pharmacologic pain management for the older adult leigh m. boehmer, pharm.d., bcop clinical...
TRANSCRIPT

Pharmacologic Pain Management for the Older Adult
Leigh M. Boehmer, Pharm.D., BCOPClinical Pharmacist, Medical OncologyBarnes Jewish HospitalApril 11, 2015
Disclosure
• Leigh M. Boehmer, Pharm.D., has no real or apparent conflicts of interest to report

Objectives
• Review how physiologic changes and altered pharmacology affect management of pain in the elderly
• Describe available tools for medication review for possible therapeutic duplication, inappropriate use, and drug interactions in the elderly
• Discuss special considerations for pharmacologic pain management in specific clinical settings in the elderly
Objectives
• Review how physiologic changes and altered pharmacology affect management of pain in the elderly
• Describe available tools for medication review for possible therapeutic duplication, inappropriate use, and drug interactions in the elderly
• Discuss special considerations for pharmacologic pain management in specific clinical settings in the elderly

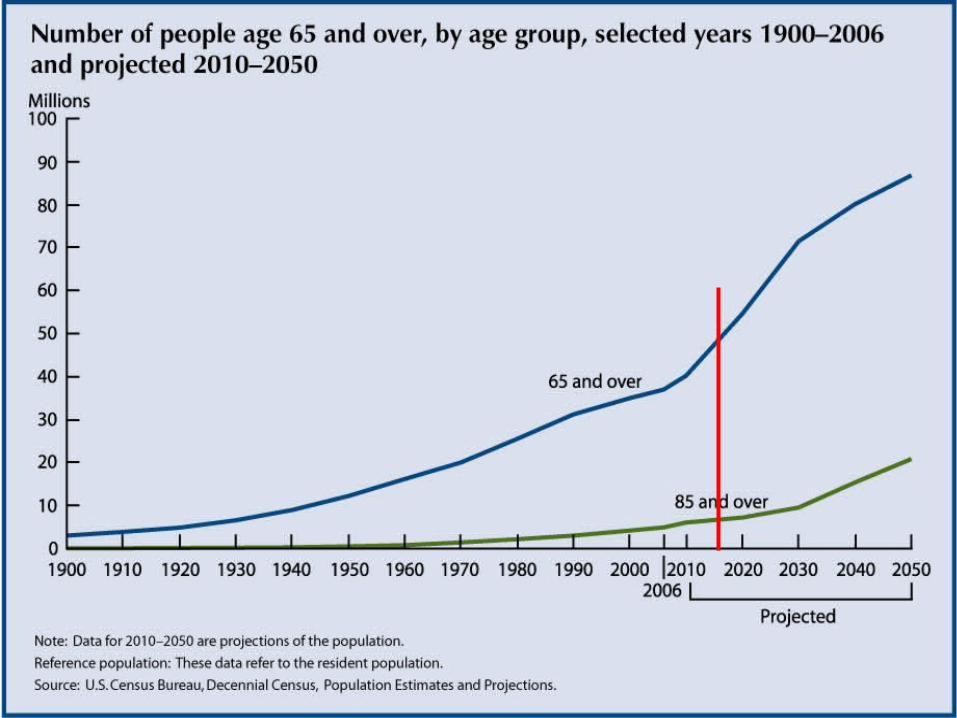
US Elderly: Demographics
• Those >85 yoa are fastest growing segment of US population– 5 million today; 20 million by 2050
• 1:6 Americans >65 yoa by 2020– 54 million elderly, up from 3 million in 1990
• 1.3 billion >65 yoa worldwide in 2040
Available at www.census.gov. Accessed on 2.14.15.
Pain Prevalence in the Elderly
• 1:5 elderly have pain– 3:5 pain lasting for ≥1 year
• 31% of women and 19% of men >75 yoa report pain in ≥3 sites
• Community-dwellers: 25-56%• Nursing home residents: 45-80%
– Pain not detected by treating MDs in 34%
American Geriatrics Society. JAGS. 2002;50: S205-24.
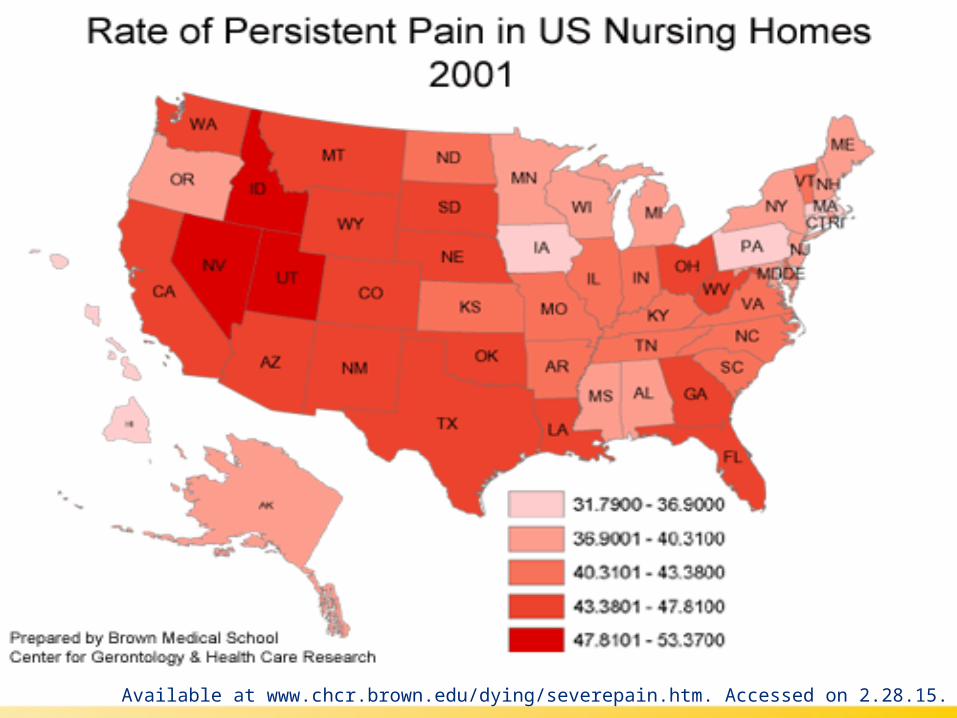
Available at www.chcr.brown.edu/dying/severepain.htm. Accessed on 2.28.15.
Age-Related Pain Changes
• ↓ # and function of peripheral nociceptive neurons
• Thermal and vibratory stimuli sensory threshold increases with age
• 50% ↓ in Pacini’s corpuscles and 10-30% ↓ in Merkle’s disks (pain receptors)
• ↓ endogenous analgesic response via ↓ secretion of endorphins
Cassel C (Ed), et al. Geriatric Medicine: An Evidence-Based Approach. 2003.
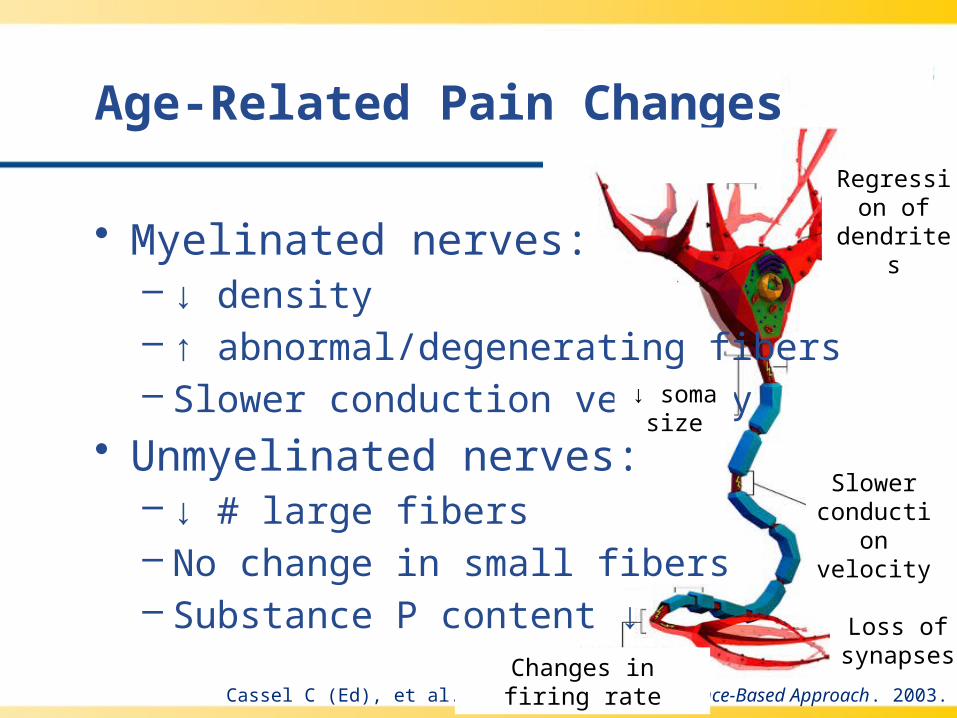
Age-Related Pain Changes
• Myelinated nerves:– ↓ density– ↑ abnormal/degenerating fibers– Slower conduction velocity
• Unmyelinated nerves:– ↓ # large fibers– No change in small fibers– Substance P content ↓
Cassel C (Ed), et al. Geriatric Medicine: An Evidence-Based Approach. 2003.
Loss of synapsesChanges in firing rate
Slower conduction
velocity
Regression of dendrites
↓ soma size

