Needs Assessment (NA) of a population/group (C1, C2, C3, C7) Completed needs assessment sign off sheet Nutrition and Dietetic Audit (C1; C2; C7) Completed audit project sign off sheet Talk to service user group (C1; C2; C5; C6) Completed as competent talk to Service User Group Assessment Tool
Case Presentation(C1, C2, C3, C4, C5, C6, C7) Completed as competent Case Presentation Assessment Tool Service and Business Management in a Dietetic Team (C7) Professionalism checklist (C1) Completed as competent professionalism checklist Observation of practice tool (C1; C2) Practice Educators should sign off the evidence when the evidence table is complete Practice Educator Name: Practice Educator Signature: Date:

65
Observation of Practice Tool Student: Witness name and role: Date: Placement Week:
Occasion/ Event witnessed: Actions Observed/Topic Discussed Please comment on the following: Professionalism Punctuality:
Communication Skills: Interest/Enthusiasm:
Signed by Witness: Date: Signed by Student: Date:
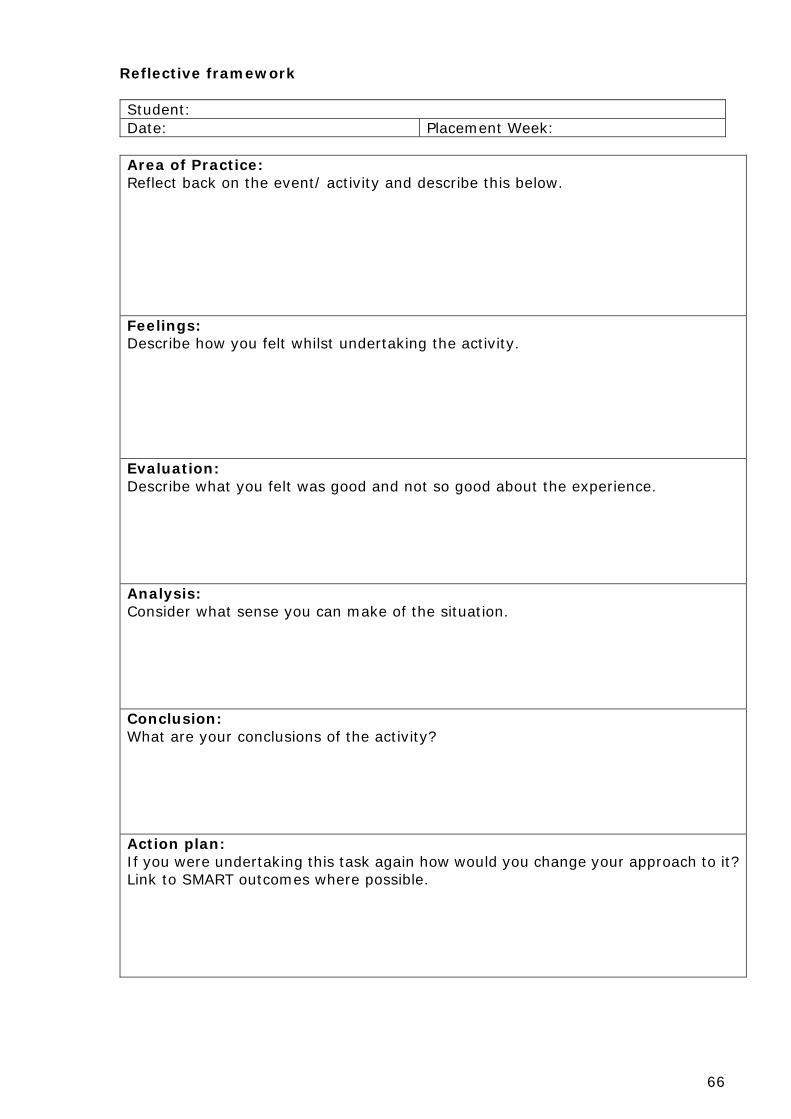
66
Reflective framework Student: Date: Placement Week:
Area of Practice: Reflect back on the event/ activity and describe this below. Feelings: Describe how you felt whilst undertaking the activity. Evaluation: Describe what you felt was good and not so good about the experience. Analysis: Consider what sense you can make of the situation. Conclusion: What are your conclusions of the activity? Action plan: If you were undertaking this task again how would you change your approach to it? Link to SMART outcomes where possible.
