patient as a radioactive source final disa and...
TRANSCRIPT

Patient as a Patient as a Patient as a Patient as a radioactiveradioactiveradioactiveradioactive source source source source ---- diagnosticsdiagnosticsdiagnosticsdiagnostics---- therapytherapytherapytherapy
DISA ÅSTRAND
ELEONOR VESTERGREN

Nuclear medicineFrom a radiation protection point of view, nuclear medicine is very different from the useof X-rays. The patient becomes a radiationsource after the administration of radioactivity.
The radiation continues after the examination or the therapy. Persons in contact with the patient might recieve a radiation dose. Therefore, there is a radiation protection issue, not only for hospital staff, but also for family, relatives, and the general public.

Euratom BSSDose limits for public exposure
2. Member States shall set the limit on the effective dose for public exposure at 1 mSv in a year.
Optimisation
5. Member States shall ensure that: (a) dose constraints are established for the exposure of carers and comforters, where appropriate.
6. Member States shall ensure that in the case of a patient undergoing treatment or diagnosis with radionuclides, the practitioner or the undertaking, as specified by Member States, provides the patient or their representative with information on the risks of ionizing radiation and appropriate instructions with a view to restricting doses to persons in contact with the patient as far as reasonably achievable. For therapeutic procedures these shall be written instructions.

ICRP 94 Release of Patients after Therapy with Unsealed Radionuclides (2004)“A dose constraint of a few mSv/episode (not a doselimit) applies to relatives, visitors and caregivers at home.”
“This document recommends that young children and infants, as well as visitors who are not engaged in direct care or comforting, should be treated as members of the public (i.e., subject to the public dose limit)”

Radionuclide therapy
Dose restrictions, Sweden and Finland
…it should be unlikely that the effective dose
• for any person in the general public exceeds 0.3 mSv
• for children relatives exceeds 1 mSv and
• for adults relatives exceeds 3 mSv or,
• for relatives aged 60 years or more, exceeds 15 mSv.

Swedish national working group on recommendations in diagnostic nuclear medicine
Swedish Society of Nuclear Medicine 2011-2013
Recommendations to limit the radiation doses to relatives and to the general public (not staff)
Dose limit to the public, 1 mSv is the sum of all the exposures during a year
The working group’s recommendations are based on 0,3 mSv
Recommendations limited to adult patients Working group:Heléne Brundin, technologistHenrik Båvenäs, medical physicistLena Engelin, technologistLena Monryd, technologistAgnetha Norén, technologistEva Persson, medical doctorEleonor Vestergren, medical physicistDisa Åstrand, medical physicistReviewers:Sigrid Leide Svegborn, medical physicistPer Grybäck, medical doctor

Sweden 2015-2016Statistics NM diagnostics
0
5000
10000
15000
20000
25000
30000
2015
2016

Radionuclides diagnostics
Nuclide Half-life Photon energy
(keV)
Exposure rate
constant Γ (µSv·m2/MBq·h)
Tc-99m 6,02 h 140 0,0204
I-123 13 h 159 0,0435
In-111 2,83 d 175, 247 0,0868
F-18 110 m 511 0,143
Ga-68 68 m 511 0,134

Radiation dose from a patient Measurements or estimations
• Cumulated dose can be measured with TLD or EPD
• Cumulated dose can be estimated from dose rate and occupancy factors
1. Dose rate◦ can be measured at different distances and time intervals,
the decrease with time can be estimated from biokinetic data of the radiopharmaceutical if measurements are few
2. Occupancy factors◦ time
◦ distance

Occupancy factorsAssumptions on the time spent at different distances from the patient (4 half lifes)
Family◦ Small children (< 3 years)◦ Children ◦ Partner
General public ◦ Waiting room◦ Transport◦ At work
References: Mountford PJ, O`Doherty MJ. Exposure of critical groups to nuclear medicine patients. Applied Radiation and isotopes. 1999; 50:89-111.Cronin B, Marsden PK, O`Doherty MJ. Are restrictions to behaviour of patients required following fluorine-18 fluorodeoxyglucosepositron emission tomographic studies? European Journal of Nuclear Medicine. 1999; 26: 121-128.

