percutaneous recanalization and balloon angioplasty of congenital isolated local atresia of the...
TRANSCRIPT

Percutaneous Recanalization and Balloon Angioplastyof Congenital Isolated Local Atresia of the
Aortic Isthmus in Adults
George Joseph,* MD, DM, Asishkumar Mandalay, MD, DM, and G. Rajendiran, MD, DM
Congenital isolated local atresia of the aortic isthmus is anatomically similar and mor-phogenetically related to congenital coarctation of the aorta and was encountered in 4out of 26 consecutive adult patients selected for coarctation angioplasty at our center.Anterograde recanalization of the atresia was safely and successfully accomplished in allfour patients, using a brachial approach. Balloon dilation in the four patients, withancillary stent implantation in one patient, resulted in reduction of translesion gradientfrom 84 6 11 mm Hg to 9 6 7 mm Hg without complications. Angiography in the threenon-stented patients after a mean follow-up of 13 months showed no evidence ofrestenosis, dissection or aneurysm formation, though one patient had mild dilatation ofthe posterior aspect of the aortic isthmus. The clinical presentation of patients withisolated local aortic atresia, and their short- to mid-term response to percutaneoustreatment, is similar to that of patients with isolated severe coarctation of aorta. CathetCardiovasc Intervent 2001;53:535–541. © 2001 Wiley-Liss, Inc.
Key words: aortic arch interruption; coarctation of aorta; balloon angioplasty
INTRODUCTION
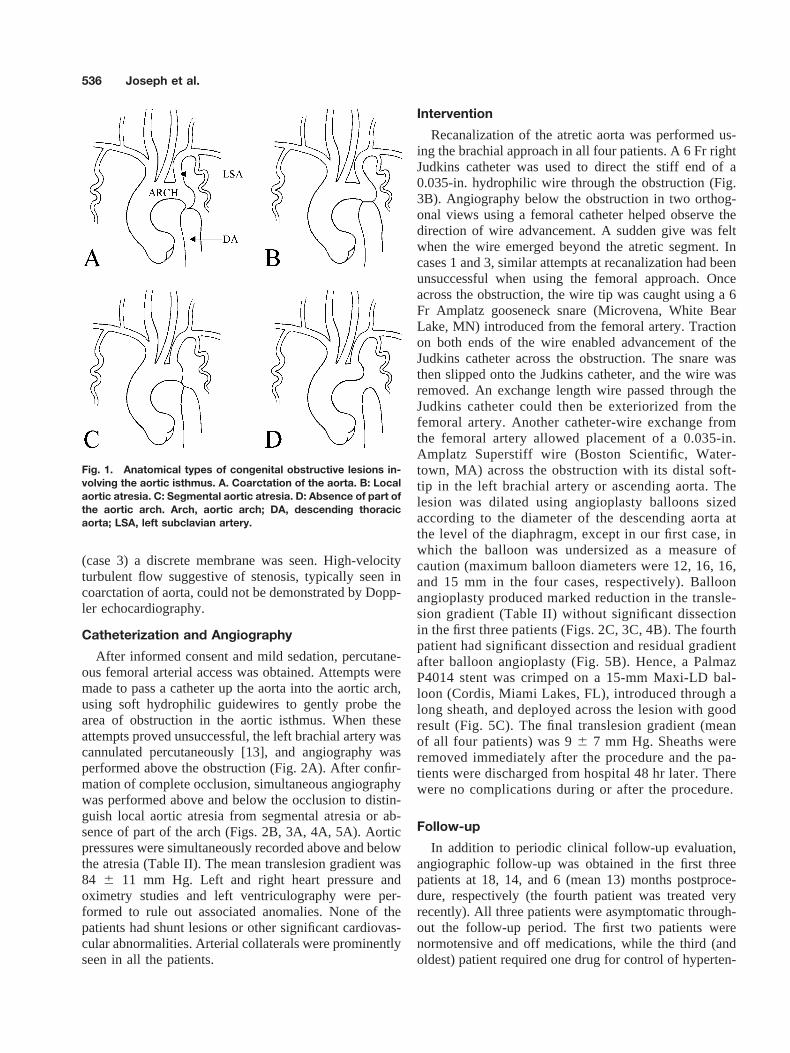
The term interruption of the aortic arch encompasseslocal and segmental aortic atresia and absence of a part ofthe aortic arch [1]. Type A aortic arch interruption (lo-cated distal to the left subclavian artery)[2] is consideredto be morphogenetically related to typical coarctation ofthe aorta, and is distinct from the other types of aorticarch interruption (located proximal to the left subclavianartery)[1]. Although hemodynamically similar, severecoarctation of the aorta and each kind of type A aorticarch interruption are anatomically distinct. In coarctationof aorta, both anatomic continuity and luminal patency ofthe aorta are preserved (Fig. 1A). In aortic arch atresia,the arch and descending aorta are connected, and there iseither local complete obliteration of the lumen (Fig. 1B)or a segment of the aortic arch is converted into a fibrouscord [1] (Fig. 1C). In absence of a part of the aortic arch,a segment of the distal arch is missing without a trace ofanatomic connection across the gap [1] (Fig. 1D). Theseanatomic features are of particular relevance in determin-ing the feasibility of percutaneous interventions in thetreatment of these conditions. Coarctation of aorta isgenerally suited to therapy with balloon angioplasty; thismethod of treatment has proved an effective alternativeto surgery in children [3–5], and in adolescents andadults as well [6–10]. Local aortic atresia is potentiallyamenable to percutaneous treatment given that (1) localatresia of the aortic isthmus anatomically resembles se-