Age-Related Pain Changes
• Central nervous system– Loss in # of dorsal horn, cortex, midbrain,
and brainstem neurons– ↓ circulating catecholamines, acetylcholine,
GABA, and serotonin – Altered cerebral evoked responses
Cassel C (Ed), et al. Geriatric Medicine: An Evidence-Based Approach. 2003.
GABA=gamma-amminobutyric acid

Age-Related Physiologic Changes
• ↓ volume of distribution– ↓ lean body weight
• ↓ serum protein concentrations• ↓ renal function• ↓ liver mass and hepatic blood flow• ↓ activity of drug-metabolizing enzymes• ↓ pulmonary function

Age-Related Pharmacologic Changes
Pharmacologic Concern Changes with Aging Common Disease Effects
Gastrointestinal (GI) absorption or function
• Slowing of GI transit time; may prolong effects of continuous release drugs
• Opioid-related GI dysmotility may be enhanced
• Disorders that alter gastric pH may ↓↑ select drug absorption
• Surgically altered anatomy may ↓ select drug absorption
Transdermal absorption• Few changes in absorption
under most circumstances• Temperature and other
patch technology may affect absorption
Distribution• ↑ fat to lean body weight
ratio may ↑ Vd for fat-soluble drugs
• Aging and obesity may result in ↑ drug half-life
Vd=volume of distribution
American Geriatrics Society. JAGS. 2009;57: 1331-46.

Achlorhydria and Drug Absorption
Which of the following agents has been associated with significantly increased GI absorption in the setting of achlorhydria?
a) morphine
b) oxycodone
c) hydromorphone
d) methadone

Achlorhydria and Drug Absorption
Which of the following agents has been associated with significantly increased GI absorption in the setting of achlorhydria?
a) morphine
b) oxycodone
c) hydromorphone
d) methadone
Garnett W. Am J Health-Syst Pharm. 1998;55: 2268-79.
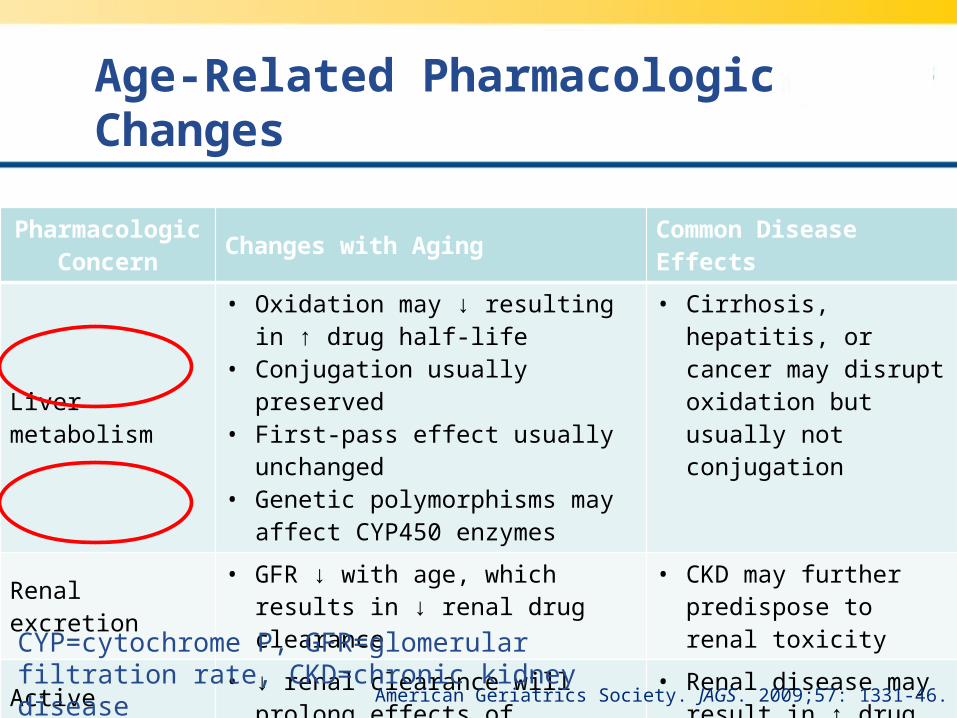
Age-Related Pharmacologic Changes
Pharmacologic Concern
Changes with Aging Common Disease Effects
Liver metabolism
• Oxidation may ↓ resulting in ↑ drug half-life
• Conjugation usually preserved• First-pass effect usually unchanged• Genetic polymorphisms may affect
CYP450 enzymes
• Cirrhosis, hepatitis, or cancer may disrupt oxidation but usually not conjugation
Renal excretion• GFR ↓ with age, which results in ↓
renal drug clearance• CKD may further
predispose to renal toxicity
Active metabolites• ↓ renal clearance will prolong
effects of metabolites• Renal disease may
result in ↑ drug half-life
CYP=cytochrome P, GFR=glomerular filtration rate, CKD=chronic kidney disease
American Geriatrics Society. JAGS. 2009;57: 1331-46.
Hepatic Changes in the Elderly
• ↓ liver mass by 1% per year after age 50• 33% ↓ in flow and 21% ↓ in portal blood
velocity over age 65• ↓ serum albumin levels and quality
– ↑ free fraction of protein bound drugs• No significant change in liver function tests• Decline in ability of liver to regenerate
– Capacity, however, remains unchanged
Kaye A, et al. The Ochsner Journal. 2010; 10(3): 179-87.
Hepatic Changes in the Elderly
• 2 CYP enzymes most important to psychotro- pic prescribing ↓ with age (-1A2 and -3A)
• Bioavailability of high first- pass elimination drugs ↑d due to 30-40% ↓ in elimin- ation of liver metabolized agents
Pergolizzi J, et al. World Institute of Pain. 2008;8(4): 287-313.

Effect of Reduced Hepatic Function on Opioid Pharmacokinetics
Opioid T1/2Metabolite [plasma]
Comment RecommendationEvidence
Level
Morphine ↑ ↓ M6G ↓ Dose ↓ IIb
Oxycodone ↑ ↑ Dose ↓ IIb
Hydromorphone ? ? No data Dose ↓ IV
Fentanyl TD ↑ ? Dose ↓ III
Buprenorphine TD
↑ ↓Low activity metabolite
Dose ↓ IIb
Methadone ↑ ? No data No dose change IIb
T1/2=half-life, M6G=morphine-6-β-glucuronide, ?=unknown, TD=transdermal
Pergolizzi J, et al. World Institute of Pain. 2008;8(4): 287-313.

Renal Changes in the Elderly
• ↓ size by 20-30% by age 70• ↓ in renal blood flow by 10% per decade
after age 20– GFR ↓ 10 mL/min per decade after age 20– Plasma filtration rate ↓ more than GFR
• ↓ free water absorption by 5% per decade after age 50
• ↓ length, #, and thickness of renal tubules• ↑ interstitial tissue and tubular diverticulaKaye A, et al. The Ochsner Journal. 2010; 10(3): 179-87.
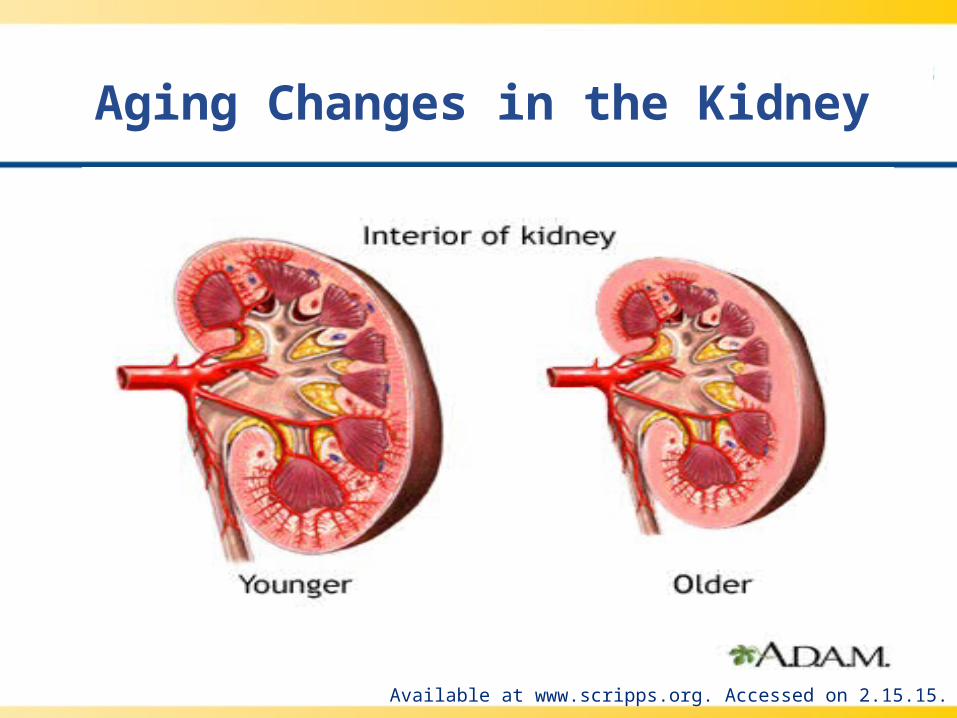
Aging Changes in the Kidney
Available at www.scripps.org. Accessed on 2.15.15.

