overuse injurues in overhead athletes 3
TRANSCRIPT

Vineet BansalSenior Sports physiotherapist.SSI/sports med.
Overuse shoulder injuries in Overhead athletes

Overuse shoulder injuries
Throwing, racquet sports, water sports, climbers
and Track & field.

Definition
Epidemiology
Mechanism
Prevention
Management
Epidemiology Upto 50% of elite female Handball players experience
shoulder pain (Cyril et al 2014).
Supraspinatus tendinosis in 67% in elite swimmers ( Matt et al 2005).
Training 15>hrs/wk and >35km/wk.
Shoulder pain is reported in 66% in swimmers. (Lenard funk et al 2015)
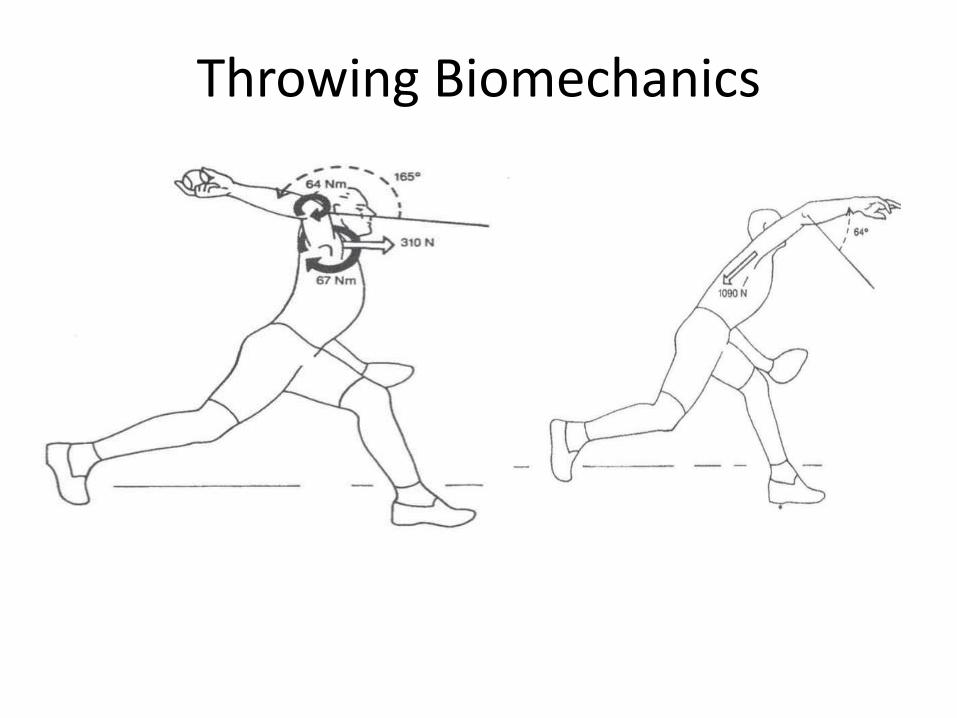
Throwing Biomechanics

Defination
Overuse injuries are charcterised by pain from gradual or insiduous onset. They are results of repetitive micro-trauma to tendons, muscles, ligaments, joints & bone.
( Bruce et al, JOSPT 2005)
More challenging to diagnose and treat.

Overuse/overload
Overhead arm action ( Volleyball, swimming, tennis) and throwing ( baseball, cricket, javelin).
Increase load, change in positional play or technique.
Clinical Diagnosis is frequently difficult.
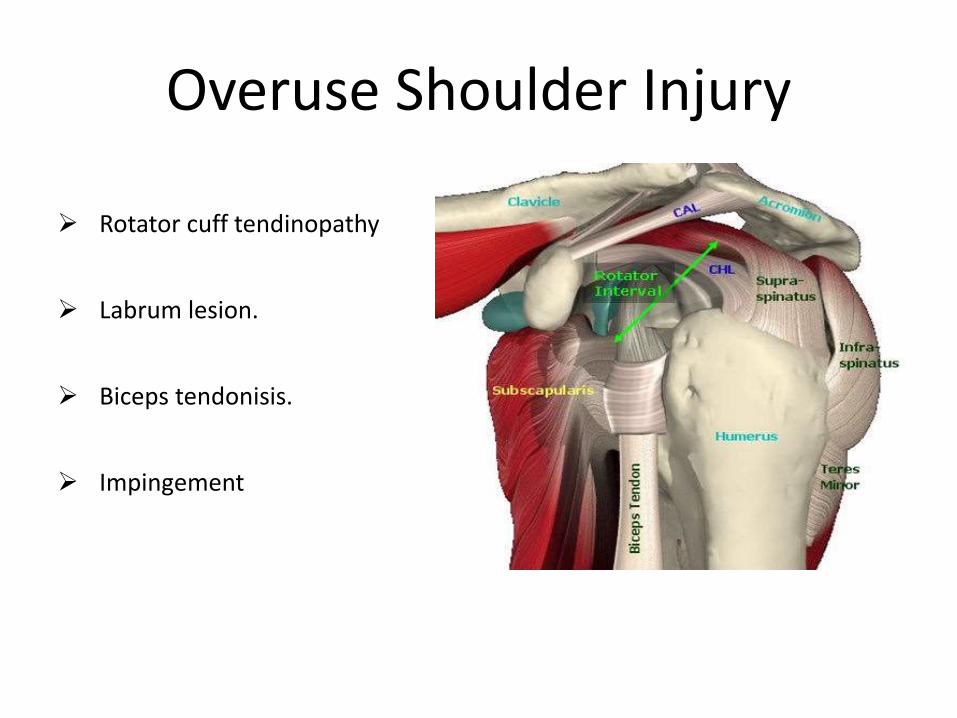
Overuse Shoulder Injury
Rotator cuff tendinopathy
Labrum lesion.
Biceps tendonisis.
Impingement
Predisposing Factors
AthleteLaxity ( Cheng et al JBJSB 2007).Proprioception ( Herrington roll)Isokinetics ( Jones & Funk 2010)Previous injurySudden increase in trainingIncomplete rehabilitation.
SPORTSpeed of play Timing Fatigue

Overuse injuries

Swimming Biomechanics

Throwing biomechanics

Late cocking phase of throwing catching phase of freestyle.

