(pharmacology) antipsychotic inggris yanti
TRANSCRIPT

•Antidepressant
•Antipsychotics (neuroleptics)
•Mood stabilizers.
•Drugs for anxiety and sleep disorders.
Following drug groups are considered

ANTIDEPRESSANT AGENTS
CHEMISTRY
A variety of different chemical
structures have been found to
have antidepressant activity.
BASIC PHARMACOLOGY OF
ANTIDEPRESSANTS
A. Tricyclics
Imipromine and amitriptyline
are prototypical drugs of the
class.
B. Heterocyclics, second
generation drugs
Amoxapine and maprotiline
resemble the structure of the
tricyclic agents, while trazodone
and bupropion are distinctive.
Venlafaxine is a newe.
C. Selective serotonin reuptake
inhibitors (SSRI)
The antimuscarinic,
antihistaminic, and alpha
adreneaceptor-blocking
actions of tricyclic
antidepressant contribute only
to the toxicity of these agents.
Fluoxetine, antidepressant
with minimal autonomic
toxicity, a highly selective
serotonin reuptake inhibitor.
Three selective serotonin
reuptake inhibitor : (1)
paroxetine (2) sertraline (3)
fluvaxamine.
D. Monoamine oxidase (MAO) inhibitors
MAO inhibitors may be classified as hydrazides, exemplified by the C-N-N moiety, as in the case of phenelzine and isocarboxazid; or nonhydrozides.
Tranycypromine a weak inhibitor of MAO.
Tranycypromine retains some of the sympthomimetic characteristic of the amphetamines.
Older MAO inhibitors nonselective inhibitors of both MAO-A and MAO-B.
Moclobemide is a new, short-acting, selective MAO-A inhibitor.
E. Sympthomimetic stimulants
Dextroamphetamine, other
amphetamines, and
amphetamine surrogates such
as methylphenidate
occasionally used ad
antidepressants.
PHARMACOKINETICS
A. Tricyclics
Most tricylics incompletely
absorbed and undergo
signigicant first-pass
metabolism.
High protein binding and relatively high lipid solubility volumes of distribution very large.
Tricylics metabolized by two major routes : transformation of the tricylics nucleus and alteration of the aliphatic side chain.
B. Heterocyclics
The pharmacokinetics of these drugs and of the tricyclics similar variable bioavailability, high protein binding, variable and large volumes of distribution, active metabolites.
Trazodone and venlafaxine shortest plasma half-lives.
C. Selective serotonin reuptake inhibitors (SSRIs)
Fluoxetine well absorbed, and peak plasma concentrations within 4-8 hours.
Its demethylated active metabolite, norfluoxetine half-life of 7-9 days at steady state; a slightly shorter half-life.
Fluoxetine inhibits various drug-metabolizing enzymes a number of significant drug-drug interactions with other antidepressants and with other drugs as well.
Sertraline and paroxetine pharmacokinetic parameters similar to those of tricyclics.
D. MAO inhibitors
MAO inhibitors readily absorbed from the gastrointestinal tract.
Hydrazide inhibitors (phenelzine and isocarboxazid) are acetylated in the liver and manifest differences in elimination depending on the acetylation phenotype of the individual.
The effect persist for from 7 days (tranycypromine) to 2 or 3 weeks (phenelzine, isocarbonazid) after discontinuance of the drug.
Moclobemide is rapidly absorbed and excreted, with over 90% of the drug appearing a metabolites in the urine within 12 hours.
MECHANISM OF ACTION
The monoamine hypothesis
propopse in depression
deficiency of the
neurotransmitters
nonadrenaline and serotonin in
the brain can be altered by
antidepressants.
Drugs affects depression modify amine storage, release, or uptake concentration of amines in nerve endings and/or at postsynaptic receptors is enhanced.
Specific serotonin reuptake inhibitors preventing serotonin reuptake and have more limited effects on nonadrenaline reuptake.
Tricylclic antidepressants
inhibit noradrenaline
reuptake, but effects on
serotonin reuptake vary
widely; desipramine and
protriptyline minimal
potential for raising,
serotonin concentration.
MAO inhibitors block a major
degradative pathway for the
amine neurotransmitters
permits more amines to
accumulate in presynaptic
and more to be released.
