perioperative evaluation and treatment of the cardiac patient undergoing noncardiac surgery
TRANSCRIPT

Perioperative Evaluation and Perioperative Evaluation and Treatment of the Cardiac Treatment of the Cardiac
Patient Undergoing Noncardiac Patient Undergoing Noncardiac SurgerySurgery
Perioperative MIPerioperative MIScope of the ProblemScope of the Problem
• 27 M noncardiac operations/year27 M noncardiac operations/year
• 8 M with known CAD or risk 8 M with known CAD or risk
factorsfactors
• CAD leading cause of nonsurgical CAD leading cause of nonsurgical
postoperative deathpostoperative death

Perioperative MIPerioperative MIScope of the ProblemScope of the Problem
• 50,000 perioperative MI (~0.2% of 50,000 perioperative MI (~0.2% of
surgeries)surgeries)
• 30-50% mortality with MI30-50% mortality with MI
• 1 M cardiac complications (~4%) 1 M cardiac complications (~4%)
• $20 billion added cost to surgery$20 billion added cost to surgery

Perioperative MIPerioperative MIMechanismsMechanisms
• Unstable plaqueUnstable plaque
• CatecholaminesCatecholamines– painpain
– anemiaanemia
• BP swingsBP swings– painpain
– anemia/hypovolemiaanemia/hypovolemia
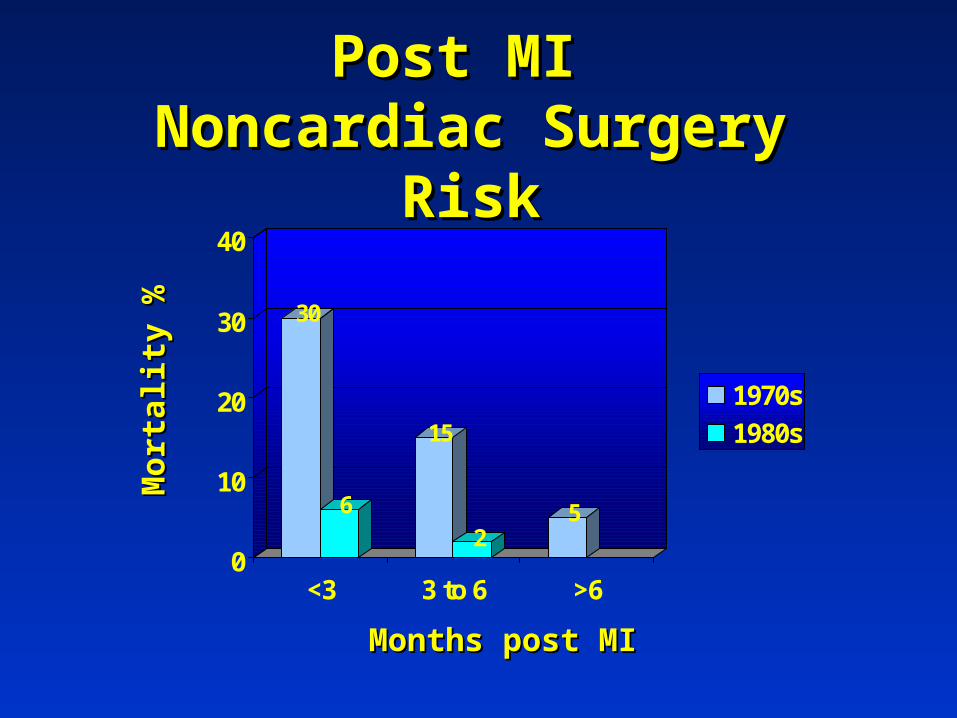
Post MI Post MI Noncardiac Surgery RiskNoncardiac Surgery Risk
30
6
15
25
0
10
20
30
40
<3 3 to 6 >6
1970s
1980s
Months post MIMonths post MI
Mor
tali
ty %
Mor
tali
ty %

