outline business case for the acute services … · outline business case for the acute services...
TRANSCRIPT

Redacted for Publication - see front cover
COMMERCIAL IN CONFIDENCE
Outline Business Case for the Acute Services Redevelopment Project
NHS Dumfries and Galloway June 2013
Some content redacted to maintaincommercial confidentiality duringprocurement process. Redactedelements will be published at a laterdate

Redacted for Publication - see front cover

Redacted for Publication - see front cover
Contents 1 INTRODUCTION .......................................................................................................... 1
1.1 Purpose ........................................................................................................... 1
1.2 Context of the Proposed Investment ............................................................ 1
1.3 Project History ................................................................................................ 2
1.4 Compliance with National Capital Investment Guidance ............................. 2
1.5 Structure of the Outline Business Case Document ..................................... 3
1.6 Further Information ........................................................................................ 4
STRATEGIC CASE ............................................................................................................... 5
2 PROFILE OF NHS DUMFRIES AND GALLOWAY ...................................................... 6
2.1 NHS Dumfries and Galloway – purpose and objectives .............................. 6
2.2 Geography ...................................................................................................... 7
2.3 Demography ................................................................................................... 8
2.4 Current Services ............................................................................................. 8
2.5 Activity and Performance .............................................................................11
2.6 Conclusion .....................................................................................................13
3 STRATEGIC CONTEXT ............................................................................................. 14
3.1 Overview ........................................................................................................14
3.2 National Context ............................................................................................14
3.3 Developing the Clinical Strategy ..................................................................14
3.4 Local Context .................................................................................................16
3.5 Conclusion .....................................................................................................21
4 BUSINESS CASE OBJECTIVES & SCOPE .............................................................. 23
4.1 Overview ........................................................................................................23
4.2 Conditions for Success .................................................................................23
4.3 Key Investment Objectives ...........................................................................29
4.4 Project Scope ................................................................................................29
4.5 Existing Arrangements .................................................................................30
4.6 The Case for Change .....................................................................................30
4.7 Implications of not providing a new District General Hospital ...................36
4.8 Conclusion .....................................................................................................37
5 MODEL OF CARE AND SERVICE SPECIFICATION ................................................ 38
5.1 Overview ........................................................................................................38
5.2 Scope of Service Provision...........................................................................38
5.3 Principles and Process in Developing the Models of Care .........................38
5.4 Proposed Models of Care .............................................................................40

Redacted for Publication - see front cover
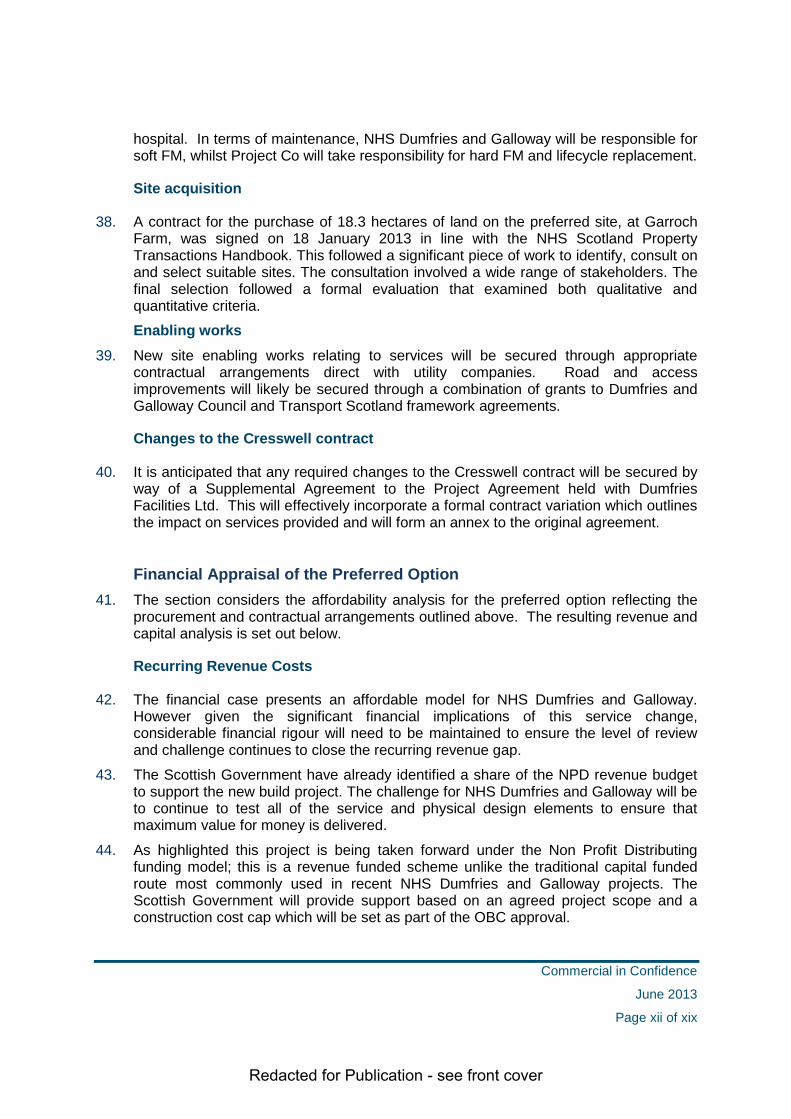
5.5 Service benefits of the new models of care .................................................44
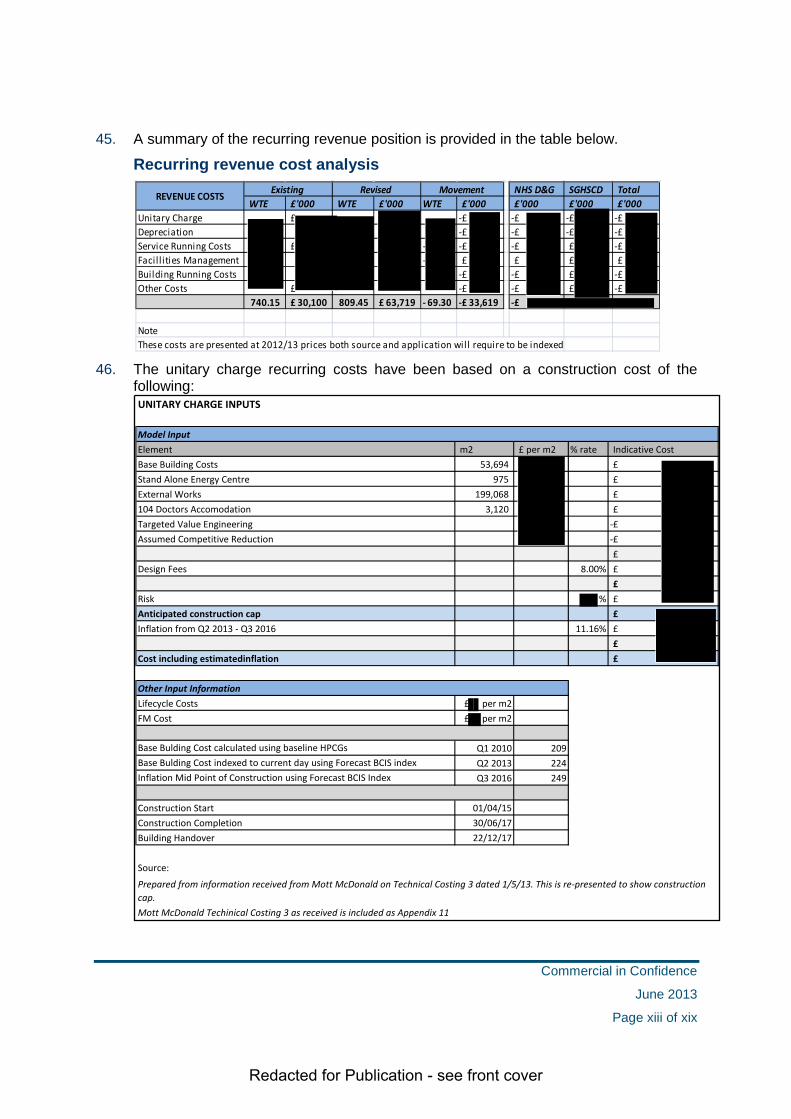
5.6 Clinical and Design Briefs.............................................................................44
5.7 Conclusion .....................................................................................................45
6 WORKFORCE PLANNING ........................................................................................ 46
6.1 Overview ........................................................................................................46
6.2 Current Staffing Position ..............................................................................47
6.3 Assessing Future Workforce Requirements ...............................................47
6.4 Management of Workforce Change ..............................................................51
6.5 Workforce Development Plans .....................................................................53
6.6 Organisational Development (OD) Support .................................................53
6.7 Conclusion .....................................................................................................53
7 FUTURE SERVICE REQUIREMENTS ....................................................................... 54
7.1 Overview ........................................................................................................54
7.2 General Approach to Service Modelling ......................................................54
7.3 Service Modelling Methodology and Assumptions.....................................55
7.4 Future Service Requirements – Admitted Patient Care ..............................61
7.5 Future Service Requirements – Theatres and Endoscopy .........................63
7.6 Summary of Current and Future Requirements ..........................................67
7.7 Conclusion .....................................................................................................68
ECONOMIC CASE .............................................................................................................. 69
8 OPTION OVERVIEW .................................................................................................. 70
8.1 Overview ........................................................................................................70
9 OPTION IDENTIFICATION ......................................................................................... 71
9.1 Overview ........................................................................................................71
9.2 Long List of Options......................................................................................71
9.3 Short Listed Options .....................................................................................72
10 OPTION APPRAISAL ................................................................................................ 73
10.1 Overview ........................................................................................................73
10.2 Non financial Benefits ...................................................................................73
10.3 Non financial Risks .......................................................................................75
10.4 Economic Appraisal ......................................................................................77
10.5 Option Appraisal Results ..............................................................................78
11 PREFERRED OPTION ............................................................................................... 79
11.1 Overview ........................................................................................................79
11.2 Analysis of the Option Appraisal Results ....................................................80
REFERENCE DESIGN ........................................................................................................ 83

Redacted for Publication - see front cover
12 REFERENCE DESIGN PROCESS ............................................................................. 84
12.1 Summary ........................................................................................................84
12.2 Hospital Building ...........................................................................................84
12.3 Ward Layout ...................................................................................................85
12.4 Ensuite single inpatient rooms .....................................................................86
12.5 Access, parking and helipad ........................................................................87
12.6 Staff residences .............................................................................................87
12.7 Energy centre ................................................................................................88
12.8 Landscaping ..................................................................................................88
12.9 Sustainable Urban Drainage System ...........................................................88
12.10 Design Development .....................................................................................88
12.11 Costing Methodology ....................................................................................90
COMMERCIAL CASE ......................................................................................................... 91
13 PROCUREMENT ROUTE ASSESSMENT ................................................................. 92
13.1 Overview ........................................................................................................92
13.2 Key Features of the Assessment..................................................................92
13.3 Proposed Procurement Route ......................................................................92
13.4 Procurement Strategy and Process .............................................................93
13.5 Community Benefits ......................................................................................95
13.6 Conclusion .....................................................................................................96
14 OTHER PROCUREMENT ISSUES............................................................................. 97
14.1 Overview ........................................................................................................97
14.2 Cresswell Wing ..............................................................................................97
14.3 Selection and Acquisition of New Hospital Site ..........................................99
14.4 Partnership Approach to Planning and Other Issues .................................99
14.5 Site Option Appraisal .................................................................................. 101
14.6 Acquisition of Garroch Farm Site ............................................................... 102
14.7 Enabling Works on the New Hospital Site ................................................. 103
14.8 Disposal of Current Hospital Site ............................................................... 103
15 PROPOSED CONTRACTUAL ARRANGEMENTS .................................................. 104
15.1 Overview ...................................................................................................... 104
15.2 Contractual Issues ...................................................................................... 104
15.3 Required Services ....................................................................................... 105
15.4 Proposals for Risk Transfer ........................................................................ 105
15.5 Proposed NPD Payment Mechanism ......................................................... 105
15.6 Non NPD Contractual Issues ...................................................................... 106

