palliative care continuum carri siedlik - aprn, achpn nurse practitioner advanced certified hospice...
TRANSCRIPT

Palliative Care Continuum
Carri Siedlik - APRN, ACHPNNurse Practitioner
Advanced Certified Hospice and Palliative NursePalliative Care Program
The Nebraska Medical Center

• Unprecedented number of older Americans with chronic illness
• Technology is prolonging life but not restoring it
• Exploding healthcare costs
• Many uninsured
• Lack of control over rising drug/device costs
• Failure to treat pain and other symptoms
Death and Dying in AmericaDeath and Dying in America
Meier, 2010

View of Advanced Illness and the Care that is Involved
• Frequent emergency room visits
• Increase of in-patient admissions
• Futile care• Promote suffering• Increase risk of depression
and anxiety• Promote complicated
bereavement for family members/caregivers
• Treatments continued near death may prevent/delay hospice services
Greer et al., 2012

• For Healthcare Team: Providing symptom management and discussing emotional aspects of the disease.
• For Patients: Achieving a sense of control, attaining spiritual peace, succeeding in having finances in order, strengthening relationships
with loved ones, believing their life had meaning.
What Constitutes Good Quality Care At the End of Life?
Grant & Dy, 2012; Jacobsen et al., 2011

Administration on Aging, 2010; Kochanek et al., 2011; Minino, et al, 2009
Early 1900s Current
Medicine's Focus Comfort Cure
Cause of Death Infectious DiseasesCommunicable Diseases
Chronic Illnesses
Death rate 1720 per 100,000(1900)
800.8 per 100, 000(2004)
Average LifeExpectancy
50 77.8
Site of Death Home Institutions
Caregiver Family Strangers/Health Care Providers
Disease/DyingTrajectory
Relatively Short Prolonged
Cause of Death Demographic and Social Trends
DeathTime
Hea
lth S
tatu
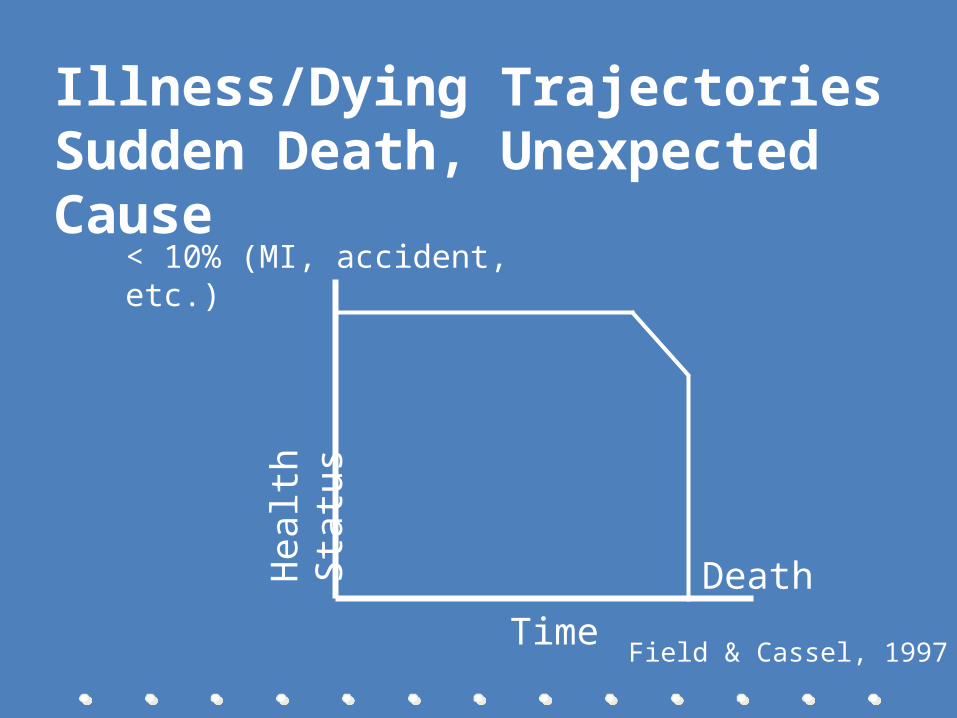
s< 10% (MI, accident, etc.)
Field & Cassel, 1997
Illness/Dying Trajectories Sudden Death, Unexpected Cause