Goldman CriteriaGoldman Criteria
• Recent MI (<6 mos)Recent MI (<6 mos)• Unstable anginaUnstable angina• CHFCHF• Abdominal or Abdominal or
thoracic surgerythoracic surgery• Severe ASSevere AS• Emergent surgeryEmergent surgery
• Age >70Age >70• Rhythm other than Rhythm other than
sinussinus
• SS33
• Other Other medical/metabolic medical/metabolic problemsproblems

Cardiac Risk Stratification Cardiac Risk Stratification ProposalsProposals
• GoldmanGoldman
• DetskyDetsky
• EagleEagle
• ASAASA

Revised Cardiac Risk IndexRevised Cardiac Risk IndexIndependent PredictorsIndependent Predictors
Lee et al. Circ 1999;100:1043.Lee et al. Circ 1999;100:1043.
• High risk surgeryHigh risk surgery
• History of ischemic heart diseaseHistory of ischemic heart disease
• History of CHFHistory of CHF
• History of CVAHistory of CVA
• Diabetes requiring insulinDiabetes requiring insulin
• Cr>2.0 mg/dlCr>2.0 mg/dl

Revised Cardiac Risk IndexRevised Cardiac Risk IndexLee et al. Circ 1999;100:1043.Lee et al. Circ 1999;100:1043.
0
0.2
0.4
0.6
0.8
1
Sen
siti
vit
y Goldman (0.70)
Detsky (0.58)
ASA (0.71)Revised (0.81)
Specificity
11 00.5
ROC CurvesValidation Set, n=1422

Revised Cardiac Risk IndexRevised Cardiac Risk Index
0.51.2
5
9.6
0
2
4
6
8
10
%
0 1 2 >2
Risk Factors
Major Cardiac Complications* (n=4315)
Lee et al. Circ 1999;100:1043.Lee et al. Circ 1999;100:1043.
*Cardiac death, MI, pulmonary edema, arrhythmic arrest, heart block

Revised Cardiac Risk IndexRevised Cardiac Risk IndexLee et al. Circ 1999;100:1043.Lee et al. Circ 1999;100:1043.
0
2
4
6
8
10
12
14
%
Other* Other Vascular AAA
Mortality By Surgical Type
012>2
Number ofRisk Factors
* Thoracic, Abdominal, Orthopedic, etc.

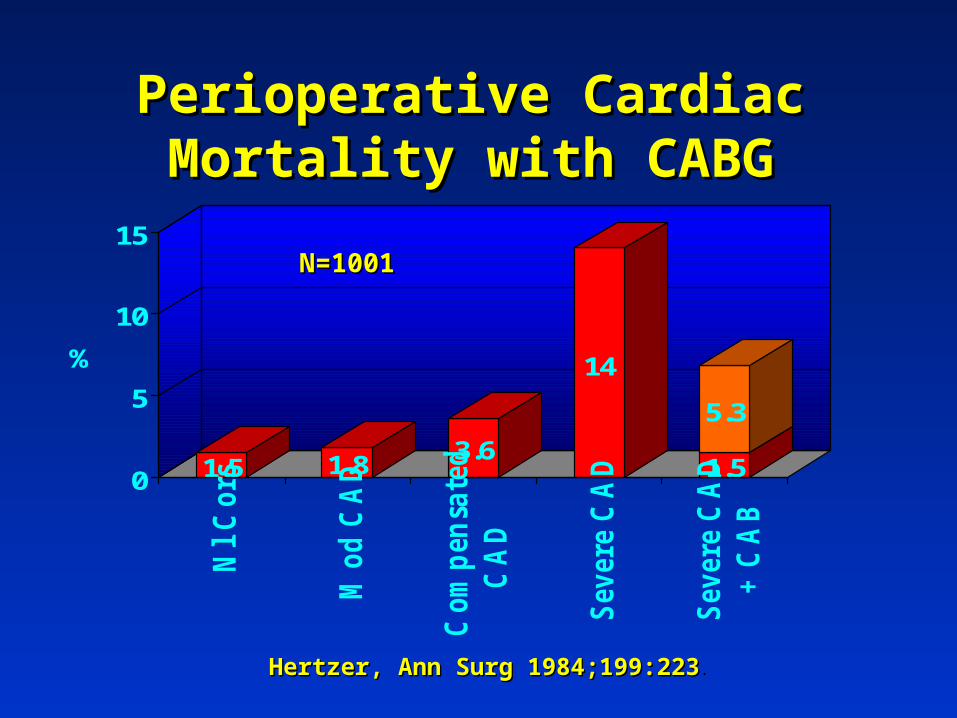
Perioperative Cardiac Mortality Perioperative Cardiac Mortality with CABGwith CABG
1.5 1.83.6
14
1.5
5.3
0
5
10
15
%
Nl
Co
rs
Mo
d C
AD
Co
mp
en
sate
d
CA
D
Sev
ere
CA
D
Sev
ere
CA
D
+ C
AB
Hertzer, Ann Surg 1984;199:223Hertzer, Ann Surg 1984;199:223.
N=1001N=1001