Redacted for Publication - see front cover
15.7 Personnel Implications ............................................................................... 107
15.8 Accountancy Treatment .............................................................................. 108
FINANCIAL CASE ............................................................................................................. 109
16 FINANCIAL APPRAISAL ......................................................................................... 110
16.1 Overview ...................................................................................................... 110
16.2 NPD Funding Model Overview .................................................................... 111
17 RECURRING REVENUE .......................................................................................... 113
17.1 Overview ...................................................................................................... 113
17.2 Unitary Charge Payment ............................................................................. 115
17.3 Depreciation ................................................................................................. 119
17.4 Service Running Costs ............................................................................... 120
17.5 Facilities Management Services ................................................................. 121
17.6 Building Running Costs .............................................................................. 122
17.7 Other Associated Costs .............................................................................. 123
17.8 Summary of Affordability ............................................................................ 123
17.9 Conclusion ................................................................................................... 125
18 CAPITAL .................................................................................................................. 126
18.1 Overview ...................................................................................................... 126
18.2 Site Acquisition ........................................................................................... 127
18.3 External Enabling Works ............................................................................ 127
18.4 Off site Capital Works ................................................................................. 127
18.5 Site Clearance Costs ................................................................................... 128
18.6 Equipment Group 2 & 3 ............................................................................... 128
18.7 Capital Cost Summary ................................................................................ 129
18.8 Optimism Bias ............................................................................................. 130
18.9 Summary of Capital Affordability ............................................................... 131
18.10 Conclusion ................................................................................................... 131
19 NON RECURRING REVENUE EXPENDITURE ....................................................... 132
19.1 Project Running Costs ................................................................................ 132
19.2 Commissioning............................................................................................ 132
19.3 Building Double Running Costs ................................................................. 132
19.4 Group 4 Equipment ..................................................................................... 132
19.5 Excess Travel Costs .................................................................................... 132
19.6 Summary of Affordability ............................................................................ 133
19.7 Conclusion ................................................................................................... 133
20 ACCOUNTANCY TREATMENT ............................................................................... 134

Redacted for Publication - see front cover
20.1 Overview ...................................................................................................... 134
20.2 Assets within the scope of NPD contract .................................................. 134
20.3 Existing PFI arrangement at Cresswell ...................................................... 135
20.4 Capital Additions ......................................................................................... 135
20.5 Impairments ................................................................................................. 136
20.6 Conclusion ................................................................................................... 136
MANAGEMENT CASE ...................................................................................................... 137
21 PROJECT MANAGEMENT & PROJECT IMPLEMENTATION TIMETABLE ........... 138
21.1 Overview ...................................................................................................... 138
21.2 Project Management Strategy and Methodology ...................................... 138
21.3 The Project Framework ............................................................................... 138
21.4 Project Roles and Responsibilities ............................................................ 139
21.5 Project Plan .................................................................................................. 148
21.6 Project Communication and Reporting Arrangements ............................. 149
21.7 Key Stage Reviews ...................................................................................... 149
22 MANAGING SUCCESSFUL DELIVERY .................................................................. 151
22.1 Overview ...................................................................................................... 151
22.2 Change Management Plan .......................................................................... 151
22.3 Approach to change management ............................................................. 153
22.4 Benefits Realisation Planning .................................................................... 153
22.5 Risk Management Plan ................................................................................ 154
22.6 Proposals for Post Project Evaluation ....................................................... 156
GLOSSARY OF TERMS ................................................................................................... 159

Redacted for Publication - see front cover
Table of Figures Figure 1-1: Structure of the Outline Business Case .................................................................. 3 Figure 2-1: Hospital services in NHS Dumfries and Galloway ................................................... 7 Figure 2-2: Inpatient care available at hospital sites .................................................................. 8 Figure 2-3: Service provided on DGRI site ................................................................................ 9 Figure 2-4: Analysis of inpatient beds at DGRI (April 2012) .................................................... 10 Figure 2-5: DGRI day case and day treatment facilities in DGRI ............................................ 10 Figure 2-6: Comparison of DGRI hospital activity with Board wide activity by Episode (2009/10 to
2011/12) ............................................................................................................................ 11 Figure 2-7: Emergency Department (ED) attendances (2009/10 to 2011/12) ......................... 12 Figure 2-8: Outpatient attendances (2009/10 to 2011/12) ....................................................... 12 Figure 2-9: Board financial performance £000......................................................................... 13 Figure 4-1: Conditions for Success .......................................................................................... 24 Figure 4-2: Investment Objectives ........................................................................................... 29 Figure 4-3: GROS population projections 2010 to 2035 .......................................................... 32 Figure 6-1: Current staffing by staff group (WTEs) at Dec 2012 ............................................. 47 Figure 7-1: Modelling methodology .......................................................................................... 56 Figure 7-2: Planning assumptions – inpatients and day case ................................................. 56 Figure 7-3: Planning assumptions – theatres and endoscopy ................................................. 57 Figure 7-4: Planning assumptions – outpatients ...................................................................... 59 Figure 7-5: Admitted patient care requirements...................................................................... 61 Figure 7-6: Analysis of general inpatient beds by bed occupancy and LoS ............................ 62 Figure 7-7: Theatre requirements ............................................................................................ 63 Figure 7-8: Endoscopy suite requirements .............................................................................. 65 Figure 7-9: Clinic room requirements ....................................................................................... 65 Figure 7-10: Summary of requirements by service area to 2026............................................. 67 Figure 8-1: Development of economic case ............................................................................ 70 Figure 9-1: Long list of options ................................................................................................. 71 Figure 9-2: OBC option shortlist ............................................................................................... 72 Figure 10-1: OBC benefit criteria and links to investment objectives ...................................... 73 Figure 10-2: Benefit scores for shortlisted options .................................................................. 74 Figure 10-3: Result of benefits sensitivity testing .................................................................... 75 Figure 10-4: Analysis of qualitative risk levels figure ............................................................... 75 Figure 10-5: Results of the risk assessment ............................................................................ 76 Figure 10-6: Results of the economic appraisal £000 ............................................................. 77 Figure 10-7: Results of NPV sensitivity analysis...................................................................... 78 Figure 10-8: Results of the option appraisal ............................................................................ 78 Figure 10-9: Results of the cost per benefit point .................................................................... 78 Figure 11-1 : Summary of option appraisal rankings ............................................................... 79 Figure 11-2 : Cost per benefit point as part of sensitivity testing ............................................. 79 Figure 15-1: Contract structure and payments ...................................................................... 104 Figure 16-1: Financial framework .......................................................................................... 110 Figure 16-2: NPD unitary charge funding arrangements ....................................................... 112 Figure 17-1: DGRI baseline budget ....................................................................................... 113 Figure 17-2: Affordability cost elements ................................................................................. 114 Figure 17-3: Input costs ......................................................................................................... 116 Figure 17-4: Unitary charge analysis ..................................................................................... 117 Figure 17-5: Unitary charge sensitivity 1 ................................................................................ 118 Figure 17-6: Unitary charge sensitivity 2 ................................................................................ 118 Figure 17-7: Depreciation analysis ........................................................................................ 119 Figure 17-8: Service running costs analysis .......................................................................... 120 Figure 17-9: FM running costs analysis ................................................................................. 122 Figure 17-10: Building running costs analysis ....................................................................... 123 Figure 17-11: Other associated costs analysis ...................................................................... 123 Figure 17-12: Revenue costs summary ................................................................................. 124 Figure 18-1: Capital cost elements ........................................................................................ 126 Figure 18-2: Capital cost requirements .................................................................................. 129 Figure 18-3: Total capital requirements ................................................................................. 130

Redacted for Publication - see front cover
Figure 18-4: Capital costs summary ...................................................................................... 131 Figure 19-1: Non recurring revenue costs summary ............................................................. 133 Figure 20-1: Accounting Treatment elements ........................................................................ 134 Figure 20-2: Impairments ....................................................................................................... 136 Figure 21-1: Project structure................................................................................................. 139 Figure 21-2: Project roles and responsibilities ....................................................................... 140 Figure 21-3: Individual roles and responsibilities ................................................................... 145 Figure 21-4: Key project milestones ...................................................................................... 148 Figure 21-5: NPD procurement journey and KSRs ................................................................ 149 Figure 22-1: Impact of change ............................................................................................... 151 Figure 22-2: Benefits Management approach........................................................................ 153 Figure 22-3: The four stages of PPE ..................................................................................... 156

Redacted for Publication - see front cover
Commercial in Confidence
June 2013
Page i of xix

Redacted for Publication - see front cover
Executive Summary
Introduction 1. This Outline Business Case (OBC) presents a compelling vision for reshaping health
services across NHS Dumfries and Galloway. At its heart are redesigned, high quality services to meet the needs of patients and to facilitate the delivery of clinical activity as close to home as possible.
2. The OBC sets out proposals for the reprovision of the Board’s main acute hospital facility, the Dumfries and Galloway Royal Infirmary (DGRI), within a modern, patient centred and highly efficient environment. This will be underpinned by more effective use of locally based services including the cottage hospitals.
3. The ageing population is one of the key challenges for the Board as is increased demand for unscheduled care. These are clearly linked.
4. The OBC is part of the NHS Board’s Clinical Strategy which is consistent with the Scottish Government’s 20:20 vision. The Clinical Strategy plans for a service within which:
• There is a marked emphasis on prevention
• Resources are directed towards management (including self management) of long term conditions and provides structured pro-active care
• Care and treatment is provided, where clinically appropriate, in primary care and community settings
• When hospital admission is required, it will be provided, where possible as a day case
• When a patient requires an inpatient stay, they will experience prompt, safe, clinically effective and person-centred care. There will be an emphasis on discharge to home or to intermediate care as soon as possible with support as needed
5. The Board’s ambition is to reshape the way services are provided and the provision of a new District General Hospital is a key component that must be viewed in the context of system wide changes.
Strategic Context 6. The national context for the development of health services in Scotland is set out in the
following policy initiatives:
20:20 Vision “Achieving sustainable quality in Scotland’s healthcare”.
The Healthcare Quality Strategy for NHS Scotland (May 2010).
Reshaping for Older People: a programme for change (2011).
Consultation on the Integration of Adult Health and Social Care published in May 2012
State of NHSScotland Assets and Facilities Report for 2012
Commercial in Confidence
June 2013
Page ii of xix

Redacted for Publication - see front cover
7. In developing the Clinical Strategy for the new hospital a number of factors were taken into account
The need to provide accessible emergency services to deal with acute illness or injury.
The Scottish Government’s “Presumption against centralisation where clinically appropriate”
Recognition of both the rurality and remoteness of Dumfries & Galloway.
8. The local context for the development of services within NHS Dumfries and Galloway both responds to the national drivers set out above and reflects on other strategies that will support the proposals set out within the OBC. The local context is centred on the following strategic areas:
Putting You First (PYF) is a five year Change Programme for Dumfries and Galloway. The aim of the programme is to develop models of service based on the principles of prevention and early intervention in an approach that supports working with partner organisations, communities and individuals.
The Role of the Cottage Hospitals The increased activity in cottage hospitals is an integral part of the planned clinical model for the new hospital: We plan that, for many patients, assessment and clinical management planning in the Combined Assessment Unit will be followed by early transfer to their local cottage hospital where treatment and rehabilitation will be progressed. This arrangement:
Helps us address the demographic challenges of the years ahead Reduces the number of acute beds needed in the new hospital Is popular with older patients Ensures effective use of our estate Helps maintain “critical mass” in localities, which in turn can support day
care, palliative care and minor injuries services.
The Financial Context provides the background for the investment in this outline business case to improve the provision of acute care across NHS Dumfries and Galloway. Through this approach the Board are confident that they can secure the delivery of long lasting / sustainable improvements in clinical services on an affordable basis. The financial case for the investment within the OBC envisages significant improvements in the use of existing resources.
The Board’s Property Strategy supports the programme of service improvement and the delivery of the Board’s vision for the future. It envisages that acute services would be provided in modern, fit for purpose facilities which, when taken with changes in the use of other hospital and community services, would fully support the proposed models of care. Furthermore it would address the significant, and increasing, backlog maintenance liability as well as reducing property running costs over time. The proposed provision of a new District General Hospital would allow many of the property strategy ambitions to be realised.
The Board’s eHealth Strategy and its successful implementation is key to supporting the Board in meeting its strategic objectives. In particular, it is
Commercial in Confidence
June 2013
Page iii of xix

