performance anxiety inventory for musicians (perfaim): a new
TRANSCRIPT

Performance Anxiety Inventory for Musicians (PerfAIM):
A New Questionnaire to Assess Music Performance Anxiety in Popular Musicians.
Audrey-Kristel Barbeau
Music Research Department
Schulich School of Music
McGill University, Montreal
June, 2011
A thesis submitted to McGill University
in partial fulfillment of the requirements
for the degree of Master of Arts in Music Education
© Audrey-Kristel Barbeau, 2011
ii
Table of Contents
Abstract ……………………………………………………………………………………... v
Acknowledgements………………………………………………………………………….. vii
List of Tables………………………………………………………………………………… viii
List of Figures………………………………………………………………………………... ix
Introduction………………………………………………………………………………….. 1
Background and Rationale……………………………………………………………………. 1
Aims and Objectives………………………………………………………………………….. 2
Chapter 1: Definitions and Theories……………………………………………………….. 4
1.1 Definitions………………………………………………………………………………… 4
1.1.1 Stress……………………………………………………………………………… 4
1.1.2 Fear………………………………………………………………………………... 6
1.1.3 Anxiety……………………………………………………………………………. 6
1.1.4 Arousal……………………………………………………………………………. 7
1.1.5 Stage Fright……………………………………………………………………….. 8
1.1.6 Music Performance Anxiety………………………………………………………. 8
1.2 Theories………………………………………………………………………………….... 12
1.1.1 Theories from Psychology………………………………………………………... 12
1.1.1.1 Lazarus‘s Theory of Cognitive Appraisal……………………………………... 12
1.1.1.2 Lupien‘s Recipe for Stress: Don‘t Go Nuts!………………………………….. 13
1.1.1.3 Spielberger‘s State-Trait Anxiety Theory…………………………………….. 14
1.1.2 Theories from Sport Psychology…………………………………………………. 14
1.1.2.1 The Yerkes-Dodson Law and Inverted-U Hypothesis………………………… 14
1.1.2.2 Individualized Zone of Optimal Functioning (IZOF)…………………………..16
1.1.2.3 Multidimensional Anxiety Theory…………………………………………….. 16
1.1.2.4 Catastrophe Model..………………………………………………………….... 17
1.1.2.5 The Four-Stage Stress Process……………………………………………….... 18
1.1.2.6 Model of Facilitative and Debilitative Anxiety..….….……………………….. 19
1.1.3 Music Performance Anxiety Theories …………………………………………... 20

iii
1.1.3.1 Lang‘s Three-System Model of Fear…………………………………………. 21
1.1.3.2 Salmon‘s Theory of MPA…………………………………………………….. 22
1.1.4 Summary…………………………………………………………………………. 22
Chapter 2: Review of Literature……………………………………………………………. 25
2.1 Prevalence of MPA among Musicians……………………………………………………. 25
2.1.1 Classical Musicians……………………………………………………………….. 25
2.1.2 Popular Musicians………………………………………………………………… 27
2.1.3 Gender Differences……………………………………………………………….. 28
2.2 Domains…………………………………………………………………………………… 30
2.2.1 Causes of MPA: Situational and Personal Sources of Stress……………………... 30
2.2.2 Temporal Occurrence of MPA……………………………………………………. 34
2.2.3 Direction of MPA…………………………………………………………………. 35
2.2.4 Manifestations of MPA (symptoms)……………………………………………… 37
2.3 Pre-Existing Measures Related to MPA………………………………………………….. 40
2.4 Questionnaire Design and Validation…………………………………………………….. 42
Chapter 3: Methods………………………………………………………………………….. 45
3.1 Overview, Population and Settings…………………………………………………….. 45
3.2 Ethical Considerations …………………………………………………………………. 48
3.3 Instrumentation………………………………………………………………………….. 49
3.4 Content Validity………………………………………………………………………… 49
3.5 Face Validity……………………………………………………………………………. 50
3.6 Scores and Means……………………………………………………………………….. 51
3.7 Internal Consistency Reliability………………………………………………………… 51
3.8 Test-Retest Reliability………………………………………………………………….. 52
3.9 Concurrent Criterion-Related Validity………………………………………………….. 52
3.10 Construct Validity (Convergent and Divergent)……………………………………….. 53
Chapter 4: Results…………………………………………………………………………… 54
4.1 Content Validity………………………………………………………………………….. 54
4.1.1 Item Generation…………………………………………………………………… 54
4.1.2 Item Reduction……………………………………………………………………. 54
4.1.3 Instructions……………………………………………………………………….. 57

iv
4.1.4 Scale………………………………………………………………………………. 58
4.1.5 Score……………………………………………………………………………….58
4.1.6 Format…………………………………………………………………………….. 59
4.1.7 Domains…………………………..………………………………………………. 59
4.2 Face Validity………………………………………………………………………………. 62
4.2.1 Main construct……………………………………………………………………. 62
4.2.2 Domains………………………………………………………………………….. 62
4.2.3 Validity…………………………………………………………………………… 63
4.3 PerfAIM‘s Scores and Means……………………………………………………………... 63
4.4 Internal Consistency Reliability…………………………………………………………... 66
4.5 Test-Retest Reliability ……………………………………………………………………. 67
4.6 Concurrent Criterion-Related Validity……………………………………………………. 67
4.7 Construct Validity (Convergent and Divergent)…………………………………………... 68
Chapter 5: Discussion……………………………………………………………………….. 69
5.1 Content Validity…………………………………………………………………………... 69
5.2 Face Validity……………………………………………………………………………… 71
5.3 PerfAIM‘s Score and Means……………………………………………………………… 72
5.4 Internal Consistency Reliability………………………………………………………….. 74
5.5 Test-Retest Reliability……………………………………………………………………. 76
5.6 Concurrent Criterion-Related Validity…………………………………………………… 76
5.7 Construct Validity (Convergent and Divergent)………………………………………….. 76
Chapter 6: Limitations and Conclusion……………………………………………………. 78
6.1 Limitations………………………………………………………………………………… 78
6.2 Conclusion………………………………………………………………………………… 80
Bibliography………………………………………………………………………………….. 83
Appendices: Recruitment Material; Consent Forms ; Content Validity Questionnaire -
Results (Focus Groups); Transcriptions (Focus Groups); Interview Oral Questions - Results
(Quantitative); Content Validity Questionnaire - Results (Experts); Interview Oral Questions
- Results (Qualitative 1); Interview Oral Questions - Results (Qualitative 2); PerfAIM; Items
Categorized by Domains……………………………………………………………………… 92

v
Abstract
The goal of this research project was to develop and validate a new measure that establishes the
extent to which highly stressful performance situations affect self-perceived levels of Music
Performance Anxiety (MPA) in popular musicians. The Performance Anxiety Inventory for
Musicians (PerfAIM), a self-report measure demonstrating appropriate psychometric properties,
was developed. The specific objectives of this research project were to estimate the validity of the
questionnaire and to assess its reliability. Content validity and face validity were established
using focus groups and interviews with experts. A sample of 69 popular professional musicians
and music students completed the inventory, with which we established the internal consistency,
the test-retest reliability, the concurrent criterion-related validity and the construct validity
(convergent and divergent). Among the sample, 66 participants completed the Performance
Anxiety Inventory (PAI, Nagel, Himle, & Papsdorf, 1989), and 61 respondents, the revised
Kenny Music Performance Anxiety Inventory (revised K-MPAI, Kenny, 2009a). A test-retest
was done at a one-week interval using a sample of 21 musicians. The PerfAIM demonstrated an
excellent internal consistency (Cronbach‘s alpha=0.93), a very good reliability (ICC=0.89 with
95% CI), and a satisfactory concurrent criterion-related validity and convergent validity (Pearson
product-moment correlation coefficient). No significant difference was found between men and
women‘s scores on the PerfAIM. In conclusion, the PerfAIM is an adequate measure for
assessing self-perceived levels of MPA, enabling musicians to develop self-awareness of the
causes, temporal occurrence, direction, and cognitive, somatic, affective and behavioral
manifestations of MPA.

vi
Résumé
Ce projet de recherche visait à développer et à valider un nouveau questionnaire permettant
d‘évaluer dans quelle mesure les performances hautement stressantes affectent la perception du
niveau d‘anxiété de performance musicale (APM) des musiciens populaires. À cet effet, nous
avons créé le « Performance Anxiety Inventory for Musicians » (PerfAIM), un questionnaire
auto-administré démontrant des propriétés psychométriques satisfaisantes. Les objectifs
spécifiques de ce projet consistaient à évaluer la validité et la fidélité du questionnaire. La
validité de contenu et la validité apparente ont été établies avec des groupes focus et des
entrevues auprès d‘experts. Un échantillon de 69 musiciens populaires (professionnels et
étudiants) ont complété le questionnaire, ce qui a permis d‘établir la consistance interne, la
fidélité test-retest, la validité de critère concomitante ainsi que la validité de construit
(convergente et divergente). Parmi l‘échantillon, 66 participants ont complété le « Performance
Anxiety Inventory » (PAI, Nagel, Himle, & Papsdorf, 1989), et 61 répondants, le « Kenny Music
Performance Anxiety Inventory » révisé (revised K-MPAI, Kenny, 2009a). Le test-retest a été
fait à une semaine d‘intervalle auprès d‘un échantillon de 21 musiciens. Le PerfAIM démontre
une excellente consistance interne (alpha de Cronbach=0.93), une très bonne fidélité (CCI=0.89
avec un IC à 95%), et une validité de critère concomitante et de construit convergente
satisfaisantes (calculées à l‘aide d‘une corrélation de Pearson). Aucune différence significative
n‘a été démontrée entre les résultats des hommes et des femmes dans le PerfAIM. En conclusion,
le PerfAIM est un questionnaire approprié pour l‘évaluation de la perception du niveau d‘APM
des musiciens, permettant à ces derniers de prendre conscience des causes, des occurrences
temporelles, de la direction, et des manifestations (cognitives, somatiques, affectives et
comportementales) de l‘anxiété de performance.

vii
Acknowledgements
First of all, I would like to thank all the students, musicians, professors and researchers
who participated in this research. Without their participation, this study would not have been
possible. I would especially like to thank my supervisor Isabelle Cossette. Her involvement,
support and encouragement made this research project achievable. I would like to acknowledge
the Schulich School of Music for its financial support through the Schulich scholarship, as well
as the SSHRC through the Joseph-Armand Bombardier scholarship. I am grateful to my
professors Sharon Wood-Dauphinee and Sara Ahmed from the ―Measurement in Rehabilitation
II‖ course: Thank you for spending time outside of class to meet with me, answer my questions,
and put me in contact with other amazing people. Thanks are also due to my teammates from the
Measurement course (Claudia Brown, Barbara Shankland et Mohamad Pakzad) for their help in
creating the preliminary version of my research protocol. I want to express my gratitude to my
colleagues from the Lucie-Bruneau Rehabilitation Center, particularly Eduardo Cisneros, Gilles
Charrette, Michelle McKerral and Sheila Schneiberg. I learned a lot by working with you as a
research assistant. Thanks to Allison Devery, Carolyn Samuel, and Kamran Ezdi who helped me
edit my manuscripts and/or the many drafts of my questionnaire. A special thank-you goes to
professor Jean-Paul DesPins (UQAM) who conveyed his passion for research and teaching to me
when I was doing my undergraduate studies. He strongly encouraged me to undertake graduate
studies and helped me believe in my capabilities. His influence changed my life! Merci à ma
mère Diane et à son mari Gilbert pour leur appui et leurs bons mots. Une pensée particulière
également pour mon père qui aurait, je pense, été très fier de sa petite fille. Finalement, je tiens à
remercier de tout mon cœur mon mari Marc-André, pour son soutien tout au long de ma maîtrise,
dans les moments les plus heureux comme les plus difficiles. Thank you all!

viii
List of Tables
Table 1. Distinguishing Debilitating Performance Anxiety From Two Other Social Phobia
Subtypes: A Clinical Model………………………………………………………… 10
Table 2. The Four Determinants of Lupien‘s Recipe for Stress……………………………… 13
Table 3. Studies on the Prevalence of MPA among Classical Musicians……………………. 26
Table 4. Twenty-Two Ranked Causes of MPA in Orchestral Musicians…………………….. 32
Table 5. MPA Symptoms Collected in the Literature and Classified into Four Components... 38
Table 6. Demographic Information – Phase 1 (Focus Groups)………………………………. 46
Table 7. Demographic Information – Phase 3 (Online Questionnaires)……………………… 48
Table 8. Interviews – Round 1.……………………………………………………………….. 55
Table 9. Interviews – Round 2.……………………………………………………………….. 56
Table 10. Interviews – Round 3.……………………………………………………………… 56
Table 11. Interviews – Final Revision.……………………………………………………….. 56
Table 12. Level of Agreement among Experts Regarding the Instructions………………….. 57
Table 13. Numbers Related to the Adjective Scale for the Summation of Scores……………. 59
Table 14. Wording and Proportion of Items Based on the Three Rounds of Interviews……... 59
Table 15. Relationship Between the NUTS Theory, the PerfAIM, and Kenny‘s Causes of
MPA……………………………………………………………………………….. 60
Table 16. Relationship Between the PerfAIM‘s Facilitating Anxiety Items and the Components
of Jone‘s Model of Facilitative and Debilitative Anxiety.………………………… 61
Table 17. Means Reported for Each Item of the PerfAIM.…………………………………… 65
Table 18. Internal Consistency of the PerfAIM by Domains: Cronbach‘s Alpha……………. 66
Table 19. Internal Consistency of the PerfAIM by Gender and by Domains: Cronbach‘s
Alpha........…………………………………………………………………………. 66
Table 20. Concurrent Criterion-Related Validity: Pearson Correlations.……………………. 67
Table 21. Convergent and Divergent Construct Validity: Pearson Correlations…………….. 68
Table 22. Means Associated to Each Item and Categorized by Level of Endorsement……… 73
Table 23. Summary of the Cronbach‘s Alpha Scores for Already Existing MPA
Questionnaires..……………………………………………………………………. 75

ix
List of Figures
Figure 1. Yerkes-Dodson Curve.……………………………………………………………… 15
Figure 2. Hanin‘s Individualized Zone of Optimal Functioning (IZOF)……………………… 16
Figure 3. Multidimensional Anxiety Theory.…………………………………………………. 17
Figure 4. The Catastrophe Model.…………………………………………………………….. 18
Figure 5. The Four-Stage Stress Model.………………………………………………………. 19
Figure 6. Jone‘s Model of Facilitative and Debilitative Anxiety…………………………….. 20
Figure 7. Levels of Performance Anxiety Associated with Various Performance
Requirements..…………………………………………………………………….. 33
Figure 8. Score Distribution – PerfAIM ………………………….………………………....... 64
Figure 9. First and Second Administrations of the PerfAIM………………………………….. 67

1
Introduction
Background and Rationale
A successful musician must not only have excellent musical and technical skills but should
also have the capacity to withstand the psychological and physical demands of performing before
public. The stress of preparing and delivering a performance can often create heightened levels
of anxiety. Music Performance Anxiety (MPA) is a condition in which a performer's response to
stress goes beyond the normal arousal state, resulting in detrimental consequences (Osborne &
Kenny, 2005). Sometimes a moderate amount of anxiety can be perceived as a facilitator of
performance (Dyce & O‘Connor, 1994). However, at a higher level it usually has a debilitating
effect (Wesner, Noyes, & Davis, 1990; Steptoe & Fidler, 1987). Determining the extent to which
stressful performances may affect musicians is thus very important to better understand the MPA
phenomenon.
Very few studies on the occurrence of MPA among popular musicians (a group including
musicians of rock, jazz, country, etc.) exist in the literature, and they are mostly related to
personality types and occupational stress (Dyce & O‘Connor, 1994; Cooper & Wills, 1989; Wills
& Cooper, 1987). Besides, MPA is not specifically assessed using standardized methods, and
musicians are only compared to population norms. In addition, studies dealing with popular
musicians use this population as a part of larger samples including classical musicians, music
therapists, and music teachers (Gillespie & Myors, 2000), and the results are not stratified. This
makes it impossible to verify the occurrence of MPA among a particular category of musicians.
Finally, an analysis of the existing questionnaires reported by Osborne and Kenny (2005) shows
that no measure assessing MPA has been validated with a specific sample of popular musicians.
There is thus a need to explore the prevalence of MPA in this population.
In an extensive review of the literature, Osborne and Kenny (2005) identified 20 measures
of MPA (the term ―measure‖ encompasses all types of questionnaires, inventories, rating scales,
surveys, etc.). These measures addressed anxiety symptoms, performance anxiety in general, or
MPA. All of them employed a self-report method (Kenny & Osborne, 2006; Osborne & Kenny,
2005; Kenny, 2005). Overall, the MPA measures reviewed reported norms and standardization
procedures that were inadequate according to the minimum criteria for basic psychometric
2
properties from McCauley and Swisher (as cited in Osborne & Kenny, 2005). Therefore, the
need for a new psychometrically sound measure is justified.
Aims and Objectives
This project aims to analyze the extent to which high-stress performance situations affect
self-perceived levels of MPA in popular musicians. To achieve this, a self-report measure
demonstrating appropriate psychometric properties in assessing MPA among popular musicians
is developed and validated. The goal of the questionnaire is to assess levels of MPA
retrospectively and to detect change over time or change related to stress management technique
implementation (before vs after treatment). The specific objectives of this research project are to
establish the validity and reliability of the questionnaire1 by conducting the following statistical
tests:
a) Content validity
b) Face validity
c) Concurrent criterion-related validity
d) Convergent and divergent construct validity
e) Internal consistency reliability
f) Test-retest reliability
The Performance Anxiety Inventory for Musicians (PerfAIM) is expected to allow any
respondent to effectively assess his or her situation by endorsing statements related to the causes
(personal and situational), the temporal occurrence, the direction and the manifestations (be they
cognitive, affective, somatic or behavioral) of MPA.
This thesis is divided into six chapters. Chapter 1 presents definitions related to MPA,
stress and anxiety (Section 1.1) and proposes theories from psychology, sport, and music (Section
1.2). Chapter 2 reviews the literature on the prevalence of MPA among musicians (Section 2.1)
and on the four domains chosen to represent the components of MPA (Section 2.2). Pre-existing
measures on MPA are also reported (Section 2.3) and the types of validation selected to conduct
1 Although we know that the terms inventory and questionnaire are not synonymous, they will be referred as such in
this thesis.

3
this project are described (Section 2.4). Chapter 3 explains the methods used for this research,
Chapter 4 presents the results of the questionnaire development and validation, and Chapter 5
analyzes the results through a discussion. At the end, the limitations of the study and a
conclusion including the expected contributions are provided (Chapter 6).
4
Chapter 1
Definitions and Theories
When reading about music performance anxiety (MPA), it is observed that some authors
utilize the terms stage fright (Bippus & Daly, 1999; Nagel, 1993; Fredrikson & Gunnarsson,
1992; Rappoport, 1989; Steptoe & Fidler, 1987), stress (Sternbach & Woody, 2008; Wills &
Cooper, 1987), arousal (Kesselring, 2006; Osborne & Kenny, 2005) or fear (Baker, 2005) as
synonymous with MPA. A few researchers also rely on the more general term anxiety to
describe MPA in a broader perspective (Lin, Chang, Zemon & Midlarsky, 2008; Gill, Murphy &
Rickard, 2006; Miller & Chesky; 2004; Kubzansky & Stewart, 1999). Often, the term
performance anxiety is used interchangeably with MPA when it assesses the phenomenon among
musicians (Khalsa, Shorter, Cope, Wyshak & Sklar, 2009; Emmons & Thomas; 2008; Kirchner,
Bloom & Skutnick-Henley, 2008; Stephenson & Quarrier; 2005; Lazarus & Abramovitz, 2004;
Nagel, 2004; Powell, 2004; Rae & McCambridge, 2004). As reported by Kenny (2006),
―performance anxiety is the general term for a group of disorders that affect individuals in a
range of endeavours, from test-taking, mathematics performance, public speaking and sport, to
the performing arts of dance, acting and music‖ (p. 52). In accordance with Kenny (2006), Nagel
(1990) describes performance anxiety as a ―constellation of attitudes, traits and unconscious
conflicts that become activated in particular circumstances such as anticipating or giving a
concert‖ (p. 38). Therefore, MPA is a type of performance anxiety specific to music.
Unfortunately, none of the words mentioned above, when taken independently, accurately
defines MPA. For this reason, terms and concepts commonly used in the literature that are
essential to a better understanding of MPA (namely: stress, fear, anxiety, arousal, and stage
fright) will be define in the following section.
1.2 Definitions
1.1.1 Stress. Stress may be interpreted in various ways. Kasper, den Boer and Ad Sitsen
(2003) state that ―stress is classically defined as a threatening of homeostasis2 to which the
2 Homeostasis: the tendency towards a relatively stable equilibrium between interdependent elements, especially as
maintained by physiological processes (Pearsall & Hanks, 2003).

5
organism, in order to survive, responds with a large number of adaptive responses‖ (p. 207). In
accordance with this quote, Sataloff, Rosen and Levy (1999) proposes three different approaches
to define stress:
1. Stress as a ―stressor‖—Stress is often used to refer to one or more
stressors, an influence that causes tension, anxiety, or disruption of
homeostasis. The stressor(s) may originate from external sources such as
danger during wartime or even difficult people. It can also arise from
internal thoughts and feelings, such as guilt, daily worries, and unfulfilled
expectations.
2. Stress as ―distress‖—Stress may refer to internal feelings of distress,
tension, or anxiety caused by a stressor(s). Thus, perturbation of the
cognitive status of the subject is an important factor when using this
definition.
3. Stress as a ―biological response‖—Some scientists and physicians have
defined stress in a more objective manner, by defining it by the existence of
measurable and predictable physiologic effects that distress or stressors
produce. (p. 122)
As shown by Bear, Connors and Paradiso (2007), ―biological stress is created by the brain,
in response to real or imagined stimuli‖ (p. 491). Stress may thus be absolute or relative, which
means that it can be produced by a real or implied threat (Lupien, Maheu, Tu, Fiocco &
Schramek, 2007). A real threat, such as an earthquake in a city, may trigger a significant (and
adaptative) stress response in every individual facing the threat. An implied threat, such as a
music performance or a public speaking task, may induce different stress responses depending on
how the situation is interpreted. Based on these definitions, a stressor may trigger a biological
response that affects homeostasis. Therefore, MPA may originate from external (e.g. an audition)
or internal (e.g. fear of being judged) stressors that may create cognitive, affective, behavioral
and/or physiological reactions that will affect the musician.
Lazarus & Folkman (1984) define the term stress as a ―particular relationship between the
person and the environment that is appraised by the person as taxing or exceeding his or her
resources and endangering his/her well-being‖ (p. 19). In fact, personal appraisal dictates if an
event is stressful or not and if cognitive and physiological responses are to be triggered. The
causes of anxiety may thus be very different for one person to another, but once a stressor is
identified and appraised (positively or negatively), a biological response is automatically
triggered, which alters the homeostasis. Greater detail will be provided in Section 2.2, when the

6
Lazarus and Folkman‘s Theory of Cognitive Appraisal will be presented.
In the context of musical performance, the interaction between a musician and his
environment explains how situational and personal factors may cause MPA. Indeed, some
performers may appraise a music audition as being the most threatening performing situation,
while others may perceive it as a great positive challenge. If the performer feels that it does not
exceed his resources, the stressor (e.g. the audition) will not create the same body response as it
would create if the person felt that he did not have the ability to cope with it.
1.1.2 Fear. Fear may be defined as being an ―adaptative response to threatening
situations‖ (Bear et al., 2007, p. 665). It is inherently negative. As explained by Baars and Gage
(2007), ―fear learning is a long lasting and stable kind of learning that is remarkably resistant to
change and voluntary control. […] While fear learning is adaptative in that it allows us to avoid
predictable dangers in the environment, it can become disabling if it is misplaced or exaggerated‖
(p. 381). This is also supported by Bear et al. (2007), who state that ―fear is not an appropriate or
adaptative response in all circumstances. The inappropriate expression of fear characterizes
anxiety disorders‖ (p. 665).
1.1.3 Anxiety. Anxiety is a response to stressors that has both a physiological (somatic)
component and a psychological (cognitive and affective) component. It is derived from a Latin
word meaning ―a condition of agitation and distress‖ (as cited in Kirchner et al., 2008, p. 60). A
current definition of anxiety comes from Barlow (2000):
Anxiety is a unique and coherent cognitive-affective structure within our
defensive motivational system. At the heart of this structure is a sense of
uncontrollability focused on future threat, danger, or potentially negative
events… Accompanying this negative affective state is a strong
physiological or somatic component that may reflect activation of distinct
brain circuits such as the corticotrophin releasing factor system…(p. 1249)
Anxiety is detrimental and affects the productivity (excessive worrying, avoidance
behavior, etc.). Kirchner et al. (2008) summarize writings about anxiety from May (1977) and
Liebert and Morris (1967):
Although anxiety can function as an essential anticipatory response for
physical protection, the threats that musical performers face today are

7
rarely life-threatening. Nevertheless, anxiety can continue to mobilize the
body for a fight-or-flight response. Conceptually, anxiety may be thought
of in terms of two components (1) worry or lack of confidence, and (2)
physiologic reactions associated with autonomic nervous system arousal
(emotionality). (p. 60)
This quote supports Bears et al.‘s (2007) findings about fear and anxiety and is in accordance
with Baars and Gage‘s (2007) explanations of misplaced/exaggerated fear.
1.1.4 Arousal. Arousal is a general state of activation that goes from deep sleep to extreme
excitement (Kenny, 2011; Weinberg & Gould, 2007). It is neither positive nor negative. As
reported by Emmons and Thomas (2008, p. 462), ―the term arousal represents the result of two
types of anxiety, ‗mental‘ and ‗physical‘ interacting and producing a state of emotional readiness
to perform‖. As everyone is different, there is not a right level of arousal common for all; the
optimal level of arousal depends on individuals, and the nature of each situation (Emmons &
Thomas, 2008). Some musicians may perform better when they feel ―up to the task‖ while others
may give excellent performances only when they are relatively calm. Some may be overexcited
to play alone in front of an audience, but will stay relaxed when they perform in groups.
Emmons and Thomas (2008) explain that ―performers speak of an Ideal Performing State, one in
which there is a feeling of being really ready, mentally and physically, to perform – that is, the
state of arousal for performance is correct and in balance‖ (p. 462). However, Kirchner et al.
(2008) specify that there is still a general trend:
In general, low arousal during the performance of an activity manifests in
boredom and low energy, resulting in a somewhat bland or uninspired
performance. Moderate arousal levels produce alertness and relaxed
energy, characteristic of an engaging performance, which is possible while
in a state of flow. Too much or excessively high arousal can result in
anxiety, producing a poor performance. (p. 60)
As explained by Steptoe (1989), a lot of artists ―argue that they ‗need‘ to be aroused
physiologically in order to perform well, and that stress is an integral component of good
performance‖ (p. 4). In addition, the author reports studies that compared anxious and non-
anxious musicians and demonstrated that both groups showed an increased physiological activity
when performing (Steptoe, 1989). Craske and Craig (1984) studied the heart rate of pianists
while performing in front of an audience and found no significant heart rate differences between
musicians reporting experiencing anxiety from those who did not. In summary, the evidence

8
supporting the existence of a general trend in levels of arousal still needs to be proven before
being able to suggest that it may have adaptative or maladaptative effects on performances.
1.1.5 Stage Fright. Stage fright may be defined as a phenomenon that ―appears at the most
inopportune and inappropriate times and, in its most severe form, can cripple and end a most
talented and promising career […] Stage fright is the term used when describing anxiety and
blocked artistic expression, particularly when it is within the bounds of performing arts‖
(Rappoport, 1989, p. 1). Powell (2004) states that stage fright is a form of debilitating anxiety
similar to public-speaking anxiety and test-taking anxiety. He gives some examples of the impact
of stage fright on individuals:
The ―stage‖ (the theater, the athletic arena) varies, but the disabling
anxiety is constant. So worried is a gifted choral soloist about her ability to
hit the first note that she considers giving up singing altogether. Stage
fright constricts an orchestra conductor‘s physical range of motion to the
point that he feels unable to move his arms in rhythm to the music. High
tension causes athletes to under-perform during competition. (Powell,
2004, p. 802)
As reported by Salmon (1990), when stage fright and performance anxiety refer to
unwarranted and/or excessive fearfulness during performances, the terms may be used
interchangeably. This is also supported by Cox and Kenardy (1993): ―Performance anxiety, or
stage fright, is a situational manifestation of anxiety, and is related to the fear of making a
mistake or not being able to control one‘s actions in front of other people‖ (p. 49). The main
difference between stage fright and MPA is that while the latter includes both facilitating and
debilitating aspects, stage fright only encompasses negative components. In addition, Lederman
(1999) reports, from Salmon, that the use of the term stage fright ―has been criticized for ignoring
the anticipatory component, which may precede the actual performance by days or even weeks‖
(p. 117).
1.1.6 Music Performance Anxiety. To date, the most common definition of MPA comes
from Salmon (1990), and it states that MPA is ―the experience of persisting, distressful
apprehension about and/or actual impairment of performance skills in a public context to a degree
unwarranted given the individual‘s musical aptitude, training, and level of preparation‖ (p. 3).
This definition is used by a number of authors (Thurber, Bodenhamer-Davis, Johnson, Chesky &
9
Chandler, 2010; Kirchner et al., 2008; Gill, Murphy & Rickard, 2006; Liston, Frost & Mohr,
2003; Reitman, 2001; Widmer, Conway, Cohen & Davies, 1997) in the literature about MPA.
However, there are some conceptual issues with this definition, as MPA does not occur only if
there is an inconsistency between a) apprehension and b) musical aptitude, training and level of
preparation. In fact, age and levels of aptitude, training, experience and preparation were shown
to not have an impact on levels of MPA (Brotons, 1994; Cox & Kenardy, 1993; Wesner et al.,
1990; Wolfe, 1989).
Thurber (2006) reports another description from Salmon stating that MPA is ―the product
of interaction between fearful thought, autonomic arousal, and behavioral responses to a
perceived threat‖ (p. 7). In accordance with Salmon‘s statement, Lederman (1999) explains that
―performance anxiety consists of behavioral, cognitive, and physiologic symptoms and signs that
may precede and/or accompany a performance or presentation and that seem out of proportion to
the specific situation‖ (p. 117). Some researchers also support the use of a fourth component to
describe MPA manifestations: the affective (Osborne & Kenny, 2008; Emmons & Thomas, 2008)
or emotional symptoms (Stephenson & Quarrier, 2005; Brotons, 1994).
Kesselring (2006) suggests that MPA is ―a state of arousal and anxiety occurring before or
while a person is performing non-anonymously in front of an audience producing a valuable or
evaluated task touching on his/her self-esteem‖ (p. 309). However, this definition does not take
into account situations such as blind auditions (where musicians perform behind a screen, thus
performing ―anonymously‖ for a jury). Baker (2005) proposes a simple definition, although
ignoring the positive aspect that may also come with MPA: ―performance anxiety is the
exaggerated and sometimes incapacitating fear of performing in public‖ (p. 1).
Another way that may help define MPA comes from the relationship between performance
anxiety and social phobia. Authors such as Thurber et al. (2010) and Sataloff et al. (1999) argue
that performance anxiety is a form of social phobia if the criteria from the DSM-IV (American
Psychiatric Association, 2002) are met. On the other hand, a subsequent study by Powell (2004)
specifies that despite the fact that social phobia and performance anxiety may be related, the
latter term does not specifically appear among the social phobia criteria described in the DSM-

10
IV. In fact, a recent review of the DSM-IV (APA, 1994) and DSM-IV-TR (APA, 2002) shows
that performance anxiety is only briefly mentioned in the revised version, in a section on
differential diagnosis in social phobia (DSM-IV-TR, APA, 2002, p. 300.323): ―Performance
anxiety, stage fright, and shyness in social situations that involve unfamiliar people are common
and should not be diagnosed as social phobia unless the anxiety or avoidance leads to clinically
significant impairment or marked distress‖. Even if debilitating performance anxiety may be a
form of social phobia, Powell (2004) explains that it should be distinguished from generalized
social phobia and non-generalized social phobia (specific social phobia). Besides, specific
criteria should be developed because the extents to which the criteria are met differ between each
form. Table 1 shows that according to the clinical model proposed by Powel (2004, p. 805),
debilitating performance anxiety meets the criteria of social phobia, but to a smaller extent than
other social phobia disorders.
From this perspective, the criteria of social phobia from the DSM-IV may not be the most
appropriate way to define MPA. Indeed, research has shown that among musicians suffering
from performance anxiety, only 27% met the criteria of social phobia (Osborne & Franklin,
2002), while two musicians out of 94 met these same criteria when interviewed for a study about
assessment and treatment of performance anxiety (Clark & Agras, 1991).
Table 1. Distinguishing Debilitating Performance Anxiety From Two Other Social Phobia
Subtypes: A Clinical Model.
Distinguishing
Qualities
Social Phobia
Nongeneralized/
Specific Social
Phobia
Debilitating
Performance Anxiety
Overall impairment More pervasive Less pervasive Limited
Focus of fear Most interactions
with others
One or few
interactions with
others
Limited to specific
performance
situations
Expectations of self Low Moderate High
Fears of scrutiny by others Primary Primary Secondary
Anticipatory anxiety High High Variable
Commitment to feared
task
Avoidant Ambivalent Committed