Preoperative TestingPreoperative TestingPositive Predictive ValuePositive Predictive Value
18.6
13.114.8
0
5
10
15
20
%
Stress ECG Dipyramidamole Tl Dobutamine Echo
MI or DeathMI or Death
Eagle et al. JACC 1996;27:910.

Preoperative TestingPreoperative TestingNegative Predictive ValueNegative Predictive Value
96.3
98.699.4
80
85
90
95
100
%
Stress ECG Dipyramadole Tl Dobutamine Echo
Freedom from MI or DeathFreedom from MI or Death
Eagle et al. JACC 1996;27:910.Eagle et al. JACC 1996;27:910.

Functional CapacityFunctional Capacity Metabolic Equivalents (METs)Metabolic Equivalents (METs)
• Low (< 4 METs)Low (< 4 METs)
– increased surgical riskincreased surgical risk
• Intermediate (4-10 METs)Intermediate (4-10 METs)
• Excellent (> 10 METs)Excellent (> 10 METs)
EatingEatingDressingDressingWalking around the houseWalking around the houseDishwashingDishwashing

Postoperative MortalityPostoperative MortalityPreoperative HemoglobinPreoperative Hemoglobin
0
5
10
15
20
6 7 8 9 10 11 12
Hemoglobin g/dl
Adj
uste
d O
dds
Rat
io
CVDNo CVD
Carson et al. Lancet 1996;348:1055.
Perioperative Cardiac Mortality Perioperative Cardiac Mortality with CABGwith CABG
1.5 1.83.6
14
1.5
5.3
0
5
10
15
%
Nl
Co
rs
Mo
d C
AD
Co
mp
en
sate
d
CA
D
Sev
ere
CA
D
Sev
ere
CA
D
+ C
AB
Hertzer, Ann Surg 1984;199:223Hertzer, Ann Surg 1984;199:223.
N=1001N=1001

Proven Indications for CABGProven Indications for CABG
• Significant left main diseaseSignificant left main disease
• 3 V CAD and LV dysfunction3 V CAD and LV dysfunction
• 2 V CAD with proximal LAD 2 V CAD with proximal LAD
involvementinvolvement
• Intractable ischemiaIntractable ischemia

Perioperative Cardiac Events Perioperative Cardiac Events with PTCAwith PTCAVascular PatientsVascular Patients
0.6 38
18
34
2.45
0
10
20
30
40-
Dob
Ech
o
Low
Ris
k
Inte
rmed
.R
isk Hig
hR
isk
+ D
obE
cho
Pos
tP
TC
A
Khot UN, Ellis SG. ACC Current J Rev 2001;10:57.Khot UN, Ellis SG. ACC Current J Rev 2001;10:57.
% D
eath
an
d N
onfa
tal M
I

PROBLEMS WITH PREOP PROBLEMS WITH PREOP CORONARY CORONARY
INTERVENTIONSINTERVENTIONSNo proven benefitNo proven benefit
May not treat the “culprit”May not treat the “culprit”
Delays surgery versus higher coronary riskDelays surgery versus higher coronary risk
PTCA : only few days but higher PTCA : only few days but higher restenosis riskrestenosis risk
Stent : two to six weeksStent : two to six weeks

Postoperative Mortality ReductionPostoperative Mortality ReductionBeta-BlockersBeta-Blockers
8
14
21
0
3
10
0
5
10
15
20
25
Placebo Atenolol
6 Months1 Year2 Years
Mangano, et al. NEMJ 1996;335:1713.

