permanent secretary visits rbhsc · 2015-03-27 · permanent secretary visits rbhsc dr stephen...
TRANSCRIPT

Issue ThreeMarch 2015
Permanent Secretary visits RBHSC
Dr Stephen Mullen, Registrar, Karin Jackson, Co-director, Richard Pengelly, Permanent Secretary, Dr Brigitte Bartholome, Lead Consultant, RBHSC ED, Amanda McCallum, ED Staff Nurse
Brigitte Bartholome, Lead Children’s Consultant, highlights the team effort involved in ensuring 33,000 children and young people are seen each year and discharged/admitted within a maximum of four hours. Delivery on this standard has risen from 78% in 2012/13 to 89% in 13/14 and 90% in 14/15 for all attendances. Brigitte said, ‘The opening of our short stay assessment unit has improved patient flow both in ED and throughout the hospital.We review the reasons patients are delayed and address any issues as a team.’
Discharge Group
An additional ImPACT Workstream has been established to lead improvements in in-patient discharge and co-ordinate the implementation of the RQIA Review of Discharge Arrangements, as part of the ImPACT drive to reduce harm, waste and variation. The Discharge Workstream is chaired by Dr John Craig. As part of this group there is a working group comprising of 12 individual MDT projects. These projects are concentrating on the non-complex discharge and the barriers to efficient discharge processes within each of the individual areas.
The specialties and wards involved are: Acute Med/Respiratory (Mater); BCH Direct & Older People Services, Oncology (BCH); and Trauma & Orthopaedics, AMU, Surgery/EmSU, Respiratory, Hepatology, Infectious Diseases, Endocrine and Vascular, all at RVH.A series of workshops have taken place, which have been very well attended by the multi-disciplinary teams from all specialties and a number of agreed project teams have been created, for example:
• AMU are building on the ‘Big Hand’ Project. This uses wireless technology to generate the patient discharge letter during the clinical ward round, thereby preventing batching and ensuring accuracy of content.
• The Mater team are focused on nurse-facilitated discharge, reviewing the requirement of a discharge lounge and determining the practicality of ensuring blood results are available to inform the morning clinical ward rounds.
• Surgery EmSU are launching their operational protocol, designed to ensure the positive progress on LOS is matched by discharge pathway improvements to minimise delay for patients.The enthusiastic involvement of all the participants has been demonstrated by the range of projects underway.
RBHSC 4hr performance
4hr Target
RVH 4hr Performance
MIH 4hr Performance
RBHSC 12hr Performance
40%
50%
60%
70%
80%
90%
100%
Perc
enta
ge o
f pat
ient
s se
en a
nd d
isch
arge
d fro
m E
D w
ithin
4hr
s
Month
RBHSC, MIH and RVH ED | 4hr Compliance | Jan 2012 to Feb 2015Percentage of patients seen and discharged from RBHSC, MIH and RVH ED within 4 hours from arrival

A second escalation table top exercise took place in early December, which highlighted good specialty co-ordination, leadership and communication across all services. Following the workshop,the escalation plan was submitted to HSCB. Specialty contingency plans for Christmas/New Year were finalised and implemented over the holiday period.
The first few months of 2015 have been particularly testing regionally. The trust escalation plan has been utilised on many occasions with a review of Elective and Urgent planned admissions. Both RVH and Mater ED’s ability to sustain an improved 12 and 4 hour performance has dipped during this period as it has in other Trusts.
Both HSCB and the Permanent Secretary recognised the significant efforts of clinical and managerial teams in sustaining a quality service at a time when patient activity increased by 6-7%. In Belfast Trust when the BCH unscheduled pathways are also considered this is equivalent to 50 more admissions per week or 7 per day.
The Fractures Team, working alongside the Flow & Take Workstream have demonstrated how additional operating capacity for patients with a fractured Neck of Femur has delivered a significant improvement in patient care and in waiting times for operations. This has improved the patient experience and the overall performance of the fracture unit at the RVH.