11
Kenny (2009b) recently proposed a new definition of MPA that takes into account the
current knowledge about anxiety and is aligned with research on anxiety disorders and social
phobia.
Music Performance Anxiety is the experience of marked and persistent
anxious apprehension related to musical performance that has arisen through
specific anxiety-conditioning experiences. It is manifested through
combinations of affective, cognitive, somatic and behavioral symptoms and
may occur in a range of performance settings, but is usually more severe in
settings involving high ego investment and evaluative threat. It may be
focal (i.e. focused only on music performance), or occur co-morbidly with
other anxiety disorders, in particular social phobia. It affects musicians
across the lifespan and is at least partially independent of years of training,
practice, and level of musical accomplishment. It may or may not impair
the quality of the musical performance (p. 433).
Overall, there is no consensus among authors regarding an appropriate (and unequivocal)
definition for MPA and what it encompasses (McGinnis & Milling, 2005). Kenny‘s (2009b)
definition seems to be the most appropriate, but at this point, it is too recent to know if it will
achieve consensus in the scientific community. Nevertheless, this definition has been used in this
thesis as a basis for the questionnaire development and its theoretical approach.
In summary, despite the fact that stress, fear, anxiety, arousal, stage fright, and MPA all
create some kind of body response, they also have their own particularities. Stage fright focuses
on negative aspects of MPA. Arousal is an activation state that allows, when in the ideal zone, an
optimal performance, but when inappropriate, may affect the musicians‘ functioning in different
ways such as cognitively, physiologically, behaviorally and affectively (Emmons & Thomas,
2008). As for stress, fear and anxiety, Griebel and Nutt (2008) give the following explanation:
Stress represents an interaction between a particular type of environmental
stimuli (stressors) and a number of specific stress response systems
(namely hypothalamic-pituitary-adrenal (HPA) axis and/or
catecholamines). Anxiety and fear, on the other hand, constitute a set of
behavioral, cognitive and physiologic responses to threatening situations
or uncertainty. While fear often constitutes a normal response to a well-
defined threat, anxiety is often dissociated from the external stimulus, and
is not necessarily associated with a particular physiological response. (p.
455)
12
Music performance anxiety is a complex issue encompassing many components that may
affect performance quality and musician‘s well being. Many performers suffer from MPA, and
the prevalence of this phenomenon, high among the musician population, will be discussed in
Chapter 2.
1.2 Theories
The following section introduces multiple theories associated with the fields of psychology,
sports psychology and MPA. Not meant to be exhaustive, the following review focuses on the
theories related to the main goal of this thesis: the development of a psychometrically sound
questionnaire for the evaluation of MPA in popular musicians.
1.2.1 Theories from Psychology.
1.2.1.1 Lazarus’s theory of cognitive appraisal. According to Lazarus and Folkman
(1984), cognitive appraisal refers to the way individuals interpret or assess their situations. They
suggest two forms of appraisal: primary and secondary appraisal. Primary appraisal is related to
the evaluation of a situation, its issues, and its costs/benefits potential. In brief, when using the
primary type of appraisal, an individual assesses what is at stake and how much it matters for
him/her (Lazarus & Folkman, 1984). The secondary type of appraisal refers to the evaluation of
the own personal resources or coping options. Lazarus and Folkman (1984) explain that “a
fundamental feature of secondary appraisal is the extent to which the person senses that
something can or cannot be done to alter the troubled person-environment relationship” (p. 316).
Based on these claims, the interaction between threat, resources and demands may thus influence
stress levels. In a music setting, a high threat environment could be an audition for a renowned
orchestra, low resources could be the inability to manage stress effectively, and a high demand
could be a very difficult piece to perform. The interaction of these aspects may create high levels
of stress. On the other hand, performing a well-known repertoire (low demand) for an audience
of friends and family members (low threat) among whom one feels very confident (high
resource) may result in much lower levels of stress (if any)! The emotional response to a given
situation is thus triggered by the cognitive appraisal, which is influenced by biological variability,
temperament, learning experiences and socio-cultural factors (Kenny, 2011). Therefore, before
any emotional reaction occurs, the information has to be minimally processed. This processing

13
may be done through primary and secondary appraisal, as shown by Lazarus and Folkman
(1984), but also through the NUTS theory presented below.
1.2.1.2 Lupien’s recipe for stress: Don’t go NUTS! In 1968, the psychologist John Mason
published a review of psychoendocrine research on the sympathetic-adrenal medullary system (as
cited by Lupien et al., 2007). In his article, he identified three psychological determinants that
could increase the stress response in a majority of persons. Lupien et al. (2007) reported Mason‘s
findings showing that ―in order for a situation to induce a stress response by the body, it has to be
interpreted as being novel, and/or unpredictable, and/or the individual must have the feeling that
he/she does not have control over the situation” (p. 210). In their meta-analytic review,
Dickerson and Kemeny (2002) confirmed the importance of these determinants and proposed a
fourth component leading to physiological stress reactivity: the presence of social evaluative
threats (Dickerson & Kemeny, 2002).
Lupien‘s recipe for stress (Table 2, Marin, Schramek, Maheu & Lupien, 2009), which can
be remembered using the acronym NUTS, includes the three determinants from Mason, and the
one from Dickerson and Kemeny. Basically, it states that in order for a situation to be stressful, it
must encompass one or more of the determinants. In addition, the more the number of
determinants that are experienced, the more likely the situation may be interpreted as stressful
(Marin et al., 2009).
Table 2. The Four Determinants of Lupien‘s Recipe for Stress.
As explained on the Centre for Studies on Human Stress web site
(http://www.humanstress.ca/stress/understand-your-stress/sources-of-stress.html, retrieved on
June 8th, 2011), this recipe is universal, which means that it is not affected by the individual‘s
characteristics. The ―ingredients‖ are consistent for everyone because novelty, unpredictability,
N — Novelty
U — Unpredictability
T — Threat to the ego
S — Sense of control decreased

14
threat to the ego and decreased sense of control are common to all people. In other words,
regardless of the situation, once a person interprets an event as novel, unpredictable, threatening
and/or uncontrollable, it results in an increased level of stress.
1.2.1.3 Spielberger’s state-trait anxiety theory. According to Spielberger‘s state-trait
anxiety theory (1966, 1972), the anxiety phenomenon may be broken down into two components.
The first component, state anxiety, refers to an anxiety triggered by specific events or situations
(Watson, 2009). Weinberg and Gould (2007) report Spielberger‘s definition of state anxiety as
an emotional state ―characterized by subjective, consciously perceived feelings of apprehension
and tension, accompanied by or associated with activation or arousal of the autonomic nervous
system‖ (p. 79). This is a temporary, ever-changing mood state (Weinberg & Gould, 2007).
Unlike state anxiety, trait anxiety refers to the natural predisposition of an individual to
experience anxiety or to appraise situations as being threatening (instead of challenging). This is
a part of the individual‘s personality. As defined by Weinberg and Gould (2007), ―trait anxiety is
a behavioral disposition to perceive as threatening circumstances that are objectively not
dangerous and to then respond with disproportionate state anxiety. Highly trait-anxious people
usually have more state anxiety in highly competitive, evaluative situations than do people with
lower trait anxiety‖ (p. 79). In fact, individuals with high levels of trait anxiety may perceive
more often than others that situations are threatening, and/or react more intensively to stressful
situations (Arneson, 2010). There is thus an interconnection between arousal, state anxiety, and
trait anxiety.
1.2.2 Theories from sport psychology. In an attempt to describe a phenomenon as
complex as performance anxiety, various theories have been proposed over the years. Many new
theories are built on old ones. We present here theories from sport psychology that may apply to
the field of music, from the simplest to the more complex ones. These theories primarily explain
concepts such as arousal and performance, but anxiety and stress processes are also included.
1.2.2.1 The Yerkes-Dodson Law and Inverted-U Hypothesis. The Yerkes-Dodson law,
originating from experiments with mice (Kenny, 2011), illustrates the relationship between stress

15
and performance, using the concepts of eustress, distress, performance, illness, and emotional
arousal (Figure 1).
The inverted-U hypothesis from Landers and Arent (2001) is derived from the Yerkes-
Dodson law and explains the relationship between arousal and performance based on the
principle that optimal performance is achieved at a moderate level of arousal, while higher and
lower arousal levels impair performance. This principle is the same for both theories, but one
focuses on emotional arousal (Yerkes-Dodson law) while the other emphasizes physiological
arousal (inverted-U hypothesis).
Figure 1. Yerkes-Dodson Curve. This model illustrates that stress occurring before midpoint is
considered eustress, and beyond midpoint, distress. Performance and illness are displayed in an
inverted relationship (when one is up, the other is low). Moderate arousal is shown to be the
optimal performance point, while low arousal creates boredom and high arousal, an overwhelmed
state (Seaward, 2004).
The inverted-U hypothesis and the Yerkes-Dodson law take into account the fact that at
very high or very low levels of arousal, performance declines. However, questions remain
regarding the shape of the arousal curve, the nature of the arousal, and the fact that optimal
arousal always occurs at the midpoint (Weinberg & Gould, 2007). As pointed out by Salmon
(1990), ―the utility of the Yerkes-Dodson relationship lies in its implication that arousal states do
indeed provide a motivating force that is channeled and harnessed more effectively by some

16
performers than by others‖ (p. 5-6). Therefore, depending on how the situation is appraised, a
particular level of arousal may or may not help musicians optimize their performances (Salmon,
1990).
1.2.2.2 Individualized zone of optimal functioning (IZOF). The individualized zone of
optimal functioning (IZOF) from Hanin (as cited in Weinberg & Gould, 2007) provides an
alternative to the inverted-U hypothesis by demonstrating that optimal levels of state anxiety may
occur at any place in the continuum and vary from person to person (Figure 2). In addition, the
optimal levels of state anxiety are not depicted as single points but instead as zones, which may
seem more flexible and easier to reach.
Figure 2. Hanin‘s Individualized Zone of Optimal Functioning (IZOF). The zone of optimal state
anxiety may vary from one athlete to another in order to achieve the best performance (Weinberg
& Gould, 2007).
One of the weaknesses of Hanin‘s IZOF hypothesis is that it does not address ―whether the
components of state anxiety (somatic and cognitive anxiety) affect performance in the same way‖
(Weinberg & Gould, 2007, p. 89).
1.2.2.3 Multidimensional anxiety theory. To compensate for the weakness in Hanin‘s
IZOF hypothesis, Martens, Vealey and Burton (as cited in Kenny, 2011) created a theory
identifying somatic and cognitive anxiety as distinct components of competitive sport anxiety.

17
As explained by Kenny (2011), ―Somatic anxiety is a conditioned fear response associated with
the performance venue and cognitive anxiety is associated with the perceived probability of
success (or failure)‖ (p. 146).
The multidimensional anxiety theory is built on a time-to-event paradigm (Figure 3). It
shows that somatic anxiety stays relatively low before the event, then increases in the six hours
preceding the event and reaches a peak during the actual performance, while cognitive anxiety
stays high and stable until the end of the performance. A decrease in somatic and cognitive
anxiety occurs in the 24 hours following the performance.
Figure 3. Multidimensional Anxiety Theory. This representation of the time-to-event paradigm
(Kenny, 2011) shows that cognitive anxiety and somatic anxiety follow different paths before the
event, but not after.
1.2.2.4 Catastrophe model. Hardy‘s catastrophe model (as cited in Weinberg & Gould,
2007) illustrates the complex interaction between performance, arousal and cognitive anxiety
(Figure 4). It goes further than the IZOF model because it reveals that ―for optimal
performance[,] an ideal physiological arousal is not enough: It is also necessary to manage or
control cognitive state anxiety‖ (Weinberg & Gould, 2007, p.90 ).

18
Figure 4. The Catastrophe Model. This model illustrates the relationship between cognitive
anxiety, physiological arousal and performance (McNally, 2002). Optimal level of performance
is achieved when cognitive anxiety is low and when physiological arousal is at its highest point
on the inverted U shape.
The three-dimensional catastrophe model (Figure 4) shows the interconnections between
performance and physiological arousal, both being also impacted by cognitive anxiety. As
explained by Weinberg and Gould (2007), this model ―predicts that with low worry, increases in
arousal or somatic anxiety are related to performance in an inverted-U manner. With great
worry, the increases in arousal improve performance to an optimal threshold, beyond which
additional arousal causes a ‗catastrophic‘ or rapid and dramatic decline in performance‖ (p. 90).
Therefore, as summarized by Kenny (2011, p. 147), ―the principal thesis of the theory is that
physiological arousal (somatic anxiety) results in a performance catastrophe only when cognitive
anxiety is high‖.
1.2.2.5 The four-stage stress process. Weinberg and Gould (2007) suggest a simple model
adapted from McGrath, but also closely related to Spielberger’s state-trait anxiety theory, that
explains the stress process in four stages: (a) environmental demand, (b) personal appraisal, (c)
stress response, and (d) behavioral consequences (Figure 5).

19
Figure 5. The Four-Stage Stress Model. This model demonstrates that the stress process follows
a cycle in which each stage influences the next. At the end, behavioral consequences may
trigger a new set of environmental demands, which starts a new loop (Weinberg & Gould, 2007,
p. 82).
When a musician has to perform, an environmental demand, be it physical (like performing
a highly technical piece) or psychological (like being judged in a contest), is placed (Stage 1).
Then, the individual appraises the environmental demand as more or less threatening (Stage 2).
At this stage, trait-anxiety exerts a strong influence. After that, a stress response is elicited (Stage
3), which leads to behavioral consequences that may alter performance or its outcome (Stage 4).
This four-stage stress process acts as a continuing cycle because possible negative social
evaluations following the behavioral consequences (Stage 4) may create an additional demand on
the person (Stage 1). Therefore, the fourth stage feeds back into the first one and the cycle may
begin again.
1.2.2.6 Model of facilitative and debilitative anxiety. As seen previously, personal
appraisal plays an important role in the interpretation of anxiety symptoms. Jones’ model (as
cited by Weinberg & Gould, 2007) suggests that anxiety symptoms may be perceived as

20
facilitative (positive for the performance) or as debilitative (negative for the performance). As
seen in Figure 6, some stressors may come from the environment, while others may originate
from the individual’s trait anxiety and self-esteem. The sense of control related to positive or
negative expectancies may influence the perception one has of the symptoms as being facilitative
or debilitative. Therefore, the relationship between anxiety and performance may be significantly
affected by the way performers perceive their symptoms (Weinberg & Gould, 2007).
Figure 6. Jone‘s Model of Facilitative and Debilitative Anxiety (adapted from Weinberg &
Gould, 2007, p. 92). This model shows that the direction of anxiety is dependent on the
individual‘s perception of control.
To enhance performance, people can either learn to cognitively restructure their negative
expectancies into positive ones or try to improve their sense of control.
1.2.3 Music performance anxiety theories. As described previously, many theories from
psychology and sport psychology may be entirely or partially applied to MPA. MPA researchers
have also developed specific theoretical frameworks. As reported by Kenny (2011), theories and
models have been created by individual researchers like De Nelsky, Montello, and Wilson, and

21
by groups of authors such as Papageorgi, Hallam, and Welch. However, Kenny (2011) also
criticized these models and theories as being incomplete, imprecise, or conceptually incorrect.
Therefore, the theories presented below describe only two simple models that have been
empirically tested in the literature (Craske & Craig, 1984). They may provide an interesting way
to categorize the symptoms of MPA.
1.2.3.1 Lang’s three-system model of fear. Lang (1971) proposed a model in which three
interactive, yet partially independent systems (behavioral, physiological, and verbal), describe the
components of fear reactions (Craske & Craig, 1984). As explained by Salmon and Meyer
(1998), ―the cognitive [or verbal] component is represented by thoughts and related mental
images of risk or danger. The behavioral manifestation of anxiety is a tendency to avoid or
escape from anything perceived as dangerous. The physiological component of anxiety involves
the somatic reactions that accompany heightened arousal‖ (p. 126-127). It seems that the term
verbal system may be used interchangeably with the terms cognitive component (Salmon &
Meyer, 1998; Salmon, 1990) and affective reports (Lang, 1969).
The three-system model of fear may be interpreted in two ways: (a)
concordance/discordance, and (b) synchrony/desynchrony. As summarized by Kenny (2011),
―Concordance refers to the level of response equivalence between the three factors [behavioral,
physiological, and verbal] at any given time; synchrony refers to the rate of change of the three
factors. Desynchrony could take the form of independence or inverse relationships between the
factors‖ (p. 145). Craske and Craig (1984) further explain that ―the degree of concordance
depends upon the intensity of the emotional response and demand features of the situation. Under
conditions which evoke strong emotional responses, […] fearful individuals will respond with
comparably high levels of anxiety in each response system (i.e. concordance). In conditions that
do not evoke strong emotional responses, the three-system model predicts discordance‖ (p. 268-
269).
Even if Lang‘s model classically comes from psychological theories, it easily lends itself to
be applied to MPA theories. Indeed, Craske and Craig (1984) tested this theory with 40 pianists
using self-report measures (verbal system), judge ratings (behavioral system) and autonomic

22
measures (physiological system). Their results provided support for the three-system model by
showing that ―there was greater synchrony among the behavioral, self-report and autonomic
response systems in the relatively anxious group, whereas there was a greater tendency toward
desynchrony in the relatively nonanxious group […] These findings indicated that the three
response systems can vary independently, particularly when the individual is only mildly
stressed‖ (Craske & Craig, 1984, p. 277-278).
1.2.3.2 Salmon’s theory of MPA. Lang‘s model inspired other researchers to develop their
own theories. As an example, Salmon‘s theory of MPA refers to the following four principles:
1. MPA comprises a loosely correlated constellation of physiological,
behavioral, and cognitive variables.
2. The physiological component of MPA reflects arousal associated
with the automonic nervous system (ANS) which, largely through
conditioning, has become excessively associated with fear.
3. The anticipation of stressful events, musical or otherwise, can evoke
as much (if not more) anxiety than the event itself.
4. Psychotherapeutic interventions for MPA appear to be successful to
the degree that they address specific components (cognitive, physiological,
behavioral) of the overall profile of anxiety. (Salmon, 1990)
Salmon‘s first principle is based on Lang‘s model and the following principles target the
interaction between the same three components. Salmon also consolidates the link between his
theory and Lang‘s model by applying the synchrony/desynchrony approach: under very stressful
circumstances, the three components become highly activated and synchronized, while under less
catastrophic situations, they diminish and become desynchronized (Salmon, 1990).
1.2.4 Summary. Based on the various theories presented and the definitions provided
earlier, we categorized MPA into four domains: (a) the causes, (b) the temporal occurrence, (c)
the direction, and (d) the symptoms.
(a) As shown by Lazarus‘s theory of cognitive appraisal (Section 1.2.1.1) and Lupien‘s
recipe for stress (Section 1.2.1.2), once a situation is interpreted as threatening or
challenging, a body reaction is triggered. Weinberg and Gould‘s four-stage stress
model (Section 1.2.2.5) also supports this idea. Spielberger‘s state-trait anxiety theory
(Section 1.2.1.3) specifies that individual differences in personality traits may also have

23
an impact on anxiety levels during specific events. Therefore, musicians with high trait
anxiety may be more prone to experiencing high state anxiety in performance
situations. Hanin‘s individualized zone of optimal functioning (Section 1.2.2.2) takes
into account the fact that different types of performers may achieve optimal
performance at different levels of state anxiety. This shows that personality and
environmental demands are closely related to MPA. Therefore, these theories support
the importance of assessing the causes of MPA (i.e. personal and situational sources of
stress) to explain which factors may generate the most anxious reactions.
(b) Based on the multidimensional anxiety theory (Section 1.2.2.3), cognitive and somatic
anxiety may be partially independent of each other and may not be experienced at the
same levels prior to and during a performance. This theory shows that the peak of
anxiety occurs during the performance. However, some research has also shown that
the highest levels of anxiety occur just before the actual performance (Su, Luh, Chen,
Lin, Liao & Chen , 2010; Ryan, 1998; Salmon, 1990). It is, therefore, important to
further study the temporal occurrence of MPA.
(c) Jone‘s model of facilitative and debilitative anxiety (Section 1.2.2.6) describes how,
depending on the musician’s sense of control and his or her expectancies, the symptoms
may be interpreted as positive or negative to performance. The Yerkes-Dodson law
(Section 1.2.2.1) illustrates that arousal may be facilitating up to a certain point, beyond
which it becomes debilitating. The catastrophe model (Section 1.2.2.4) shows that great
worries combined with high arousal may create a rapid decline in performance. These
worries may thus be related to a form of debilitating anxiety. This model also
demonstrates that with low worry, the arousal is related to performance in an inverted-U
shape. These three theories show that MPA may be either positive or negative, based
on individuals’ perceptions and/or levels of arousal.
(d) Lang‘s three-system model of fear (Section 1.2.3.1) and Salmon‘s theory of MPA
(Section 1.2.3.2) are related to the symptoms experienced by musicians. As supported
by these theories, MPA reactions may be categorized into three components: somatic,

24
behavioral, and cognitive (the cognitive component may also be expressed as the verbal
system or the affective report, which will be further described in Chapter 2). At low
levels of anxiety, the symptoms are partially independent of each other, while at high
levels, they become synchronized. In the design of a new questionnaire, it is thus
essential to take into account each of these components when evaluating the symptoms
of MPA.

25
Chapter 2
Review of Literature
This review of literature reports findings on (a) prevalence of MPA among classical and
popular musicians, (b) gender differences, (c) the four domains selected for the questionnaire
design, (d) pre-existing measures, and (e) the types of validation used to establish the
questionnaire psychometric properties in psychological assessment.
2.5 Prevalence of MPA among Musicians
2.5.1 Classical musicians. Plaut (as cited in Kirchner, 2003) reported that 80% of people
experience anxiety when they become the center of attention. Some studies reveal that musicians
and singers have higher levels of anxiety than normative samples of the general population. This
makes them more vulnerable to occupational stressors such as performance anxiety (Kenny,
Davis & Oates, 2004; Wills & Cooper, 1987; Kemp, 1981). In his review of literature, Lederman
(1999) explains that the prevalence of MPA ranges “from about 16% to as high as 72%,
suggesting that the observed prevalence varies depending on how the question is asked as well as
who is asking, who is responding, and in what context” (p. 118). The following studies report
even broader ranges of results.
As shown in Table 3, the largest study on MPA prevalence was conducted by Fishbein,
Middlestadt, Ottati, Strauss and Ellis (1988). Other authors (Kenny, 2004; Montello, 1995;
Clark & Agras, 1991) still regularly report this study, especially as its results have been
supported by a subsequent research from Wesner et al. (1990). Recent studies also show that a
higher percentage of musicians is affected by MPA. In fact, MPA seems to affect between 59%
and 96% of musicians (Table 3).

26
Table 3. Studies on the Prevalence of MPA among Classical Musicians.
Authors Population Results
Miller & Chesky
(2004)
71 college musicians from the
University of North Texas
College of Music
83.1% experienced performance anxiety.
Bohne (as cited
in Güsewell,
2010)
Musicians from 19 Canadian
orchestras
96% experienced health problems more or less
associated with MPA.
James (1998) Musicians from 56 orchestras 70% were subject to MPA that had detrimental
effects on performances and 16% experienced it
more than once a week.
Van Kemenade,
van Son, & van
Heesch (1995)
155 professional musicians
from symphonic orchestras in
The Netherlands
59% suffered from debilitating MPA (severe enough
to affect performance quality). Anticipation anxiety
was experienced days before performance (36%);
weeks before performance (10%); and months
before performance (5%).
Salmon (1995) 154 musicians 69.5% were affected by MPA: 43% of this sample
experienced minimal or slight anxiety, 26% mild
anxiety, 21% moderate anxiety, 6% severe anxiety
and 4% extreme anxiety.
Cox & Kenardy
(1993)
32 music students at the
University of Newcastle’s
Faculty and Conservatorium of
Music
All experienced anxiety in performance contexts:
84% mentioned MPA as being detrimental to their
performances in opposition to 9.4% reporting that
anxiety was not. 6.2% of the sample considered that
MPA was only occasionally detrimental.
Wesner et al.
(1990)
302 students and faculty
members of the University of
Iowa School of Music
21% experienced significant distress while
performing and 16.5% experienced debilitating
MPA affecting their performance quality
Fishbein et al.
(1988)
2212 professional orchestra
members of the International
Conference of Symphony and
Opera Musicians
24% referred to stage fright as being a problem and
16% as being a severe problem.
While comparing the prevalence and levels of MPA between populations (students,
amateurs, and professional musicians), Steptoe and Fidler (1987) surveyed 41 music students
from Guildhall School of Music, 40 members of an amateur orchestra and 65 experienced
professional orchestral players (London Philharmonic and Royal Philharmonic). The authors
demonstrated that the music students had the highest levels of stage fright, followed by the
amateur group and then by the professional orchestra members (Steptoe & Fidler, 1987). Dews

27
and Williams (1989) studied sources of stress for 201 music students, and among the 22 issues
identified, stress and pre-performance nervousness were at the top of the list. Stage fright
appeared in the ninth position, preceded by depression. This research supports the findings from
Steptoe and Fidler (1987) and shows that students are concerned with MPA and other stress
issues.
Regarding the issue of age, Fishbein et al. (1988) showed that 19% of the musicians
between the ages of 35 and 45 years experienced severe stage fright, in comparison with 17%
for those under 35, and 11% for those over 45. Relationship between instrument types and stage
fright revealed that 22% of brass instrument players, 14% of string players, and 14% of
woodwind players reported severe stage fright. Among the other instrument types (e.g. harp,
percussion, keyboard), 17% of the players experienced severe stage fright (Fishbein et al.,
1988). Analysis was also made to compare ensemble types and stage fright: Ryan and Andrews
(2009) compared solo and ensemble performances among 201 singers in seven semi-
professional choirs and showed that, not surprisingly, performers perceived solo performances
as more stressful than ensemble performances. Fishbein et al.’s (1988) results suggest that the
smaller the ensemble, the more likely musicians may experience severe stage fright (17% in
small ensembles compared with 14% in large ensembles). However, the study does not mention
whether the relationships between age/stage fright, instrument type/stage fright, and ensemble
type/stage fright are statistically significant. This is important, since it may be compared with
other studies demonstrating that age (Kenny, 2006), number of years of experience as a
musician (Cox & Kenardy, 1993; Steptoe & Fidler, 1987), the type of the instrument played, and
the time spent playing (Gillespie & Myors, 2000) are not related to the incidence of MPA.
2.5.2 Popular musicians. Wills and Cooper (1987) report that popular musicians (this
study refers to jazz, rock, pop and commercial music performers) are about 15% more likely to
have above-average levels of psychological anxiety, as compared to the general population. This
trend is similar to the above-average levels of anxiety found in classical musicians (Kemp, 1981).
However, popular musicians differ from classical musicians because of the social nature of their
working environment (Gillespie & Myors, 2000). Indeed, they are more closely related to the
world of popular entertainment and "show business" (Cooper & Wills, 1989). Wills and Cooper

28
(1987) show that the main predictors of mental distress in popular musicians are performance
anxiety and performance-related anxiety. The authors explain that popular musicians set
themselves high standards, are prone to performance anxiety, and often have to ―endure
unpleasant circumstances related to playing, in order to bring entertainment to the general public‖
(Wills & Cooper, 1987). Popular musicians tend to be extraverted (Dyce & O‘Connor, 1994;
Marchant-Haycox & Wilson, 1992) and appear to be particularly subjective to stress, as conveyed
by reports of premature deaths and arrests for drug abuse in the popular press (Wills & Cooper,
1987), and as reflected by high levels of neuroticism (Cooper & Wills, 1989; Dyce & O‘Connor,
1994; Gillespie & Myors, 2000). Arneson (2010) and Kemp (1981) support the idea that the
level of neuroticism correlates directly with performance anxiety. However, the lack of studies
using populations of popular musicians shows a gap that needs to be filled in the literature. As
suggested by Kemp (1996), further research should thus be done solely on popular musicians,
especially as no measure assessing MPA has been validated using this specific sample (Osborne
& Kenny, 2005).
2.5.3 Gender differences. Gender difference is a significant factor to take into account
when assessing MPA. Demographic analysis has shown that MPA is two to three times more
likely in females (Kenny, 2006; Kenny et al., 2004). In fact, women tend to report more
impairment due to performance anxiety than men (Wesner et al., 1990) and mention at a higher
rate (19% vs 14%) that stage fright is a severe problem (Fishbein et al., 1988). They also tend to
perceive the audience as a threatening presence instead of a supporting one (LeBlanc, Jin, Obert
& Siivola, 1997). Women’s higher levels of anxiety are also supported by studies from Khalsa et
al. (2009), Papageorgi, Hallam and Welch (2007), Osborne and Kenny (2005), Kenny et al.
(2004), Osborne and Franklin (2002), and Sinden (1999).
Hamilton, Kella and Hamilton (1995) studied 48 elite performers in dance and music and
suggested that men are less able to cope effectively with occupational stress. Stephenson and
Quarrier (2005) explained that the patterns of anxiety sensitivity are affected by gender
differences: the association between fears of cardiovascular and respiratory symptoms and
performance anxiety is stronger in women, while the relationship between fears of lack of
cognitive control and performance anxiety is more strongly associated in men. Widmer et al.

29
(1997) studied the role of hyperventilation in MPA and found that women “were about three
times more likely than the males to suffer from a hyperventilation problem in a performance
situation or generally in life” (p. 97). This shows that hyperventilation may be an underlying
problem associated with MPA, particularly among women (Widmer et al., 1997). Osborne and
Kenny (2008) analyzed the causal relationship between sensitizing experiences and MPA in 298
teenager music students. They showed that female adolescents report more emotional distress
than male adolescents when they are asked to describe their worst performances and other
related situations (Osborne & Kenny, 2008). Leblanc et al. (1997) tested 27 high school band
members under three performance situations (alone in a practice room, in a practice room with
one researcher and in front of an audience in a rehearsal room). They found that females have
significantly higher heart rates than men in the first and third situations and thus that gender is a
significant predictor of heart rate variability during performance. The authors demonstrated that
even though women report higher levels of anxiety than men when performing in front of an
audience, they also perform better (Leblanc et al., 1997). Women’s higher levels of subjective
anxiety were also reported in a study from Abel and Larkin (1990), but the authors found that
men displayed greater increases in systolic blood pressure than women. This is consistent with
the research of Craske and Craig (1984) showing that female performers were mostly classified
as being relatively anxious (16 out of 24 women) but that they displayed less autonomic
reactivity than male participants (Craske & Craig, 1984).
Ryan (2004) studied gender differences among young musicians and presented a complex
relationship between MPA and gender in children. Measures of heart rate and behavior showed
that boys display more anxious behavior than girls before and while performing, and that their
heart rates exceed those of the girls during (but not prior to) the performances (Ryan, 2004).
Miller and Chesky (2004) showed that women are more negatively impacted by cognitive and
somatic symptoms of MPA than men, even though both genders report similar levels of
cognitive and somatic intensity (Miller & Chesky, 2004). Rae and McCambridge (2004) also
found that females report higher levels of MPA, but they pointed out that it might be due to the
fact that “females are more likely to openly express feeling anxious than males” (Rae &
McCambridge, 2004, p. 437), which is also supported by Abel and Larkin (1990). This is in
accordance with the findings of Brody and Hall (as reported by Kubzansky & Stewart, 1999, p.
30
80): “Research has found consistent evidence that women are considered to be more expressive
of and more likely to display anxiety, whereas men are considered to be more likely to display
anger”. Kubzansky and Stewart (1999) studied the relationship between anxiety, gender and
performance. They demonstrated that self-perceived levels of anxiety are similar between men
and women, but evaluators tend to perceive women as being more anxious than men
(Kubzansky & Stewart, 1999).
In summary, many studies demonstrate that there is a difference in the experience of MPA
between men and women. However, some research also shows that the relationship between
gender and MPA is complex and that self-perceived levels of anxiety are sometimes similar
between men and women.
2.6 Domains
Domains are broad categories targeting the facets of a construct of interest (adapted from
Haynes et al., 1995). In this thesis, the domains selected to represent MPA are namely the
causes, the temporal occurrence, the direction, and the manifestations. The following section
reviews the literature supporting the importance of assessing each of these domains.
2.6.1 Causes of MPA: Situational and personal sources of stress. Evidence suggests
that personal and environmental factors are associated with MPA (Esplen & Hodnett, 1999). As
supported by Robson, Davidson and Snell (1995), this shows that anxiety may be caused by
internal and external stimuli. Environmental factors (or situational sources of stress) refer to any
circumstances surrounding a performance that may have an impact on levels of MPA experienced
by the musicians. Emmons and Thomas (2008) propose examples of environmental factors that
may affect performers: (a) the presence of an audition panel; (b) another musician performing the
same repertoire; (c) the presence of the voice or instrumentalist teacher during an audition or
competition; (d) an opening night with press event; (e) an accompanist arriving late, etc.
Situational factors also include people on whom the performer depends. For instance, in music
ensembles, conductors are known to induce MPA (Emmons & Thomas, 2008). In fact, they
appear as the primary factor of anxiety induction in choral singers‘ experience of MPA (Ryan &
Andrews, 2009).