Effect of Impaired Renal Function on Opioid Pharmacokinetics
Opioid T1/2Metabolite [plasma]
CommentRecomm-endation
Evidence Level
Morphine ↑ ↑↑↑ M6G and M3G may lead to ↓ respiratory drive
Dose ↓ IIa
Oxycodone ↑ ↑↓ clearance of parent compound and metabolite
Dose ↓ IIb
Hydromorphone ↑ ↑↑Metabolite accumulation described
Dose ↓ IIb
Fentanyl TD ↑ ↑ ↓ clearance in elderly Dose ↓ IIb
Buprenorphine TD
= =No clinically relevant changes
Adjust ± IIa
Methadone ↑ ↑ Use with caution Dose ↓ IV
T1/2=half-life, M6G=morphine-6-β-glucuronide, M3G=morphine-3-glucuronide, TD=transdermal
Pergolizzi J, et al. World Institute of Pain. 2008;8(4): 287-313.

Narrowed Therapeutic Window↑
Dru
g C
on
cen
trat
ion
Available at www.neurology.org. Accessed on 2.28.15.

Factors Affecting Pain Perception
• Uncontrolled pain ↓ overall quality of life• Loneliness ↓s pain threshold and is a risk
factor for depression– Lack of intimate relationships, dependency
and loss ↑ loneliness• Depression and anxiety limit patients’
engagement in treatment and ↑ healthcare needs
Deane G and Smith H. Clin Geriatr Med. 2008;24(2): 185-201.
Factors Affecting Pain Perception
• Uncontrolled pain ↓ overall quality of life• Loneliness ↓s pain threshold and is a risk
factor for depression– Lack of intimate relationships, dependency
and loss ↑ loneliness• Depression and anxiety limit patients’
engagement in treatment and ↑ healthcare needs
Deane G and Smith H. Clin Geriatr Med. 2008;24(2): 185-201.

Objectives
• Review how physiologic changes and altered pharmacology affect management of pain in the elderly
• Describe available tools for medication review for possible therapeutic duplication, inappropriate use, and drug interactions in the elderly
• Discuss special considerations for pharmacologic pain management in specific clinical settings in the elderly
Objectives
• Review how physiologic changes and altered pharmacology affect management of pain in the elderly
• Describe available tools for medication review for possible therapeutic duplication, inappropriate use, and drug interactions in the elderly
• Discuss special considerations for pharmacologic pain management in specific clinical settings in the elderly
Managing Pain in Older Adults
• Thorough pain assessment• Knowledge of underlying condition(s)• Consideration of comorbidities• Past response to therapies• Psychologic and social circumstances• Economic factors• Caregiver and living situation• Patient’s comfort and functional goals• Treatment team’s goals• Polypharmacy concerns• Drug-drug interactions Arnstein P. Pain Management Nursing. 2010;11(2): S11-22.

Pain Assessment Challenges
• Fear of becoming addicted• Myth that pain is a “natural” part of aging• Sensory and cognitive impairments• Under-reporting of pain• Complications of comorbidities• Caregivers’ perception of pain (lack of
congruence with patient)
Stein W. Clinics in Geriatric Medicine. 2001;17(3): 575-94.

Potentially Inappropriate Medication Use
Estimated annual US healthcare costs related to the use of potentially inappropriate medications (PIM) was which of the following?
a) $3 billion
b) $5.5 billion
c) $7.2 billion
d) $9.3 billion
Potentially Inappropriate Medication Use
Estimated annual US healthcare costs related to the use of potentially inappropriate medications (PIM) was which of the following?
a) $3 billion
b) $5.5 billion
c) $7.2 billion
d) $9.3 billionFu A, et al. Med Care. 2007;45: 472-6.
Screening Tool to Alert doctors to the Right Treatment (START)
• “Inappropriate” prescribing:– Acts of commission (giving unsuitable drugs)– Acts of omission (failure to give when
indicated)• N=600 elderly (≥65 yoa) patients admitted
with acute illness to a teaching hospital– START used to assess errors of omission– ≥1 omissions found in 57.9% of patients
Barry P, et a. Age and Ageing. 2007;36: 632-8.

START Criteria (Select Examples)
• Cardiovascular system• Respiratory system• Central nervous system (CNS)
– Antidepressant in the presence of clear-cut symptoms, lasting at least 3 months (N=10)
• GI system• Locomotor system
– Anti-rheumatic drug therapy with known, mod-severe disease lasting >12 weeks (N=13)
• Endocrine system Barry P, et a. Age and Ageing. 2007;36: 632-8.

Likelihood of Omission
• 65-74 yoa: 55.2% (1 med omitted)• 75-84 yoa: 54.8% (1 med omitted)
– OR 1.05, CI 0.71-1.45; P=0.93
• ≥85 yoa: 72.2% (1 med omitted)– OR 2.08, CI 1.24-3.5; P<0.01
• Females vs. males (1 med omitted)– OR 2.29, CI 1.65-3.19; P<0.01
Barry P, et a. Age and Ageing. 2007;36: 632-8.

2012 Updated Beers Criteria: Pain
Therapeutic Class/Drug(s)
Rationale RecommendationQuality of Evidence
Strength of Recommendation
Meperidine- Neurotoxicity- Not effective in doses used
Avoid High Strong
Non-COX selective NSAIDs
- ↑ risk GI bleeding and peptic ulcer dx
Avoid chronic use, unless other options are not available
Moderate Strong
IndomethacinKetorolac
- ↑ risk GI bleeding- Most AEs of all NSAIDs (indomethacin)
AvoidModerate/
HighStrong
2012 Beers Criteria Update Expert Panel. JAGS. 2012;1-16.
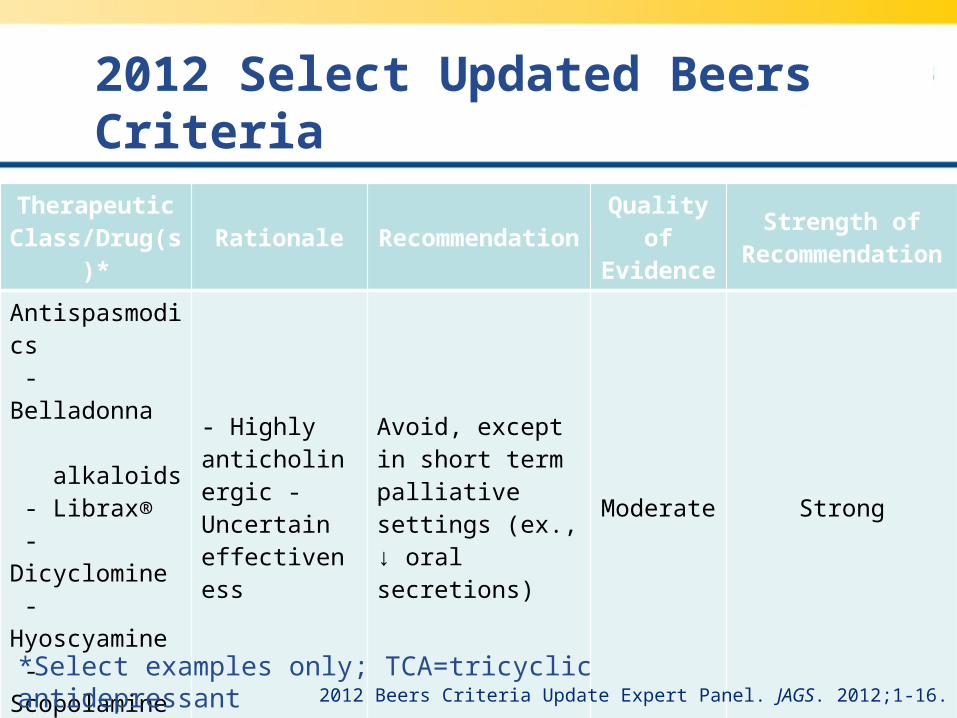
2012 Select Updated Beers Criteria
Therapeutic Class/Drug(s)*
Rationale RecommendationQuality of Evidence
Strength of Recommendation
Antispasmodics - Belladonna alkaloids - Librax® - Dicyclomine - Hyoscyamine - Scopolamine
- Highly anticholinergic - Uncertain effectiveness
Avoid, except in short term palliative settings (ex., ↓ oral secretions)
Moderate Strong
Tertiary TCAs - Amitriptyline - Clomipramine - Doxepin (>6 mg/day) - Imipramine
- Highly anticholinergic- Sedating- Orthostatic hypotension
Avoid High Strong
2012 Beers Criteria Update Expert Panel. JAGS. 2012;1-16.
*Select examples only; TCA=tricyclic antidepressant
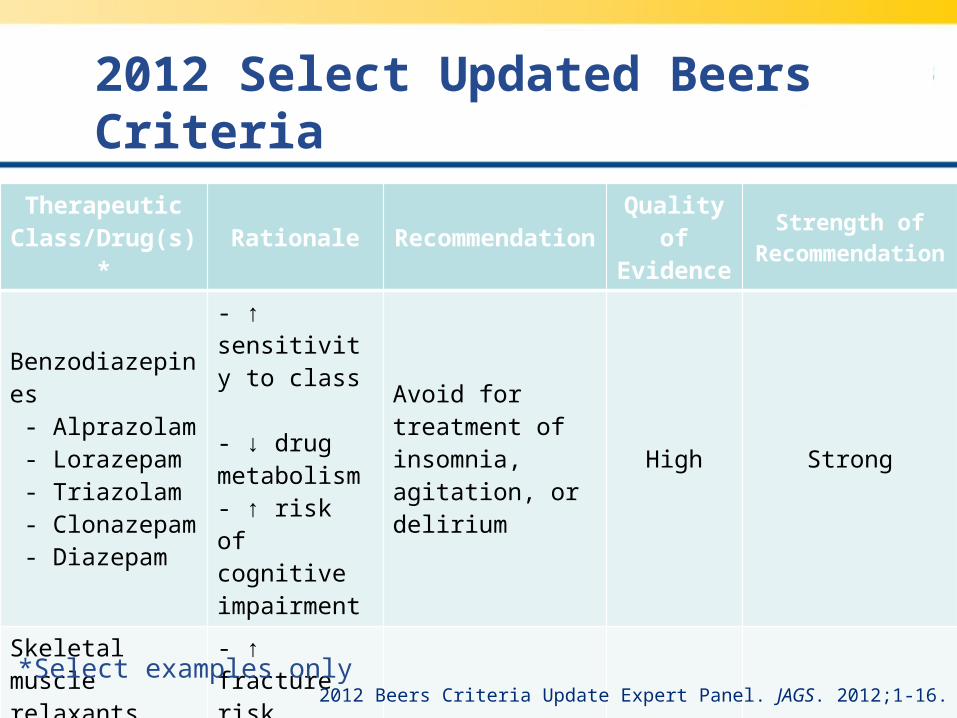
2012 Select Updated Beers Criteria
Therapeutic Class/Drug(s)*
Rationale RecommendationQuality of Evidence
Strength of Recommendation
Benzodiazepines - Alprazolam - Lorazepam - Triazolam - Clonazepam - Diazepam
- ↑ sensitivity to class - ↓ drug metabolism- ↑ risk of cognitive impairment
Avoid for treatment of insomnia, agitation, or delirium
High Strong
Skeletal muscle relaxants - Carisoprodol - Flexeril® - Metaxolone - Methocarbamol
- ↑ fracture risk, sedation- Efficacy at tolerable doses questionable
Avoid Moderate Strong
2012 Beers Criteria Update Expert Panel. JAGS. 2012;1-16.*Select examples only

