pcos as a metabolic syndrome sang ho yoon division of reproductive endocrinology and infertility...
TRANSCRIPT

PCOS as a Metabolic syn-drome
Sang Ho Yoon
Division of Reproductive Endocrinology and Infertility
Department of Obstetrics and Gynecology
Dongguk University Graduate School of Medicine

Diagnostic criteria for Metabolic syn-drome : International Diabetes Federation (IDF)
Stein & Leventhal in the 1930s• Described the association between PCO mor-
phology, hirsutism, menstrual disturbances and obesity
The most common endocrine disorder in women
3 ~ 10 % of women of reproductive age 25 ~ 30% of infertility patients Major cause of anovulatory infertility
• 75% of PCOS: infertility d/t anovulation
Polycystic ovary syndrome (PCOS)
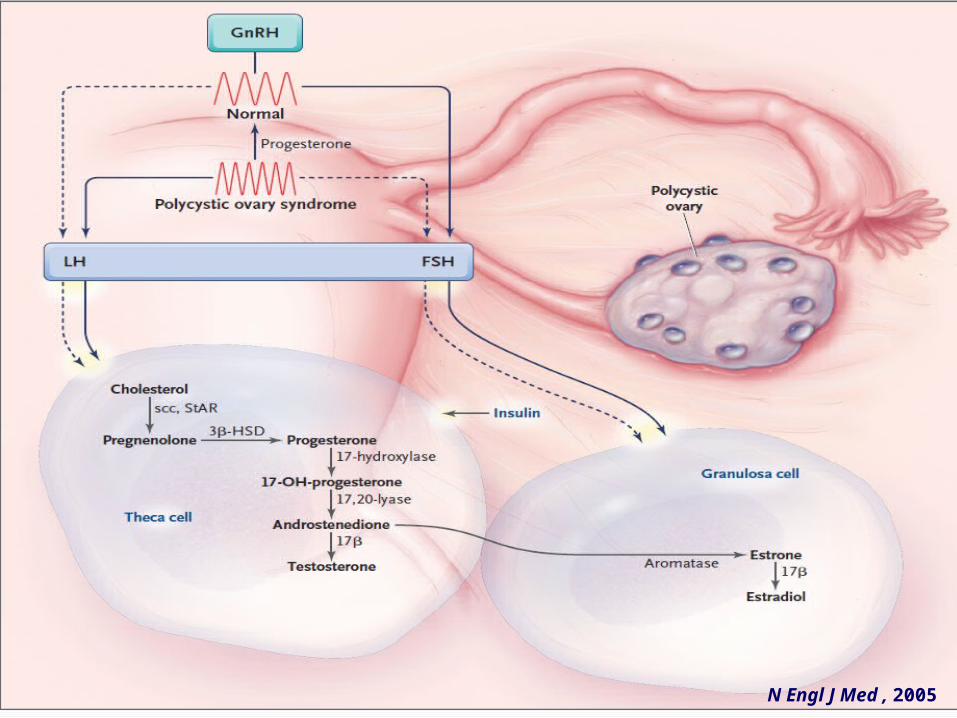
N Engl J Med , 2005

PCOS pathogenesis
Jayasena et al., Nat Rev Endocrinol, 2014

Clinical problem in PCOS
배란장애에 의한 불규칙한 월경 및 불임
남성호르몬 과다증세
당뇨 , 심혈관계 질환 위험도 증가Katsiki et al, Drugs, 2009

Lifelong complications
Norman et al., Lancet, 2007

Diagnostic criteria for PCOS
Jayasena et al., Nat Rev Endocrinol, 2014

Polycystic Ovary Definition
• TV USG• Follicular phase • 12 or more follicles measuring 2–9 mm in diam-
eter• Increased ovarian volume (>10 mL)
Serum anti-Műllerian hormone (AMH)• Secretion : granulosa cells of developing folli-
cles• Potential surrogate for USG• Correlate : AFC • If USG is inappropriate or unavailable