31
There is a strong relationship between personality and performance anxiety (Arneson,
2010; Meharg, 1988). Personality traits such as neuroticism, introversion, low self-esteem and
perfectionism have been associated with MPA (Papageorgi et al., 2007). General trait anxiety
has also been correlated positively with MPA (Cox & Kenardy, 1993; Hamann, 1982). Abril
(2007) explains that MPA may originate from past negative experiences. He claims that music
teachers and family members exert a great influence regarding the singer‘s identity and his/her
singing ability. This may shape the beliefs and may emotionally impact the individual for a long
time (Abril, 2007). Meharg (1988) explains that parents and teachers contribute to performance
anxiety by placing unrealistic expectations on music students. Musicians‘ previous experiences
have thus the power to alter the subjective appraisal of forthcoming performances: bad
experiences may create fear about performing again, while positive experiences may increase the
performer‘s confidence (Papageorgi et al., 2007). Therefore, MPA may be perceived as
facilitating or debilitating ―depending on a variety of personality and situational factors‖
(Kubzansky & Stewart, 1999, p. 77).
Apart from individual differences, certain situations are known to be more anxiety-
inducing than others. Cooper and Wills (1989) made in-depth interviews where popular
musicians reported the following sources of stress: performance anxiety, public ignorance, low
self-esteem, work overload or under-load, career development worries, and relationships at work.
A year later, Salmon (1990) suggested that causes accounting for increased anxiety included poor
technical skills, rigid performance rituals, inappropriate repertoire, and insufficient or
inappropriate practice habits. Then, Roland (1994) interviewed professional performers who
reported that the three main causes for MPA were a lack of preparation, feelings of insecurity,
and a lack of ability to perform a repertoire that is above the performer‘s level. Recently, Kenny
(2011) identified 22 causes for MPA in 357 professional orchestral musicians (Table 4). This
seems to encompass all previous research findings.
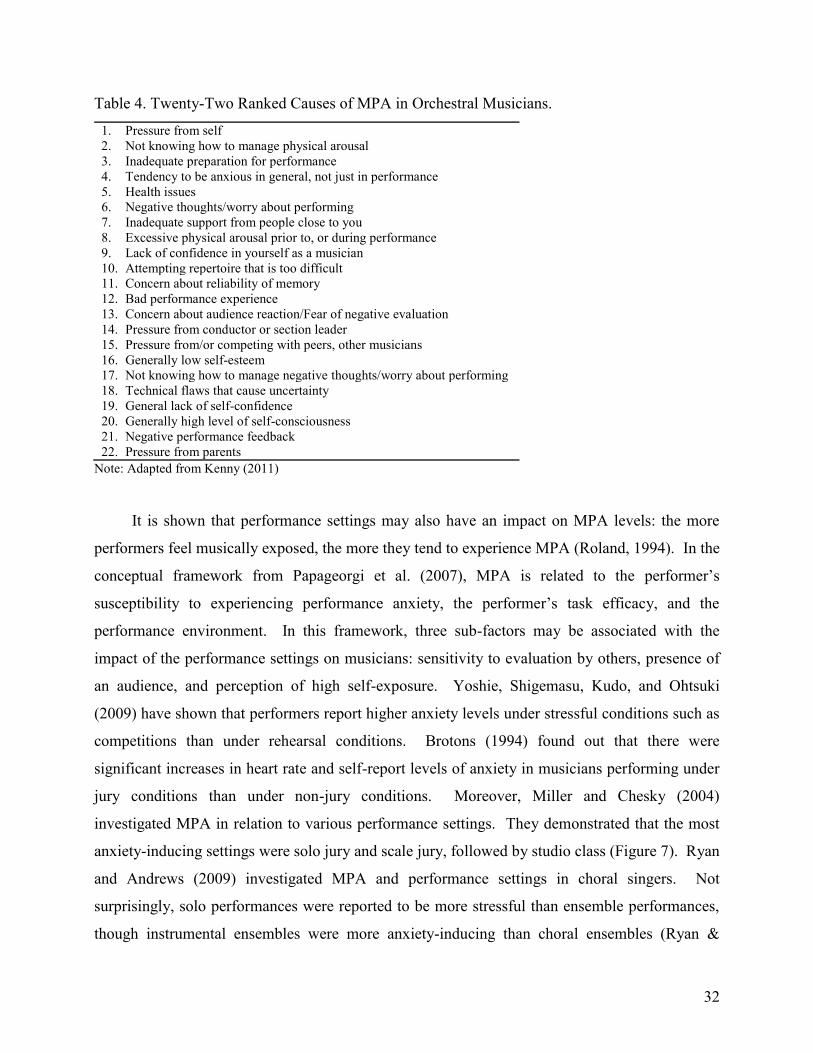
32
Table 4. Twenty-Two Ranked Causes of MPA in Orchestral Musicians.
1. Pressure from self
2. Not knowing how to manage physical arousal
3. Inadequate preparation for performance
4. Tendency to be anxious in general, not just in performance
5. Health issues
6. Negative thoughts/worry about performing
7. Inadequate support from people close to you
8. Excessive physical arousal prior to, or during performance
9. Lack of confidence in yourself as a musician
10. Attempting repertoire that is too difficult
11. Concern about reliability of memory
12. Bad performance experience
13. Concern about audience reaction/Fear of negative evaluation
14. Pressure from conductor or section leader
15. Pressure from/or competing with peers, other musicians
16. Generally low self-esteem
17. Not knowing how to manage negative thoughts/worry about performing
18. Technical flaws that cause uncertainty
19. General lack of self-confidence
20. Generally high level of self-consciousness
21. Negative performance feedback
22. Pressure from parents
Note: Adapted from Kenny (2011)
It is shown that performance settings may also have an impact on MPA levels: the more
performers feel musically exposed, the more they tend to experience MPA (Roland, 1994). In the
conceptual framework from Papageorgi et al. (2007), MPA is related to the performer‘s
susceptibility to experiencing performance anxiety, the performer‘s task efficacy, and the
performance environment. In this framework, three sub-factors may be associated with the
impact of the performance settings on musicians: sensitivity to evaluation by others, presence of
an audience, and perception of high self-exposure. Yoshie, Shigemasu, Kudo, and Ohtsuki
(2009) have shown that performers report higher anxiety levels under stressful conditions such as
competitions than under rehearsal conditions. Brotons (1994) found out that there were
significant increases in heart rate and self-report levels of anxiety in musicians performing under
jury conditions than under non-jury conditions. Moreover, Miller and Chesky (2004)
investigated MPA in relation to various performance settings. They demonstrated that the most
anxiety-inducing settings were solo jury and scale jury, followed by studio class (Figure 7). Ryan
and Andrews (2009) investigated MPA and performance settings in choral singers. Not
surprisingly, solo performances were reported to be more stressful than ensemble performances,
though instrumental ensembles were more anxiety-inducing than choral ensembles (Ryan &

33
Andrews, 2009). These results are similar to those of Cox and Kenardy (1993), who showed that
solo performances produced higher levels of MPA than group performances, and that group
performances produced higher anxiety than practice sessions.
Large ensemble
Lessons Small ensemble
Studio class Scale jury Solo jury
Performance Scenarios
Figure 7. Levels of Performance Anxiety Associated with Various Performance Requirements (Miller & Chesky, 2004). This demonstrates that levels of MPA increase in accordance with the
perception of self-exposure.
In summary, because they are more or less controllable by musicians, the causes of MPA
(be they personal or situational) may have an impact on levels of anxiety. They may also
provide valuable qualitative information to better understand the occurrence of MPA in
musicians. For example, musicians may experience debilitating anxiety in contexts such as
auditions and contests, but not in dress rehearsals or concerts; or they may be very stressed
during solo performances, but not during group performances, etc. Besides, learning which
causes increase MPA may help in guiding treatment: inappropriate repertoire may be adjusted,
new practice habits may be learned, communication with other musicians may be improved, etc.
Because of their impact on MPA, their valuable sources of information and their potential leads
to direct treatment, the causes of MPA are important to assess among music performers. In
addition, as MPA has been shown to be higher under specific performance contexts, targeting
only the most stressful situations when evaluating levels of performance anxiety may facilitate
the completion of the questionnaire by the musicians.

34
2.6.2 Temporal occurrence of MPA. Salmon‘s studies (1989, 1990) showed that the
anticipation of a performance may be more stressful than the actual performance. A performer‘s
stress may increase while waiting for the performance to begin, or in anticipation of problems to
occur during the performance (Salmon, 1990). It may also undermine the musician‘s confidence
(Nagel, 1990). Emmons and Thomas (2008) explain that ―pre-performance stress‖ may occur
anytime from weeks before the performance to seconds before walking on stage. It may also
happen at the beginning of the performance (Emmons & Thomas, 2008).
As pointed out by Lazarus and Folkman (1984), the temporal factor is an important
parameter of stressful situations. This factor includes components of imminence and duration,
which means that the levels of anxiety may be affected by the interval of time during which a
musician anticipates a performance, and by the duration of the performance. The temporal factor
may also influence threat and challenge appraisals. Yoshie et al.‘s findings (2009) support that
positive appraisal helps pianists to improve their performance quality. Indeed, the appraisal may
become more or less intense if musicians perceive their situation as harmful and dangerous, or as
stimulating and challenging. The manner in which musicians interpret their situations allows
them to manage stress through cognitive coping (challenging appraisal) or through more complex
coping processes (threat appraisal) like hyper vigilance, obsessive thinking, avoidance, etc.
(Lazarus & Folkman, 1984).
Salmon and Meyer (1998) suggest that experienced musicians, because of the way they
may interpret their stress, seem to master anxiety more easily than inexperienced musicians.
However, this does not mean that they are free of MPA. Salmon et al. (1989) showed that
experienced musicians were more likely to have an anxiety peak prior to the performance, while
less experienced musicians tended to reach a peak of anxiety during the performance. The four
time periods evaluated in that study were one day prior, one hour prior, during musical
performance, and overall average. In their study about the effect of relaxation breathing training
on MPA reduction, Su et al. (2010) demonstrated that the peak of anxiety occurred half an hour
before the performance. Ryan (1998) studied the timing of MPA in sixth-grade piano students
and found that perceived levels of MPA were the highest while entering the stage. The study
from Salmon et al. (1989) did not assess the timing of MPA as a continuum. Therefore, it failed

35
to show accurately the exact timing of MPA peaks as demonstrated in Su et al. (2010) and Ryan‘s
(1998) studies.
Güsewell (2010) makes a distinction between the temporal occurrence of performance
anxiety (Lampenfieber in German, or trac in French) and stage fright (Bühnenangst or
Podiumsangst in German, peur de la scène in French), and explains that while performance
anxiety diminishes once the performance has begun, the anxiety produced by stage fright remains
high, which prevents musicians from performing at their normal level and is counterproductive.
Wilson (2002) states that MPA may be detrimental if its highest level is reached during the
performance, but may serve a positive purpose when it occurs before the performance: it releases
an extra amount of energy that prepares the body to meet the demand of the performance
(Güsewell, 2010; Wilson, 2002; Nagel, 1993).
Imagining a threatening situation can evoke the same anxious reaction as being confronted
with a real danger (Esplen & Hodnet, 1999). This means that musicians thinking about a
stressful performance may activate the same body response as if they were actually performing.
As it has been shown that the anticipation of performing may be more stressful than the actual
performance (Salmon, 1990), using this pre-performance anxiety as an opportunity to practice
stress management techniques is an interesting treatment option. The temporal occurrence of
MPA is a significant factor to consider because it may assist in the selection and implementation
of appropriate coping strategies and treatment techniques (Salmon, 1990; Nagel, Himle &
Papsdorf, 1989).
2.6.3 Direction of MPA. The direction of MPA refers to the fact that anxiety may be
either debilitating or facilitating. Debilitating anxiety is detrimental for musicians and worsens
performances (Lehrer, 1990). Facilitating MPA, on the other hand, improves performances
(Lehrer, 1990). It is known that MPA comprises both a positive and a negative component (i.e. a
constellation of facilitating and debilitating traits) (Wolfe, 1989, 1990).
Like temporal occurrence, direction of anxiety is related to the musician‘s perception.
Indeed, musicians may appraise performances as threatening or challenging, resulting in

36
variations of self-perceived levels of MPA. Gould, Greenleaf, and Krane (2002) report that
depending on each individual‘s cognitive appraisal, the same levels of arousal may be perceived
as a form of excitement or anxiety. It was shown that anxiety levels were higher when events
were appraised as ―threatening‖ (Esplen & Hodnet, 1999). As explained by Hamann and Sobaje
(1983), even if musicians experience both positive and negative MPA, they usually put their
attention on the negative aspect of anxiety.
Many researchers (Kirchner et al., 2008; Ely, 1991; Wolfe, 1989; Meharg, 1988) support
the idea that a small amount of anxiety is essential to facilitate performance. Kirchner et al.
(2008) specify that some anxiety may be healthy and even improve performance if the musicians
feel highly confident about what they are doing. This is in accordance with Miller and Chesky
(2004) who showed that self-confidence, which was interpreted as facilitative, had an impact on
MPA. In addition, as reported by Gill et al. (2006), perceived control also influenced MPA.
Indeed, musicians who feel in control over a situation and have positive expectancies will be
more likely to interpret their anxiety as facilitating, regardless of the actual control they may
really exert. Conversely, musicians who perceive that they have a low personal control may
appraise MPA as more debilitating than facilitating (Mor, Day & Flett, 1995).
Stephenson and Quarrier (2005) found that negative performance outcomes were not
necessarily associated with moderate or moderately high levels of MPA. They reported that
negative effects were detected only at the highest levels of anxiety while positive effects were
detected at lower and moderate levels (Stephenson & Quarrier, 2005). This tendency is similar to
the one found in competitive sports (Brotons, 1994; Hamann & Sobaje, 1983). In a pilot-study
about MPA (Esplen & Hodnet, 1999), music students reported that a certain amount of MPA
enhanced performance. In accordance with the literature, the authors supported that there was an
association between performance quality and an optimal level of anxiety (Esplen & Hodnet,
1999).
It is to be noted that the distinction between facilitating and debilitating anxiety is unclear:
anxiety ranges from an almost non-existent stress to a pathological stage fright. Somewhere in
between these two extremes, there is an optimal level of anxiety (Güsewell, 2010). This follows

37
the same continuum as for the arousal, which goes from deep sleep to extreme excitement
(Kenny, 2011), but is tinged with an emotional appraisal. As explained by Salmon (1990), ―a
specific level of arousal may or may not optimize performance, depending on how it is
interpreted by the performer‖ (p. 5). Emmons and Thomas (2008) report that many singers
perceive stress as a facilitating phenomenon, but in order to manage MPA, those singers always
have to make an effort to think about performance in a positive way. In their study about the
effects of state anxiety on music performance, Yoshie et al. (2009) discovered that cognitive
anxiety direction positively predicted global performance. Osborne and Kenny (2008) found that
for teenagers, ―the presence of negative cognitions in the worst experience descriptions improved
the prediction of MPA over trait anxiety and gender alone‖ (p. 447). This is in accordance with
Lehrer (1990) who showed that debilitating MPA was associated with worry, judgmental
attitudes, concerns with the reactions of others, and concerns with distraction, while facilitating
MPA was related to the use of anxiety coping strategies and positive judgment of relative
performance quality.
Depending on personal appraisal, MPA can thus be perceived as facilitating or debilitating
(Yoshie et al., 2009). Gill et al. (2006) even suggest that the direction of anxiety may exert a
greater influence on a musician‘s performance than the intensity of anxiety experienced.
Therefore, it is a significant component of MPA assessment (Yoshie et al., 2009) and has to be
taken into account while developing a new measure.
2.6.4 Manifestations of MPA (symptoms). MPA is comprised of cognitive, somatic,
behavioral, and affective factors (or symptoms) interacting with each other (Kenny, 2009b;
Osborne & Kenny, 2008; Emmons & Thomas, 2008; Abril, 2007; Leary & Kowalski, 1995;
Brotons, 1994; Ely, 1991). Somatically, MPA symptoms may include muscle tension, tremors,
perspiration, altered heart rate and shallow respiration (Kenny, 2006; Osborne & Kenny, 2005;
Lehrer, 1987). Cognitively, the musician may demonstrate negative thinking regarding the
performance, difficulty in concentrating, and perfectionism (Kenny, 2006; Osborne & Kenny,
2005). Behaviorally, MPA may provoke increased complaining, avoidance, or external
manifestations such as nervous tics, fidgeting and pacing (Osborne & Kenny, 2005). Affectively,
the musician may show anger, irritability, guilt, shame, or worries (Emmons & Thomas, 2008).

38
Table 5 shows a non-exhaustive list of symptoms collected during the literature review process.
Table 5. MPA Symptoms Collected in the Literature and Classified into Four Components.
Somatic Cognitive Behavioral Affective
Headache Backache Muscle tension and stiffness Diarrhea Constipation Nausea/vomiting Dizziness Chest pain Cold hands Shaky hands Shaky legs Racing heart or palpitation Shortness of breath Irregular breath Dry mouth Lack of finger control Urge to urinate Perspiration Hot flashes Sweaty hands Feel apathetic Upset stomach Tiredness Numbness or tingling Feel jittery
Memory slips Inability to focus Narrowing of attention Decreased concentration Decreased decision-making Situation-irrelevant thoughts Negative thoughts Perfectionism
Impaired coordination Rapid talking Nail biting Foot taping Pacing Fidgeting Increased eye blinking Trembling/tremors Broken voice Lack of voice control Nervous tic “Freezing” Making performance errors Make up excuses like poor preparation or not feeling well Interpersonal problems with other musicians (back stage or on stage) Avoidance (avoid difficult passages, avoid performing alone, avoid more stressful performance like audition, etc.) Early leaving the venue Being late for performance Showing anger, fear, worry, shame or guilt
Feeling of panic
Feeling of overwhelmed Feeling of confusion Feeling of insecurity Feeling of inadequacy Feeling of meaninglessness or hopelessness Nervousness Restlessness Lack of confidence
Worries Guilt Shame Emotional instability: Overreaction Hypersensitivity Irritability Fright
Fear the worst Fear of failure Fear of judgment and disaproval
With increased anxiety, MPA manifestations may occur in all four components, creating a
synchronous activation of physiological, cognitive, affective, and behavioral factors. In less
catastrophic circumstances, the factors become desynchronized. This explains the variety of
symptoms expressed by performers (Salmon, 1990). Therefore, a musician may experience a
certain amount of anxiety regarding a performance without experiencing symptoms in all four
components (Abril, 2007).
The affective domain is often neglected in the experience of anxiety (Osborne & Kenny,
2008; Barlow, 2002). It is to be noted that the three-factor model of MPA (which includes the
somatic, cognitive, and behavioral factors) has been tested empirically and is well supported in
the literature (Kenny, 2006; Kenny & Osborne, 2006; Ryan, 2004; Reitman, 2001; Lederman,
1999; Salmon, 1990; Salmon & Meyer, 1998; Abel & Larkin, 1990; Wolfe, 1990; Lehrer, 1987;
39
Craske & Craig, 1984). It provides an appropriate theoretical basis to assess the various
dimensions of MPA. On the other hand, the fact that this model does not distinguish the
cognitive from the affective domain results in a less accurate classification.
In sport psychology, performance anxiety is usually divided into two components:
cognitive and somatic anxiety (Kenny, 2011; Weinberg & Gould, 2007; Martens, Vealey &
Burton 1990), which means that the behavioral and affective factors are taken apart. In music,
although they evaluate levels of self-confidence, which may be associated with the affective
domain, some researchers also classify MPA into somatic and cognitive anxiety (Yoshie et al.,
2009; Miller & Chesky, 2004).
The literature shows that the cognitive factor seems to have a strong impact on anxiety
levels (Osborne & Kenny, 2008; Stephenson & Quarrier, 2005; Liston et al., 2003; Craske &
Craig, 1984). In fact, cognitive manifestations of anxiety are more strongly related to
performance disruption than somatic (Yoshie et al., 2009; Stephenson & Quarrier, 2005,
Reitman, 2001; Kleine, 1990), affective and behavioral manifestations (Kenny & Osborne, 2006).
Indeed, Liston et al.‘s (2003) study showed that catastrophization (a cognitive symptom) explains
a large part of the variance in predicting MPA. Kirchner (2003) also reported that cognitive and
affective factors were predominant in experiencing MPA and had an impact on levels of self-
confidence.
The somatic domain is the easiest to recognize and characterize (Lederman, 1999; Ely,
1991) because it manifests itself as physiological symptoms of anxiety in the body. It interacts
with cognitive anxiety and may even contribute to its increase in some circumstances
(Stephenson & Quarrier, 2005; Wolfe, 1989). For instance, a flutist‘s dry mouth may cause
failure to produce a tone, which may then result in heightened cognitive anxiety (Wolfe, 1989).
Stephenson and Quarrier (2005) call the phenomenon anxiety sensitivity, which refers to ―the
tendency of the individual to be aware of or frightened by particular bodily sensations or
experiences‖ (p. 120). In their research about anxiety sensitivity, Stephenson and Quarrier
(2005) do not integrate a behavioral component into their description of anxiety. Instead, they

40
specify that trait and state anxiety are broad constructs that comprise cognitive, emotional and
physiological aspects (Stephenson & Quarrier, 2005).
According to the literature mentioned, the four components of MPA interact and
sometimes overlap. That makes it difficult to establish if they should be equally represented in a
self-report measure. Indeed, the cognitive factor seems to play an important role in the
experience of MPA. However, as the affective component is very often merged into the
cognitive component, the analysis to find out if one is a stronger predictor of MPA than the other
may be problematic. Another important aspect is that the behavioral domain seems difficult to
self-evaluate accurately because musicians are usually not the most objective judges of
themselves. In fact, musicians tend to focus on symptoms that are specific to their instruments
(Gill et al., 2006). Therefore, it is important to create a sample of items that is thorough, in order
for it to be representative, no matter what is the played instrument. It is also important to
remember that the number of symptoms experienced during a performance may not be as
important for the musicians as the actual intensity of the symptoms (Gould et al., 2002).
2.3 Pre-existing Measures Related to MPA
The previous sections helped in determining the important parameters regarding MPA and
in selecting the domains to be assessed by a new measure on performance anxiety. The literature
review also helped in finding pre-existing questionnaires and inventories on MPA. As mentioned
earlier, Osborne and Kenny (2005) identified 20 questionnaires on MPA. The authors reviewed
the psychometric properties for each of them (which included descriptions of normative sample,
sample size, item analysis, means and standard deviations, concurrent validity, predictive
validity, test–retest reliability, test procedures, and tester qualifications) and showed that none of
the measures established predictive validity and test-retest reliability.3 Among the pre-existing
questionnaires identified above, three inventories have been selected as silver standards4 for the
validation process and are presented below.
3 For more information on the psychometric properties of these 20 questionnaires, articles from Kenny (2006) and
Osborne and Kenny (2005) are suggested. 4 Gold standards refer to measures that have been ―used and accepted in the field‖ (Streiner & Norman, 2009, p. 254)
and that are ―considered accurate‖ (Hulley, Cummings, Browner, Grady, Hearst & Newman, 2001, p. 43). Because
psychological and/or behavioral measures cannot prove without any doubt that they represent effectively and
accurately a construct of interest, they are considered as silver standards.

41
1) The Performance Anxiety Inventory (PAI) from Nagel et al. (1989) comprises 20 items based
on the three-factor model of anxiety (somatic, cognitive and behavioral), and assesses MPA with
a four-point scale of frequency ranging from 1 (almost never) to 4 (almost always). The range of
possible scores goes from 20 to 80. The PAI takes around 5 minutes to complete. The reliability
of this measure was calculated with a Cronbach‘s alpha score of 0.89 (Nagel et al., 1989), which
is considered high (Streiner & Norman, 2009). This inventory has also been utilized in many
studies (Chang, 2001; Deen, 1999; Stanton, 1994). On the other hand, the PAI cannot be
categorized as a gold standard because it assesses only the frequency of MPA symptoms, without
taking into account the direction of anxiety (facilitating/debilitating) and the potential causes for
heightened anxiety levels.
2) The revised Kenny Music Performance Anxiety Inventory (revised K-MPAI) from Kenny
(2009a) is a self-questionnaire comprising 40 items assessed with a 7-point scale of endorsement
(strongly disagree to strongly agree). The range of possible scores goes from 0 to 240.
Completion of this inventory takes 10 to 12 minutes. The first K-MPAI demonstrated a high
internal consistency, with a Cronbach‘s alpha score of 0.94 (Kenny & Osborne, 2006). The alpha
reliability coefficient for the revised K-MPAI has not been published yet. Both the first and the
revised K-MPAI inventories have a scale system similar to the one used for the PerfAIM (Likert
scale of endorsement) and can be used as a predictive measure and as an evaluative measure
sensitive to change (Kenny & Osborne, 2006). However, their theoretical framework differs
from the PerfAIM: the aim of the K-MPAI (and revised K-MPAI) is to explore the inter-
relationships between state/trait anxiety, occupational stress, perfectionism, aspiration and MPA
(Kenny et al., 2004). The items are thus too broad to assess only MPA. Besides, the revised K-
MPAI does not encompass the same somatic, cognitive, affective and behavioral domains used in
the PerfAIM. The items are therefore quite different. The revised K-MPAI, though promising, is
categorized as a silver standard because all the psychometric properties of this inventory are not
available at this point.
3) The State-Trait Anxiety Inventory (STAI) from Spielberger (1983) is one of the most
frequently used assessment instruments for MPA (Osborne & Kenny, 2005; Widmer et al.,

42
1997; Brodsky, 1996). Even though it is primarily a tool used by psychologists to evaluate
anxiety disorders, it lends itself easily to an application for MPA. The STAI assesses state (or
situational) anxiety (STAI-S) and trait (or general) anxiety (STAI-T). The questionnaire
comprises 20 items in each category (state and trait), and the answers are collected with a four-
point scale of frequency ranging from 1 (never) to 4 (almost always). STAI completion takes
around 5 minutes per subscale. Usually, only the state-anxiety subscale (STAI-S) is used to
conduct researches related to the occurrence of MPA in performance contexts (Osborne &
Kenny, 2005) because subjects may report their symptoms at a particular point in time (e.g. just
before performing). The STAI possesses the required psychometric properties, including good
construct validity and high internal consistency, but only assesses the intensity of symptoms and
cannot be used retrospectively. Besides, since it was created to diagnose anxiety disorders,
some statements are too general and not always pertinent for musicians.
2.4 Questionnaire Design and Validation
Validation is a process that aims to assess the accuracy of the measure in representing the
construct of interest (Hulley et al., 2001), i.e. MPA. Validity thus represents the degree to which
the interpretation of scores is an adequate reflection of the construct to be measured. The goal of
the validation process is to verify that the measure is actually measuring what it is supposed to
measure, in order to be able to make valid assumptions from the results of the questionnaire. In
fact, a scale appropriately validated allows a researcher to make accurate inferences about an
individual (Streiner & Norman, 2009).
There are different types of validation that may be used to establish the psychometric
properties of a questionnaire. Those selected for the PerfAIM validation are briefly described
below.
Content validity is a form of validity that evaluates the degree to which the content of the
instrument is an adequate reflection of the construct to be measured (Haynes, Richard, &
Kubany, 1995). Streiner and Norman (2009) specify that content validity ―differs from other
forms of validity testing in one important aspect: it is not based on the scores from the scale,
differences between people, or changes based on some intervention; only on the judgment of

43
experts regarding the content of the items‖ (p. 253). Items must thus be generated and selected
carefully to ensure that the content effectively represents the selected construct. Vogt, King and
King (2004) support the use of focus groups as a way to enhance content validity. Focus groups
are also mentioned to be a component frequently overlooked in content validation procedures
(Haynes et al., 1995). In fact, a review of the existing measures about MPA (Kenny, 2006;
Osborne & Kenny, 2005) shows that none of the authors report their procedure about
questionnaire development, except when the questionnaire was adapted from pre-existing
measures. As mentioned by Vogt et al. (2004), ―content validity includes, but is not limited to,
careful specification of constructs, review of scaling procedures by content-validity judges, and
consultation with experts and members of the population‖ (p. 232). Haynes et al. (1995) provide
further guidelines to establish content validity.
Face validity is a part of content validity and represents the degree to which the items of the
measure look as if they are an adequate reflection of the construct to be measured, i.e. the degree
to which the items appear pertinent, practical and related to the construct (Nevo, 1985). It is a
―subjective judgment about whether a measurement makes sense intuitively, whether it is
reasonable‖ (Hulley et al., 2001). Nevo (1985) suggests using an absolute method to rate a
measure and its item on a 5-point scale ranging from extremely suitable (5) to
irrelevant/unsuitable (1). Face validity may be important to assess because, as explained by
Streiner and Norman (2009), ―if the item appears irrelevant, then the respondent may very well
object to it or omit it, irrespective of its possibly superb psychometric properties‖ (p. 83).
Therefore, it may help to assess if people who use and/or administer the questionnaire agree that
the measure is acceptable (Haynes et al., 1995).
Concurrent criterion-related validity is the degree to which scores of the instrument are an
adequate reflection of a gold standard (Foster & Cone, 1995; Streiner & Norman, 2009). If a
gold standard cannot be found (because it still does not exist or because it is impossible to prove
without any doubt that it can effectively assess the construct), investigators can rely on silver
standards (i.e. validated psychological and/or behavioral measures). In order to verify the
concurrent criterion-related validity, scores of the measure to be validated are compared and
correlated with scores of other established questionnaires.

44
Construct validity (convergent and divergent) is the degree to which relationships of
different instrument scores adequately reflect the constructs to be measured (Streiner & Norman,
2009). In order to estimate convergent validity, scores of similar domains have to be correlated
(Foster & Cone, 1995). If a positive correlation exists between scores from different
questionnaires, it means that there is a relationship between the measures and that they all
converge toward the same construct. The higher the correlation, the stronger is the relationship
(thus, the more valid is the new measure). To estimate divergent validity, scores from divergent
domains (e.g. scores relative to cognitive symptoms with scores relative to behavioral symptoms)
must be compared to verify how they correlate. If the validity is good, the correlation between
scores from divergent domains will be lower than the correlation between scores of similar ones.
A measure must not only be valid, it must also be reliable. Reliability refers to
reproducibility, repeatability or consistency of scoring. More precisely, it is ―usually quoted as a
ratio of the variability between individuals to the total variability in the scores‖ (Streiner &
Norman, 2009, p. 7). Internal consistency and stability provide ways to assess reliability. The
internal consistency is the extent to which the items correlate in their assessment of the
underlying construct. It represents ―the average of the correlations among all the items in the
measure‖ (Streiner & Norman, 2009, p. 8). Kenny (2006) describes the internal reliability as the
consistence of a measure within itself, which occurs when ―all the items are measuring the same
construct or psychological factor‖ (p. 59). The stability refers to the extent to which the
questionnaire provides the same results on repeated trials (test-retest). As explained by Streiner
and Norman (2009, p. 7), ―a first step in providing evidence of the value of an instrument is to
demonstrate that measurements of individuals on different occasions […] produce the same or
similar results‖.

45
Chapter 3
Methods
The goal of this thesis is to develop and validate a new questionnaire to assess MPA in
popular musicians. To determine the psychometric properties of the PerfAIM, the validity and
reliability of the measure need to be calculated.
This chapter begins by presenting the population, the ethical considerations, and the
instrumentation used for the project. In the later parts, the chapter describes how content validity
and face validity were established based on a two-phase process using samples of music students
and experts, and how concurrent criterion-related validity, construct validity (convergent and
divergent), internal consistency, and test-retest reliability were estimated using a sample of
popular musicians.
3.1 Overview, Population and Settings
The recruitment of participants was divided into three phases: (a) Focus group sessions
(item generation process); (b) Interviews with experts (item reduction process); and (c) Online
questionnaire completions with popular music students and musicians (questionnaire validation).
The first two phases lasted between 30 and 60 minutes each, while the third phase lasted around
20 minutes.
Phase 1 (Focus Groups): The population for the development of the measure consisted of
music students from the Schulich School of Music (McGill University) attending courses
related to MPA (―Practicing and Coping Strategies for Performance Enhancement‖ and
―Coping Strategies for Optimal Performance‖, respectively for undergraduate and graduate
music students). One week before the focus group, the project was explained to each class
and participants were recruited. Recruitment material and consent forms are provided in
Appendices A and B. The focus group took place during class hour. Those not wanting to
participate were free to leave at any time. The professor left the classroom during both the
recruitment and the focus group to ensure that no one felt any obligation to participate. In the
end, six undergraduate students and seven graduate students participated in the first phase.

46
Demographic data are summarized in Table 6.
Table 6. Demographic Information – Phase 1 (Focus Groups).
Phase 2 (Interviews with Experts): Recruitment of the sample was carried out via e-mail and
telephone, and each participant signed a consent form (Appendices A and B). In total, 12
experts (four women and eight men) were interviewed. The interviews were divided into
three rounds: six experts participated in the first round (six men), three in the second round
(one man, two women), and three in the third (one man, two women). All of the experts had
completed graduate studies. Regarding their occupations, 12 of them were university
professors in the fields of music performance, music education, psychology and kinesiology.
They were recruited at McGill University (Montreal), Conservatoire de musique du Québec
(Québec), Berklee College of Music (Boston), and University of Sydney (Australia). Among
them, three were also professional jazz musicians. A neuropsychology PhD candidate
specializing in human stress was also interviewed.
Sample of undergraduate and graduate music students
MUGT-474 (Undergraduate)
MUPP-694 (Graduate)
Gender Male 3 50% Female 3 50% 7 100%
Age Range 19-23 22-30 Mean (SD) 21 (1.87) 23.7 (2.87)
Full-time occupation Student 4 66.6% 4 57.1% Student and
music teacher 1 16.7% 1 14.3%
Student and freelance musician
1 16.7% 2 28.6%
Primary instrument Violin 1 16.6% 3 42.8% Piano 1 16.6% 1 14.3% Flute 1 16.6%
Cello 1 16.6% Sax 1 16.6% Bass 1 16.6% Viola 2 28.6% Voice 1 14.3%
Years of musical Range 6-16 10-26 training Mean (SD) 12.5 (3.50) 16.7 (5.40)
Hours of practice/week
Range Mean (SD)
6-25 16.5 (5.71)
4-30 18.7 (8.76)
Most frequently Classical 4 66.7% 7 100% performed style Jazz 2 33.3%
Has MPA been Y 5 83.3% 6 85.7% previously experienced?
N 1 16.7% 1 14.3%
Is MPA still frequently Y 4 66.7% 5 71.4% experienced? N 2 33.3% 2 28.6%
Is medication taken to control anxiety?
N Missing answer
4 2
66.7% 33.3%
7
100%

47
Phase 3 (Online Questionnaires): Music students were recruited at rehearsals of Jazz
Ensembles and Big Bands at McGill University. The online questionnaires were sent through
list servers. Professional musicians were recruited via e-mail. An invitation was also sent to
students from the following universities: British Columbia, Manitoba, and Toronto. More
than 370 persons were contacted. Recruitment and consent material is provided in
Appendices A and B. Of the sample, 69 persons participated (38 men and 32 women): 62
completed the entire questionnaire booklet (90% of the sample) and seven (10%) partially
filled it out. Among the sample, 21 musicians agreed to be part of the reliability testing and
completed the PerfAIM a second time one week later. Demographic information is
summarized in Table 7.
Inclusion criteria for the subjects were to be over 18 years of age and to be fluent in
English. For the third phase, music students and professional musicians following a treatment
including psychotropic medication (e.g. antidepressant, lithium) were excluded to avoid any bias
that might be induced by changes in perception, mood, consciousness, cognition, and behavior
(Hulley et al., 2001). In order to respect the inclusion criteria, demographic information was
collected right before each phase of the study. After the completion and submission of the online
questionnaires, the subjects‘ demographic information was verified and the data of participants
who did not meet the inclusion criteria were excluded. These data and demographical information
were all destroyed. Overall, three subjects (two men and one woman) did not meet the inclusion
criteria and were thus excluded from the study.
No financial compensation was offered to the participants of the first two phases. In order
to encourage participation for the completion of the online questionnaire booklet, musicians were
invited, on a voluntary basis, to provide their name and e-mail address at the end of the
questionnaire in order to get a chance to win one of three ITune gift-cards of 25$ that were drawn
on May 1st, 2011.

48
Table 7. Demographic Information – Phase 3 (Online Questionnaires).
3.2 Ethical Considerations
The Research Ethics Board Office of McGill University reviewed and approved this
project. All participants were asked to complete an informed consent form (Appendix B) and to
provide demographic information. The consent form stated the purpose of the project and
described the participants‘ requested tasks. Through the study, participants were assured of
confidentiality and were told that they could withdraw from the project at any time, should they
so choose. The names and contact information of the researchers were provided. All subject data
Sample of popular professional musicians and music students
Raw data Percentage
Gender Male Female
38 31
55% 45%
Age Range 18-53 Mean (SD) 29 (8)
Education High school 5 7 %
Cegep 13 19% University 51 74%
Full-time occupation Student Musician
27 24
39% 35%
Music teacher 6 9% Musician and music teacher
Other Unemployed
4 7 1
6% 10% 1%
Primary instrument Guitar Voice
18 13
26% 19%
Bass/Double bass 14 20% Piano 10 15%
Drum/Percussion 3 4% Saxophone
Trumpet Trombone Violin Flute
3 3 2 2 1
4% 4% 3% 3% 1%
Level of musical proficiency
Beginner Intermediate
1 6
1% 9%
Advanced Professional/Expert
25 37
36% 54%
Hours of practice/week Range Mean (SD)
0-40 11.4 (9.5)
Training style (1 missing answer)
Pop and/or other non-classical styles Classical
41 4
59% 6%
Both 23 33%
Most frequently performed style
Pop and/or other non-classical styles Classical
63 0
91% 0%
(1 missing answer) Both 5 7%
Has MPA been Yes 59 85%
previously experienced? No 10 15%
Is MPA still experienced frequently?
Yes No
21 44
32% 68%
Use of alcohol to Yes 8 12% manage MPA No 61 88%
Use of drugs to Yes 2 3% manage MPA No 67 97%

49
were kept confidential and were stored in a locked space. Subject names on documents were
replaced by identification codes whenever possible.
3.3 Instrumentation
As mentioned in Section 2.3, in order to verify the different types of validity for the
PerfAIM (concurrent criterion-related validity and convergent/divergent construct validity),
comparison and correlation with other selected questionnaires were carried out. The three self-
administered questionnaires selected to serve as silver standards to evaluate self-perceived MPA
and symptoms of anxiety were the PAI (Nagel et al., 1989), the revised K-MPAI (Kenny, 2009a)
and the STAI-Trait subscale (Spielberger, 1983). For the study, all questionnaires were provided
in a computerized format.
3.4 Content Validity
Content validity was achieved through the six following steps:
1. Establishment of a rationale for the proposed study and selection of a specific
research question. This step was described in detail in the introduction and in
Chapter 1 of this thesis. In addition, definitions (Section 1.1) and current theories
(Section 1.2) were presented in order to provide a solid theoretical framework for
the questionnaire design.
2. Review of the literature on MPA. Chapter 2 reported a literature review on the
prevalence of MPA in musicians, on the parameters influencing MPA (domains)
and on pre-existing measures assessing performance anxiety. This review of
literature was the first step toward the item generation process: it helped in
creating a pool of items, in finding a major construct and its domains, in
comparing the existing measures (instructions, items, formats, scales and response
options, etc.), and in establishing the needs and requirements for the questionnaire
development. In addition, books on research methods and measurement were
consulted to ensure that methodological issues were avoided.
3. Confirmation of the major domains of MPA. Focus groups with students and
interviews with experts were organized to consolidate the major domains gathered
from the literature review and to verify their relevance.