Work outlineCollected dose rate data from many hospitals in Sweden
◦ Common types of examinations
◦ Distance, 0 – 100 cm
◦ Different time intervals post administration
The measured data were used together with biokinetic data to get an averagetime – dose rate curve
Integral dose was calculated for persons in contact with the patient using the occupancy factors
Recommendations were formulated for different examinations
A written report published on the webpage of the SFNM

Dose rate variation with patient size
0
5
10
15
20
25
Dose r
ate
(uS
v/h
)
20 40 60 80 100 120 140
Weight (kg)
Distance 1m1000 MBq Tc99m-HMPAO

Measured dose rates per activity unit(shortly after adminostration)
Radiopharma-ceutical
Anterior: different distances(µSv/h/MBq)
1 cm 10 cm 50 cm 100 cm18F-FDG 2,50 1,28 0,40 0,1599mTc – all compounds*
0,38 0,20 0,04 0,02
111In-octreotide 1,18 0,69 0,19 0,06123I-DatScan 0,50 0,24 0,06 0,02123I-mIBG 0,44 0,26 0,12 0,04123I-NaI 0,44 0,23 0,06 0,03
*The value for Tc-99m-phosfonates is used for all Tc-99m compounds, valid for radiation protection purposes.
Reference: Gomez-Palacios M, Terrón JA, Domínguez P, Vera DR, Osuna RF. Radiation doses in the surroundings of patients undergoing nuclear medicine diagnostic studies. Health Physics. 2005; 89(2 Suppl): 27-34.

Dose rate from patients(shortly after admdinistration)
RadiopharmaceuticalAdminstered
activity(MBq)
10 cmDose rate (µSv/h)
100 cmDose rate (µSv/h)
F-18 FDG 350 448 53
I-123 mIBG 200 52 8
In-111 Octreotide 170 117 10
Tc-99m all < 200 Mbq < 200 < 40 < 4
Tc-99m- sestamibi/tetrofosmin
600 120 12
Tc-99m- phosponates 600 120 12

Dose rate and distance18FDG 350 MBq
1 m
52 µSv/h
0,5
m
0,1
m
140 µSv/h
450 µSv/h
1
m
12 µSv/h
0,5
m
0,1
m
120 µSv/h
24 µSv/h
99Tcm HDP 600 MBq

I-123 mIBG 200 MBq enligt SSM-statistikWorst case 0h-53h 1 cm 943 µSv
Småbarn, 0h-4T½Med nattmatning 363µSv SMÅBARNtidpunkt (småbarn dos < 0.3 mSv) 3h
Inget nära umgänge (< 1m) under 3 timmar efter injektionoch första natten i egen säng
Dagtid + natt (4h själv + 8h vuxen) 523µSvtidpunkt (småbarn dos < 0.3 mSv) >8h
Större barn, 0h-4T½Dagtid + natt (4h själv + 8h vuxen) 342µSv STÖRRE BARN
tidpunkt (barn < 0.3 mSv) 5hUndvik nära umgänge (< 1m) under 5 timmar efter injektion
Dagtid (natt i egen säng 12 h) 150µSvtidpunkt (barn < 0.3 mSv) h
Vuxen partner (inkl. gravida), 0h-4T½
Dagtid+natt (10 cm) 212µSvVUXEN PARTNER
tidpunkt (vuxna < 0.3 mSv) Inga begränsningar
Väntrum0h-4h + 20h-24h, 10 cm 217µSv VÄNTRUM
Inga begränsningar
Resa, kommunalt
0h-4h 10 cm 188µSvRESA, KOMMUNALTInga begränsningar
Resa, privat bil0h-4h 50 cm 87µSv RESA, PRIVAT BIL
Inga begränsningar

Recommendations
Radionuclide RadiofarmaceuticalActivity(MBq)
Recommendationshours (h)
Small childrenAvoid close
contact(< 1m)
Children Avoidclose contact
(< 1m)
PartnerAvoid close
contact(< 1m)
18F FDG 350 4 h 2 h -
123IIoflupan(DatScan)
185 6* h 0* h -
123I NaI 185 4 h - -
123I mIBG 200 3* h 5 h -
111In Octreotid 170 113* h 88* h 59* h
99mTcAll compounds< 200 MBq # < 200 - - -
99mTcSestamibi/ tetrofosmin
600 6* h 0* h -
99mTcDifosfonater (MDP, HDP,DPD)
600 4 h - -
*Valid if the patient doesn´t sleep in the same bed as the child/partner during the first night after the administration. The corresponding value for In-111 (octreotid) is 5 nights for small children, 4 nights for children and 2 nights for partner.