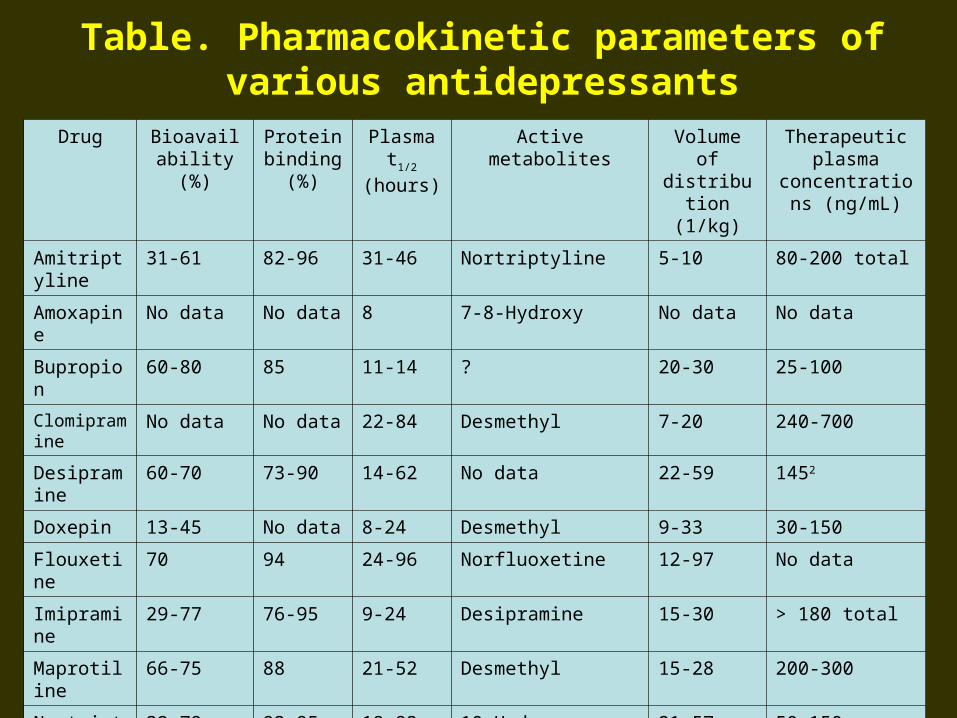
Table. Pharmacokinetic parameters of various antidepressants
Drug Bioavailability (%)
Protein binding (%)
Plasma t1/2 (hours)
Active metabolites Volume of distribution
(1/kg)
Therapeutic plasma concentrations
(ng/mL)
Amitriptyline 31-61 82-96 31-46 Nortriptyline 5-10 80-200 total
Amoxapine No data No data 8 7-8-Hydroxy No data No data
Bupropion 60-80 85 11-14 ? 20-30 25-100
Clomipramine No data No data 22-84 Desmethyl 7-20 240-700
Desipramine 60-70 73-90 14-62 No data 22-59 1452
Doxepin 13-45 No data 8-24 Desmethyl 9-33 30-150
Flouxetine 70 94 24-96 Norfluoxetine 12-97 No data
Imipramine 29-77 76-95 9-24 Desipramine 15-30 > 180 total
Maprotiline 66-75 88 21-52 Desmethyl 15-28 200-300
Nortriptyline 32-79 93-95 18-93 10-Hydroxy 21-57 50-150
Paroxeline 50 95 24 None 28-31 No data
Protriptyline 77-93 90-95 54-198 No data 19-57 70-170
Sertraline No data 98 22-35 Desmethyl 20 No data
Trazodone No data No data 4-9 m-Chlorophenyl-piperazine
No data No data
CLINICAL INDICATIONS
A.Depression.
B.Panic disorder.
C.Obsessive-compulsive disorders.
D.Enuresis.
E.Chronic pain.
DRUGS CHOICE
Antidepressant drugs are apt
most successful in patients
with”vegetative”
characteristics, including
psychomotor retardation, sleep
disturbance, poor appetite and
weight loss, and loss of libido.
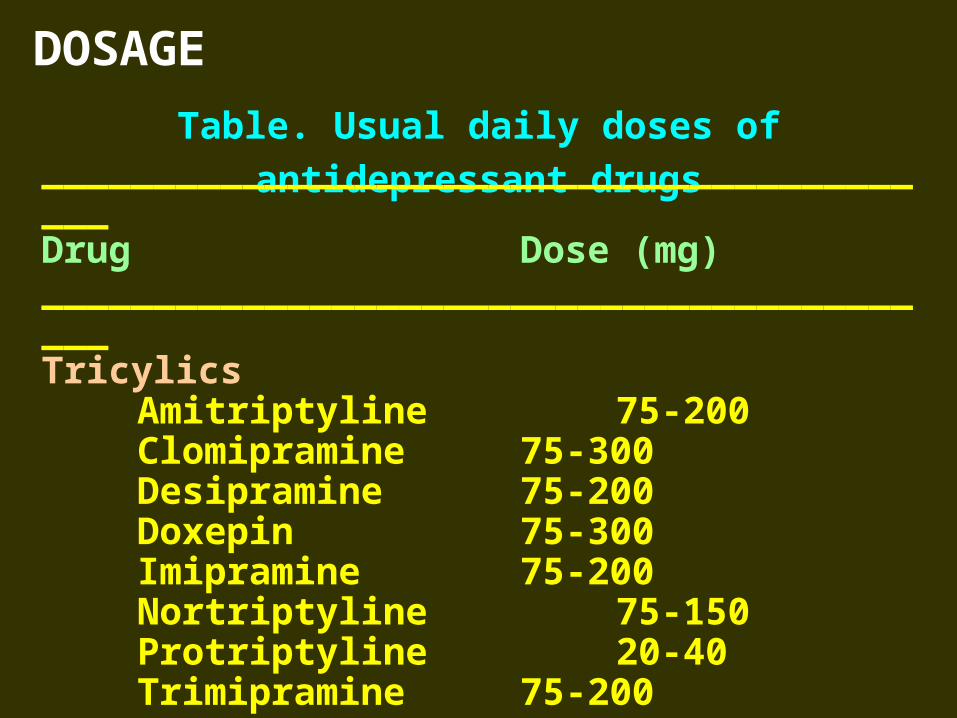
DOSAGE