Postoperative Cardiac Events Postoperative Cardiac Events In In High Risk PatientsHigh Risk Patients
17 17
3.4
00
5
10
15
20
25
%
Placebo Bisoprolol
Beta-Blockade
Cardiac DeathNon-fatal MI
Bisoprolol n=59Placebo n=53
Poldermans et al. NEJM 1999;341:1789.Poldermans et al. NEJM 1999;341:1789.

BETA-BLOCKERSBETA-BLOCKERSUNKNOWN FACTORSUNKNOWN FACTORS
What is the optimal dose?What is the optimal dose?How frequent are complications?How frequent are complications?Who should receive therapy?Who should receive therapy?Are all beta blockers effective?Are all beta blockers effective?When should they be started?When should they be started?How long should they be used?How long should they be used?Are Alpha-Blockers also effective?Are Alpha-Blockers also effective?

Statin Use and Perioperative DeathStatin Use and Perioperative Death
• Patients: PV surgery 1991-2000Patients: PV surgery 1991-2000• Study Type: retrospective case-controlled Study Type: retrospective case-controlled
– 160 deaths (5.6% of total) 160 deaths (5.6% of total) – 2:1 survivors: non-survivors 2:1 survivors: non-survivors
• Vascular death: 104 (65% cases)Vascular death: 104 (65% cases)• Statin use: Statin use:
– 8% cases vs 25% controls (p<0.001)8% cases vs 25% controls (p<0.001)– odds ratio 0.22, (95% CI 0.10-0.47)odds ratio 0.22, (95% CI 0.10-0.47)
Poldermans et al. Circ 2003;107:1848.Poldermans et al. Circ 2003;107:1848.


Minor Clinical PredictorsMinor Clinical Predictors
• Advanced ageAdvanced age
• Abnormal ECGAbnormal ECG
• Rhythm other than sinusRhythm other than sinus
• History of CVAHistory of CVA
• Uncontrolled HTNUncontrolled HTN





In-Hospital MortalityIn-Hospital MortalityPerioperative PA CatheterPerioperative PA Catheter
1994 Randomized High Risk Surgical Patients1994 Randomized High Risk Surgical Patients
OverallOverall
NYHANYHA I or III or II III or IVIII or IV
% Difference% Difference00 +10+10-10-10
Favors PA Catheter Favors Standard CareFavors PA Catheter Favors Standard Care
Sandham et al. NEJM 2003;348:5.Sandham et al. NEJM 2003;348:5.

Major Clinical Predictors Major Clinical Predictors
• Acute or recent MI (< one month)Acute or recent MI (< one month)
• Unstable or severe anginaUnstable or severe angina
• Large ischemic burden (stress testing)Large ischemic burden (stress testing)
• Decompensated CHFDecompensated CHF
• Significant arrhythmiasSignificant arrhythmias

Intermediate Clinical Intermediate Clinical PredictorsPredictors
• Remote MI ( >1 month)Remote MI ( >1 month)
• Stable anginaStable angina
• Compensated CHFCompensated CHF
• Creatinine Creatinine 2.0 2.0
• DiabetesDiabetes

Surgery Specific RiskSurgery Specific RiskHigh (>5% Mortality)High (>5% Mortality)
• Emergent (esp. in the elderly)Emergent (esp. in the elderly)
• AorticAortic
• Peripheral vascularPeripheral vascular

Surgery Specific RiskSurgery Specific RiskIntermediate (1-5% Mortality)Intermediate (1-5% Mortality)
• Intraperitoneal /intrathoracicIntraperitoneal /intrathoracic
• OrthopedicOrthopedic
• Head & neckHead & neck
• Carotid endarterectomyCarotid endarterectomy
Surgery Specific RiskSurgery Specific RiskLow (<1% Mortality)Low (<1% Mortality)
• Endoscopic (cholecystectomy, Endoscopic (cholecystectomy,
arthroplasty, urologic, etc.)arthroplasty, urologic, etc.)
• BreastBreast
• SkinSkin
• CataractsCataracts

