picking the low hanging fruit and reaching beyond
TRANSCRIPT

Kirthana R. Beaulac, PharmD BCPS
Antimicrobial Stewardship In Acute CarePicking the Low Hanging Fruit and Reaching Beyond

Objectives
• Review the principals and objectives of an antimicrobial stewardship program
• Outline the regulatory requirements surrounding Antimicrobial Stewardship in Hospitals
• Identify the barriers to implementing a successful stewardship program in academic and community hospitals
• Integrate evidence-based practices and resources to improve antimicrobial usage

The bugs are becoming harder to treat…
3

4
…and the antibiotic pipeline is drying up
4Ventola CL. PT. 2015; 40(4):277-283.

ANTIMICROBIAL STEWARDSHIP
• IDSA defines Antimicrobial Stewardship as “an activity that includes appropriate selection, dosing, route, and duration of antimicrobial therapy”
• Goals of Stewardship• Attenuate or reverse antimicrobial resistance• Prevent antimicrobial-related toxicity• Reduce the costs of inappropriate antimicrobials• Decrease health care associated infections
Dellit T, et al. CID. 2007; 44: 159-177.

6
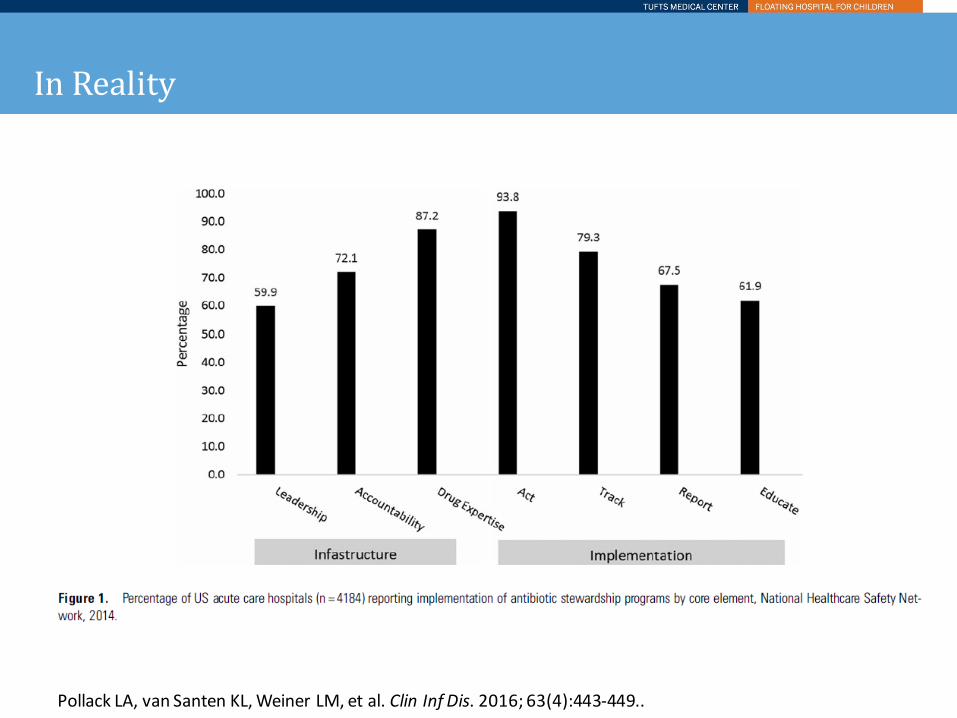
In Reality
Pollack LA, van Santen KL, Weiner LM, et al. Clin Inf Dis. 2016; 63(4):443-449..