Table. Usual daily doses of antidepressant drugs__________________________________________Drug Dose (mg)__________________________________________Tricylics
Amitriptyline 75-200Clomipramine 75-300Desipramine 75-200Doxepin 75-300Imipramine 75-200Nortriptyline 75-150Protriptyline 20-40Trimipramine 75-200
__________________________________________
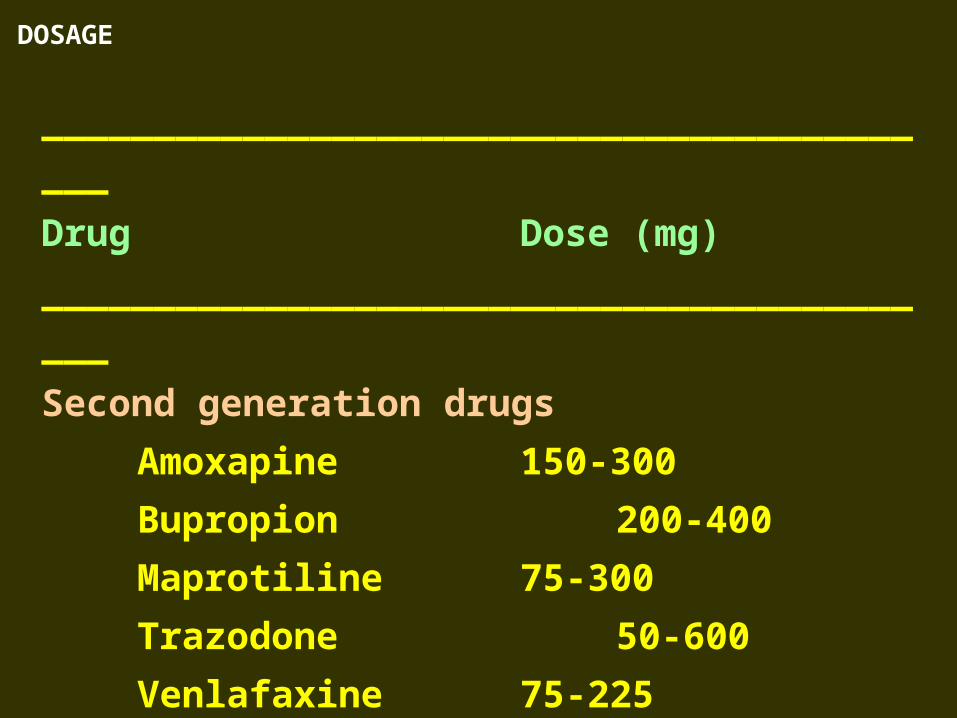
DOSAGE
__________________________________________
Drug Dose (mg)
__________________________________________
Second generation drugs
Amoxapine 150-300
Bupropion 200-400
Maprotiline 75-300
Trazodone 50-600
Venlafaxine 75-225
__________________________________________
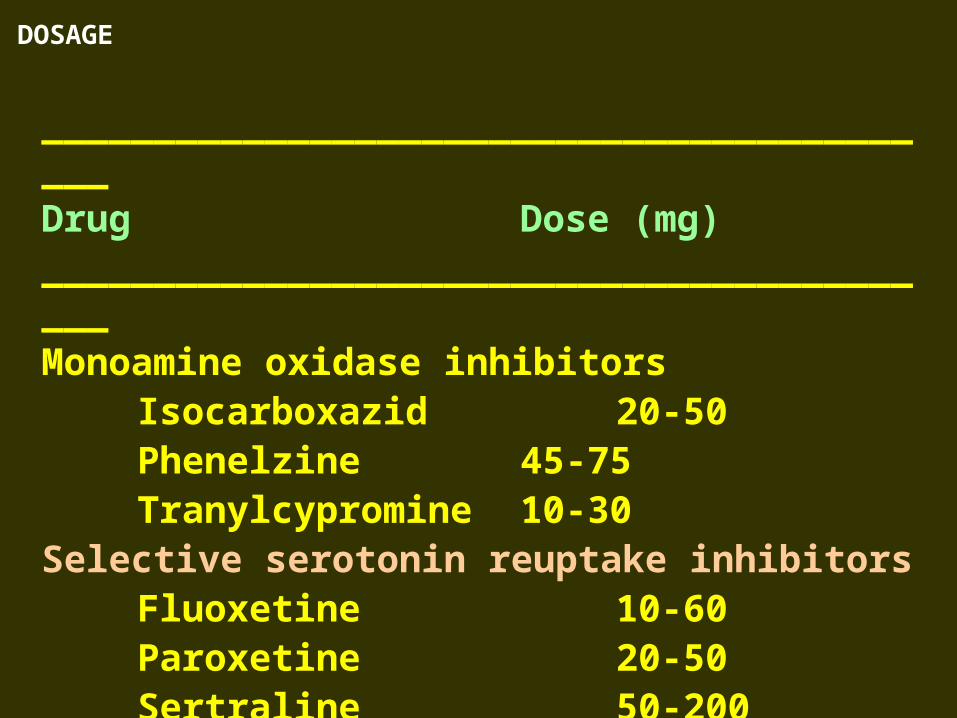
DOSAGE
__________________________________________Drug Dose (mg)__________________________________________Monoamine oxidase inhibitors
Isocarboxazid 20-50Phenelzine 45-75Tranylcypromine 10-30
Selective serotonin reuptake inhibitorsFluoxetine 10-60Paroxetine 20-50Sertraline 50-200
__________________________________________
ADVERSE EFFECTS
A. Tricyclic antidepressant
Unwanted effect antimuscarinic action, i.e. dry mouth (predisposing to tooth decay), blurred vision and difficulty with accommodation, raised intraocular pressure (glaucoma may be precipitated), bladder neck obstruction (may lead yo urinary retention in older males).
Postural hypotension, interference with sexual function, weight gain, prolongation of the QT interval of the ECG.