Functional CapacityFunctional Capacity Metabolic Equivalents (METs)Metabolic Equivalents (METs)
• Low (< 4 METs)Low (< 4 METs)
– increased surgical riskincreased surgical risk
• Intermediate (4-10 METs)Intermediate (4-10 METs)
• Excellent (> 10 METs)Excellent (> 10 METs)

Functional CapacityFunctional Capacity Metabolic Equivalents (METs)Metabolic Equivalents (METs)
• Low (< 4 METs)Low (< 4 METs)
– increased surgical riskincreased surgical risk
• Intermediate (4-10 METs)Intermediate (4-10 METs)
• Excellent (> 10 METs)Excellent (> 10 METs)
Climbing a flight of stairsClimbing a flight of stairsLevel walking at 4 mphLevel walking at 4 mphScrubbing floorsScrubbing floorsMoving heavy furnitureMoving heavy furnitureGolfGolf

Functional CapacityFunctional Capacity Metabolic Equivalents (METs)Metabolic Equivalents (METs)
• Low (< 4 METs)Low (< 4 METs)
– increased surgical riskincreased surgical risk
• Intermediate (4-10 METs)Intermediate (4-10 METs)
• Excellent (> 10 METs)Excellent (> 10 METs)
SwimmingSwimmingSingles tennisSingles tennisBasketballBasketball

Operative Risk StratificationOperative Risk Stratification
Surgical UrgencySurgical Urgency
OROR
emergentemergent
Eagle et al. ACC/AHA Executive Summary. JACC 2002;39:542-53.Eagle et al. ACC/AHA Executive Summary. JACC 2002;39:542-53.

Operative Risk StratificationOperative Risk Stratification
Surgical UrgencySurgical Urgency
OROR Prior (<5 years) Prior (<5 years) revascularizationrevascularization
Recurrent signs/symptomsRecurrent signs/symptoms
urgent or electiveurgent or elective
yesyesnono
FurtherFurtherRiskRiskStratificationStratification
yesyes
nono

Operative Risk StratificationOperative Risk Stratification
Clinical PredictorsClinical Predictors
MajorMajor IntermediateIntermediate Minor/noneMinor/none
Eagle et al. ACC/AHA Executive Summary. JACC 2002;39:542-53.Eagle et al. ACC/AHA Executive Summary. JACC 2002;39:542-53.

Operative Risk StratificationOperative Risk Stratification
Clinical PredictorsClinical Predictors
MajorMajor IntermediateIntermediate Minor/noneMinor/none
Postpone Surgery?Postpone Surgery?
Medical Rx andMedical Rx andRisk Factor OptimizationRisk Factor Optimization
CoronaryCoronaryAngiographyAngiography

Operative Risk StratificationOperative Risk Stratification
Clinical PredictorsClinical Predictors
MajorMajor IntermediateIntermediate Minor/noneMinor/none
Stress TestingStress Testing Surgical Procedural RiskSurgical Procedural Risk
> 4 METs> 4 METs
HighHigh
< 4 METs< 4 METs
Intermediate or LowIntermediate or Low
OROR

Operative Risk StratificationOperative Risk Stratification
Clinical PredictorsClinical Predictors
MajorMajor IntermediateIntermediate Minor/noneMinor/none
Surgical Procedural RiskSurgical Procedural Risk
Intermediate or LowIntermediate or Low
< 4 METs< 4 METs > 4 METs> 4 METs
OROR

Operative Risk StratificationOperative Risk Stratification
Clinical PredictorsClinical Predictors
MajorMajor IntermediateIntermediate Minor/noneMinor/none
Surgical Procedural RiskSurgical Procedural Risk
< 4 METs< 4 METs
Stress TestingStress Testing
HighHigh

Operative Risk StratificationOperative Risk StratificationStress Testing SummaryStress Testing Summary
Surgery Specific RiskSurgery Specific RiskM
edic
al R
isk
Med
ical
Ris
kLow Intermediate HighLow Intermediate High
Min
or I
nte
rmed
iate
M
ajor
Min
o r I
nte
rmed
iate
M
ajor
Stress testStress test
Functional capacity <4 METs: stress testFunctional capacity <4 METs: stress testOROR
Optimize RF and/or further eval.Optimize RF and/or further eval.