Rotterdam Criteria of PCOS
Polycystic Ovaries
Androgen Excess
Anovulation
2
1
3
Area 2 Hyperandrogenism
(clinical and/or biochemical)Polycystic ovaries
Regular cycles
Area 3Anovulation
Polycystic ovaries No evidence of androgen ex-
cess
Area 1NIH criteria 1990
Frank S, J Clin Endocrionol Metab, 2006

All possible phenotypes
Features
Hyperandrogenemia
Hirsutism
Oligoanovulation
Polycystic ovaries
NIH 1990 criteria
Rotterdam 2003 crite-ria
AES 2006 criteria
+
+
+
+
A
+
+
+
-
B
+
-
+
+
C
+
-
+
-
D
-
+
+
+
E
-
+
+
-
F
+
+
-
+
G
-
+
-
+
H
+
-
-
+
I
-
-
+
+
J
+
+
-
-
K
-
-
-
+
L
-
-
+
-
M
-
+
-
-
N
+
-
-
-
O
-
-
-
-
P
Phenotypes
Azzizz et al, J Clin Endocrionol Metab, 2006

Hyperandrogenism
Nuremberg chronicle – Strange people – Hairy lady, 1493

Definition Clinical signs: hirsutism, acne, alopecia
(male-pattern balding) and frank viriliza-tion
Biochemical indicators• ↑total testosterone & androstenedione, • ↑free androgen index• However, these markers has proved markedly in-
consistent d/t problems with various assays
→ Reliable detection of this feature is not straightforward
The ESHRE/ASRM Rotterdam Consensus Meeting, 2003
Norman et al., Lancet, 2007

Clinical sign: Hirsutism
Being present in 65-75% of patients with PCOS defined by the NIH criteria
Rarely present in Asian women
Degrees vary greatly in different ethnic population
Modified FG score might underestimate clinical sign • Threshold of abnormality should be measured on
a population basis
Androgen Excess Society Guideline., JCEM, 2006Legro et al., JCEM, 2013
Carmina et al., AJOG, 1992DeUgarte et al., JCEM, 2006

Assessment of Hirsutism
95th percentile as upper normal limit in the white or black: 6-8
modified Ferri-man-Gallwey score
Ferriman D, Gallwey JD, JCEM. 1961

Escobar-Morreale., Hum Reprod Update, 2012
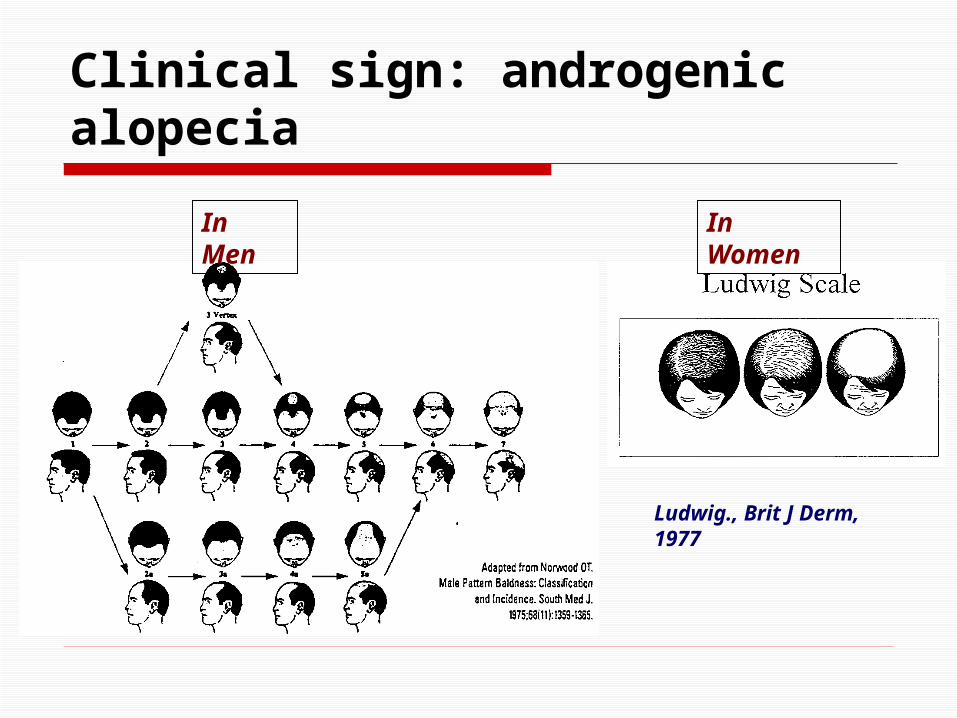
Clinical sign: androgenic alopecia
Ludwig., Brit J Derm, 1977
In Men In Women

