peads- diamond blackfan anemia
TRANSCRIPT

Presented by:1) Cheong Kai Liang0701002332) Baran Baran Palanimuthu070100287
Supervisor :Prof. Dr. Hj. Bidasari
Lubis,SpA(K)

Definition- Also known as congenital pure red cell
- Refers to condition in which Red Blood Cell (RBC)
precursors in bone marrow are nearly absent, while
megakaryocytes and White Blood Cell (WBC) precursors are usually present at normal levels

Epidemiology
Frequency- Since 1936 – United States - hundreds of cases
havebeen reported.
- At the moment it is still not known how’s the prevalence in Indonesia.
Race and SexNo racial and sex predilection is observed.

Mortality/Morbidity- Most individuals survive to early adulthood.
- Some have physical abnormalities.
- Treatment of anemia can contribute to significant morbidity, as follows:
i) Transfusion therapy => hemosiderosis ii) Iron overload => growth retardation, delay in
sexual maturity, cardiac arrhythmias, and cardiac failure.
iii) Transfusions can also transmit infections.iv) Corticosteroid therapy => growth retardation,
osteopenia, diabetes, and other complications.

Etiology- Dominant or recessive patterns of inheritance
are indicated by familial occurrence in about 15% of patients
- 25% of sporadic and inherited cases there are mutations in a gene (DBA1) for a ribosomal protein S19, mapped to chromosome 19q13.
-A second gene for Diamond-Blackfan anemia has been linked to chromosome 8p



Clinical Manifestations- Anemic (i.e: pallor, weakness, and dyspnea)
- One third of patients develop physical abnormalities: involving the head, upper limbs, thumbs, urogenital system, or cardiovascular system.
- Growth retardation and unusual thumb formation (Polydactyly)





PathophysiologyNormal erythropoiesis process in children- Developmental hematopoiesis - three anatomic
stages: mesoblastic, hepatic, and myeloid =>
i)Mesoblastic hematopoiesis: yolk sac - 10th and 14th days of gestation and ceased by 10th - 12th week
ii) Hepatic hematopoiesis: liver - from 6th - 8th week of gestation through 20 – 24th week
iii) Myeloid hematopoiesis: bone marrow - 6th month of gestation
* And as child grow: central bones of the body, i.e: vertebrae, sternum, ribs and pelvis
* marrow in extremities and skull replaced with fat

Hemoglobin- Major hemoglobin of a normal adult (Hb A) -
α2β2 - Major hemoglobin in the fetus (Hb F) - α2γ2- RBCs of an embryo, fetus, child, and adult, six
different hemoglobins may normally be detected:
i) embryonic hemoglobins: Gower-1 (ζ2ε2), Gower-2 (α2ε2), Portland (ζ2γ2)
ii) Fetal hemoglobin, Hb Fiii) Adult hemoglobins, Hb A and Hb A2 (α2δ2)


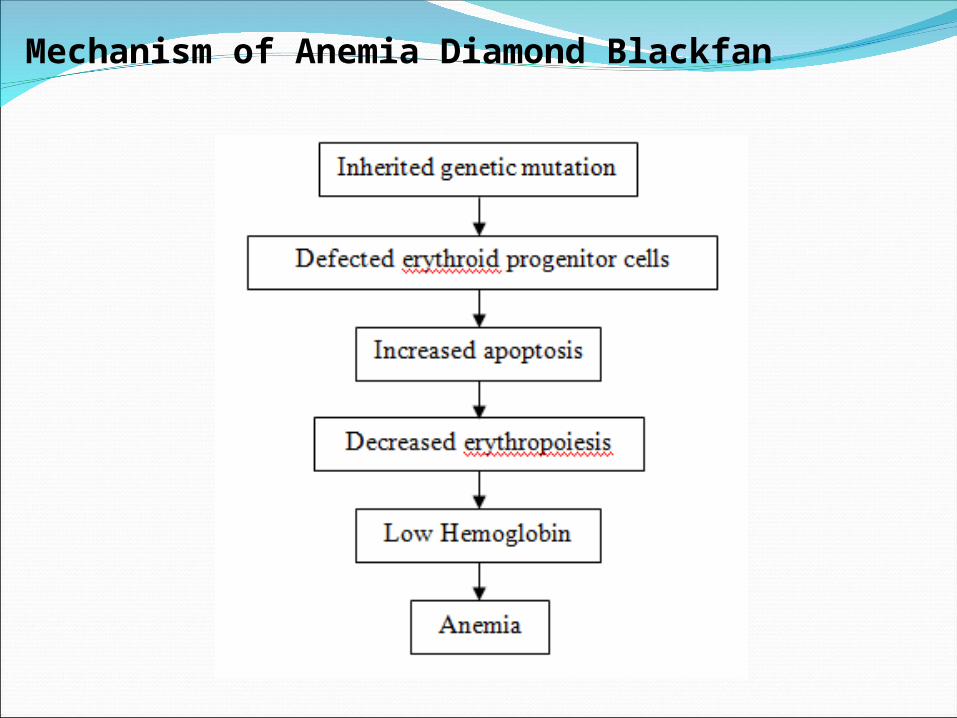
Mechanism of Anemia Diamond Blackfan
Diagnosisi) Laboratory findingsa) Fetal Hb and erythrocyte adenine deaminase
levelsb) Serum folate and vitamin B-12 levelsc) Genetic testingd) Peripheral smear results - Can show
megaloblastic changese) Reticulocytes are characteristically very low
ii) Imaging Studies- Chest radiograph (posteroanterior and lateral)- CT scan to rule out a thymoma- MRI to rule out thymoma