Prevention of Perioperative MIPrevention of Perioperative MIGoalsGoals
• Identify severe or symptom limiting Identify severe or symptom limiting
CAD - risk stratificationCAD - risk stratification
• Minimize risk from CAD (standard Minimize risk from CAD (standard
Rx of CAD)Rx of CAD)

Perioperative IssuesPerioperative Issues
• Risk stratificationRisk stratification
• Minimize riskMinimize risk
• MonitoringMonitoring
• Treating complicationsTreating complications
History, physical, ECG, lab testsHistory, physical, ECG, lab testsSelective stress testingSelective stress testingClinically indicated catheterizationClinically indicated catheterization
Perioperative IssuesPerioperative Issues
• Risk stratificationRisk stratification
• Minimize riskMinimize risk
• MonitoringMonitoring
• Treating complicationsTreating complications
-blockers-blockersCorrect anemiaCorrect anemiaRisk directed PCIRisk directed PCIClinically indicated CABGClinically indicated CABG

Perioperative MIPerioperative MIRisk PredictorsRisk Predictors
• Severity of underlying CAD Severity of underlying CAD
– clinical markersclinical markers
• Type of surgery Type of surgery
– hemodynamic stress and durationhemodynamic stress and duration
• Functional capacityFunctional capacity

Diabetes and Coronary Diabetes and Coronary MortalityMortality
1373 Nondiabetic 1059 Diabetic
18.8 20.2
45
3.50
10
20
30
40
50
%
Prior MIAlone
DM Alone Both Neither
7 Year Incidence Fatal and Nonfatal MI
Haffner et al. NEJM 1998;339:229.Haffner et al. NEJM 1998;339:229.

Preop Stress TestingPreop Stress TestingBasic PrinciplesBasic Principles
• Same indications as with the non-preop Same indications as with the non-preop
patientpatient
• Without standard indications for stress Without standard indications for stress
testing - intermediate cardiac risktesting - intermediate cardiac risk
• How will the results will change How will the results will change
management?management?

Preoperative Imaging TestingPreoperative Imaging Testing
• Higher risk with ischemia versus scarHigher risk with ischemia versus scar
• Graded risk with ischemia by severity Graded risk with ischemia by severity
and extentand extent
• LBBB special case (adenosine Tl)LBBB special case (adenosine Tl)

Postoperative MortalityPostoperative MortalityPreoperative HemoglobinPreoperative Hemoglobin
0
10
20
30
40
6 7 8 9 10 11 12 >12
Hemaglobin g/dl
% M
ort
alit
y
n=1958n=1958
Carson et al. Lancet 1996;348:1055.

Postoperative MortalityPostoperative MortalityOperative Fall in HemoglobinOperative Fall in Hemoglobin
Cardiovascular Disease
0
50
100
150
200
250
6 7 8 9 10 11 12
Hemoglobin g/dl
Adj
uste
d O
dds
Rat
io
<22 to 4>4

Role of Preoperative EchoRole of Preoperative EchoHalm et al. Ann Int Med 1996;125:433.Halm et al. Ann Int Med 1996;125:433.
• Not an independent predictorNot an independent predictor
• Only for standard indicationsOnly for standard indications– murmur/valvular diseasemurmur/valvular disease
– atrial fibrillation/flutteratrial fibrillation/flutter
– dyspnea/CHF/cardiomyopathydyspnea/CHF/cardiomyopathy
– unstable anginaunstable angina