Other clinical signs
Acne • Affects 14-25% of PCOS pts. • Unclear whether the prevalence of acne is signif-
icantly increased than general population Androgenic alopecia
• The prevalence in PCOS is unclear• Less frequent and presents later
Acne or androgenic alopecia could not be used reliably as clinical sign of hyperan-drogenism.
Androgen Excess Society Guideline., JCEM, 2006Norman et al., Lancet, 2007Legro et al., JCEM, 2013

Biochemical hyperandro-genism
Elevated circulating androgen levels• In 60-80% of PCOS pts.• The vast majority of abnormal value: free testos-
terone Low SHBG
• Excellent diagnostic accuracy for PCOS• Surrogate marker of insulin resistance and andro-
gen excess
However, between 20-40% of PCOS will have androgen levels within the normal range• Assays for androgens tend to be highly variable
and inaccurate• Some patients have normal levels of free T
Androgen Excess Society Guideline., JCEM, 2006Jayasena., Nat Rev Endorinol, 2014
Conway et al., Eur J Endocrinol, 2014

Biochemical assessment
Single most reliable indices of hyperandro-genism• Hirsutism & free T levels
Total testosterone is the first-line recom-mendation for assessing androgen excess in women• RIA to measure free T directly → been criticized for lack of accuracy, so should not
be used
FAI (Free androgen index) • By measurement serum total T and SHBG (T/
SHBG x 100)• Practical alternative to the measurement of free
T• Androstenedione, DHEAS → need in severe hirsu-
tim
Jayasena., Nat Rev Endorinol, 2014Conway et al., Eur J Endocrinol, 2014
Conway et al., Eur J Endocrinol, 2014
Norman et al., Lancet, 2007

Excessive ovarian androgen pro-duction
PCOS is the underlying factor in as many as 92% of women with hirsutism & 84% with persistent acne
PCOS should primarily be regarded as a disorder of excessive androgen biosynthe-sis, use or metabolism
Adams et al., BMJ, 1986Homburg., Hum Reprod, 1996
Androgen Excess Society Guideline., JCEM, 2006

Hyperandrogenism PCO
• Associated with hypersecretion of LH• Thickened theca cell layer• Theca cells secrete excessive androgens in basal
state or in response to LH stimulation
Both insulin and LH, alone and in combina-tion, exacerbate ovarian androgen produc-tion
Homburg., Best Pract Res Clin Obstet Gynecol, 2008Jayasena., Nat Rev Endorinol, 2014
Insulin resistance