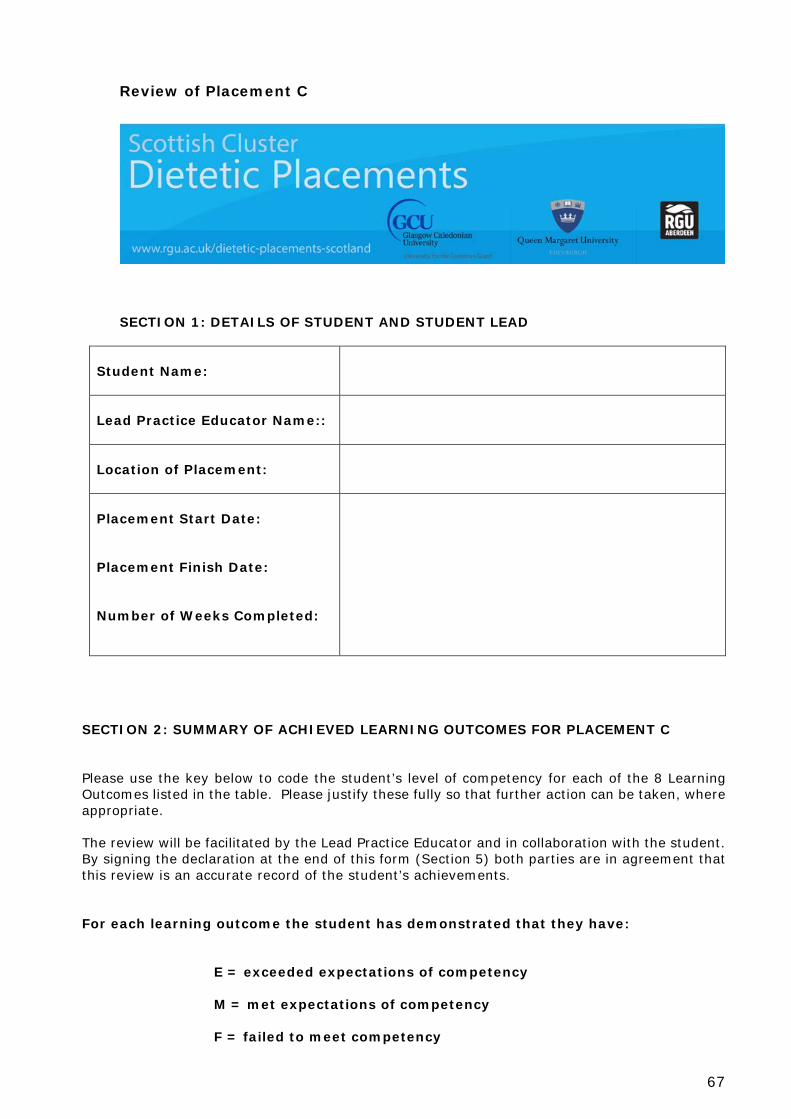
67
Review of Placement C
SECTION 1: DETAILS OF STUDENT AND STUDENT LEAD
Student Name:
Lead Practice Educator Name::
Location of Placement:
Placement Start Date: Placement Finish Date: Number of Weeks Completed:
SECTION 2: SUMMARY OF ACHIEVED LEARNING OUTCOMES FOR PLACEMENT C Please use the key below to code the student’s level of competency for each of the 8 Learning Outcomes listed in the table. Please justify these fully so that further action can be taken, where appropriate. The review will be facilitated by the Lead Practice Educator and in collaboration with the student. By signing the declaration at the end of this form (Section 5) both parties are in agreement that this review is an accurate record of the student’s achievements.
For each learning outcome the student has demonstrated that they have:
E = exceeded expectations of competency M = met expectations of competency F = failed to meet competency

68
Learning Outcome Code Justification Action Plan C1 Demonstrate consistent
professional behaviour in accordance with legal and ethical boundaries, requirements of HCPC and local standards/policies
C2 Demonstrate effective verbal and non-verbal communication skills using a variety of different methods and techniques
C3 Demonstrate applied knowledge and understanding of the identification of nutritional need and assessment
C4 Demonstrate applied knowledge and understanding of nutritional diagnosis
C5 Demonstrate applied knowledge and understanding of planning and implementing interventions
C6 Demonstrate applied knowledge and understanding of monitoring, review and evaluation
C7 Demonstrate applied knowledge and understanding of quality improvement and service evaluation processes
C8 Demonstrate the ability to undertake independent practice
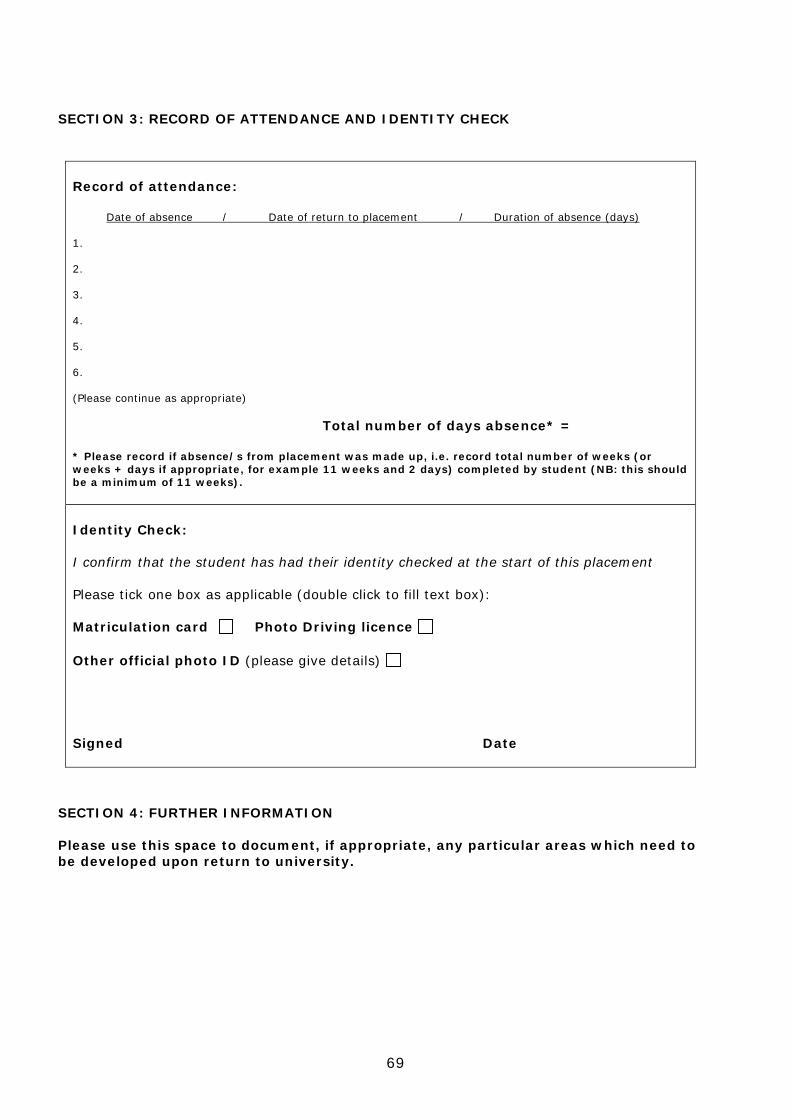
69
SECTION 3: RECORD OF ATTENDANCE AND IDENTITY CHECK
Record of attendance: Date of absence / Date of return to placement / Duration of absence (days) 1. 2. 3. 4. 5. 6. (Please continue as appropriate) Total number of days absence* = * Please record if absence/s from placement was made up, i.e. record total number of weeks (or weeks + days if appropriate, for example 11 weeks and 2 days) completed by student (NB: this should be a minimum of 11 weeks). Identity Check: I confirm that the student has had their identity checked at the start of this placement Please tick one box as applicable (double click to fill text box): Matriculation card Photo Driving licence Other official photo ID (please give details) Signed Date
SECTION 4: FURTHER INFORMATION Please use this space to document, if appropriate, any particular areas which need to be developed upon return to university.