Role of Preoperative EchoRole of Preoperative EchoRohde LE, et al. Am J Cardiol 2001;87:505.Rohde LE, et al. Am J Cardiol 2001;87:505.
• Clues to order echo:Clues to order echo:
– Prior CHF or MIPrior CHF or MI
– Evidence of valvular heart diseaseEvidence of valvular heart disease
• Predictive utility only for Revised Predictive utility only for Revised
Cardiac Risk Index III and IVCardiac Risk Index III and IV

Perioperative MI PreventionPerioperative MI PreventionTransesophageal Echo (TEE)Transesophageal Echo (TEE)
• Detects new wall motion Detects new wall motion abnormalitiesabnormalities
• Labor intensiveLabor intensive
• Interpreter expertiseInterpreter expertise
• ExpensiveExpensive
• No objective evidence of benefitNo objective evidence of benefit

Perioperative MI PreventionPerioperative MI PreventionSwan-Ganz CatheterizationSwan-Ganz Catheterization
• Early detection of altered filling Early detection of altered filling pressurespressures
• Expertise in interpreting and Expertise in interpreting and troubleshootingtroubleshooting
• Presumed benefit:Presumed benefit:– high risk cardiac patients (AS, MS, CHF)high risk cardiac patients (AS, MS, CHF)– surgery with likely major fluid shiftssurgery with likely major fluid shifts

Perioperative MI PreventionPerioperative MI PreventionNitroglycerinNitroglycerin
• Reduces myocardial ischemiaReduces myocardial ischemia– arterial and venodilatorarterial and venodilator
– reduces ventricular preloadreduces ventricular preload
• Hypotension can exacerbate Hypotension can exacerbate ischemiaischemia
• No proven benefit in prophylaxisNo proven benefit in prophylaxis

Diagnosing Perioperative MIDiagnosing Perioperative MI
• Often without typical anginaOften without typical angina
• 2/3 present with ST depression2/3 present with ST depression
• CK-MB/TroponinsCK-MB/Troponins
• ECG/Troponin (high risk patients)ECG/Troponin (high risk patients)– q 8 h first 24 hrs thenq 8 h first 24 hrs then– next 2 daysnext 2 days

Treatment of Postoperative MITreatment of Postoperative MI
• ST depression (non ST elevation)ST depression (non ST elevation)
– medical Rx with appropriate diagnostic medical Rx with appropriate diagnostic
testingtesting
• ST elevationST elevation
– acute intervention (emergent PCI or CABG) acute intervention (emergent PCI or CABG)
as bleeding risk warrantsas bleeding risk warrants
• Aggressive medical Rx:Aggressive medical Rx:– Antiplatelet RxAntiplatelet Rx blockerblocker– StatinStatin– ACEIACEI– Correct anemiaCorrect anemia
• Further noninvasive assessmentFurther noninvasive assessment
• Appropriate revascularizationAppropriate revascularization

Treatment of Postoperative MITreatment of Postoperative MI
• ST depressionST depression
– medical Rx with appropriate diagnostic medical Rx with appropriate diagnostic
testingtesting
• ST elevationST elevation
– acute intervention (emergent PCI or CABG) acute intervention (emergent PCI or CABG)
as bleeding risk warrantsas bleeding risk warrants

Postoperative MIPostoperative MIImmediate Invasive StrategyImmediate Invasive Strategy
• 48 patients 1.6 48 patients 1.6 1.9 days post surgery 1.9 days post surgery– intraabominal 14, ortho 11, vascular 11, intraabominal 14, ortho 11, vascular 11,
misc. 12 misc. 12
• ST elevation MI in 33 (75%) ST elevation MI in 33 (75%)
• Shock in 21(44%)Shock in 21(44%)
• Cardiac arrest in 12 (25%)Cardiac arrest in 12 (25%)
Berger PB, et al. Am J Cardiol 2001;87:1100-2.

• Intervention:Intervention:
– 41 PTCA41 PTCA
– 2 CABG2 CABG
– 4 medical4 medical
– 1 died in cath.1 died in cath.
• Results:Results:– Survival in 31 Survival in 31
(65%)(65%)– Post arrest 9/12 Post arrest 9/12
(75%)(75%)– Post shock 11/21 Post shock 11/21
(52%)(52%)
Postoperative MIPostoperative MIImmediiate Invasive StrategyImmediiate Invasive Strategy
Berger PB, et al. Am J Cardiol 2001;87:1100-2.