Redacted for Publication - see front cover
anticipated that key benefits will arise through faster access to relevant information (allowing for improved patient safety and more timely delivery of care) as well as increasing flexibility in the way the Board utilises its workforce.
Business Case Objectives
9. The key SMART project Investment Objectives are summarised below:
Key SMART objectives
Ref OBC - Key Investment Objectives
1 Clinical Effectiveness & Sustainability: to ensure the Board provides services which are clinically effective and sustainable over the long term e.g. 30+ years.
2 Physical Environment: to facilitate the provision of services in a high quality environment which is ‘fit for purpose’ for patients, staff and visitors.
3 Capacity & Demand: to ensure the Board can respond to the demand for inpatient, day case and outpatient services.
4 Delivering models of care in line with the developing clinical strategy: to ensure that secondary care services facilitate joint planning in the development of patient focussed services, in a primary and community setting.
5 Access: to maximise access to hospital services for the local population.
6 Performance & Efficiency: to ensure the hospital is developed in such a way as to maximise performance and improve efficiency.
7 Recruitment, retention of staff and students: to ensure the Board is able to recruit and retain highly skilled staff to support the delivery of high quality patient care.
10. The Investment Objectives are underpinned by a set of ‘Conditions for Success’ which set out conditions that need to be in place to ensure a successful outcome from the OBC in terms of output and performance. A description of the conditions for success and the data that will enable measurement of progress are detailed in the document
Scope of Service Provision 11. The full range of services that are presently delivered from the existing acute hospital
will be provided from the new District General Hospital (with the exception of Renal, Ophthalmology and a number of AHP outpatient clinics which will be delivered from Cresswell).
Commercial in Confidence
June 2013
Page iv of xix

Redacted for Publication - see front cover
Case for Change 12. The Case for Change is built around four key themes, all of which are critical to
delivering a successful outcome for the project. These are:
a. The need to be able to respond to National Policy such as 2020 vision, the Quality Strategy and Reshaping Care for Older People and to facilitate the delivery of local initiatives such as Putting You First.
b. The need to be able to respond to and manage future demographic change. The demographic change impacts on both the ageing population and their health needs and the workforce for the future.
c. The need to further modernise services, focusing on quality and clinical effectiveness.
d. The need to address backlog maintenance and the lack of functional suitability of current DGRI facilities, along with the need to improve the patient environment, in order to be able to modernise service delivery and meet targets and objectives.
Model of Care and Service Specification 13. The models of care will support the delivery of the NHS Board’s vision of shifting the
balance of care. The future demographic projections predict that there will be greater demands on the social and healthcare systems. There will also be a potentially reduced workforce to provide the traditional models of care. A new hospital with a person centred reconfigured model of care is a crucial part of increasing productivity.
14. Key areas for redesign have been identified and include:
Emergency Care
Care of Older People
Theatres/ Endoscopy/ Day Surgery/ 23 Hour Care
Critical Care
15. The overarching principle is to reduce the rate of increase in acute hospital admissions while ensuring that those who require admission can be seen, fully investigated and treated as quickly as possible. Clinical services, responsive to patient need, will be available over a 24/7 period and must support a seamless patient pathway across primary and secondary care and facilitate improved utilisation of the Board’s cottage hospitals.
Future Service Requirements 16. Future service requirements include a range of core planning assumptions plus a
series of service changes designed to enhance the effectiveness of services provided within the new District General Hospital and more widely across NHS Dumfries and Galloway. Capacity requirements and outputs have been developed for:
Inpatient beds
Day case and ambulatory care
Theatres
Commercial in Confidence
June 2013
Page v of xix

Redacted for Publication - see front cover
Scoping suites
Outpatient consulting rooms
17. The table below summaries the future capacity requirements for 2026. This year was chosen as a realistic timeframe that would reflect essential components of demographic change, and includes the following:
Current DGRI capacity
The outcome of a capacity planning exercise utilising a range of planning assumptions about future service requirements
Capacity planned to be provided within the hospital development, taking due account of departmental and ward configuration etc.
Summary of requirements by service area to 2026
Facility Current Actual
Future Service
Requirements
Actual number provided
Medical/Surgical Wards 271 214 210
Combined Assessment 0 42 42
23 Hour 0 14 14
Critical Care 18 16 17
Palliative Care 8 8 8
Children's Unit 23 24 24
Obstetrics 38 29 29
Total inpatient beds 358 347 344
Day Case Unit trolleys 14 20 20 Ambulatory Care trolleys/chairs 8 10 10 Total trolleys/chairs 22 30 30
Theatres 9 9 81
Scoping suites 3 3 4
Outpatient consulting rooms 27 33 33
1 Excludes the Ophthalmology Theatre that will be based in Cresswell
Commercial in Confidence
June 2013
Page vi of xix

Redacted for Publication - see front cover
Workforce Planning 18. The Board has developed a robust process for assessing and managing the impact of
the changes to staffing brought about by implementing the proposals contained within the OBC. This includes an assessment of the following areas:
The factors that affect the workforce plan
How the Board will identify future staffing requirements
How the change process will be managed
19. The Board have applied the 6 Steps methodology to support its workforce planning processes. This sets out a consistent, practical framework to develop workforce plans. The 6 steps of this framework are summarised as follows:
Defining the plan
Mapping service change
Defining the required workforce
Understanding workforce availability
Developing an action plan
Implement, monitor and refresh
20. Workforce development will be a crucial element in delivering new models of care and ensuring a safe, skilled and effective workforce. Future focus will be on the development of integrated team working. Work has already been undertaken to identify the learning and development needs of staff in relation to the models of care. A number of initiatives are currently being tested and trialled through our strategic change programme “Putting You First”, such as the Dumfries Health and Social Care Hub. This is a multi-disciplinary / multi-agency service with a single point of contact to streamline patient care.
Option Appraisal 21. This section of the OBC sets out the options considered as part of the option appraisal
process and the resulting preferred option. The primary aim is to demonstrate which option offers best value for money by considering the benefits, costs and risks.
22. The case clearly highlights the preferred option which can demonstrate the optimal balance across the core elements.
Commercial in Confidence
June 2013
Page vii of xix

Redacted for Publication - see front cover
Option Identification 23. A long list of options were considered and the following short list of options were taken
forward Option Name Description
1 Do Minimum Addresses backlog maintenance relating to existing DGRI whilst providing some additional ward accommodation. This is achieved through a combination of upgrade to the existing estate and new build. The Cresswell wing is retained in its current form.
2 New DGRI on current site
Provides for a new DGRI on the existing hospital site utilising current car parking space. The Cresswell wing is retained but function reviewed in light of issues associated with links to the new development.
3 New DGRI on alternative site
Provides for a new DGRI on a greenfield site within Dumfries. Cresswell wing is retained but with alternative use.
Option Appraisal Results 24. To assess the relative value for money a comparison of the NPV per benefit point has
been undertaken and is shown below. This is calculated by dividing the NPV by the benefit score for each option to provide a comparable cost per benefit point.
Results of the cost per benefit point
Option 1 Option 2 Option 3
NPV over appraisal period (£000)
Benefits Appraisal (points) 462.90 816.40 890.10
NPV per Benefit Point (£000)
Ranking 3 2 1
25. The results show that when comparing the relative costs and benefits of the alternative solutions, Option 3 has the lowest overall cost per benefit point indicating this option delivers the best value for money of the short listed options.
Commercial in Confidence
June 2013
Page viii of xix

Redacted for Publication - see front cover
Preferred Option 26. The analysis of the short-listed options and associated sensitivities identifies that
Option 3; a new DGRI on an alternative site is the preferred option. This solution satisfies the project investment objectives and evidences the best overall value for money. It delivers the proposed models of care, the required capacity and an appropriate clinical environment.
27. The key features of the preferred option include:
• A new build hospital on a site located within Dumfries adjacent to major transport routes
• Re-provision of all clinical and non-clinical services in fully fit for purpose accommodation with optimal adjacencies
• A change of use for the Creswell wing to ensure optimal future function
• An overall construction programme of 2 years and 3 months with construction completion in June 2017 and, following a period of commissioning and migration, opening of the new facilities in March 2018
• Demolition of the majority of the existing hospital site and subsequent disposal
Reference Design
28. The Board has worked with its advisors to develop a reference design for the Project. This includes the following:-
• A new hospital building, of low rise design of no more than four stories in height, to accommodate some 350 in-patient beds, with an internal floor space of approx 53,500sqm;
• formation of new access from an enlarged A75 / Garroch roundabout and realignment of the Glen Road; separate dedicated emergency entrance, and secondary goods and services access;
• 980 car parking spaces and 80 cycle parking spaces;
• a helipad;
• staff residences;
• a dedicated energy centre;
• landscaping, including extensive cut and fill operations to level the site, with retention /re-use of all material along eastern site boundary;
• provision of Sustainable Urban Drainage scheme; & off-site road infrastructure improvement works.
29. The ward layout aims to capture as much natural light and ventilation as possible whilst delivering care efficiently and effectively. The wards will comprise 100% single rooms with ensuite facilities. The single room accommodation will provide increased privacy and dignity for patients and reduce the risk of acquiring an infection during their stay in
Commercial in Confidence
June 2013
Page ix of xix

Redacted for Publication - see front cover
hospital. Single rooms also provide the advantage of increased flexibility in the use of beds during periods of peak activity.
30. The reference design has been developed to RIBA Stage C and has been used to inform the estimation of the build cost for the Project. The costs are outlined in Technical Cost 3 and are based on current Health Planning Cost Guides (HPCG) adjusted for site/ design premiums associated with this Project. The forecast construction cost has been used within the Financial Case.
Procurement Strategy 31. As part of the Scottish Government draft budget announcement on 17 November 2010,
£2.5bn of revenue funded investment pipeline was identified of which £750m related to NHS Scotland projects. Specific provision was incorporated to support the delivery of the new hospital project utilising the Non Profit Distributing (NPD) programme supported by the Scottish Futures Trust (SFT). The project is also incorporated within the Scottish Government Infrastructure Investment Plan published on 4 February 2013.
32. The key factors influencing the selection of this approach are:
There will be few if any anticipated derogations required from the standard NPD contract
There has been a strong focus on ensuring adequate flexibility as part of the development of clinical requirements
The level of design work undertaken to date provides for further innovation across the procurement phase of the project
Acquisition of the proposed site is well progressed ensuring that this will not cause a delay to the project
The Board has established a sound governance and management structure for the project
The Board has already appointed technical, financial and legal advisers to augment its own resources and has appointed an experienced Project director.
The scale of the project ensures that transaction costs will be justifiable
Early indications are that there will be significant market interest in the project
33. Within the procurement strategy Community Benefits will be emphasised as key evaluation criteria in the selection of a preferred bidder. Bidders will be required to submit details of their proposals to actively promote and sustain such benefits, by, for example how their own business and employment policies will promote local employment, training and business opportunities with small and medium sized enterprises (SMEs). Bidders will be required to set out their proposals on how they will collaborate with established community benefit initiatives (e.g. existing local authority frameworks, trade associations and other similar organisations operating in Dumfries and Galloway).
Commercial in Confidence
June 2013
Page x of xix