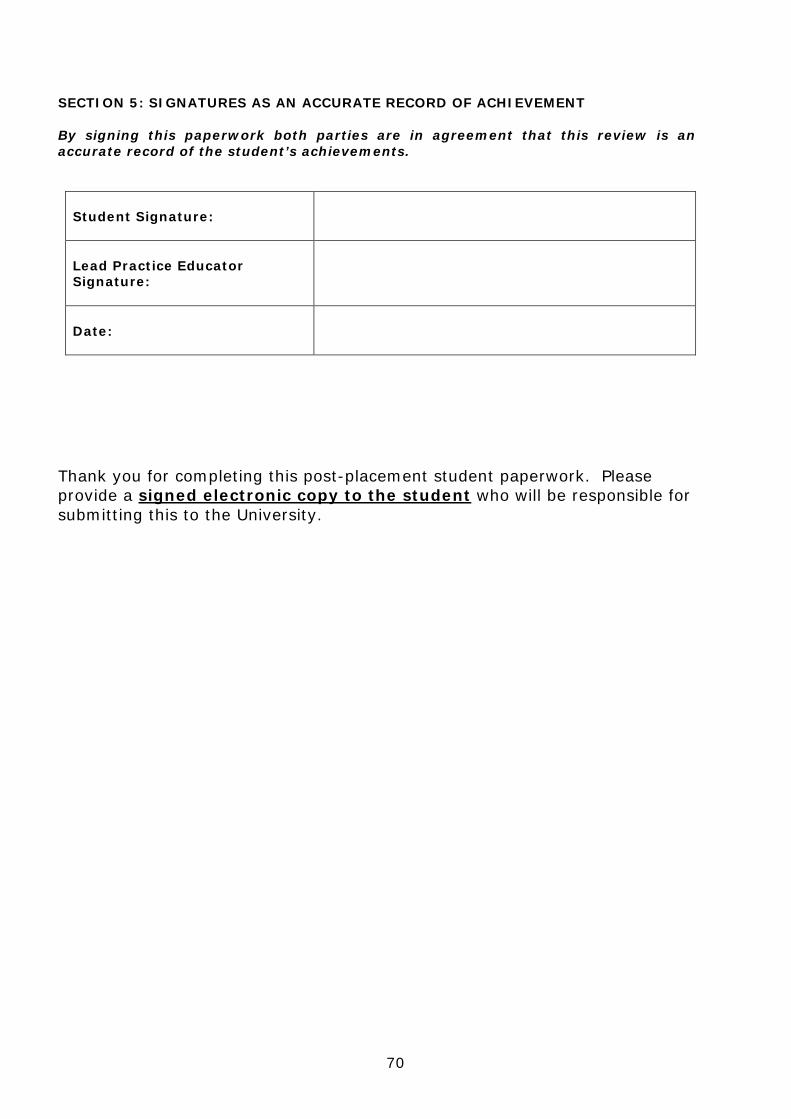
70
SECTION 5: SIGNATURES AS AN ACCURATE RECORD OF ACHIEVEMENT By signing this paperwork both parties are in agreement that this review is an accurate record of the student’s achievements.
Student Signature:
Lead Practice Educator Signature:
Date:
Thank you for completing this post-placement student paperwork. Please provide a signed electronic copy to the student who will be responsible for submitting this to the University.
71
APPENDICES
72
Understanding Duty of Care What is duty of care? Duty of care is the legal obligation that dietitians (and all health professionals) have to reasonably ensure that no harm comes to any patient under their care. When do you open a duty of care? Following receipt and triage of a referral the dietitian undertakes an assessment and, based on analysis of this assessment, the dietitian makes an evidenced based judgement as to whether dietetic intervention (or education) would or would not be of benefit to the patient. If it is judged that dietetic intervention would benefit a patient it is at this point that the duty of care is opened. If it is judged that dietetic intervention would be of no benefit to a patient then no duty of care is opened. Closing or passing on a duty of care
• Duty of care would normally be closed in the following circumstances: • A patient has met agreed goal(s)/outcome(s). • Further dietetic consultation is judged to be not required (or not
appropriate) and, if intervention is to continue, the duty of care may be passed on to the patient or other appropriate health and social care profession. The decision on when and who to pass the duty of care to rests with the dietitian. For example, when a patient is seen in a consultative capacity the duty of care would be closed and may be passed on to the patient.
• Further dietetic consultation is unlikely to be of benefit.
Important points to remember
• Collecting information on a referral this does not mean duty of care has been opened.
• When you speak to a patient to ask about their medical or nutritional history, this also does not mean a duty of care has been opened.
• If a patient/individual refuses/fails to attend an appointment, or consent to intervention, then a duty of care cannot be opened.
• If you do not open a duty of care this should be communicated back to the referrer, clearly and succinctly, outlining the rationale for your decision (N.B. It is unlikely that you will use the term ‘not open a duty of care’).
