pediatric dermatology. differences in adult and neonatal skin adult skinneonatal skin...
TRANSCRIPT
Pediatric dermatology
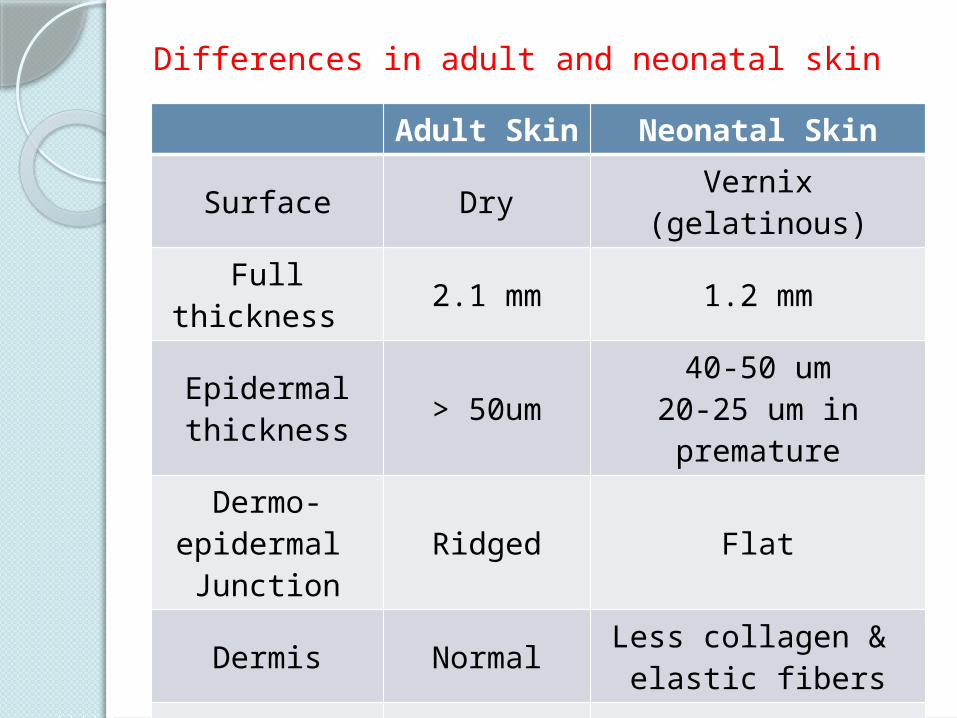
Differences in adult and neonatal skin
Adult Skin Neonatal Skin
Surface Dry Vernix (gelatinous)
Full thickness 2.1 mm 1.2 mm
Epidermalthickness
> 50um40-50 um
20-25 um in premature
Dermo-epidermal Junction
Ridged Flat
Dermis NormalLess collagen &
elastic fibers
Melanosomes Normal Fewer
Hair Normal Less
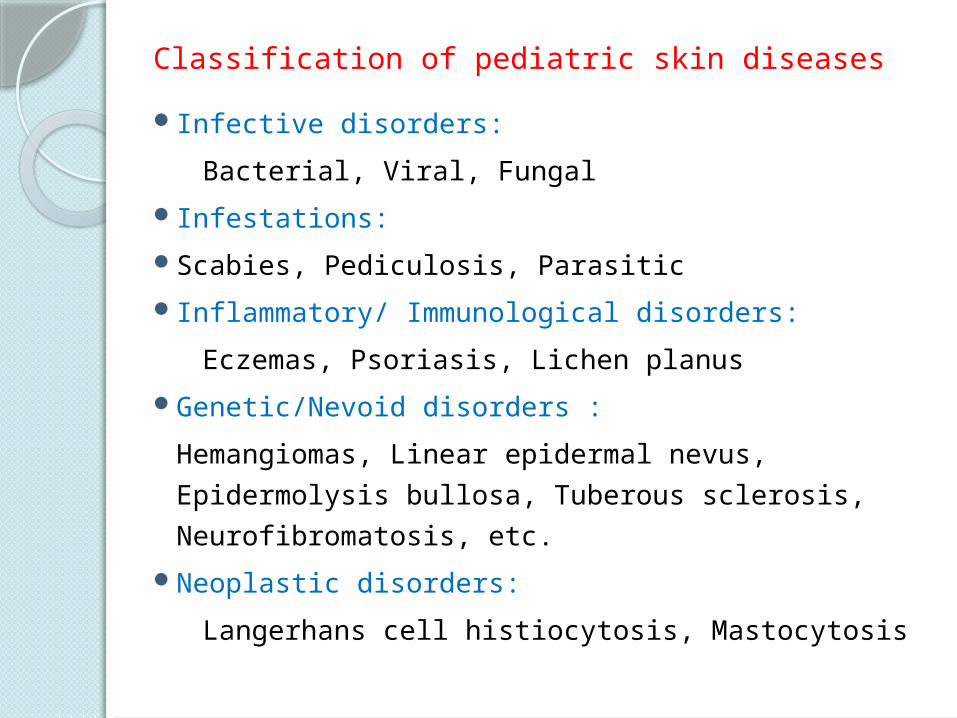
Classification of pediatric skin diseasesInfective disorders:
Bacterial, Viral, FungalInfestations: Scabies, Pediculosis, ParasiticInflammatory/ Immunological disorders:
Eczemas, Psoriasis, Lichen planusGenetic/Nevoid disorders :
Hemangiomas, Linear epidermal nevus, Epidermolysis bullosa, Tuberous sclerosis, Neurofibromatosis, etc.
Neoplastic disorders:
Langerhans cell histiocytosis, Mastocytosis
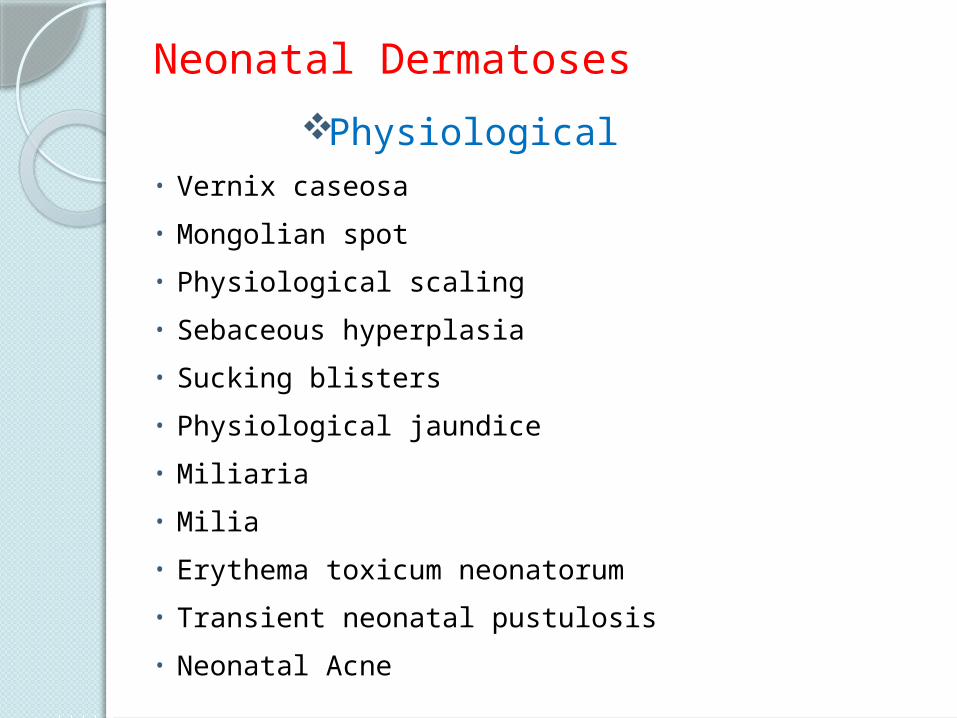
Neonatal Dermatoses
Physiological• Vernix caseosa
• Mongolian spot
• Physiological scaling
• Sebaceous hyperplasia
• Sucking blisters
• Physiological jaundice
• Miliaria
• Milia
• Erythema toxicum neonatorum
• Transient neonatal pustulosis
• Neonatal Acne
Mongolian spotSingle or multiple slate gray or blue macules of
size 3 to 10 cmsSeen at birth Seen over lumbosacral region, buttocks,
shouldersFade within the first 3-4 years of life

Physiological scalingSeen in 75% normal infantsOccurs within first week of lifeFirst around the ankles, later on hands and feet
and soon becomes generalizedMaximum intensity by eighth day, subsides by
3-4 weeksNo treatment required
Sucking blisterOne or two solitary blistersPresent at birthSeen over fingertips / hands / forearmCaused by vigorous suckingHeals rapidly without treatment within 2 weeks
of lifeDifferential diagnosis: Herpes simplex, Bullous
impetigo, Epidermolysis bullosa
Miliaria
Superficial vesicles resulting from sweat retention in stratum corneum
A. Miliaria crystallina:Following fever, phototherapyTiny clear vesicles seen over forehead, neckErythema absentPeels off within 24 hrs
Miliaria
B. Miliaria rubra (prickly heat)Seen in hot weatherNon follicular papules on erythematous base1 to 4 mm in diameterTrunk, faceSubside in 2 to 3 daysItching, secondary infection is common