vere coarctation; and (2) percutaneous procedures havebeen successful in analogous situations such as pulmo-nary valve atresia [11] and inferior vena cava webs [12].In this article, we discuss the cases of four adult patientswho presented with congenital isolated local atresia ofthe aortic isthmus and underwent successful percutane-ous intervention.
CASE REPORTS
Twenty-six adult patients (mean age 276 12 years,range 15–54 years, 22 males/4 females), diagnosed tohave congenital coarctation of the aorta based on clinicalfeatures and noninvasive evaluation, underwent angiog-raphy, followed by angioplasty (with ancillary stent de-ployment in eight patients) at our center over the lastseven years. Four of these patients had isolated localatresia of the aortic isthmus (see Table I for clinicalfeatures). In three patients, the atresia could not be visu-alized by surface echocardiography, but in one patient
Department of Cardiology, Christian Medical College Hospital,Vellore, South India.
*Correspondence to: Dr. George Joseph, Department of Cardiology,Christian Medical College Hospital, Vellore 632 004, South India.E-mail: [email protected]
Received 27 November 2000; Accepted 5 March 2001
Catheterization and Cardiovascular Interventions 53:535–541 (2001)
© 2001 Wiley-Liss, Inc.
(case 3) a discrete membrane was seen. High-velocityturbulent flow suggestive of stenosis, typically seen incoarctation of aorta, could not be demonstrated by Dopp-ler echocardiography.
Catheterization and Angiography
After informed consent and mild sedation, percutane-ous femoral arterial access was obtained. Attempts weremade to pass a catheter up the aorta into the aortic arch,using soft hydrophilic guidewires to gently probe thearea of obstruction in the aortic isthmus. When theseattempts proved unsuccessful, the left brachial artery wascannulated percutaneously [13], and angiography wasperformed above the obstruction (Fig. 2A). After confir-mation of complete occlusion, simultaneous angiographywas performed above and below the occlusion to distin-guish local aortic atresia from segmental atresia or ab-sence of part of the arch (Figs. 2B, 3A, 4A, 5A). Aorticpressures were simultaneously recorded above and belowthe atresia (Table II). The mean translesion gradient was84 6 11 mm Hg. Left and right heart pressure andoximetry studies and left ventriculography were per-formed to rule out associated anomalies. None of thepatients had shunt lesions or other significant cardiovas-cular abnormalities. Arterial collaterals were prominentlyseen in all the patients.