• If you feel a patient referred to you and/or assessed by you is out with your scope and range of practice you should not enter into a duty of care. In such an instance you should refer the patient on to an appropriate colleague or consult your clinical team lead.
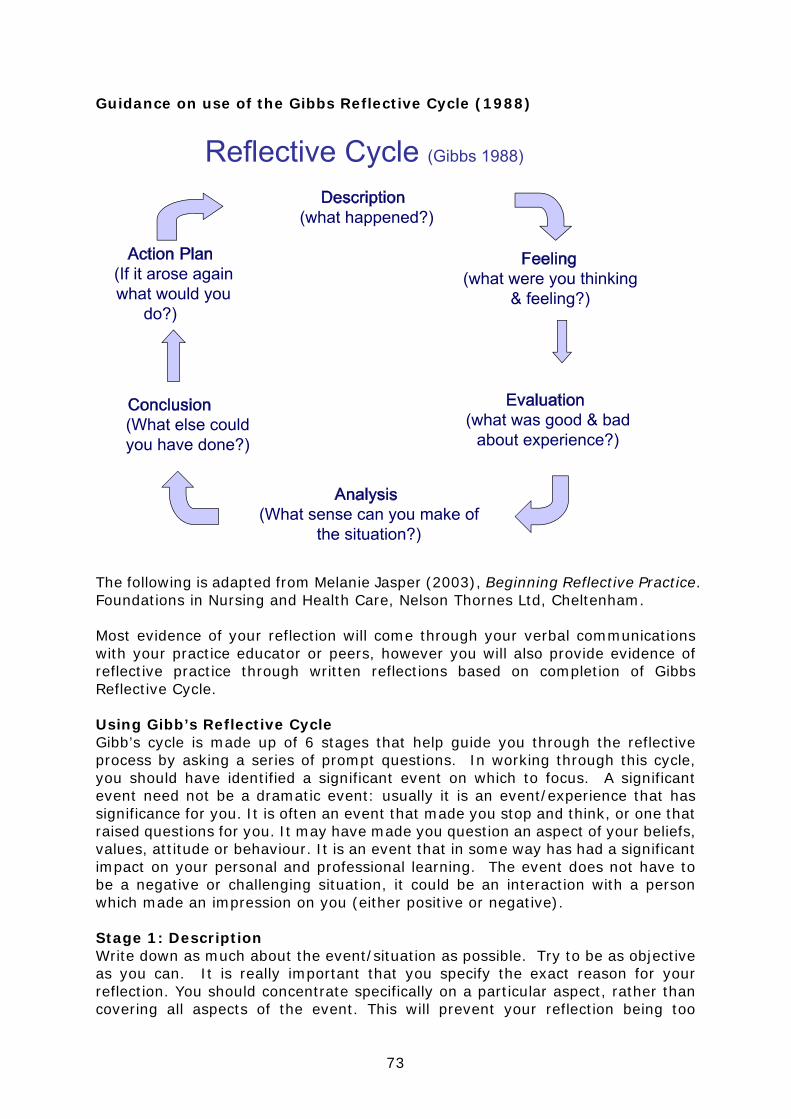
73
Guidance on use of the Gibbs Reflective Cycle (1988)
The following is adapted from Melanie Jasper (2003), Beginning Reflective Practice. Foundations in Nursing and Health Care, Nelson Thornes Ltd, Cheltenham. Most evidence of your reflection will come through your verbal communications with your practice educator or peers, however you will also provide evidence of reflective practice through written reflections based on completion of Gibbs Reflective Cycle. Using Gibb’s Reflective Cycle Gibb’s cycle is made up of 6 stages that help guide you through the reflective process by asking a series of prompt questions. In working through this cycle, you should have identified a significant event on which to focus. A significant event need not be a dramatic event: usually it is an event/experience that has significance for you. It is often an event that made you stop and think, or one that raised questions for you. It may have made you question an aspect of your beliefs, values, attitude or behaviour. It is an event that in some way has had a significant impact on your personal and professional learning. The event does not have to be a negative or challenging situation, it could be an interaction with a person which made an impression on you (either positive or negative). Stage 1: Description Write down as much about the event/situation as possible. Try to be as objective as you can. It is really important that you specify the exact reason for your reflection. You should concentrate specifically on a particular aspect, rather than covering all aspects of the event. This will prevent your reflection being too
74
descriptive, as you have a focus for your reflection. Some of the items you might want to consider are: Where were you? Who else was there? Why were you there? What were you doing? What were other people doing? What was the context of the event? What happened? What was your part in this? What parts did the other people play? What was the result? Stage 2: Feelings You should try to identify what you were feeling at the time of the event/situation. You may find this difficult to share with others. You may find the following questions useful: How were you feeling when the event started? What were you thinking at the time? What were you thinking about when it happened? How did it make you feel then? What did other people’s actions/words make you think? What did these make you feel? How did you feel about the outcome of the event? What do you think about it now? List the emotions that you have gone through from the start to the finish of the event Which of these is most significant or important to you? Stage 3: Evaluation Evaluation is a process where we measure something against a standard. We are trying to make a judgement about the event/situation so we can consider all its components. You may want to ask: What was good about the experience? What was not so good about the experience? Stage 4: Analysis Analysis is to ‘break things down into their component parts’ so that they can be explored separately. You need to ask yourself more detailed questions such as: What went well? What did I do well? What did others do well? What went wrong, or did not turn out the way I thought it should? In what ways did I contribute to this? In what ways did others contribute to this? Why might these things have happened? Stage 5: Conclusion
75
Different from the evaluation stage in that you have explored the event/situation from different angles and have more information on which to base your judgements/conclusions. You are likely to have insight into your own and others behaviour in relation to how they participated in the event. This can be difficult because you may realise that how you went about something was perhaps not the most competent way. You should remember, however, that the purpose of reflecting is to learn from your experience! Without the detailed analysis and honest exploration that occurs by working through these stages, it is likely that opportunities for learning will be missed. You may want to ask yourself: What could I have done differently as part of this stage? Stage 6: Action plan What would you do if you encountered this event/situation again? Would you act differently or would you act the same way again? This is an important stage as it demonstrates that you have learned from your experience. Try and make your action plan SMART where possible. For example, saying ‘I will be more confident next time’ is not SMART, however if it was phrased as ‘I will prepare by making notes/ researching the topic/practicing my presentation. I will ask, if appropriate, for one of the dietitians to give me feedback on a draft submission. By putting these goals into action I feel this should help me be more confident with presentations’, this is more specific and measurable. The