Infantile and Childhood dermatoses
Infective and inflammatory diseases have been discussed in respective chapters. Certain common and genetic-naevoid conditions seen in infants and children will be discussed including: Cradle cap, Diaper dermatitis Nevus depigmentosus, Linear epidermal nevus Haemangiomas, Vascular malformations Sturge Weber syndrome Neurofibromatosis, Tuberous sclerosis Epidermolysis bullosa Ichthyosis
Cradle cap Seborrhoeic dermatitis of scalp Thick, greasy, adherent scales on scalp Commonly begins in the first 3 months Self limitingApply oil for few hours to soften scales, rinse, 1%
hydrocortisone cream can be used
Diaper dermatitis (Napkin rash) Irritant dermatitis in the perineal regionDue to occlusion, fricton and prolonged skin
contact with urine, faeces and fabrics Wetness leads to maceration of skin Secondary infection by C.albicans is common
Nevus Depigmentosus Single, well circumscribed, hypopigmented or
depigmented macule or patch Seen at birth Stable in size and distribution Seen over trunk and proximal extremities
Linear epidermal nevus Congenital hamartomas of embryonal ectodermal
origin Seen in early childhood as a linear raised warty
lesion Located over neck, trunk and extremities
HemangiomasIncidence more in preterm infantsFemale predilection Begin at one month of ageUndergo a proliferative phase followed by
stabilization and eventual spontaneous involution
ComplicationsUlceration, bleedingSecondary infectionMutilation and scarringCosmetic disfigurement
Vascular malformationsStable dilatations of superficial or deep
vasculatureCan be capillary, arterial, venous, lymphatic or
mixed
Clinical types: Salmon patchPortwine stainSturge-Weber syndromeKlippel-Trenaunay syndrome
Salmon Patch Present in 30 to 40% of neonatesSuperficial, red or pink flat lesionsSeen over forehead, upper eyelid, glabellar area,
nape of neckResolution in first year of life
Portwine Stain (Nevus flammeus) Present at birthCommon sites are face, neck and mucous
membraneFlat pink-red lesion Sharply unilateral in distributionPersist in childhood and darker in adulthood
Complications Glaucoma, Choroidal angiomas
Sturge-Weber SyndromePortwine stain in distribution of first branch of
trigeminal nerve May be associated with seizures, ipsilateral