Screening Tool of Older Persons’ potentially inappropriate Prescriptions (STOPP)
Gallagher P and O’Mahony D. Age and Ageing. 2008;37: 673-9.
Study population
715 consecutive admissions to a university teaching hospital in patients ≥65 yoa
DesignSTOPP and Beers criteria applied to prospective review of diagnoses, reason for admission, and concurrent medications
Results
•Primary endpoint: identification of PIM via STOPP and Beers criteria•Secondary endpoint: Proportion of PIM with causal connection to reason for admission

STOPP Results
• STOPP criteria:– 336 PIMs divided amongst 35% (N=247)
• 25% one PIM, 7% two PIMs, 2% three PIMs, 1% four PIMs; 1 patient with five PIMs
– 91% AEs responsible for admission “caught”• Beers criteria:
– 226 PIMs divided amongst 25% (N=177)• 19% one PIM, 5% two PIMs, 3% three PIMs; 1
patient with four PIMs
– 48% AEs responsible for admission “caught”Gallagher P and O’Mahony D. Age and Ageing. 2008;37: 673-9.

STOPP (Select) Criteria
Criterion N PIM AE as a causal factor to admission
Long term, long-acting benzodiazepine
6526 (fall 9; fall + fracture 8; fall + head injury 1; overdose 1; cognitive decline 7)
NSAID with h/o PUD or GI bleeding 3 1 (PUD)
NSAID with h/o mod-severe HTN 20 3 (GI bleed 2; PUD 1)
Long-term NSAID for joint pain 9 1 (PUD)
NSAID with chronic renal failure 9 1 (acute renal failure)
Long-term opiates in those with recurrent falls
1 1 (fall + femur fracture)
Long-term opiates as first-line therapy for mild-mod pain
13 3 (fall + femur fracture)
Long-term opiates in those with dementia, unless mod-severe pain
2 2 (delirium 1; fall + femur fracture 1)
Gallagher P and O’Mahony D. Age and Ageing. 2008;37: 673-9.
h/o=history of, PUD=peptic ulcer disease, HTN=hypertension

Dietary Supplements
• Herbals• Megavitamins• Minerals• Amino acids• Folk remedies• Lifestyle diets
$30 billion market annually
Choi J, et al. Support Care Cancer. 2009; 17: 231-40.
Dietary Supplement Health and Education Act of 1994
• Not FDA regulated• No safety or efficacy requirements• Must state product not intended to
diagnose, treat, cure, or prevent disease• General well being and benefit statements
are permitted• FDA may ban if unsafe for human
consumption
Wesa K, et al. Hematol Oncol Clin N Am. 2008; 22: 343-53.

Conditions for which CAM is Most Frequently Used
Back
pain
Head
cold
Neck
pain
Joint
pain
Arthrit
is
Anxiet
y/de
pres
sion
Stom
ach
upse
t
Heada
che
Recur
ring
pain
Inso
mnia
0
5
10
15
20
Pe
rce
nt
CAM=complementary and alternative medicineAdapted from Bruckenthal P. Pain Management Nursing. 2010; 11(2): S23-31.

Let’s Talk…
What drug/supplement interaction database(s) do you use in your practice?
a. Lexi-Comp®
b. MicroMedex®
c. Natural Medicines Comprehensive Database®
d. Other
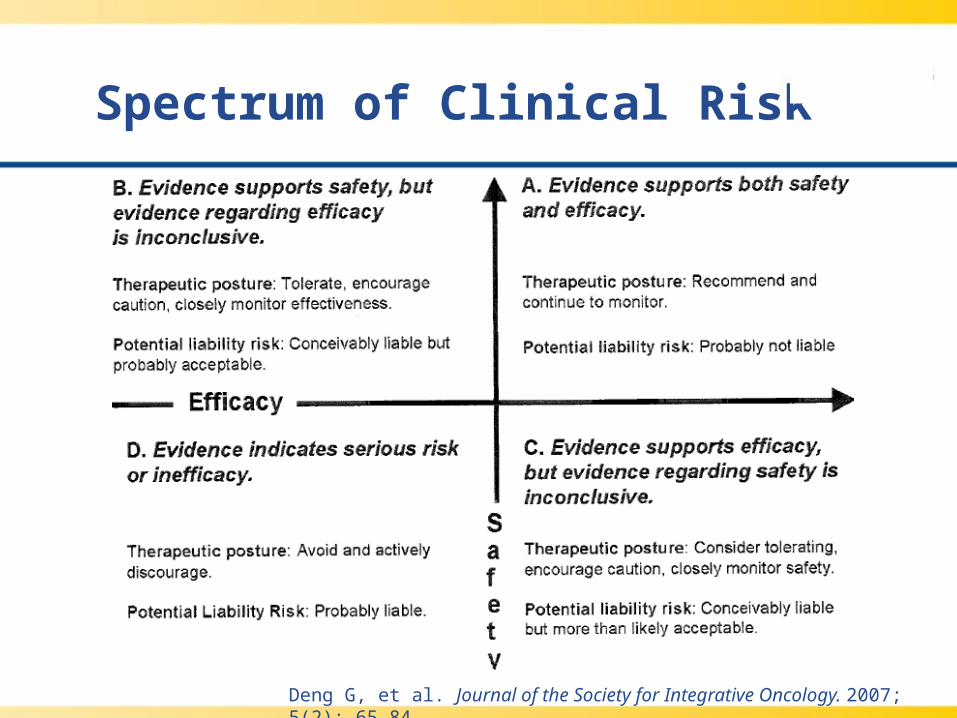
Spectrum of Clinical Risk
Deng G, et al. Journal of the Society for Integrative Oncology. 2007; 5(2): 65-84.
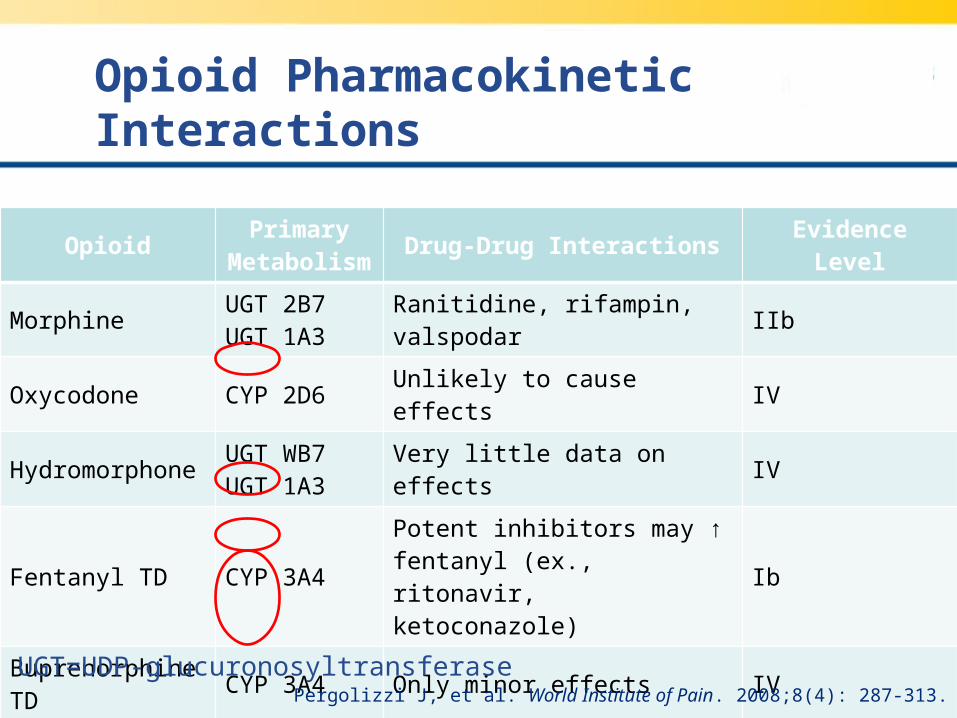
Opioid Pharmacokinetic Interactions
OpioidPrimary
MetabolismDrug-Drug Interactions Evidence Level
MorphineUGT 2B7UGT 1A3
Ranitidine, rifampin, valspodar IIb
Oxycodone CYP 2D6 Unlikely to cause effects IV
HydromorphoneUGT WB7UGT 1A3
Very little data on effects IV
Fentanyl TD CYP 3A4Potent inhibitors may ↑ fentanyl (ex., ritonavir, ketoconazole)
Ib
Buprenorphine TD CYP 3A4 Only minor effects IV
MethadoneCYP 3A4CYP 2B6CYP 2C19
Inducers and inhibitors of respective CYP enzymes
IV
Pergolizzi J, et al. World Institute of Pain. 2008;8(4): 287-313.
UGT=UDP-glucuronosyltransferase