Some TCAs (especially trimipramine and amitriptyline) heavily sedating through combination of antihistaminergic and -adrenergic blocking actions.
Clinical features of overdose
(1) antimuscarinic effect (2)
consciousness (3) respiration
depression (4) hypothermia (5)
neurological signs include
hyperreflexia, myoclonus and
divergent strabismues. Extensor
plantar responses (6) sinus
tachycardia.
B. Selective serotonin reuptake
inhibitors
Unwanted effects nausea,
anorexia, dizziness,
gastrointestinal disturbance,
agitation, akathisia, (motor
restlessness) and anorgasmia
(failure to experience an orgasm).
Disrupt the pattern of sleep with increased awakenings, transient reduction in the amount of REM and increased REM latency but eventually sleep improves due to elevation of mood.
The serotonin syndrome restlessness, tremor, shivering and myoclonus possibly on to convulsions, coma and death.
C. Monoamine oxide inhibitors
Adverse effect postural
hypotension (especially in
elderly) and dizziness.
Less common headache, irritability, apathy, insomnia, fatigue, ataxia, gastrointestinal disturbances including dry mouth and constipation, sexual dysfunction (especially anorgasmis), blurred vision, difficult micturition, sweating, peripheral, oedema, tremulousness, restlessness, and hyperthermia.Appetite may increase inappropriately, causing weight gain.
INTERACTIONS
A. TCAs and SSRIs
Pharmacodynamic interaction : TCAs cause sedation and co-prescription with other sedative agents such as opioid analgesics, antihistamines, anxiolytics, hypnotics and alcohol excessive drowsiness and daytime somnolence.
Risk of QT prolongation with
many other cardiovascular drugs.
TCAs and SSRIs central
nervous system toxicity of co-
prescribed with the dopaminergic
drugs entacapone and selegiline
(for Parkinson’s disease).
SSRIs increase the risk of toxicity
when combined with other drugs
which upregulate serotonin
transmission.
Tricyclics and SSRIs lower the
convulsion threshold epilepsy more
difficult to control by anti-epilepsy
drugs and lengthening seizure time
in electroconvulsive therapy.
Pharmacokinetic
interactions : TCAs and
SSRIs metabolised
extensively by cytochrome
P450 enzymes.
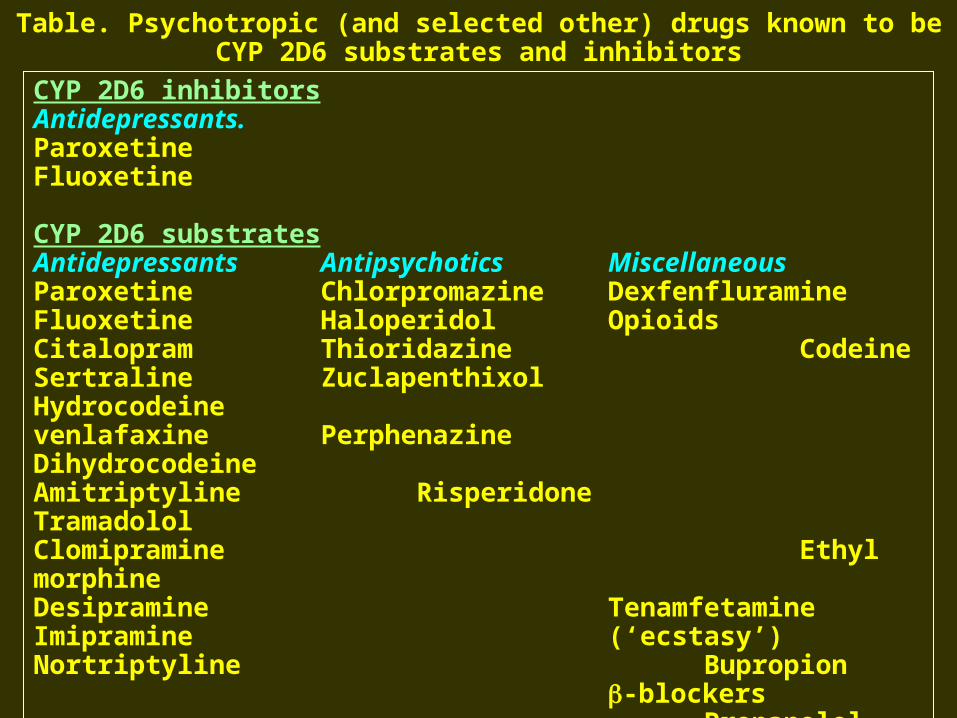
Table. Psychotropic (and selected other) drugs known to be CYP 2D6 substrates and inhibitors
CYP 2D6 inhibitorsAntidepressants.ParoxetineFluoxetine
CYP 2D6 substratesAntidepressants Antipsychotics MiscellaneousParoxetine Chlorpromazine DexfenfluramineFluoxetine Haloperidol OpioidsCitalopram Thioridazine CodeineSertraline Zuclapenthixol Hydrocodeinevenlafaxine Perphenazine DihydrocodeineAmitriptyline Risperidone TramadololClomipramine Ethyl morphineDesipramine TenamfetamineImipramine (‘ecstasy’)Nortriptyline Bupropion
-blockersPropanololMetoprololTimololBufaralol
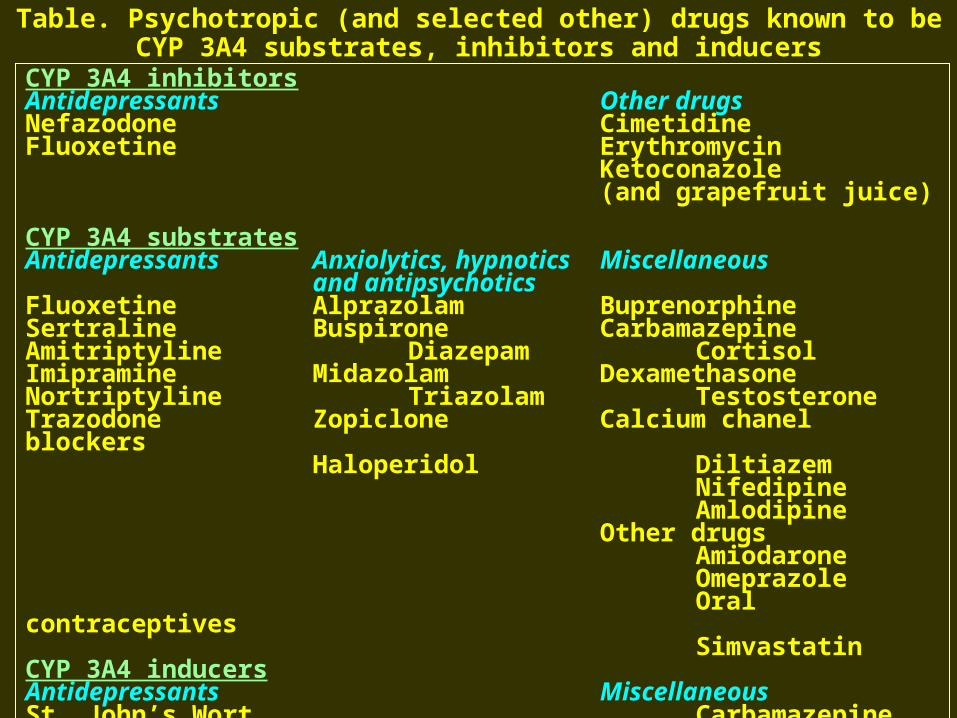
Table. Psychotropic (and selected other) drugs known to be CYP 3A4 substrates, inhibitors and inducers