Redacted for Publication - see front cover
Contractual Arrangements 34. The Board and its advisers have carefully considered the proposed contractual issues
relating to both the NPD and non NPD elements of the project which include the following:
New hospital development (NPD)
Site acquisition (non NPD)
Enabling works for the site
Adaptations to the Creswell building (non NPD)
Changes to the existing Creswell PFI contract (non NPD)
NPD Contract
35. A summary of the proposed NPD contract structure and associate payments is provided in the schematic below.
NPD Contract structure and payments
36. It is proposed that the form of contract will follow the standard form NPD project agreement. The contract will follow a 25 year duration post completion of construction and commissioning. It is intended that there will be no provision for breaks/review during this period.
37. NHS Dumfries and Galloway and Project Co will have specific roles and responsibilities in relation to the proposed deal, which will follow the standard NPD Contract split whereby Project Co will design, build, finance and maintain the new
Commercial in Confidence
June 2013
Page xi of xix
Redacted for Publication - see front cover
hospital. In terms of maintenance, NHS Dumfries and Galloway will be responsible for soft FM, whilst Project Co will take responsibility for hard FM and lifecycle replacement.
Site acquisition
38. A contract for the purchase of 18.3 hectares of land on the preferred site, at Garroch Farm, was signed on 18 January 2013 in line with the NHS Scotland Property Transactions Handbook. This followed a significant piece of work to identify, consult on and select suitable sites. The consultation involved a wide range of stakeholders. The final selection followed a formal evaluation that examined both qualitative and quantitative criteria.
Enabling works
39. New site enabling works relating to services will be secured through appropriate contractual arrangements direct with utility companies. Road and access improvements will likely be secured through a combination of grants to Dumfries and Galloway Council and Transport Scotland framework agreements.
Changes to the Cresswell contract
40. It is anticipated that any required changes to the Cresswell contract will be secured by way of a Supplemental Agreement to the Project Agreement held with Dumfries Facilities Ltd. This will effectively incorporate a formal contract variation which outlines the impact on services provided and will form an annex to the original agreement.
Financial Appraisal of the Preferred Option
41. The section considers the affordability analysis for the preferred option reflecting the procurement and contractual arrangements outlined above. The resulting revenue and capital analysis is set out below.
Recurring Revenue Costs
42. The financial case presents an affordable model for NHS Dumfries and Galloway. However given the significant financial implications of this service change, considerable financial rigour will need to be maintained to ensure the level of review and challenge continues to close the recurring revenue gap.
43. The Scottish Government have already identified a share of the NPD revenue budget to support the new build project. The challenge for NHS Dumfries and Galloway will be to continue to test all of the service and physical design elements to ensure that maximum value for money is delivered.
44. As highlighted this project is being taken forward under the Non Profit Distributing funding model; this is a revenue funded scheme unlike the traditional capital funded route most commonly used in recent NHS Dumfries and Galloway projects. The Scottish Government will provide support based on an agreed project scope and a construction cost cap which will be set as part of the OBC approval.
Commercial in Confidence
June 2013
Page xii of xix
Redacted for Publication - see front cover
45. A summary of the recurring revenue position is provided in the table below.
Recurring revenue cost analysis
46. The unitary charge recurring costs have been based on a construction cost of the
following:
NHS D&G SGHSCD TotalWTE £'000 WTE £'000 WTE £'000 £'000 £'000 £'000
Unitary Charge £ -£ -£ -£ -£ Depreciation -£ -£ -£ -£ Service Running Costs £ - -£ -£ £ -£ Facil l ities Management - £ £ £ £ Building Running Costs -£ -£ £ -£ Other Costs £ -£ -£ £ -£
740.15 30,100£ 809.45 63,719£ 69.30- 33,619-£ -£
NoteThese costs are presented at 2012/13 prices both source and application will require to be indexed
REVENUE COSTS Existing Revised Movement
UNITARY CHARGE INPUTS
Element m2 £ per m2 % rate Indicative CostBase Building Costs 53,694 £ Stand Alone Energy Centre 975 £ External Works 199,068 £ 104 Doctors Accomodation 3,120 £ Targeted Value Engineering -£ Assumed Competitive Reduction -£
£ Design Fees 8.00% £
£ Risk % £ Anticipated construction cap £ Inflation from Q2 2013 - Q3 2016 11.16% £
£ Cost including estimatedinflation £
Lifecycle Costs £ per m2FM Cost £ per m2
Base Bulding Cost calculated using baseline HPCGs Q1 2010 209Base Bulding Cost indexed to current day using Forecast BCIS index Q2 2013 224Inflation Mid Point of Construction using Forecast BCIS Index Q3 2016 249
Construction Start 01/04/15Construction Completion 30/06/17Building Handover 22/12/17
Source:
Model Input
Prepared from information received from Mott McDonald on Technical Costing 3 dated 1/5/13. This is re-presented to show construction cap. Mott McDonald Techinical Costing 3 as received is included as Appendix 11
Other Input Information
Commercial in Confidence
June 2013
Page xiii of xix

Redacted for Publication - see front cover
47. The build cost highlighted above is based on the work that has been carried out on the reference design.
48. Based on the information presented above an increase of £33.619m at current day prices is required to take forward this project; this equates to an additional investment of £ m for NHS Dumfries and Galloway and a £ m contribution from Scottish Government.
49. The above table indicates that the recurring cost to NHS Dumfries and Galloway will be £ m which is made up of a combination of Unitary Charge, depreciation, facility and revised service model costs. The Board has ring fenced £3.8m to offset the additional cost of the new build project. The estimated revenue gap of £ m will need to be secured through a dual approach of reducing the identified increased cost areas as described in the revenue section and also by releasing additional funding from the Board’s Five Year Financial Plan. This will be a challenging task; however, the latest iteration of the Board’s Financial Plan has made provision to fund this gap.
Capital Costs
50. The Board has developed a robust capital model which identifies all likely capital expenditure which is outwith the NPD model. The estimated cost of £53m is anticipated to be funded by Scottish Government as project specific funding.
51. The table below highlights when capital funding is likely to be needed in order to carry out the capital works and the associated funding assumptions.
Capital cost analysis 2013/14 2014/15 2015/16 2016/17 2017/18 2018/19 2019/20 2020/21 TOTAL
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000Site AcquisitionExternal Enabling WorksOff Site Capital WorksSite Clearance CostsEquipmentCapital Cost inc VAT & Fees 832 4,128 3,419 0 27,650 10,336 5,205 1,448 53,019
2013/14 2014/15 2015/16 2016/17 2017/18 2018/19 2019/20 2020/21 TOTAL£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
NHS Dumfries & GallowayScottish GovernmentCapital Cost inc VAT & Fees 832 4,128 3,419 0 27,650 10,336 5,205 1,448 53,019
Anticipated Costs
Funding Assumption
52. As previously highlighted NHS Dumfries and Galloway do not have sufficient capital
formula allocation to support this level of expenditure; it is therefore assumed that project specific funding will be allocated from Scottish Government.
Non Recurring Revenue Costs
53. The following table identifies the anticipated costs and the funding available to support the non recurring revenue requirements.
Commercial in Confidence
June 2013
Page xiv of xix

Redacted for Publication - see front cover
Non recurring revenue costs analysis
2013/14 2014/15 2015/16 2016/17 2017/18
Between 18/19 & 21/22 Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000Project Team & External AdvisorsAll other non recurring costsTotal Non Recurring Revenue Costs
2013/14 2014/15 2015/16 2016/17 2017/18
Between 18/19 & 21/22 Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000Currently within Financial PlanCurrently banked with SGHSCDTotal Non Recurring Revenue Costs
NON RECURRING COSTS
NON RECURRING FUNDING
54. The analysis shows that as a minimum £ m will be required to cover these costs. The Board are in a good financial position with regards to supporting these costs, having already identified £ m within future financial plans and having banked m in 2012/13 with Scottish Government towards these future costs. The final shortfall identified will require to be delivered through the identification of non-recurring sources in advance of 2017/18.
Accounting Treatment
55. A number of technical accounting issues arise as part of this project, the table below highlights the areas which need considered:
•Capital Purchases
•Capital Grants
•Exisiting DGRI•New Build DGRI•Cresswell
•NHS D&G Accounts
•National Accounts
•NHS D&G Accounts
•National Accounts
Assets within scope of NPD
contract
Existing PFI arrangement for Cresswell
Capital additionsImpairments
Commercial in Confidence
June 2013
Page xv of xix

Redacted for Publication - see front cover
56. It is assumed that the new hospital development will be on balance sheet for NHS Dumfries & Galloway purposes however off balance sheet for national accounting purposes.
57. It is further assumed that Cresswell will have no impact on the existing accounting treatment for either NHS Dumfries & Galloway or Scottish Government.
58. Capital additions will be capitalised by NHS Dumfries & Galloway in accordance with current guidance.
59. It is anticipated that assets will require to be impaired as part of this process. The table below gives an indicative view on values and the assumptions around funding however these will require to be refined as the external auditor’s opinion becomes available and the most current valuations are available.
Impairment TimingFinancial Year
Estimate £m
Funding Source
Existing DGRI Financial Close 2014-15 £ SGHSCD as part of Annually Managed Expenditure (AME)New DGRI Formal Handover 2017-18 £ SGHSCD as part of Annually Managed Expenditure (AME)Cresswell Formal Handover 2019-20 £ SGHSCD as part of IFRS Non Core Allocation
£
Note: These values require to be firmed upwith the professional external advisor once further clarity is available
Commercial in Confidence
June 2013
Page xvi of xix

Redacted for Publication - see front cover
Project Management Arrangements and Timetable
60. This project embraces the principles of project and programme management to ensure that the project is successfully delivered. The Acute Services Redevelopment Project is one of a series of projects within a framework of wider changes to the health system within Dumfries and Galloway. The diagram below sets out:
The overall project structure
How the Project Board and the Project Team fit into this structure
The key Project Management roles
Project structure
Investment Decision Maker (IDM) Dumfries and Galloway NHS Board
Performance Committee
Project Owner – NHS Dumfries and Galloway
Chief Executive
Project Director – Acute Services Redevelopment
Project Manager
Project Board
Project Team -Redevelopment led by
Project Manager
Stakeholder Groups
Project Group
Project Sponsor NHS Dumfries and Galloway Chief Operating Officer
External Advisors
Commercial in Confidence
June 2013
Page xvii of xix

Redacted for Publication - see front cover
61. The dates detailed in the table below highlight the key milestones for the project.
Project Milestones
Milestone Expected Date
OBC approved by NHS Dumfries and Galloway Board 08/04/2013
OBC submission to SGHD Capital Investment Group 16/04/2013
OBC approved by SGHD Capital Investment Group 21/05/2013
Commencement of new site enabling works 21/05/2013
NPD OJEU notice published 24/06/2013
NPD PQQ responses evaluated 24/09/2013
Issue of NPD ITPD 25/09/2013
Conclude NPD Competitive Dialogue 09/06/2014
Final NPD tender evaluation complete 05/09/2014
Selection of NPD Preferred Bidder 05/09/2014
NPD Financial Close 06/02/2015
New hospital construction start 01/04/2015
New hospital construction completion 30/06/2017
New hospital construction commissioning and handover 22/12/2017
Completion of service migration to new hospital 02/03/2018
First patients at new hospital 05/03/2018
Commencement of Cresswell adaptations 01/05/2018
Cresswell handover with adaptations 30/04/2019
Conclusion 62. The combined strategic, economic, financial, commercial and management cases
within this Outline Business Case (OBC) provides a compelling vision for reshaping health services across NHS Dumfries and Galloway.
63. The OBC sets out a robust case to transform and meet the future health needs of the population against the backdrop of considerable demographic and economic challenges facing the Board. The preferred option is a new acute facility on a new site serving the entire Dumfries and Galloway community. This option will enable the most economic and affordable implementation of new models of care that will transform the
Commercial in Confidence
June 2013
Page xviii of xix

Redacted for Publication - see front cover
way in which healthcare will be provided and will address the major deficiencies in the current estate. The development will provide enhanced services and quality for patients and will enable staff to work more efficiently and effectively in modern, accessible, safe and sustainable facilities located in the heart of the community.
64. The significant capital investment is shown to reflect NHS Dumfries and Galloway’s Local Plan in responding to national strategies. The OBC demonstrates with the benefit of a recently completed Independent Design Review that the preferred option represents best value for money and confirms that it is affordable to the Board.
65. The OBC describes the commercial viability of the procurement route chosen. The OBC competently describes the management plans and attendant governance structures that are already in place to deliver the project on an affordable basis, monitored at every stage.
66. The OBC confirms the Board’s strong commitment and approval of the preferred option and in submitting the OBC the Board is seeking the support to move to the Full Business Case of this essential development.
Commercial in Confidence
June 2013
Page xix of xix

