pact and hf-how can we optimize care delivery for our patients susan kirsh md consultant for pact!,...
TRANSCRIPT

PACT and HF-How can we Optimize Care Delivery for our
Patients
Susan Kirsh MDConsultant for PACT!, Diabetes QUERI, Center
for Implementation Practice and Research Support
Louis Stokes Cleveland VAMC
Quality Enhancement
Research Initiative

Goals and Objectives
• Chronic disease care needs improvement
• Principles of PACT!• Examples of the
Chronic Care Model and PACT!
• Applying PACT! Principles to heart failures across VA
• Opportunities for collaboration

Veterans on average have 3 chronic conditions
3

4
Poor Care Coordination Leads to Unnecessary Hospitalizations
0 718
36
62
95
131
169
219236
261
0
50
100
150
200
250
300
0 1 2 3 4 5 6 7 8 9 10+
Number of Chronic Conditions
Hos
pita
lizai
tons
for
Am
bula
tory
C
are
Sens
itiv
e C
ondi
tion
s P
er
1000
Med
icar
e B
enef
icia
ries
A
ges
65+
Source: Medicare Standard Analytic File, 1999.

5
Failures in chronic disease quality
• Guidelines translate poorly into practice
• Measures not adequate• Underuse of information
management and decision support tools
• Resistance to change, even in the face of demonstrable failures
• Hard to influence public policy

Barriers to Effective Chronic Disease Management
• Rushed practitioners not following established practice guidelines (according to surveys)
• Lack of care coordination • Lack of active follow-up to ensure the
best outcomes • Patients inadequately trained to
manage their illnesses

Sub Optimal Functional and Clinical Outcomes
UnpreparedPractice
Team
Uninformed,Passive Patient
FrustratingProblem-Centered
Interactions
Usual Care ModelUsual Care Model
improving chronic illness care

PatientPatient
PCPCProviderProvider
Ho
sp
ita
lists
No
n-V
A C
are
Current Current Primary Care Primary Care
ModelModel

Chronic Care Model as a Solution/Recipe
The Chronic Care Model (CCM) identifies the essential elements of a health care system that encourage high quality chronic illness care
There are six fundamental elements “pillars of care” of the Chronic Care Model
Evidence-based change concepts under each element
Source: http://www.improvingchroniccare.org9

10
Joint Principles of the Joint Principles of the Patient-Centered Medical Home Patient-Centered Medical Home
TenetsTenets“Replaces episodic care based on illness and patient complaintswith coordinated care and a long‐term healing relationship” in
outpatient setting
• Ongoing relationship with personal physician or team-continuity
• Physician directed medical practice-or Primary Care Provider• Whole person orientation-Patient preferences • Enhanced access to care-appointments/services/information • Coordinated care across the health system-team care • Quality and safety-performance measures, registries
http://www.pcpcc.net/content/joint-principles-patient-centered-medical-home

PCMH/PACT!What it is; what it is not
• It is a series of attributes – some are very clear; some less so
• It is not a specific structure; the specific form will follow function, but is dependent on context
• It is the model the VA has chosen• It is not carte blanche to gain resources