glaucoma, behavioral problems, mental retardation
Characteristic intracranial S-shaped calcifications
Neurofibromatosis (NF)Riccardi classified NF into eight distinct clinical
types in 1982 Autosomal dominant disorder Affects skin, soft tissue, nervous system, bone,
other organsClassical skin lesions are café au lait macules,
neurofibromas
Neurofibromatosis - 1 (Von Recklinghausen’s disease)
Diagnostic criteria for NF-1
Presence of two or more of the following:Six or more café au lait macules larger than 5 mmTwo or more neurofibromas of any type or 1
plexiform neurofibroma Axillary or inguinal frecklingTwo or more Lisch nodules (brown coloured small
nodules on iris surface)Optic gliomaA distinctive osseous lesionA first-degree relative with NF-1
Neurofibromatosis - 2Bilateral acoustic neuromasMultiple CNS tumorsFew café au lait maculesFew neurofibromasNo axillary frecklingNo Lisch nodules
Tuberous sclerosis (Bourneville’s disease)
Syn. EPILOIA (Epilepsy, Low IQ, Adenoma sebaceum)
Ash leaf macules/ hypopigmented maculesAdenoma sebaceum (angiofibroma) begins at 2-5 years of age as small pink papules on mid-
faceShagreen’s patch (yellowish brown plaque on
lumbo - sacral area)Koenen’s tumors (periungual fibroma)Mental retardationSeizures
Epidermolysis bullosaInherited bullous disorders characterized by
blister formation in response to mechanical trauma
Onset at birth or shortly after Seen on sites of trauma and frictionTypes: Simple, Junctional, DystrophicSome subtypes, especially the milder EB forms,
improve with ageAutosomal recessive types have bad prognosis
with severe mucosal, esophageal involvement and atrophic scarring of skin

IchthyosisInherited disorder of keratinization Characterized by the accumulation of scales on the
skin surface, dry skinFish like scales most prominent over the trunk,
abdomen, buttocks and legs May be associated with ectropion, eclabion, nail
dystrophy, internal organ involvement
Types: Ichthyosis vulgaris X-linked ichthyosis Lamellar ichthyosis Collodion baby / Harlequin fetus
Adolescent DermatosesAcneDandruffStriaePseudo-acanthosis nigricansContact dermatitis to cosmetics, perfumes,
artificial jewellery / accessories (metals)Hyperhidrosis
Acne vulgarisCharacterized by comedones, papules, pustules