DeathTime
Hea
lth S
tatu
s
Field & Cassel, 1997
Illness/Dying TrajectoriesSteady Decline, Short Terminal Phase
Illness/Dying TrajectoriesSteady Decline, Short Terminal Phase
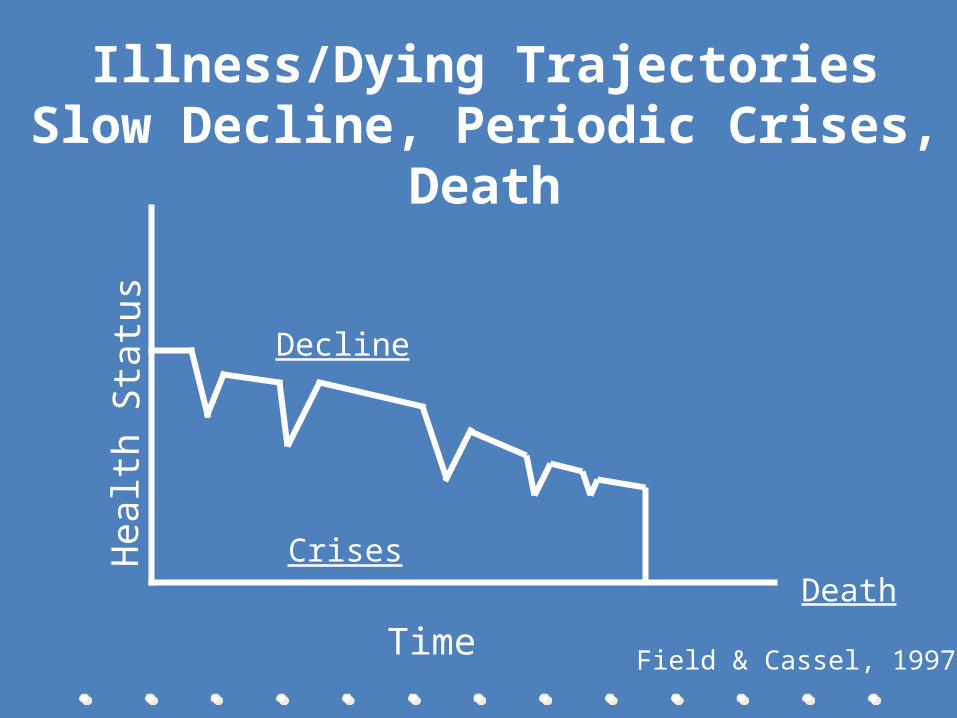
Illness/Dying TrajectoriesSlow Decline, Periodic Crises, Death
Illness/Dying TrajectoriesSlow Decline, Periodic Crises, Death
Hea
lth S
tatu
s
Time
CrisesDeath
Decline
Field & Cassel, 1997

• Patients fear they will be a physical and financial burden
• If “nothing more can be done,” will healthcare providers abandon them?
• How do families and caregivers adjust to role changes?
• Many drain life savings and/or go bankrupt to cover medical costs
• Older adults may be cared for by an aged spouse who is also ill
• Older children caring for a parent may also have acute or chronic illness(es)
Toll of Death and Dying on Patients & Families/Caregivers
Egan-City & Labayak, 2010; Given et al., 2012

• Over 44 million adults provide unpaid care to sick/disabled adults
• Average of 21 hours a week
• ~ 33% are elderly• Most are women in
their mid 40’s, working full-time
• 40% of women and 26% of men caregivers report emotional strain
• Cost of uncompensated care = $257 B/year
Overview of Caregivers: Their Commitment and The Cost
Meier, 2010

• US Veterans: 23,442,000• 900 WW II Veterans die a day• Veteran deaths account for almost
28% of all US deaths• Nearly 40% of enrolled Veterans
live in rural communities• 121,000 Veterans are without
shelter or healthcare, hence no access to hospice or palliative care
Casarett 2008, NHPCO, 2011
Remember Patients Who Are Veterans: 96% of all Veterans Die in Non-VA
Facilities

• National Consensus Project (NCP) for Quality Palliative Care: Promotes evidence-based practices to optimize palliative care programs
• National Quality Forum: Developed quantifiable quality indicators
• The Joint Commission: Advanced Certification in Palliative Care
Changes Must Be Made: Development of Standards to Guide Practice
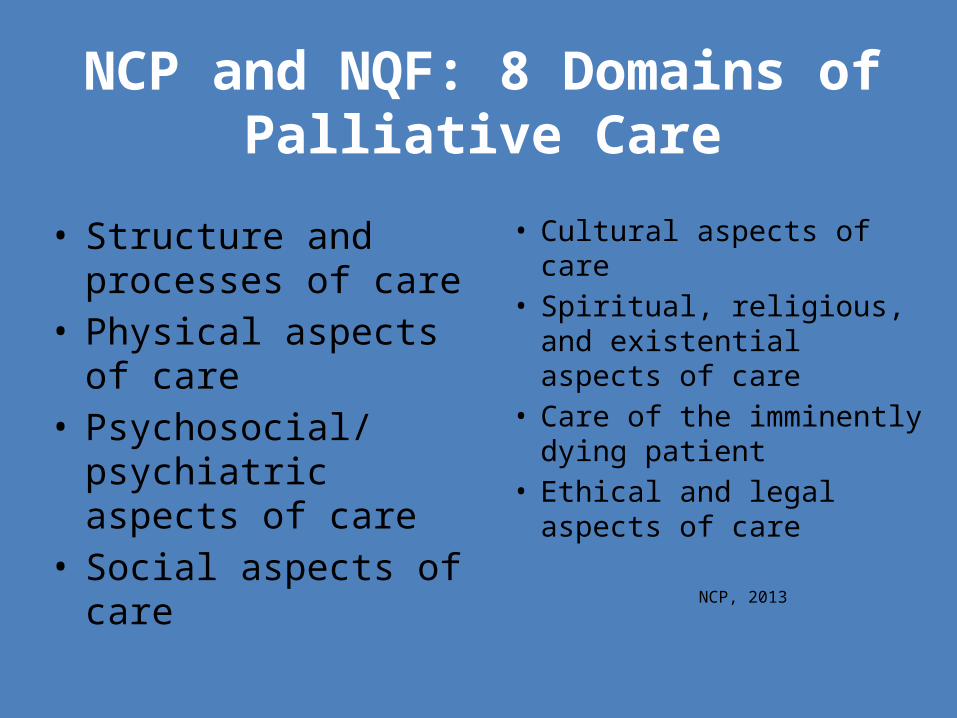
• Structure and processes of care
• Physical aspects of care• Psychosocial/psychiatric
aspects of care• Social aspects of care
• Cultural aspects of care• Spiritual, religious, and
existential aspects of care• Care of the imminently
dying patient• Ethical and legal aspects
of care
NCP, 2013
NCP and NQF: 8 Domains of Palliative Care