Select CYP450 Drug Interactions
CYP3A4 CYP2D6 CYP2C9 CYP2C19
Substrate
AlfentanilHydrocodoneOxycodone
Propoxyphene
CodeineFentanylMorphine
OxycodoneTramadol
CelecoxibIbuprofen
Methadone
CarisoprodolMethadone
InhibitorClarithromycin
DiltiazemVerapamil
AmiodaronePropranololParoxetine
AmiodaroneClopidogrelFluconazole
CimetidineFluoxetine
Omeprazole
InducerRifampin
DexamethasonePhenytoin
Not inducible
AprepitantCarbamazepine
Phenytoin
Phenobarbital
GinkgoPhenytoin
CYP450 Drug Interactions. The Pharmacist’s Letter. 2009 update

Let’s Talk…
AL has been on oxycodone for chronic, severe pain for 4 months. She was recently discharged on rifampin for osteomyelitis and presents to clinic with 9/10 uncontrolled pain. Aware of a potential interaction, you suggest…
a. increasing oxycodone dose
b. rotating to morphine for duration of antibiotics
c. starting diltiazem to balance the interaction
d. adding alfentanil as a second pain agent
Let’s Talk…
AL has been on oxycodone for chronic, severe pain for 4 months. She was recently discharged on rifampin for osteomyelitis and presents to clinic with 9/10 uncontrolled pain. Aware of a potential interaction, you suggest…
a. increasing oxycodone dose
b. rotating to morphine for duration of antibiotics
c. starting diltiazem to balance the interaction
d. adding alfentanil as a second pain agent
Reasons for De-Prescribing in Geriatric Patients
• ↓ potential adverse effects• ↓ associated drug(s) costs• ↓ polypharmacy • Improved quality of life• Improved medication adherence
Lindsay J, et al. Support Care Cancer. 2014;22: 1113-9.Reeve E, et al. Int J Clin Pharm. 2014; 36: 26-9.
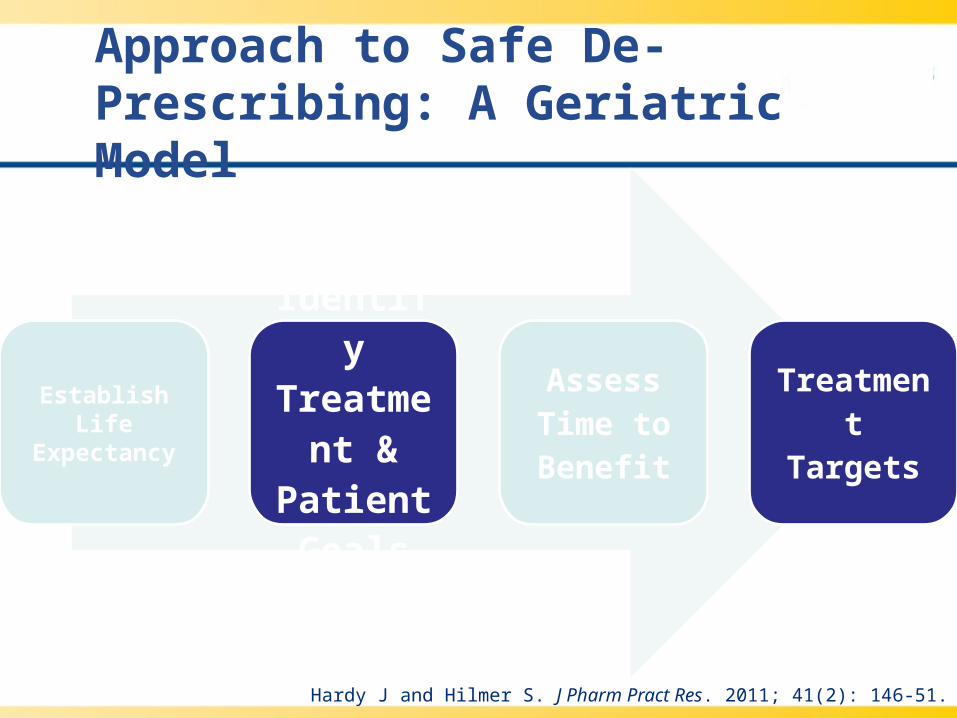
Approach to Safe De-Prescribing: A Geriatric Model
Establish Life Expectancy
Identify Treatmen
t & Patient Goals
Assess Time to Benefit
Treatment Targets
Hardy J and Hilmer S. J Pharm Pract Res. 2011; 41(2): 146-51.
Approach to Safe De-Prescribing: A Geriatric Model
AccurateMed List
Assess AdjustFollow Up and
Repeat
Hardy J and Hilmer S. J Pharm Pract Res. 2011; 41(2): 146-51.

Use Caution when De-Prescribing
Drug/Class Adverse withdrawal effect(s) Suggested action
Alpha-blockers Rebound HTN, agitation Wean gradually
Beta-blockersRebound tachycardia, palpitations, angina re-emergence
Wean gradually
Nitrates Angina re-emergence Gradual tapering
Furosemide Re-emergence of heart failure Caution if h/o heart failure
Benzodiazepines Delirium, insomnia, seizures Wean gradually
Anticholinergics Anxiety, nausea, vomiting, dizziness Wean gradually
Steroids HPA suppression if long-term use Wean gradually if long-term
Antipsychotics Dyskinesia, nausea, agitation Wean gradually
Antidepressants Dysphoric mood, agitation Wean gradually
Digoxin Re-emergence of A. fib Caution if h/o rapid A. fib
HTN=hypertension, HPA=hypothalamic-pituitary axis, A. fib=atrial fibrillation Hardy J and Hilmer S. J Pharm Pract Res. 2011; 41(2): 146-51.
Objectives
• Review how physiologic changes and altered pharmacology affect management of pain in the elderly
• Describe available tools for medication review for possible therapeutic duplication, inappropriate use, and drug interactions in the elderly
• Discuss special considerations for pharmacologic pain management in specific clinical settings in the elderly
Objectives
• Review how physiologic changes and altered pharmacology affect management of pain in the elderly
• Describe available tools for medication review for possible therapeutic duplication, inappropriate use, and drug interactions in the elderly
• Discuss special considerations for pharmacologic pain management in specific clinical settings in the elderly

Chronic-Pain vs. Addicted Patient Characteristics
Chronic-pain patients Addicted patients
Medication use is not out of control Medication use is out of control
Medication use improves quality of life Medication use impairs quality of life
Wants to decrease medication is adverse effects develop
Medication use continues or increases despite adverse effects
Is concerned about the physical problem being treated with the drug
Unaware of or in denial about any problems that develop as a result of treatment
Follows the practitioner-patient agreement for opioid use
Does not follow opioid agreement
May have leftover medication Does not have leftover medication
Loses prescriptions
Always has a story about why more drug is needed
Adapted from Webster LR and Dove B. Avoiding Opioid Abuse While Managing Pain. 2007.