8
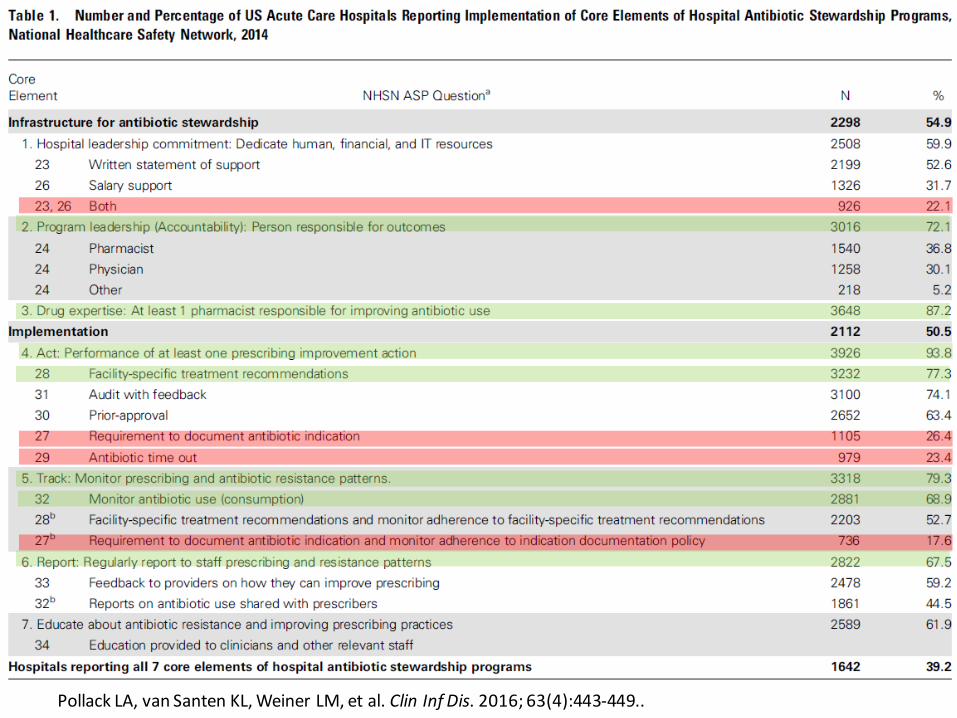
Pollack LA, van Santen KL, Weiner LM, et al. Clin Inf Dis. 2016; 63(4):443-449..

9
Massachusetts Results
0%10%20%30%40%50%60%70%80%90%
100%
201420152016
10
Pollack LA, van Santen KL, Weiner LM, et al. Clin Inf Dis. 2016; 63(4):443-449..

The Easy Stuff
• IV to PO• Implement protocols
and guidelines• Formulary restriction• PK dose optimization

Parenteral To Oral Conversion
• Several antibiotics have good oral bioavailability• Fluoroquinolones• Linezolid• Metronidazole• Clindamycin• SMX/TMP• Fluconazole
• Associated with Decreased:• Length of stay• Cost of care• Risk for line-related
infections• Additional Benefits
• Fluid / sodium restriction• Enterohepatic cycling• Patient Satisfaction
Jones M, et al. Infect Control Hosp Epidemiol. 2012; 33(4): 362-367.

Guidelines and Protocols

Make the Right Choice the Easy Choice

Impact of Protocol
Lancaster JW, et al. Pharmacotherapy. 2008;28(7):852–862.

Restricting Antimicrobials
• Highly effective, but need specialized personnel to be effective• Authorizations done by chief resident compared to no
authorization needed• No difference in antibiotic use
• Authorizations done by ID attending and ID pharmacist compared to ID fellow• Improved antimicrobial appropriateness• Increased clinical cure• Trend towards improved economic outcome
DeVito JM, et al. Arch Intern Med. 1985; 145:1053–6.Gross R, et al. Clin Infect Dis. 2001; 33:289–95.

Dose Optimization
• Patient Characteristics• Age, renal function, weight
• Causative Organism• Site of Infection• Pharmacokinetics
• Extended or continuous infusion of β lactams• High-dose once daily aminoglycoside
Nicasio AM, et al. Journal of Critical Care. 2010; 25: 69-77.Falagas ME, et al. Clin Infect Dis. 2013 Jan;56(2):272-82

Higher Level Interventions
• Bolstering non-specialists
• Complex antibiograms• Antibiotic Time Out• Application of rapid
diagnostics
• Culture change

Non-ID Trained Pharmacists
• Non-specialized clinicians can be effective in stewardship activities with guidance from ID-trained pharmacists or ID Physicians
DiazGranados CA. AJHP. 2011; 68(18): 1691-1692.Laible BR et al. Journal of Pharmacy Practice. 2010; 23: 531-534.

Vancomycin Per Pharmacy
Development of Kidney Dysfunction
Recovery of KidneyFunction
Use of Concomitant Nephrotoxins
Vanco PerPharm (VPP)
48 / 640 (7.5%)
17 / 48 (35.4%)
40 / 48 (83%)
First 4 months without VPP
72 / 684 (10.5%)
p=0.05
39 / 72 (54.12%)
72 / 72 (100%)
1 year after VPP
61 / 767 (7.6%) p>0.05
35 / 61 (57.4%)
55 / 61 (61%)

Syndromic Antibiogram
Wick J, Beaulac KR, Doron S. Inf Ctrl Hosp Epi. 2016; 37)9):1101-1104.

