perinatal database: still &pre- viable fetus · “owing to limited data it is difficult to...
TRANSCRIPT

Perinatal Database: Still &Pre- Viable fetus
Dr Neelam Aggarwal
Addl Prof, PGIMER, Chandigarh


GENESIS OF THE PROJECT

GENESIS OF THE PROJECT
STILL BORNS NEWBORNS ,N,BD,SICK
PRE-VIABLE

Retracing the journey
• From conception to delivery

ROAD MAP

• Not mentioned in MDGs
• Absent from global indicators of disease
• Interventions rarely studied/evaluated
• Indirect reflection of maternal health
• Estimates of stillbirth rates rely on registration data, national survey and special studies
“Owing to limited data it is difficult to assess the share of congenital syphilis and birth defects, which are amongst the many causes of still birth”


Still birth surveillance

OVERVIEW STILLBIRTH ISSUES: HIDDEN REALITY
One of the common adverse outcomes of the pregnancy
More than 3.2milloin stillbirths occur globally each year
98% still births happen in low and middle income countries

Country variation in stillbirth rates
2.65 million third trimester stillbirths each year
Applying high-income country stillbirth definitions (second and third trimester)
this number may be 40% higher
10 countries account for 66% of the world’s stillbirths – and also 66% of neonatal deaths and over 60% of maternal deaths 1. India 2. Pakistan 3. Nigeria 4. China 5. Bangladesh 6. Dem Rep Congo 7. Ethiopia 8. Indonesia 9. Tanzania 10. Afghanistan

Irony of still births
Most poorly recognized from the countries of most common ocurrence .

Mismatch of Burden to Action
• Hidden reality
• Social taboo
• Lack of data

International Awakening

Global Community - Goal By 2020
For countries with SBR >5 , reduction in still
birth rate by 50% from 2008 rate
For countries with SBR <5,to eliminate all
preventable stillbirths

Why ,When and Where still birth
occurs
Supported the development of stillbirth protocols AND has developed and pretested the tools for still births
“Need to make standard protocols for
SB surveillance to generate data for
preventive planning & effective
interventions to reduce SBs”


Invisibility & Confusions
Out of sight out of mind

Challenges of making stillbirth protocol
• Missing numbers
• Varied definitions
• Classification bias
• Records
• Uniformity
• Choose relevant in
the national context

Defining stillbirths
WHO international
definition

Mammoth Task ?

STILL BIRTH SURVEILLANCE: EXPERTS
• Clinical experts, neonatology, pathology, school
of public health – National imminence
• Experts from WHO, UNFPA, ICMR, MOHFW.
• All WHO CCs



Brainstorming sessions
• Definitions , Classification ,strategies

Finalization of definitions
• Definition
• Count from 20 weeks gestation
• Categorize
• Early 20-27 weeks
• Late > 28 weeks
• Assign cause from CODAC simplified

Genesis of still birth surveillance proforma
First Meeting at Chandigarh (Nov. 2011)
“Development of protocols for stillbirths review & guidelines for sentinel surveillance”
Conclusion :Gestation of still birth & Consensus of classification system could not be finalized
Second Meeting at Chandigarh (FEB 2012) •Definition and gestation of still birth finalized Early 20-27 weeks Late > 28 weeks •Pretesting of proforma to be done by modified CODAC classification.
•Third meeting at Chandigarh(July 2013)
“Orientation workshop on stillbirth surveillance tools” Autopsy requisition to be included in the proforma . 5 centers identified for the testing of the surveillance proforma.

Still birth proforma








What next ?
Surveillance proforma tested by sharing retrospective data of 25,177 deliveries by 5 centers and analyzed(July-Oct 2013)
Prospectively two live births were enrolled for each still birth (Sep to Nov 2013).A total of 291 still births and 606 live births
were recorded in this proforma and analysis was done.
5 more centers recruited and proforma filling continued in NNPD Project (Nov 2013-Contd)
Meanwhile, PGIMER, Chandigarh became the nodal centre for NNPD Project.

Prevention and control of BDs in SEAR: Strategic framework(2013-2017) - Target reduction
FA preventable
by 35%
Thalassemic births by
50%
congenital rubella
congenital syphilis

Still birth surveillance in NBBD
To create a standard and reliable database on still births as part of NBBD : Indian Experience

Genesis of the study
NBBD captured all beyond 20 weeks.
Unaccounted ONES??