ProceduresBone marrow aspiration and biopsy are indicated
to confirm the diagnosis
Differential Diagnosis. - DD with other anemias with low reticulocyte
counts:i) Hemolytic anemia of the newborn can have a
protracted course and, on occasion, be associated with markedly reduced erythropoiesis. Usually terminates spontaneously at 5-8 weeks of age.
ii) Aplastic anemic crises characterized by reticulocytopenia and by decreased numbers of RBC precursors, frequently caused by parvovirus B19 infections
iii) Transient erythroblastopenia of childhood may be differentiated by its relatively late onset

Treatment i) Corticosteroid therapy - Prednisone in three divided doses totaling 2
mg/kg/24 hr is used as an initial trial- Once the Hb concentration is increasing, dose of
corticosteroid may be reduced gradually (tapering divided doses) ----- > single, lowest effective daily dose
- Dose should then be doubled, used on alternate days, and tapered still further while maintaining the hemoglobin level at 9 g/dL or above

ii) Blood transfusion- At intervals of 4-8 weeks- Chelation therapy for iron overload (serum
ferritin levels exceeding 1,500 mg/dL)

Prognosis and complications- Median survival is probably more than 40 years
old- Half of patients are long-term responders. In the
others, survival depends on transfusions- Regularl blood transfusion ---- > hemosiderosis- Complications of chronic transfusions in
Diamond-Blackfan anemia are similar to those in β-thalassemia major
- Other significant COD: complications associated with stem cell transplantation, steroid therapy (opportunistic infections), and iron overload

PATIENTS STATUS.........

A patient, J, male, 5 years and 5 months old, 17.5 kg, 113 cm, was admitted to the pediatrics non-infectious unit of Haji Adam Malik General Hospital on 31th May 2011 at 19.45.
The main reason he was admitted is because of paleness .Patient was suffering from paleness for the past 1 week. History of bleeding (-), Epistaxis (-), Bloody fecal (-), Hematoma (-). History of high fever (-) and cough (-). Loss of appetite (+) for the past 1 week, Diarrhea (-), Defecation (+) normal and Urination (+) normal.
Patient was previously treated by hematooncology unit with the diagnosis of Diamond Blackfan Anemia.

History of previous illness : Patient was previously treated by hematooncology unit with the diagnosis of Diamond- Blackfan Anemia.
History of previous treatment: Washed PRC transfusion, Folic Acid 1x1mg, Vitamin E 1x100 IU
On Physical Examination, the following findings were confirmed. Body Weight was 17,5 kg, body height was 113 cm, and body temperature 37.60C.
Physical Examinations:Sens: CMAnemic (+)Cyanosis (-)Icteric eyes (-)Dyspnoe (-) Edema (-).

Head:
Eyes -light reflexes +/+, isochoric pupils, Inferior conjunctiva palpebra paleness +/+, Palpebra oedematous -/-.
Ears -Normal.
Nose -Normal
Mouth -Mucus paleness (+)
Neck: Normal jugular vein pressure, Lymph node enlargement (-)
Chest -Symmetrical fusiformic, retraction (-)
HR : 140 bpm, regular
RR : 20 tpm, regular, rales (-)

Abdomen:
-Soepel, normal peristaltic.
-Liver : Palpable 3cm below the right costal arch.
-Spleen: Palpable until the range of SII-III.
Extremities:
-Pulse 140 bpm, regularly, Pressure/Volume was adequate.
-Warm extremities. CRP < 3’
Genitalia: Male, Abnormalities (-)

Working Diagnosis : Diamond-Blackfan Anemia + Mild Malnutrition
Therapy :
Transfusion of washed PRC (1st Bag)
IVFD D5 NaCl 0,45% (20 gtt/ I, micro)
O2 1-2 l/I
Folic Acid 1 x 1 mg
Vit E 1 x 100 IU.