CYP 3A4 inhibitorsAntidepressants Other drugsNefazodone CimetidineFluoxetine Erythromycin
Ketoconazole(and grapefruit juice)
CYP 3A4 substratesAntidepressants Anxiolytics, hypnotics Miscellaneous
and antipsychoticsFluoxetine Alprazolam BuprenorphineSertraline Buspirone CarbamazepineAmitriptyline Diazepam CortisolImipramine Midazolam DexamethasoneNortriptyline Triazolam TestosteroneTrazodone Zopiclone Calcium chanel blockers
Haloperidol DiltiazemNifedipineAmlodipine
Other drugsAmiodaroneOmeprazoleOral contraceptivesSimvastatin
CYP 3A4 inducersAntidepressants MiscellaneousSt. John’s Wort Carbamazepine
PhenobarbitalPhenytoin
B. Monoamine oxidase inhibitors
Sympathomimetic substances
highly dangerous hypertensive
reactions if taken by patient
using MAC inhibitors.
ANTIPSYCHOTIC AGENTS
The terms antipsychotic ––
a group of drugs that have
been used mainly for
treating schizophrenia.
CHEMICAL TYPES
The drugs can be classified into
several groups.
BASIC PHARMACOLOGY OF
ANTIPSYCHOTIC AGENTS
A. Phenothiazine Derivatives
Three subfamilies of
phenothiazines (1) Aliphatic
derivatives [eg.chlorpromazine]
(2) Piperidine derivatives
[eg.thiodazine] (3) Piperazine
derivatives.
B. Thioxanthene Derivatives
C. Butyrophenone Derivatives.
D. Miscellaneous Structures : • Diphenylbutylpiperidines
(pimozide).
• Dihyroindolones (molindone).
• Dibenzoxazepines (loxapine).
• Dibenzodiasepines (clozapine).
• Benzamides (remoxipride).
PHARMACOKINETICS
A. Absorption & Distribution
Most antipsychotic drugs are
readily but incompletely
absorbed.
Many of these drugs undego
significany first-pass
metabolism.
Oral doses of chlorpromazine
and thioridazine, haloperidol,
which is less likely to be
metabolized, has an average
systemic availability of about
65%.
Highly lipid-soluble, protein-
bound (93-99%).
Metabolites of chlorpromizine
may be excreted in the urine
weeks after the last dose.
B. Metabolism.
Almost completely metabolized
by a variety of processes.
C. Excretion.
Elimination half-lives vary from
10-24 hours.
PHARMACOLOGIC EFFECTS
The first phenothiazine
antipsychotic drugs, with
chlorpromazine as the
prototype, proved to have a wide
variety of CNS, autonomic, and
endocrine effects.
These actions were traced to
blocking effects at a remarkable
number of receptors.
These include dopamine and
alpha-adrenoceptor, muscarinie,
H1 histaminic and serotonin (5-
HT2) receptors.
A. Dopaminergic systemic.
After dopamine was recognized
as a neurotransmitter, various
experiments showed that its
effects on production of cAMP
by adenylyl cyclase could be
blocked by most antipsychotic
drugs.
Antipsychotic action is now
though to be produced by their
ability to block dopamine in the
mesolimbic and mesofrontal
systems.
B. Dopamine Receptors and
Their Effects.
At present, five different
dopamine receptors have been
described, consisting of two
separate families, the D1-like and
D2-like receptor groups.