50
4. Generation and selection of the items for each domain. The items were
designed using the pool of items created previously and were refined based on the
suggestions from the participants of the focus groups and the experts‘ interviews.
Wording was adjusted to make sure that the same information would be obtained
in different ways, which would confirm the reliability of the questions and the
participant‘s response.
5. Reduction of redundant items. The items were mainly reduced based on the
ratings from the experts. To assess the items, the experts rated each statement
using a 5-point scale of importance ranging from 1 (Not important/relevant) to 5
(Extremely important/relevant). If fewer than 80% of the experts rated an item
above 3, the item was dropped (Streiner & Norman, 2009). However, because the
interviews were divided into three rounds and as there were minor changes
between each round, last decisions about keeping or removing specific items for
the final version had to be taken by the investigators of this study.
6. Revision of the questionnaire for item clarification and fulfillment of the
intended purpose. Experts were asked to re-word any item that seemed unclear
to them, and to propose new items that may have been missed. After the
interviews, the PerfAIM was revised one last time based on the comments from
the experts. It was also ensured that the items were worded in a language suitable
for a 12-year-old, as suggested by Streiner and Norman (2009).
3.5 Face Validity
Face validity was established by interviewing experts. To select the experts, Nevo (1985)
suggested that raters should be individuals representing the population for whom the test is
designed, individuals working with the test results, and individuals taken from the general
population. For this project, the selected experts were part of the first two categories and
included professional jazz musicians and instructors at McGill University, psychologist(s), music
professor(s) and researchers. However, no member of the general population was included
because the questionnaire is specifically designed to assess parameters related to music, which
would not be relevant to non-musicians.

51
Expert-participants were asked to rate the validity of the PerfAIM using the absolute
method (i.e. assessing the whole questionnaire, as well as the construct, domains, and items using
5-point scales of clarity, relevance, importance, or appropriateness, depending on the context).
Preliminary data collection and statistical analysis were carried out by calculating the means,
standard deviations, distributions of responses, and percentages of endorsement. It is important to
note that one expert completed the content validity questionnaire twice (once in the first round
and once in the third one), which means that a portion of the statistical analysis was done with 13
experts.
3.6 Scores and Means
After completion of the questionnaire by the sample of 69 musicians, scores and means
were compiled. The distribution of scores was also established. Additionally, scores and means
were reported by gender and by level of musical proficiency. Finally, the means and standard
deviations were calculated for each item of the PerfAIM.
3.7 Internal Consistency Reliability
To establish homogeneity or internal consistency reliability (Streiner & Norman, 2009) of
the PerfAIM, the item correlation was calculated using Cronbach‘s Coefficient alpha, with the
expected values of 0.7 to 0.9 (Streiner & Norman, 2009; Portney & Watkins, 2009). This
calculation was done using the PerfAIM data gathered from the respondents involved in the
validity testing (69 musicians). The internal consistency of the items was computed for the
whole questionnaire as well as for each domain.
Gender stratification was performed by analyzing results for men and women separately.
In this way, the relationship between gender and MPA levels was examined to verify if this
variable had a confounding effect on the results. This was done by comparing stratified analyses
with un-stratified analyses, and by determining if the results significantly differed from one
another (Hulley et al., 2001).

52
3.8 Test-Retest Reliability
From the initial sample recruited for the validity test, more than 20 participants (Hobart,
Cano & Thompson, 2006) were asked to fill out the PerfAIM a second time, one week later, to
assess test-retest reliability. Twenty-one participants completed the questionnaire under the same
circumstances (i.e. receiving an invitation through e-mail and filling out the same computerized
version of the PerfAIM) to confirm test-retest reliability (Streiner & Norman, 2009). Completion
time did not exceed 10 minutes.
To analyze test-retest reliability between the scores of these two test sessions, the intra-
class correlation coefficient (ICC) was calculated, with an expected value greater than 0.75
(Portney & Watkins, 2009). As the questions of the questionnaire were mandatory, there was no
missing answer in the data.
3.9 Concurrent Criterion-Related Validity
To assess the concurrent criterion-related validity (Streiner & Norman, 2009) of the
questionnaire, participants were asked to complete a questionnaire booklet, which contained the
PerfAIM, the PAI (Nagel et al., 1989), and the revised K-MPAI (Kenny, 2009a). Questionnaire
booklet completion lasted between 15 and 30 minutes. The correlation results of these tests
illustrated the degree of concurrent validity of the questionnaire. Standardized means were
utilized. Acceptable expectable values were in the range of 0.3-0.4 (Osborne & Kenny, 2005).
Standards for educational and psychological testing (as cited in Osborne & Kenny, 2005)
suggested at least 100 participants per subgroup as a minimum criterion for adequate sample
sizes, but Hobart et al. (2006) reported that a sample size of 40 participants was considered
sufficient to estimate the validity of a questionnaire. It was thus expected to recruit at least 40
participants to establish concurrent criterion-related validity. As mentioned in Section 3.1, 69
persons filled out the PerfAIM, but all of them did not complete the questionnaire booklet (three
persons stopped before filling out the PAI, and eight persons did not fill out the revised K-
MPAI). In the end, 66 people completed both the PerfAIM and PAI, and 61 completed both the
PerfAIM and the revised K-MPAI.
53
3.10 Construct Validity (Convergent and Divergent)
To assess construct validity, measures using the same theoretical framework must be
utilized. In order to do the statistical analysis, results of the PerfAIM were thus correlated with
scores on the PAI (Nagel et al., 1989). Like in the concurrent criterion-related validity testing, a
sample size of 66 individuals was used. Standardized means were also utilized. Correlation
between similar domains of the PerfAIM and the PAI (Nagel et al., 1989) were assessed to
indicate the degree of convergent construct validity (Streiner & Norman, 2009), with expected
values between 0.3 and 0.4. Lower correlation (less than 0.3) between different domains of
questionnaires (e.g. the somatic domain of the PerfAIM and the cognitive domain of the PAI)
was expected to support the divergent construct validity (Streiner & Norman, 2009).

54
Chapter 4
Results
4.1 Content Validity
4.1.1 Item generation. The goal of the two focus group sessions (Section 3.2.1 Overview,
Population and Settings) was to consolidate the item generation process, to clarify the construct
and to further develop general themes and ideas. Participants of the focus group were also asked
to fill out a preliminary version of the PerfAIM and to rate the importance/relevance of the items
(complete results are reported in Appendix C). They also shared their opinion on the accuracy
of the scale and on the choice of the format for the questionnaire. Each session lasted no more
than 60 minutes. The session ended when no new themes or ideas emerged (Streiner & Norman,
2009). After the focus group sessions, the PerfAIM was revised to integrate items that had been
missing and to improve some aspects that had been criticized. In order to do this, audio-
recordings were analyzed and the answers of the two focus groups were compared (transcripts
are shown in Appendix D). In the end, four new items were added to the questionnaire: ―I can't
help thinking of past experiences where I performed poorly, and it increases my anxiety‖, ―I feel
very nervous when I perform new material/repertoire‖, ―I feel very stressed after having
performed‖, and ―Alcohol and/or recreational drugs help me cope with my performance
anxiety‖. In addition, a box was created at the end of the questionnaire, titled ―Additional
thoughts or comments‖, to let musicians share anything they thought would be important.
4.1.2 Item reduction. As mentioned in the Methods (Chapter 3), three rounds of
interviews with experts were done to: (a) target missing items, (b) reduce the number of already
existing items, and (c) revise the whole questionnaire.
To reduce the number of items in the PerfAIM, ratings were compiled and the distribution
of answers was calculated for each question (Appendix F). Modifications were based on three
criteria: (a) items not reaching the 80% level of agreement threshold; (b) items qualified as
redundant; and (c) items missing that should be added to the questionnaire. The information
thus obtained is summarized in Tables 8, 9 and 10.
During the first round, 15 items were removed and 12 new items were added (Table 8).

55
During the second round, five items were added and two were withdrawn (Table 9). After the
third round, some items were deleted and new ones were created in response to the comments of
the experts (Table 10). In addition, the items previously deleted after the second round were re-
introduced.
Table 8. Interviews – Round 1.
Items deleted (15)
< 80% level of agreement (11) Redundancies (4) Doing last minute gigs stresses me out. Before performing, I feel confident that
everything will be fine.
I tend to give up worthwhile performance opportunities
due to anxiety.
I worry I will become distracted by my own
thoughts or by external disturbances.
I can't help thinking of past experiences where I
performed poorly, and it increases my anxiety.
I worry about the performance and feedback I
will receive.
I feel very stressed after having performed. I feel inadequate when I am on stage.
When I perform, it seems like I will never get through it.
Performing is challenging.
I think the audience can perceive my nervousness
because of my: o Facial expression
o Stiffness
o Nervous tics
o Trembling
o Musical mistakes or memory blanks
Items added (12) My level of performance anxiety increases significantly due to: A difficult repertoire.
I feel highly anxious, worried and/or stressed: A day prior to the performance.
After having performed, I feel depressed and/or exhausted.
I feel out of control.
Prior to the performance, I adopt repetitive behaviors (pacing, tapping, etc.)
I can easily get over my mistakes when I perform.
In performance situations, I deal with my nervousness by applying one or more stress management techniques
(deep breathing, imagery, self-talk, relaxation, etc.)
Under stressful performance situations, I am affected by these symptoms: (n.) Nervous tics; (o.) Headache;
(p.) Other(s): Please, specify____
Under stressful or challenging situations, I feel that my performance anxiety helps me perform well.
Since health issues may influence your level of music performance anxiety, please indicate any medical
condition that you are aware of (i.e. Raynaud’s phenomenon, tachycardia, anxiety disorder, depressions, etc.)

56
Table 9. Interviews – Round 2.
Items deleted (2) My level of performance anxiety increases significantly due to: (e.) a specific type of performance; (g.)
Other(s).
Items added (5) My level of performance anxiety increases significantly due to: An unfamiliar performance environment.
Performing without the score is really stressful.
I feel so anxious during the performance that I can’t perform to my normal level.
When I perform, I am totally focused and engaged in the music.
I worry over the same things over and over.
Table 10. Interviews – Round 3.
Items deleted (10)
< 80% level of agreement (5) Redundancies (5) I dread sight-reading during a performance. I feel so anxious during the performance that I
can’t perform to my normal level.
Improvising in front of people makes me feel nervous. I feel overwhelmed by the performance
After having performed, I feel depressed and/or
exhausted.
I have positive thoughts about performances.
Under stressful performance situations, I am affected
by these symptoms: (n.) Nervous tics; (o. Headache)
Under stressful performance situations, I am
affected by these symptoms: (m.) lack of voice
and/or finger control.
Under stressful or challenging situations, I feel
that my performance anxiety helps me perform
well.
Items added (7)
I suffer from music performance anxiety.
My level of performance anxiety increases significantly due to: The presence of significant others.
I feel highly anxious, worried and/or stressed: A week prior to the performance.
I am afraid the audience won’t respond favorably to my performance.
I fear that I am not good enough as a performer.
My level of performance anxiety increases significantly due to: A specific type of performance
My level of performance anxiety increases significantly due to: Other(s)
In the end, it was decided to keep some items that did not reach the 80% agreement
threshold (Table 11) because they were added during the interview process and were rated by
only three experts, which was not considered a significant number of raters to allow the removal
of the items in the questionnaire.
Table 11. Interviews - Final Revision.
Items kept despite a level of agreement < 80% (4)
My level of performance anxiety increases significantly due to: (d.) An unfamiliar performance environment.
When I perform, I am totally focused and engaged in the music.
I worry over the same things over and over.
Under stressful performance situations, I am affected by these symptoms: Numbness/tingling

57
Suggestions of re-wording and of items to add or remove were collected and analyzed
(Appendices G, H). Modifications were made when there was an agreement among raters (for
instance, when more than one expert suggested the same change) or when, based on our
judgment, it led to an improvement of the questionnaire.
4.1.3 Instructions. The instructions of the PerfAIM were also modified between each
round of interviews. At first, 67% of the experts responded that the instructions were extremely
clear. However, 33% described them as moderately (16.5%) or slightly clear (16.5%). An
expert pointed out an inconsistency between the instructions and the items. In fact, instructions
contained statements about MPA occurring before or during performances, while in the
questionnaire, some items referred to post-performance situations. In addition, some experts
said that they had problems answering some items using the likelihood scale because MPA
levels changed depending on the situations. For this reason, it was decided to target only
stressful performance situations. The instructions were thus re-worded before the second round
of interviews. A third (33 %) of the experts of Round 2 rated this new set of instructions as very
clear, and 67% rated it as moderately clear. One expert mentioned that these instructions were
too complex and might be overwhelming for the respondents. Therefore, they were simplified
for Round 3 of interviews. Finally, 66% of the experts rated these new instructions as extremely
clear and very clear, and 33% rated them as moderately clear. Results are summarized in Table
12.
Table 12. Level of Agreement among Experts Regarding the Instructions.
Sets of
instructions Instructions
Agreement among
raters
Round 1 ―Below are some general and specific statements about how
you feel before and during a performance. Please circle one
number to indicate how much you agree or disagree with
each statement.‖
The instructions are: -Extremely clear (67%)
-Very clear (0%)
-Moderately clear (16.5%)
-Slightly clear (16.5%)
-Not clear at all (0%)
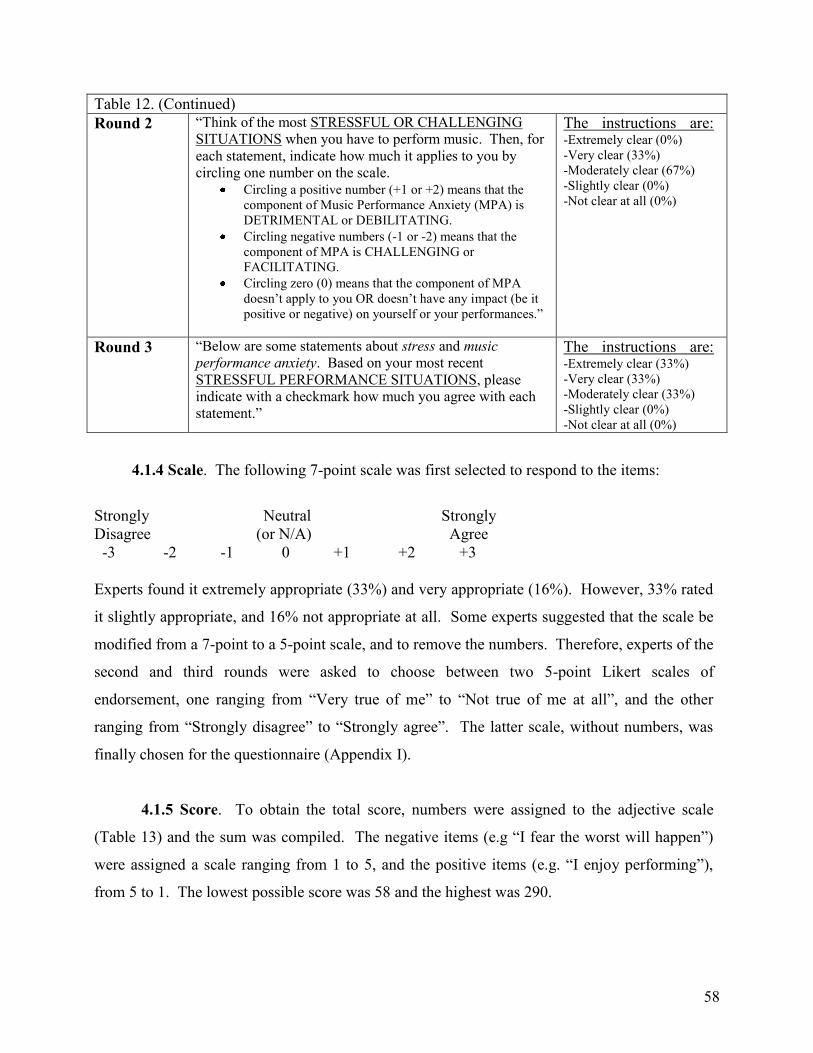
58
Table 12. (Continued)
Round 2 ―Think of the most STRESSFUL OR CHALLENGING
SITUATIONS when you have to perform music. Then, for
each statement, indicate how much it applies to you by
circling one number on the scale. Circling a positive number (+1 or +2) means that the
component of Music Performance Anxiety (MPA) is
DETRIMENTAL or DEBILITATING.
Circling negative numbers (-1 or -2) means that the
component of MPA is CHALLENGING or
FACILITATING.
Circling zero (0) means that the component of MPA
doesn‘t apply to you OR doesn‘t have any impact (be it
positive or negative) on yourself or your performances.‖
The instructions are: -Extremely clear (0%)
-Very clear (33%)
-Moderately clear (67%)
-Slightly clear (0%)
-Not clear at all (0%)
Round 3 ―Below are some statements about stress and music
performance anxiety. Based on your most recent
STRESSFUL PERFORMANCE SITUATIONS, please
indicate with a checkmark how much you agree with each
statement.‖
The instructions are: -Extremely clear (33%)
-Very clear (33%)
-Moderately clear (33%)
-Slightly clear (0%)
-Not clear at all (0%)
4.1.4 Scale. The following 7-point scale was first selected to respond to the items:
Strongly Neutral Strongly
Disagree (or N/A) Agree
-3 -2 -1 0 +1 +2 +3
Experts found it extremely appropriate (33%) and very appropriate (16%). However, 33% rated
it slightly appropriate, and 16% not appropriate at all. Some experts suggested that the scale be
modified from a 7-point to a 5-point scale, and to remove the numbers. Therefore, experts of the
second and third rounds were asked to choose between two 5-point Likert scales of
endorsement, one ranging from ―Very true of me‖ to ―Not true of me at all‖, and the other
ranging from ―Strongly disagree‖ to ―Strongly agree‖. The latter scale, without numbers, was
finally chosen for the questionnaire (Appendix I).
4.1.5 Score. To obtain the total score, numbers were assigned to the adjective scale
(Table 13) and the sum was compiled. The negative items (e.g ―I fear the worst will happen‖)
were assigned a scale ranging from 1 to 5, and the positive items (e.g. ―I enjoy performing‖),
from 5 to 1. The lowest possible score was 58 and the highest was 290.

59
Table 13. Numbers Related to the Adjective Scale for the Summation of Scores.
PerfAIM‘s items Strongly
disagree
Disagree Neutral Agree Strongly
agree
Negative : 1-6, 8, 9, 11-15, 19-25, 28-31 1 2 3 4 5 Positive: 7, 10, 16-18, 26, 27, 32 5 4 3 2 1
4.1.6 Format. A new question was added after the first round of interviews to gather
information about the visual display of the PerfAIM. Based on the comments from the
participants, the format was modified to facilitate completion: the font was enlarged, textured
markers were used, colors were changed, etc. All the experts agreed that the format was
appropriate (67% extremely appropriate, 17% very appropriate, 17% moderately appropriate,
Appendix E). However, it was decided, in the end, to create an online version of the PerfAIM.
Limesurvey was used to create the online questionnaire, which limited the choices regarding the
format, the colors, and the structure, but significantly facilitated the distribution of the
questionnaire, its completion and the data gathering.
4.1.7 Domains. Ninety-one percent of the experts rated the wordings of the items as
extremely clear and accurate (64%) and very clear and accurate (27%). They also agreed that
the proportion of items representing each domain was appropriate (Appendices E, J, and Table
14). On the other hand, because the wording of the items and the proportion of items per
domain changed along the process - a new component was added (the affective symptoms) - the
percentage of agreement is not representative. Table 14 shows results based on the three rounds
of interviews. It demonstrates that the level of agreement increased throughout the interviews,
which supports the fact that the modifications led to an improvement of the questionnaire.
Table 14. Wording and Proportion of Items Based on the Three Rounds of Interviews.
Interviews Items’ clarity and accuracy:
number of experts (%)
Proportion of items/domain:
number of experts (%)
Round 1 -Extremely clear and accurate: 3 (60%)
-Very clear and accurate: 1 (20%)
-Moderately clear and accurate: 0 (0%)
-Slightly clear and accurate: 0 (0%)
-Not clear and accurate at all: 1 (20%)
-Extremely appropriate: 3 (60%)
-Very appropriate: 0 (0%)
-Moderately appropriate: 2 (40%)
-Slightly appropriate: 0 (0%)
-Not appropriate at all: 0 (0%)

60
Table 14. (Continued)
Round 2 -Extremely clear and accurate: 2 (67%)
-Very clear and accurate: 1 (33%)
-Moderately clear and accurate: 0 (0%)
-Slightly clear and accurate: 0 (0%)
-Not clear and accurate at all: 0 (0%)
-Extremely appropriate: 1 (33%)
-Very appropriate: 0 (0%)
-Moderately appropriate: 2 (67%)
-Slightly appropriate: 0 (0%)
-Not appropriate at all: 0 (0%)
Round 3
-Extremely clear and accurate: 2 (67%)
-Very clear and accurate: 1 (33%)
-Moderately clear and accurate: 0 (0%)
-Slightly clear and accurate: 0 (0%)
-Not clear and accurate at all: 0 (0%)
-Extremely appropriate: 2 (67%)
-Very appropriate: 1 (33%)
-Moderately appropriate: 0 (0%)
-Slightly appropriate: 0 (0%)
-Not appropriate at all: 0 (0%)
After the interviews, the PerfAIM was revised one last time to verify that the items were
clear enough to fulfill their intended purpose. In addition, the items were associated to the
theories presented previously (Chapter 1).
The causes of MPA were related to the NUTS theory (PerfAIM‘s personal and situational
factors targeting one or more components of the Lupien‘s recipe) and the 22 causes of MPA
identified by Kenny (2011, Table 15). The association between the NUTS theory, the causes
from Kenny‘s study and the PerfAIM shows that the items of the PerfAIM demonstrate a strong
theoretical basis.
Table 15. Relationship Between the NUTS Theory1, the PerfAIM, and Kenny‘s
2 Causes of MPA.
NUTS1
PerfAIM: Causes (personal and situational sources of stress)
Kenny‘s causes of MPA2
T-S 1. I suffer from music performance anxiety. -Not knowing how to manage physical arousal -Excessive physical arousal prior to, or during performance -Not knowing how to manage negative thoughts/worry about performing
S 2. I am an anxious person in my daily life. -Tendency to be anxious in general, not just in performance
- 3. My level of performance anxiety increases significantly due to:
-
U-S a. A lack of preparation -Inadequate preparation for performance
T b. A low level of self-confidence -Lack of confidence in yourself as a musician -Generally low self-esteem -General lack of self-confidence
T c. An intimidating audience -Concern about audience reaction/Fear of negative evaluation
T d. The presence of significant others -Inadequate support from people close to you -Pressure from parents
N e. An unfamiliar performance environment -
U-S f. Other musicians with whom I perform -Pressure from conductor or section leader -Pressure from/or competing with peers, other musicians
U g. A difficult repertoire -Attempting repertoire that is too difficult -Technical flaws that cause uncertainty

61
Table 15. (Continued)
T h. A specific type of performance (e.g. auditions)
-Negative performance feedback -Concern about audience reaction/Fear of negative evaluation
U-S i. Other (bad acoustics, room temperature, etc.) -Bad performance experience
U-S 4. Performing without the score is really stressful. -Concern about reliability of memory
N-U 5. I feel very nervous when I perform new material/a new repertoire.
-Pressure from self
1 NUTS theory (Marin et al., 2009): Novelty, Unpredictability, Threat to the ego, and Sense of control decreased
2 Causes identified in a sample of 357 orchestral musicians (Kenny, 2011).
Regarding the temporal occurrence, it was ensured that the items from the PerfAIM
targeted the components of the multidimensional theory (as cited in Kenny, 2011) by evaluating
the presence of MPA up to one week prior to the performance.
As for the direction of MPA, the first drafts of the PerfAIM included around one third of
positive statements about MPA (facilitating anxiety) and two thirds of negative statements
(debilitating anxiety). However, experts argued that many of the positive items were not
relevant, so most of them were removed. In the end, 50 items were selected to target debilitating
MPA, and only eight were kept to assess facilitating MPA. These eight positive items were thus
associated to Jone‘s model of facilitative and debilitative anxiety (Weinberg & Gould, 2007) to
ensure that they were targeting relevant components of his model (Table 16).
Table 16. Relationship Between the PerfAIM‘s Facilitating Anxiety Items and the Components of
Jone‘s Model of Facilitative and Debilitative Anxiety.
PerfAIM Components of Jone‘s model At some point while performing, my anxiety lessens or goes
away.
Positive sense of control
In a performance situation, I am easily able to relax physically. Positive expectancies of ability to cope
I feel excited and energized when performing in front of
people.
Symptoms interpreted as facilitative
I perform most effectively under pressure. Positive expectancies of goal attainment
When I perform, I am totally focused and engaged in the
music.
Positive sense of control
I can easily get over my mistakes. Positive expectancies of ability to cope
I enjoy performing. Symptoms interpreted as facilitative
In performance situations, I deal with my nervousness by
applying one or more stress management techniques (deep
breathing, imagery, self-talk, relaxation, etc.).
Positive sense of control
Positive expectancies of ability to cope

62
4.2 Face Validity
4.2.1 Main construct. The clarity and understandability of the construct was verified by
determining whether experts agreed with the main definition used to describe MPA. Only 50%
of the experts described Salmon’s definition, which was first selected, as extremely clear and
understandable, while 33% rated it moderately clear and 17%, not clear at all. In addition,
inconsistencies were found between this definition and the four domains of MPA. Therefore, a
new and more appropriate definition was chosen (Kenny, 2009b, p. 433) in alignment with the
domains. All the experts agreed that Kenny’s definition was either extremely clear and
understandable (50%) or very clear and understandable (50%), thus showing that they supported
the definition used for MPA in this thesis (Appendix E).
4.2.2 Domains. More than 90% of the experts rated the four domains as very relevant or
higher (Appendix E), which is considered an excellent agreement among participants. During the
interviews, it was observed that the PerfAIM items representing the causes of MPA were in fact
situational factors. As the items were mostly related to performing circumstances that might
heighten the levels of anxiety (size of the crowd, type of audience, and so on), the domain named
causes was replaced by situational factors. However, the experts from the second and third round
observed that some items like “lack of preparation” and “low level of self-confidence” were not
considered situational factors. Therefore, after the interviews, it was decided to bring the initial
name back (Causes) but to add a sub-component (personal and situational sources of stress) that
would justify the selection of all the items in this domain. The experts of the first round agreed
that the causes were a domain extremely relevant (83%) or very relevant (16%) to assess, and
100% of the experts from the subsequent rounds found that the situational factors were also
extremely relevant. Therefore, both were combined into one domain.
When asked about the importance of assessing facilitating and debilitating symptoms,
83% of the experts found that assessing facilitating symptoms was either very (33%) or
extremely important (50%), while 17% did not think that it was important at all. As for the
assessment of debilitating symptoms, it was considered extremely important for 75% of the
experts, very important for 17% of them, and moderately important for 8% of them. These
63
results, summarized in Appendix E, showed that there was a good agreement about the
importance of assessing both facilitating and debilitating symptoms of MPA.
The items were categorized by domains (causes, temporal occurrence, and behavioral,
cognitive, somatic and affective manifestations) and were rated by the experts to establish if they
were representative of their respective domains. Results are presented in Appendix E. The items
representing the causes were first described as extremely representative at 40% and very
representative at 60%. After this domain was renamed situational factors, experts agreed that the
items were extremely (50%) and very (50%) representative. However, they mentioned that some
items were not situational factors and that changes were required to adapt either the items or the
name of the domain, which was done subsequently. When the affective component was added,
after the first round of interviews, the classification changed and some items from the cognitive
category were moved into the affective one. It did not seem to lower the level of agreement
among experts. Indeed, 60% rated the items as extremely representative of the cognitive domain
after the first round, against 83% after the second and third rounds. In addition, all the experts
agreed that the items in the affective domain were very (40%) or extremely (60%) representative
of this new component. Overall, the average percentage of agreement regarding the items was
that they were extremely representative of their domains at 60%, very representative at 27%,
moderately representative at 11%, and slightly representative at 2%. These results demonstrate a
very good level of agreement, which supports that the items may be appropriate in representing
their respective domains.
4.2.3 Validity. Finally, experts were asked if the PerfAIM appeared to be a valid measure
to assess MPA. Eighty-three percent of them answered yes (Appendix E). Those who
responded negatively (17%) were all part of the first round of interviews. Among them, one
expert specified that the questionnaire was not valid yet. Still, because modifications were made
throughout the interview process, all the experts of the subsequent rounds found that the PerfAIM
appeared to be a valid measure. This showed an excellent level of agreement among experts.
4.3 PerfAIM’s Scores and Means
The final version of the PerfAIM comprised 58 statements divided into 34 items and 24

64
sub-items (Appendix I). Two additional items were open-ended questions that were not included
in the statistical analysis. Possible scores thus ranged from 58 to 290. The distribution of scores
followed a normal distribution curve (Figure 8).
The scores of the PerfAIM filled out by a sample of 69 popular musicians ranged from 81
to 205 (M=155, SD=29). Females‘ scores ranged from 113 to 202 (M=162, SD=26.4), while
males‘ scores ranged from 81 to 205 (M=149, SD=29.9). An independent samples t-test was
conducted to compare results on the PerfAIM in men and women. There was no significant
difference between the scores for men (M=2.57, SD=0.52) and women (M=2.80, SD=0.46),
t(67)=1.96, p=0.054. These results suggest that the difference between scores on the PerfAIM
may not be attributed to gender.
Figure 8. Score Distribution – PerfAIM. Results compiled from 69 popular musicians.
The majority of the participants obtained a score between 100 and 205, which could be
considered to be a normal amount of MPA in stressful performance situations, as experienced by
66 people out of 69 (more than 95% of the sample). Two musicians scored below 100, therefore
showing mild MPA, and one scored over 205, demonstrating high MPA.
When divided by levels of musical proficiency, results showed that the sole participant
who reported being a beginner obtained a score of 191 (M=3.29, SD=2.83). Six musicians
described themselves as intermediate and scored between 137 and 186 (M=2.98, SD=0.85).
0
2
4
6
8
10
12
14
16
18
20
58 to78
79 to99
100 to120
121 to141
142 to162
163 to183
184 to204
205 to225
226 to246
247 to267
268 to290

65
Twenty-five participants were advanced musicians and their scores ranged from 107 to 202
(M=2.82, SD=0.96). Finally, 37 expert/professional musicians got a score ranging from 81 to
205 (M=2.51, SD=0.92). Based on these results, the distribution of scores becomes wider with
the increase in musical proficiency. However, the more experienced the musicians, the lower
their reported means on the PerfAIM. These values suggest that MPA tends to decrease with an
increase in musical proficiency.
The means were compiled for each item with the responses from the 69 popular musicians.
Results are summarized in Table 17. The means from the 50 items representing debilitating
anxiety go from 1.74 to 4.06, while the eight items representing facilitating anxiety (using an
inverted scale) range from 1.45 to 3.16.
Table 17. Means Reported for Each Item of the PerfAIM. Items Means (SD) Items Means (SD)
1. I suffer from music performance anxiety. 2.81 (1.24) 18. When I perform, I am totally focused and engaged in 2.12 (0.87)
2. I am an anxious person in my daily life. 2.83 (1.16) the music.*
3. My level of performance anxiety increases 19. I feel out of control. 2.03 (0.97)
significantly due to: (a. A lack of preparation) 3.57 (1.28) 20. I tend to avoid difficult pieces or 2.22 (1.00) 3. (b. A low level of self-confidence) 3.06 (1.28) passages for fear of failing in front of an audience.
3. (c. An intimidating audience ) 3.09 (1.17) 21. I fear the worst will happen. 2.07 (1.02)
3. (d. The presence of significant others) 3.55 (1.05) 22. I find it hard to concentrate in front of people. 2.01 (0.90) 3. (e. An unfamiliar performance environment) 2.71 (1.11) 23. I am afraid of being judged. 3.29 (1.21)
3. (f. Other musicians with whom I perform) 3.09 (1.17) 24. I tend to have memory blanks. 2.49 (1.13)
3. (g. A difficult repertoire) 3.57 (1.12) 25. I feel that when I am nervous, I don‘t 2.07 (0.91) 3. (h. A specific type of performance (e.g. auditions) 4.06 (1.08) have enough energy to perform well.
3. (i. Other (bad acoustics, room temperature, etc.) 2.86 (1.25) 26. I can easily get over my mistakes. * 2.42 (1.02) 4. Performing without the score is really stressful. 2.29 (1.10) 27. I enjoy performing.* 1.45 (0.53)
5. I feel very nervous when I perform new material/a new
repertoire.
3.01 (1.04) 28. I tend to be very sensitive or to overreact to any
issues that occur during the performance (musical
2.43 (1.22)
6. I feel highly anxious, worried and/or stressed: mistakes, external disturbances such ambient noises,
6. (a. A week prior to the performance ) 2.14 (1.13) inattentive audience, inadequate lighting, etc.)
6. (b. A day prior to the performance) 2.65 (1.25) 29. I worry about the same things over and over. 2.58 (1.24)
6. (c. Before going on stage) 3.57 (1.27) 30. Under stressful performance situations, I am affected
6. (d. While walking on stage) 2.91 (1.22) by these symptoms: (a. Muscle tension and stiffness) 2.90 (1.21) 6. (e. During the first pieces) 3.26 (1.13) 30. (b. Upset stomach/butterflies) 3.20 (1.32)
6. (f. During the most complicated pieces) 3.32 (1.18) 30. (c. Cold and/or sweaty palms) 2.96 (1.44)
6. (g. During the entire performance) 2.01 (0.96) 30. (d. Trembling (lips, voice, fingers, legs, etc.) 2.62 (1.27) 7. At some point while performing, my anxiety 1.99 (0.88) 30. (e. Racing and/or pounding heart) 3.22 (1.19)
lessens or goes away. * 30. (f. Shortness of breath) 2.25 (1.12)
8. I am so stressed before a performance that I have trouble 2.22 (1.04) 30. (g. Dry mouth) 2.78 (1.22) sleeping. 30. (h. Urge to urinate) 2.91 (1.26)
9. I am afraid the audience won‘t respond 2.57 (1.13) 30. (i. Perspiration/flushing) 2.67 (1.30)
favorably to my performance. 30. (j. Numbness/tingling) 1.74 (0.80) 10. In a performance situation, I am easily able to relax 3.16 (1.07) 30. (k. Dizziness) 1.84 (0.92)
physically.* 30. (l. Impaired coordination) 2.17 (1.08)
11. I am afraid of making mistakes. 3.52 (1.09) 30. (m. Other(s ) 2.03 (1.00) 12. Negative thoughts and worries interfere with my 2.94 (1.10) 31. Alcohol and/or recreational drugs help me cope with 1.97 (1.12)
performance. my performance anxiety.
13. I fear that I am not good enough as a performer. 3.19 (1.29) 32. In performance situations, I deal with my 2.36 (1.04) 14. I engage in repetitive behaviors (pacing, tapping, etc.) 2.52 (1.02) nervousness by applying one or more stress management
15. I tend to make musical mistakes because of my anxiety. 2.97 (1.08) techniques (deep breathing, imagery, self-talk, relaxation,
16. I feel excited and energized when performing in front of people.*
1.80 (0.83) etc.).*
17. I perform most effectively under pressure.* 2.90 (1.05)
* Inverted scale