Intervention
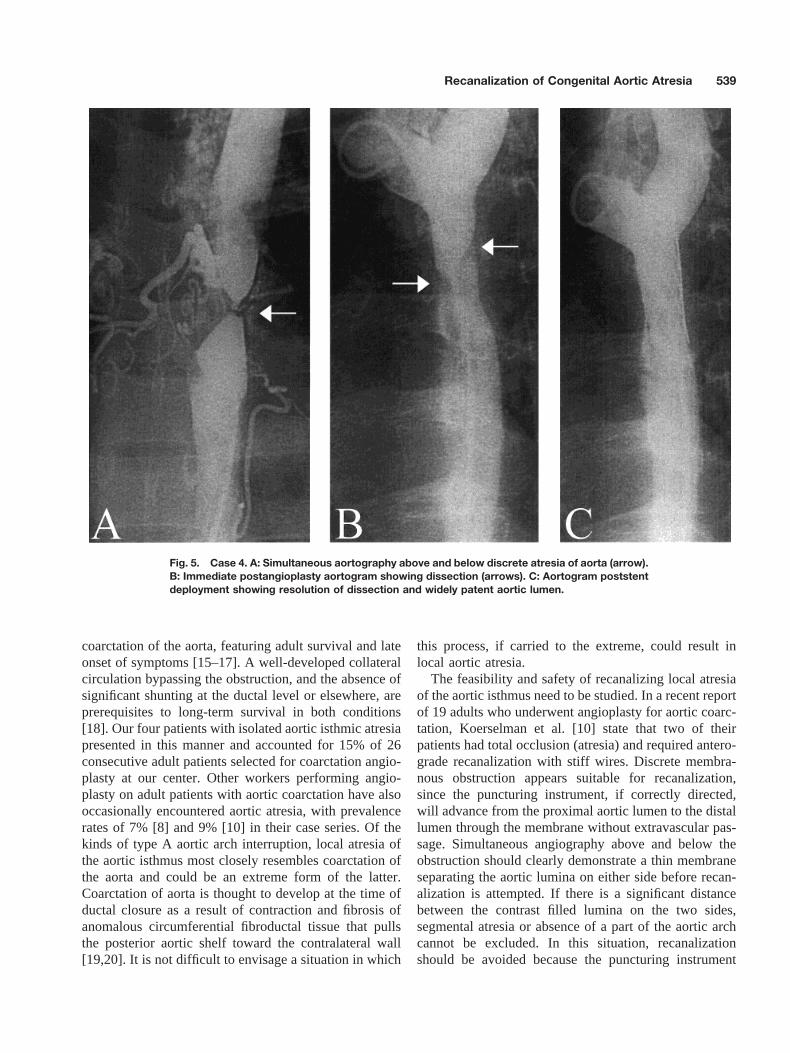
Recanalization of the atretic aorta was performed us-ing the brachial approach in all four patients. A 6 Fr rightJudkins catheter was used to direct the stiff end of a0.035-in. hydrophilic wire through the obstruction (Fig.3B). Angiography below the obstruction in two orthog-onal views using a femoral catheter helped observe thedirection of wire advancement. A sudden give was feltwhen the wire emerged beyond the atretic segment. Incases 1 and 3, similar attempts at recanalization had beenunsuccessful when using the femoral approach. Onceacross the obstruction, the wire tip was caught using a 6Fr Amplatz gooseneck snare (Microvena, White BearLake, MN) introduced from the femoral artery. Tractionon both ends of the wire enabled advancement of theJudkins catheter across the obstruction. The snare wasthen slipped onto the Judkins catheter, and the wire wasremoved. An exchange length wire passed through theJudkins catheter could then be exteriorized from thefemoral artery. Another catheter-wire exchange fromthe femoral artery allowed placement of a 0.035-in.Amplatz Superstiff wire (Boston Scientific, Water-town, MA) across the obstruction with its distal soft-tip in the left brachial artery or ascending aorta. Thelesion was dilated using angioplasty balloons sizedaccording to the diameter of the descending aorta atthe level of the diaphragm, except in our first case, inwhich the balloon was undersized as a measure ofcaution (maximum balloon diameters were 12, 16, 16,and 15 mm in the four cases, respectively). Balloonangioplasty produced marked reduction in the transle-sion gradient (Table II) without significant dissectionin the first three patients (Figs. 2C, 3C, 4B). The fourthpatient had significant dissection and residual gradientafter balloon angioplasty (Fig. 5B). Hence, a PalmazP4014 stent was crimped on a 15-mm Maxi-LD bal-loon (Cordis, Miami Lakes, FL), introduced through along sheath, and deployed across the lesion with goodresult (Fig. 5C). The final translesion gradient (meanof all four patients) was 96 7 mm Hg. Sheaths wereremoved immediately after the procedure and the pa-tients were discharged from hospital 48 hr later. Therewere no complications during or after the procedure.