next time a similar event occurs it will be the focus of another reflective cycle, perhaps more of a reflective ‘spiral’ as you will have brought your previous experience to the current one. See example of completed reflective cycle. Description: Reflect back on your conversation and describe this below. I am currently in week 4 of my C placement and have been base in both community and acute settings. Ellen* was one of the patients assigned to me during my weeks on a stroke rehab unit. She was an older inpatient (81y) undergoing rehabilitation following a stroke, which left her aphasic (she could not speak but could understand others) and unable to swallow. When my supervisor handed over her case, she was currently awaiting confirmation from all members of the multidisciplinary team (MDT) that she could be transferred to a nursing home. From a dietetic perspective, the family was requesting her PEG insertion to be removed prior to transfer. Ellen had started to be able to eat solids a few weeks previously and now was only requiring PEG to receive fluids and medication. I needed to be certain she was capable of meeting her nutritional and fluid requirements before giving go ahead for PEG removal. On my initial visit I introduced myself to Ellen and explained who I was and what my role was. I was reliant on nursing staff and written records to assess what her food and fluid intake was like as Ellen was aphasic. I spoke with speech and language therapists who said she was now ok to drink thickened fluids and take medications orally. I calculated her fluid and nutritional requirements and requested

76
a detailed food and fluid chart was kept for remainder of the week and for Ellen to continue to be weighed weekly. When I went to review Ellen at the end of the week, I did not recognise any of the nursing staff (staffing problems had led to shortage and lots of bank nursing staff). None of them were aware of the request for charts and this meant I had no evidence to show if Ellen was meeting her requirements. I spoke with the senior nurse and emphasised the importance of keeping the charts in allowing Ellen to go home - the nursing notes had shown her family were becoming impatient and could not understand the hold up. I reinstated the care plan and went back to visit early the next week. The completed charts, and stable weight, allowed me to document that Ellen was meeting her requirements for food and was managing her medications orally. The fluid charts however revealed while Ellen was managing to drink fluids without difficulty, she was not meeting her requirements. I discussed with nursing staff and they felt that if encouraged she could drink more and they would try offering more drinks to Ellen. I went back to visit on my last day and feedback from nursing staff and the fluid charts showed that Ellen was meeting her fluid requirements. A blood test I had also requested came through and showed that the patient was not dehydrated. I informed Ellen of the plan and wrote in the notes that from dietetic viewpoint, Ellen could have PEG removed. After each review of Ellen in the ward, I discussed my plans with my supervisor and she counter signed my notes (in nursing notes, dietetic notes and record card). She agreed with my dietetic care plans and was happy to see the progress of Ellen over the past two weeks as she had been under her care for several months. I need to reflect on my progress on managing this patient as it highlights a number of skills and competencies that I have demonstrated and want to make sense of. Feelings: Describe how you felt whilst undertaking this activity. I initially felt quite apprehensive about being given a patient who was aphasic as I had never spoken to someone with this condition before and I also worried I would struggle by myself on the ward in terms of the environment itself, knowing where all the notes were and talking to MDT members. However, when I was actually in the ward I felt at ease and confident. I became accustomed to the lay out of the ward and could locate the notes and know where to look for the relevant information. I felt a bit apprehensive in speaking to the nurses at the start as they seemed so busy but quickly became more confident as 1 had to do it often for my other patients. I felt like part of team when members of MDT and nurses would say hello to me on the wards and this made it easier to ask them questions about how Ellen was getting on. I was disappointed to find that the charts had not been filled in, as I had written in all the correct places for the plan to be put in place. However, I realised that this was just a challenge and I had to find a way around it. Speaking to the head nurse was scary as I didn’t want to appear bossy about the fluid/food charts as they were really short staffed that week and she was always rushing around. When they were correctly filled in next time I felt proud that my actions had paid off. My courage to push for the charts to be filled in had been successful as it would have been easy option to give up and just document that it was not possible to calculate fluid intake.