66
Based on Table 17, results below 3 show that musicians tend to disagree with the statements,
while values exceeding 3 show that they agree (N.B. the scale is reversed for the items 7, 10, 16,
17, 18, 26, 27, and 32).
4.4 Internal Consistency Reliability
The PerfAIM had a high internal consistency (Cronbach‘s alpha = 0.93), which is
considered excellent. When calculated for each domain, the internal consistency ranged from
0.45 to 0.94 (Table 18). When suppressing one item of the PerfAIM, the Cronbach‘s alpha
ranged from 0.927 to 0.932. Ranges are also reported for each domain in Table 18. When
stratified by gender, the internal consistency proved to be higher in men than in women
(respectively 0.94 and 0.92, Table 19). While there was a large discrepancy between values in
each domain for men (0.22-0.94), results were closer together for women (0.65 to 0.91). When
one item was deleted in the statistical calculations based on gender, the Cronbach‘s alpha range
differed by less than 0.01 (around 0.93 for men and 0.91 for women).
Table 18. Internal Consistency of the PerfAIM by Domains: Cronbach‘s Alpha. Domains All Direction
Debilitating Facilitating Causes Temporal
occurrence
Symptoms
Number
of items 58 50 8 12 9 34
Sample (69) 0.930 0.935 0.453 0.767 0.823 0.895
Range* 0.927 to 0.932 0.932 to 0.936 0.368 to 0.481 0.733 to 0.770 0.783 to 0.845 0.886 to 0.898
*Cronbach's Alpha if one item deleted
Table 19. Internal Consistency of the PerfAIM by Gender and by Domains: Cronbach‘s Alpha. Domains All Direction
Debilitating Facilitating Causes Temporal
occurrence
Symptoms
Number
of items 58 50 8 12 9 34
Male (38) 0.935 0.942 0.218 0.776 0.827 0.906
Range* 0.932 to 0.938 0.939 to 0.944 0.144 to 0.259 0.740 to 0.797 0.784 to 0.854 0.897 to 0.913
Female (31) 0.916 0.913 0.648 0.732 0.792 0.871
Range* 0.912 to 0.918 0.909 to 0.915 0.568 to 0.661 0.698 to 0.748 0.750 to 0.808 0.859 to 0.875
*Cronbach's Alpha if item deleted

67
4.5 Test-Retest Reliability
To verify the test-retest reliability of the PerfAIM, an intra-class correlation coefficient
(ICC) model (2, 1) was used with a 95% confidence interval. The test-retest analysis showed that
the ICC for the score assessment (56 items) was 0.89 with 95% CI (0.75-0.95), which is
considered a good reliability. Scores between the first and second administrations are illustrated
in Figure 9.
Figure 9. First and Second Administrations of the PerfAIM. Scores reported for a sample of 21
musicians (10 men and 11 women).
4.6 Concurrent Criterion-Related Validity
A Pearson product-moment correlation coefficient was computed to assess the relationship
between the scores of the PerfAIM and two other questionnaires (PAI and revised K-MPAI,
Table 20). Standardized means were utilized. There was a statistically significant positive
correlation between the PerfAIM and the PAI (r=0.593, n=66, p=0.001), as well as between the
PerfAIM and the K-MPAI (r=0.681, n=61, p=0.001). Overall, the positive correlations showed
that, for instance, when scores were high in one questionnaire, they tended to be high in the
others as well.
Table 20. Concurrent Criterion-Related Validity: Pearson Correlations.
PerfAIM* PAI* K-MPAI*
PerfAIM* 1 0.59 0.68
PAI* 0.59 1 0.62
rev. K-MPAI* 0.68 0.62 1
*Standardized means

68
4.7 Construct Validity (Convergent and Divergent)
A Pearson product-moment correlation coefficient was also computed to establish the
relationship between similar and non-similar domains of the PerfAIM and the PAI. Standardized
means were utilized. Significant correlations were found between similar domains of the
PerfAIM and the PAI. Table 21 summarizes the findings (results in bold correspond to the
correlations between similar domains). Divergent validity was assessed, with correlations
between non-similar domains ranging from 0.07 to 0.45. Values lower than 0.3 were non-
significant, which showed that, as predicted, there was no relationship between these domains.
Values higher than 0.3 were considered significant, showing that some divergent domains were
positively correlated.
Table 21. Convergent and Divergent Construct Validity: Pearson Correlations.
PAI: All
symptoms
PAI: Somatic
symptoms
PAI: Cognitive
symptoms
PAI: Behavioral
symptoms
PerfAIM: Causes 0.22 0.12 0.25 0.07
PerfAIM:Temporal Occurrence 0.34** 0.22 0.35** 0.22
PerfAIM: All symptoms 0.48*** 0.39*** 0.45*** 0.37**
PerfAIM: Somatic symptoms 0.38** 0.44*** 0.31* 0.21
PerfAIM: Cognitive and
Affective symptoms 0.43*** 0.22 0.44*** 0.41***
PerfAIM: Behavioral symptoms 0.44*** 0.34** 0.42** 0.35**
***Significant correlations at the 0.001 level
**Significant correlations at the 0.01 level
*Significant correlations at the 0.05 level
A paired samples t-test was conducted to compare self-perceived level of state anxiety in
the PerfAIM using the item "I am an anxious person in my daily life" and scores on the STAI-T
questionnaire. Without the use of standardized means, there was a significant difference in the
score for the item of the PerfAIM (M=2.81, SD=1.18) and the scores of the STAI-T (M=2.45,
SD=0.28); t(62)=2.65, p=0.01. However, when values were adjusted using standardized means,
no significant difference was found in the item of the PerfAIM (M=-0.0019, SD=0.999) and the
scores of the STAI-T (M=0.0000, SD=1.00; t(62)=-0.014, p=0.989). These results suggest that
one item in the PerfAIM may be adequate to assess self-perceived levels of general anxiety.

69
Chapter 5
Discussion
The goal of this thesis was to design a psychometrically sound questionnaire to assess
MPA in order to analyze the extent to which highly stressful performance situations affect self-
perceived levels of music performance anxiety in popular musicians. To validate the
questionnaire, content validity, face validity, internal consistency reliability, test-retest reliability,
concurrent criterion-related validity, and construct validity (convergent and divergent) were
estimated as reported in the Methods and Results sections.
5.1 Content Validity
To our knowledge, no other measure of MPA has been found to report content validity,
although many authors emphasize its importance in psychological assessment (Streiner &
Norman, 2009; Vogt et al., 2004; Haynes et al., 1995; Nevo, 1985).
During the development of the PerfAIM, we based our procedure on Vogt et al. (2004):
Activities were for the most part simultaneous and iterative rather than
strictly linear. The process of developing construct definitions both
preceded and followed from the focus groups. Likewise, a preliminary
item pool proposed prior to the conduct of focus groups was refined and
enhanced following focus groups and elaboration of construct definitions.
In addition, the literature was consulted to identify preliminary
conceptualizations of key constructs (Clark & Watson, 1995) and to
identify relevant item sets (p. 236).
In accordance with this procedure, and to enhance the content validity of the PerfAIM, focus
groups with members of the population (music students) and interviews with experts (professors,
researchers, psychologists, and professional musicians) were organized. Focus groups helped in
generating more items for the PerfAIM, while the experts‘ interviews were used to reduce the
length of the questionnaire and review its content. As suggested by Vogt et al.‘s procedure,
modifications of the PerfAIM were made throughout the content validation process (i.e. after the
focus groups and after each round of the interviews with the experts).

70
The sample of experts was selected to be heterogeneous: participants had various
professional backgrounds (musicians, psychologists, researchers, and professors) and came from
different countries. This group was thus expected to share different opinions regarding MPA. As
a matter of fact, some comments were in contradiction with each other, so at the end, based on
the analysis of the interviews, we made the last decisions to finalize the PerfAIM. Regarding the
data gathering, Nevo‘s (1985) suggestion was followed (i.e. rating the importance and relevance
of each item of the PerfAIM using the absolute technique), and the final set of items reached
satisfactory levels of agreement among experts. In addition, these selected items were also
associated to study results and theories presented earlier.
Somatic symptoms reported in the PerfAIM reached a high level of agreement. Regarding
the cognitive and affective domains, experts agreed that the items were representative, but
because there were some changes during the interview process, levels of agreement were
calculated with fewer experts, which may have affected the significance of the results. The
behavioral symptoms did not reach consensus among experts during the first round of interviews,
so many were removed for the next rounds. Despite the fact that this may have affected the
proportion of items in this category, it was found in the literature that behavioral self-assessment
was not a good predictor of actual behavior (Douglas, Lindsay & Brooks, 1988). It was thus
established that reporting behavioral symptoms using a self-report method was not the most
effective way to assess this type of symptoms. Therefore, we think that removing these items
probably only improved the validity and reliability of the questionnaire.
Due to the lack of balance between the proportion of positive and negative items, it was not
expected that the PerfAIM would be accurate enough to discriminate between facilitating and
debilitating anxiety. However, as supported by Jone‘s model of facilitative and debilitative
anxiety (Weinberg & Gould, 2007), it may still provide interesting information regarding the way
musicians perceive their anxiety in terms of sense of control, expectancies, and interpretations of
symptoms.
As suggested by the experts, a 5-point Likert scale of endorsement was chosen for the
PerfAIM. It was evidenced that 5- to 9-point scales were ideal in most situations, but people
might have difficulty discriminating much beyond seven levels (Streiner & Norman, 2009).
71
Therefore, the 5-point level of endorsement seemed the most appropriate. It may be important
to note that this endorsement scale has been used in the past to develop a measure of MPA and
has also proved effective among opera chorus artists to measure the sensitivity to change at
different times (e.g. before and after a treatment) or under different conditions (e.g. for
auditions, concerts, etc.; Kenny et al., 2004). In addition, this type of scale makes it possible to
evaluate components of trait anxiety and state anxiety within the same questionnaire (Kenny &
Osborne, 2006).
At first, numbers were assigned to the scale beside each item of the PerfAIM. Based on
Kenny‘s first K-MPAI (Kenny et al., 2004), the scale ranged from -3 to +3. However, Streiner
and Norman (2009) established that attributing numbers below an adjective scale had an impact
on the way participants respond, particularly when the numbers were negative. In fact, Schwartz
et al.‘s study (as cited in Streiner & Norman, 2009) showed that ―when only positive integers
were used, 34% of the subjects used the lower (relatively unsuccessful) half of the scale (0 to 5)
and had a mean value of 5.96. However, when the -5 to +5 numbering scheme was used, only
13% used the lower half, and the mean value was pushed up to 7.38‖ (p. 52). Therefore, it was
decided to remove all numbers attached to the scale in the PerfAIM. This was supported by some
experts who mentioned that the numbers tended to be confusing because the scale was sometimes
inverted.
Regarding the format of the PerfAIM, we created two final versions: a paper-and-pencil
version and a computerized version. For this thesis, only the online version was used because it
was easier to send a link through e-mail than to try to meet with musicians for a paper-and-pencil
completion. It also allowed many more musicians to be contacted than what would have been
possible otherwise. To be consistent, the other questionnaires were also sent in computerized
versions using the same software.
5.2 Face Validity
The first step in establishing face validity was to ensure that the experts accepted the
proposed MPA definition and selected domains. As explained by Haynes et al. (1995), ―The
importance of content validation for the validation of the target construct varies depending on

72
how precisely the construct is defined and the degree to which ‗experts‘ agree about the domain
and facets of the construct. Content validation is particularly challenging for constructs with
fuzzy definitional boundaries or inconsistent definitions‖ (p. 239). After it was decided to use
Kenny‘s definition (2009b), experts agreed that the way MPA was defined was clear and
understandable. As for the domains, the changes made regarding the ―Causes of MPA‖ and how
the name was modified to ―Situational factors‖, then to ―Causes: personal and situational source
of stress‖ altered the validity of the results. Although the final name is based on experts‘
comments, they did not have the opportunity to approve it because the change was made
afterwards. Therefore, it would be interesting to see if experts would agree with this new name.
Regarding the face validity of the whole questionnaire, there was an excellent level of
agreement among experts, particularly after the first round, which shows that the PerfAIM
appeared to be a valid measure to assess MPA.
5.3 PerfAIM’s Score and Means
Scores on the PerfAIM followed a normal distribution curve. This justified the use of
parametric statistics in the validation process of the PerfAIM (Streiner & Norman, 2009).
As explained by Streiner and Norman (2009), ―if we assume that the scores on the test are
fairly normally distributed, then we use the normal curve to determine what proportion of people
score higher and lower‖ (p. 147). Based on the score distribution, more than 95% of the sample
ranged in the middle of the normal distribution curve, and less than 5% in the tails. It may be
hypothesized that scores between 100 and 205 correspond to the normal range of values for MPA
in stressful situations, while higher and lower values are associated with the most extreme cases.
This is interesting because it allows any researcher to ―see where a person stands in relation to
everybody else‖ (Streiner & Norman, 2009, p. 147), which may help in the score interpretation.
No gender difference was found when scores on the PerfAIM were compared using a t-
test. This is consistent with findings from Miller and Chesky (2004) and with the ones of
Kubzansky and Stewart (1999), who showed that self-perceived levels of anxiety were similar
between males and females. However, when the internal consistency calculation was stratified

73
by gender, the alpha reliability coefficient was slightly higher in men than in women, although
the discrepancy between the values in each domain was larger. In fact, the only difference
between genders regarding the Cronbach‘s alpha scores is with the facilitating component of the
direction of MPA (0.22 in men and 0.65 in women). According to these results, the items
representing facilitating anxiety better correlate in their assessment of MPA in women than in
men.
When the scores were distributed based on levels of musical proficiency, the mean
analysis seemed to show that MPA decreased with an increase in expertise. This is in accordance
with Steptoe and Fidler‘s study (1987). However, no significant conclusion can be drawn from
these results because the means were not statistically correlated.
Finally, the means were compiled for each item independently. The values reported
indicated which items were endorsed positively (agree or strongly agree) or negatively (disagree
or strongly disagree). Table 22 summarizes the level of endorsement for each item.
Table 22. Means Associated to Each Item and Categorized by Level of Endorsement.
Strongly
disagree
Disagree Neutral Agree Strongly
agree
- 4. Performing without the score is really stressful.
6. I feel highly anxious, worried
and/or stressed: (a. A week prior to the performance )
1. I suffer from music performance anxiety.
2. I am an anxious person in my
daily life.
3. My level of performance anxiety increases significantly due to: (a. A
lack of preparation)
3. (d. The presence of significant others)
27. I enjoy performing.*
6. (g. During the entire
performance)
3. (b. A low level of self-
confidence)
3. (g. A difficult repertoire)
8. I am so stressed before a
performance that I have trouble
sleeping.
3. (c. An intimidating audience )
3. (e. An unfamiliar performance
environment)
3. (h. A specific type of
performance (e.g. auditions)
6. (c. Before going on stage)
16. I feel excited and energized
when performing in front of
people.*
3. (f. Other musicians with whom
I perform)
7. At some point while performing,
my anxiety lessens or goes away. *
19. I feel out of control. 3. (i. Other (bad acoustics, room
temperature, etc.)
11. I am afraid of making mistakes.
20. I tend to avoid difficult pieces or passages for fear of failing in
front of an audience.
5. I feel very nervous when I perform new material/a new
repertoire.
18. When I perform, I am totally focused and engaged in the music.*
21. I fear the worst will happen. 6. (b. A day prior to the
performance) 26. I can easily get over my
mistakes. *
22. I find it hard to concentrate in front of people.
28. I tend to be very sensitive or
to overreact to any issues that occur during the performance
(musical mistakes, external disturbances such ambient noises,
inattentive audience, inadequate
lighting, etc.)
6.(d. While walking on stage) 6. (e. During the first pieces)
6.(f. During the most complicated
pieces) 9. I am afraid the audience won‘t
respond favorably to my performance.
Physically.*
32. In performance situations, I deal with my nervousness by applying
one or more stress management
techniques (deep breathing, imagery, self-talk, relaxation,
etc.).*

74
Table 22 (continued) Strongly
disagree
Disagree Neutral Agree Strongly
agree
- 30. (f. Shortness of breath)
30. (j. Numbness/tingling)
10. In a performance situation, I
am easily able to relax - -
30. (k. Dizziness) 30. (l. Impaired coordination)
30. (m. Other(s))
12. Negative thoughts and worries interfere with my
performance.
31. Alcohol and/or recreational drugs help me cope with my
13. I fear that I am not good enough as a performer.
performance anxiety. 14. I engage in repetitive
behaviors (pacing, tapping, etc.)
15. I tend to make musical
mistakes because of my anxiety.
17. I perform most effectively under pressure.*
23. I am afraid of being judged.
24. I tend to have memory blanks.
25. I feel that when I am nervous,
I don‘t have enough energy to perform well.
29. I worry about the same things
over and over.
30. Under stressful performance
situations, I am affected by these
symptoms: (a. Muscle tension and stiffness)
30. (b. Upset stomach/butterflies)
30. (c. Cold and/or sweaty palms)
30. (d. Trembling (lips, voice,
fingers, legs, etc.)
30. (e. Racing and/or pounding
heart)
30. (g. Dry mouth)
30. (h. Urge to urinate)
30. (i. Perspiration/flushing) * Positive items
5.4 Internal Consistency Reliability
George and Mallery (as cited in Gliem & Gliem, 2003) report that results of Cronbach‘s
alpha scores ≥ 0.9 are excellent, ≥ 0.8 are good, ≥ 0.7 are acceptable, ≥0.6 are questionable, ≥ 0.5
are poor, and below 0.5 are unacceptable. Nunally (Streiner & Norman, 2009) supports the
contention that internal consistency of a measure should be at least 0.8 for basic research and 0.9
for clinical instruments. Streiner and Norman (2009) argue that values exceeding 0.9 may show
some redundancy, which indicates that some items should be removed. In fact, Cronbach‘s alpha
scores are dependent on the magnitude of the correlation and on the number of items (Streiner &
Norman, 2009; Gliem & Gliem, 2003). Therefore, the longer the questionnaire, the higher the
internal consistency.

75
The PerfAIM‘s alpha reliability coefficient is 0.93. This score demonstrates that, based on
Gliem and Gliem (2003), the PerfAIM is a psychometrically robust measure. However, this may
also show that some items are redundant, or that there are too many items in the questionnaire.
As explained by Streiner and Norman (2009): ―As you add more items, the variance due to error
of measurement goes in direct proportion to the number of items‖ (p. 94). Because the PerfAIM
has 58 items, it is reasonable to think that the number of items made an impact on the reliability
score.
The Cronbach‘s alpha scores were calculated for the PAI (0.88) and the revised K-MPAI
(0.89) using the sample of popular musicians who participated in this study. In addition, a review
of the literature showed that the alpha reliability coefficient of the PerfAIM was lower than those
of the Cox and Kenardy MPA scales (CK-MPAS and CK-MPAC) and K-MPAI, but higher than
those of the PAI, revised K-MPAI, AAS-MAS, Music Performance Anxiety Scale, and MPAI-A
(Table 23).
Table 23. Summary of the Cronbach‘s Alpha Scores for Already Existing MPA Questionnaires.
Study Questionnaire(s) Sample Items Cronbach’s alpha score
Nagel et al.,
1989
Performance Anxiety Inventory (PAI) 20 respondents 20 PAI: 0.89
Wolfe, 1989 Adaptative Anxiety Scale (AAS)
Maladaptative Anxiety Scale (MAS)
Music Performance anxiety scale :
Cognitive-Attentional subscale (CAS);
Emotional-Autonomic subscale (EAS)
divided into 2 parts: Feelings and
Interference.
193 respondents 8
10
11
44
AAS: 0.73
MAS: 0.81
CAS: 0.79
EAS-FEEL: 0.84
EAS-INTRFR: 0.86
Kenny et al.,
2004
Cox and Kenardy MPA scale:
for solo performance (CK-MPAS);
for choral performance (CK-MPAC)
Kenny Music Performance Anxiety
Inventory (K-MPAI)
32 chorus artists 20
26
CK-MPAS: 0.95
CK-MPAC: 0.94
K-MPAI: 0.94
Osborne and
Kenny, 2005
Music Performance Anxiety Inventory
for Adolescents (MPAI-A)
298 teenagers 15 MPAI-A: 0.91
Kenny, 2009 Revised K-MPAI 151 dance and
music students
40 Rev. K-MPAI: Not
available
Note: Bold indicates Cronbach‘s alpha scores higher than the PerfAIM.
Because the PerfAIM includes more items than the other measures, the internal consistency
was also estimated for each domain. Based on Gliem and Gliem (2003), results were qualified as
acceptable for the causes (0.77), and good for the temporal occurrence (0.82) and the symptoms
76
(0.89). Regarding the direction of MPA, results were excellent for the debilitating component
(0.93) but unacceptable for the facilitating component (0.45). This means that the correlation
between the positive statements was not significant, thus showing that people did not endorse
these items consistently. This may have been due to the fact that there were not enough items in
that category to represent effectively the facilitating component, or that the items were too
different from each other to establish a significant relationship.
5.5 Test-Retest Reliability
Nunnally (as cited in Streiner & Norman, 2009, p. 194) ―recommended a minimum
reliability of 0.70 when the scale is used in research and 0.90 when it is used clinically‖. Weiner
and Stewart (as cited in Streiner & Norman, 2009) proposed a correlation of 0.85. At 0.89, the
result from the PerfAIM‘s test-retest shows a very good reliability, practically reaching the
requirements suggested for clinical applications.
5.6 Concurrent Criterion-Related Validity
Because all questionnaires use different scales and scoring systems, standardized means
were utilized (Streiner & Norman, 2009). Kaplan and Saccuzzo (as cited in Osborne & Kenny,
2005) state that ―validity coefficients in the order of 0.3–0.4 are considered high, and values >0.6
are rare‖ (p. 742). According to this, the correlations between the PerfAIM, the PAI and the K-
MPAI may be considered very high.
It is important to note that, because the three questionnaires are based on different
theories, use different scales, and do not have the same length, the results show that they assess
MPA from different perspectives. This means that the measures could not be replaced by one
another, and it also explains why the correlations do not exceed 0.7.
5.7 Construct Validity (Convergent and Divergent)
The results of the Pearson correlations made to establish convergent and divergent
validity ranged from 0.12 to 0.48. Using the same values suggested by Kaplan and Saccuzzo (as
cited in Osborne & Kenny, 2005), correlations between similar domains of the PerfAIM and the
PAI were considered high as they all exceeded 0.3. Although the correlations were below 0.5, it
77
does not mean that the results are poor. Indeed, Streiner and Norman (2009) specify that scales
too highly correlated ―would indicate that they are measuring the same thing‖ (p. 262), which, for
this thesis, is not desirable. Therefore, the results for the convergent validity are highly
satisfactory.
Divergent validity did not yield consistent results. For instance, while no significant
correlation was established between the causes of MPA (which is unique to the PerfAIM) and
each domain of the PAI, significant positive correlations were found between divergent domains
of the questionnaires (e.g. PerfAIM-Temporal occurrence and PAI-Cognitive symptoms). This
may be explained by the fact that both questionnaires are assessing the same overall construct
(i.e. the domains are not as divergent as previously expected). Therefore, it is not a surprise if the
PerfAIM-All symptoms correlate positively with every domain of the PAI, and if the PAI-All
symptoms also correlate with the domains of the PerfAIM (except for the causes).
For exploratory purpose only, a paired-samples t-test was done to compare one item of the
PerfAIM with the STAI-T (Trait subscale). Using simple means to conduct the test, a significant
difference was found, but when standardized means were used, no significant difference
appeared. As explained previously, the use of standardized means was the most appropriate way
to compare these two measures that use a different metric and do not have the same number of
items (Streiner & Norman, 2009). Therefore, it may be concluded that one item is enough to
report self-perceived levels of general anxiety in the PerfAIM. It is important to note that this
single item is not meant to replace a whole questionnaire about trait anxiety or to diagnose an
anxiety disorder. It only means that if musicians report high levels of general anxiety in the item
of the PerfAIM, they may also report high levels of MPA, as supported by Arneson (2010),
Weinberg and Gould (2007), Cox and Kenardy (1993), and Hamann (1982). Therefore, it may
provide valuable information to understand a potential source of MPA. However, at this point,
further evidence would be needed.

78
Chapter 6
Limitations and Conclusion
6.1 Limitations
This thesis has limitations that must be acknowledged. The collection of the demographic
information did not include information about whether musicians were performing publicly, and
if they were soloists or group performers (small or large ensembles). Therefore, it was not
possible to draw a conclusion about the relationship between these data and the results of the
PerfAIM.
Regarding the sampling procedure, the questionnaires were sent by e-mail to a sample of
popular music students and professional musicians. It is possible that the individuals who agreed
to participate differed from those who declined to participate. In fact, the former may have been
more interested in completing the survey because they considered themselves to be suffering
from MPA. If this is the case, the proportion of popular musicians who suffer from MPA may
come out slightly inflated in the reported results.
Many musicians who participated in this study were native French speakers. It is not
known if their proficiency in English was adequate to understand all questions, and this may have
had an impact on the results.
Because this study assessed MPA retrospectively and was not associated with experts‘
evaluation of performance, it is hard to establish whether self-perceived MPA reported in the
PerfAIM has a real impact on performance quality. This study is thus limited by the use of self-
reports only, and by the fact that no gold standard was actually available for comparisons. It
would have been interesting to measure physiological activation (gold standard) during the
course of the project, and to organize a performance in which the musicians would have been
judged on performance quality and overt anxiety manifestations.
Gender difference analyses provided in this thesis were solely based on the PerfAIM‘s
scores. Therefore, they are not as robust as if they would have been compared to the scores

79
stratified by gender obtained with the PAI and the revised K-MPAI. It is thus not possible to
generalize the results obtained with the PerfAIM only.
During the interviews with the experts, there were not enough participants in each round
to do any type of correlations between the results from the data gathered. Only descriptive
statistics were used to analyze them. A bigger sample could have been used, but this would have
required more time than what is available for a typical master‘s thesis.
As stated previously and reported in the literature, years of experience do not have an
impact on MPA (Cox & Kenardy, 1993; Steptoe & Fidler, 1987). We had thus expected that no
significant difference would be found. Although our results seem to suggest that MPA decreases
with higher levels of proficiency, a t-test should have been done to compare the means between
beginner, intermediate, advanced and expert musicians, in order to establish if there was a
significant difference between each group.
Due to the size of our current sample, no attempt was made to assess the factorial
structure of the questionnaire. As factorial analyses are important to determine construct validity
(Haynes et al., 1995), a larger sample (i.e. more than 100 popular musicians) should be used to
allow this type of statistical analysis in the future.
Finally, to facilitate the interpretation of results, the scoring system could be improved.
One suggestion would be to subtract the number 58 from the total score (or to simply change the
numbers attributed to the scale from 1 to 5 to 0 to 4) to obtain a score from 0 to 232 instead of 58
to 290. This would not affect the validity of the questionnaire as estimated here and would
facilitate the score interpretation.
Because there is no existing norm for the popular musicians‘ population, the data acquired
provide a starting point for further studies. Obviously, more data needs to be collected among
this population.

80
6.2 Conclusion
Performing in front of an audience demands physical and psychological strength. To
sustain the pressure, musicians must learn to cope with stress. Studies have been done among
classical musicians to understand the phenomenon of MPA. However, popular musicians have
been virtually ignored in the literature. Therefore, the lack of existing studies on the incidence of
performance anxiety in this population led us to develop a questionnaire specifically for popular
professional musicians and music students.
Although measures of MPA already existed, none of them reached the minimal
psychometric property requirements suggested by McCauley and Swisher (as cited by Osborne &
Kenny, 2005). Thus, we decided to establish the validity and reliability of the PerfAIM by
following the validation processes suggested by researchers in psychological assessment (Streiner
and Norman, 2009; Vogt et al., 2004; Foster & Cone, 1995; Haynes et al., 1995, Hulley et al.,
2001; Nevo, 1985). The internal consistency was calculated using the entire sample (a=0.93),
then results were stratified by gender (a=0.94 in men, a=0.92 in women). Values were also
reported for each domain (Chapter 4, Section 4.4). These steps showed that the PerfAIM was a
measure with an excellent internal consistency. A test-retest was done at a one-week interval.
The questionnaire demonstrated a very good stability and reliability (0.89 with 95% CI).
Concurrent criterion-related validity was established by comparing the PerfAIM to other
measures. Results showed a significant positive correlation between all questionnaires (PerfAIM
and PAI=0.59; PerfAIM and K-MPAI=0.68), which was considered highly satisfactory.
Convergent and divergent construct validity were estimated by correlating similar and non-
similar domains of the PerfAIM and the PAI. Similar domains were positively correlated with
values ranging from 0.35 to 0.48. Divergent domains were either non-correlated or moderately
correlated (0.07 to 0.45), which made the results quite inconsistent and somehow difficult to
interpret. Finally, the scores on the STAI-T were correlated to the scores on one item of the
PerfAIM. No significant difference was found, which meant that the statement ―I am an anxious
person in my daily life‖ was adequate to represent the level of general anxiety among the sample.

81
Overall, these results show that the PerfAIM is an adequate measure for assessing self-
perceived levels of MPA. It demonstrates an excellent internal consistency, a very good
reliability, and a satisfactory concurrent criterion-related validity and convergent validity.
After the completion of the PerfAIM by the 69 popular musicians, the analysis of the
means showed that experienced musicians tended to have lower levels of MPA than less
experienced musicians. When divided by gender, women reported higher means on the PerfAIM
than men, but the difference was not significant. Because the distribution of scores in the
PerfAIM followed a normal curve, it was established that the normal range of MPA in stressful
situations was between 100 and 205 (more than 95% of the sample reported scores ranging in-
between those values). Results outside this range were endorsed by less than 5% of the sample,
thus demonstrating that fewer people reported extreme levels of MPA (be they very high or very
low).
In response to the research question ―What is the extent to which highly stressful
performance situations affect self-perceived levels of MPA in popular musicians‖, results showed
that the musicians who participated in this study did not tend to report extreme levels of MPA in
stressful contexts. When the means were calculated for each item, none of them was reported in
the lowest level of endorsement (strongly disagree), thus demonstrating that participants actually
experience a certain amount of MPA in stressful situations. Still, the facilitating item ―I enjoy
performing‖ showed the highest level of endorsement (strongly agree), which means that
performing is a positive experience for popular musicians, despite the level of stress associated
with the event.
Further research needs to be done to revise and shorten the PerfAIM. Additional research
is also required to determine the generalizability of this questionnaire to other groups of
musicians (i.e. classical musicians) and to establish the responsiveness of the measure (sensitivity
to detect changes over time or before/after treatments). To improve the validation process, a
factor analysis could also be done with a larger sample of musicians. Furthermore, as the
population of the province of Quebec is predominantly French-speaking, there is a need to
translate and validate the measure in this language in order to compare results between languages

82
and see whether there is a cultural difference in levels of MPA between the English and French
speaking populations.
Additionally, a study measuring physiological activation, performance quality and overt
anxiety manifestations in a performance context would help to establish a relationship between
these data and the PerfAIM. Gender difference should also be analyzed using more than one self-
report measure. This would allow a comparison between men‘s and women‘s results using
different samples in previously published articles.
In conclusion, the PerfAIM will be a valid questionnaire to be used by voice and
instrumentalist teachers in settings such as private music schools, colleges or universities. It will
enable musicians to develop self-awareness of the causes, temporal occurrence, direction and
cognitive, somatic, affective and behavioral manifestations of MPA. Eventually, this tool will
help performers to take advantage of the positive aspects of MPA, and to implement stress
management techniques when confronted with the negative aspects of MPA.