Redacted for Publication - see front cover
1 INTRODUCTION
1.1 Purpose 1.1.1 The purpose of this Outline Business Case (OBC) is to present proposals
and seek approval to begin procurement for the development of a new replacement District General Hospital for Dumfries and Galloway which will support the health system in the delivery of new models of clinical care to better meet the future health needs of the local population.
1.1.2 This section of the OBC provides an overview of:
The context of the proposed investment
The project history
Relevant NHS Scotland Capital Investment Guidance
The structure and content of the OBC
1.2 Context of the Proposed Investment 1.2.1 Demographic projections show that over the next 20 years there will be a
steady increase in the number of frail older people, people living with multiple long term conditions and people with dementia. Despite the expectation that the ageing population may have on average better health than in the past, there will be substantially greater demands on the health and social care systems locally.
1.2.2 However, at the same time, there will be a decreasing number of working age people available to support this growing older population and this will be accompanied by continuing financial constraints. This Outline Business Case for a new acute facility sits within the overall context of the delivery of a new, future model of health and social care which meets the dual challenge of increasing demand on healthcare resources and is deliverable within a challenging environment, both economically and from a workforce perspective.
1.2.3 NHS Dumfries and Galloway’s corporate aims include “delivering excellent care that is “person centred, safe, effective, efficient and reliable”. The Board’s key change programme “Putting You First” was published in March 2011. It articulates delivery of these aims and identifies a range of areas to be targeted. The key ethos of this programme of work is to ensure the delivery of services and support as close to home as possible and to minimise reliance on hospital based services.
1.2.4 As work has progressed, a number of key service objectives have emerged. These include the development of effective and efficient pathways of care which support people to remain in their own home for as long as possible.
Commercial in Confidence
June 2013
Page 1 of 164

Redacted for Publication - see front cover
1.2.5 The challenging financial outlook for the public sector for the foreseeable future will require fundamental change in the way NHS services are provided and new ways of working to achieve the Board’s objectives.
1.2.6 The emerging models of care are intended to ensure that patients will only spend the time in an acute hospital environment that is clinically required and they will transfer from the more active and intense period of acute care to a more appropriate setting as soon as is possible (ideally home with support as necessary).
1.2.7 This change in emphasis towards reducing avoidable admissions, increasing throughput and further reducing average lengths of stay is essential if NHS Dumfries and Galloway is to continue to meet the demographic challenges highlighted above.
1.2.8 Achievement of these ambitions will require significant changes to the way we deliver services within the acute setting e.g. through an effective Combined Assessment Unit (CAU) which actively supports appropriate throughput of patients. This needs to be supported by a renewed focus on improving pathways of care through the general hospital to minimise lengths of stay and encourage appropriate use of community based support.
1.2.9 In addition, an extensive review of the fabric of the current hospital has indicated that it is beyond its useful economic life and significant backlog maintenance would be required to be addressed in order to sustain services. The current configuration does not support the required models of care. This project will enable the Board to deliver these key service objectives for the benefit of the people of Dumfries and Galloway. The changes in models of care need to be supported by a modern, fit for purpose inpatient facility.
1.3 Project History 1.3.1 Planning for the project has been underway for some years and initially
conceived a major refurbishment of the existing hospital or a rebuild on the existing site. In discussion with Scottish Government, the Board was invited to consider the project as part of the £2.5 billion Infrastructure Investment Plan. The Plan identified a replacement hospital for Dumfries and Galloway, as part of the health sector programme to be delivered through the Non Profit Distributing procurement model.
1.4 Compliance with National Capital Investment Guidance 1.4.1 The proposals are presented in the form of an Outline Business Case (OBC)
consistent with the requirements of the Scottish Government Health Directorates Capital Investment Manual issued via CEL 19 (2009) and any supplementary guidance.
1.4.2 The OBC framework allows the investment benefits, costs and risks to be identified and evaluated in a systematic way. It ensures that NHS Dumfries and Galloway can demonstrate that the investment is economically sound, financially viable and deliverable.
Commercial in Confidence
June 2013
Page 2 of 164
Redacted for Publication - see front cover
1.5 Structure of the Outline Business Case Document 1.5.1 The structure reflects the ‘5 Case’ approach as reflected in current Scottish
Government Health Directorates guidance and accepted best practice in Business Case development and presentation.
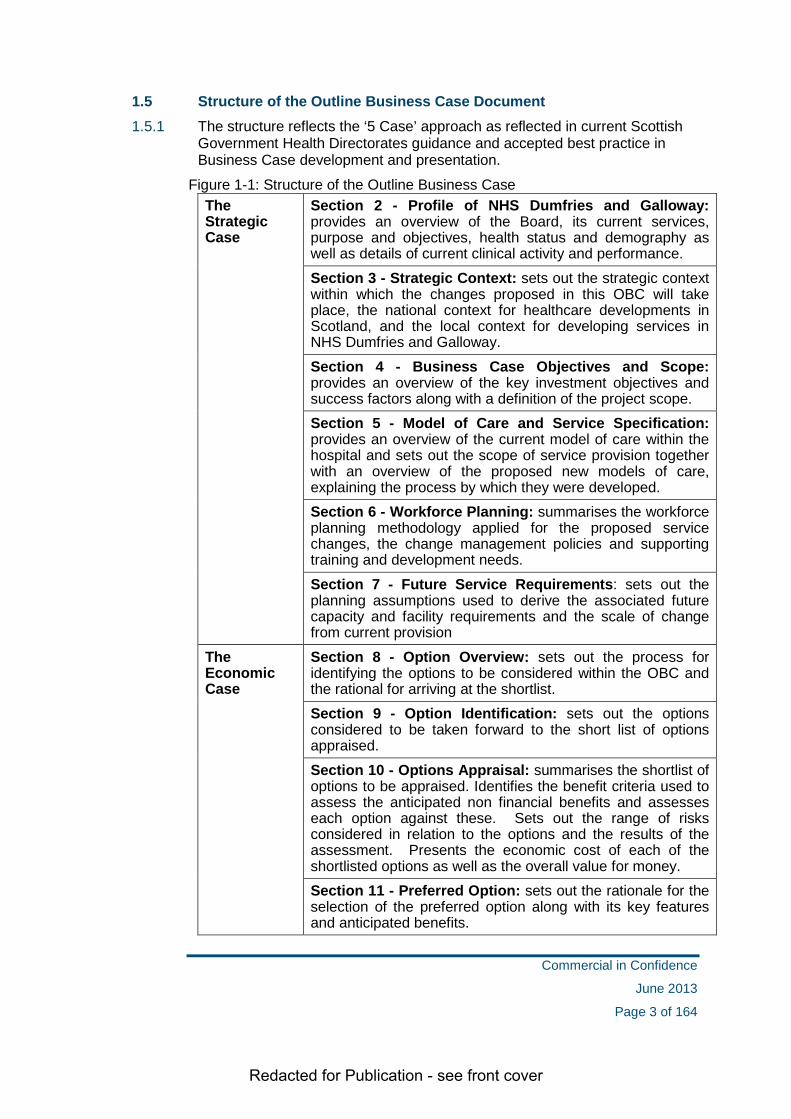
Figure 1-1: Structure of the Outline Business Case The Strategic Case
Section 2 - Profile of NHS Dumfries and Galloway: provides an overview of the Board, its current services, purpose and objectives, health status and demography as well as details of current clinical activity and performance.
Section 3 - Strategic Context: sets out the strategic context within which the changes proposed in this OBC will take place, the national context for healthcare developments in Scotland, and the local context for developing services in NHS Dumfries and Galloway. Section 4 - Business Case Objectives and Scope: provides an overview of the key investment objectives and success factors along with a definition of the project scope. Section 5 - Model of Care and Service Specification: provides an overview of the current model of care within the hospital and sets out the scope of service provision together with an overview of the proposed new models of care, explaining the process by which they were developed. Section 6 - Workforce Planning: summarises the workforce planning methodology applied for the proposed service changes, the change management policies and supporting training and development needs. Section 7 - Future Service Requirements: sets out the planning assumptions used to derive the associated future capacity and facility requirements and the scale of change from current provision
The Economic Case
Section 8 - Option Overview: sets out the process for identifying the options to be considered within the OBC and the rational for arriving at the shortlist. Section 9 - Option Identification: sets out the options considered to be taken forward to the short list of options appraised. Section 10 - Options Appraisal: summarises the shortlist of options to be appraised. Identifies the benefit criteria used to assess the anticipated non financial benefits and assesses each option against these. Sets out the range of risks considered in relation to the options and the results of the assessment. Presents the economic cost of each of the shortlisted options as well as the overall value for money. Section 11 - Preferred Option: sets out the rationale for the selection of the preferred option along with its key features and anticipated benefits.
Commercial in Confidence
June 2013
Page 3 of 164

Redacted for Publication - see front cover
Reference Design
Section 12 – Reference Design: sets out the summary features of the reference design and the work underlying the estimation of the capital construction costs
The Commercial Case
Section 13 - Procurement Route Assessment: outlines the assessment of the potential procurement routes and sets out the proposed arrangements. Section 14 - Other Commercial Issues: sets out the issues and status for commercial issues outwith the main hospital procurement process e.g. Cresswell wing, site acquisition etc. Section 15 - Proposed Contractual Arrangements: sets out the proposed deal in respect of the preferred way forward.
The Financial Case
Section 16 - Financial Appraisal of Preferred Option: presents a profile of the capital and revenue costs of the preferred option and the associated projected impact on the Board’s income and expenditure as well as a statement on overall affordability. Section 17 – Recurring Revenue: presents the overall affordability position of the Board
Section 18 - Capital Funding: reviews the capital requirements for the project and the enabling works Section 19 Non Recurring Revenue: reviews the funding required on a non recurring basis to support the project Section 20 – Accounting Treatment: sets out the technical accounting issues that arise as a result of the project
The Management Case
Section 21 - Project Management & Project Implementation Timetable: describes how the Board intends to manage the various phases of the project and sets out the proposed timetable and key milestones. Provides details of the governance arrangements and key roles and responsibilities. Section 22 - Managing Successful Delivery: establishes proposed arrangements for change management, benefits realisation, risk management and post project evaluation.
1.6 Further Information 1.6.1 For further information about this Outline Business Case please contact:
Jeff Ace, Chief Executive & Project Owner NHS Dumfries and Galloway Crichton Hall Bankend Road Dumfries DG1 4AP Tel: 01387 272743
Commercial in Confidence
June 2013
Page 4 of 164

Redacted for Publication - see front cover
STRATEGIC CASE
Commercial in Confidence
June 2013
Page 5 of 164

