pad launch day - don griesdale
TRANSCRIPT
What’s Pain Got to Do With It?
PAD Launch DayMarch 30th, 2015
Donald Griesdale MD MPH FRCPCAssistant ProfessorDepartment of Anesthesiology, Pharmacology & Therapeutics Division of Critical Care MedicineUniversity of British [email protected]
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
1. Objectives
2. Disclosure
52 year old female, previously healthy
Immediate onset of pain and weakness in both hands
Immobilized at scene and transferred to hospital
CC licence: Ludovic Peron
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
Neurology: Grade 1 – 2 motor strength in bilateral upper extremities
4 – 5/5 strength in her legs
Decreased sensation in her hands
Conservative management
Transferred to spine ICU
Current pain management: Acetaminophen 975 mg PO q6h regularly
Hydromorphone 2 – 4 mg q4h prn (used 16 mg in 24 hours)
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
Describes 2 types of pain Neck pain (NRS 2 – 3 / 10)
“Burning, electrical shocks” in both arms and hands
NRS 8 – 10 / 10
Opioids dull the pain slightly, but don’t help much
Unable to sleep
Even the sheets touching her arms cause excruciating pain
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
Nociceptive Neuropathic
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
“Pain caused by a lesion or disease of the somatosensory nervous system”
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
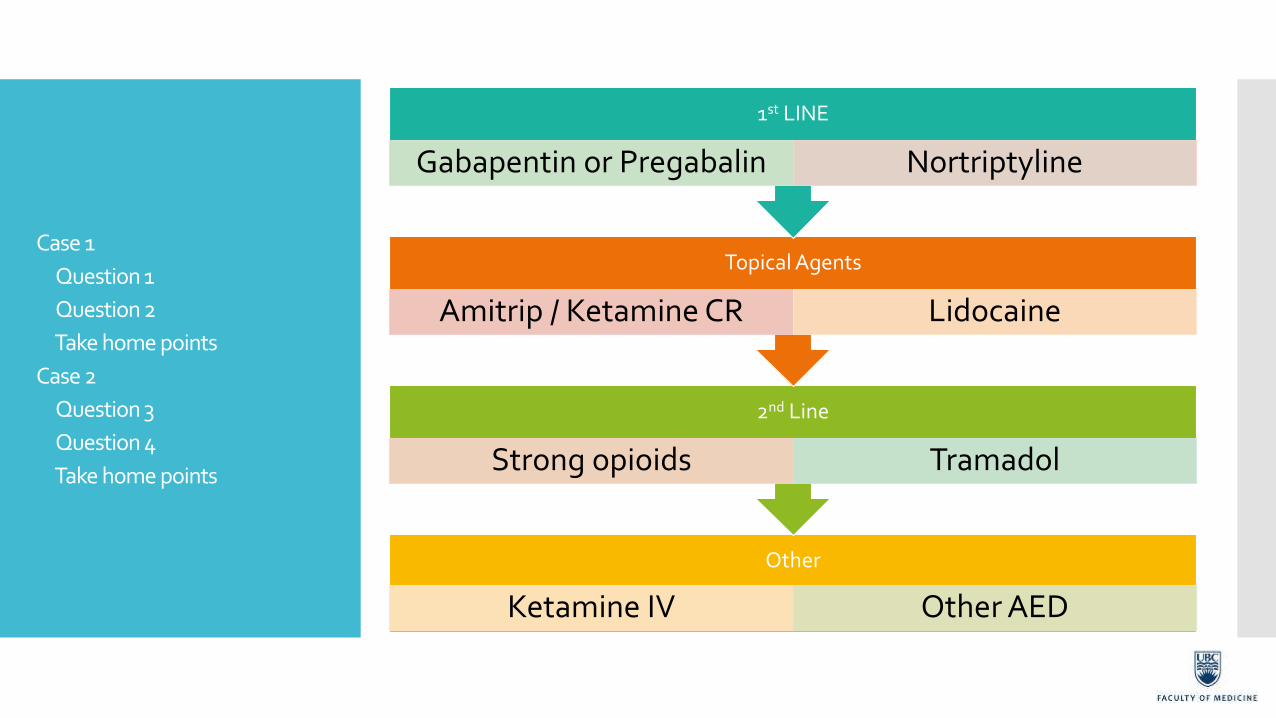
Other
Ketamine IV Other AED
2nd Line
Strong opioids Tramadol
Topical Agents
Amitrip / Ketamine CR Lidocaine
1st LINE
Gabapentin or Pregabalin Nortriptyline
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
Gabapentin
Start at 300 mg / day
Titrate up to 4800 mg / day
tid
SE: dizziness, somnolence, nausea, rash, blurred vision
Pregabalin
Start at 150 mg / day
Titrate up to 600 mg / day
bid
Similar SE to gabapentin
Better bioavailability
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
Initially started on: Pregabalin 150 mg / day
Nortriptyline 10 mg in AM and 25 mg qHS
Topical amitriptyline – ketamine cream
Oxycodone prn
Despite increasing her pregabalin, her neuropathic pain worsened
Repeat MRI to ensure no obvious worsening pathology
Started on ketamine IV
Topiramate 25 mg BID
Methadone 1 mg PO TID
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
Recognize and consider neuropathic pain
What is the etiology of neuropathic pain?