Clinical Case Clinical Case HistoryHistory
• 46 y/o male smoker46 y/o male smoker
• T3-4 diskectomy and laminectomy T3-4 diskectomy and laminectomy
for herniated discfor herniated disc
• Post ectopy v. tach v.fib defibPost ectopy v. tach v.fib defib

Clinical CaseClinical CaseHospital CourseHospital Course
• Echo: LVEF 40% Echo: LVEF 40%
• Cath: 100% proximal LAD, Cath: 100% proximal LAD,
• PTCA without anticoagulationPTCA without anticoagulation
• IABPIABP
• Beta-blockade, ACEIBeta-blockade, ACEI

Clinical CaseClinical CaseHospital CourseHospital Course
• Repeat cath day 10: reocclusion of Repeat cath day 10: reocclusion of LAD, 50% OM1, 65% prox RCALAD, 50% OM1, 65% prox RCA
• Repeat PCA with stentRepeat PCA with stent
• D/C meds:D/C meds:– lisinoprillisinopril– metropololmetropolol– ASA and ticlopidineASA and ticlopidine

Perioperative MIPerioperative MITreatment LimitationsTreatment Limitations
• Few randomized studies concerning Few randomized studies concerning
treatment to prevent MItreatment to prevent MI
• No studies specifically on treating No studies specifically on treating
perioperative MIsperioperative MIs

Thrombolysis of Acute MIThrombolysis of Acute MI
• Reduces mortality from 10-15% to 7-Reduces mortality from 10-15% to 7-10%10%
• Indicated for:Indicated for:– ST elevationST elevation– <12 hrs. from onset<12 hrs. from onset
• Contraindicated for:Contraindicated for:– excessive bleeding riskexcessive bleeding risk

Acute MI MortalityAcute MI MortalityISIS-2. Lancet 1988;2:349.ISIS-2. Lancet 1988;2:349.
13.5
10.1 10.4
7.8
0
2
4
6
8
10
12
14
%
Placebo Strepto. ASA Both
30 day Mortality
PlaceboStrepto.ASABoth

Acute MI RevascularizationAcute MI RevascularizationGusto IIbGusto IIb
75.7 6
4.4
2.3
0.20
2
4
6
8
10
%
Death (Re) MI Stroke
30 Day Endpoints
Angioplasty Substudy
t-PA (n=573)PTCA (n=565)

Optimizing Patency After Optimizing Patency After PTCAPTCA
• HeparinHeparin
• Glycoprotein IIb/IIIa inhibitorGlycoprotein IIb/IIIa inhibitor
• IABPIABP
• StentsStents

IABP After Primary PTCAIABP After Primary PTCAStone et al. JACC 1997;29:1459.Stone et al. JACC 1997;29:1459.
3.1
4.3
8
6.25.5
6.7
0
2.4
0
2
4
6
8
10
%
Death Reinfarction Reocclusion Stroke
No IABP
IABPP=0.03P=0.03
(n=226)
(n=211)

Clinical Markers of Severe Clinical Markers of Severe CADCAD
• MajorMajor
– recent MIrecent MI
– unstable or severe anginaunstable or severe angina
– uncompensated CHFuncompensated CHF

Clinical Markers of Severe Clinical Markers of Severe CADCAD
• IntermediateIntermediate– less severe from “major”less severe from “major”– DMDM
• MinorMinor– advanced ageadvanced age– abnormal ECGabnormal ECG– poor functional capacitypoor functional capacity

Preoperative RevascularizationPreoperative RevascularizationRisk GuidelinesRisk Guidelines
• Standard indications for Standard indications for
revascularizationrevascularization
• Noncardiac surgery risk > 5%Noncardiac surgery risk > 5%
• Cardiac revascularization risk < 3%Cardiac revascularization risk < 3%