The D1 receptor is coded by a
gene on chromosome 5,
increases cAMP by activation of
adelylyl cyclase, and is located
mainly in the putamen, nucleus
accumbens, and olfactory
tubercle.
The second member of this
family, D5, is coded a gene on
chromosome 4, also
increases cAMP, and is found
in the hypocampus and
hypothalamus.
C. Differences Among
Antipsychotic Drugs.
Although all effective
antipsychotic drugs block D2
receptors, the degree of this
blockade in relation to other
actions on receptors varies
considerably between drugs.
D. Neurophysiologic Effects.
Antipsychotic drugs produce
shifts in the patient of
electroencephalographic,
frequencies.
The slowing (hypersynchrony) is
sometimes focal or unilateral,
which.
E. Endocrine Effects.
Amenorrhea-galactorrhea, false-
positive pregnancy tests, and
increased libido have been
reported in women, whereas men
have experienced decreased
libido & gynecomastia.
F. Cardiovascular Effects.
Orthostatic hypotension and high
resting pulse rates frequently
result from use of the “high dose”
(low potency) phenothiazines.
Mean arterial pressur, peripheral
resistance, and stroke volume are
decreased.
INDICATION
A. Psychiatric Indications.
Schizophrenia is the primary
indication for these drugs.
CLINICAL PHARMACOLOGY OF
ANTIPSYCHOTIC AGENTS
Other psychiatric indications for
the use of antipsychotics include
Tourette’s syndrome and the
need to control disturbed
behavior in patients with senile
dementia of the Alzheimer type.
Antipsychotics in small
doses have been promoted
for the relief of anxiety
associated with minor
emotional disorders.
B. Nonpsychiatric Indications
Most antipsychotic drugs, a
strong antiemetic effect.
DOSAGE
The range of effective dosage
among various antipsychotics is
quite broad.
Patients who fail to respond to
one drug may respond to
another.
ADVERSE REACTIONS
A. Behavioral Effects.
A “pseudodepression” that may be due to drug-induced akinesia usually responds to treatment with antiparkinsonism.
Toxic-confusional states may occur.
B. Neurologic Effects.
Extrapyramidal reactions occuring early during treatment include typical Parkinson’s syndrome, akathisia (uncontrollable restlessness), and acute dystonic reactions (spastic retrocollis or torticollis), tardive dyskinesia, seizures.
C. Autonomic Nervous System Effects.
Most patients become tolerant to antimuscarinic adverse effects of antipsychotic drugs.
Orthostatic hypotension or impaired ejaculation – common complications of therapy with chlorpromazine or mesoridazine-should.
D. Metabolic and Endocrine
Effects.
Hyperprolactinemia in women
results in the amenorrhea-
galactorrhea syndrome and
infertility; in men, loss of libido,
importance, and infertility may
results.
E. Toxic or Allergic Reactions.
Agranulocytosis, cholestatic
jaundice, and skin eruptions
occur rarely with the high-
potency antipsychotic drugs
currently used.
F. Ocular Complications.
Deposits in the anterior
portion of the eye (cornea and
lens) are a common
complication of
chlorpromazine therapy.
G. Cardiac Toxicity.
Thioridazine in dose exceeding
300 mg daily is almost always
associated with minor
abnormalities of T waves.
H. Use in Pregnancy;
Dysmorphogenesis.
I. Neuroleptic Malignant
Syndrome.
MOOD STABILISERS
Mode of action not fully
understood.
Main effect inhibit hydrolysis
of inositol phosphate reducing
the recycling free inositol for
synthesis of
phosphatidylinositides.
LITHIUM
Pharmacokinetics
Therapeutic plasma concentration
close to the toxic concentration
(low therapeutic index).
Orally rapidly absorbed.
Peak plasma lithium concentration
5 h.
Distributed throughout the
total body water higher
concentration in brain, bones
and thyroid gland.
Filtered by the glomerulus,
80% is reabsorbed by the
proximal tubule.
Chronic use the plasma t1/2 of
lithium 15-30 h.
Lithium given 12 hourly to
avoid unnecessary fluctuation,
maintain a plasma
concentration just below the
toxic level.
A steady-state plasma
concentration 5-6 days (i.e. 5
x t1/2) in patients with normal
renal function.
Old people and patients with
impaired renal function a
longer t1/2.
Indications and Use
Lithium carbonate effective treatment in > 75% of episodes of acute mania of hypomania.
Lithium used in combinations with benzodiazepine.
For prophylaxis, lithium is indicated two episodes of mood disturbance in two years.
Adverse Effects• Fine tremor (especially involving
the fingers), constipation, polyuria and polydipsia, metallic taste in the mouth, weight gain, oedema, goitre, hypothyroidism, acne, rash, diabetes insipidus and cardiac arrhytmias. Mild cognitive and memory impairment.
• Signs of infoxication (plasma concentration greater than 1.5 mmol/1) gastrointestinal (diarrhoea, anorexia, vomiting), neurological, (blurred vision, miscle weakness, drowsiness, sluggishness, coarse tremor, leading on to giddiness, ataxia, dysarhria).
• Severe overdosage or rapid
reduction in renal clearance
hyperreflexia,
hyperextension of limbs,
convulsions, toxic
psychoses, syncope,
oliguria, coma, death.
Interactions
Drug interfere with lithium
excretion by the renal tubules
diuretics, ACE inhibitors
and angiotensin-11 antagonis,
non steroidal anti-
inflammatory analgesics.
Theophylline and sodium-
containing antacids plasma
lithium concentration.