Risk Assessment Tools
Tool Use Administrator Length Availability
Current Opioid Misuse Measure (COMM)
Monitor for misuse by patients currently on long-term opioid therapy
Self-report 17 items www.inflexxion.com/COMM/
Diagnosis, Intractability, Risk, Efficacy (DIRE)
Opioid addiction screening
Clinician 7 items Belgrade MJ, et al. J Pain. 2006;7:671-81.
Opioid Risk Tool (ORT)
Opioid addiction screening
Clinician or self-report
5 Y/N questions
www.opioidrisk.com/node/887
Screener and Opioid Assessment for Patients with Pain (SOAPP, -R)
Opioid addiction screening
Self-report 24 items www.inflexxion.com/SOAPP/
Chou E, et al. J Pain. 2009;10(2): 113-30.
Acetaminophen (APAP) MOA
• Centrally acting analgesic, increases pain threshold
• MOA not well understood...– Nitric oxide pathway interaction– COX-2 inhibition– Interaction with serotonergic, opioidergic, or
endocannabinoid systems• Antipyretic due to action in hypothalamus
– Vasodilation; ↑ peripheral blood circulation
Jones, V. Journal of Pain & Palliative Care Pharmacotherapy. 2011; 25: 340-9.
Oncology Drug Development
Used as an analgesic and antipyretic, acetaminophen is available in more than ____ pharmaceutical products in the US?
a) 200
b) 400
c) 600
d) 800

Oncology Drug Development
Used as an analgesic and antipyretic, acetaminophen is available in more than ____ pharmaceutical products in the US?
a) 200
b) 400
c) 600
d) 800
Pickens, L et al. Journal of Pediatric Nursing. 2011; 26: 494-7.

APAP Highlights
• Treatment of choice for osteoarthritis• Maximum daily dose usually 4 Gm
– ↓ 50-75% in those with hepatic dysfunction or h/o alcohol abuse
• As of 3/2014, all products with >325 mg per dose have discontinued marketing
American Geriatrics Society. JAGS. 2009;57: 1331-46.
IV Acetaminophen (Ofirmev®)
• Approved for mild-to-mod pain and mod-to-severe pain in combination with opioids
• 3 active comparitor studies found no significant difference in efficacy or AEs; 1 showed numerical ↓ in opioid consumption
• 2 meta-analyses showed ~20% reduced morphine requirements on post-op day 1
• Markedly more expensive than alternatives: oral or rectal acetaminophen and IV ketorolac
Remy C, et al. British Journal of Anaesthesia. 2005; 94(4): 505-13.
Elia N, et al. Anesthesiology. 2005; 103: 1296-1304.

Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
• 23.5% of elderly adverse drug event-related hospitalizations due to NSAIDs
• Non-acetylated forms (ex., salsalate) may have lower GI toxicity than aspirin
• COX-2 selective agents (ex., celecoxib) have fewer significant GI adverse events
• Concomitant administration of H2RAs or PPIs may ↓ the risk of GI ulceration
• Eradication of H. pylori ↓ NSAID-associated peptic ulcerationCOX=cyclooxygenase, H2RA=H2 receptor antagonists,
PPI=proton pump inhibitor American Geriatrics Society. JAGS. 2009;57: 1331-46.

NSAID COX-1/-2 Selectivity
Fowler T, et al. J Am Assoc Nurse Pract. 2014;26(8): 414-23.
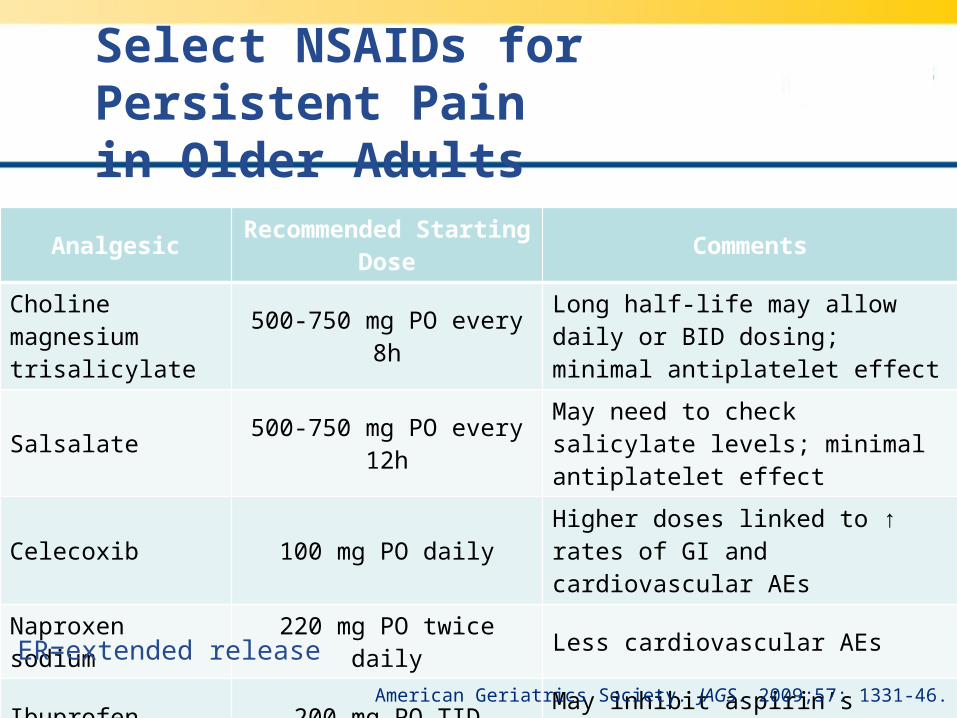
Select NSAIDs for Persistent Pain in Older Adults
AnalgesicRecommended Starting
DoseComments
Choline magnesium trisalicylate
500-750 mg PO every 8hLong half-life may allow daily or BID dosing; minimal antiplatelet effect
Salsalate 500-750 mg PO every 12hMay need to check salicylate levels; minimal antiplatelet effect
Celecoxib 100 mg PO dailyHigher doses linked to ↑ rates of GI and cardiovascular AEs
Naproxen sodium 220 mg PO twice daily Less cardiovascular AEs
Ibuprofen 200 mg PO TID May inhibit aspirin’s antiplatelet effect
Diclofenac sodium50 mg PO BID or
75 mg ER PO dailyMay see higher cardiovascular risk profile
ER=extended release
American Geriatrics Society. JAGS. 2009;57: 1331-46.

Common NSAID Adverse Events
System Adverse Event(s)
GI• Dyspepsia, abdominal pain, gastric ulcers, bleeding, perforation• ↑ risk with non-selective NSAIDs
Cardiovascular• ↑ blood pressure, myocardial infarction, congestive heart failure,
cerebrovascular accident• ↑ risk with COX-2 selective NSAIDs
Hematologic • ↑ risk for bleeding and anemia
Renal• Water and sodium retention, ↓ renal blood flow, electrolyte
imbalances, prerenal azotemia, hyporeninemic hypoaldosteronism
Hepatic • ↑ transaminases, hepatitis
Fowler T, et al. J Am Assoc Nurse Pract. 2014;26(8): 414-23.
Patient Case Question
PD is a 60 yo female with OA of her right knee and a PMH of mod liver dysfunction and controlled HTN. She has been taking ibuprofen (IBU) 600 mg PO TID for 4 weeks with good relief, but her BP today is 187/92 mmHg. The best option for continued treatment of her OA is…?
a) APAP 1 Gm PO QID
b) Continue with current IBU schedule
c) Celecoxib 200 mg PO daily
d) Diclofenac gel 4 Gm TOP QID

Patient Case Question
PD is a 60 yo female with OA of her right knee and a PMH of mod liver dysfunction and controlled HTN. She has been taking ibuprofen (IBU) 600 mg PO TID for 4 weeks with good relief, but her BP today is 187/92 mmHg. The best option for continued treatment of her OA is…?
a) APAP 1 Gm PO QID
b) Continue with current IBU schedule
c) Celecoxib 200 mg PO daily
d) Diclofenac gel 4 Gm TOP QID

Short-Acting Opioid Highlights
• μ-opioid receptor agonism (primary)• No ceiling effect and have been shown to
relieve all types of pain• Every patient should be prescribed a bowel
regimen to prevent constipation• Long-term therapy associated with hormonal
suppression• Scheduled administration before anticipated
pain episode(s) may be appropriate in patients with cognitive impairmentArnstein P. Pain Management Nursing. 2010;11(2); S11-22.

Available at www.practicalpainmanagement.com. Accessed on 2.15.15.