77
I felt like a had contributed to Ellen’s care and it felt good to be able to tell her on my last visit with her that her PEG was going to be able to come out. Although she couldn’t communicate back, it was good to be able to tell her this. While I had initially felt self conscious about speaking to her in front of the nurses and other ward patients (as she couldn’t reply) I quickly got used to it and realised that everyone was busy getting on with their own work and weren’t judging me. I was aware that I wanted to work ethically too and this was best achieved by speaking to Ellen even though she couldn’t respond I knew she could hear me. I also paid closer attention to any facial expressions and shifts in body language that would indicate how she was feeling and aimed to be aware of my own verbal and non-verbal body language – smile, lean forward when speaking, taking time to make sure I was understood, eye contact etc. I enjoyed feeding back my findings to my supervisor as it acted to build my confidence when she agreed with my care plans, but also widen my perspective when she gave her own suggestions and opinions. While I did feel under pressure to get the situation sorted as her family were not happy, I knew that it was an important decision that needed firm evidence to allow for PEG removal. As Ellen had been under my supervisor’s case for several months I was also anxious that I did not want to do anything she did not approve of. However, our discussions allowed me to see I was doing the right thing and I became more trusting of my judgment. I really cared for this patient and it was fulfilling to see her case was resolved and it was a good outcome. It was a rewarding experience and a great way to build my confidence for the duration of my C placement. Evaluation Describe what you felt was good and bad about the experience. I was able to collect all the relevant information necessary to formulate dietetic care plan for Ellen. This involved collecting information from her previous stay at a larger hospital immediately after her stroke, the notes from her stay at this hospital over the past few months, information from the portal (medications and blood results), weight records, information from my supervisor and verbal communication from the MDT. This was due to effective communication skills and my ability to collect relevant information. I was able to implement a strategy to gather the additional information I wanted (fluid and food intake) by successful documentation in the relevant places and verbal communication with the staff. While initially this was not taken on board, I was assertive and re-emphasised the plan and I got the information needed next time I reviewed. I was able to use clinical reasoning to assess the information collected and I realised that I did not have the necessary information required to give go ahead for PEG removal and I assured that I did before giving this advice. I effectively communicated with MDT members to gather, relay and request information. I managed my time well, organising my time in advance to allow for several review visits and time to discuss with my supervisor my plans in addition to my other patients. I acted professionally and with correct conduct when speaking to the MDT team and also in a non-discriminatory way towards an older and aphasic patient. The case

78
was resolved and the patient and her family were satisfied with the care they had received. On the negative side I still sought reassurance from my supervisor that my care plan was correct but was confident to decide upon one before discussing it with her. This was the first time I felt confident to do this with a patient of this type, especially with some of the barriers I needed to contend with, e.g. charts not being completed, busy staff, etc. Analysis Consider what sense you make of the situation. I managed my time well due to good organisational and prioritising skills. This allowed Ellen to receive the care she required and for me to review her case several times over the 2 weeks which was required to see her care plan through to the outcome of giving approval for PEG removal. My assertiveness allowed for fluid charts to be correctly filled in- I did not take easy option of sitting back and accepting that the nurses were too busy to document it. I was always polite and friendly to the nurses, showing an understanding that they were really busy and filling in the sheets was just another of many tasks. Through discussion with the head nurse about the necessity of the completed charts to allow for Ellen to go home, she could emphasise to the ward nurses, and bank staff, the importance of completing the sheets. I always showed my appreciation of the effort they put in and I feel this resulted in the nurses taking the time to fill in the charts, encouraging Ellen to drink throughout the day and informing me of Ellen’s progress. This experience has made me realise just how important it is to build good relations with other nursing and AHP staff to ultimately benefit patient care. I also realise that no matter how busy staff are, by taking a few minutes to explain the importance of the charts and how this affected Ellen’s care can galvanise staff to action. I will always aim to give a rationale for why I need certain information, when appropriate. My supervisor was impressed with the progress as she informed me that she and other dietitians had struggled to get the nursing staff to complete charts when requested. My ability to communicate effectively with other members of the MDT allowed everyone to be aware of the latest proceedings in the case. This was due to my ability to relay information in a concise way and document it correctly in the notes so that these busy members of staff could get a quick overview of latest update. It was also due to my time spent in earlier weeks shadowing members of the MDT, which allowed me to fully appreciate their responsibilities as interprofessional education has been found to improve professional practice and patient care. I believe our effective MDT work contributed to Ellen’s successful treatment as the benefits of a MDT approach to patient care are well documented. My ability to reflect upon my practice allowed me to see that just writing in the notes was not going to be sufficient and I would have to develop a new strategy (discussion with nurses) to ensure charts were kept. My clinical judgment skills allowed me to consider all the relevant factors before deciding upon any changes to make to Ellen’s care plan. For example, while the fluid charts were being kept on my third visit and the nurses said she could meet her requirements if she was encouraged, I did not think this was sufficient for give go ahead for such a big decision of PEG being removed. While it meant the case would be further delayed, I requested charts to be continued and fluids to be pushed. It was only on my last
79
visit that I felt there was sufficient evidence to justify my decision. I feel this is a result of my experience over the last 12 weeks of B placement and 4 weeks of C, and my increasing confidence in my ability to make such judgements. However, I still doubted my decisions, seeking approval from my supervisor. I still feel my clinical reasoning skills have improved though as I would decide upon her care plan independently, I just sought reassurance that it was correct. I remained aware of my limitations in knowledge base and skills and sought help from my supervisor when required. I need to realise that I am in effect only week 4 of my C training and still have much in the way of practicing my skills before I am considered at the stage of being “fit to practice”. Knowing this will encourage me to learn from my mistakes and also to be confident in my decision making abilities with the proviso that I may still need support from my supervising dietitians (and this is fine!) Conclusion What are your conclusions of the activity? Over the past 12 weeks of B and 4 weeks of C I have developed my skills and knowledge through practice based experience and I feel my care for Ellen, and others during my placements, illustrates my attainment of the LOs. I am now capable of independently collecting the necessary information; efficiently and accurately recording notes; communicating with patients, supervisors and MDT members; acting with proper conduct and professionalism in the hospital setting; organising and managing my time effectively; reflecting upon my practice; applying clinical reasoning based on each patient’s individual presentation and reviewing and evaluating patients care. It has surprised me that I can use skills developed with other patients/clients and bring them to the current experience, in this case a patient with aphasia. I have come to appreciate that through reflection and supervisor support, and as my experiences develop, I can use my clinical reasoning in new situations and do not have to look for “black and white” answers, for example from university/books etc but instead can think more critically to come up with the right solutions for each individual patient/client. I effectively overcame factors out with my control, e.g. nursing staff shortages- to allow for Ellen’s case to be resolved. While I still sought reassurance from my supervisor, confidence to be truly independent in my practice will develop with further experience and currently I should be conscious of my limitations and not be afraid to ask for help if I am unsure. I now realise that this level of practice could only be achieved with the underpinning practise I got from the previous weeks on placement and I would not have handled this situation earlier on – this reflection helped me see the progress I have made which I may not have done had I not taken the time to do this.