Follow-up
In addition to periodic clinical follow-up evaluation,angiographic follow-up was obtained in the first threepatients at 18, 14, and 6 (mean 13) months postproce-dure, respectively (the fourth patient was treated veryrecently). All three patients were asymptomatic through-out the follow-up period. The first two patients werenormotensive and off medications, while the third (andoldest) patient required one drug for control of hyperten-
Fig. 1. Anatomical types of congenital obstructive lesions in-volving the aortic isthmus. A. Coarctation of the aorta. B: Localaortic atresia. C: Segmental aortic atresia. D: Absence of part ofthe aortic arch. Arch, aortic arch; DA, descending thoracicaorta; LSA, left subclavian artery.
536 Joseph et al.

sion. The noninvasive lower limb blood pressure wasmarginally less than upper limb blood pressure (TableII). Catheterization showed minor residual translesiongradient (mean 136 11 mm Hg), which was not signif-icantly different from that obtained immediately after theprocedure (mean 116 6 mm Hg). Angiography revealedmild dilation of the posterior aspect of the aortic isthmusin case 1, and no evidence of aneurysm formation ordissection in any of the cases (Figs. 2D, 3D, 4C).
DISCUSSION
Interruption of the aortic arch can be considered anextreme expression in the spectrum of obstructive tho-racic aortic anomalies that begin with coarctation [14].Aortic arch interruption is usually ductus dependent andassociated with poor survival but infrequently occurs asan isolated anomaly [14]. The natural history of isolatedaortic arch interruption resembles that of isolated severe
Fig. 2. Case 1. A: Arch aortogram, showing atresia of the aortic isthmus (arrow). B: Simulta-neous aortography above and below discrete atresia of aorta (arrow). C: Immediate postangio-plasty aortogram, showing satisfactory result. D: Follow-up aortogram, showing absence ofrestenosis and mild dilation of the posterior aspect of the aorta (arrow).
TABLE I. Clinical Features*
CaseAge(yr) Sex
Wt(kg) Presentation Duration Chest x-ray Other features
1 19 M 43 Exertional dyspnea, mildlower limbclaudication,hypertension
7 mo8 mo8 mo
Cardiomegaly, rib notching Bicuspid aortic valve with32-mm Hg peakgradient, skeletaldysmorphism
2 28 F 44 Exertional palpitations,hypertension
1 yr2 yr
LV configuration, ribnotching, figure 3silhouette
Bicuspid aortic valve with22-mm Hg peakgradient
3 54 M 64 Asymptomatic,hypertension
4 yr Rib notching, figure 3silhouette
Bicuspid aortic valve withmild regurgitation
4 21 M 47 Lower limb fatigue,hypertension
2 yr2 mo
LV configuration, ribnotching
Bicuspid aortic valve withmild regurgitation
M, male; F, female; LV configuration, left ventricular configuration.*Duration denotes time since presenting feature was first experienced or detected.
Recanalization of Congenital Aortic Atresia 537

Fig. 3. Case 2. A: Simultaneous aortography above and below discrete atresia of aorta (arrow).B: Anterograde puncture of atretic membrane with stiff wire. C: Immediate postangioplastyaortogram showing satisfactory result. D: Follow-up aortogram showing absence of restenosisor aneurysm formation.
Fig. 4. Case 3. A: Simultaneous aortography above and below discrete atresia of aorta (arrow).B: Immediate postangioplasty aortogram showing satisfactory result. C: Follow-up aortogramshowing absence of restenosis or aneurysm formation.
538 Joseph et al.
coarctation of the aorta, featuring adult survival and lateonset of symptoms [15–17]. A well-developed collateralcirculation bypassing the obstruction, and the absence ofsignificant shunting at the ductal level or elsewhere, areprerequisites to long-term survival in both conditions[18]. Our four patients with isolated aortic isthmic atresiapresented in this manner and accounted for 15% of 26consecutive adult patients selected for coarctation angio-plasty at our center. Other workers performing angio-plasty on adult patients with aortic coarctation have alsooccasionally encountered aortic atresia, with prevalencerates of 7% [8] and 9% [10] in their case series. Of thekinds of type A aortic arch interruption, local atresia ofthe aortic isthmus most closely resembles coarctation ofthe aorta and could be an extreme form of the latter.Coarctation of aorta is thought to develop at the time ofductal closure as a result of contraction and fibrosis ofanomalous circumferential fibroductal tissue that pullsthe posterior aortic shelf toward the contralateral wall[19,20]. It is not difficult to envisage a situation in which
this process, if carried to the extreme, could result inlocal aortic atresia.
