medial elbow problems in overhead athletes. outline anatomy biomechanics valgus instability valgus...
TRANSCRIPT

Medial Elbow Problems in Overhead Athletes

Medial Elbow Problems in Overhead Athletes

Outline
Anatomy
Biomechanics
Valgus Instability
Valgus Extension
Overload
Medial Epicondylitis

Anatomy
Normal carrying angle 11-16 deg of valgus
50% elbow stability due to boney configuration (<20 deg, and > 90 deg)
3 main soft tissue component
Anterior capsule
Radial Collateral complex
Ulnar Collateral Complex

AnatomyLigament Biomechanics
AMCL & RCL taught throughout ROM
Axis of elbow rotation occurs thru RCL Humeral insertion
PMCL taught at >65 deg
AMCL strongest and stiffest
Failure load 260 N
Palmaris Longus 357 N
Regan, Morrey CORE ‘91

AnatomyUlna Collateral Ligament Complex
Anterior Bundle: inserst on medial coronoid process (sublime tubercule) eccentrically located
Consists of Ant and Post bands Ant band 10 restraint to valgus 0-90 deg.Post band increases restraint from 60-max flexion
Post band more important in Overhead athlete
ElAttrache, F. Jobe

Anatomy
Ulnar Collateral Complex
Anterior Bundle
Ant. band
Post. band

AnatomyAnt. Medial collateral: Length 27.1mm
Width 4.7mm

Anatomy
Ulnar Collateral Complex
Posterior Bundle: inserst on medial margin of Semilunar notch
Fan shaped
Thinner and weaker
20 restraint at >90 deg
Vulnerable to stress only if ant bundle disrupted
Callaway, Field JBJS ‘97
Anatomy
Ulnar Collateral Complex
Posterior Bundle
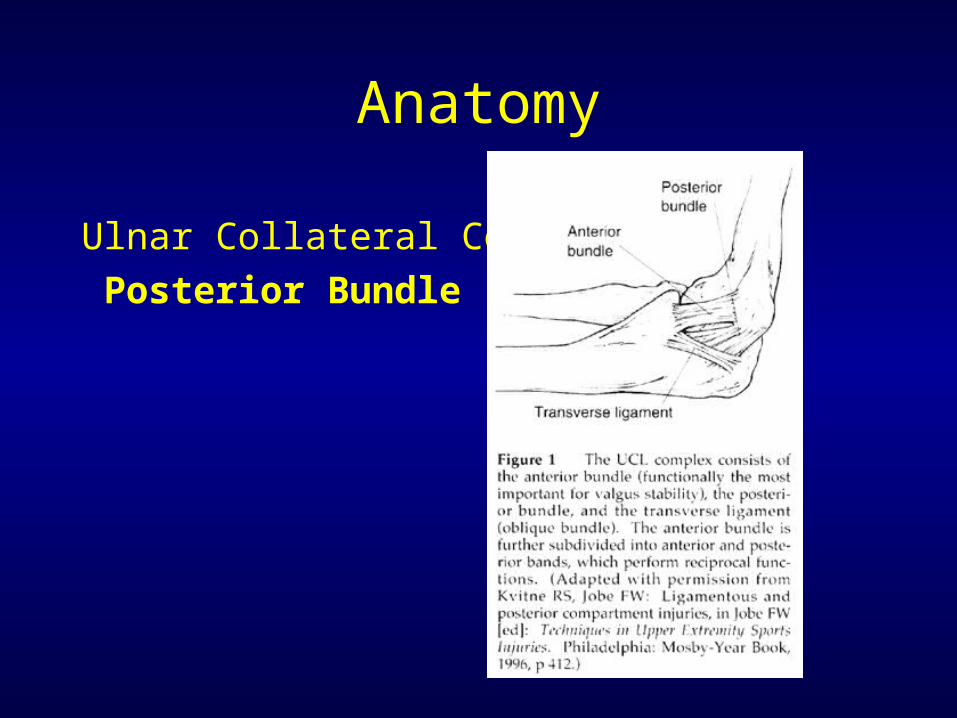
Anatomy
Ulnar Collateral Complex
Oblique/Transverse Bundle:
Deepens sigmoid notch
Flexor Pronator muscle mass
PT, FCR, PL, FDS, FCU
Dynamic contribution to valgus stability

Biomechanics: Stages of Pitching Motion
I Windup
II Early cocking, from ball leaving glove until forward foot contacts ground

Biomechanics: Stages of Pitching Motion
III Late cocking, maximal shoulder Ext rotation and Abduction, 90-120deg elbow flexion w/ increasing pronation

Biomechanics: Stages of Pitching Motion
IV Rapid acceleration, ends w/ ball releaseoccurs over only 40-50 msecangular acceleration of 600K deg/ secMaximal valgus stressLoad on MCL approaches tensile strength

Biomechanics: Stages of Pitching Motion
IV Rapid acceleration, ends w/ ball release