Redacted for Publication - see front cover
2 PROFILE OF NHS DUMFRIES AND GALLOWAY
2.1 NHS Dumfries and Galloway – purpose and objectives
2.1.1 NHS Dumfries and Galloway has a clear purpose, which is
To deliver excellent care that is person centred, safe, efficient, effective, and reliable.
To reduce health inequalities across Dumfries and Galloway.
2.1.2 Underpinning this are a set of outcomes which outline the priority areas the Board will focus on in achieving its purpose. These are:
Improved outcomes for patients that reflect learning from patient experience in order to ensure a person-centred focus is maintained.
Improved staff experience and health and wellbeing of staff.
The delivery of continuous quality improvement and sustainability through services that are effective and efficient.
All children have the best possible start in life through a variety of interventions.
A population in Dumfries and Galloway who are enabled and assisted to have more control over all aspects of their life, health and wellbeing.
2.1.3 In addition to the purpose and outcomes the Board has established a set of corporate objectives which it will use to measure how well it is performing in terms of its purpose and achieving the intended outcomes for its stakeholders. These objectives are set out below.
To reduce health inequalities across NHS Dumfries and Galloway.
To promote and embed continuous quality improvement by connecting the range of quality and safety activities which underpin delivery of the three ambitions of the Healthcare Quality Strategy
person-centred
safe
effective care
To review the model of service delivery across Dumfries and Galloway to deliver person-centred services as close to home as clinically appropriate.
To ensure that NHS Dumfries and Galloway has an engaged and motivated workforce that is supported and valued in order to deliver high quality service and achieve excellence for the population of Dumfries and Galloway.
To maximise the benefit of the financial allocation by delivering clinically and cost effective services efficiently.
Commercial in Confidence
June 2013
Page 6 of 164
Redacted for Publication - see front cover
Continue to support and develop partnership working to improve outcomes for the people of Dumfries and Galloway.
To meet and where possible, exceed goals and targets set by the Scottish Government Health Directorate for NHSScotland, whilst delivering the measurable targets in the Single Outcome Agreement.
2.2 Geography 2.2.1 NHS Dumfries and Galloway serves a population of just over 148,000
dispersed across a large geographical area of approximately 2,400 square miles. The largest town in the region is Dumfries with a population of some 31,600. The two other main towns are Stranraer with a population of 10,800 and Annan, whose population is 8,300. All other settlements have populations of 4,500 or less.
2.2.2 Dumfries and Galloway stretches from Langholm in the East to Drummore in the West, and from Kirkconnel and Carsphairn in the North down to the Solway Coast. The Health Board employs around 4,500 staff excluding independent GPs and Dentists.
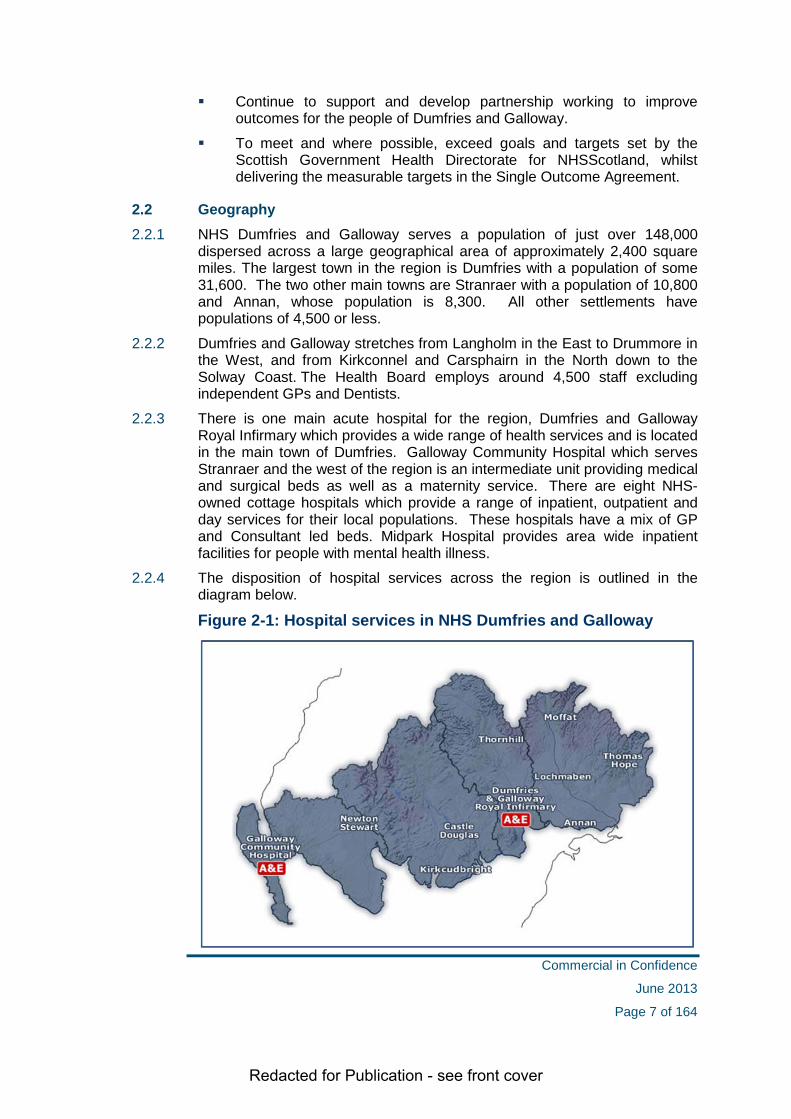
2.2.3 There is one main acute hospital for the region, Dumfries and Galloway Royal Infirmary which provides a wide range of health services and is located in the main town of Dumfries. Galloway Community Hospital which serves Stranraer and the west of the region is an intermediate unit providing medical and surgical beds as well as a maternity service. There are eight NHS-owned cottage hospitals which provide a range of inpatient, outpatient and day services for their local populations. These hospitals have a mix of GP and Consultant led beds. Midpark Hospital provides area wide inpatient facilities for people with mental health illness.
2.2.4 The disposition of hospital services across the region is outlined in the diagram below.
Figure 2-1: Hospital services in NHS Dumfries and Galloway
Commercial in Confidence
June 2013
Page 7 of 164

Redacted for Publication - see front cover
2.3 Demography 2.3.1 Whilst the total NHS Dumfries and Galloway population is expected to
decline from 148,190 in 2010 to 141,500 in 2035, a decrease of 4.5%, current demographic projections show that the over 75 population in Dumfries & Galloway is likely to grow by 77% by 2035. This will mean that the over 75 population in Dumfries & Galloway will increase from under 14,850 in 2010 to 26,291 in 2035. The number of residents aged 90 years or over is projected to increase from around 1,100 to over 4,400 over the same period. This rise in older age groups has considerable importance when planning future health services.
2.3.2 A further important impact of the demographic change will be on the working age population. The working age population (16 to 64) will reduce by 22% from 90,800 in 2010 to 70,608 in 2035. NHS Dumfries and Galloway is a major employer within the region and will compete with other organisations to secure continuity and appropriate staffing levels. It is essential that clinical services are sustainable in the future and that we are able to recruit and retain the necessary skills to deliver the high quality range of services to the population and that we are able to adapt the skills of our workforce to meet the changing healthcare needs.
2.4 Current Services 2.4.1 Health services within Dumfries and Galloway are managed by 7 operating
directorates; Acute Services, Diagnostic Services, Primary and Community Care Directorate (East), Primary and Community Care Directorate (West), Mental Health, Women and Children’s and Operational Services.
2.4.2 Inpatient care is provided across a range of Acute, Community and Cottage Hospital settings as set out in the table below.
Figure 2-2: Inpatient care available at hospital sites
Location Acute Care Intermediate Care
Dumfries and Galloway Royal Infirmary
Thornhill Community Hospital
Castle Douglas Hospital
Kirkcudbright Hospital
Annan Hospital
Lochmaben Hospital
Moffat Hospital
Thomas Hope Hospital, Langholm
Galloway Community Hospital, Stranraer
Newton Stewart Hospital
Commercial in Confidence
June 2013
Page 8 of 164

Redacted for Publication - see front cover
2.4.3 In addition to the above the Board utilises capacity within Allanbank private Nursing Home located in Dumfries which provides a total of 67 beds. Within the home 40 beds are purchased by the Health Board to provide NHS care, 16 beds for older people with dementia or mental health illness, and 24 beds for the frail older person and young people with chronic illness. This care is delivered through partnership with Allanbank and the Health Board. Allanbank plays a key role as part of our overall system approach to bed management and is essentially the cottage hospital for the town of Dumfries.
2.4.4 Secondary acute healthcare services for Dumfries & Galloway are provided primarily on DGRI site in Dumfries. The hospital provides the following range of clinical and associated services:
Figure 2-3: Service provided on DGRI site
Clinical and Support Services
Professional and support services
Anaesthetics Cardiology Care of Older People Clinical Haematology Dental Laboratory Dermatology Diabetes Dietetics Electrocardiogram Emergency
Department Ear, Nose and Throat Gastroenterology General Medicine General Surgery Genito Urinary
Medicine Gynaecology Infectious Diseases Laboratories Neo-natal Care Neurology Obstetrics Oncology
Occupational therapy Ophthalmology Oral Surgery Orthopaedics Orthoptics Orthotics Paediatrics Palliative Care Pharmacy Physiotherapy Radiology Rehabilitation Medicine Renal Care Respiratory Medicine Rheumatology Speech and Language
Therapy Stroke Theatres and
Anaesthetics Urology
Catering Domestic Services Education & Training Estates Maintenance Information
Management and Technology
Linen Services Management &
Administration Medical Physics Patient Administration Portering Sterile Supply and
Decontamination Supplies Procurement Secretarial Services Telephony
Commercial in Confidence
June 2013
Page 9 of 164

Redacted for Publication - see front cover
2.4.5 Inpatient bed numbers as at April 2012 is summarised in the table below. This indicated that DGRI had 358 inpatient beds in use.
Figure 2-4: Analysis of inpatient beds at DGRI (April 2012)
Specialty & Location No of beds
Medicine Acute Medicine – ward 7, 9 &12 87
Medical/Haematology/Gastroenterology/Infectious Diseases – ward 10 30
Rehabilitation/Care of Older People –ward 14&18 50
Sub Total - Medical Specialties 167
Surgery Surgical/Ear, Nose and Throat/Maxilo-facial /Gynaecology – ward 3 & 6 60
Orthopaedics – ward 16 30
Short Stay – ward 4 14
Sub Total - Surgical Specialties 104
Critical Care Intensive Care Unit/Surgical High Dependency Unit/Medical High Dependency Unit 18
Oncology Palliative Care – Alexandra Unit 8
Paediatrics Ward 15 23
Obstetrics Cresswell Wing – Maternity/Birthing Suite/Neo-natal 38
Total number of inpatient beds 358
2.4.6 In addition the Board also provide a range of facilities designated for day case surgery and other day procedures covering a mix of emergency and planned treatments. As at April 2012 there were a total of 44 day beds, chairs and trolleys in DGRI as detailed below.
Figure 2-5: DGRI day case and day treatment facilities in DGRI
Day Procedures / Treatments Number
Day surgery – trolleys 14
Renal Unit - stations 18
Ophthalmology day case 4
Ambulatory care - chairs 8
Total 44
Commercial in Confidence
June 2013
Page 10 of 164

Redacted for Publication - see front cover
2.5 Activity and Performance Clinical activity
2.5.1 The tables below provide an analysis of the Board’s clinical activity across DGRI and other hospital care settings covering:
Inpatient and day cases episodes
Emergency Department attendances
Outpatient consultations
Figure 2-6: Comparison of DGRI hospital activity with Board wide activity by Episode (2009/10 to 2011/12)
Activity type Location
Year 2009/10 2010/11 2011/12
Elective
DGRI 3,731 3,757 3,848
Community / Cottage hospitals 69 56 68
Total 3,800 3,813 3,916
Emergency (includes transfers)
DGRI 18,613 19,093 19,381
Community / Cottage hospitals 2,780 2,639 2,720
Total 21,393 21,732 22,101
Day Case
DGRI 12,031 11,832 11,416
Community / Cottage hospitals 1,631 1,645 1,555
Total 13,662 13,477 12,971
Total
Total DGRI 34,375 34,682 34,645 Total Community / Cottage hospitals 4,480 4,340 4,343 Total Health Board activity 38,855 39,022 38,988
2.5.2 The table above shows that as the main clinical centre DGRI is where the most clinical activity is undertaken. The activity figures also show that the number of emergency admissions at DGRI is increasing year on year. The rate of emergency admissions has been continuing to increase during 2012/13 with emergency inpatients showing an increase of over 6% on the previous year.
2.5.3 Elective activity has remained broadly flat over the period, however, daycase activity has reduced year on year reflecting the fact that more procedures are now being undertaken in ambulatory settings (e.g. outpatient clinics).
Commercial in Confidence
June 2013
Page 11 of 164

Redacted for Publication - see front cover
Figure 2-7: Emergency Department (ED) attendances (2009/10 to 2011/12)
Location Year
2009/2010 2010/2011 2011/2012 DGRI 35,368 35,308 33,542
Galloway Community Hospital 12,795 11,685 11,668
Total 48,163 46,993 45,210
2.5.4 The main factor driving the reduction in ED attendances at the DGRI is the improved flow of GP referrals for admission in-hours direct to the assessment ward, meaning they are not seen in the Emergency Department. In addition a significant amount of work has been undertaken locally to improve the flow of patients through the Emergency Department for example, through the introduction of a Surgical Assessment Unit. A programme of activity has commenced in partnership with our GPs to reduce the use of the Emergency Department by the local population.
Figure 2-8: Outpatient attendances (2009/10 to 2011/12)
Location Year
2009/2010 2010/2011 2011/2012 DGRI 127,388 131,266 138,252
Other locations 57,735 71,120 92,119
Total 185,123 202,386 230,371
2.5.5 As can be seen from the analysis outpatient attendances have increased year on year with the most significant changes being at the non DGRI locations. This reflects the Board’s strategy to deliver more care closer to home where it can be delivered safely and appropriately.
2.5.6 The Board has performed well in relation to the new 12 week Treatment Time Guarantee (TTG), continues to deliver the 18 weeks Referral To Treatment (RTT) standard, has the lowest Did Not Attend (DNA) rate of any mainland NHS Board.
Commercial in Confidence
June 2013
Page 12 of 164