Combination Antibiogram
Wick J, Beaulac KR, Doron S. Inf Ctrl Hosp Epi. 2016; 37)9):1101-1104.

VAP Antibiogram
Randhawa V, Sarwar S, Walker S, et al. Critical Care. 2014; 18: R112.

Age-Stratified Antibiogram
Swami SK, Banerjee R. SpringerPlus. 2013; 2:63.

Antibiotic Time-Out
• Hard Stop vs. Soft Stop• Electronic vs. Manual • Passive Alert vs.
Actionable Item• Resources for next steps

2626

27
Graber CJ, Jones MM, Glassman PA, et al. Hosp Pharm. 2015; 50(11):1011-1024.

Rapid Molecular Diagnostics: Most Common Applications
• Blood• Multiplex PCR (polymerase chain reaction)• MALDI-TOF (matrix assisted laser desorption/ionization- time of flight)• PNA-FISH (peptide nucleic acid fluorescence in situ hybridization)
• Respiratory Viruses• RADT (rapid antigen detection test)• NAAT (nucleic acid amplification test)• PCR
• Stool• Immunoassay and PCR for C. diff• PCRs for various common stool bacteria and viruses
28

Molecular Rapid Diagnostics
29
Timbrook TT, Morton JB, McConeghy KW, et al. Clin Inf Dis. 2017; 64(1):15-23.

30
Application of Multiplex PCR for Bacteremia at Tufts
Page Clinician
• Micro lab alerts clinician as Critical Value
Written Guidance
in EMR
• Pathogen-directed treatment guidance designed by Tufts Antimicrobial Management Team
Follow-up from
AMT
• Antimicrobial Management Team checks to ensure appropriate antibiotics are initiated within 1 hr
Positive BiofireResult
• Incorporates previous year’s antibiogram, hospital formulary and policies, and DPH reporting requirements

31

32

33
Time to Adequate Therapy
Composite Outcome:Hours to adequate
therapy (including d/c abxfor contaminants)
median (IQR)(N= 152)
Pre- Implementation
(N= 82)
23.95 (6.29-58.50)
Post- Implementation
(N= 70)
14.82 (4.07-44.79)

Culture change
• Solicit feedback and give feedback• Provide a helpful (“teaching”) service• Use concepts of behavior change theory• Physician Reluctance

35
Beerlage-de Jong N, Wentzel J, Hendrix R, et al. Am J Inf Ctrl. 2017; 45:365-71.
Evaluation of Programmatic Changes to the ASP Program with House Officer Feedback• House officer survey on Tufts Medical Center ASP• 2008 Survey• Programmatic interventiono Enhanced training on ASP procedures at orientationo Changes to the antimicrobial order formo “ASP question of the week”
• 2010 Survey
Hong SY, Epstein LH, Lawrence K, Davidson L, Taur Y, Nadkarni L, Doron S. Journal of Evaluation in Clinical Practice 2012:1365-2753.

Antimicrobial Stewardship Program (ASP) Impact on Patient Care 2008 and 2010
Differences between 2008 and 2010
Hong SY, Epstein LH, Lawrence K, Davidson L, Taur Y, Nadkarni L, Doron S. Journal of Evaluation in Clinical Practice 2012:1365-2753.

Small Nudges
38
Hallsworth M, Chadburn T, Salis A, et al. Lancet. 2016; 387; 1743-1752.

3939

Dealing with Holdout Prescribers
• Cater to their wants and needs• Preferred communication methods
• Tug at their heart strings• Make it personal• Underscore their role in protecting the greater good
• Call in reinforcement if needed• But make sure you have leadership on your side first!
• Steward around them• Micro/Laboratory Stewardship• Nursing support
40
Goldstein EJC, Goff D, Reeve W, et al. Clin Inf Dis. 2016; 63(4):532-538.Olans RN, Olans RD, DeMaria A. Clin Inf Dis. 2016; 62(1):84-89.

Let me pull out my violin…
• The CDC estimates 37,000 deaths annually as a consequence of antibiotic overuse (antibiotic resistant infections and C. difficile)• 32,000 deaths annually from motor vehicle accidents• 15,000 deaths annually from homicide• 33,000-38,000 deaths annually from opiate overdose
• How many people have that have died from one of those 3 things at this institution?
• How many people do you think have died as a consequence of antibiotic overuse at this institution?• What percent were your patients?
41

A Moment For Reflection
• Based on the strategies discussed here today, are there any feasible strategies that you think you can implement?
• What are the barriers that you face that have not been addressed?
42

We’re All In This Together, But It Starts With You
43
Antibiotic Resistance