Biomechanics: Stages of Pitching Motion
V Follow-through, dissipation of stress rapidly, large decelerating forces
No greater adverse effects on elbow w/ Curveball Sisto, Jobe Am J Sp Med ‘87
Biomechanics: Stages of Pitching Motion
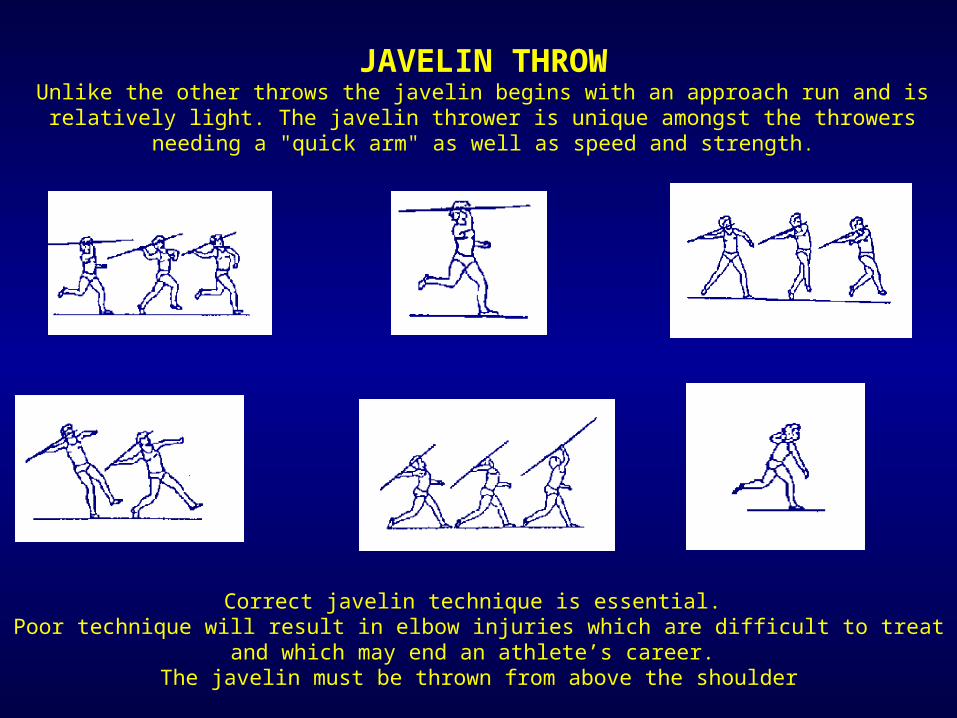
JAVELIN THROWUnlike the other throws the javelin begins with an approach run and is relatively light. The javelin
thrower is unique amongst the throwers needing a "quick arm" as well as speed and strength .
Correct javelin technique is essential. Poor technique will result in elbow injuries which are difficult to treat and which may end an athlete’s career.
The javelin must be thrown from above the shoulder

JAVELIN THROWUnlike the other throws the javelin begins with an approach run and is relatively light. The javelin thrower is unique amongst the throwers
needing a "quick arm" as well as speed and strength.

Valgus Instability
Traumatic
not subtle, hear/feel pop
Repetitive micro-trauma
more common, chronic
subtle exam
Valgus Instability
Pitchers w/ UCL deficiency have dec.activity of Flex/pronator muscles during pitch sequence by EMG
Glousman, Jobe Am J Sports Med ‘92
Leads to cycle of injury
Inc. instability inc. force 20 stabilizers radial/capitellar jt chondromalcia

Valgus Instability: Diagnosis
History:
Medial elbow pain w/ throwing >60-75% suggestive of ligament attenuation
Mechanical c/o
Sensation of instability
Check for Ulna nerve symptoms- 40% incidence

Valgus Instability: Diagnosis
PE:
ROM - limited terminal extension
Tenderness w/ palpation
Pain w/ resisted wrist flexion, pronation
Valgus stress test and Milking Maneuver

Valgus Instability: DiagnosisPE: Valgus stress testposition b/w 30-900
stabilize against body, apply stresscompare side-side difference
Only 3-4mm of opening w/ complete rupture

Valgus Instability: DiagnosisPE: Milking ManeuverPullng on pt’s thumb w/ forearm supination,shoulder extension, elbow flexed > 90 deg
Tests posterior bandof anterior bundle

Valgus Instability: Diagnosis
Imaging:
Xray- loose bodies, osteophytes, calcifications
Gravity stress: >3mm diagnostic
*may be neg w/ known UCL lig rupture
MRI- Study of choice, perform w/elbow in extension, 3mm coronal sections, +/- gad

Valgus Instability:Treatment
Nonoperative
Understand Pt’s goals
Rx of choice for acute injury in non-throwers
PT, technique changes, relative rest 3-6 months
50% success at returning athlete to pre-injury level

Valgus Instability:Treatment

Valgus Instability:Treatment
Operative
Indications: failure of above x 3-6 months, commitment to play at competitive level, (baseball,volleyball, javelin, gymnastics, tennis)
Or acute injury in above patients