Redacted for Publication - see front cover
Financial performance
2.5.7 The table below shows the Board’s overall financial position for the period 2009/10 through to 2011/12 covering both revenue and capital expenditure.
Figure 2-9: Board financial performance £000
2009/10 2010/11 2011/12
Clinical Service Costs 276,553 274,594 285,684
Non Clinical Service Costs 5,912 5,457 6,571
Net Operating Costs 282,465 280,051 292,255
Less: FHS Non Discretionary Allocation (14,722) (14,990)
(16,003)
Less: capital grants/profit/loss on disposal of fixed assets/annually managed expenditure (3,005) 151
Net Resource Outturn 264,738 265,061 276,403
Revenue Resource Limit 266,966 269,270 278,550
Saving against Revenue Resource Limit 2,228 4,209 2,147 Capital Expenditure 6,418 16,511 18,166
Capital Resource Limit 6,488 16,513 18,267
Saving against Capital Resource Limit 70 2 101
2.5.8 The financial results for NHS Dumfries and Galloway evidence the Board’s ability to continue to achieve positive financial results whilst also delivering increasing activity and improved quality services indicators. The stepped change in financial and projected activity demands will test the ability of the board to continue to deliver against all of its key performance targets. The Board’s services will require to innovate to deliver increased productivity and efficiency to meet the financial challenges.
2.6 Conclusion
2.6.1 NHS Dumfries and Galloway is a health care system that is delivering against key performance targets both clinical and financial.
2.6.2 However, we are clearly facing significant challenges in terms of future demography and changes in disease profiles meaning a considerable redesign is required in terms of models of clinical care in order that the Board can continue to deliver successfully in all of these areas.
Commercial in Confidence
June 2013
Page 13 of 164

Redacted for Publication - see front cover
3 STRATEGIC CONTEXT
3.1 Overview 3.1.1 This section of the OBC sets out the strategic context within which the
changes proposed in this OBC will take place, and covers:
the national context for healthcare developments in Scotland
the local context for developing services in Dumfries and Galloway
3.2 National Context 3.2.1 The national context for the development of health services in Scotland is set
out in a range of policy initiatives, the most relevant of which are:
2020 Vision (September 2011)
The Healthcare Quality Strategy for NHS Scotland (May 2010)
Reshaping Care for Older People: A Programme for Change (2011)
Integration of Adult Health and Social Care in Scotland – Consultation Proposals (Scottish Government, 2012)
State of NHSScotland Assets and Facilities Report for 2012
3.2.2 Further details of each of these is provided in Appendix 1.
3.3 Developing the Clinical Strategy 3.3.1 In reviewing the clinical strategies underpinning the case for the new
hospital, the Board has been clear that it has had to be guided by a number of factors, namely:
• The need to provide accessible emergency services to deal with acute illness or injury.
• The Scottish Government’s “Presumption against centralisation where clinically appropriate”
• Recognition of both the rurality and remoteness of Dumfries & Galloway.
3.3.2 The Board has noted that while a clinical case has been made for centralisation of some differentiated emergency clinical scenarios (such as Optimal Reperfusion of acute MIs in Glasgow, and Acute Vascular Surgery for ruptured aortic aneurysm) the majority of emergency presentations are undifferentiated symptom complexes or injuries, and as such need local resuscitation and support, investigation and initial or on-going management.
Commercial in Confidence
June 2013
Page 14 of 164

Redacted for Publication - see front cover
3.3.3 Having concluded that there was a clear requirement to provide a comprehensive level of emergency services covering major specialities (e.g.: A&E, Anaesthetics, Orthopaedics, General Medicine, General Surgery, Urology, Paediatrics, Obstetrics & Gynaecology, ENT, Ophthalmology and supporting services), the board has significant capacity and capability to provide a range of elective services.
• Provision of elective services locally, where clinically appropriate, was considered to have many advantages:
• Ease of access for patients, and their relatives
• Reduction in healthcare uptake inequalities (research both locally and nationally has shown decreased uptake of more distant healthcare services by the most deprived or older people groups in society – for example, the repatriation of chemotherapy from Edinburgh has significantly increased uptake rates in the west of the region). The age profile of the population of Dumfries & Galloway shows a high and increasing number of older people, and the socio-economic data indicates low and declining average earnings amongst the workforce.
• Best Value: Provision of elective services allows fuller use of facilities and staff who have been arranged to provide emergency services. Our experience of specialist services being delivered outwith Dumfries & Galloway suggests that the contracting out of more routine services would increase costs to the Board
• Public and political acceptability: we recognise the politically sensitive “Presumption against Centralisation”, and the context of the Scottish Government’s “20:20 vision” for Healthcare in Scotland.
• Capacity elsewhere: Initial discussions with potential alternative providers confirmed our concerns that little excess capacity exists to arrange for the re-provision of services elsewhere
• Recruitment and retention: In order to recruit and retain clinical staff to provide emergency services, the local provision of elective services allows us to offer more rewarding and satisfying clinician posts.
• Follow-up: the provision of services locally allows local follow up of acute care episodes.
• Long-term conditions: Scenario planning shows that there is a need for a greater emphasis on the pro-active, structured management of long term conditions: While this is often best delivered by GPs, there is a need for local consultant capacity to support and lead this care.
• Integration: Local delivery of services where clinically possible allows local staff to readily interact with (and eventually integrate with) local authority staff including social work, education, occupational therapy etc.
• Telemedicine support: We are conscious that advances in telemedicine can make delivery of specialist healthcare more accessible locally if there is appropriate infrastructure in place (in
Commercial in Confidence
June 2013
Page 15 of 164

Redacted for Publication - see front cover
terms of staff, facilities and equipment) We have used this to our advantage in for example acute maxillo-facial injuries where linkage from our A&E department to the Southern General Hospital in Glasgow allows us to deliver treatment locally, with the benefit of expert advice. We anticipate that technology may over time mean that more complex expertise may be made available locally if we have sufficient skills and capacity to support its use.
3.3.4 In conclusion, although consideration was given to regional or national delivery of services generally, the Board felt unable to support distant provision of services - except where there was a case to be made on the grounds of clinical safety or improved clinical outcomes (e.g. Neurosurgery and other low volume specialist services) or excessive cost.
3.3.5 Having considered the options for changing the nature and volume of healthcare services the Board took an early decision that the preferred position would therefore be the delivery of the same range of services as at present, with repatriation of some services such as non specialist orthopaedics from Carlisle and Glasgow, and uro-oncology from Edinburgh. This improves patient access and makes efficient use of local capacity.
3.4 Local Context 3.4.1 The local context for the development of services within NHS Dumfries and
Galloway both responds to the national drivers set out above and reflects on other strategies that will support the proposals set out within the OBC. The local context is centred on the following strategic areas, each of which is described in more detail below.
Putting You First
Role of Cottage Hospitals
Financial Context
The Board’s Property Strategy
The Board’s e-Health Strategy
Putting you First
3.4.2 The government’s vision for the integration of health and social care is to address the variability of health and social care outcomes across Scotland. The vision includes making it easier for people to remain in their own homes rather than being admitted to hospital and to get people out of hospital quicker and back to a more homely setting.
3.4.3 The vision will be achieved by promoting joint accountability across health and social care organisations and partnerships and through initiatives such as embedding GPs, other clinicians and care professionals in the process of service planning, investment and provision.
3.4.4 Putting You First (PYF) is a five year Change Programme for Dumfries and Galloway. The aim of the programme is to develop models of service based on the principles of prevention and early intervention in an approach that
Commercial in Confidence
June 2013
Page 16 of 164

Redacted for Publication - see front cover
supports working with partner organisations, communities and individuals. This change programme has to be delivered against the backdrop of the financial and demographic challenges highlighted above.
3.4.5 To meet this challenge, in March 2011 PYF was agreed by the NHS Board as a direction of travel for health and care services in Dumfries and Galloway that supports a broad range of change. It is a partnership approach between Dumfries and Galloway Council, NHS Dumfries and Galloway, the Third and Independent Sectors and working together with individuals, their families and carers and communities: to design, develop and deliver new ways of working that deliver sustainable, high quality services for the future.
3.4.6 PYF will identify and deliver new health and social care services that;
Place people firmly at the centre of the services they receive
Are developed and delivered with people as partners in their own care supported to make their own decisions
Are flexible enough to be able to be responsive to the unique and changing circumstances of someone’s life
Are delivered at or as close to the person’s own home as possible
Ensure staff and partners have or develop the skills and resources necessary to deliver new ways of working.
Become predominantly proactive and pre-emptive in their care delivery taking a prevention or early intervention approach
Promote and deliver one, seamless service of care to the individual
3.4.7 A range of initiatives and work under the Programme is now being supported by the newly established PYF Programme Team. The initial focus for this work is the East of the region with funding available including the national ‘Re-shaping Care for Older People’ Change Fund to support development from a range of sources.
Role of Cottage Hospitals 3.4.8 The local cottage hospitals represent an area of relative underuse in the
recent past: This has been noted in relation to low occupancy rates, relatively high average lengths of stay and a reluctance to admit patients with significant morbidity.
3.4.9 As part of the wider clinical strategy, the Board has determined that Cottage Hospitals should be use as efficiently as possible: This will lead to an increased occupancy rate, a reduced average length of stay, and the development of staff skills to allow patients requiring more complex support and care to be transferred to community hospitals.
3.4.10 The increased activity in cottage hospitals is an integral part of the planned clinical model for the new hospital: We plan that, for many patients, assessment and clinical management planning in the Combined Assessment Unit will be followed by early transfer to their local cottage hospital where treatment and rehabilitation will be progressed. This arrangement:
• Helps to address the demographic challenges of the years ahead
Commercial in Confidence
June 2013
Page 17 of 164

Redacted for Publication - see front cover
• Reduces the number of acute beds needed in the new hospital
• Is popular with older patients
• Ensures effective use of our estate
• Helps maintain “critical mass” in localities, which in turn can support day care, palliative care provision of a range of intermediate and rehabilitation services.
3.4.11 One hospital (Kirkcudbright) has also developed chronic renal replacement therapy services in the form of a nurse-led dialysis unit. This flexibility allowed us to provide new local services to meet increased demand: We anticipate, particularly with developments in telehealth, that there may be further opportunities to develop this service in the East of the Region.
3.4.12 Clinical protocols have been developed for the use of cottage hospitals in a range of clinical scenarios –in particular rehabilitation after acute stroke, rehabilitation after hip fracture and after major joint replacement when required. Work has progressed in terms of ensuring that nursing and allied health professional staff have developed the required skills and competencies to deliver these models of care.
3.4.13 In order to address the potential difficulties associated with delayed discharges a local STARS (Short Term Augmented Rehab Service) has been developed which allows for support of patients in the first few weeks of return home, and have had negotiations with the local authority regarding the increasing need for social care packages. All of these changes are designed to reduce average length of stay, and support early discharge of patients from acute wards in the new hospital to cottage hospitals
3.4.14 A new contract for medical input to cottage hospitals has been agreed to specify the quantity and quality of service to be delivered, and sets a clear clinical governance framework in place. Doctors who provide input will be supported to improve their skills and knowledge, and will be encouraged obtain the Diploma in Geriatric Medicine.
3.4.15 AHP input to the cottage hospital has been reviewed to ensure that a positive re-ablement approach is taken to all patients.
3.4.16 Training, retention of skills, and increase in funded establishment of nursing and AHP staff will have significant resource implications. This will be addressed as part of the organisation’s clinical change programme.
3.4.17 Through the local work being undertaken under ‘Reshaping Care for Older People’ significant partnership work with the Local Authority, 3rd and Independent Sectors, we are assessing innovative ways of supporting older people to remain at home and independent in their communities with the right support. Current work includes testing the use of Care Home beds for ‘step up/step down’ GP-led care and the development of integrated community teams which focus on seamless care and reduction in unplanned admissions.
Commercial in Confidence
June 2013
Page 18 of 164