Opioid-Induced Immunosuppression
Opioid Animals Humans Evidence Level
Morphine ++++ ++++ Ia/b
Oxycodone (--) ND IIa
Hydromorphone (--) ND IIa
Fentanyl ++++ ++++ Ib
Buprenorphine (--) ND Ib
Methadone ? ND IIb
Pergolizzi J, et al. World Institute of Pain. 2008;8(4): 287-313.
++++=high degree of immunosuppression, (--)=not immunosuppressive, ?=data inconclusive, ND= not determined
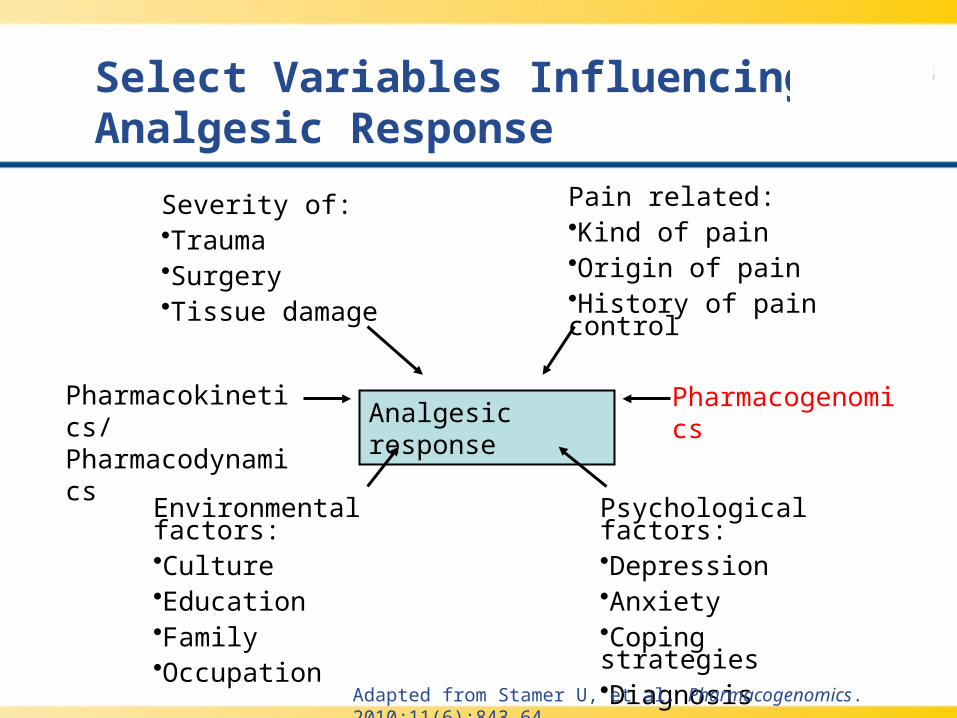
Select Variables Influencing Analgesic Response
Pharmacokinetics/ Pharmacodynamics Analgesic response
Pharmacogenomics
Pain related:•Kind of pain•Origin of pain•History of pain control
Environmental factors:•Culture•Education•Family•Occupation
Psychological factors:•Depression•Anxiety•Coping strategies•Diagnosis
Severity of:•Trauma•Surgery•Tissue damage
Adapted from Stamer U, et al. Pharmacogenomics. 2010;11(6):843-64.

Pharmacogenomic Targets
Gene Variant Opioids Affected Outcome(s)
CYP2D6Poor;
ultra rapid metabolizers
Codeine, Tramadol, Oxycodone
↓ analgesia; excessive side effects
ABCB1 3435C > T MorphineTT carriers experience
greater pain relief
OPRM1 118A > GMorphine, Alfentanil, Fentanyl, Methadone
↑ dose requirements due to ↓ efficacy
COMT 1947G > A MorphineGG carriers
experience less pain relief
Jannetto P and Bratanow N. Expert Opin Drug Metab Toxicol. 2011; 7(6): 745-52.

Pertinent LA Opioid Prescribing Information for Elderly Patients
Avinza® Morphine sulfate ER: 30-, 45-, 60-, 75-, 90-, and 120 mg capsules
Dosing interval Once a day
Dosing highlights • Titrate using a minimum of 3-day intervals• May open capsule and sprinkle pellets on applesauce; do not
chew; use immediately• Max daily dose: 1600 mg due to renal toxicity risk of fumaric acid
Drug interactions • Alcohol may result in rapid release of a potentially fatal dose• PGP inhibitors may ↑ absorption by about two-fold
Butrans® Buprenorphine TD: 5-, 10- and 20 mcg/hr
Dosing interval One transdermal system every 7 days
Dosing highlights • Initial dose in mild to moderate hepatic dysfunction: 5 mcg/hr• Maximum dose of 20 mcg/hr due to risk of QTc prolongation
Drug interactions • CYP3A4 inhibitors may ↑ levels; CYP3A4 inducers may ↓ levels• Class Ia and III antiarrhythmics may ↑ risk of QTc prolongation
LA= long-acting, PGP=P-glycoproteinLexicomp®: Avinza and Butrans monographs. Accessed on 2.17.15.
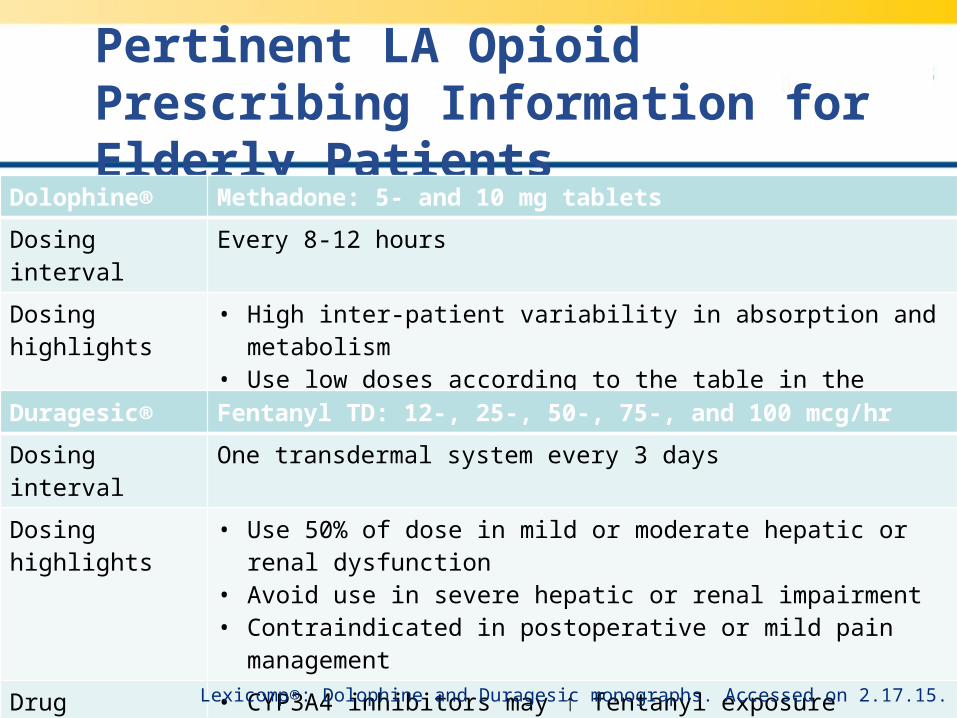
Pertinent LA Opioid Prescribing Information for Elderly Patients
Dolophine® Methadone: 5- and 10 mg tablets
Dosing interval Every 8-12 hours
Dosing highlights • High inter-patient variability in absorption and metabolism• Use low doses according to the table in the package insert
Drug interactions • CYP450 inducers may ↑ levels; CYP450 inhibitors may ↓ levels• Potentially arrhythmogenic agents may ↑ risk of QTc prolongation
Duragesic® Fentanyl TD: 12-, 25-, 50-, 75-, and 100 mcg/hr
Dosing interval One transdermal system every 3 days
Dosing highlights • Use 50% of dose in mild or moderate hepatic or renal dysfunction• Avoid use in severe hepatic or renal impairment• Contraindicated in postoperative or mild pain management
Drug interactions • CYP3A4 inhibitors may ↑ fentanyl exposure• CYP3A4 inducers may ↓ fentanyl exposure
Lexicomp®: Dolophine and Duragesic monographs. Accessed on 2.17.15.
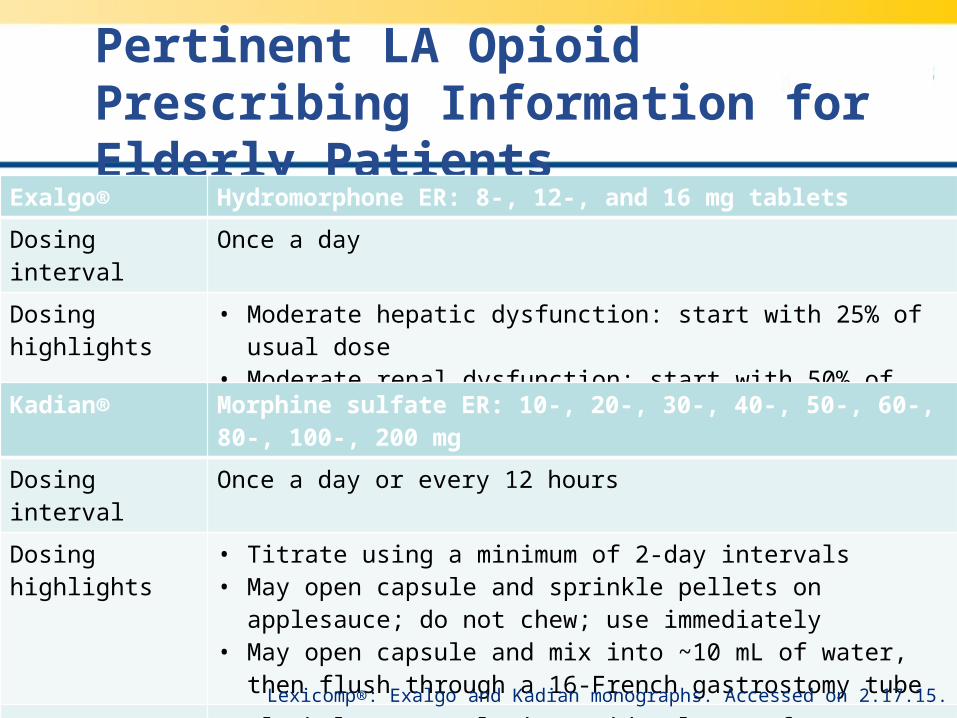
Pertinent LA Opioid Prescribing Information for Elderly Patients
Exalgo® Hydromorphone ER: 8-, 12-, and 16 mg tablets
Dosing interval Once a day
Dosing highlights • Moderate hepatic dysfunction: start with 25% of usual dose• Moderate renal dysfunction: start with 50% of usual dose• Must be able to swallow tablets whole
Drug interactions • Do not use in patients with a sulfa allergy (sodium metabisulfite)
Kadian® Morphine sulfate ER: 10-, 20-, 30-, 40-, 50-, 60-, 80-, 100-, 200 mg
Dosing interval Once a day or every 12 hours
Dosing highlights • Titrate using a minimum of 2-day intervals• May open capsule and sprinkle pellets on applesauce; do not
chew; use immediately• May open capsule and mix into ~10 mL of water, then flush
through a 16-French gastrostomy tube
Drug interactions • Alcohol may result in rapid release of a potentially fatal dose• PGP inhibitors may ↑ absorption by about two-fold
Lexicomp®: Exalgo and Kadian monographs. Accessed on 2.17.15.
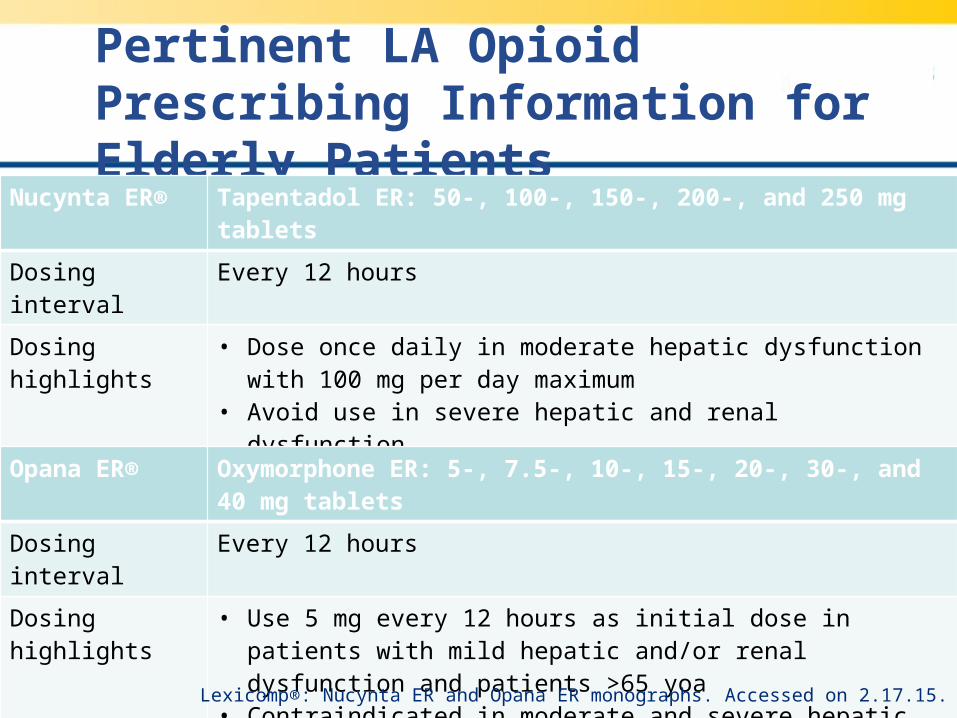
Pertinent LA Opioid Prescribing Information for Elderly Patients
Nucynta ER® Tapentadol ER: 50-, 100-, 150-, 200-, and 250 mg tablets
Dosing interval Every 12 hours
Dosing highlights • Dose once daily in moderate hepatic dysfunction with 100 mg per day maximum
• Avoid use in severe hepatic and renal dysfunction• Serotonin syndrome has been described
Drug interactions • Alcohol may result in rapid release of a potentially fatal dose• Contraindicated in patients taking MAOIs
Opana ER® Oxymorphone ER: 5-, 7.5-, 10-, 15-, 20-, 30-, and 40 mg tablets
Dosing interval Every 12 hours
Dosing highlights • Use 5 mg every 12 hours as initial dose in patients with mild hepatic and/or renal dysfunction and patients >65 yoa
• Contraindicated in moderate and severe hepatic dysfunction
Drug interactions • Alcohol may result in rapid release of a potentially fatal dose
Lexicomp®: Nucynta ER and Opana ER monographs. Accessed on 2.17.15.