Valgus Instability:Treatment
Operative
Techniques: direct repair for acute injury
or those w/ limited career
Similar recovery time (Jobe)
Ligament reconstruction
graft choice: palmaris, semitendinosis, allograft, plantaris, strip of achilles or FCR

Valgus Instability:TreatmentOperative Technique

Valgus Instability:TreatmentOperative Technique
Preserve branches of Antebrachial cutaneous N
Preserve Common flexor origin at epicondyle
Split flexor mass at post 1/3 in line w/ fibers
Separate Lig complex, incise and check joint.
Drill holes and weave tendon, check isometry
Tension at 45deg. Neutral varus/valgus
Transpose nerve only if pre-op neuritis, subluxation, or constriction noted at surgery

Valgus Instability:TreatmentOperative Technique

Valgus Instability:TreatmentPostoperative
Immobilize 7-10 days
Active ROM x 4-6 weeks
Wrist and Forearm strengthening
Avoid valgus stress for 4 months
After 6 months begin lobbing ball, progressively increasing distance and speed; back to mound at 8-9 months w/ <70% velocity until 1 yr.

Valgus Instability:TreatmentOperative Results
Conway, Jobe ’92 JBJS 70 pts, F/U 6.3 yrs
Direct repairReconstructed
Return to 7/14 38/56
sport
G&E 10/14 45/56
Previous operation led to dec ability to return to sport
All w/ ant. Transposition of Ulna N
Complications: 15 P-op neuropathy; 6 transient 9 requiring decompression

Valgus Instability:TreatmentOperative Results
Thompson, Jobe ’01 JSES83 pts w/o Ulna transpositionAll reconstructed w/ muscle splitting aproach23% Pre-op ulna symptoms5% Transient post-op ulna neuropathyIn 33 pts w/ >2 yr f/u : 82% excellent, 12% good
resultsAll pts returned to sport, 82% at same level 4 w/ re-op: 1 for re-tear of flexor/pronator muscle
3 w/ arthroscopic posterior debridement

Valgus Instability:TreatmentOperative Results
Azar, Andrews ’00 Am J Sports Med
59/78 reconstructions and 8/13 repairs, F/U 36mos
81% recon, 63% repairs returned to same level
Overall 79% success rate
Ave time to competitive throwing 9.8 months
9/10 w/ ulna neuropathy resolved P-op

Valgus Instability:TreatmentOperative Results
Azar, Andrews ’00 Am J Sports Med
Complications: 1 ulna neuropathy (resolved @10 months)
1 arthroscopic lysis of adhesion, 1 arthroscopic posterior debridement
2 c/o pain at palmaris harvest site, 2 superficial infections at graft site, 1 at elbow wound

Valgus Extension Overload
Secondary to insufficiency of UCL
Leads to subluxation in extension, w excessive forces at lateral and posterior aspects of elbow
Radiocapitellar chondromalacia => OCD, OC Fx, loose bodies

Valgus Extension Overload
Diagnosis
Symptoms: catching, locking
Tenderness at medial olecranon
Pain during late acceleration and follow thru
Xray: Spurs post medial olecranonloose bodies

Valgus Extension Overload
Treatment
RICE
Rehab
Surgery if failure to respond

Valgus Extension Overload
Surgical Treatment
Arthroscopy
eval for laxity w/ valgus stress test
If >1-2mm of medial ulna-humeral opening=> ant bundle insufficiency.
If >4mm => complete MCL insufficiency Field Altcheck AJSM
‘96
Avoid resection of >3mm from olecranon

Valgus Extension OverloadSurgical Treatment Results
Fideler, Kvitne JSES ‘97
113 professional baseball players
100% dec pain and symptoms
74% G&E results w/ return to same level
Bradley JSES ’95
6/6 NFL Linemen w/ G&E results 2 yrs post debridement
Medial Epicondylitis
Golfer’s elbow
Patholigic degenerative changes in Flexor/pronator insertion
7-20x less common than Lat Epi
Usually involves humeral origin of Pronator Teres, FCR and less frequently FCU
PT most active in overhead athletes
Medial Epicondylitis
PE: + TTP, eval stability
60% assoc w/ Ulna neuropathy
RX:
Rest, Nsaids, good short term relief w/ steroid injection(<6)
Change technique, PT
90% success w/ no-op treatment

Medial EpicondylitisSurgery indicated if failed > 6 mos conservative Rx.
Frequently find full thickness tears.
Debridement, w/ secure tendinous repair

Medial EpicondylitisSurgical Results:
Vangsness, Jobe JBJSB’ 91
34/35 pts G&E results
86% no limitations, all returned to sport
Isokinetic and grip strength difference not significant

Medial EpicondylitisSurgical Results:
Gabel, Morrey JBJS ‘9526 pts, 30 elbows
96% G&E results
Those w/ ulna symptoms only 40% (2/5) G&E

The END