• Follow up 1st June 2011
SUBJECT : Paleness (+) , Fever (-)
OBJECTIVE :
Sens : CM, T : 37,6 ºC , Anemic (+), cyanosis (-), icteric eyes (-), Dyspnoe(-) ,Edema (-).
Head:
Eyes: Light reflexes +/+, isochoric pupils,Inferior conjunctiva palpebra paleness +/+, palpebra oedematous -/-.
Ears: Normal , Nose: Normal, Mouth: Mucus paleness (+)

• Cardiovascular system:
Neck: Jugular Vein Distension R-2cmH2O
HR = 140 bpm,regular; Pulse Pressure/volume adequate• Respiratory System:
Symmetrical fusiform (+), retraction (-),RR= 30 tpm, regular, crackles (-).
• GIT System: Abdomen: soepel, peristaltic (+)normal,
Liver : Palpable 3cm below the right costal arch.
Spleen : Palpable until the range of SII-III.
• Extremities :Pulse 140 bpm, regularly, Pressure/Volume adequate.Warm extremities. CRP < 3’
• Assessment:Diamond-Blackfan Anemia
• PlanningTotal bed rest O2 1-2 l/i
Folic Acid 1x1 mgVit E 1x100 IU
• Futher examinationTransfusion 2nd bag of PRC

• Follow up 2nd June 2011
SUBJECT : Paleness (+) ↓ , Fever (-)
OBJECTIVE :
Sens :CM, T : 37,0 ºC , Anemic (+), cyanosis (-), icteric eyes (-), dyspnoe(-) ,Edema (-).
Head:
Eyes -Light reflexes +/+, isochoric pupils,Inferior conjunctiva palpebra paleness +/+, palpebra oedematous -/-.
Ears: Normal , Nose: Normal, Mouth: Mucus paleness (+)

• Cardiovascular system:
Neck: Jugular Vein Distension R-cmH2O HR = 128 bpm,regular; Pulse Pressure/volume adequate
• Respiratory System: Symmetrical fusiform (+), retraction (-),RR= 28 tpm, regular, crackles (-).
• GIT System: Abdomen: Soepel, Peristaltic (+)normal Liver :Palpable 3cm below the right costal
arch. Spleen : Palpable until the range of SII-III.
• Extremities :Pulse 128 bpm, regularly, Pressure/Volume adequate.Warm extremities. CRP < 3’

Assessment:Diamond-Blackfan Anemia
PlanningTotal bed rest O2 1-2 l/i
Folic Acid 1x1 mgVit E 1x100 IU
Futher examination:
Transfusion 3rd bag of PRC + Complete blood check
Lab results: Hb/Ht/L/T = 6,4/21,1/7630/370,000
PRC transfusion requirement = (10-6,4) x 17,5 x 4
=252 cc (1 ½ bag)

• Follow up 3rd June 2011
SUBJECT : Paleness (+) ↓ , Fever (-)
OBJECTIVE :
Sens :CM, T : 37,0 ºC , Anemic (+), cyanosis (-), icteric eyes (-), dyspnoe(-) ,Edema (-).
Head:
Eyes -Light reflexes +/+, isochoric pupils,Inferior conjunctiva palpebra paleness +↓/+↓, palpebra oedematous -/-.
Ears: Normal , Nose: Normal, Mouth: Normal

• Cardiovascular system:
Neck: Jugular Vein Distension R-2cmH2O HR = 100 bpm,regular; Pulse Pressure/volume adequate
• Respiratory System: Symmetrical fusiform (+), retraction (-),RR= 20 tpm, regular, crackles (-).
• GIT System : Abdomen:Soepel, Peristaltic (+)normal, Liver :Palpable 3cm below the right costal
arch. Spleen : Palpable until the range of SII-III.
• Extremities :Pulse 100 bpm, regularly, Pressure/Volume adequate.Warm extremities. CRP < 3’

Assessment:Diamond-Blackfan Anemia
PlanningTotal bed rest O2 1-2 l/i
Folic Acid 1x1 mgVit E 1x100 IU
Futher examination:Transfusion of washed PRC =1 bag- Post transfusion – check for Hb sahli = 10mg/dl

Thank You