What was being missed?
<20 weeks

1st Trimester
2nd Trimester
CMF
199 169 132
PGIMER 1 YEAR DATA

Genesis of PVBD surveillance proforma
Fourth Meeting at Chandigarh (2014 ) & training workshop for pathologists
“Inclusion of Pre Viable birth defects surveillance”
Initially case control records with 2 normal pregnancies
•Plan of making it online submission


Methodology Screen all •USG at 16-18 week
Inclusion criteria • Cases All diagnosed BD <20 weeks •Controls –two for each case
Controls Antenatal clinic Management as per protocol
Cases MTP clinic Termination as per protocol Fetal autopsy, final diagnosis
Analysis Comparison of risk factors Autopsy correlation with ultrasound

Screened 11,280
CMF 428 Controls 771
RESULTS

Distribution according to maternal age

Distribution according to Gestation (in weeks)

Distribution according to FA intake during pregnancy

Distribution according to Preconceptional FA intake

Category CMF(N=452)
Previous History Of Birth Defects 22(4.8%)
Distribution according to previous history of birth defects

Distribution according to previous
history of birth defects
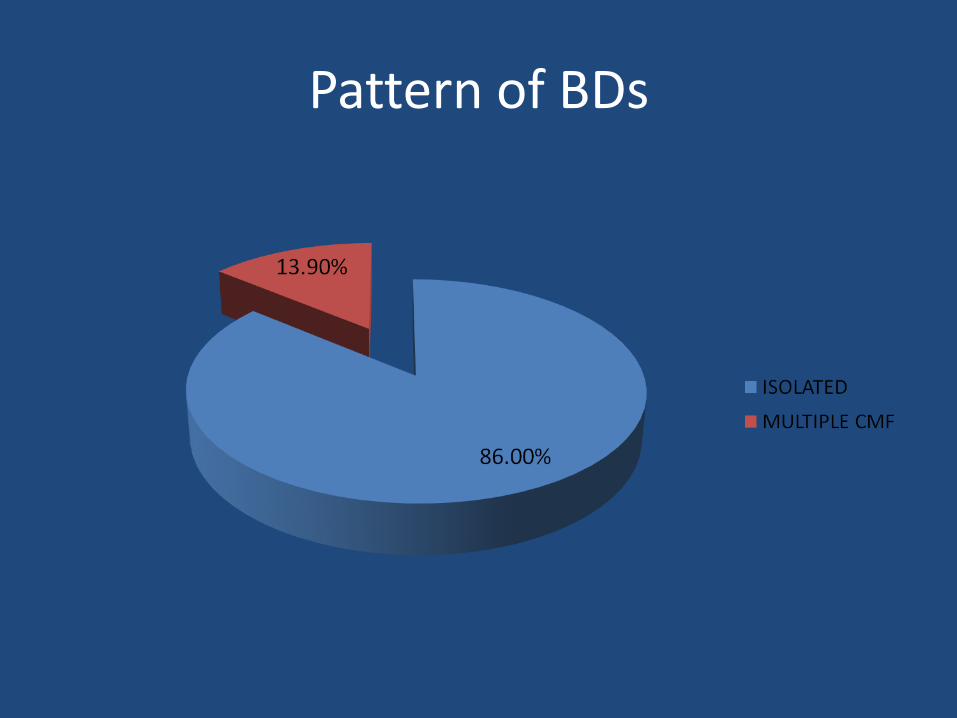
Pattern of BDs



GI defects(N=25)

GU defects(N=28)

Genetic defects & Others(N=36)

Autopsy
All
CM
F’s
sho
uld
be
su
bje
cted
to
au
top
sies
.
Ass
oci
ated
Mal
form
atio
ns
Gen
etic
co
un
selli
ng
acco
rdin
gly.

? ENCEPHALOCELE ? SPINA BIFIDA OCCULTA

OCCIPITAL MYELOCELE

HYDROCEPHALOUS


B/L MCDK
PD
DPM
Kidneys

PATHOLOGISTS’ WORD
• Meckle Gruber syndrome – AR
– B/L Multicystic dysplasia - Kidneys
– Ductal plate malformation – liver
– B/L hypoplastic lungs
– Neural Tube defects – Occipital meningocele, spinal meningomyelocele
– Hydrocephalous
– Polydactyly

Final Autopsy Diagnosis- Became
• Meckle Gruber syndrome
• From Encephalocoel to AR condition (5-25%)
• Genetic counselling, prognosis
From – Occipital encephalocele to AR

Challenges faced
Ascertaining the gestational age
• Induced termination of pregnancy for conditions like severe preeclampsia, previable PTPROM
WHERE TO LIST
Completeness of data

CHALLENGES FACED
Timeliness
•Reporting
•Filling
•Collection of forms
•Online submission
Accurate delineation and description OF CAUSE OF DEATH

CHALLENGES FACED Photographs:
Often Not taken
Poor quality
Placenta for Histopathology
Not sent
Infantogram
No consent
Autopsy
No consent
SOCIOCULTURAL ISSUES??

Preventable yet not???
SB/ NB/ Uterine scar
Severe Maternal morbidity, Preterm,
Resources/LOGISTICS

Overcoming Challenges
Standardization of SB proformas
Standard SOPs
Ensure Quality & Quantity
Sensitizing Pathologists

Way Forward
• Hospital based : Extend this NBBD surveillance to all facilities.Nodal centres, technical co-ordinators.
• Population based : Roll out at community level
• Online submission of PVBD forms
• Scale up already in pipeline by MOH, India.

Capacity Building
Integrated & Comprehensive
care
Changing the attitude
Way forward