Hospital staffNot included in the scope of the work group
Occupancy factors are difficult to to estimate. Depends on:
• Number and type of examinations
• How the work tasks are distributed among staff at the department
• Time spent with individual patients
However, the dose rate data can be used to estimate doses to the stafftogether with information on the parameters above.

Children I-123-mIBG”Worst case” in paediatric NM diagnostics due to:
◦ the photon energy and exposure rate constant
◦ half-life
◦ a relatively high administered activity (10 MBq/kg)
◦ often quiet ill, need much care and close contact withparents/caretakers

Dose rate children 123I mIBGMeasured shortly after injection of 10 MBq/kg body weight
0
20
40
60
80
100
120
140
0 20 40 60 80 100 120
Do
se r
ate
uSv
/h
Distance (cm)
4,8 kg
8 kg
14 kg

0
200
400
600
800
1000
1200
1400
1600
1800
Radionuclide therapies Sweden 2015/2016
Sweden 2015 Sweden 2016
Swedish radiation safety authority

Isotope Radiation Half life
P-32 Beta max: 1710 keV 14 d
Sr-89 Beta max: 1500 keV 50 d
Y-90 Beta max: 2280 keV 64 h
I-131 Beta max: 606 keVGamma: 364 keV (81 %)
8 d
Lu-177 Beta max: 490 keVGamma: 113 keV (3 %)210 keV (11 %)
7 d
Sm-153 Beta max: 808 keVGamma: 103 keV (28 %)
2 d
Ra-223 Alfa (95.3%),Beta (3.6%) and Gamma (1.1%)
11 d
Radionuclides

Isotope Aim Compound Typicaladministeredactivity MBq
Dose rate,patient @ 1m (µSv/h)
P-32 Polycytemia Vera NaP 150-260 -
Sr-89 Pain relief Bone metastases Metastron 148 -
Y-90 Joints Silikat 200 -
Y-90 Intratumorial, liver - 1000 -
I-131 Tyreotoxicosis NaI 200-800 40
I-131 Thyroidcancer NaI 1100-7400 400
I-131 Neuroendocrin tumour mIBG 3700-7400 300
Lu-177 Neuroendocrin tumour Octreotid 7400 50
Sm-153 Pain relief Bone metastases Quadramet 1850-3700 15
Ra-223 Pain relief Bone metastases Xofigo 3-6 0,5
Therapies

I-131, Tyreotoxicosis
I-131 used to suppress an overactive thyroidgland.
200-800 MBq
24 hour uptake and effective half life aremeasured for dose planing
1 m40 µSv/h
800 MBq, post administration

IAEA, No. 63 Release of Patients After Radionuclide Therapy

I-131, contaminationRadioactive iodine is primarily excreted in the urine, with smaller amounts in saliva, sweat and faeces, a small amount is exhaled.
Usually, for adult relatives, the internal dose due to contamination is less than 10% of the external dose.
IAEA, No. 63 Release of Patients After Radionuclide Therapy

Karin, 30 year 800 MBq,
T24 = 40 %, EHT = 6 d
� 1. Avoid close contact with adults 7 days
� 2. Avoid children and pregnant women 23 days
� 3. Stay home from work -
� 4. Cinema and theater visits 2 days
� 5. Avoid long trips 2 days
� 6. Take extra care with hygiene 3 days

I-131, Thyroidcancer
I-131 used to ablate post surgery of thyroid. Administration with preprepared capsules.
1100-7400 MBq1 m
370 µSv/h
7400 MBq, post administration0
1000
2000
3000
4000
5000
6000
7000
8000
0 10 20 30 40 50 60 70 80 90 100
Rad
ioac
tivi
ty (
Bq
)
Time (h)

WC
3,7 GBq
14 µSv/h
10 µSv/h
6 µSv/h
0,6 µSv/h
Background:
0,1-0,2 µSv/h
corridor
Exampel3,7 GBq

I-131, NET (mIBG) children
I-131 labelled with mIBG.
> 3700 MBq1 m
150 µSv/h
3700 MBq, post administration0
1000
2000
3000
4000
5000
6000
0 10 20 30 40 50 60 70 80 90 100
110
120
Rad
ioac
tivi
ty (
Bq
)
Time (h)

I-131, NET (mIBG) staff and relatives exposureStaff who administers the treatment: highamounts to infuse during 30 min.About 0,1 mSv/treatment
Staff who take care of hospitalized patients: Children with lots of caretaking needs. 0,1-0,5 mSv/treatment.
Family members staying in the hospital withthe child recieve a dose of 1-6 mSv/treatment.