Pharmacologic management is different than with nociceptive pain
Early use of gabapentin / pregabalin and TCA’s
Use of topical agents for allodynia
Referral to a pain specialist for refractory neuropathic pain
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
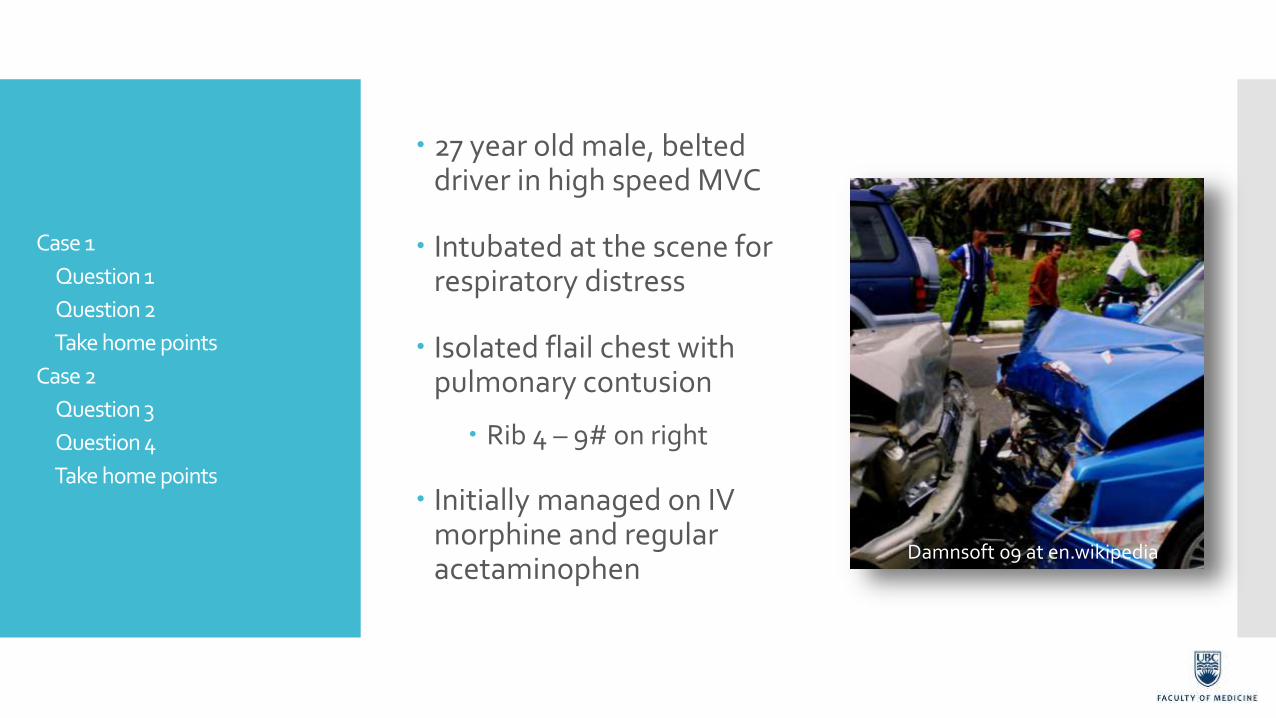
27 year old male, belted driver in high speed MVC
Intubated at the scene for respiratory distress
Isolated flail chest with pulmonary contusion
Rib 4 – 9# on right
Initially managed on IV morphine and regular acetaminophen