• Palliative care compliments national aim to improve quality of care at the local/state/national level– Better Care: Must be patient-
centered, reliable, accessible, safe– Affordable Care: Reduce cost for
individuals, families, employers, government
http://www.healthcare.gov/news/reports/quality03212011a.html
Report to Congress: National Strategy For Quality Improvement in
Healthcare

Barriers to Quality Care at the End of Life
• Failure to acknowledge the limits of medicine• Lack of training for healthcare providers• Hospice/palliative care services are poorly
understood• Rules and regulations• Denial of death
Meir, 2010; NHPCO, 2011

What is Hospice?
• Definition• History• Services included• Statistics
What is Palliative Care?
• Definition• History

Curative Treatment
Palliative Care Hospice
Current Practice of Hospice and Palliative Care

Disease-Modifying Treatment
Hospice Care
Bereavement Support
Palliative Care
Terminal Phase of Illness
Death
Continuum of Care

Hospice Medicare Benefit Eligibility Criteria:
• The patient’s doctor and the hospice medical director use their best clinical judgment to certify that the patient is terminally ill with life expectancy of six months or less, if the disease runs its normal course
• The patient chooses to receive hospice care rather than curative treatments for his/her illness
• The patient enrolls in a Medicare-approved hospice program
http://www.nhpco.org

• Hospice:– Medicare– Medicaid– Most private
health insurers
• Palliative Care:– Philanthropy– Fee-for-service– Direct hospital
support
Payment for Hospice and Palliative Care
Which of the following patients could benefit from palliative care? • A. 64 year-old with congestive heart failure,
hypertension and diabetes• B. 32 year-old with acute myelogenous
leukemia • C. 57-year-old with newly diagnosed
amyotrophic lateral sclerosis• D. 76 year-old with Parkinson’s disease
Stop and Consider

Let’s Practice: A Case Study
• 70 y/o woman with newly diagnosed pancreatic cancer.
• Live alone. Retired school teacher.
• Only Son lives in another state

PhysicalFunctional AbilityStrength/Fatigue
Sleep & RestNauseaAppetite
ConstipationPain
PsychologicalAnxiety
DepressionEnjoyment/Leisure
Pain DistressHappiness
FearCognition/Attention
Quality of Life
SocialFinancial BurdenCaregiver Burden
Roles and RelationshipsAffection/Sexual Function
Appearance
SpiritualHope
SufferingMeaning of Pain
ReligiosityTranscendence
http://prc.coh.org
Quality-of-Life Model

Maintaining Hope in the Midst of Death
• Experiential processes• Spiritual processes• Relational processes• Rational thought processes• Remember the caregiver
Ersek & Cotter, 2010
Tools and Resources for Palliative Care
Assessment Tools• Physical symptoms• Emotional symptoms• Spirituality• Quality of life• Caregivers outcomes
http://prc.coh.org

Prognostication• Consists of 2 parts:
– foreseeing (estimating prognosis) – foretelling (discussing prognosis)
• Performance status
– Karnofsky – ECOG poor predictors, multiple symptoms,
biological markers (e.g. albumin)
– “Would I be surprised if this patient died in the next 6
months?”Hui, 2012

• Kay, a 68-year-old woman with heart failure– Dyspnea at rest– On ACE inhibitors and beta blockers– Ejection fraction (EF) < 20%– Syncope– Resistant ventricular or supraventricular
arrhythmias• Would she qualify for hospice care, given
these symptoms?
Stop and Consider: Prognostication

• Some things cannot be “fixed”
• Use of therapeutic presence
• Maintaining a realistic perspective
Role of the Nurse in Improving Palliative Care

Extending Palliative Care Across Settings
• Nurses as the constant• Expanding the concept of healing• Becoming educated (Certification, HPNA)
Final Thoughts…..
• Quality palliative care addresses quality-of-life concerns
• Increased nursing knowledge is essential
• “Being with”• Importance of interdisciplinary
approach to care

“… touching the dying, the poor, the lonely, and the unwanted
according to the grace we have received, and let us not be ashamed or slow to do the
humble work.”-Mother Teresa

To Comfort Always