The feasibility and safety of recanalizing local atresiaof the aortic isthmus need to be studied. In a recent reportof 19 adults who underwent angioplasty for aortic coarc-tation, Koerselman et al. [10] state that two of theirpatients had total occlusion (atresia) and required antero-grade recanalization with stiff wires. Discrete membra-nous obstruction appears suitable for recanalization,since the puncturing instrument, if correctly directed,will advance from the proximal aortic lumen to the distallumen through the membrane without extravascular pas-sage. Simultaneous angiography above and below theobstruction should clearly demonstrate a thin membraneseparating the aortic lumina on either side before recan-alization is attempted. If there is a significant distancebetween the contrast filled lumina on the two sides,segmental atresia or absence of a part of the aortic archcannot be excluded. In this situation, recanalizationshould be avoided because the puncturing instrument
Fig. 5. Case 4. A: Simultaneous aortography above and below discrete atresia of aorta (arrow).B: Immediate postangioplasty aortogram showing dissection (arrows). C: Aortogram poststentdeployment showing resolution of dissection and widely patent aortic lumen.
Recanalization of Congenital Aortic Atresia 539
could exit and reenter the aorta, and balloon dilation ofthis track could have untoward consequences. During therecanalization procedure, the direction of movement ofthe puncturing instrument should be monitored underfluoroscopy in two orthogonal views, and the aortic lu-men on the other side of the obstruction should beobserved by repeated contrast injections. This will helpthe operator direct the instrument appropriately and min-imize the chances of aortic perforation.
The anatomic similarity between local atresia of theaortic isthmus and coarctation of the aorta prompted us toequate the size of angioplasty balloon used to the diam-eter of the descending aorta at the level of the diaphragm,as is done in coarctation angioplasty [7,21]. In three ofthe four patients, this produced marked and sustainedreduction in translesion gradient to acceptable levels, andsatisfactory angiographic appearance of the dilated le-sion. The need for ancillary stenting in one of the fourpatients is consistent with the requirement of stents in30% of adult patients undergoing angioplasty for aorticcoarctation at our center. Although there was no evidenceof aneurysm formation at follow-up, dilation of the pos-terior aspect of the aorta that was noted in one patientmakes long-term surveillance of aortic dimensions man-datory in all patients. The persistence of systemic hyper-tension in one patient despite successful angioplasty out-come is not unexpected. Normalization of blood pressurewithout medication after angioplasty for aortic coarcta-tion occurs in 74–79% of adult patients, but not in theremainder [9,22]. The current trend in practice favorstranscatheter therapy over surgery in older children and
adults with coarctation of aorta [23]. Before the same canbe said of local aortic atresia, more such procedures needto be done and long-term follow-up must be obtained. Ofparticular relevance to aortic atresia would be informa-tion on potential complications such as dissection orperforation related to the recanalization procedure, aswell as long-term development of restenosis or aneu-rysms at the angioplasty site.
In conclusion, percutaneous treatment is feasible incertain cases of local atresia of the aortic isthmus. Withproper case selection and appropriate precautions, recan-alization and balloon angioplasty/stenting can be safelyand successfully performed. The clinical presentation ofpatients with isolated local aortic atresia, and their short-to mid-term response to percutaneous treatment, is sim-ilar to that of patients with isolated severe coarctation ofaorta. This is in keeping with the anatomic similarity andmorphogenetic relation that exists between the two con-ditions.
REFERENCES
1. Van Mierop LHS, Kutsche LM. Interruption of the aortic arch andcoarctation of the aorta: pathogenetic relations. Am J Cardiol1984;54:829–834.
2. Celoria GC, Patton RB. Congenital absence of the aortic arch. AmHeart J 1959;58:407–413.
3. Cooper RS, Ritter SB, Rothe WB, Chen CK, Griepp R, GolinkoRJ. Angioplasty for coarctation of the aorta: long-term results.Circulation 1987;75:600–604.