The barchart shows that the percentage of fractured neck of Femurs operated on in 48hrs (where the patient is fit for surgery) has increased to 100% in Jan 2015 (slight reduction in February). This was the best outcome the Trust has ever delivered against the DoH target (95% of fractured neck of femurs should be operated on in 48hrs).
Significant improvement in overall performance of fracture unit
Trust Escalation Plan

Discharge Expectations by Hospital
Royal Victoria Hospital
Day Accident and Emergency
General Medicine
Cardiology Cardiac Surgery
Burns Colorectal Ear, Nose & Throat
Monday 8 19 12 3 2 1 5Tuesday 7 17 15 3 1 1 8Wednesday 8 17 15 4 1 1 6Thursday 6 16 13 3 1 1 10Friday 8 20 16 3 1 1 5Saturday 6 14 6 2 1 1 4Sunday 7 12 5 2 1 1 2
Day Endocrinology Fracture Gastroenter-ology
General Surgery Geriatric Medicine
Hepatology (Liver)
Infectious Diseases
Monday 2 10 4 12 1 3 2Tuesday 4 11 5 14 2 4 1Wednesday 3 12 5 13 1 4 1Thursday 3 9 4 14 1 4 1Friday 2 10 5 12 1 4 1Saturday 2 7 4 11 1 2 1Sunday 2 7 3 9 1 2 1
Day Neurology Neurosurgery Neurovascular Ophthalmology Orthopaedics Plastic Surgery Thoracic Medicine
Monday 3 4 4 2 1 2 11Tuesday 3 4 3 3 1 1 11Wednesday 3 4 4 3 1 1 9Thursday 3 5 5 4 1 1 8Friday 3 5 4 4 1 1 9Saturday 2 3 2 3 2 1 5Sunday 2 2 2 1 1 1 5
Day Thoracic Surgery
Vascular Surgery
Total
Monday 3 4 116Tuesday 4 3 125Wednesday 4 5 127Thursday 4 4 121Friday 3 4 124Saturday 2 2 83Sunday 2 4 74
Day GeriatricsMonday 5Tuesday 4Wednesday 4Thursday 5Friday 4Saturday 3Sunday 5
Musgrave Park Hospital
Nursing teams in all wards across the four sites have been updating their wards activity data on a daily basis. This has generated a valuable resource of information that has helped us understand how many patients no longer require acute inpatient care and therefore we need to efficiently facilitate their discharge so that we can ensure we have adequate capacity for patients awaiting admission. A breakdown of this data per specialty is presented below.
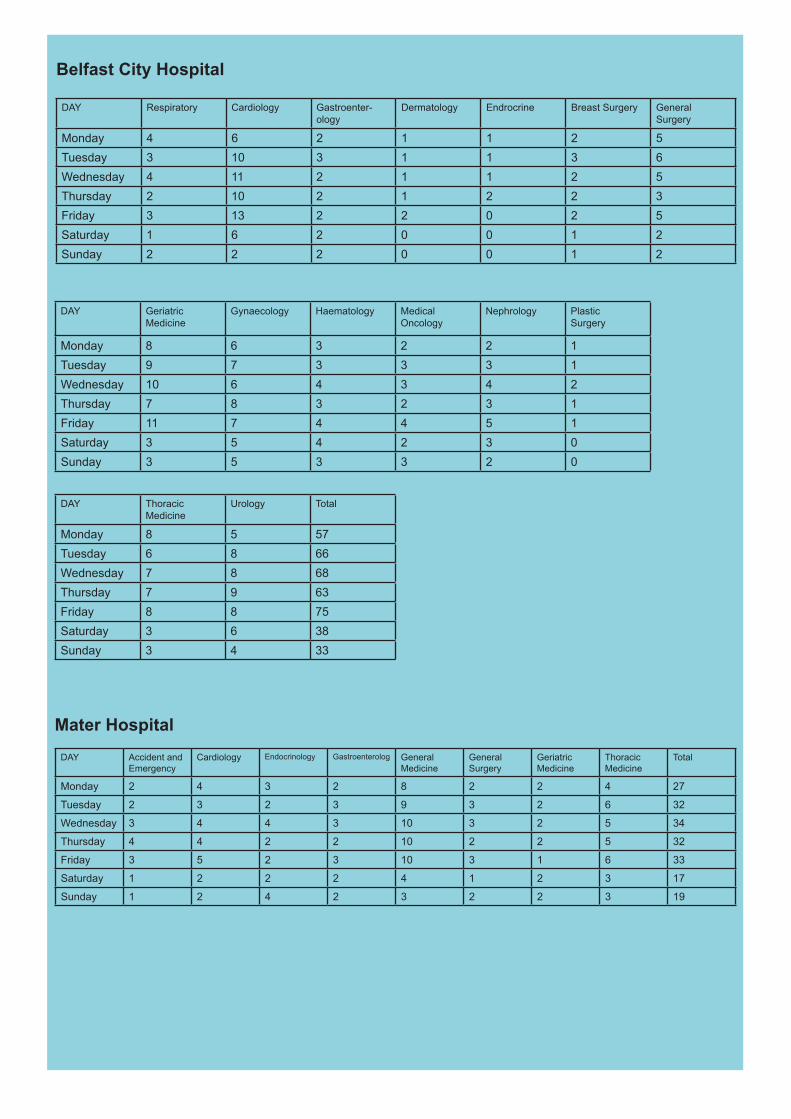
DAY Respiratory Cardiology Gastroenter-ology
Dermatology Endrocrine Breast Surgery General Surgery
Monday 4 6 2 1 1 2 5Tuesday 3 10 3 1 1 3 6Wednesday 4 11 2 1 1 2 5Thursday 2 10 2 1 2 2 3Friday 3 13 2 2 0 2 5Saturday 1 6 2 0 0 1 2Sunday 2 2 2 0 0 1 2