Pertinent LA Opioid Prescribing Information for Elderly Patients
OxyContin® Oxycodone CR: 10-, 15-, 20-, 30-, 40-, 60-, and 80 mg tablets
Dosing interval Every 12 hours
Dosing highlights • Hepatic dysfunction: start with 30-50% of usual dose• Renal dysfunction (CrCl <60 mL/min): start with 50% of usual
dose• Consider using other analgesics in patients with GI disorders that
may predispose them to obstruction
Drug interactions • CYP3A4 inhibitors may ↑ oxycodone exposure• CYP3A4 inducers may ↓ oxycodone exposure
Lexicomp®: Oxycodone monograph. Accessed on 2.17.15.CR=controlled release

Healthcare System Opioid Barriers
• Lack of a neighborhood pharmacy• Transportation issues• Absence of high dose opioid at pharmacy• No caregiver to help with drug preparation
and/or administration• Negative attitudes toward patients needing
opioid therapy
Zuccaro S, et al. Clin Drug Investig. 2012;32(1): S11-9.

Select Adjuvant Pain Agents
Agent(s)Recommended Starting
DoseComments
Desipramine, nortriptyline, amitriptyline
10 mg PO at bedtimeSignificant risk of AEs (anticholinergic and cardiovascular) in older patients
Duloxetine 20 mg PO daily Monitor BP, dizziness, and cognitive effects
Milnacipran12.5 mg PO daily; titrate to
50 mg PO BID↓ dose 50% if CrCl <30 mL/min; do not use with narrow angle glaucoma
Gabapentin 100 mg PO at bedtime Monitor sedation, ataxia, edema
Baclofen 5 mg PO up to TIDMonitor urinary function, cognitive effects, sedation; avoid abrupt discontinuation
Tramadol 12.5-25 mg PO every 4-6hMixed opioid, serotonin- and norepinephrine-reuptake inhibitor; monitor opioid AEs, seizures, serotonin syndrome
Tapentadol 50 mg PO every 4-6h Trials suggest ↓ GI AEs relative to opioids
American Geriatrics Society. JAGS. 2009;57: 1331-46.
Non-Pharmacologic Management
• Massage: ↓ pain, improves circulation, ↓ anxiety, ↑ joint mobility
• Exercise: moderate intensity, ≥30 min 3-4 times per week
• Chiropractic: rule out spinal cord injury or nerve root involvement prior to start
• Transcutaneous electrical nerve stimulation• Patient education
Norelli L and Harju S. Clin Geriatr Med. 2008;24(2): 335-44.

Non-Pharmacologic Management
• Relaxation: repetitive focus on sound, sensation, muscle tension, inattention towards intrusive thoughts; requires individual acceptance and training
• Meditation: guided or self-directed, allows conscious awareness of thoughts, emotions, and sensations without judgment
• Hypnosis: state of inner absorption and focused attention; reduces pain by distraction, altered perception, and ↑ pain threshold
Norelli L and Harju S. Clin Geriatr Med. 2008;24(2): 335-44.

Non-Pharmacologic Management
• Cognitive-behavioral therapy: focuses on changing individual cognitive activity to modify associated behavior, thoughts, and emotions; conducted by trained therapist
• Operant behavior therapy: use of negative and positive consequences to modify behavior
• Mind-body conditioning: Yoga, tai chi, qigong
Norelli L and Harju S. Clin Geriatr Med. 2008;24(2): 335-44.

Future of Pain Management
• Non-traditional analgesics– Targeted gene therapy
• Vectors deliver enkephalins to sensory nerves
– Spicamycin derivative• Non-opioid acetylcholinesterase inhibitor
– Tetrodotoxin derivative• Non-peptide, non-opioid neurotoxin
– Cytokine and nerve growth factor inhibitors
Available at www.clinicaltrials.gov. Accessed on 2.28.15.

Parting Pearls
• Identify applicable age-related pharmacologic changes
• Conduct a prospective review for drug-drug/-herbal interactions before a prescription is written
• Remember PIMs to avoid and errors of omission• Prescribe non-opioids, where appropriate• Begin therapy with the lowest possible dose and
increase slowly• Consider the need for preventive, concurrent
medications• Discuss role of non-pharmacologic management

Pharmacologic Pain Management for the Older Adult
Leigh M. Boehmer, Pharm.D., BCOPClinical Pharmacist, Medical OncologyBarnes Jewish HospitalApril 11, 2015