83
Bibliography
Abel, J. L., & Larkin, K. T. (1990). Anticipation of performance among musicians: Physiological
arousal, confidence, and state-anxiety. Psychology of Music, 18, 171-182.
Abril, C. R. (2007). I have a voice but I just can't sing: A narrative investigation of singing and social
anxiety. Music Education Research, 9(1), 1-15.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th
ed.). Washington, DC: Author.
American Psychiatric Association. (2002). Diagnostic and statistical manual of mental disorders (4th
ed., text revision). Washington, DC: Author.
Arneson, C. (2010). Performance anxiety: A twenty-first century perspective. Journal of Singing,
66(5), 537-546.
Baars, B. J., & Gage, N. M. (2007). Cognition, brain, and consciousness. Introduction to cognitive
neuroscience. London: Elsevier, Academic Press.
Baker, K. R. (2005). Psychological, physiological, and phenomenological response in musicians with
performance anxiety (Psy.D. degree). Graduate School of Clinical Psychology, George Fox
University, Newberg, Oregon, United States.
Barlow, D. H. (2002). Anxiety and its disorders: The nature and treatment of anxiety and panic (2nd
ed.). New York: The Guilford Press.
Bear, M. F., Connors, B. W., & Paradiso, M. A. (2007). Neuroscience: Exploring the brain (3rd ed.).
Baltimore: Lippincott Williams & Wilkins.
Bippus, A. M., & Daly, J. A. (1999). What do people think causes stage fright?: Naïve attributions
about the reasons for public speaking anxiety. Communication Education, 48(1), 63-72.
Brodsky, W. (1996). Music performance anxiety reconceptualized: A critique of current research
practices and findings. Medical Problems of Performing Artists, 11, 88–98.
Brotons, M. (1994). Effects of performing conditions on music performance anxiety and performance
quality. Journal of Music Therapy, 31(1), 63-81.
Chang, J. C-W. (2001). Effect of meditation on music performance anxiety. Doctor of Education
Dissertation, Teachers College, Columbia University. Dissertation Abstracts International, AAT
3014754.
Clark, D. B., & Agras, W. S. (1991). The assessment and treatment of performance anxiety in
musicians. American Journal of Psychiatry, 148, 598–605.
Cooper, C. L., & Wills, G. I. D. (1989). Popular musicians under pressure. Psychology of Music, 17,
22-36.
84
Cox, W. J., & Kenardy, J. (1993). Performance anxiety, social phobia and setting effects in
instrumental music students. Journal of Anxiety Disorders, 7(1), 49-60.
Craske, M. G., Craig, K. (1984). Musical performance anxiety: the three-systems model and self-
efficacy theory. Behaviour Research and Therapy, 22, 267-280.
Deen, D. R. (1999). Awareness and breathing: Keys to the moderation of musical performance
anxiety. Unpublished doctoral dissertation, University of Kentucky.
Dews, C. L. B., & Williams, M. S. (1989). Student musicians‘ personality styles, stresses, and coping
patterns. Psychology of Music, 17, 37-47.
Dickerson, S. S., & Kemeny, M. E. (2002). Acute stressors and cortisol reactivity: A meta-analytic
review. Psychosomatic Medicine, 54, 105-123.
Douglas, A. R., Lindsay, W. R., & Brooks, D. N. (1988). The three systems model of fear and
anxiety: Implications for assessment of social anxiety. Behavioural Psychotherapy, 16, 15-22.
Dyce, J. A., & O‘Connor, B. P. (1994). The personalities of popular musicians. Psychology of Music,
22, 168-173.
Ely, M. C. (1991). Stop performance anxiety! Music Educators Journal, 78(2), 35-39.
Emmons, S., & Thomas, A. (2008). Understanding performance anxiety. Journal of Singing, 64(4),
461-465.
Esplen, M. J., & Hodnett, J. (1999). A pilot study investigating student musicians‘ experiences of
guided imagery as a technique to manage performance anxiety. Medical Problems of Performing
Artists, 14, 127-132.
Fishbein, M., Middlestadt, S. E., Ottati, V., Straus, S., & Ellis, A. (1988). Medical problems among
ICSOM musicians: Overview of a national survey. Medical Problems of Performing Artists, 3, 1-
8.
Fredrickson, M., & Gunnarsson, G. (1992). Psychobiology of stage fright: The effect
of public performance on neuroendocrine, cardiovascular and subjective reactions. Biological
Psychology, 33, 51-61.
Foster, S. L., & Cone, J. D. (1995). Validity issues in psychological assessment. Psychological
Assessment, 7(3), 248-260.
Gill, A., Murphy, F., & Rickard, N. S. (2006). A preliminary examination of the roles of perceived
control, cortisol, and perceptions of anxiety in music performance. Australian Journal of Music
Education, 1, 32-47.
Gillespie, W., & Myors, B. (2000). Personality of rock musicians. Psychology of Music. 28, 154-165.
Gliem, J. A., & Gliem, R. R, (2003, 8-10 October). Calculating, Interpreting, and Reporting
Cronbach’s Alpha Reliability Coefficient for Likert-Type Scales. Paper presented at the Midwest

85
Research-to-Practice Conference in Adult, Continuing, and Community Education, held at The
Ohio State University, Columbus, OH. Retrieved on March 20, 2011, from
https://scholarworks.iupui.edu/bitstream/handle/1805/344/Gliem+&+Gliem.pdf?sequence=1
Gould, D., Greenleaf, C., & Krane, V. (2002). Arousal-anxiety and sport behaviour. In T. S. Horn
(Ed.), Advances in sport psychology (2nd ed., p.207-241). Champaign, Ill: Human Kinetics
Publishers.
Griebel, G. & Nutt, D. (2008). Handbook of anxiety and fear. Handbook of behavioral neuroscience,
vol. 17. Amsterdam: Elsevier Academic Press.
Güsewell, A. (2010). Exercices respiratoires comme méthodes de gestion du trac – étude pilote.
Recherche en Éducation Musicale, 28, 49-64.
Hamann, D. L. (1982). An assessment of anxiety in instrumental and vocal performances. Journal of
Research in Music Education, 30(2), 77-90.
Hamann, D. L., & Sobaje, M. (1983). Anxiety and the college musician: A study of performance
conditions and subject variables. Psychology of Music, 11(1), 37-50.
Hamilton, L. H., Kella, J. J., & Hamilton, W. G. (1995). Personality and occupational stress in elite
performers. Medical Problems of Performing Artists, 10, 86-89.
Haynes, S. N., Richard, D. C. S., & Kubany, E. S. (1995). Content validity in psychological
assessment: A functional approach to concepts and methods. Psychological Assessment, 7(3),
238-247.
Hobart, J. C., Cano, S. J., & Thompson, A. J. (2002). What sample size for reliability and validity?
Quality of Life Research, 11, 636 (Abstract).
Hulley, S. B., Cummings, S. R., Browner, W. S., Grady, D., Hearst, N., & Newman, T. B. (2001).
Designing clinical research (2nd ed.). Philadelphia: Lippincott Williams & Wilkins.
James, I. (1998). Western orchestral musicians are highly stressed. Resonance: International Music
Council [France], 26, 19-20.
Kasper, S., den Boer, J. A., & Ad Sitsen, J. M. (2003). Handbook of depression and anxiety (2nd ed.
revised and expanded). New York: Marcel Dekker.
Kemp, A. E. (1981). The personality structure of the musician. Identifying a profile of traits for the
performer. Psychology of Music, 9(1), 3-14.
Kemp, A. E. (1996). The musical temperament, psychology and personality of musicians. Oxford :
Oxford University Press.
Kenny, D. T. (2005). A systematic review of treatments for music performance anxiety. Anxiety,
Stress & Coping, 18(3), 183-208.
Kenny, D. T. (2006). Music performance anxiety: Origins, phenomenology, assessment and

86
treatment. Context, 31, 51-63.
Kenny, D. T. (2011). The psychology of music performance anxiety. Oxford: University Press.
Kenny, D. T. (2009a). The factor structure of the revised Kenny Music Performance Anxiety
Inventory. In A. Williamon, S. Pretty, and R. Buck (eds), Proceedings of the International
Symposium on Performance Science 2009 (p.37-41). Utrecht, The Netherlands : European
Association of Conservatoires (AEC).
Kenny, D. T. (2009b). Negative emotions in music making: Performance anxiety. In P.N. Juslin, &
J.A. Sloboda (Eds.), Handbook of music and emotion: Theory, research, applications. Oxford,
UK: Oxford University Press.
Kenny, D. T., Davis, P. J., & Oates, J. (2004). Music performance anxiety and occupational stress
amongst opera chorus artists and their relationship with state and trait anxiety and perfectionism.
Journal of Anxiety Disorders, 18, 757-777.
Kenny, D. T., & Osborne, M. S. (2006). Music performance anxiety: New insights from young
musicians. Advances in Cognitive Psychology, 2(2-3), 103-112.
Kesselring, J. (2006). Music performance anxiety. In E. Altenmueller, M. Wiesendanger, & J.
Kesselring, Motor Control and the Brain (p.309-319). Oxford : University Press.
Khalsa, S. B. S., Shorter, S. M., Cope, S., Wyshak, G., & Sklar, E. (2009). Yoga ameliorates
performance anxiety and mood disturbance in young professional musicians. Applied
Psychophysiology and Biofeedback, 34, 279-289.
Kirchner, J. M. (2003). A qualitative inquiry into musical performance anxiety. Medical Problems of
Performing Artists, 18, 78–82.
Kirchner, J. M., Bloom, A. J., & Skutnick-Henley, P. (2008). The relationship between performance
anxiety and flow. Medical Problems of Performing Artists, 23, 59–65.
Kleine, D. (1990). Anxiety and sport performance: A meta analysis. Anxiety research, 2, 113-131.
Kubzansky, L. D., & Stewart, A. J. (1999). At the intersection of anxiety, gender, and performance.
Journal of Social and Clinical Psychology, 18, 76-97.
Lang, P. J. (1969). The mechanics of desensitization and the laboratory study of human fear. In C. M.
Franks, (Ed.), Assessment and status of the behavior therapies. New York: MacGraw Hill.
Lang, P. J. (1971). The application of psychophysiological methods in the study of psychotherapy and
behaviour modification. In A. E. Bergin & S. L. Garfield (Eds.), Handbook of psychotherapy
and behavior change (pp.75-125). New York : Wiley.
Lazarus, A. A., & Abramovitz, A. (2004). A multimodal behavioral approach to performance anxiety.
Journal of Clinical Psychology : In Session, 60(8), 831–840.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal and coping. New York: Springer.

87
Leary, M. R., & Kowalski, R. M. (1995). Social anxiety. New York : Guilford Press.
LeBlanc, A., Jin, Y. C., Obert, M., & Siivola, C. (1997). Effect of audience on music performance
anxiety. Journal of Research in Music Education, 45(3), 480-496.
Lederman, R. J. (1999). Medical treatment of performance anxiety. Medical Problems of Performing
Artists, 14, 117–121.
Lehrer, P. (1987). A review of the approaches to the management of tension and stage fright
in music performance. Journal of Research in Music Education, 35(3), 143-153.
Lehrer, P., Goldman, N., & Strommen, E. (1990). A principal components assessment of performance
anxiety among musicians. Medical Problems of Performing Artists, 5, 12-18.
Liebert, R. M., & Morris, L. W. (1967). Cognitive and emotional components of test
anxiety: A distinction and some initial data. Psychological Reports, 20, 975-978.
Lin, P., Chang, J., Zemon, V., & Midlarsky, E. (2008). Silent illumination: a study on Chan (Zen)
meditation, anxiety, and musical performance quality. Psychology of Music, 36, 139-155.
Liston, M., Frost, A. A. M., & Mohr, P. B. (2003). The prediction of musical performance anxiety.
Medical Problems of Performing Artists,18, 120-125.
Lupien, S. J., Maheu, F., Tu, M., Fiocco, A., & Schramek, T. E. (2007). The effects of stress and
stress hormones on human cognition: Implications for the field of brain and cognition. Brain and
Cognition, 65, 209-237.
Marchant-Haycox, S. E., & Wilson, G. D. (1992). Personality and stress in performing artists.
Personality and Individual Differences, 13, 1061-1068.
Marin, M. F., Schramek, T. E., Maheu, F. S., & Lupien, S. J. (2009). Stress, emotion and memory:
The good, the bad and the intriguing. In H. Soreq, A. Friedman & D. Kaufer (Eds.), Stress -
From molecules to Behavior: A comprehensive analysis of the neurobiology of stress responses
(pp. 167-188). Germany: Wiley-VCH.
Martens, R., Vealey, R. S., & Burton, D. (1990). Competitive anxiety in sport. Champaign, IL:
Human Kinetics.
May, R. (1977). The Meaning of Anxiety. New York: Norton & Company.
McGinnis, A. M., & Milling, L. S. (2005). Psychological treatment of musical performance anxiety:
Current status and future directions. Psychotherapy: Theory, Research, Practice, Training, 42(3),
357-373.
Meharg, S. S. (1988). Help for the anxious performer. Music Educators Journal, 72(2), 34-37.
McNally, I. M. (2002). Contrasting Concepts of Competitive State-Anxiety in Sport:
Multidimensional Anxiety and Catastrophe Theories. Athletic Insight, 4(2), 10-22.

88
Miller, S. R., & Chesky, K. (2004). The multidimensional anxiety theory: An assessment of and
relationships between intensity and direction of cognitive anxiety, somatic anxiety, and self-
confidence over multiple performance requirements among college music majors. Medical
Problems of Performing Artists, 19, 12-20.
Montello, L. (1995). Music therapy for musicians: Reducing stress and enhancing immunity.
International Journal of Arts Medicine, 4(2), 14-20.
Mor, S., Day, H. I., & Flett, G. L. (1995). Perfectionism, control, and components of performance
anxiety in professional artists. Cognitive Therapy and Research, 19(2), 207-225.
Nagel, J. J. (1990). Performance anxiety and the performing musician: A fear of failure or a fear of
success? Medical Problems of Performing Artists, 5(1), 37-40.
Nagel, J. J. (1993). Stage fright in musicians: A psychodynamic perspective. Bulletin of the
Menninger Clinic, 57(4), 492-504.
Nagel, J. J. (2004). Performance anxiety theory and treatment: One size does not fit all. Medical
Problems of Performing Artists, 19, 39-43.
Nagel, J. J., Himle, D. P., & Papsdorf, J. D. (1989). Cognitive-behavioral treatment of musical
performance anxiety. Psychology of Music, 17, 12-21.
Nevo, B. (1985). Face validity revisited. Journal of Educational Measurement, 22(4), 287-293.
Osborne, M. S., & Franklin, J. (2002). Cognitive processes in music performance anxiety. Australian
Journal of Psychology, 54, 86-93.
Osborne, M. S., & Kenny, D. (2005). Development and validation of music performance anxiety
inventory for gifted adolescent musicians. Anxiety Disorders, 19, 725-751.
Osborne, M. S., & Kenny, D. (2008). The role of sensitizing experiences in music performance
anxiety in adolescent musicians. Psychology of Music, 36(4), 447-462.
Papageorgi, L., Hallam, S., & Welch, G. F. (2007). A conceptual framework for understanding
musical performance anxiety. Research Studies in Music Education, 28, 83-107.
Pearsall, J., & Hanks, P. (2003). Homeostasis. In Oxford Dictionary of English (2nd ed., p.831).
Oxford: Oxford University Press.
Portney, L.G., & Watkins, M.P. (2009). Foundations of Clinical Research: Applications to
Practice (3rd ed.). Upper Saddle River, N.J.: Pearson/Prentice Hall.
Powell, D. H. (2004). Treating individuals with debilitating performance anxiety: An introduction.
Journal of Clinical Psychology : In Session, 60(8), 801-808.
Rae, G., & McCambridge, K. (2004). Correlates of performance anxiety in practical music exams.
Psychology of Music, 32(4), 432-439.

89
Rappoport, P. (1989). A study of stage fright: Its history, its etiology, and an approach to treatment
(Ph.D.). Union of Experimenting Colleges and Universities, The Union Graduate School,
Dissertation Abstracts International.
Reitman, A. D. (2001). The effects of music-assisted coping systematic desensitization on music
performance anxiety. Medical Problems of Performing Artists, 16, 115–125.
Robson, B., Davidson, J., & Snell, E. (1995). ―But I‘m not ready, yet‖: Overcoming audition anxiety
in the young musician. Medical Problems of Performing Artists, 10, 32–37.
Roland, D. (1994). How professional performers manage performance anxiety. Research Studies in
Music Education, 2, 25-35.
Ryan, C. (1998). Exploring musical performance anxiety in children. Medical Problems of
Performing Artists, 13(3), 83-88.
Ryan, C. (2004). Gender differences in children‘s experience of musical performance anxiety.
Psychology of Music, 32(1), 89-103.
Ryan, C., & Andrews, N. (2009). An investigation into the choral singer's experience of music
performance anxiety. Journal of Research in Music Education, 57, 108-126.
Salmon, P. G. (1990). A psychological perspective on musical performance anxiety: A review of the
literature. Medical Problems of Performing Artists, 5, 2-11.
Salmon, G., & Meyer, R. G. (1998). Notes from the green room: Coping with stress and
anxiety in musical performance. San Francisco: Jossey-Bass.
Salmon, P., Powell Shook, C., Lombart, K. G., & Berenson, G. (1995). Performance impairments,
injuries, and stress hardiness in a sample of keyboard and other instrumentalists. Medical
Problems of Performing Artists, 10, 140-146.
Salmon, P., Schrodt, R., & Wright, J. (1989). A temporal gradient of anxiety in a stressful
performance context. Medical Problems of Performing Artists, 4(2), 77-80.
Sataloff, R. T., Rosen, D. C., & Levy, S. (1999). Medical treatment of performance anxiety: A
comprehensive approach. Medical Problems of Performing Artists, 14, 122-126.
Seaward, B. L. (2004). Managing stress: Principles and strategies for health and well-being (4th ed.).
Sudbury, MA: Jones and Bartlett.
Sinden, L. M. (1999). Music performance anxiety: Contributions of perfectionism, coping style, self-
efficacy, and self-esteem. Thesis/Dissertation, Arizona State University.
Spielberger, C. D. (1966). Anxiety and behavior. New York: Academic Press.

90
Spielberger, C. D. (1972). Anxiety as an emotional state. In C. D. Spielberger (Ed.), Anxiety: Current
trends in theory and research (pp. 24-49). New York: Academic Press.
Spielberger, C. (1983). Manual for the State-Trait Anxiety Inventory. Palo Alto, CA:
Consulting Psychologists.
Stanton, H. E. (1994). Reduction of performance anxiety in music students. Australian Psychologist,
29, 124-127.
Stephenson, H., & Quarrier, F. (2005). Anxiety sensitivity and performance anxiety in college music
students. Medical Problems of Performing Artists, 20(3), 119-125.
Steptoe, A. (1989). Stress, coping and stage fright in professional musicians. Psychology of Music,
17, 3-11.
Steptoe, A., & Fidler, H. (1987). Stage fright in orchestral musicians: A study of cognitive
and behavioural strategies in performance anxiety. British Journal of Psychology, 78, 241-249.
Sternbach, D. J., Woody, R. H. (2008). Stress in the lives of music students. Music Educators
Journal, 94(3), 42-48.
Streiner, D. L. & Norman, G. R. (2009). Health measurement scales: A practical guide to
their use (4th ed.). Oxford: Oxford University Press.
Su, Y. H., Luh, J. J., Chen, H. I., Lin, C. C., Liao, M. J., & Chen, H.S. (2010). Effects of using
relaxation breathing training to reduce music performance anxiety in 3rd to 6th graders. Medical
Problems of Performing Artists, 25, 82-86.
Thurber, M. R. (2006). Effects of heart-rate variability biofeedback training and emotional regulation
on music performance anxiety in university students (Ph.D.). University of North Texas, United
States.
Thurber, M. R., Bodenhamer-Davis, E., Johnson, M., Chesky, K., & Chandler, C. K. (2010). Effects
of heart rate variability coherence biofeedback training and emotional management techniques to
decrease music performance anxiety. Biofeedback, 38(1), 28-39.
Van Kemenade, J. F., Van Son, M. J., & Van Heesch, N. C., (1995). Performance anxiety among
professional musicians in symphonic orchestras: A self-report study. Psychological Reports,
77(2), 555–562.
Vogt, D. S., King, D. W., & King, L. A. (2004). Focus groups in psychological assessment:
Enhancing content validity by consulting members of the target population. Psychological Assessment, 16(3), 231-243.
Watson, A. H. D. (2009). The biology of musical performance and performance-related injury. Plymouth, UK: Scarecrow Press.
Weinberg, R. S., & Gould, D. (2007). Foundations of sport and exercise psychology. Champaign, Il.:
Human Kinetics.

91
Wesner, R. B., Noyes, R., & Davis, T. L. (1990). The occurrence of performance anxiety among
musicians. Journal of Affective Disorders, 18, 177-185.
Widmer, S., Conway, A., Cohen, S., & Davies, P. (1997). Hyperventilation: A correlate and predictor
of debilitating performance anxiety in musicians. Medical Problems of Performing Artists, 12(4),
97–106.
Wills, G. I., & Cooper, C. L. (1987). Stress and professional popular musicians. Stress Medicine, 3,
267-74.
Wilson, G. D. (2002). Psychology for performing artists (2nd ed.). London: Whurr.
Wolfe, M. L. (1989). Coping with musical performance anxiety: Problem-focused and emotion-
focused strategies. Medical Problems of Performing Artists, 5, 33–36.
Wolfe, M. L. (1990). Relationship between dimensions of music performance anxiety and behavioral
coping strategies. Medical Problems of Performing Artists, 5, 139–144.
Yoshie, M., Shigemasu, K., Kudo, K., & Ohtsuki, T. (2009). Effects of state anxiety on music
performance: relationship between the Revised Competitive State Anxiety Inventory-2
subscales and piano performance. Musicae Scientiae, 13(1), 55-84.

92
Appendix A
Recruitment Material

93
1. Recruitment for Focus Group Sessions (Oral script)
Hi,
My name is Audrey-Kristel Barbeau. I am doing a master‘s degree in Music Education at McGill
University under the supervision of Dr Isabelle Cossette.
For my thesis project, I want to develop a questionnaire to evaluate Music Performance Anxiety
(MPA). It will be called the ―Performance Anxiety Inventory for Musicians‖ (PerfAIM). The
aim of this project will be to create and validate a self-report measure that demonstrates
appropriate properties in assessing Music Performance Anxiety (MPA).
You are invited to participate in the first phase of this study: a focus group session. This session
is expected to last between 30 and 60 minutes. Your opinion will help to consolidate the item
generation process and to clarify the main construct (MPA) and various domains (symptoms,
causes, etc.).
You are free to accept or not to participate in this study.
The session will be audio-recorded but no name will be mentioned during the discussion. All
information collected will thus remain anonymous. Nobody will have access to this information
except me. Otherwise, it will be kept in a locked cabinet. Dr Cossette will have access to the
information, only after having given you your grades.
Do you have questions?
You will have one week to decide if you want to participate in the focus group session.
Hope to see you there!
2. Recruitment for Interviews with Experts
Hello ________________,
My name is Audrey-Kristel Barbeau. I am doing a master‘s degree in Music Education at McGill
University under the supervision of Dr Isabelle Cossette who gave me your contact info.
For my thesis project, I am interested in creating a questionnaire to evaluate Music Performance
Anxiety (MPA) among popular musicians (which encompasses performers of jazz, rock, pop and
commercial music). The aim of this project is to develop and validate a self-report measure that
demonstrates appropriate properties in assessing the situational factors, the temporal occurrence
and the symptoms of anxiety (be they facilitating or debilitating).
You are invited to participate in the second phase of this study and to be interviewed as an
expert in your field. Your opinion will help to consolidate the item reduction process. You will
be asked to complete the Performance Anxiety Inventory for Musicians (PerfAIM) and to answer

94
questions about the relevance and accuracy of the items of the questionnaire. You will also be
asked to give your opinion about the questionnaire item content (irrelevant, relevant, missing
items, etc.).
If you agree to participate, we will ask you to sign a consent sheet and will collect demographic
data. We will also set a meeting date at your convenience. Face-to-face interview and
questionnaires completion in a paper-and-pencil version will occur at a convenient time and
place for you. If a face-to-face interview is not possible, a telephone interview will be offered at
a convenient time for you. In this case, you will be asked to fill out computerized versions of
the questionnaires (sent previously by email). The interview is expected to last between 30 and
60 minutes, which include the time to complete questionnaires and answer investigator‘s
questions.
If you agree to participate, respond to this email by giving me your availabilities regarding the
best time and location to meet. Please, suggest more than one possible time for the interview; it
will facilitate the organization of the schedule.
I will be happy to answer any of your questions at any time.
Hope to hearing from you soon!
Best regards
Audrey-Kristel Barbeau
Isabelle Cossette: [email protected] (514) 398-4535 ext. 089797
3. Recruitment for the Questionnaire Booklet (Oral Script)
Hello,
My name is Audrey-Kristel Barbeau. I am presently doing a Masters in Music Education under
Dr Isabelle Cossette‘s supervision.
My thesis focuses on Music Performance Anxiety in jazz and popular musicians. I have created a
questionnaire to assess the causes, the temporal occurrence and the symptoms of Music
Performance Anxiety (MPA). My questionnaire is called the ―Performance Anxiety Inventory for
Musicians‖ (PerfAIM).
As you may have noticed, there are not a lot of studies about us, jazz and pop musicians. This is a
good opportunity to learn more about the prevalence of Music Performance Anxiety among our
jazz/pop musician‘s population.
95
If you decide to participate, you will be asked to fill out a survey that will require between 15 min
and 20 min of your time. The survey consists of different questionnaires that I will compare in
order to establish the scientific validity of my questionnaire (the PerfAIM).
By the end of the week, I will send a message to the jazz student email list providing you the link
to fill out the survey online. You are free to accept or not to participate. Attached to the email,
you will find the consent and information sheets. You can read them and let me know if you have
any questions.
Your participation will give you the chance to win one of the three 25$-ITune gift cards to be
drawn on May 1st.
A week after the full survey will have been sent, I will send another link to participate in the next
step of the validation process. I will ask you to fill out the PerfAIM only, a second time. That
should not take more than 5 minutes. By participating in this second step, you will have an
additional chance to win one of the gift cards.
On a voluntary basis, if you want to participate in the draw, we will ask you your name and email
address. Be ensured that nobody will have access to this information except Dr Isabelle Cossette
(my supervisor) and I. As for the results of the questionnaire completion, everything will remain
anonymous (names will be replaced by numbers as soon as the data are gathered).
Do you have any questions?
Thank you very much and I hope you will participate in this study on jazz/pop musician‘s
population. Please spread the word to any of your jazz musician friends!
4. Recruitment material (Email Invitation for the Questionnaire Booklet Completion)
Online survey on Music Performance Anxiety
Are you: A Jazz and/or Pop musician?
English speaker?
18 years old or over?
Get a chance to win one of three ITune gift cards
(25$ each)
Below is the information and consent sheet. Please read it, then click on the link to begin the survey. https://surveys.mcgill.ca/limesurvey/index.php?sid=64138&lang=en

96
Appendix B
Consent Forms

97
1. Consent form – Phase 1
McGill University
SUBJECT INFORMATION AND CONSENT SHEETS
Project Title: Development and validation of the Performance Anxiety Inventory for
Musicians (PerfAIM) – Phase 1: Focus group for the item generation process. Investigators: Isabelle Cossette, D. Mus. Schulich School of Music, McGill University, Strathcona Building, Department of Music Research, 555 Sherbrooke Street West, Montréal, Québec, Canada, H3A 1E3 Tel. : 514-398-4535, ext. 089797, e-mail : [email protected] Student Researcher: Audrey-Kristel Barbeau, Master‟s level [email protected] You are invited to participate in the experiment described below. Introduction and Aim We are interested in creating a questionnaire to evaluate Music Performance Anxiety (MPA) among popular musicians (which encompasses performers of jazz, rock, pop and commercial music). The aim of this project is to develop and validate a self-report measure that demonstrates appropriate properties in assessing the causes, the temporal occurrence and the symptoms of anxiety (be they facilitating or debilitating). The Performance Anxiety Inventory for Musicians (PerfAIM) will be used to assess self-perceived MPA in general, or in relation to performances in various settings. This tool will enable voice and instrumentalist teachers in settings such as private music schools, colleges or universities, to help their students develop self-awareness of cognitive, somatic and behavioral symptoms of MPA, be they positive or negative. As an evaluative tool, the measure will also serve to assess the efficacy of MPA management techniques. Description of Experiment - methods and demands This study is divided into three phases:
1. Focus group sessions (item generation); 2. Interviews with experts (item reduction);

98
3. Self-completion questionnaires (PerfAIM and 3 other questionnaires) (reliability and validity testings);
You are invited to participate in the first phase of this study: a focus group session. If you agree to participate, we will ask you to sign this consent sheet and will collect demographic data. You will have to answer open-ended questions and to share your opinion regarding Music Performance Anxiety. The focus group will be audio-taped to facilitate the discussion and the data analysis afterwards. Your opinion will help to consolidate the item generation process and to clarify the constructs. During this focus group session, we will also ask you to fill out the first draft of the PerfAIM and to complete the “Content Validity Questionnaire”. The session will occur during class hour, and will be part of the “Practicing and Coping Strategies for Performance Enhancement” course (MUPG 474 - Undergraduate music students) or “Coping Strategies for Optimal Performance” seminar (MUPP 694 - Graduate music students). The session is expected to last between 30 and 60 minutes. Benefits and Possible Risks The development and validation of the PerfAIM will provide a psychometrically sound self-administered questionnaire that will help musicians develop or increase their awareness of the cognitive, somatic and behavioral symptoms. It will also help them recognize the causes and temporal occurrence of MPA. Furthermore, it will enable individuals to appropriately evaluate their needs in order to select appropriate coping strategies and treatments. It will finally allow the assessment of strategy efficacy by the completion of the questionnaire before and after strategy implementation. No risk is associated with this study. Withdrawal from Study At all times you will be free to decline to continue with a particular task, or to cease participating in the project. You will be asked to sign a consent sheet prior to any implication in the project to indicate that you are aware of the research topic and the nature of your participation. Subject Rights
Your decision whether or not to participate will not prejudice your future relations with McGill University or the teacher of the class. If you decide to participate, you will be free to withdraw your consent and to discontinue participation at any time without prejudice. Your participation in this study is voluntary and you will have the right to ask questions at any time. Confidentiality
The focus group session will be audio-taped, but no names will be used, so that your anonymity will be preserved. For the questionnaire completion, an arbitrary number will be assigned to you as soon as the data will be collected to help protect your identity. The results of the analysis may be published but your name will not be identified. The audio recordings and the consent forms will be stored in locked cabinet in Dr. Cossette‟s office. Only the researchers will have access to the recorded content.

99
Contacts We will be delighted to answer any further questions that you may have. Please do not hesitate to contact the investigators, Dr. Isabelle Cossette and the master‟s student Audrey-Kristel Barbeau. Their details are being listed on the first page of this document. If you have any questions or concerns about your rights or welfare as a participant in this research study please contact the McGill Research Ethics Officer at 514-398-6831. Signature I acknowledge that I have read the above statement which explains the nature, object and the possible risks of the investigation, and that the statement has been explained to me to my satisfaction. I agree to participate in the experiments described above. ___________ _________________________ ___________________________ DATE Name of Subject Signature of Subject __________ __________________________ ___________________________ DATE Name of Responsible Investigator Signature of Responsible Investigator

100
2. Consent Form – Phase 2
McGill University
SUBJECT INFORMATION AND CONSENT SHEETS
Project Title: Development and validation of the Performance Anxiety Inventory for
Musicians (PerfAIM) – Phase 2: Interviews with experts for the item reduction process.
Investigators: Isabelle Cossette, D. Mus. Schulich School of Music, McGill University, Strathcona Building, Department of Music Research, 555 Sherbrooke Street West, Montréal, Québec, Canada, H3A 1E3 Tel. : 514-398-4535, ext. 089797, e-mail : [email protected] Student Researcher: Audrey-Kristel Barbeau, Master‟s level [email protected] You are invited to participate in the experiment described below. Introduction and Aim We are interested in creating a questionnaire to evaluate Music Performance Anxiety (MPA) among popular musicians (which encompasses performers of jazz, rock, pop and commercial music). The aim of this project is to develop and validate a self-report measure that demonstrates appropriate properties in assessing the causes, the temporal occurrence and the symptoms of anxiety (be they facilitating or debilitating). The Performance Anxiety Inventory for Musicians (PerfAIM) will be used to assess self-perceived MPA in general, or in relation to performances in various settings. This tool will enable voice and instrumentalist teachers in settings such as private music schools, colleges or universities, to help their students develop self-awareness of cognitive, somatic and behavioral symptoms of MPA, be they positive or negative. As an evaluative tool, the measure will also serve to assess the efficacy of MPA management techniques. Description of Experiment - methods and demands This study is divided into three phases:
1. Focus group sessions (item generation); 2. Interviews with experts (item reduction);
101
3. Self-completion questionnaires (PerfAIM and 3 other questionnaires) (reliability and validity testings);
You are invited to participate in the second phase of this study and be interviewed as an expert in your field. Your opinion will help to consolidate the item reduction process. You will be asked to complete the PerfAIM questionnaire and to answer questions about the relevance and accuracy of the items of the questionnaire. You will also be asked to give your opinion about the questionnaire item content (irrelevant, relevant, missing items, etc.). If you choose to participate, you will be contacted by Audrey-Kristel Barbeau to set a meeting date at your convenience At the time of the meeting, we will ask you to sign this consent sheet and will collect demographic data. Face-to-face interview and questionnaires completion in a paper-and-pencil version will occur at a convenient time and place for you. If a face-to-face interview is not possible, a telephone interview will be offered at a convenient time for you. In this case, you will be asked to fill out computerized versions of the questionnaires (sent previously by email). The interview is expected to last between 30 and 60 minutes, which includes the amount of time required to complete the questionnaires and answer questions orally. Benefits and Possible Risks The development and validation of the PerfAIM will provide a psychometrically sound self-administered questionnaire that will help musicians develop or increase their awareness of the cognitive, somatic and behavioral symptoms. It will also help them recognize the causes and temporal occurrence of MPA. Furthermore, it will enable individuals to appropriately evaluate their needs in order to select appropriate coping strategies and treatments. It will finally allow the assessment of strategy efficacy by the completion of the questionnaire before and after strategy implementation. No risk is associated with this study. Withdrawal from Study At all times you will be free to decline to continue with a particular task, or to cease participating in the project. You will be asked to sign a consent sheet prior to any implication in the project to indicate that you are aware of the research topic and the nature of your participation. Subject Rights Your decision whether or not to participate will not prejudice your future relations with McGill University. If you decide to participate, you will be free to withdraw your consent and to discontinue participation at any time without prejudice. You may also refuse to answer any question at any time. Your participation in this study is voluntary and you will have the right to ask questions at any time. Confidentiality
Your name will be replaced by an arbitrary number as soon as the data will be collected to help protect your identity. The interview will not be audio-taped, but notes will be taken by the investigator during the

102
meeting. The results of the analysis may be published but your name will not be identified. The consent forms will be stored in locked cabinet in Dr. Cossette‟s office. Contacts We will be delighted to answer any further questions that you may have. Please do not hesitate to contact the investigators, Dr. Isabelle Cossette and the master‟s student Audrey-Kristel Barbeau. Their details are being listed on the first page of this document. If you have any questions or concerns about your rights or welfare as a participant in this research study please contact the McGill Research Ethics Officer at 514-398-6831. Signature I acknowledge that I have read the above statement which explains the nature, object and the possible risks of the investigation, and the statement has been explained to me to my satisfaction. I agree to participate in the experiments described above. ___________ _________________________ ___________________________ DATE Name of Subject Signature of Subject __________ __________________________ ____________________________ DATE Name of Responsible Investigator Signature of Responsible Investigator

103
3. Consent Form – Phase 3
McGill University
SUBJECT INFORMATION AND CONSENT SHEETS
Project Title: Development and validation of the Performance Anxiety Inventory for
Musicians (PerfAIM) – Phase 3: Self-completion questionnaires. Investigators: Isabelle Cossette, D. Mus. Schulich School of Music, McGill University, Strathcona Building, Department of Music Research, 555 Sherbrooke Street West, Montréal, Québec, Canada, H3A 1E3 Tel. : 514-398-4535, ext. 089797, e-mail : [email protected] Student Researcher: Audrey-Kristel Barbeau, Masters [email protected] You are invited to participate in the experiment described below. Introduction and Aim We are interested in creating a questionnaire to evaluate Music Performance Anxiety (MPA) among popular musicians (which encompasses performers of jazz, rock, pop and commercial music). The aim of this project is to develop and validate a self-report measure that demonstrates appropriate properties in assessing the causes, the temporal occurrence and the symptoms of anxiety (be they facilitating or debilitating). The Performance Anxiety Inventory for Musicians (PerfAIM) will be used to assess self-perceived MPA in general, or in relation to performances in various settings. This tool will enable voice and instrumentalist teachers in settings such as private music schools, colleges or universities, to help their students develop self-awareness of cognitive, somatic and behavioral symptoms of MPA, be they positive or negative. As an evaluative tool, the measure will also serve to assess the efficacy of MPA management techniques. Description of Experiment - methods and demands This study is divided into three phases:
4. Focus group sessions (item generation); 5. Interviews with experts (item reduction); 6. Self-completion questionnaires (PerfAIM and 3 other questionnaires) (reliability and
validity testings);
104
You are invited to participate in the third phase of this study and to fill out a questionnaire booklet. Your participation will help to accumulate data to test the psychometric properties of the PerfAIM questionnaire. If you choose to participate, we will ask you to sign this consent sheet and will collect demographic data. You will then have to complete computerized or paper-and-pencil versions of the questionnaires. You may also be asked to fill out the PerfAIM a second time one week later, in order to establish its reliability (test-retest). Completion of the 4 questionnaires is expected to last between 15 and 30 minutes in total. As for the completion of the PerfAIM one week later, it is expected to last no more than 10 minutes. Benefits and Possible Risks The development and validation of the PerfAIM will provide a psychometrically sound self-administered questionnaire that will help musicians develop or increase their awareness of the cognitive, somatic and behavioral symptoms. It will also help them recognize the causes and temporal occurrence of MPA. Furthermore, it will enable individuals to appropriately evaluate their needs in order to select appropriate coping strategies and treatments. It will finally allow the assessment of strategy efficacy by the completion of the questionnaire before and after strategy implementation. No risk is associated with this study. Withdrawal from Study At all times you will be free to decline to continue with a particular task, or to cease participating in the project. You will be asked to sign a consent sheet prior to any implication in the project to indicate that you are aware of the research topic and the nature of your participation. Subject Rights Your decision whether or not to participate will not prejudice your future relations with McGill University. If you decide to participate, you will be free to withdraw your consent and to discontinue participation at any time without prejudice. Your participation in this study is voluntary and you will have the right to ask questions at any time. Confidentiality
Your name will be replaced by an arbitrary number as soon as the data will be collected to help protect your identity. The results of the analysis may be published but your name will not be identified. The consent forms will be stored in locked cabinet in Dr. Cossette‟s office. Contacts We will be delighted to answer any further questions that you may have. Please do not hesitate to contact the investigators, Dr. Isabelle Cossette and the master‟s student Audrey-Kristel Barbeau. Their details are being listed on the first page of this document. If you have any questions or concerns about your rights or welfare as a participant in this research study please contact the McGill Research Ethics Officer at 514-398-6831.