DAY Geriatric Medicine
Gynaecology Haematology Medical Oncology
Nephrology Plastic Surgery
Monday 8 6 3 2 2 1Tuesday 9 7 3 3 3 1Wednesday 10 6 4 3 4 2Thursday 7 8 3 2 3 1Friday 11 7 4 4 5 1Saturday 3 5 4 2 3 0Sunday 3 5 3 3 2 0
DAY Thoracic Medicine
Urology Total
Monday 8 5 57Tuesday 6 8 66Wednesday 7 8 68Thursday 7 9 63Friday 8 8 75Saturday 3 6 38Sunday 3 4 33
Belfast City Hospital
DAY Accident and Emergency
Cardiology Endocrinology Gastroenterolog General Medicine
General Surgery
Geriatric Medicine
Thoracic Medicine
Total
Monday 2 4 3 2 8 2 2 4 27
Tuesday 2 3 2 3 9 3 2 6 32
Wednesday 3 4 4 3 10 3 2 5 34
Thursday 4 4 2 2 10 2 2 5 32
Friday 3 5 2 3 10 3 1 6 33
Saturday 1 2 2 2 4 1 2 3 17
Sunday 1 2 4 2 3 2 2 3 19
Mater Hospital
Message from Dr Cathy Jack ImPACT Chair
The winter period continues to be challenging for everyone working in healthcare. We treat 200 more patients a month. This puts additional pressure on the system and at times we have had to open theatre recovery and some day wards. Many of our staff have come in while off duty to help out and do extra shifts or doubled up on call rotas to ensure patients received a daily consultant review.
It is a privilege to work alongside and support the staff recognising that this is one of the most challenging times of the year.
It is also important to reflect on the improvements that within six months of ImPACT have already been achieved despite the additional workload:
1 100% of patients with a fracture of neck of femur are being treated within the NICE guidance.
2 Weekend discharges have increased with five of the ten large unscheduled care specialties discharging more patients at the weekend compared with only one in September 2014.
3 Length of stay has fallen in respiratory and general surgery reflecting changing approaches to unscheduled care.
Looking forward to spring and summer it has been recognised that work needs to start on the elective care process. More information will be provided about this in next months update!
Finally I would like to pay tribute to all our fantastic staff who have worked so hard over these winter months to ensure that patients receive ongoing quality, safe and effective care.
Thanks to all of you
Cathy Jack