80
Action Plan: If you were undertaking this task again how would you change your approach to it? Link to SMART outcomes where possible. I will continue to practise at this level of practice with different patients, in different settings for the duration of my placement. I will continue to reflect upon each experience to recognise areas where I can improve-of which there always is! I will make a conscious effort to reflect upon my confidence levels and through further experience I believe I will achieve a level of confidence in which I do not seek reassurance. To achieve this I will ensure I have debrief with my supervising dietitian which will benefit me in two ways 1. I will be reassured that I did the best for the patient and didn’t miss anything. 2. I will be able to consolidate my learning by reflecting on the experiences I have and can discuss possible alternatives (maybe more than one solution that didn’t occur at the time). I also appreciate that at my stage, I should remain aware of my limitations and know when I need to seek the advice of supervisors. This should occur less often as I progress through placement C. However I also recognise that dietitians of all levels always benefit from seeking input from other dietitians who may have experience with a similar case or can view the situation from another perspective. This is something I have seen other dietitians do and it gives me the confidence to know that it is part of professional learning to share practice so this is something I have taken on board and will continue to do in future. I also want to improve my communication skills by researching on how to better communication with people who have difficulties, such as aphasia, as I want to ensure I give the same level of care as those who do not have any difficulties.
*name has been changed

81
DIET-COMMS Formative Communication Assessment Tool DIET-COMMS is a validated tool, designed to support the assessment of communication skills for behaviour change within dietetic one-to-one consultations. This tool has been incorporated into this placement portfolio as a useful aid in identifying specific areas for development of a dietetic student’s communication with service users and carers. DIET-COMMS is supported by an online training package which can be used by students and Practice Educators (or as a CPD activity for qualified staff either by peer assessment or self-assessment). This comprehensive and extensively referenced training package includes many freely downloadable resources including guidance sheets on how to setup peer observation programmes, assessing students, self-assessment and how to give constructive feedback. There are feedback sheets on each of the items on the DIET-COMMS tool which can help direct skill development. Included are videos of consultations in an outpatient setting (with inpatient and home visit settings coming). There are three versions of the same consultation; bad, reasonable and good. You can see the views of the Dietitian, the actor playing the patient and a real service user on the impact of communication skills in the consultations. You can download the DIET-COMMS tool and practise assessing the videos and then look at the expert view to improve your understanding. The online training package is available at the University of Nottingham: http://www.nottingham.ac.uk/toolkits/play_13244. The tool has 20 items that should be scored on a 3-point scoring system (0=not done or not achieved, 1=partly achieved or attempted, 2=fully achieved). There are descriptors available that explain what each of the items mean. To score just tick the box that relates best to the score you want to give (0, 1 or 2). At the bottom, there is space for a ‘global assessment’ which is to indicate the overall feel of whether the consultation is a clear pass, is borderline, or would fail. Remember there is not an absolute pass score as each consultation is different and some items may be considered more important in some situations than others. Similarly there are some items that will always be highly relevant e.g. scoring 0 for ‘Maintains non-judgmental attitude’ would imply that the person was judgmental and therefore it would not be a competent consultation. Similarly scoring 0 for ‘establishes rapport’ would suggest no rapport was established at all which again would not be competent. Please do spend some time familiarising yourself and DIET-COMMS and the package prior to using it with the student. For further information, please access the package or contact Dr Kirsten Whitehead at [email protected] Reference Whitehead K.A., Langley-Evans S.C., Tischler V.A. & Swift J.A. (2014) Assessing communication skills in dietetic consultations: the development of the reliable and valid DIET-COMMS tool. J Hum Nutr Diet. doi:10.1111/jhn.12136

82
Assessment of Communication skills in dietetic client consultations Year of Study 1 2 3 4 Post graduate (circle as appropriate) Dietitian/student dietitian name/number ITEM No. ITEM
SCORE 0=not done or not achieved 1=partly achieved or attempted 2=fully achieved 0 1 2
1 Greeting and introductions 2 Establishes what led up to & clarifies reason for
consultation.
3. Outlines what to expect from the visit.
4 Listening to and demonstrating understanding of the client’s story
5 Establishes rapport. 6 Checks understanding of medical condition. 7 Offers information on how food relates to the condition 8 Completes (clinical, behavioural and dietary)
assessment.
9 Works in partnership with client to identify possible dietary changes. Explores possible difficulties.
10 Checks understanding and agreement on client determined goals. Develops a plan prioritising key goals.
11 Offers written information to reinforce verbal. 12 Agrees next steps with the client. 13 Interview structured in a logical sequence. 14 Interview completed in a timely fashion. 15 Uses active listening skills (including appropriate
questions) to check joint understanding throughout interview.
16 Maintains non judgemental attitude. 17 Acknowledges clients views and feelings. 18 Uses appropriate non verbal communication
throughout.
19 Uses appropriate language throughout. 20 Summarises appropriately throughout the consultation. Total
Global Assessment Clear pass Borderline Fail � � � Date Used with kind permission of KA Whitehead.

83
Student Progression AlgorithmThis process should be followed on a weekly basis, with consideration of the placement ‘Know, Can, Do’ model.
Is the student progression as expected in accordance with the ‘Know, Can, Do’ model?
Yes. No.
Has progress been shown?
Complete end of week review and action form in conjunction with
the student.
Yes.Now progressing as expected.