Pathophysiology-hyperinsu-linemia
Speroff 8th ed., 2011
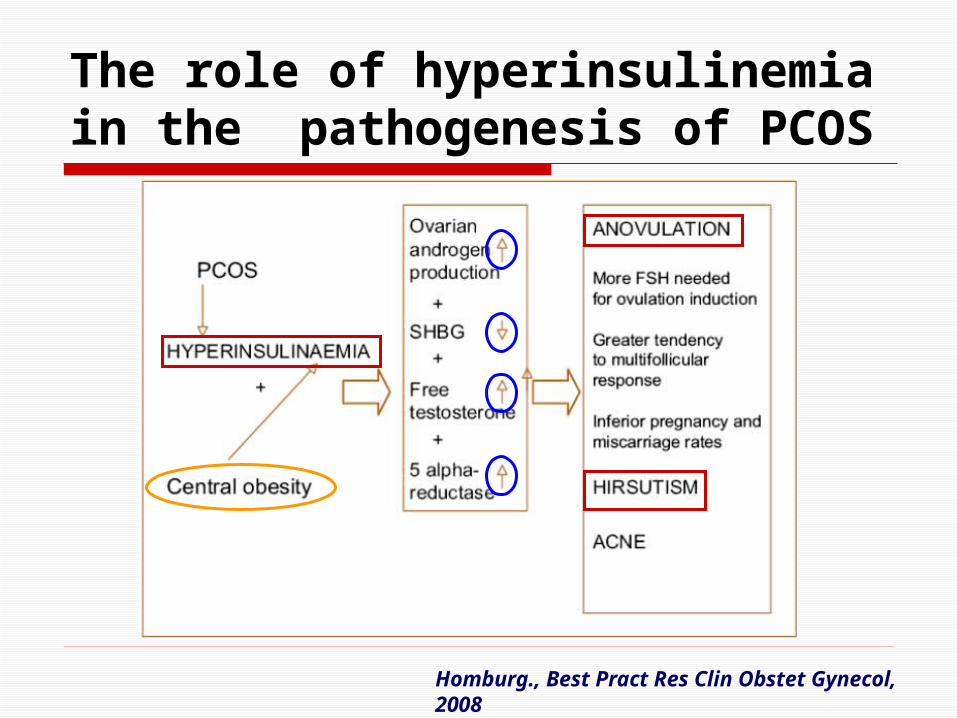
The role of hyperinsulinemia in the pathogenesis of PCOS
Homburg., Best Pract Res Clin Obstet Gynecol, 2008

Reported IR in PCOS
Legro et al., Obstet Gynecol Survey, 2004
Assessment of IR Still several problems…
• Apparent lack of consensus on “normal” insulin sensitivity
• Ethnic and genetic variability• Other factors contributing to IR such as obe-
sity, stress, and aging• Concern about whether simplified models of IR
have the precision to predict treatment needs, response, and future morbidity.
Assessment of insulin as a fasting hor-mone or as a surrogate of IR (HOMA…) is of little value although widely used for re-search studies. Norman et al., Lancet, 2007
Legro et al., Obstet Gynecol Survey, 2004
Consensus
No test of insulin resistance is needed ei-ther to make the diagnosis of or to select treatment for PCOS
Recommend the use of 75g OGTT to screen for IGT and T2DM in adolescent and adult women with PCOS
The ESHRE/ASRM Rotterdam Consensus Meeting, 2003
Legro et al., JCEM, 2013

Hyperinsulinemia Overall prevalence of IGT among US women
with PCOS was 30-35%, and 3-10% had T2DM• Non-obese PCOS: 10-15% prevalence of IGT and
1-2% prevalence of T2DM
A diagnosis of PCOS confers a 5-10-fold in-creased risk of developing T2DM
Key factor in the pathogenesis of anovula-tion and hyperandrogenism
Legro et al., JCEM, 2013

Cardiovascular events

Cardiovascular events in PCOS
Initial studies did not find an increased prevalence of nonfatal/fatal CVD in women with PCOS (Pierpoint et al., 1998; Wild et al., 2000)
Lifetime risk for CVD in PCOS women is high and mostly preventable, all PCOS women should be screened for CVD risk factors
Wild et al., JCEM, 2010

Incidence
Glucose intolerance: 30% of adolescents with PCOS
Dyslipidemia: 70 % of reproductive aged PCOS women
Non obese PCOS women: also may have
• Glucose intolerance
• Dyslipidemia
Syndrome X

Metabolic abnormalities: 외국 data
저자 국가 PCOS 대조군
제 2 형 당뇨
Ehrmann et al., 1999
USA 10% (13.5-40 years)
2.5% (NHANES II, 20-44 years)
이상지혈증 Legro et al., 2001 USA 70%
고혈압 Lo et al., 2006 USA 12% 4.9%
대사증후군 Apridonidze et al., 2005
USA 43%*
* Nearly 2-fold higher than age-matched general population