4. Rao PS, Thapar MK, Galal O, Wilson AD. Follow-up results ofballoon angioplasty of native coarctation in neonates and infants.Am Heart J 1990;120:1310–1314.
TABLE II. Pressure Data*
Pressures
Noninvasiveright arm
pressure S/D
Noninvasivelower limb
pressure S/DProximal aortic
pressure S/D (M)Distal aortic
pressure S/D (M)Peak systolic
gradient
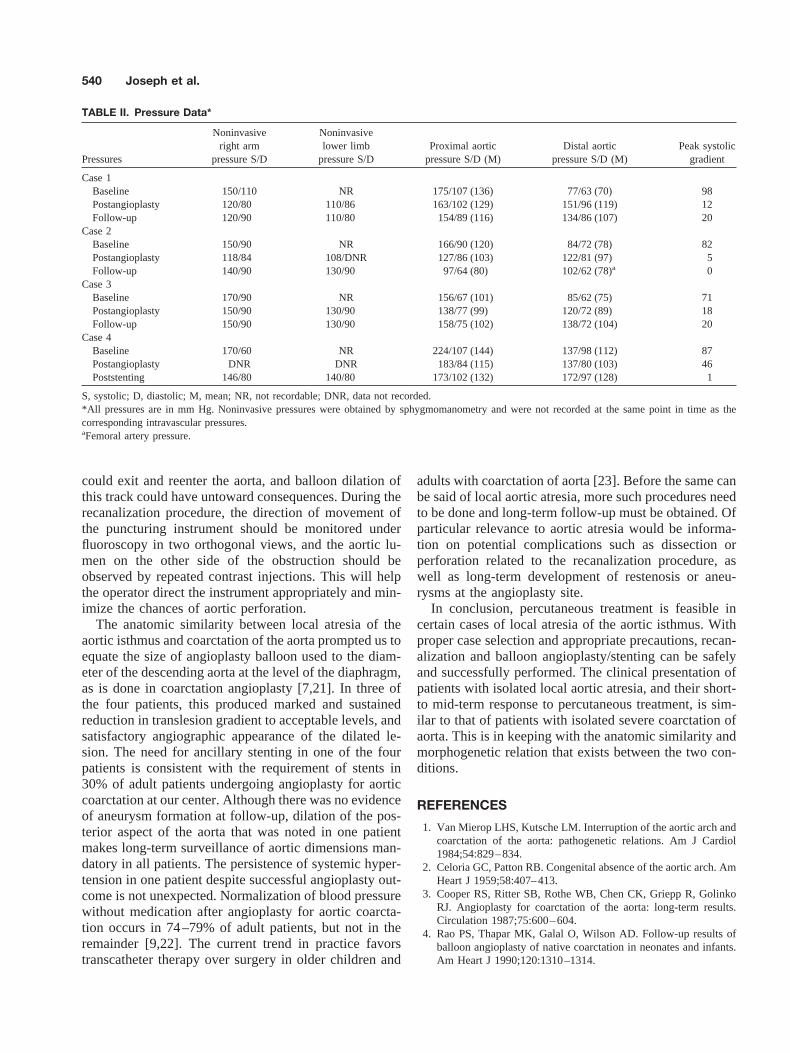
Case 1Baseline 150/110 NR 175/107 (136) 77/63 (70) 98Postangioplasty 120/80 110/86 163/102 (129) 151/96 (119) 12Follow-up 120/90 110/80 154/89 (116) 134/86 (107) 20
Case 2Baseline 150/90 NR 166/90 (120) 84/72 (78) 82Postangioplasty 118/84 108/DNR 127/86 (103) 122/81 (97) 5Follow-up 140/90 130/90 97/64 (80) 102/62 (78)a 0
Case 3Baseline 170/90 NR 156/67 (101) 85/62 (75) 71Postangioplasty 150/90 130/90 138/77 (99) 120/72 (89) 18Follow-up 150/90 130/90 158/75 (102) 138/72 (104) 20
Case 4Baseline 170/60 NR 224/107 (144) 137/98 (112) 87Postangioplasty DNR DNR 183/84 (115) 137/80 (103) 46Poststenting 146/80 140/80 173/102 (132) 172/97 (128) 1
S, systolic; D, diastolic; M, mean; NR, not recordable; DNR, data not recorded.*All pressures are in mm Hg. Noninvasive pressures were obtained by sphygmomanometry and were not recorded at the same point in time as thecorresponding intravascular pressures.aFemoral artery pressure.