Diltiazem, verapamil,
carbamazepine and phenytoin
neurotoxicity.
Concomitant use of thioridazine
ventricular arrhythmias.
Carbamazepine as an alternative of lithium for prophylaxis of bipolar affective disorder.
Mode of action involve anonism in inhibitory GABA transmission at the GABA-benzodiazepine receptor complex.
Carbamazepine
Valproic acid licenced for
use in the treatment of acute
mania unresponsive to
lithium.
Valproic Acid
DRUGS USED IN ANXIETY AND SLEEP
DISORDERS
Treatment
Fast-acting benzodiazepine such as alprazolam (1-3 mg/day p.o.), drug with delayed efficacy but fewer problems of withdrawal such as a TCA, e.g. clomipramine (100-250 mg/day p.o) or an SSRI, e.g. paroxetine (20-50 mg/day p.o).
PANIC DISORDER

Treatment
The drugs SSRI, paroxetine,
the MAOI, phenelzine and the
RIMA, moclobemide in the
same doses as for depression.
SOCIAL ANXIETY DISORDES
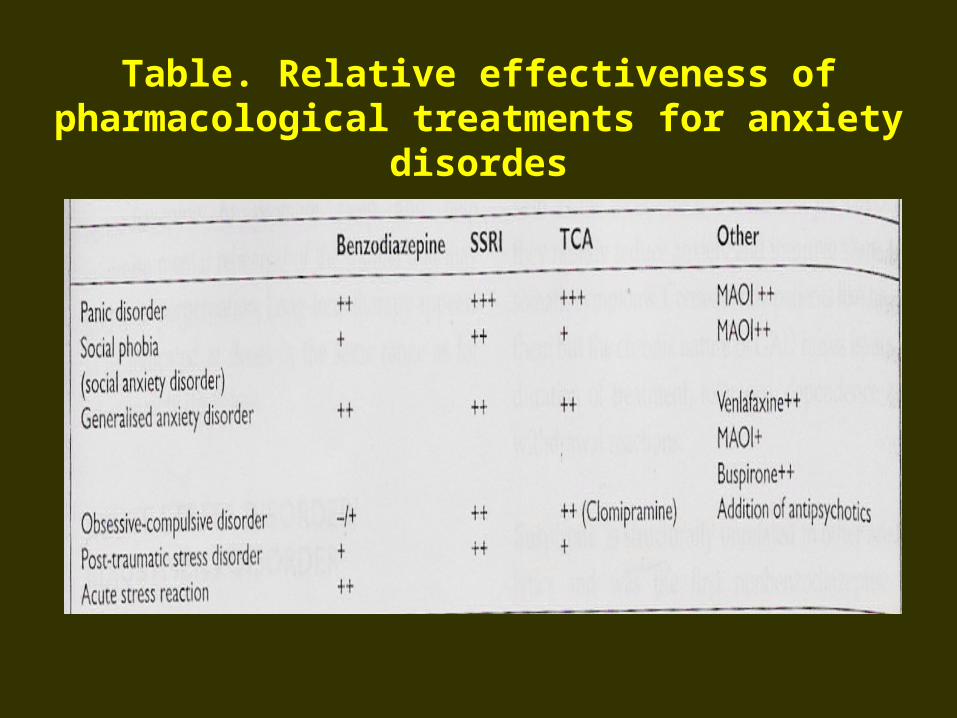
Table. Relative effectiveness of pharmacological treatments for anxiety disordes
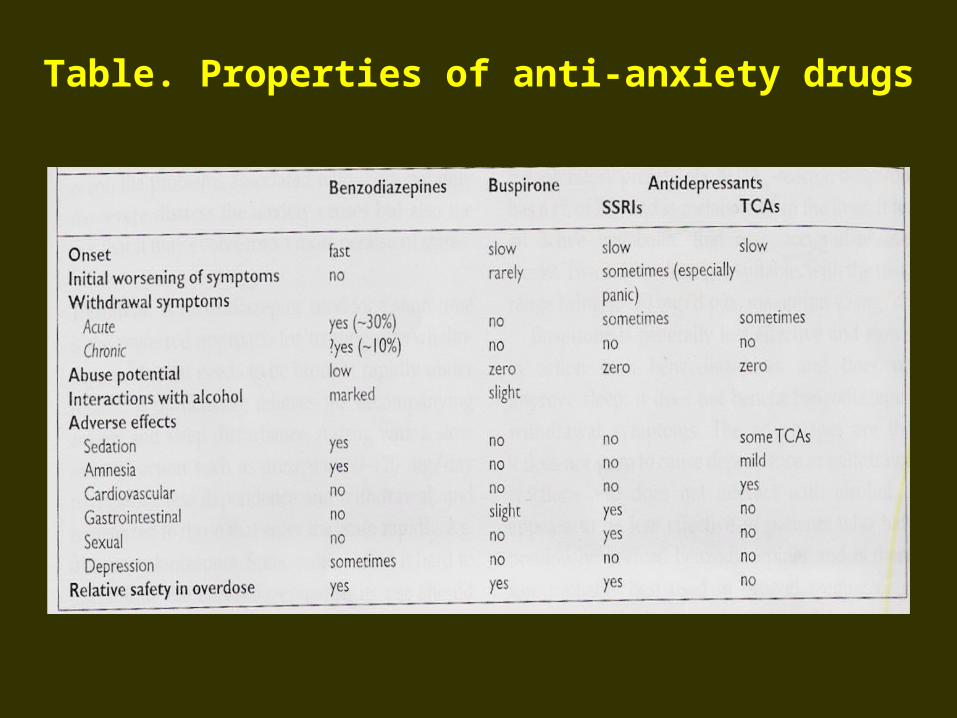
Table. Properties of anti-anxiety drugs
Treatment is poorly researched.