Mechanism
Repetitive activity, muscles, tendons & ligaments get stronger and more functional.
Remodeling process
Break down> build up tissue= injury

Painfree Shoulder Painful Shoulder
in swimmers in swimmers
UT activated No significant difference in
timing of onset of UT & LT
SA almost immediate
LT after approximate 15 SA consistently significantly
Abduction. delayed in Onset.
Wadsworth & Bullock 1997
Recruitment patterns of scapular muscles

Normal Swimmers
20% MVC in serratus anterior throughout swim stroke.
Painful Swimmers
Reduction in activity in serratus anterior throughout swim stroke
Increased activity in Rhomboids.
Pink et al 1991
Recruitment patterns of scapular muscles

Athletes often train 6-7 days/wk, 2/day.
Swimmers >15 hrs or >35 km chance of injury.
Technical faults increase chance of injury.
overuse/overload

1. Concentric ratio
CER :CIR (previously injured players < injury-free players).
2. Functional ratio
EER :CIR (Previously injured players < injury-free players).
Weakness in External rotaters.
Risk of reinjury.
Emphasis on Internal rotaters.
Zoe Poh & Marcus Lee
Profiling of shoulder strength and overhead throwing of singapore water polo players: the implications for injury prevention.
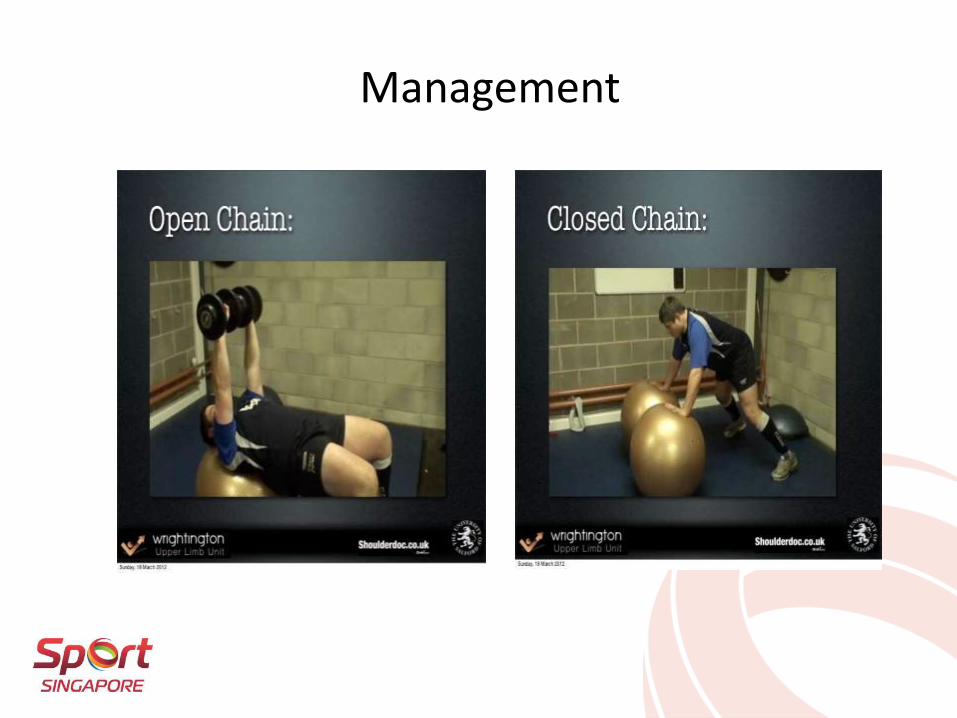
Management

Scapular muscles strengthening

Rehabilitation
Integrate kinetic chain into shoulder rehab exercises
Focus on open and closed chain exercises.
Challenge sports specific positions and movements.
• (Kibler AJSM 1998,
Lintner Sports Med 2008,
• Cools BJSM 2008)

Scapular exercises improves isokinetic muscle strength and muscle balance
in healthy adolescents swimmers. (Vd Velde JAT 2010, and ER strength
strength in volleyball players ).

Pendular exercises are started 3rd day onwards.
Upto 3 wks----Sling, AAROM, PROM.
Post capsule streching is continued.
From 4-6 wks External rotation in abduction will be started.
From 6-8 wks RC strengthening & biceps strenthening.
6-7 months Gradual return to overhead activity.
Post operative rehabilitation after SLAP repair

Reduce Training errors.
Comprehensive rehab program to develop muscle strength, flexibility, endurance & balance.
Eccentric strength is key to injury prevention.
Strengthening of Serratus anterior and subscapularis is key in injury prevention in swimmers
Reduce training volumes (FIT), 10% rule.
Early clinical diagnosis and management.
PREVENTION
Conclusion
Prevention is most important.
Shoulder pain can be improved with comphrensive rehabilitation program.
Timely clinical assessment.
Team approach critical ( Athlete + Coach + Parents + therapist+ Physician).

THANK YOU!