Damnsoft 09 at en.wikipedia
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
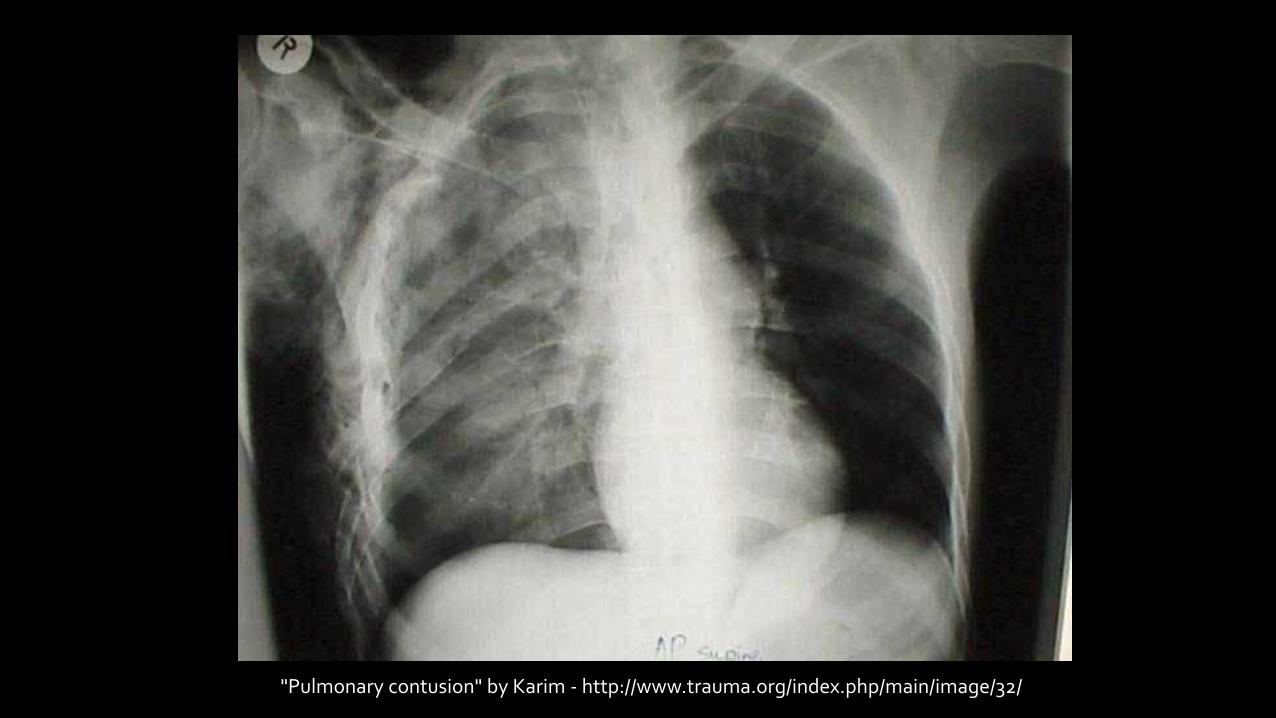
"Pulmonary contusion" by Karim - http://www.trauma.org/index.php/main/image/32/
Complications:
Pneumonia & empyema
Respiratory failure
Chronic pain & long term disability
Primary goals:
Excellent pain control
Pulmonary volume expansion
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
8 am the next day:
Currently on PSV 5, PEEP 5 with FiO2 0.40
You are now wanted to extubate this patient
Try to wean his propofol infusion!