Metabolic abnormalities: 국내 data
Chae et al., 2008 (SNUH) Other Korean reports
제 2 형 당뇨 2.0% 1.0% (Lee et al., 2009)
이상지혈증 28.6% (14.1% in controls)
고혈압 (≥140/90mmHg)
13.6% (2.6% in controls)
대사증후군 23.3% (1.4% in controls)
14.5% (Park et al., 2007)
비만 (BMI≥25kg/m2) 25.2% 28.4% (Lee et al., 2009)
Chae et al, Hum Reprod, 2008
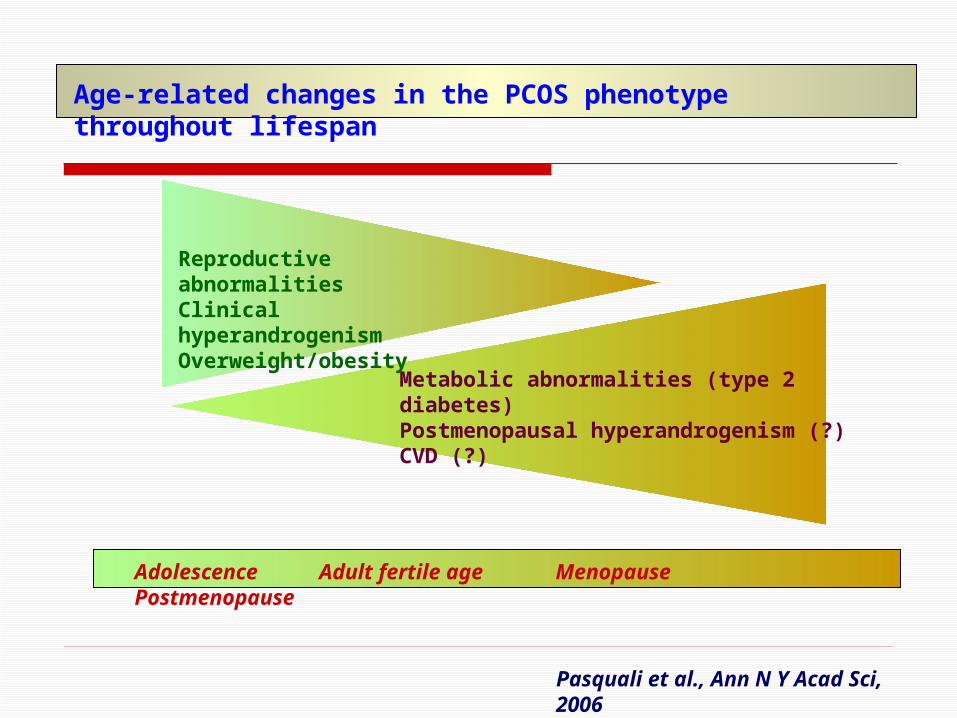
Age-related changes in the PCOS phenotype through-out lifespan
Reproductive abnormali-tiesClinical hyperandro-genismOverweight/obesity
Metabolic abnormalities (type 2 dia-betes)Postmenopausal hyperandrogenism (?)CVD (?)
Adolescence Adult fertile age Menopause Postmenopause
Pasquali et al., Ann N Y Acad Sci, 2006

Therapeutic goals in pt. with PCOS Restore menses and reduce the signs of
hyperandrogenism.
Prevention of endometrial cancer
Achieve successful pregnancy.
Avoidance of the long-term complication that are associated with obesity, insulin re-sistance, glucose intolerance, and type 2 DM.
The Amsterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group, Hum Reprod 2012

Korean data

Prevalence of the PCOS sub-groups
Ethnics IM+HA+PCO IM+HA IM+PCO HA+PCO
Welt et al (2006-12)USA,
Iceland298 (71.3%) 7 (1.7%) 36 (8.6%) 77 (18.4%)
Dewailly et al (2006-10) France 246 (60.6%) 27 (6.7%) 66 (16.3%) 67 (16.5%)
Hsu et al (2007) Taiwan 88 (51.7%) 15 (8.8%) 31 (18.2%) 36 (21.1%)
Pehlivanov et al (2007) Bulgaria 41 (58.6%) 8 (11.4%) 7 (10.0%) 14 (20.0%)
Diamanti-Kandarakis (2007)
Greece 284 (46.4%) 251 (39.6%) 43 (6.8%) 46 (7.2%)
SNUH (2008) Korea 87 (52.4%) 23 (13.9%) 52 (31.3%) 4 (2.4%)
IM: Irregular menstruation (oligo-anovula-tion)
HA: Hyperandrogenism, PCO: Polycystic Ovary