and nodules Common in malesSeen around puberty Sites: face, upper part of the chest, back,
shoulders
Complications Psychological impact Hyperpigmentation Scarring
Dandruff (Pityriasis sicca/capitis)
Most common condition affecting the scalpCausative organism: Malassezia speciesSeen as mild, moderate or severe scaling of scalpMay or may not associated with itchingSimple dandruff does not cause hair loss
Striae (stretch marks)
Seen as pinkish white lines around knees, axillae, outer aspect of thighs, lumbosacral region
Sudden increase in height or weight causes rupture of connective tissue beneath an intact epidermis
Pseudo-acanthosis nigricans
Weight gain in puberty produces dark, thick, velvety skin in neck, axillae, groins
Asymptomatic
Side effects of cosmetic products
Cosmetic products like eye liner, ‘fairness’ creams, lipstick, nail polish, henna can produce contact reactions
Reactions may be immediate or delayed
Types of reactions Folliculitis Acneiform eruptions Contact dermatitis Pigmentary changes
Child abuse
Includes physical abuse, neglect, sexual exploitation
Cutaneous manifestations Bruises Traumatic alopecia Thermal burnsSexual abuse: Vaginal tears, anal tears,
hematomasSexually transmitted infections
Care of newborn
Gentle handlingAvoid frictional traumaUse gentle soaps, cleansers Too frequent bathing may lead to drynessMaintain hygiene after feeds, diaper changesKeep body folds dry and ventilated
Skin care in pre-termsGentle handlingUse adhesive tape sparinglyAvoid frictional trauma
General principles of skin care in children
Bathing, soaps and cleansersThere is no need to use special cleansing
productsExcessive cleansing, scrubbing and incomplete
rinsing lead to irritation
ShampoosShould be isotonic to tears and less irritating to
eyesShampooing twice a week controls normal flaking
Care of the diaper areaFrequent diaper changes with gentle cleansing
and limiting use of plastic or rubber diaper cover
Differences in treatment of Paediatric and Adult Patients
Conservative management is bestSurface area is more in children as compared
with adultsPercentage of absorption of topical drugs is
moreTry to use lowest effective dose of medicationsDo not use treatments which may retard growth
or mental developmentAvoid off-label uses of medications

Thank you