Tachypneic, fighting ventilator
Hypertensive, tachycardic
RASS +2 to +3
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
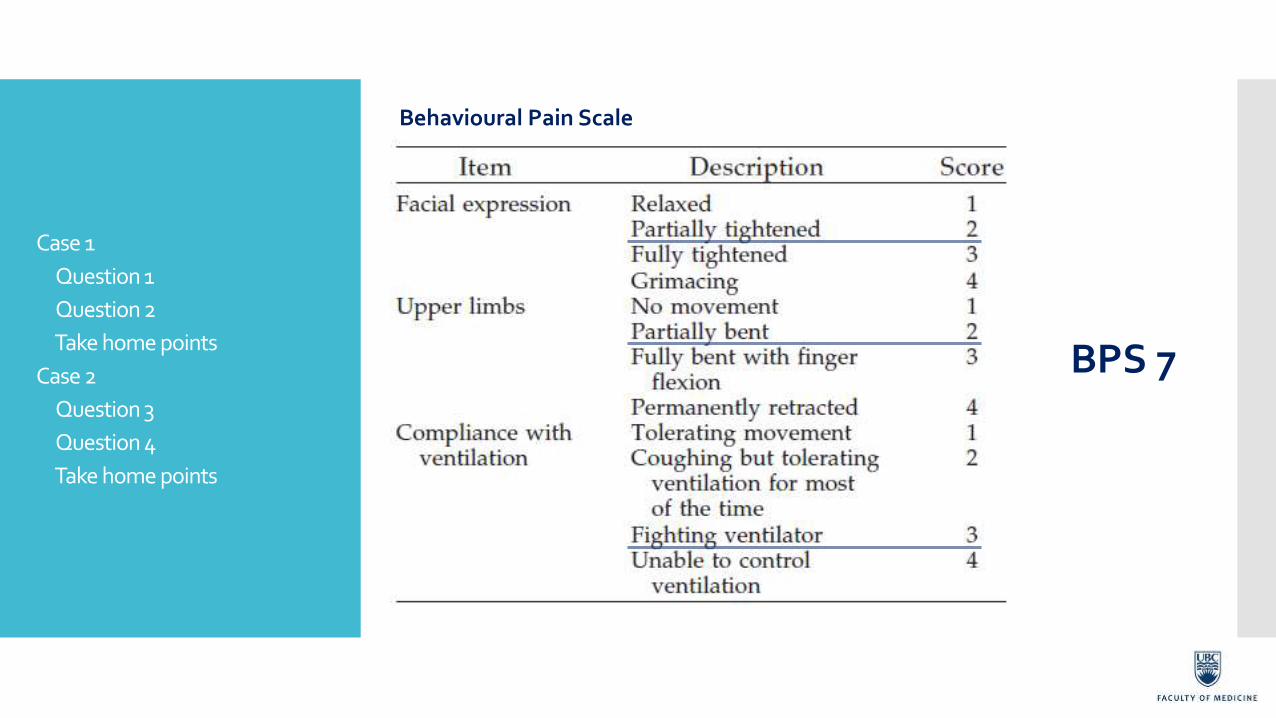
Behavioural Pain Scale
BPS 7
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points

ICDSC Score
Altered LOC 1
Inattention 1
Disorientation 1
Hallucinations – delusions 0
Psychomotor agitation or retardation 1
Sleep/wake cycle disturbances 0
Symptom fluctuation 1
TOTAL 5
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
Overnight pain management: Morphine total of 40 mg IV total
Tylenol 975 mg NG q6h
Methyltrimeprazine 20 mg IV total
Propofol infusion for sedation and ventilator synchrony