105
Signature I acknowledge that I have read the above statement which explains the nature, object and the possible risks of the investigation, and the statement has been explained to me to my satisfaction. I agree to participate in the experiments described above. ___________ _________________________ __________________________ DATE Name of Subject Signature of Subject __________ __________________________ _____________________ DATE Name of Responsible Investigator Signature of Responsible Investigator

106
Appendix C
Content Validity Questionnaire - Results (Focus Groups)

110
Appendix C - Content Validity Questionnaire - Results (Focus Groups)
MUGT-474 Seminar Score Distribution Score Distribution Percentages
1 2 3 4 5 6 7 8 9 10 11 5 4 3 2 1
Ratio
5
Ratio
4
Ratio
3
Ratio
2
Ratio
1 1. I am an anxious person in my daily life.
4 5 4 5 3 5 5 4 5 4 5 6 4 1 0 0 0.55 0.36 0.09 0.00 0.00 2. My level of debilitating anxiety increases due to: a. A lack of preparation 5 3 5 4 3 5 5 4 4 4 4 4 5 2 0 0 0.36 0.45 0.18 0.00 0.00 b. A low level of self-confidence 5 3 5 4 3 5 5 5 5 4 5 7 2 2 0 0 0.64 0.18 0.18 0.00 0.00 c. An intimidating audience 4 3 5 4 4 3 5 5 5 5 3 5 3 3 0 0 0.45 0.27 0.27 0.00 0.00 d. A specific type of performance (concert, audition, solo performance, etc.) 4 4 5 4 5 1 5 5 4 5 4 5 5 0 0 1 0.45 0.45 0.00 0.00 0.09 e. Other musicians with whom I perform 4 1 3 4 3 2 5 3 2 1 2 1 2 3 3 2 0.09 0.18 0.27 0.27 0.18 f. Other (please, specify): 3 - 5 - - - 3 - - - - 1 0 2 0 0 0.09 0.00 0.18 0.00 0.00 3. Doing last minute gigs stresses me out. 4 2 4 3 3 4 3 3 3 5 3 1 3 6 1 0 0.09 0.27 0.55 0.09 0.00 4. I dread sight reading during a performance. 4 1 3 3 2 5 4 3 1 3 3 1 2 5 1 2 0.09 0.18 0.45 0.09 0.18 5. Improvising in front of people makes me feel nervous 4 1 5 3 4 5 1 3 2 5 3 3 2 3 1 2 0.27 0.18 0.27 0.09 0.18 6. I tend to give up worthwhile performance opportunities due to anxiety.
4 1 5 5 3 5 5 3 4 1 5 5 2 2 0 2 0.45 0.18 0.18 0.00 0.18 7. I am so stressed before a performance that I have trouble sleeping. 4 2 4 4 2 4 5 5 4 1 3 2 5 1 2 1 0.18 0.45 0.09 0.18 0.09 8. I feel highly anxious and/or stressed: a. Before going on stage 4 5 5 3 5 5 5 4 4 5 5 7 3 1 0 0 0.64 0.27 0.09 0.00 0.00 b. While entering the stage 4 5 5 3 5 5 5 3 3 4 5 6 2 3 0 0 0.55 0.18 0.27 0.00 0.00 c. During the first pieces 4 5 5 3 5 5 5 3 4 5 5 7 2 2 0 0 0.64 0.18 0.18 0.00 0.00 d. During the most complicated pieces 4 5 5 3 5 5 5 4 3 5 5 7 2 2 0 0 0.64 0.18 0.18 0.00 0.00 e. During the entire performance 4 5 5 3 5 5 5 4 5 3 5 7 2 2 0 0 0.64 0.18 0.18 0.00 0.00 9. At some point while performing, my anxiety lessens/goes away. 4 5 5 4 5 5 5 3 5 4 5 7 3 1 0 0 0.64 0.27 0.09 0.00 0.00 10. Before performing, I feel confident that everything will be fine. 4 5 5 3 2 - 5 3 3 - 5 4 1 3 1 0 0.36 0.09 0.27 0.09 0.00

111
Content Validity Quest. Results (Focus Groups) MUGT-474 Seminar
Score Distribution Score Distribution Percentages
(Continued) 1 2 3 4 5 6 7 8 9 10 11 5 4 3 2 1
Ratio 5
Ratio 4
Ratio 3
Ratio 2
Ratio 1
11. I think the audience can perceive my nervousness because of my: a. Facial expression 4 5 5 4 2 5 5 4 5 1 3 5 3 1 1 1 0.45 0.27 0.09 0.09 0.09 b. Stiffness 4 5 5 4 2 5 5 4 5 5 3 6 3 1 1 0 0.55 0.27 0.09 0.09 0.00 c. Nervous tics 4 5 5 4 1 5 5 3 5 2 3 5 2 2 1 1 0.45 0.18 0.18 0.09 0.09 d. Trembling 4 5 5 4 4 5 5 4 5 2 3 5 4 1 1 0 0.45 0.36 0.09 0.09 0.00 e. Musical mistakes or memory blanks 4 5 5 4 4 5 5 4 5 5 3 6 4 1 0 0 0.55 0.36 0.09 0.00 0.00 12. I tend to avoid difficult pieces or difficult passages for fear of failing in front of an audience. 4 5 5 5 3 5 5 5 4 1 3 6 2 2 0 1 0.55 0.18 0.18 0.00 0.09 13. I tend to make mistakes because of my anxiety. 4 5 5 5 4 5 5 5 5 5 5 9 2 0 0 0 0.82 0.18 0.00 0.00 0.00 14. I tend to forget what I am playing when I perform. 4 5 5 5 3 4 5 5 5 1 5 7 2 1 0 1 0.64 0.18 0.09 0.00 0.09 15. I perform most effectively under pressure. 4 5 5 5 1 4 5 4 5 1 5 6 3 0 0 2 0.55 0.27 0.00 0.00 0.18 16. I find it hard to concentrate in front of people. 4 5 5 5 4 - 5 4 5 4 5 6 4 0 0 0 0.55 0.36 0.00 0.00 0.00 17. I am afraid of making mistakes in front of people. 4 5 5 5 4 5 5 4 5 5 5 8 3 0 0 0 0.73 0.27 0.00 0.00 0.00 18. I have positive thoughts about performances. 4 5 5 5 2 5 5 4 4 3 5 6 3 1 1 0 0.55 0.27 0.09 0.09 0.00 19. I feel anxious even though I am well prepared. 4 5 5 5 4 5 5 4 5 5 4 7 4 0 0 0 0.64 0.36 0.00 0.00 0.00 20. I enjoy performing. 3 5 5 5 1 5 5 5 4 3 4 6 2 2 0 1 0.55 0.18 0.18 0.00 0.09 21. I fear the worst will happen when performing. 4 4 5 4 3 5 5 4 5 3 4 4 5 2 0 0 0.36 0.45 0.18 0.00 0.00 22. I feel overwhelmed by the performance. 4 4 5 5 4 5 5 4 5 4 3 5 5 1 0 0 0.45 0.45 0.09 0.00 0.00 23. Negative thoughts interfere with my performance. 4 4 5 5 2 5 5 5 5 4 5 7 3 0 1 0 0.64 0.27 0.00 0.09 0.00 24. Performing is challenging. 4 4 5 2 2 4 5 4 4 5 3 3 5 1 2 0 0.27 0.45 0.09 0.18 0.00 25. I tend to be hypersensitive or to overreact to any issues that occur during the performance. 4 4 5 5 2 5 5 4 5 3 3 5 3 2 1 0 0.45 0.27 0.18 0.09 0.00 26. I worry I will become distracted by my own thoughts or by external disturbances. 4 4 5 5 1 5 5 4 5 2 4 5 4 0 1 1 0.45 0.36 0.00 0.09 0.09 27. I am afraid of being judged. 4 4 5 5 3 5 5 4 5 5 5 7 3 1 0 0 0.64 0.27 0.09 0.00 0.00

112
Content Validity Quest. Results (Focus Groups) MUGT-474 Seminar
Score Distribution Score Distribution Percentages
(Continued) 1 2 3 4 5 6 7 8 9 10 11 5 4 3 2 1
Ratio 5
Ratio 4
Ratio 3
Ratio 2
Ratio 1
28. To be satisfied with myself, I must perform perfectly. 5 1 5 5 3 1 5 3 5 2 5 6 0 2 1 2 0.55 0.00 0.18 0.09 0.18 29. I worry about the performance and feedback I will receive. 4 4 5 5 4 5 5 4 5 5 4 6 5 0 0 0 0.55 0.45 0.00 0.00 0.00 30. When I perform, it seems like I will never get through it. 3 1 5 3 2 4 5 3 5 3 3 3 1 5 1 1 0.27 0.09 0.45 0.09 0.09 31. I feel inadequate when I am on stage. 4 1 5 5 3 5 5 4 5 4 5 6 3 1 0 1 0.55 0.27 0.09 0.00 0.09 32. I feel in control when performing. 4 5 5 5 4 - 5 4 5 4 5 6 4 0 0 0 0.55 0.36 0.00 0.00 0.00 33. I feel I don‟t have enough energy to perform well. 4 5 5 3 1 4 5 4 4 3 3 3 4 3 0 1 0.27 0.36 0.27 0.00 0.09 34. I am easily able to relax in a performance situation. 3 5 5 5 4 4 5 4 4 3 5 5 4 2 0 0 0.45 0.36 0.18 0.00 0.00 35. I feel excited and energized when performing in front of people. 4 5 5 3 - 5 5 4 - - - 4 2 1 0 0 0.36 0.18 0.09 0.00 0.00 36. These symptoms bother me before or while performing: a. Muscle tension and stiffness 5 4 5 5 5 5 5 3 5 5 5 9 1 1 0 0 0.82 0.09 0.09 0.00 0.00 b. Upset stomach/butterflies 5 3 5 5 5 4 5 4 5 1 5 7 2 1 0 1 0.64 0.18 0.09 0.00 0.09 c. Cold and/or sweaty palms 5 4 5 5 5 - 5 4 5 5 5 8 2 0 0 0 0.73 0.18 0.00 0.00 0.00 d. Trembling (lips, voice, fingers, legs, etc.) 5 4 5 5 5 5 5 4 5 1 5 8 2 0 0 1 0.73 0.18 0.00 0.00 0.09 e. Racing and/or pounding heart 5 4 5 5 5 4 5 4 5 5 5 8 3 0 0 0 0.73 0.27 0.00 0.00 0.00 f. Shortness of breath 5 4 5 5 5 5 5 4 5 5 5 9 2 0 0 0 0.82 0.18 0.00 0.00 0.00 g. Dry mouth 5 3 5 5 5 5 5 4 5 2 5 8 1 1 1 0 0.73 0.09 0.09 0.09 0.00 h. Urge to urinate 4 1 5 5 5 4 5 3 5 2 5 6 2 1 1 1 0.55 0.18 0.09 0.09 0.09 i. Perspiration / flushing 4 1 5 5 5 4 5 4 5 1 5 6 3 0 0 2 0.55 0.27 0.00 0.00 0.18 j. Numbness 4 5 5 5 5 5 5 4 5 1 5 8 2 0 0 1 0.73 0.18 0.00 0.00 0.09 k. Dizziness 5 5 5 5 5 5 5 4 5 1 5 9 1 0 0 1 0.82 0.09 0.00 0.00 0.09 l. Impaired coordination 5 5 5 5 5 5 5 4 5 2 5 9 1 0 1 0 0.82 0.09 0.00 0.09 0.00 m. Lack of voice and/or finger control 5 5 5 5 5 5 5 4 5 3 5 9 1 1 0 0 0.82 0.09 0.09 0.00 0.00 37. Overall, I feel my anxiety has a debilitating effect on my performance. 4 5 5 5 5 5 5 5 5 4 3 8 2 1 0 0 0.73 0.18 0.09 0.00 0.00

113
Appendix D
Transcriptions (Focus Groups)

114
Appendix D - Transcriptions (Focus Groups)
Questions Undergraduate students Graduate students 1- In your own words, define “Music Performance Anxiety”
“I think it‟s your body‟s reaction to a stressor, external stressors, that make you react a certain way, when you're not performing; can often have a negative -- or,, more often has a negative effect” “It‟s also mental. And it seeps into your performance, which is physical” “It‟s mainly a mental thing, which then transfers to the body. All comes from the brain basically”. -Investigator: “So it can be created by external sources as well as internal sources?” “It differs from person to person, because your perception of it, particular stressors, can be different from that person's” “ It is basically the same stress as when you are asking a girl for „prom‟ or you are asking for a raise”
“It‟s when your body and mind experience symptoms that are bad, I guess” “I could just say that it is when you get nervous, but that is not specific enough” “It is the body and mind reaction to external stimuli in performance”
2- Standard terms are used to describe the components of MPA: causes, temporal occurrence, direction (facilitating or debilitating) and symptoms (cognitive, behavioral and somatic). I would like you to define each of these terms:
2.1 What is a cause? What is creating MPA?
“Perception of external threat, I guess, to your performance” “Fear of judgment” “Fear of failure” “and the consequences that go with that” “Putting yourself on the line. Those scenarios are sort of causes, those we perceive and we create in our minds. For one person it may be no big deal, but for another person you can be put up.”
“Something that makes something else happen”
2.2 What is a temporal occurrence? The moment when anxiety happens, when anxiety reaches a peak.
“Originally, the impression I got from this class was that it happens right before you perform, but I think the daily stress that you experience with the music is MPA, so you‟re actually dealing with it daily” “It is actually the same feeling you experience when you are auditioning or when you are interviewing for a job” “I think it also lasts afterwards, in the sense that you might not still feel anxious but the way that you‟re perceiving the way you played is affected by your anxiety symptoms. For example, if you have fear of failure or judgement or whatever, that can keep going after you‟ve played because you‟re replaying everything you did in your head, and judging it over and over again.
“Something that happens at a certain moment” "It starts it" “the timeframe within when your symptoms start and end”
2.3 What is a facilitating anxiety? “Anxiety that helps you perform. It is more a nervousness that causes an excitement rather than stress” “Excitement and enhancement of concentration. You are more in the moment”
“Anxiety that is good for your performance or whatever you are doing” “Enhance performance” “Positive”
2.4 What is a debilitating anxiety? “An anxiety that limits your ability to perform successfully and effectively” “Anxiety that makes you play terribly, or feel terrible”
2.5 What is a cognitive symptom? “Catastrophizing, telling yourself that the situation is actually worst than it is, planning ahead to fail” “It is in your mind, the way you process, the way that you think and perceive” “Not necessarily something that other people can notice”
“It‟s a mental symptom”
2.6 What is a behavioral symptom? “It is the affect of how you act, how you conduct yourself” “the way you manifest your mental symptoms. It is more what people can actually see and hear”
„Something that you do, not something that you think or say” “It‟s not in your mind, it‟s a physical act.” “It‟s not how your body reacts but it‟s like what you decide to do, because of how your body is reacting, I guess”

115
2.7 What is a somatic symptom? “I think somatic symptom is purely physical and behavioral would be the combination of the two[cognitive and somatic]”
“Any physical manifestation”
2.8 Do you think other components should be assessed? Yes No
Yes and No (see below) Yes
a. What would they be? “I think just by putting more details on the types of external sources, the types of people that affect us” “I think there is a lot of ambiguity and overlaps and that it is already overanalysed as it is.” “It makes categories out of things that don‟t have to be categorised necessarily” “It can help our brain to process something by putting it into a category, but it also can obstruct it so I think it's kind of already overanalyzed; I wouldn't dice it up more.”
“Maybe the background of the students, what cause them to be anxious on a base level, not related to performing”
b. How would you define them? - -
3- The first component refers to the causes of MPA. What causes MPA? Can you give me some examples? Probe* : Think about the external causes (uncontrollable events or people that can increase nervousness) and internal causes (inside you).
External causes: orchestra Internal causes: “Memory of failure in the past, you make the situation more fearful than it is” “Fear of having to memorize something can cause internal anxiety” “or placing a great deal of importance on performance so that you cause yourself stress internally” “The money one's pretty big that you've mentioned too at some point. You audition so you can get a job so you can pay things.”
“Being unprepared for performances you have to do” “Knowing that you are being judged by other people” “I care too much about what others think about my playing” “Low self-esteem” “Knowing that you may get or not get your degree based on how you sing or how you play” Internal “If you can‟t let go of your past experiences that have been poor, if you just bring everything that is bad to your performance, you will always be nervous” External “Getting a degree out of your performance” “The time, the way that the stage is, anything physical that is totally outside of your control”
4- The second component refers to temporal occurrence. a) Please give examples of temporal occurrence? (i.e. when does anxiety reach a peak ?)
“It depends, sometimes it happens 2 hours before, some other times, I have been very nervous and shaky during the performance, and sometimes even afterwards. I notice it more afterwards, as a thing that is suppressed and then that comes up” “It‟s also in relation to the other things going on at the same time. Little things become a lot more stressful just because there is a lot of them” “The first time you perform a work, you are nervous about it, but once you have been through it once or twice, you are less nervous during or around the performance”
”It depends on the person. Sometimes it is right before going on stage, sometimes it‟s while you are on the stage, sometimes it‟s two weeks before you‟re on stage, sometimes it‟s the entire time” “I don‟t know if it is ever after” “Sometimes it‟s after” “You can get anxious about how well or how poorly you did”
5.1 a. Please give examples of DEBILITATING cognitive symptoms?
“Negative self-talk” “Lack of concentration” “Having unrelated thoughts” “Catastrophizing”
”Thinking too bad” (Investigator: “Self-talk?”) “Yes, negative self-talk”
5.1 b. Of FACILITATING cognitive symptoms?
“Instructional or positive self-talk” “If you don‟t think of the effects that the music has on the listener, and you just simply focus on the music, then it‟s really helpful”
“Positive self-talk” “Think about controlling what you can control”
5.2 a. Please give examples of DEBILITATING behavioral symptoms?
“Insomnia” “Trembling”
”Apparently not eating before a concert” “Not sleeping, drinking alcohol, smoking”
5.2 b. Of FACILITATING behavioral symptoms?
“Practicing more” ”Working out” “Coming up with a pre-performance routine”
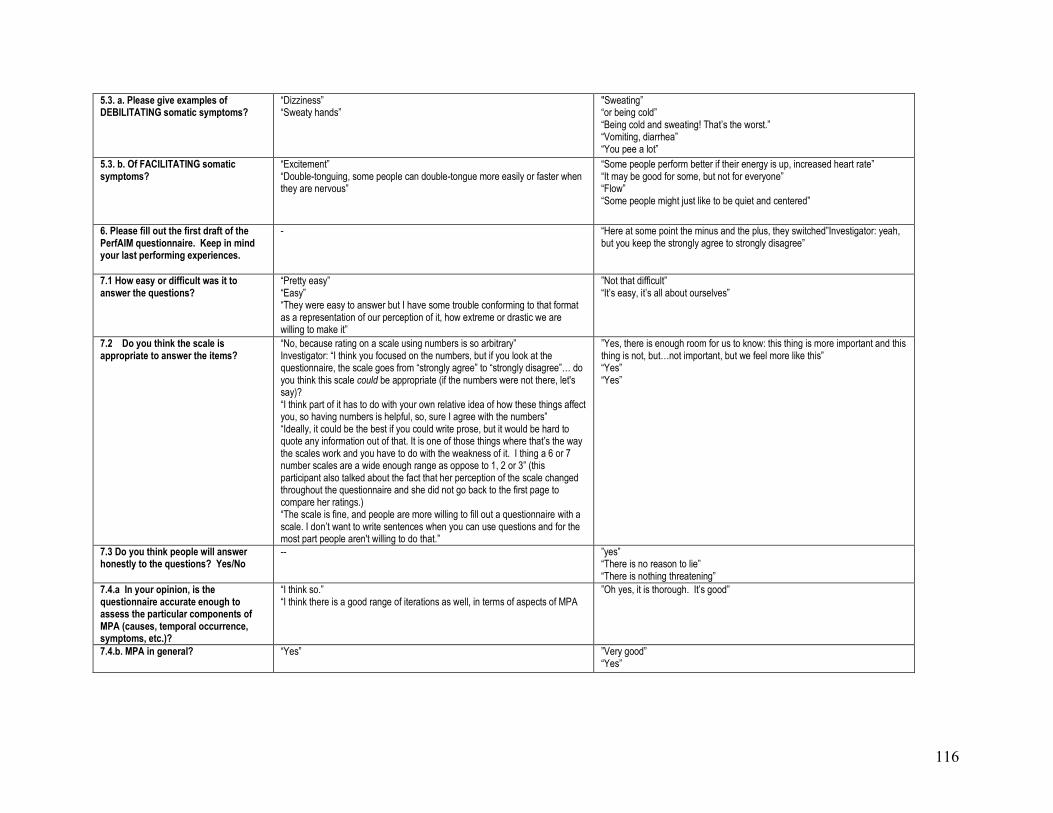
116
5.3. a. Please give examples of DEBILITATING somatic symptoms?
“Dizziness” “Sweaty hands”
"Sweating” “or being cold” “Being cold and sweating! That‟s the worst.” “Vomiting, diarrhea” “You pee a lot”
5.3. b. Of FACILITATING somatic symptoms?
“Excitement” “Double-tonguing, some people can double-tongue more easily or faster when they are nervous”
“Some people perform better if their energy is up, increased heart rate” “It may be good for some, but not for everyone” “Flow” “Some people might just like to be quiet and centered”
6. Please fill out the first draft of the PerfAIM questionnaire. Keep in mind your last performing experiences.
- “Here at some point the minus and the plus, they switched”Investigator: yeah, but you keep the strongly agree to strongly disagree”
7.1 How easy or difficult was it to answer the questions?
“Pretty easy” “Easy” “They were easy to answer but I have some trouble conforming to that format as a representation of our perception of it, how extreme or drastic we are willing to make it”
”Not that difficult” “It‟s easy, it‟s all about ourselves”
7.2 Do you think the scale is appropriate to answer the items?
“No, because rating on a scale using numbers is so arbitrary” Investigator: “I think you focused on the numbers, but if you look at the questionnaire, the scale goes from “strongly agree” to “strongly disagree”… do you think this scale could be appropriate (if the numbers were not there, let's say)? “I think part of it has to do with your own relative idea of how these things affect you, so having numbers is helpful, so, sure I agree with the numbers” “Ideally, it could be the best if you could write prose, but it would be hard to quote any information out of that. It is one of those things where that‟s the way the scales work and you have to do with the weakness of it. I thing a 6 or 7 number scales are a wide enough range as oppose to 1, 2 or 3” (this participant also talked about the fact that her perception of the scale changed throughout the questionnaire and she did not go back to the first page to compare her ratings.) “The scale is fine, and people are more willing to fill out a questionnaire with a scale. I don‟t want to write sentences when you can use questions and for the most part people aren't willing to do that.”
”Yes, there is enough room for us to know: this thing is more important and this thing is not, but…not important, but we feel more like this” “Yes” “Yes”
7.3 Do you think people will answer honestly to the questions? Yes/No
-- ”yes” “There is no reason to lie” “There is nothing threatening”
7.4.a In your opinion, is the questionnaire accurate enough to assess the particular components of MPA (causes, temporal occurrence, symptoms, etc.)?
“I think so.” “I think there is a good range of iterations as well, in terms of aspects of MPA
”Oh yes, it is thorough. It‟s good”
7.4.b. MPA in general? “Yes” ”Very good” “Yes”

117
7.5. If you had to create a questionnaire, what proportion of items would be debilitating symptoms vs facilitating symptoms ? (50-50%? 60-40? 80-20? etc.)
“It would make more sense to be 50-50” “I‟d say maybe 70-30”
”Let‟s say 30 for bad symptoms, 30 for positive symptoms and another 30 for general stuff, because it‟s not only black or white. I like that there is some kind of daily life stress. I‟m more stressed out in life than when I perform.” “I think I‟d made it more like 50-50. That way I could assess whether the people with debilitating performance anxiety also have an equal amount of facilitating anxiety and vice versa.”
7.6 If you had to create a questionnaire, would cognitive, behavioral and somatic symptoms be equally represented? Would one of them be more important than the others? What would be the appropriate proportion? (33-33-33%? 40-20-40%? Etc.)
“They should probably be equally represented because it‟s different for each person” “They overlap so much, especially behavioral and somatic. Cognitive would probably be the most important, like 50% or something.” “It could be 40-40 and 20 for behavioral”
”45-45-10 for behavioral” “I think I‟m just more about equality” “It would be more effective to do 33-33-33”
8. After the Content Validity questionnaire completion: a) Are the items relevant?
(This question was not asked due to insufficient time) “They were mostly good. In the first section, some of the items don‟t apply to me, but it may be relevant in some contexts” “It is a well-balanced questionnaire”
b) Do you think some items may be missing? If so, what are they?
(This question was not asked due to insufficient time) “The first item is very important. You would need a whole separated section to get into that” “Something about insomnia, can it fit it? And maybe a bigger component about personal life” “Maybe five questions on that, anxiety and personal life” “Something like do you find yourself attracting or do you find yourself smart, because these things in your personal life will make you the performer you are. There is a direct link to the way you are, the way you perceive yourself and the way you perceive yourself in a performance”
9. In conclusion, do you have any final comments to make about this questionnaire? (Ask each participant to share his/her point of view).
“It is a good questionnaire” “People may want to add a little extra, so something like „additional thoughts or comment‟. A lot of people would like to write a few sentences and comments on it. That would be hard to evaluate but if you are in the mood to collect more data, it might be a good idea” “Just a little box after each category. If you have to write a few sentences, you‟re going to come up with something new” “When I got to the „other, specify‟, I didn‟t know, I was like [she makes a face]” “Yes, I cannot come up with my own because I‟m already overloaded with information.” “It is definitely more thorough than some of the questionnaires that we did in class” “The reason I like your questionnaire is because it wasn‟t fancy, it cut to the chase. I think it‟s good and it is simple” “And you may be able to collect better data with this kind of questionnaire. I like that there is a neutral, the scale is good”
Additional question: How much time did it take you to complete the questionnaire?
General consensus: around five minutes

118
Appendix E
Interview Oral Questions - Results (Quantitative)

119
Appendix E - Interview Oral Questions – Results: Quantitative
Interview questions
1st round of interviews
2nd round
3rd round Means SD Score Distribution Score Distribution Percentages
1 2 3 4 5 6 8 9 10 11 12 13 5 4 3 2 1 Ratio
5 Ratio
4 Ratio
3 Ratio
2 Ratio
1
1.1 Instructions
5 2 5 3 5 5 1.1 Instructions 4 3 3 3 5 4 - - - -
-
-
-
- - - - -
1.3 Format 5 5 3 4 5 5 4.50 0.84 4 1 1 0 0 0.67 0.17 0.17 0.00 0.00
2. MPA definition from Salmon (1990)
3 5 3 1 5 5 2. MPA definition from Kenny (2009)
4 4 4 5 5 5 - - - -
-
-
-
- - - - -
3.1 Causes: a relevant domain to assess
5 5 5 4 5 5
3.1 Situational factors: a relevant domain to assess
5 5 5 5 5 5 - - - -
-
-
-
- - - - -
3.2 Temporal occurrence: a relevant domain to assess
5 5 4 5 5 5 5 3 5 5 5 5 4.75 0.62 10 1 1 0 0 0.83 0.08 0.08 0.00 0.00
3.3 Direction: a relevant domain to assess
5 5 5 1 5 5 5 4 4 5 4 5 4.42 1.16 8 3 0 0 1 0.67 0.25 0.00 0.00 0.08
3.4 Symptoms: a relevant domain to assess
5 5 5 3 5 5 5 5 5 5 5 5 4.83 0.58 11 0 1 0 0 0.92 0.00 0.08 0.00 0.00
4.Importance of assessing facilitating symptoms
1 4 5 1 4 5 5 4 5 4 5 5 4.00 1.48 6 4 0 0 2 0.50 0.33 0.00 0.00 0.17
5. Importance of assessing debilitating symptoms
4 5 5 3 4 5 5 5 5 5 5 5 4.67 0.65 9 2 1 0 0 0.75 0.17 0.08 0.00 0.00
6. Is the proportion of items appropriate?
5 5 5 - 3 3 5 3 3 5 5 4 4.18 0.98 6 1 4 0 0 0.55 0.09 0.36 0.00 0.00
7. Scale (7-point scale of endorsement
2 5 4 2 1 5 Scale (5-point Likert scale)
5 5 5 5 4 - - - -
-
-
-
- - - - -
8. Wording of the items clear and accurate
5 5 4 - 1 5 5 5 4 5 5 4 4.36 1.21 7 3 0 0 1 0.64 0.27 0.00 0.00 0.09

120
Interview Oral Questions – Results: Quantitative (continued)
Interview questions
1st round of interviews
2nd round
3rd round Means SD Score Distribution Score Distribution Percentages
1 2 3 4 5 6 8 9 10 11 12 13 5 4 3 2 1 Ratio 5 Ratio 4 Ratio
3 Ratio
2 Ratio
1
9. Are the following items* representative of the causes of MPA?
- 5 5 4 4 4
Are the following items representative of the situational factors of MPA?
5 5 4 4 5 4 - - - - -
-
-
- - - - -
10.Are the following items* representative of the temporal occurrence of MPA?
4 5 5 5 4 3 5 5 3 4 5 4 4.33 0.78 6 4 2 0 0 0.50 0.33 0.17 0.00 0.00
11.Are the following items* representative of the behavioral symptoms of MPA?
5 5 5 4 4 3 5 5 3 5 5 2 4.25 1.06 7 2 2 1 0 0.58 0.17 0.17 0.08 0.00
12. Are the following items* representative of the cognitive symptoms of MPA?
- 5 5 5 2 4
(Same question, less items because of the addition of the affective component)
5 5 5 5 5 4 - - - - -
-
-
- - - - -
13.Are the following items* representative of the somatic symptoms of MPA?
5 5 5 5 3 5 5 5 4 5 4 4.64 0.67 8 2 1 0 0 0.73 0.18 0.09 0.00 0.00
14. Are the following items* representative of the affective symptoms of MPA?
5 5 4 5 4 4.60 0.55 3 2 0 0 0 0.60 0.40 0.00 0.00 0.00
* See Appendix J for the categorization of the items Average % of agreement for the representativeness of the
items (Questions 9 to 14): 0.60 0.27 0.11 0.02 0.00
Y N Ratio
Y
Ratio
N
Does this
questionnaire
appear valid?
Y Y Y N N Y Y Y Y Y Y Y 10 2 0.83 0.17

