physician reentry into the workforce holly j. mulvey, ma ethan alexander jewett, ma co-directors...
TRANSCRIPT

Physician Reentry into the Workforce
Holly J. Mulvey, MAEthan Alexander Jewett, MACo-Directors
Physician Reentry into the Workforce Project

Definition
Physician reentry into the workforce can be defined as
returning to professional activity/clinical practice for
which one has been trained, certified or licensed after
an extended time period.

Who are the stakeholders?
Federal/state governments Regulatory groups (state
licensing boards) Federal agencies Hospitals (including The
Joint Commission) Medical/specialty
societies Specialty boards
Organizations invested in physician workforce planning
Groups with an agenda that focuses on women in medicine
Individual physicians

Some reasons for leaving the workforce
Health Substance abuse Retirement Burnout Loss of licensure Family needs (children, elderly parents) Career change (eg, administrative position, research)

Some reasons for reentering the workforce
Financial reasons Responding to a need
in the community (ie, natural disaster)
To pursue a new challenge or area of medicine
Miss colleagues and/or practice environment
Miss caring for patients Too much free time on
my hands

Why is this issue important?
Many physicians leave clinical medicine for a period of time
Federal investment in GME – “Medicine is a public good.”
Unmet patient need – underserved areas and anticipated public health crisis
A mechanism to bring more flexibility into the system (eg, the attractiveness of medicine as a career)

Some questions to consider
Is the structure of the health care system too rigid to accommodate diverse practice/career/personal needs?
Do MDs need to “leave” because the system won’t give?
Will we face an unstable MD workforce?

AAP participation in the AAMCSurvey of Physicians Over 50
Collaboration of AAMC, AAP, and 8 medical associations
AAP used existing Periodic Survey of Fellows survey instrument
1158/1600 surveyed (72% response rate) Women=26%; Men=74%

Work/practice opportunities
98
188
80
n=366
(21.9%)(26.8%)
(51.4%)
No Change
UncertainLaterRetirement
If flexible work hours or part-time option had been available at the time of your retirement, how would you have changed your practice?

Reduced hours/part-time
219
167Yes
No
n=386
(43.3%)
(56.7%)
Have you worked in a reduced-hour or part-time position during your medical career?
Mean=6.1 years
If yes, did you take the time to care for children or other family members?
678
428
0
200
400
600
800
1000
1200
1
Yes
No
n=1106
(38.7%)
(61.3%)
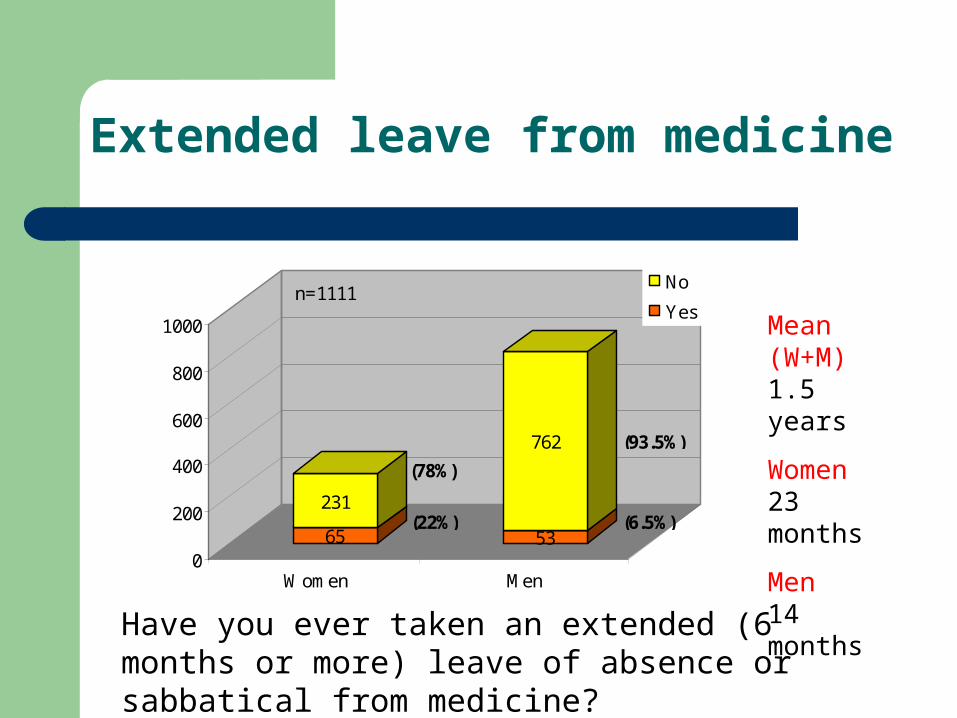
65
231
53
762
0
200
400
600
800
1000
Women Men
No
Yesn=1111
(78%)
(93.5%)
(22%) (6.5%)
Have you ever taken an extended (6 months or more) leave of absence or sabbatical from medicine?
Mean (W+M)1.5 years
Women23 months
Men14 months
Extended leave from medicine