No significant differ-ence in the prevalence of metabolic syndrome between women with O+P and control sub-jects, even in obese women
Shroff et al., Fertil Steril, 2007
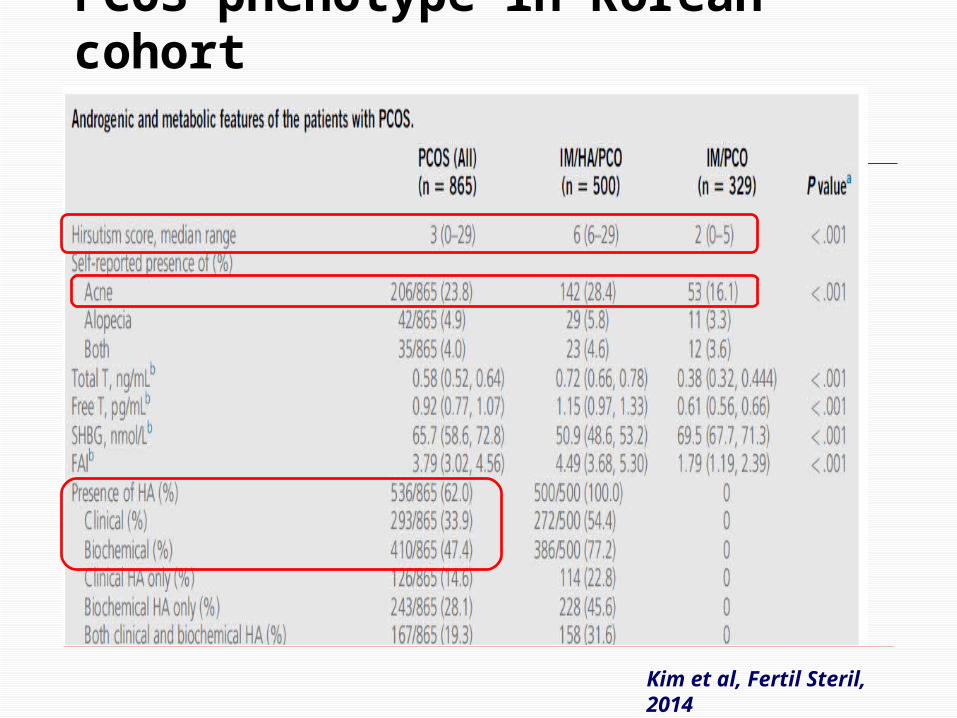
PCOS phenotype in Korean cohort
Kim et al, Fertil Steril, 2014

PCOS phenotype in Korean cohort
Kim et al, Fertil Steril, 2014

PCOS phenotype in Korean cohort
Kim et al, Fertil Steril, 2014

Summary PCOS is the most common cause of hyper-
androgenic chronic anovulation and infertil-ity
Overproduction of androgens is at the heart of PCOS, often exacerbated by asso-ciated hyperinsulinemia
Obesity is common feature of PCOS but not a prerequisite for its development
Increased risk of developing type 2 dia-betes and cardiovascular disease
Summary PCOS without HA are common in Korea
and are less likely to have metabolic dys-function, insulin resistance and elevated BP
PCOS without HA may be a mild pheno-type of PCOS
PCOS in Korea could have a reduced like-lihood of having metabolic syndrome compared with other ethnicities

Needs Research…
Norman et al., Lancet, 2007Shroff et al., Fertil Steril, 2007Homburg., Best Pract Res Clin Obstet Gynecol, 2008
Risk of metabolic syndrome may vary among the phenotypes→ Individualization of treatment according to pheno-type