Benzodiazepines, TCAs and
MAOIs; paroxetine (SSRI) (20-
50 mg/day p.o) licenced for
this indications.
POST-TRAUMATIC STRESS DISORDES
(PTSD)
Buspirone
Structurally unrelated to other
anxiolytics efficacy in GAD.
Mode of action suppresses 5HT
neurotransmission through a
selective activation of the inhibitory
presynaptic 5HT1A-receptor.
GENERALISED ANXIETY DISORDER
Buspirone a t1/2 of 7 h, metabolised
in the liver, an active metabolite that, may accumulate over weeks.
Twice daily dosing range being 15-30 mg/d p.o., max. 45 mg/d.
Adverse effect can dizziness, headache, nervousness, excitement, nausea, tachycardia and drowsiness.
The Duration of Therapy
Depends on the nature of the
underlying illness.
Paroxetine (SSRI) & Venlafaxine (SNRI)
Effective.
TCAs benefit.
DRUGS FOR INSOMNIA
Benzodiazepines
All benzodiazepines and newer
benzodiazepine safe and
effective for insomnia.
INSOMNIA
Pharmacokinetics.
Benzodiazepines effective after
administration by mouth but
enter the circulation at very
different rates that are reflected
in the speed of onset of action.
Liver metabolises usually to
inactive metabolites, some
compounds produce active
metabolites, some with long t1/2
which greatly extends drug
action.
Uses.
Benzodiazepine used for : insomnia, anxiety, alcohol withdrawal states, muscle spasm due to a variety of causes, including tetanus and cerebral spasticity, epilepsy (clonazepam), anaesthesia and sedation for endoscopies and cardioversion.
• Intravenous formulations, e.g. diazepam 10-20 mg, given at 5 mg/min into a large vein (antecubital fossa) to minimise thrombosis: the dose may be repeated once in 10 min for status epilepticus or in 4 h for severe acute anxiety or agitation.
Doses.
Oral doses as anxiolytics given with their indications :
• Intramuscular injection of
diazepam is absorbed,
slower in acting than an
oral dose.
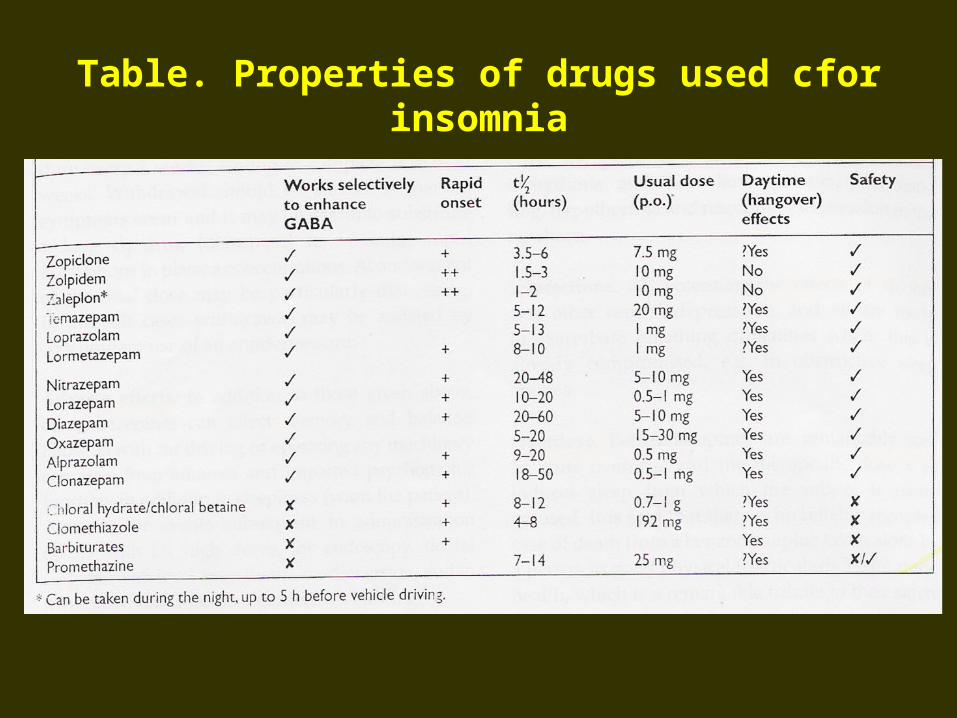
Table. Properties of drugs used cfor insomnia
Adverse Effects.
Benzodiazepines affect memory and balance.
Paradoxical behaviour effect, perceptual disorders.
Headache, giddiness, alimentary tract upset, skin rashes and reduced libido can occur.
Extrapyramidal reaction.
Interactions.
All potentiate the effects of
alcohol, other central
depressants.
Overdose.
Benzodiazepines are
remarkably, safe in acute
overdose and the therapeutic
dose x 10.
Deaths have occurred
combination with alcohol.
• Drug treatment : effective for a short period (2-4 weeks).
• Some patients need long-term medication.
SUMMARY OF PHARMACOTHERAPY
FOR INSOMNIA
• Intermittent medication, taken only nights that symptoms occur, modern, short-acting, compound.
• Discontinuing hypotic drugs not a problem.