Reasons for extended leave
6051
No
Yes
(45.9%)
(54.1%)
n=111
Did you take the time to care for children or other family members?
Women = 71%Men = 14%
(for Pediatrics)

Retraining before reentry
85
22
Yes
No(20.6%)
(79.4%)
n=107
Did you have any retraining before reentering medicine?
Women = 23%Men = 18%
(for Pediatrics)

Reasons for reentry
23
23
23
43
47
63
20
0 10 20 30 40 50 60 70
Other
Financial reasons
Too much free time
Miss colleagues/practice
Community need
Miss caring for patients
Want a new challenge n=113(17.7%)
(55.8%)(41.6%)
(38.1%)
(20%)
(20%)
(20%)
Why have you considered reentering medicine?

Physician Reentry into the Workforce Project

What are our assumptions?
Physicians returning to the workforce will face questions about their competence to resume clinical practice.
The educational needs of physicians who wish to return to clinical practice are extremely diverse.
With the growing proportion of women in pediatrics and other specialties, there will likely be an increase in the number of pediatricians taking an extended leave during their career or returning to medicine after retiring.
Physicians who choose to leave the workforce for a period of time risk losing their state licensure, their Board certification and hospital privileges.

Assessment and Evaluation
This workgroup will need to identify appropriate methods
for evaluating an individual physician’s competence and
need for retraining. Once a physician has undergone
retraining, a valid assessment will need to be in place to
assure the public that the physician is skilled and
competent to resume the practice of medicine.
Education
This workgroup will be charged with determining how to
respond to each physician’s educational needs through
Web-based and live CME, shadowing, preceptorships,
mini-residencies, and formal reentry programs. This
group should also identify strategies to defray the costs of
such training opportunities to make them affordable to the
individual physician.

Licensure, Maintenance of Certification, and Credentialing
One of the challenges of this workgroup will be to
identify strategies to help physicians maintain their
professional standing while they are absent from the
workforce. It will also need to propose a process for
physicians to regain their professional credentials if
they lose them and wish to return to active clinical
practice.

Workforce
This workgroup will need to determine how the workforce
is likely to be affected, and how to mobilize physicians
into the workforce once they indicate a wish to return to
practice. Additionally, the group should consider how to
marshal workforce resources in innovative ways to
respond to public health emergencies and emerging
models of health care delivery.

Works-in-progress: Workforce survey
Random sample of 5000 physicians under 65 listed as inactive in the AMA Masterfile.
3 mailings, 1/4/08, 2/1/08, 3/11/08 1,515 valid surveys, 584 bad addresses 2,868 nonrespondents 34.6% response rate, as of 3/28/08 Data presented at June 2008 AMA-HOD
Annual Meeting (Women Physicians Congress)

Reentry survey topics
Licensure and maintenance of board certification
Liability insurance Financial need Family responsibilities Professional satisfaction Work hours and
professional responsibilities Part-time practice Retraining modalities
What do we hope to learn?
Reasons for physician exit and reentry
Incentives to encourage inactive physicians to return to medicine
Barriers to inactive physicians returning to medicine
Demographics of inactive physicians
Specialties most affected by physician exit and/or reentry
Retraining/educational needs of reentering physicians
Availability of opportunities and portals to reenter medicine

Works-in-Progress:Reentry Web page redesign
Redesign in March 2008 to mark transition from planning to implementation
Expansion of resources related to the work of the Project and its workgroups (internal)
Addition of resources for physicians seeking to reenter the workforce (external)
Showcase research initiatives


Other reentry products in development
Journal article on reentry data on pediatricians from joint AAP-AAMC Survey of Physicians over 50
Proposed joint AMA-AAP conference in fall 2008 on physician reentry issues
Abstracts and manuscript on reentry survey data planned for 2009

Visit us at www.aap.org/workforce
Contact the Division of Workforce &
Medical Education Policy
Holly J. Mulvey, MA
Director
Division of Workforce and Medical Education Policy
American Academy of Pediatrics
141 Northwest Point Blvd.
Elk Grove Village, IL 60007
847.434.7915
847.434.8000 (fax)
Ethan Alexander Jewett, MA
Senior Health Policy Analyst
Division of Workforce and Medical Education Policy
American Academy of Pediatrics
141 Northwest Point Blvd.
Elk Grove Village, IL 60007
847.434.7914
847.434.8000 (fax)