121
Appendix F
Content Validity Questionnaire - Results (Experts)

122
Appendix F- Content Validity Questionnaire - Results (Experts) Respondents Experts Mean SD Score Distribution Score Distribution Percentages
1 2 3 4 5 6 7 8 9 10 11 12 13
5 4 3 2 1 Ratio
5 Ratio
4 Ratio
3 Ratio
2 Ratio
1 I am an anxious person in my daily life. 5 4 5 1 4 5 5 4 5 4 2 5 4.1 1.31 6 4 0 1 1 0,50 0,33 0,00 0,08 0,08
My level of performance anxiety increases significantly due to: a. A lack of preparation
5 5 5 5 5 5 5 4 4 5 5 5 5 4.8 0.38 11 2 0 0 0 0,85 0,15 0,00 0,00 0,00
b. A low level of self-confidence 5 5 5 1 5 5 5 5 5 5 5 5 5 4.7 1.11 12 0 0 0 1 0,92 0,00 0,00 0,00 0,08
c. An intimidating audience 5 5 5 - 5 5 5 5 5 4 5 5 4 4.8 0.39 10 2 0 0 0 0,83 0,17 0,00 0,00 0,00
d. An unfamiliar performance environment 5 3 4 4 1 1 1 1 0 0 0,33 0,33 0,33 0,00 0,00
c. A specific type of performance (please, specifiy:)
5 5 5 5 5 5 5 5 4 3 4.7 0.67 8 1 1 0 0 0,80 0,10 0,10 0,00 0,00
e. Other musicians with whom I perform 5 5 5 5 5 5 4 4 3 4 4 5 4 4.5 0.66 7 5 1 0 0 0,54 0,38 0,08 0,00 0,00
f. A difficult repertoire. 5 5 4 5 4 4.6 0.55 3 2 0 0 0 0,60 0,40 0,00 0,00 0,00
g. Other (please, specify): - - 5 4 - 5 - 5 2 5 4.3 1.21 4 1 0 1 0 0,67 0,17 0,00 0,17 0,00
I dread sight-reading during a performance. 4 4 5 4 5 5 3 2 3 4 5 5 3 4 1 5 4 3 1 0 0,38 0,31 0,23 0,08 0,00
Improvising in front of people makes me feel nervous.
4 5 5 5 5 5 3 5 3 4 5 5 3 4.4 0.87 8 2 3 0 0 0,62 0,15 0,23 0,00 0,00
Performing without the score is really stressful. 5 5 5 5 0 3 0 0 0 0 1,00 0,00 0,00 0,00 0,00
I feel very nervous when I perform new material/repertoire.
5 5 5 5 5 5 5 4 4 5 5 4 4.8 0.45 9 3 0 0 0 0,75 0,25 0,00 0,00 0,00
I am so stressed before a performance that I have trouble sleeping.
5 5 5 5 5 5 4 5 5 4 4 5 4 4.7 0.48 9 4 0 0 0 0,69 0,31 0,00 0,00 0,00
I feel highly anxious, worried and/or stressed: a. The day prior to the performance
5 3 4 5 5 4 4.3 0.82 3 2 1 0 0 0,50 0,33 0,17 0,00 0,00
b. Before going on stage 5 5 4 5 5 5 3 5 3 5 5 5 4 4.5 0.78 9 2 2 0 0 0,69 0,15 0,15 0,00 0,00
c. While entering the stage 5 5 4 5 5 5 3 5 3 5 5 5 4 4.5 0.78 9 2 2 0 0 0,69 0,15 0,15 0,00 0,00
d. During the first pieces 5 5 4 5 5 5 4 5 3 5 5 5 4 4.6 0.65 9 3 1 0 0 0,69 0,23 0,08 0,00 0,00
e. During the most complicated pieces 5 5 4 5 5 5 4 5 3 5 5 5 4 4.6 0.65 9 3 1 0 0 0,69 0,23 0,08 0,00 0,00
f. During the entire performance 5 5 4 5 5 5 5 5 3 5 5 5 5 4.8 0.6 11 1 1 0 0 0,85 0,08 0,08 0,00 0,00
At some point while performing, my anxiety lessens/goes away.
4 5 4 5 5 5 3 5 3 5 5 5 4.5 0.8 8 2 2 0 0 0,67 0,17 0,17 0,00 0,00
I feel so anxious during the performance that I can‟t perform to my normal level.
5 5 5 0 2 0 0 0 0 1,00 0,00 0,00 0,00 0,00
In performance situations, I deal with my nervousness by applying one or more stress management techniques (deep breathing, imagery, self-talk, relaxation, etc.).
5 4 4 5 5 4 4.5 0.55 3 3 0 0 0 0,50 0,50 0,00 0,00 0,00
I am easily able to relax in a performance situation.
5 5 5 5 5 5 5 4 4 5 5 4 4.8 0.45 9 3 0 0 0 0,75 0,25 0,00 0,00 0,00
I tend to make musical mistakes because of my anxiety.
5 5 5 5 5 5 5 5 5 5 5 5 5 5 0 13 0 0 0 0 1,00 0,00 0,00 0,00 0,00
Negative thoughts and worries interfere with my performance
5 5 5 5 5 5 5 5 5 5 5 5 5 5 0 13 0 0 0 0 1,00 0,00 0,00 0,00 0,00
I feel overwhelmed by the performance. 5 5 3 5 5 5 5 5 5 5 5 2 4.6 1 10 0 1 1 0 0,83 0,00 0,08 0,08 0,00
I engage in repetitive behaviors (pacing, tapping, etc.)
5 4 5 5 5 3 4.5 0.84 4 1 1 0 0 0,67 0,17 0,17 0,00 0,00

123
Content Validity Questionnaire - Results (Continued)
Respondents Experts Mean SD Score Distribution Score Distribution Percentages
1 2 3 4 5 6 7 8 9 10 11 12 13
5 4 3 2 1 Ratio
5 Ratio
4 Ratio
3 Ratio
2 Ratio
1 I am afraid of making mistakes. 5 5 4 5 5 5 5 5 4 4 5 5 5 4.8 0.44 10 3 0 0 0 0,77 0,23 0,00 0,00 0,00
I feel excited and energized when performing in front of people
5 4 5 5 5 5 5 5 4 5 3 4 4.6 0.67 8 3 1 0 0 0,67 0,25 0,08 0,00 0,00
I perform most effectively under pressure. 5 5 5 5 5 5 3 5 5 5 5 5 3 4.7 0.75 11 0 2 0 0 0,85 0,00 0,15 0,00 0,00
When I perform, I am totally focused and engaged in the music
5 5 3 4.3 1.15 2 0 1 0 0 0,67 0,00 0,33 0,00 0,00
I feel out of control. 5 5 4 5 5 5 4.8 0.41 5 1 0 0 0 0,83 0,17 0,00 0,00 0,00
I tend to avoid difficult pieces or difficult passages for fear of failing in front of an audience.
4 4 5 5 5 5 4 5 5 4 5 5 5 4.7 0.48 9 4 0 0 0 0,69 0,31 0,00 0,00 0,00
I fear the worst will happen. 5 5 5 5 5 5 5 5 5 4 5 5 5 4.9 0.28 12 1 0 0 0 0,92 0,08 0,00 0,00 0,00
I find it hard to concentrate in front of people. 5 5 4 5 5 5 4 5 5 5 5 4 4 4.7 0.48 9 4 0 0 0 0,69 0,31 0,00 0,00 0,00
I am afraid of being judged. 5 5 5 5 5 5 4 5 5 4 5 5 4 4.8 0.44 10 3 0 0 0 0,77 0,23 0,00 0,00 0,00
I tend to have memory blanks. 5 5 5 5 5 5 5 5 5 5 5 5 5 5 0 13 0 0 0 0 1,00 0,00 0,00 0,00 0,00
Alcohol and/or recreational drugs help me cope with my performance anxiety.
5 4 5 5 3 5 5 5 4 5 5 5 4 4.6 0.65 9 3 1 0 0 0,69 0,23 0,08 0,00 0,00
I can easily get over my mistakes. 5 4 4 5 4 4 4.3 0.52 2 4 0 0 0 0,33 0,67 0,00 0,00 0,00
I have positive thoughts about performances. 4 5 5 5 5 5 5 5 4 4 5 5 3 4.6 0.65 9 3 1 0 0 0,69 0,23 0,08 0,00 0,00
I enjoy performing. 5 5 5 5 5 5 5 5 4 4 5 5 3 4.7 0.63 10 2 1 0 0 0,77 0,15 0,08 0,00 0,00
I feel that when I am nervous, I don‟t have enough energy to perform well.
5 5 5 5 5 3 5 4 5 5 4 3 4.5 0.8 8 2 2 0 0 0,67 0,17 0,17 0,00 0,00
After having performed, I feel depressed and/or exhausted.
5 2 5 5 5 2 4 1.55 4 0 0 2 0 0,67 0,00 0,00 0,33 0,00
I tend to be very sensitive or to overreact to any issues that occur during the performance (musical mistakes; external disturbances such ambient noises, inattentive audience, inadequate lighting; etc)
5 4 5 5 5 5 5 5 5 5 2 5 4.7 0.89 10 1 0 1 0 0,83 0,08 0,00 0,08 0,00
I worry over the same things over and over 5 2 5 4 1.73 2 0 0 1 0 0,67 0,00 0,00 0,33 0,00
Under stressful performance situations, I am affected by these symptoms:
a. Muscle tension and stiffness 5 4 5 5 5 5 5 5 3 5 5 5 5 4.8 0.6 11 1 1 0 0 0,85 0,08 0,08 0,00 0,00
b. Upset stomach/butterflies 5 4 5 5 5 5 5 5 4 5 5 5 4 4.8 0.44 10 3 0 0 0 0,77 0,23 0,00 0,00 0,00
c. Cold and/or sweaty palms 5 4 5 5 5 5 5 5 4 5 5 5 4 4.8 0.44 10 3 0 0 0 0,77 0,23 0,00 0,00 0,00
d. Trembling (lips, voice, fingers, legs, etc.) 5 4 5 5 5 5 5 5 4 5 5 5 5 4.8 0.38 11 2 0 0 0 0,85 0,15 0,00 0,00 0,00
e. Racing and/or pounding heart 5 4 5 5 5 5 5 5 3 5 5 5 4 4.7 0.63 10 2 1 0 0 0,77 0,15 0,08 0,00 0,00
f. Shortness of breath 5 4 5 5 5 5 5 5 4 5 5 5 4 4.8 0.44 10 3 0 0 0 0,77 0,23 0,00 0,00 0,00
g. Dry mouth 5 4 5 5 5 5 5 5 4 5 5 5 5 4.8 0.38 11 2 0 0 0 0,85 0,15 0,00 0,00 0,00
h. Urge to urinate 5 4 5 5 5 5 4 5 3 5 5 5 4 4.6 0.65 9 3 1 0 0 0,69 0,23 0,08 0,00 0,00
i. Perspiration/flushing 5 4 5 5 5 5 4 5 3 5 5 5 4 4.6 0.65 9 3 1 0 0 0,69 0,23 0,08 0,00 0,00
j. Numbness/tingling 5 4 5 5 5 5 4 5 3 5 5 3 3 4.4 0.87 8 2 3 0 0 0,62 0,15 0,23 0,00 0,00
k. Dizziness 5 4 5 5 5 5 4 5 3 5 5 5 3 4.5 0.78 9 2 2 0 0 0,69 0,15 0,15 0,00 0,00
l. Impaired coordination 5 4 5 5 5 5 5 5 3 5 5 5 5 4.8 0.6 11 1 1 0 0 0,85 0,08 0,08 0,00 0,00

124
Content Validity Questionnaire - Results (Continued)
Respondents Experts Mean SD Score Distribution Score Distribution Percentages
1 2 3 4 5 6 7 8 9 10 11 12 13
5 4 3 2 1 Ratio
5 Ratio
4 Ratio
3 Ratio
2 Ratio
1 m. Lack of voice and/or finger control 5 4 5 5 5 5 5 5 4 5 5 5 5 4.8 0.38 11 2 0 0 0 0,85 0,15 0,00 0,00 0,00
n. Nervous tics 5 3 5 5 5 3 4.3 1.03 4 0 2 0 0 0,67 0,00 0,33 0,00 0,00
o. Headache 5 2 5 5 2 3.8 1.64 3 0 0 2 0 0,60 0,00 0,00 0,40 0,00
p. Other (please, specify): 5 2 5 5 5 4.4 1.34 4 0 0 1 0 0,80 0,00 0,00 0,20 0,00
Under stressful or challenging situations, I feel that my performance anxiety helps me perform well.
5 4 5 5 5 3 4.5 0.84 4 1 1 0 0 0,67 0,17 0,17 0,00 0,00
Since health issues may influence your level of music performance anxiety, please indicate any medical conditions that you are aware of (i.e. Raynaud‟s phenomenon, tachycardia, anxiety disorder, depression, etc.) :
5 3 5 5 5 4 4.5 0.84 4 1 1 0 0 0,67 0,17 0,17 0,00 0,00
Additional thoughts and comments:
5 5 5 5 3 5 5 4.7 0.76 6 0 1 0 0 0,86 0,00 0,14 0,00 0,00

125
Appendix G
Interview Oral Questions - Results (Qualitative 1)
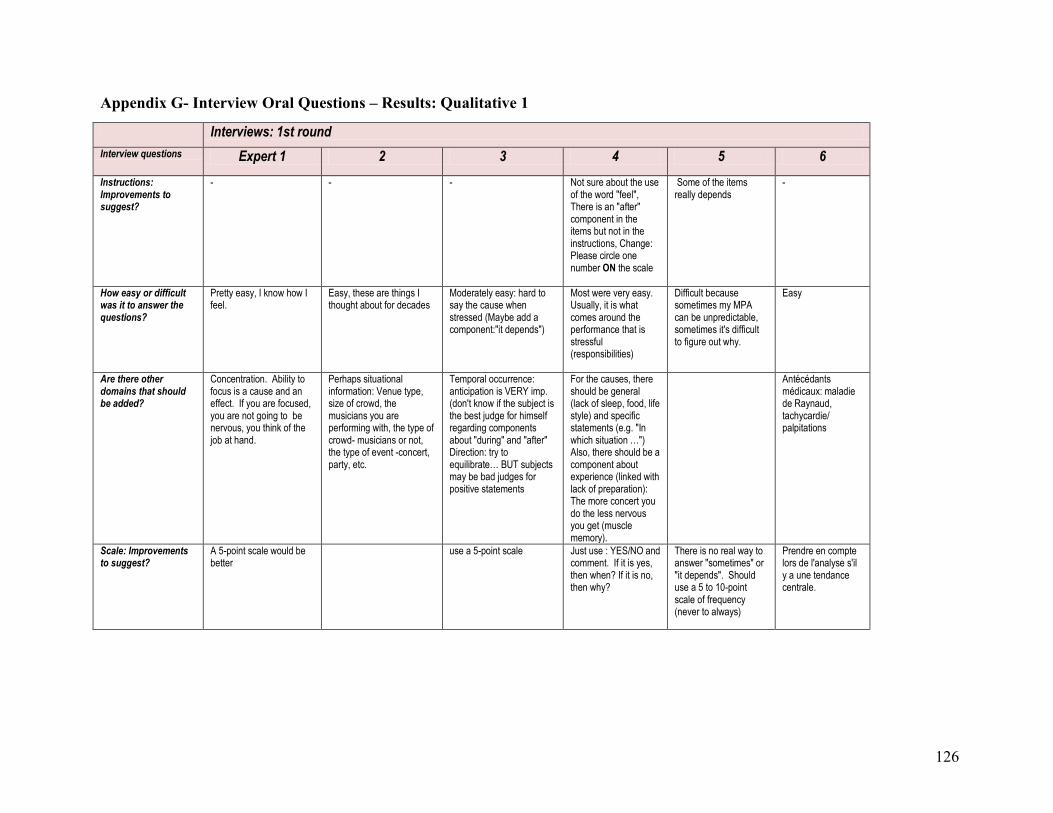
126
Appendix G- Interview Oral Questions – Results: Qualitative 1
Interviews: 1st round
Interview questions Expert 1 2 3 4 5 6
Instructions: Improvements to suggest?
- - - Not sure about the use of the word "feel", There is an "after" component in the items but not in the instructions, Change: Please circle one number ON the scale
Some of the items really depends
-
How easy or difficult was it to answer the questions?
Pretty easy, I know how I feel.
Easy, these are things I thought about for decades
Moderately easy: hard to say the cause when stressed (Maybe add a component:"it depends")
Most were very easy. Usually, it is what comes around the performance that is stressful (responsibilities)
Difficult because sometimes my MPA can be unpredictable, sometimes it's difficult to figure out why.
Easy
Are there other domains that should be added?
Concentration. Ability to focus is a cause and an effect. If you are focused, you are not going to be nervous, you think of the job at hand.
Perhaps situational information: Venue type, size of crowd, the musicians you are performing with, the type of crowd- musicians or not, the type of event -concert, party, etc.
Temporal occurrence: anticipation is VERY imp. (don't know if the subject is the best judge for himself regarding components about "during" and "after" Direction: try to equilibrate… BUT subjects may be bad judges for positive statements
For the causes, there should be general (lack of sleep, food, life style) and specific statements (e.g. "In which situation …") Also, there should be a component about experience (linked with lack of preparation): The more concert you do the less nervous you get (muscle memory).
Antécédants médicaux: maladie de Raynaud, tachycardie/ palpitations
Scale: Improvements to suggest?
A 5-point scale would be better
use a 5-point scale Just use : YES/NO and comment. If it is yes, then when? If it is no, then why?
There is no real way to answer "sometimes" or "it depends". Should use a 5 to 10-point scale of frequency (never to always)
Prendre en compte lors de l'analyse s'il y a une tendance centrale.

127
Interview Oral Questions – Results: Qualitative 1 (Continued)
Interviews: 2nd round Interviews: 3rd round Interview questions Expert 8 9 10 11 12 13 Instructions: Improvements to suggest?
Add : « music » after perform_in the first sentence. the more information you put the more confusing it gets, it is very clear what you put here instead of bullet points, add : there are 5 categories of response: to the left very true of me, in the middle… to the right… (stay very clear). Some participant may be overwhelmed… smaller, clearer, the easy it gets to be. Terms : facilitating, /detrimental, etc. I don‟t think you want to lead them into their responses by insinuating the term in their heads
Les instructions sont OK, mais le questionnaire est plus ou moins claire à cause du fait que l'échelle (-2 à +2) est quelques fois inversée. Il serait mieux de reformuler les items pour que l'échelle soit toujours du même côté. (Investigateur: "il a été suggéré d'enlever carrément les numéros...") C'est une bonne idée
À retravailler, enlever les numéros dans les instructions et dans l'échelle (et préciser "mettre un X" plutôt que d'encercler)
Use just the word stressful (and not challenging); "when you have performED" (past tense)
Underline the word MPA. Item one is not a question about MPA so it contradicts the instructions
Make the instruction more specific by adding: during your LAST most stressful situations. Don't put the headings in the questionnaire
How easy or difficult was it to answer the questions?
Very easy to answer. Facile Facile It may add confusion about how to answer the items (e.g. I may not experience MPA for this item or I just may not experience the item)
Add an item to ask if they actually SUFFER from MPA: give a definition of MPA including + and - components and ask them on a scale of 1 to 5 how much they suffer (“Not at all” to “A lot”)
Be careful about the double negative (in the item and in the scale) like in item 2. Every item should stand on its own
Format: improvements to suggest?
I would not use the numbers (-2 to +2). It may raise alarm bells for the participants. To give you a better picture, ask them to put a checkmark instead. Straightforward, simpler, less intimidating.
Non En vert c'est magnifique, mais la réalité risque d'être du noir et blanc, donc ajuster le format en conséquence. La police utilisée est trop petite (c'est trop forçant). Quadriller l'échelle à l‟endroit où les gens ne sont pas supposé répondre ( par exemple: items 2, 7 et 24)
Add a question right at the beginning about if they suffer from MPA of not (or replace an existing item)
The look is very nice but the structure needs improvement: remove the headings (we don't want to influence them or lead them in any way) + no blanks in the scale (4 generally true and 5 definitely true)

128
Interview Oral Questions – Results: Qualitative 1 (Continued)
Interviews: 2nd round Interviews: 3rd round Interview questions Expert 8 9 10 11 12 13
Are there other domains that should be added?
- Santé car peut avoir une influence
Teachers: what effect they produce on them and what strategies they taught them
Underlying psychological vulnerability
Scale: Improvements to suggest?
no no no Rated 5 only if it is changed for "strongly agree to strongly disagree". Otherwise the words "of me" are too much, and the side of the scale should be inverted to have "Not true" to "Very true"
Invert the side of the scale (neg. 1 pos.5)
Remove the blanks and replace them with new adjectives
Do you think the affective, cognitive, behavioral and somatic manifestations have the same importance? Should the proportion be the same ?
My feeling is that cognitive component is much more debilitating than the other components. I could not say if they have the same importance. Maybe keep the proportion the same because every person is different, and see what you get.
Ils sont tous importants Non, Behavioral est moins important
All important, I don't know if the proportion should be exactly the same
Yes they are all very important
They should be the same, yes, but fundamentally, the affect component is the most important, even though people focus more on the somatic
Proportion of items: Any improvement to suggest?
Use a percentage to compare between the categories instead of worrying about the proportion
Somatic a beaucoup de poids (car c'est facile à évaluer), et cognitif est petit. Faire un peu de recherche
Devrait avoir plus de cognitif et moins de somatic
no no no

129
Appendix H
Interview Oral Questions - Results (Qualitative 2)

130
Appendix H -Interview Oral Questions - Results: Qualitative 2
Interviews: 1st round
Interview questions
Expert 1 2 3 4 5 6
Items to reword of modify
Rewording: 23. "I feel anxious even though I am capable of performing the repertoire" 37. "I feel that when I am nervous, I don't have the energy to perform well"
- Items 2a., 3 5 and 23 are related; Items 2c., 4 and 31 are related; Item 7 should be developed; Item 9 is also a behavioral manifestation; item 13 is the opposite of item 10a. (so probably not required); item 14 should be developed (coping questionnaire); 27. What about positive thoughts?; 29. Give examples for "hypersensitive" and "overreact"; items 20-29 and 30 are all related; 30 and 31 are related; 35. Is it referring to the capacities?; 37 and 39 are related.
The words "anxious" and "overwhelmed" can be used in both direction (they are not implicitly negative), so it should be replaced by: stressed, nervous, troubled, worried) OR the items should be classified FACILITATING/ DEBILITATING
#2: add the term MPA; #3 add usually;#6 rarely of often?; #11 usually; #13 often/rarely; #15 When I am experiencing MPA, I often experience: a. Tics b. memory lapses (etc.) OR I believe the audience can perceive my nervousness when I am experiencing: a. tics b. memory lapses (etc.) #18 (is positive or negative?); #28 and 29 ???; #31 …judge negatively; #32 Musical expectations must be met to be completely satisfied?; #33 remove "the performance"; #35,36,37, 39,40 rarely/usually
29. suggestion d'ajouter le mot "extramusical" entre les mots "any" et "issues". Énoncé 30 : - suggestion d'ajouter l'expression "during a performance" à la fin de l'énoncé, si c'est vraiment cela que l'on veut mesurer. suggestion de retirer l'expression "performance and". En effet, la prestation et la rétroaction sont deux concepts distincts qu'il faudrait éviter de confondre et/ou qu'il conviendrait de mieux cibler distinctement. - suggestion de ne pas présenter ces deux énoncés l'un à la suite de l'autre. Leur contraste très vif pourrait éventuellement causer un biais en induisant chez le répondant un sentiment (peut-être excessif) de vulnérabilité ou d'assurance.
Causes of MPA: Items to delete
- - - item 3 - -
Items missing? 1. External distractions and responsibilities (those not related to the action of performing); 2. Performing beyond one's skill level.
Difficulty of music or lack of familiarity with either the style or the actual piece
- Add an item about experiencing anxiety because something is beyond control; Item 1 could be more specific (ex. Do I feel that anxiety in my daily life affects my performance"). Items 2 a and b are related/ interconnected. Item 4 should be reworded
Lack of sleep. Tiredness. Also when using the word "feel": often versus rarely.
-
Temporal occurrence: Items to delete
- - maybe delete item 13 because of 10a.
Delete item 12 or reword it using "relieved", "satisfied"?
12 -
Items missing? - - - Exterior distractions: -poor sound, acoustic, -bad leader -bad artist -bad audience, etc.
Reword 10: "The peak point of my anxiety occurs:"
10. "The day prior to the performance…" ; 12. Post depression (Imp.): After having perform, I feel very depressed.

131
Interview Oral Questions – Results: Qualitative 2 (Continued)
Interview questions
Expert 1 2 3 4 5 6
Behavioral symptoms: Items to delete
- - - - 14 (Why ask about alcohol and not about betablockers, yoga, recreational drugs, etc.
-
Items missing? - - - Level of enthusiasm for the music will be facilitating. Where does the pressure come from? (or not) : artist, music, leader, lack of preparation?
How they cope (maybe add another section)
Prior to the performance, I tend to adopt repetitive behaviors (pacing, taping, etc.); 15. Scinder en deux: e. musical mistakes f. memory blanks
Cognitive symptoms: Items to delete
- - - - - -
Items missing? "I have trouble concentrating because of my nervousness"
- positive aspects Conditions surrounding the gig: -$$, -Length of day, -Orchestra preparation (rehearsal)
This section needs work: change items, add rarely/usually, clarify things
29. Add "extramusical issues" (musical issues are already attended); 30. Add a temporal occurrence ("before" or "during a performance"); 31. Very important (Cognition): l'anxiété est dirigée vers le futur (et il n'y a généralement pas d'agent objectivement identifiable); le stress, vers le présent (et il a un agent stresseur objectivement identifiable); la dépression vers le passé. MPA est à cheval entre le stress et l'anxiété
Somatic symptoms: Items to delete
37 to 39: overlap - no -
Items missing? - - Headache + Add items from #15 + Add in #40: n. Other__
- rewording needed Distancer les items 35 et 36 (et transformer 35 en positif: I feel my preparation is adequate)

132
Interview Oral Questions – Results: Qualitative 2 (Continued)
Interviews: 2nd round Interviews: 3rd round Interview questions
Expert 8 9 10 11 12 13
Items to reword of modify
in 1d list the types of performances, or add: please indicate the type (e.g. jury, competition, Small ensembles…) #4 Maybe reword this one – “I experience greater anxiety when I perform new repertoire‟ – or something like that. #11 I think this one needs to be reworded. Maybe “I focus well when I am stressed. #23 Good, but change hypersensitive to „very sensitive‟ #25.Good, but re-word in simpler terms.(e.g. It helps my performance). Use simpler term than facilitating/ debilitating: Do you think your performance are better or worst (reword it to something along those lines, Does it improve your performance, something like that).
Enlever "debilitating" et le remplacer par "it affects negatively" Partie 1 Item 7 (I feel highly anxious, worried and/or stressed) Veux-tu demander s'il y a une perte de contrôle? On peut être stressé sans perdre ses moyens. Item 9: After having perform I feel depressed "just thinking about it"? à rajouter ?Partie 2: Items semblables (6-12-14-16; 8-13; 11-19; 9-10-11-22) 24 m. Changer pour Lack of control (voice, fingers, etc.);
Adapt the language to easily connect with pop musicians
Situational factors of MPA: Items to delete
I would take solo performance out of b and add it on its own e.g in solo versus group
Low level of self-confidence is more an affective symptoms than a situational factor; Specific type of performance is not as important because you already refer to the most stressful performances
Some of them are not situational (e.g. item 1: I am an anxious person…)
Item 1 #3 I dread sight reading + lack of preparation and self-confidence are not situational factors
Items missing? Performing without the score Lieu inconnu (familiarité)
Imprévus Distractions, type of performance, and change the wording of the last 4
Something about teachers: how they affect me and how they help me (a "significant others, please specifiy, may be added in question 2)
Problematic acoustic, temperature. Make emphasis on the audience responsivity (which may be very stressful for pop performers)
Temporal occurrence: Items to delete
- Déplacer After having performed I feel depressed dans Manifestations
The items are conflated (conceptually overlapping)

133
Interview questions
Expert 8 9 10 11 12 13
Items missing? #6: add: a week prior to the performance; #7 add a space to specify when exactly it lessens
Ajouter "after the performance" dans l'item "I feel highly anxious, worried and/or stressed:"
A week or even a month before would be important
A week before
Behavioral symptoms: Items to delete
- Non, mais l'item sur les stress management techniques n'est pas un symptôme, c'est une stratégie.
There are overlaps with cognitive
Items missing? - La médication prescrite pour la personne (ex. Beta-blockers) et pas "empruntée" + est-ce qu'ils ont reçu un training pour l'anxiété?
Parler trop vite What kind of mistakes? Rushing, slowing down, over pedalling? + Rewording: I engage in nervous and/or repetitive behaviors + Looking relax or smile (inability to convey an appropriate demeanor)
I get facial tics
Cognitive symptoms: Items to delete
- Non, mais certains ont été déplacé dans Affective car étaient mal catégorisés
Items missing? Worries should be more in cognitive than affective
Débit des pensées est important et "unrelated thoughts
Breaking down the items for cognitive distorsions (catastrophization, all or nothing thinking, etc.)
#15 I find it hard to concentrate in front of people (too vague should be more specific)
Somatic symptoms: Items to delete
- Some items are overlapping with the cognitive: part 2 #3(relax) #9 (excited and energized) #22(don't have enough energy) #23 (depression)
The first 4 are problematics:#3(relax) #9 (excited and energized) #22(don't have enough energy) #23 (depression)
Items missing? - Rire nerveux I feel exhausted after having performed
Symptoms related to my instrument (shaking bow, over pedaling, etc.)
I am easily able to relax: Is this the body or the thoughts??? You have to make this clear
Diarrhea + j. Numbness/tingling
Affective symptoms: Items to delete
- Non, mais envoyer l'item sur "hypersensitive and to overreact" dans behavioral
I feel overwhelmed
Items missing? Change the word hypersensitive to "very sensitive"
Discours interne négatif, qui tourne, qui n'arrête pas
Internalized judgment (e.g. I fear that I am not good enough as a performer)

134
Appendix I
PerfAIM

135
Performance Anxiety Inventory for Musicians (PerfAIM) Below are some statements about stress and music performance anxiety. Based on your most recent STRESSFUL PERFORMANCE SITUATIONS, please indicate with a checkmark how much you agree with each statement.
Strongly disagree
Disagree Neutral Agree Strongly agree
1. I suffer from music performance anxiety.
2. I am an anxious person in my daily life.
3. My level of performance anxiety increases significantly due to:
a. A lack of preparation……………………………………………
b. A low level of self-confidence……………………………….
c. An intimidating audience …………………………………….
d. The presence of significant others………………………..
e. An unfamiliar performance environment……………...
f. Other musicians with whom I perform…………………..
g. A difficult repertoire…………………………………………….
h. A specific type of performance (e.g. auditions)……... Please specify:_________________________________________
i. Other (bad acoustics, room temperature, etc.).....…… Please specify: _________________________________________
4. Performing without the score is really stressful.
5. I feel very nervous when I perform new material/a new repertoire.
6. I feel highly anxious, worried and/or stressed:
a. A week prior to the performance …………………………
b. A day prior to the performance……………………………
c. Before going on stage…………………………………………..
d. While walking on stage………………………………………..
e. During the first pieces…………………………………………
f. During the most complicated pieces……………………..
g. During the entire performance…………………………….
7. At some point while performing, my anxiety lessens or goes away. Please specify:___________________
8. I am so stressed before a performance that I have trouble sleeping.
136
Strongly disagree
Disagree Neutral Agree Strongly agree
9. I am afraid the audience won’t respond favorably to my performance.
10. In a performance situation, I am easily able to relax physically.
11. I am afraid of making mistakes.
12. Negative thoughts and worries interfere with my performance.
13. I fear that I am not good enough as a performer.
14. I engage in repetitive behaviors (pacing, tapping, etc.)
15. I tend to make musical mistakes because of my anxiety.
16. I feel excited and energized when performing in front of people.
17. I perform most effectively under pressure.
18. When I perform, I am totally focused and engaged in the music.
19. I feel out of control.
20. I tend to avoid difficult pieces or passages for fear of failing in front of an audience.
21. I fear the worst will happen.
22. I find it hard to concentrate in front of people.
23. I am afraid of being judged.
24. I tend to have memory blanks.
25. I feel that when I am nervous, I don’t have enough energy to perform well.
26. I can easily get over my mistakes.
27. I enjoy performing.
28. I tend to be very sensitive or to overreact to any issues that occur during the performance (musical mistakes, external disturbances such ambient noises, inattentive audience, inadequate lighting, etc.)
29. I worry about the same things over and over.

137
Strongly disagree
Disagree Neutral Agree Strongly agree
30. Under stressful performance situations, I am affected by these symptoms:
a. Muscle tension and stiffness…………………………………
b. Upset stomach/butterflies……………………………………
c. Cold and/or sweaty palms……………………………………
d. Trembling (lips, voice, fingers, legs, etc.)………………
e. Racing and/or pounding heart……………………………..
f. Shortness of breath………………………………………………
g. Dry mouth…………………………………………………………...
h. Urge to urinate…………………………………………………….
i. Perspiration/flushing…………………………………………...
j. Numbness/tingling……………………………………………….
k. Dizziness…………………………………………………………….
l. Impaired coordination…………………………………………
m. Other(s). Please specify: ____________________________
31. Alcohol and/or recreational drugs help me cope with my performance anxiety.
32. *In performance situations, I deal with my nervousness by applying one or more stress management techniques (deep breathing, imagery, self-talk, relaxation, etc.).
33. Physical state of health (Since physical health issues may influence your level of music performance anxiety, please indicate any medical conditions that you are aware of: Raynaud’s phenomenon, tachycardia, etc.)
__________________________________________________________________ __________________________________________________________________ __________________________________________________________________
34. Mental state of health (Since mental health issues may influence your level of music performance anxiety, please indicate any medical conditions that you are aware of: anxiety disorder, depression, etc.)
__________________________________________________________________ __________________________________________________________________ _________________________________________________________________
Additional thoughts and comments:

138
Appendix J
Items Categorized by Domains

139
Items Categorized by Domains
Causes / Situational factors
I am an anxious person in my daily life.
Under stressful or challenging situations, my performance anxiety affects me negatively due to:
a. A lack of preparation
b. A low level of self-confidence
c. An intimidating audience
d. An unknown/unfamiliar performance environment
e. Other musicians with whom I perform
f. A difficult repertoire.
g. Other (please, specify):__________________________
I dread sight-reading during a performance.
Improvising in front of people makes me feel nervous.
Performing without the score is really stressful.
I feel very nervous when I perform new material/repertoire.
Temporal occurrence I am so stressed before a performance that I have trouble sleeping.
I feel highly anxious, worried and/or stressed:
a. The day prior to the performance
b. Before going on stage
c. While entering the stage
d. During the first pieces
e. During the most complicated pieces
f. During the entire performance
At some point while performing, my anxiety lessens/goes away.
Cognitive manifestations Negative thoughts interfere with my performance When I perform, I am totally focused and engaged in the music I find it hard to concentrate in front of people. I tend to have memory blanks when I perform. I can easily get over my mistakes when I perform. I have positive thoughts about performances.
I worry about the same things over and over
Affective manifestations I feel so anxious during the performance that I can‘t perform to my normal level. I feel overwhelmed by the performance. I am afraid of making mistakes in front of people. I feel the outcome of the performance is beyond my control. I fear the worst will happen when performing. I am afraid of being judged. I enjoy performing. Under stressful or challenging situations, I feel that my performance anxiety helps me perform well.

140
Behavioral manifestations In performance situations, I deal with my nervousness by applying one or more stress management
techniques (deep breathing, imagery, self-talk, relaxation, etc.). I tend to make musical mistakes because of my anxiety. Prior to the performance, I adopt repetitive behaviors (pacing, taping, etc.) I perform most effectively under pressure. I tend to avoid difficult pieces or difficult passages for fear of failing in front of an audience. Alcohol and/or recreational drugs help me cope with my performance anxiety. I tend to be very sensitive or to overreact to any issues that occur during the performance (musical
mistakes; external disturbances such ambient noises, inattentive audience, inadequate lighting; etc)
Somatic manifestations I am easily able to relax in a performance situation I feel excited and energized when performing in front of people I feel that when I am nervous, I don‘t have enough energy to perform well. After having performed, I feel depressed and/or exhausted Under stressful or challenging performance situations, these symptoms bother me EXTREMELY:
a. Muscle tension and stiffness
b. Upset stomach/butterflies
c. Cold and/or sweaty palms
d. Trembling (lips, voice, fingers, legs, etc.)
e. Racing and/or pounding heart
f. Shortness of breath
g. Dry mouth
h. Urge to urinate
i. Perspiration / flushing
j. Numbness
k. Dizziness
l. Impaired coordination
m. Lack of voice and/or finger control
n. Nervous tics
o. Headache
p. Other (please, specify):