540 Joseph et al.

5. Shaddy RE, Boucek MM, Sturtevant JE, Ruttenberg HD, JaffeRB, Tani LY, Judd VE, Veasy LG, McGough EC, Orsmond GS.Comparison of angioplasty and surgery for unoperated coarctationof the aorta. Circulation 1993;87:793–799.
6. Fawzy ME, Dunn B, Galal O, Wilson N, Shaik A, Sriram R,Duran CMG. Balloon coarctation angioplasty in adolescents andadults. early and intermediate results. Am Heart J 1992;124:167–171.
7. Tyagi S, Arora R, Kaul UA, Sethi KK, Gambhir DS, KhalilullahM. Balloon angioplasty of native coarctation of the aorta inadolescents and young adults. Am Heart J 1992;123:674–680.
8. Phadke K, Dyet JF, Hartley W. Balloon angioplasty of adult aorticcoarctation. Br Heart J 1993;69:36–40.
9. Schrader R, Bussmann WD, Jacobi V, Kadel C. Long-term effectsof balloon coarctation angioplasty on arterial blood pressure inadolescent and adult patients. Cathet Cardiovasc Diagn 1995;36:220–225.
10. Koerselman J, de Vries H, Jaarsma W, Muyldermans L, ErnstJMPG, Plokker HWM. Balloon angioplasty of coarctation of theaorta: a safe alternative for surgery in adults: immediate andmid-term results. Cathet Cardiovasc Intervent 2000;50:28–33.
11. Redington AN, Cullen S, Rigby MC. Laser or radiofrequencypulmonary valvotomy in neonates with pulmonary atresia withintact ventricular septum using a commercially available radiofre-quency catheter. Pediatr Cardiol 1997;18:61–63.
12. Yang XL, Cheng TO, Chen CR. Successful treatment by percu-taneous balloon angioplasty of Budd-Chiari syndrome caused bymembranous obstruction of inferior vena cava: an eight-year fol-low-up study. J Am Coll Cardiol 1996;28:1720–1724.
13. Joseph G, Baruah DK, Krishnaswami S. Combined brachial and
femoral approach to balloon angioplasty in coarctation of aorta.Cathet Cardiovasc Diagn 1997;42:196-200.
14. Perloff JK. The clinical recognition of congenital heart disease.Philadelphia: WB Saunders; 1994. 156 p.
15. Dische MR, Tsai M, Baltaxe HA. Solitary interruption of the archof the aorta. Clinicopathologic review of eight cases. Am J Cardiol1975;35:271–277.
16. Milo S, Massini C, Goor DA. Isolated atresia of the aortic arch ina 65-year-old man. Surgical treatment and review of publishedreports. Br Heart J 1982;47:294–297.
17. Sharratt GP, Carson P, Sanderson JM. Complete interruption ofaortic arch, without persistent ductus arteriosus, in an adult. BrHeart J 1975;37:221–224.
18. Kauff MK, Bloch J, Baltaxe HA. Complete interruption of theaortic arch in adults. Radiology 1973;106:53–57.
19. Talner NS, Berman MA. Postnatal development of obstruction incoarctation of the aorta: role of the ductus arteriosus. Pediatrics1975;56:562–569.
20. Rocchini AP. Coarctation of the aorta and interrupted aortic arch.In: Moller JH, Hoffman JIE, editors. Pediatric cardiovascularmedicine. New York: Churchill Livingstone; 2000. p 567–593.
21. Rao PS. Transcatheter therapy in pediatric cardiology. New York:Wiley-Liss; 1993. 157 p.
22. Fawzy ME, Sivanandam V, Pieters F, Stefadouros MA, Galal O,Dunn B, Kinsara A, Khan B, Al-Halees Z. Long-term effects ofballoon angioplasty on systemic hypertension in adolescent andadult patients with coarctation of the aorta. Eur Heart J 1999;20:827–832.
23. McCrindle BW. Coarctation of the aorta. Curr Opin Cardiol1999;14:448–452.
Recanalization of Congenital Aortic Atresia 541