Complete end of week review and action form in conjunction with
the student. Pass copy directly to next facilitator
and to Practice Placement Lead. Identify specific action points and
time period for resolution.
Little or no progress shown. Some progress shown but not yet progressing as expected
for stage of placement.
Complete end of week review and action form in conjunction with
the student. Pass copy directly to next facilitator
and to Practice Placement Lead. Practice Placement Lead to contact
University tutor for support/ advice/ guidance.
Identify specific action points and time period for resolution
Has progress been shown?
Little or no progress shown or persistent lack of significant progress.Follow FtP Algorithm
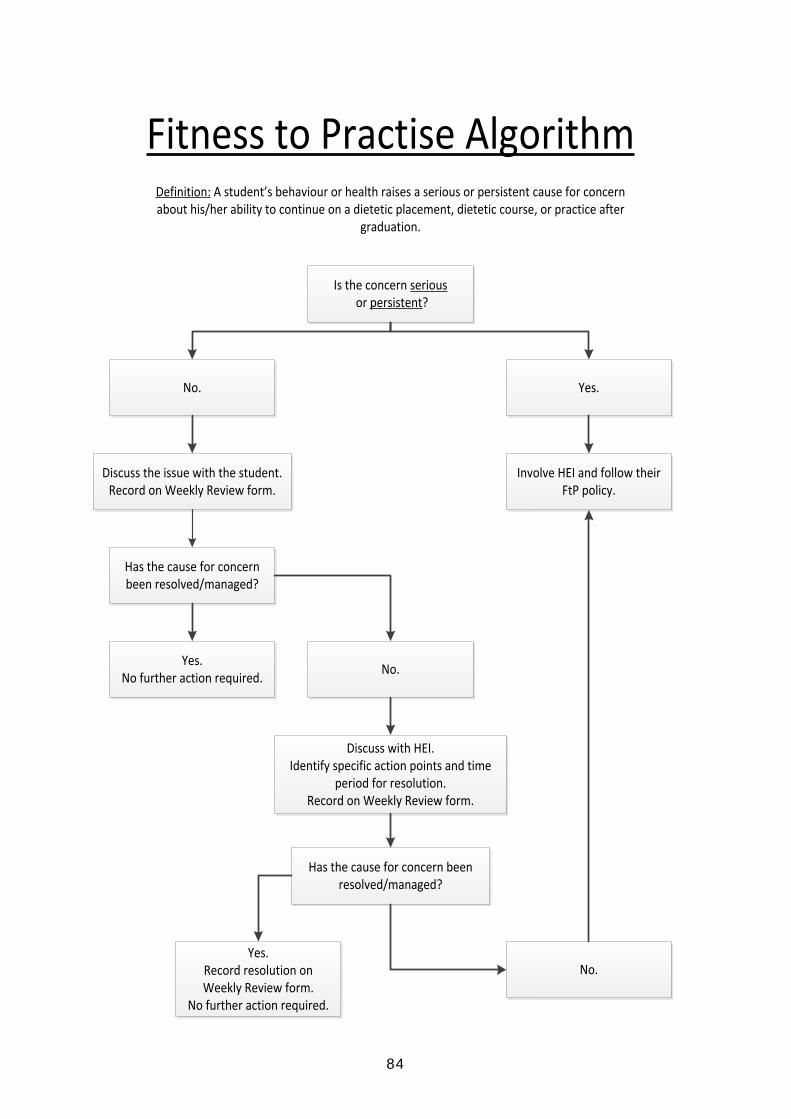
84
Fitness to Practise AlgorithmDefinition: A student’s behaviour or health raises a serious or persistent cause for concern about his/her ability to continue on a dietetic placement, dietetic course, or practice after
graduation.
Is the concern serious or persistent?
No. Yes.
Involve HEI and follow their FtP policy.
Discuss the issue with the student.Record on Weekly Review form.
Has the cause for concern been resolved/managed?
Yes.No further action required. No.
Discuss with HEI. Identify specific action points and time
period for resolution. Record on Weekly Review form.
Has the cause for concern beenresolved/managed?
No.Yes.
Record resolution on Weekly Review form.
No further action required.

85
Raising a Concern Algorithm
Seeking AdviceIf you are unsure about whether, or how, to raise a concern at any stage, you should seek advice from your Programme Leader or Personal Academic Tutor.*Independent confidential advice is also available from the British Dietetic Association (for student members) or Public Concerns at Work (PCaW).
I have concerns about the safety or well-being of people in my care or in the environment in which I work.
Is there an immediate risk of harm?
Report your concerns, without delay, to the appropriate person or
Authority.
Yes. No.
If you are unable to do this for any reason
ORYour concern is not addressed
adequately and/ or there is an immediate risk to others.
Stage 1Raise your concern:
1. internally, with your Practice Placement Supervisor
2. with your Programme Leader.
Stage 2Escalate your concern:
1. internally, to a higher level (Senior Practitioner or Line Manager)
2. contact your Programme Leader.
Key Points1. Take immediate or prompt action2. Protect confidentiality3. Refer to whistleblowing policies4. Keep an accurate record of your concerns and actions taken.
Whilst we do not anticipate any problems, should such a situation arise it is important that you understand the steps that you can take to find a resolution.
Many problems occur due to misunderstandings and faulty communications, which can be easily solved if approached sensitively. Problems raised at the end of the placement generally cannot be satisfactorily resolved and it is therefore essential that you highlight any concerns as they arise. If, however, you do not feel that your concerns have been adequately resolved, you should contact your Programme Leader or Personal Academic Tutor to discuss further.
Equally, if you have any concerns about the safety or well-being of the people in your care, or the care environment you are working in, then these should be raised using the algorithm below. This may include concerns about other Healthcare Professionals, or other students.