WC
8 GBq
400 µSv/h
280 µSv/h
160 µSv/h
16 µSv/h
Background:
0,1-0,2 µSv/h
Corridor
Exempel
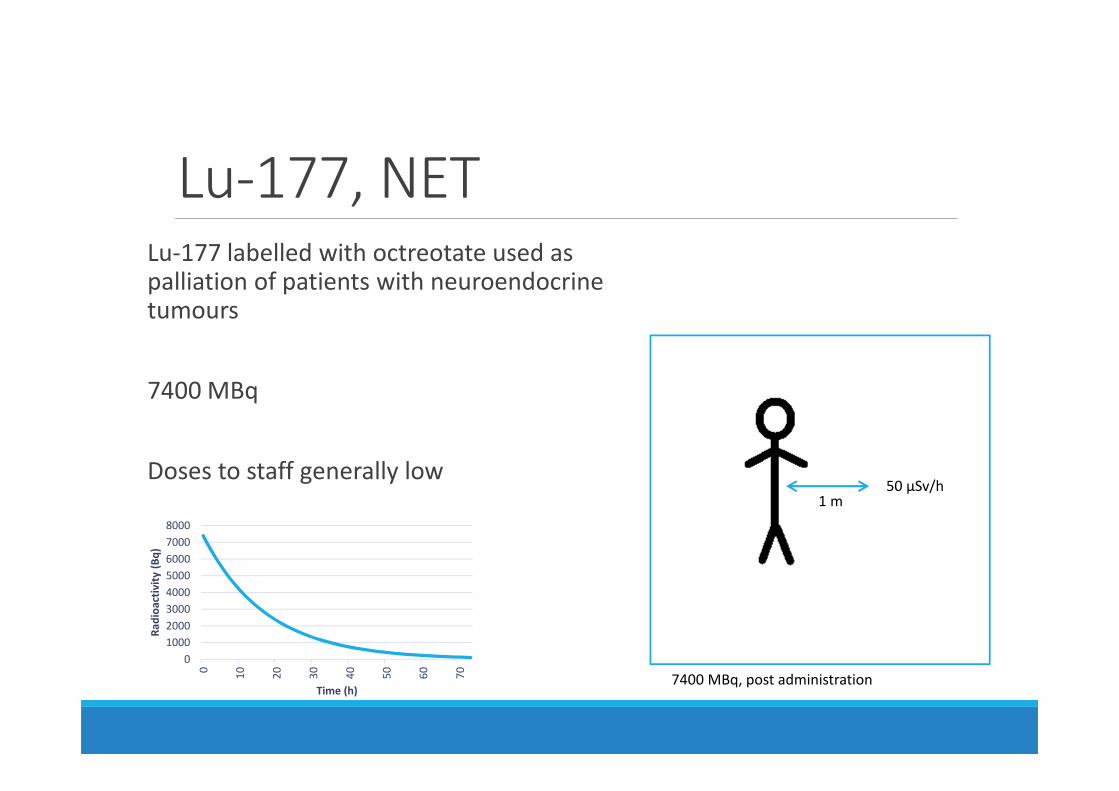
Lu-177, NETLu-177 labelled with octreotate used as palliation of patients with neuroendocrinetumours
7400 MBq
Doses to staff generally low
0
1000
2000
3000
4000
5000
6000
7000
8000
0 10 20 30 40 50 60 70
Rad
ioac
tivi
ty (
Bq
)
Time (h)
1 m50 µSv/h
7400 MBq, post administration

Summary• Diagnostic NM generally gives low doses. But special concern is sometimes needed for children during the first hours afteradministration.
• I-131 therapy is the main radiation safety issue.
• Hospitalization is sometimes needed for therapy patients -> mightincrease the radiation dose to staff.
• Instructions and restrictions are needed in order to minimize doses to family and the public when therapy patients leave the hospital.