Report: “Either awake, agitated and confused or too sedated”
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
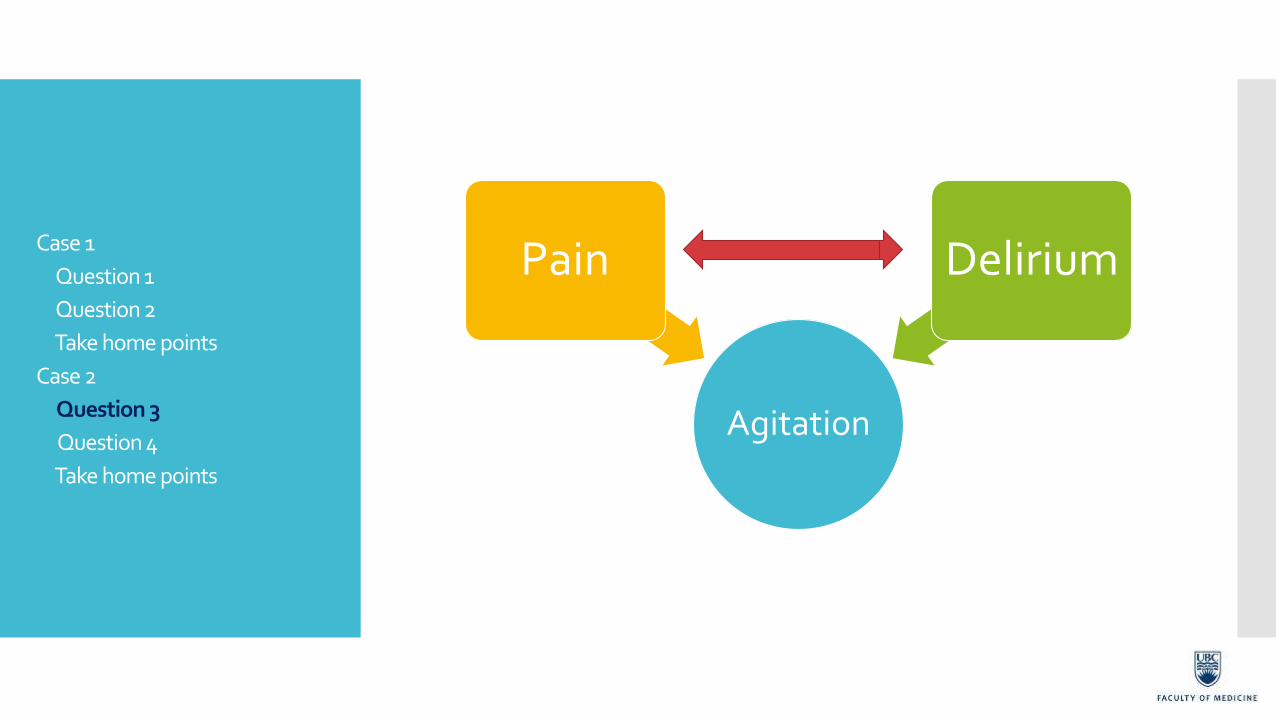
Agitation
Pain Delirium
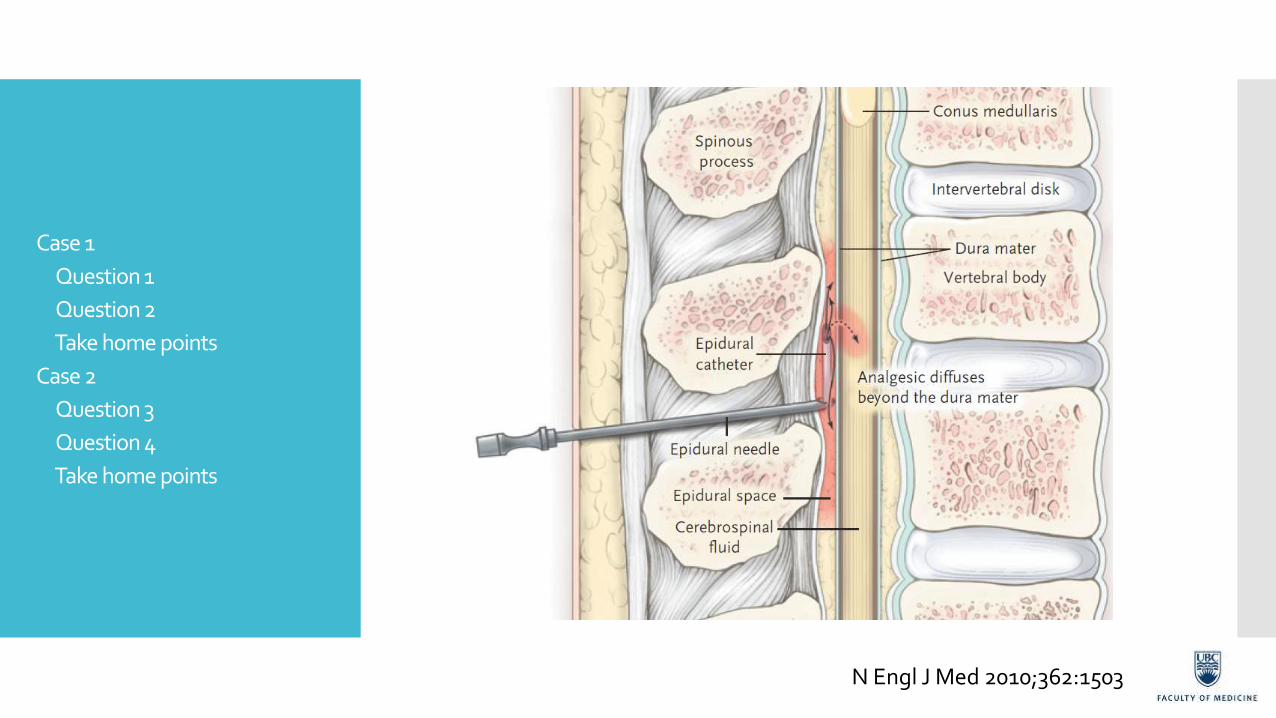
N Engl J Med 2010;362:1503
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
Infusion of local anesthetic & opioid
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points

Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
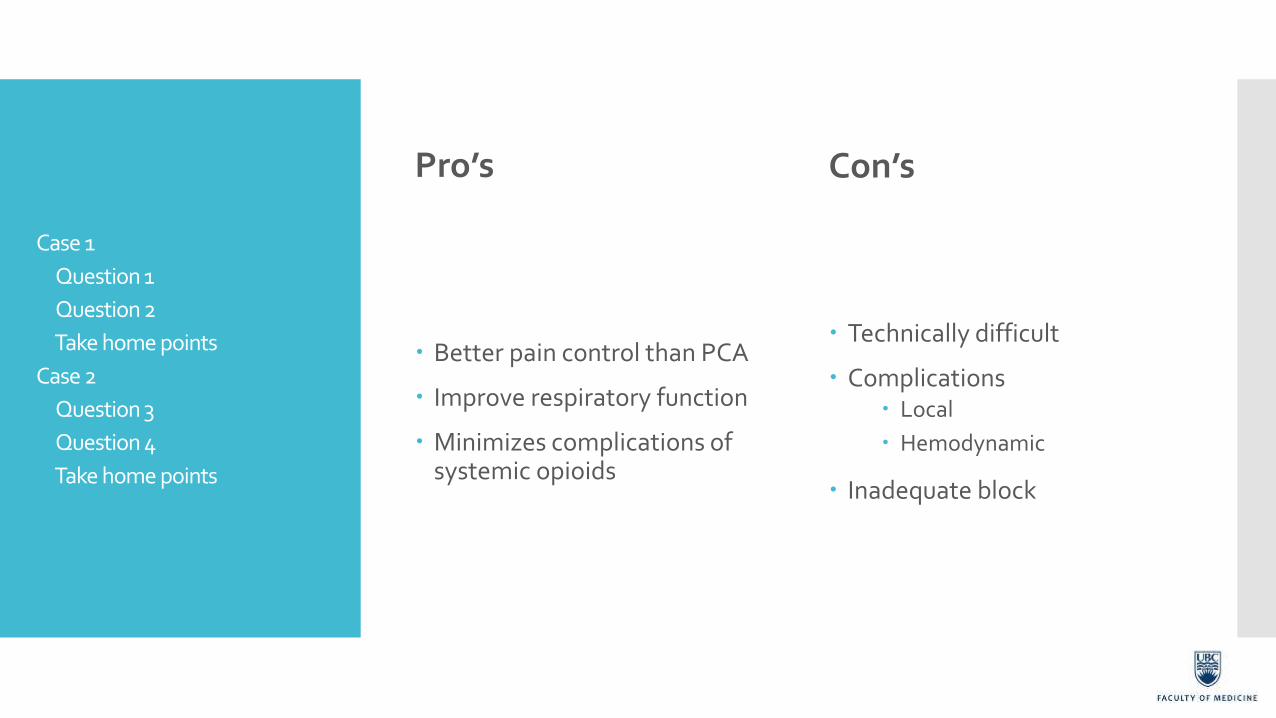
Pro’s
Better pain control than PCA
Improve respiratory function
Minimizes complications of systemic opioids
Con’s
Technically difficult
Complications Local
Hemodynamic
Inadequate block
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points

Contraindications to epidural anesthesia:
Coagulopathy Antiplatelet agents (e.g. Clopidogrel)
LMW heparin
Elevated ICP
Local or systemic infection
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
Epidural analgesia is a level1 recommendation for
the management of severe blunt chest injury
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points
Pain scales may not be specific
Consider the interactive effect of pain & delirium
Alternates to opioid analgesia where appropriate
Case 1
Question 1
Question 2
Take home points
Case 2
Question 3
Question 4
Take home points