The chronic care model with PCMH (Patient Aligned Care
Team)
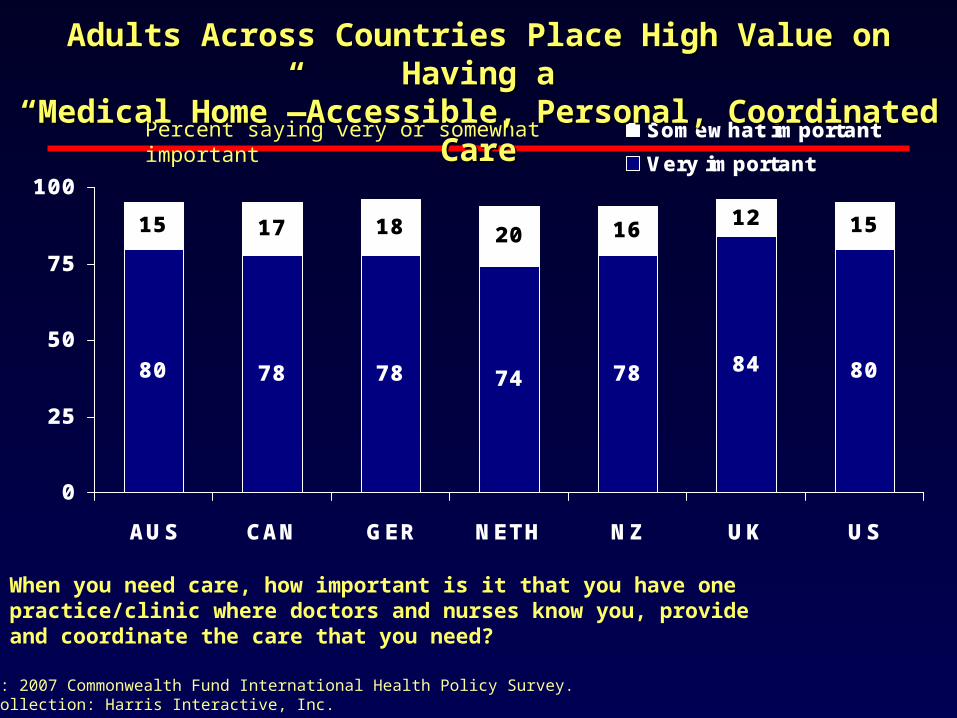
80 78 78 74 78 84 80
15 17 18 20 16 12 15
0
25
50
75
100
AUS CAN GER NETH NZ UK US
Somewhat important
Very important
Percent saying very or somewhat important
Adults Across Countries Place High Value on Having aAdults Across Countries Place High Value on Having a“Medical Home”—Accessible, Personal, Coordinated Care“Medical Home”—Accessible, Personal, Coordinated Care
When you need care, how important is it that you have one practice/clinic where doctors and nurses know you, provide and coordinate the care that you need?
Source: 2007 Commonwealth Fund International Health Policy Survey.Data collection: Harris Interactive, Inc.
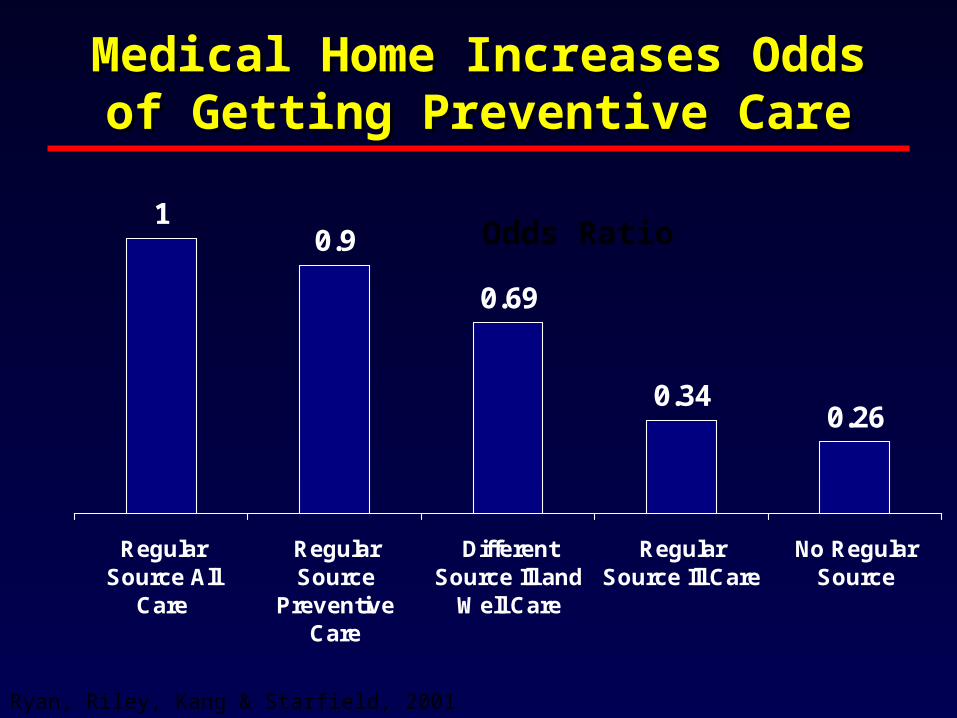
Medical Home Increases Medical Home Increases Odds of Getting Preventive Odds of Getting Preventive
CareCare1
0.9
0.69
0.340.26
RegularSource All
Care
RegularSource
PreventiveCare
DifferentSource Ill and
Well Care
RegularSource Ill Care
No RegularSource
Ryan, Riley, Kang & Starfield, 2001
Odds Ratio

15

Current PACT! initiatives
• Demonstration labs• IHI style improvement or learning sessions-6-
share information• Teamlet training• Tool development in CPRS
– Primary care almanac, decision support, risk tools
• Additional staff– nurse care coordinators– health promotion disease prevention staff
• National evaluation-ACP biopsy

Learning Sessions Focus on Pillars
• Enhanced access to care– Telephone clinics, CCHT (telehealth), my
health e vet, secure text messaging, huddles for daily open slots
• Coordinated care across the health system– TEAMS and populations-Shared medical
appointments, nurse and pharmacy planned care, nurse protocols, innovation for homeless, mental health, CKD, service agreements with specialists

Attributes in Primary Care
• Quality and Safety– Performance measures, next available
appointment, post-hospitalization follow up, medication reconciliation
• Whole person orientation– Patient preferences, shared decision making,
patient understands the disease process, realizes his/her role as the daily self manager, family and caregivers engaged, provider is a guide on the side
HF Clinic as a Medical Home
• Class III/IV HF-Cardiology is their home?• Principles can be applied to enhance care
delivery– Improve Access: Telephone clinics, CCHT,
telehealth consultation Cardiologists– Care Coordination: HF SMAs-MANUAL, NP
or Pharmacists following sickest patients with registries, close post-hospitalization clinics, electronic reminders to patients for labs, follow up appointments
Opportunities for Collaboration
• Go to staff • Shared templates• Service
agreements• Hospital discharge
coordination• Other suggestion-
we need sharing of best practices!