Redacted for Publication - see front cover
Financial Context 3.4.18 NHS Dumfries and Galloway is committed to a sustainable future through
promoting the values of excellence, improved efficiency, effective team working and clinical improvement allowing it to achieve superior performance and make a distinctive impact over a sustained period of time. The challenging financial outlook for the public sector for the foreseeable future will require fundamental change in the way NHS services are provided and new ways of working to achieve the Board’s objectives.
3.4.19 The Board’s strategy for achieving this is embedded in a number of specific and measurable objectives, many of which are fundamental to the proposals presented in this OBC. These objectives are supported through a number of initiatives designed to deliver higher quality, affordable and sustainable services.
3.4.20 The Health Board’s Financial Strategy evidences the affordability of the OBC for the reprovision of the Acute Care across NHS Dumfries and Galloway. The strategy provides the robust financial context for the Board to progress with this ambitious capital development. The benefits realisation from the investment will focus on the delivery of efficient, sustainable and innovative services able to meet the twin challenges of demography and financial austerity.
3.4.21 The additional investment in services at the front door of the hospital, specifically within the Combined Assessment Unit (CAU), will allow the Board to implement improved management of emergency activity and patient flows. This will result in a reduced requirement for general inpatient beds (arising through a reduction in avoidable admissions, reduced bed days and improvements in length of stay) and improved utilisation of Cottage Hospitals allowing existing resources to be redistributed and / or used more effectively.
3.4.22 The specific nature and impact of these improvements is presented in Sections 5, 6 and 7 of the OBC and the overall financial implications of the proposals captured within the Financial Case.
Property Strategy 3.4.23 The Board’s strategic estate priorities are set out within its Property and
Asset Management Strategy (PAMS), covering the period 2012 – 2022.
3.4.24 Critical to the development of a robust property strategy is the requirement for this to be driven by the Boards Corporate and Strategic aims. The Board’s ambitious programme of service change and modernisation as described in its Clinical Strategy ‘Putting You First’ will require:
Investing in current buildings that have a role to play in delivering the new models of care so that they effectively and efficiently support service delivery.
Investing in new buildings to enable and facilitate the new models of care and service delivery to be fully implemented.
Commercial in Confidence
June 2013
Page 19 of 164

Redacted for Publication - see front cover
Disposing of buildings that are no longer fit for health care purposes and are deemed surplus to requirements.
3.4.25 The PAMS details the requirement to modernise the current Cottage Hospital infrastructure to facilitate the delivery of the revised service model. Significant investment has been made over the past two years to begin the modernisation process. It is recognised that additional investment will continue to be required to ensure the buildings are fit to match the evolving service model. Capital resources will be prioritised as part of future iterations of the Boards PAMS to deliver the clinical change programme
3.4.26 In addition the Board are acutely aware of the need to address improvements in environmental performance and energy management. Both of which are key enablers in improving the quality of the estate and reducing the revenue costs over time.
3.4.27 The Board’s vision and ambitious agenda for change over the next decade simply cannot be achieved without significant change and investment in its estate. The Board has developed a capital investment programme, which taken together will support a major shift in the provision of health care in Dumfries & Galloway. Whilst this investment will be focussed on redesigning and modernising services it must also address the current poor condition and performance of much of the existing estate.
3.4.28 The Property Strategy is aligned to the Annual State of NHSScotland Assets and Facilities Report. This report sets targets for 2020 for estate performance and the development of the new hospital will play a key role in the local achievement of these targets. The KPIs contained within the National Report are reflected through the PAMS and are used to monitor our progress against the targets and to help shape our local investment programme.
3.4.29 This programme involves a 10 year plan that will see significant property performance improvements.
3.4.30 A new District General Hospital would allow many of the property strategy ambitions to be realised. Acute services would be provided in modern, fit for purpose facilities which, when taken with changes in the use of other hospital and community services, would fully support the proposed models of care. Furthermore it would address the significant, and increasing, backlog maintenance liability.
eHealth Strategy 3.4.31 The eHealth Strategy will bring about transformational change:
A single electronic clinical record will improve patient care by making clinical records instantly available to clinical staff thus improving patient safety, clinician productivity and communication with primary care
Electronic prescribing will improve patient safety, allow the automatic incorporation of some treatment protocols, increase formulary
Commercial in Confidence
June 2013
Page 20 of 164

Redacted for Publication - see front cover
compliance, streamline discharge processes and make pharmacy ordering more efficient
Electronic ordering of diagnostic tests will allow rapid access to tests, will ensure that all test results are acted on and reduce duplication of tests
Increased monitoring of patients will be available, along with electronic recording of observations (MEWS Scoring)
Increased use of telehealth – providing out-patient reviews at locations remote from the main hospital without the need for clinician or patient travel
Increased video-conferencing facilities for business and clinical meetings
Enhanced business information to inform real time audit and service planning
Linking of systems with social services systems will increase integrated working – and linkage to primary care will increase safety across the interface of primary & secondary care
Increased electronic handling of all aspects of the business will allow an increase in home working
3.4.32 The strategy and its successful implementation is key to supporting the Board in modernising clinical services and reducing costs. In particular it is anticipated that key benefits will arise through faster access to relevant information (allowing for improved patient safety and more timely delivery of care) as well as increasing flexibility in the way the Board utilises its workforce.
3.5 Conclusion 3.5.1 The Board’s change programme Putting You First sets out the direction of
travel in relation to the provision of services in the future. The focus on partnership working, prevention of admission and support for individuals to remain at home wherever possible is a fundamental requirement of NHS Dumfries and Galloway’s ability to respond to the future financial and demographic challenges.
3.5.2 The Role of the Cottage Hospitals will require to be embedded in the new model of care. Development is underway to ensure that clinical management of patients in the Combined Assessment Unit will be followed by early transfer to the local cottage hospital where treatment and rehabilitation will be progressed
3.5.3 The challenging financial context means that a significant amount of service redesign is required in order that we continue to deliver against our financial and service targets. The significant investment in a new modern fit for purpose District General Hospital provides the Board with a catalyst to redesign our services to ensure they are fit for the future.
3.5.4 The PAMS strategy sets out the Board’s vision for the next ten years in terms of the efficient utilisation of its estate. The delivery of a new District General
Commercial in Confidence
June 2013
Page 21 of 164
Redacted for Publication - see front cover
Hospital will significantly improve the Board’s overall position with regards to a range of performance indicators.
3.5.5 The E-Health strategy will deliver increased productivity by clinical staff, improved safety, better management information and a reduction in the need for medical record storage facilities.
Commercial in Confidence
June 2013
Page 22 of 164

Redacted for Publication - see front cover
4 BUSINESS CASE OBJECTIVES & SCOPE
4.1 Overview 4.1.1 This section of the OBC sets out the criteria used to confirm the objectives
and scope of the project which is set within a defined overall development programme and the case for change.
4.1.2 The content of this section includes:
Conditions for Success
The refinement of the Key Investment Objectives
Confirmation of the scope of the project
A description of existing arrangements
The case for change
4.2 Conditions for Success 4.2.1 The table below sets out the following:
The definitions of success for the redevelopment of acute services
A description of the conditions for success
The data that will enable measurement of progress
4.2.2 The targets are set using a range of measures, some adopting the agreed HEAT targets, others using a range of national averages and upper quartile performance. These targets will be further developed over the next few months and incorporated into the conditions for success/benefits management programme
4.2.3 Subsequently the proposed Models of Care as set out in Section 5 of the OBC outlines how the Board aims to reshape service delivery across the health system as a means of setting out the key changes required to support the performance improvements underpinning the main aims of the OBC. It also establishes the anticipated benefits associated with these changes
Commercial in Confidence
June 2013
Page 23 of 164

Redacted for Publication - see front cover
Figure 4-1: Conditions for Success Theme What does success look like? What are the conditions for delivering success? Measurement of success Current Target
Appropriate alternatives to admission Reduction in rate of 75+ emergency admission bed days (HEAT target)
4746 per 1000 4010 per 1000
Occupancy Rate 68% 80%Reduction in Length of Stay in Cottage Hospitals
19.2 days TBC
Improvement to the transfer or discharge processes to ensure 7 day a week discharge by appropriate healthcare professional
Reduction in average inpatient LOS (Acute) 5.2 days 4.6 days
Availability of AHPs and Social Care over a 7 day periodIncrease in the number of weekend discharges 15.70% 20%
As far as practicable, within the constraints of the current building, to implement the Operational Policy for a CAU, covering both medical and surgical emergency admissions. This will include the review of medical, nursing and ANP staffing support (note, appointment of 2 additional Acute Physicians and the planned training programme for ANP’s)
Increased use of Ambulatory Care
TBC TBC
Rapid availability of diagnostic testing Improved turnaround time for diagnostic tests
TBC TBC
Delivery of 4 hour HEAT target in ED 95% 98%Time to initial assessment in EDTime to treatment to ED
Improvements in pre-assessment pathway Admissions on day of surgery (AODOS) for targetted surgical and endoscopy admissions
95%
Improved theatre utilisation BADS performance 85% 90%
Clinical Performance and Productivity
Reductions in acute hospital length of stay
Increased utilisation of cottage hospitals
Improving the management of emergency care
Improved patient flows through the Emergency Department
Increasing day case rates
Commercial in Confidence
June 2013
Page 24 of 164

Redacted for Publication - see front cover
Theme What does success look like? What are the conditions for delivering success? Measurement of success Current Target
Reduction in SAB rates0.32 per 1000
OBDs0.25 per 1000
OBDs
Reduction in CDI rates
0.34 per 1000 over 65s OBDs
0.25 per 1000 OBDs over age of 15
Reduction in Significant Events
- Central Line Infections2 in last 12mths
Reduce by 50%
- Ventilator associated pneumoniaNo VAP since
Sept 2011 Maintain - Medicines reconciliation compliance (current national guidance is 95%) 98% Maintain
- Reduction in adverse events21 per 1000
OBDs 30% reductionElectronic prescribing
Reduced medication errorsElectronic ordering of diagnostic tests
Reductions in duplicate testsEnhanced monitoring of patients/electronic MEWS recording Monitor reliability of MEWS
99% in Feb 2013 Maintain
Improvements in Clinical EffectivenessIncrease in clinically proven ambulatory care Compliance with Ambulatory Care
DirectoryEnhanced Risk Management System
Reductions in Adverse Events21 per 1000
OBDs 30% reductionImproved patient pathways
Incorporation of evidence based design/ 100% single rooms
Patient Satisfaction Surveys/ reductions in complaints
Ongoing staff involvement in patient workstreams Staff SurveysAwareness Sessions Sickness Absence Rates 4.39% 4%Effective Communication (2-way)Newsletters, BlogsEngage with Staff Side representative (Area Partnership Forum)
‘Non-Smoking’ SiteDevelopment and implementation of local Tobacco Policy in accordance with SG Tobacco Strategy Smoke free site
2 smoking shelters
0 smoking shelters
Clinical engagement in use of telehealth Reduction in patient and clinician travel
Roll out of OCS across all health service properties.Increased percentage of consultations being undertaken electronically
Reduced hospital acquired infection
Rapid and full access to clinical information
Quality Enhancements
Enhanced patient safety
Improved patient experience
Improved Staff Experience
Improved use of telehealth opportunities
Commercial in Confidence
June 2013
Page 25 of 164

Redacted for Publication - see front cover
Theme What does success look like? What are the conditions for delivering success? Measurement of success Current Target
Structured, pro-active management of long term conditions in primary care – closer working with GPs and community nurses identifying and responding to the care planning for relevant patients
Reduced outpatient attendances
Review and reconfiguration of community nursing servicesDelivery of the D&G Carers strategyPrimary care access to full range of investigations e.g. Echocardiograms, ETTs, CT scans,
Reduced outpatient referrals
Increased productivity within community nursing teams Increased face to face contact with patients
Increased identification and support to ‘hidden’ carers
Testing, evaluation and implementation of a range of intermediate care models
Increased Occupancy rates in cottage hospitals to 80%.
68% 80%
Enhanced community based AHP services Implementation of service specification and contractual arrangements for GP input to cottage hospitals
Implementation of appropriate alternatives to admission e.g. HUB initiativeEstablishment of multi-agency, multi-disciplinary teams in the communityImproved integration between general health and mental health nursing and medical staffConsistency in the medical management of patients in cottage hospitalsAppropriate placement and support either in the general setting or the mental health setting. Number of nurses undertaking experiential training
Nil 10 per year
Electronic Case Notes, Electronic Portal, E-Pen, Order Communications,
Improvement in availability of casenotes.
Electronic provision of patient information Reduced spend on administrative processes e.g. medical records/ ward clerks
Paper less service Reduction in adverse eventsGP immediate access to hospital information Reductions in unnecessary diagnostic
tests
Shifting the Balance of Care
Maintaining patients in their own home where clinically appropriate
Enhanced range of community based services
Improvements in information exchange across primary and secondary care
Commercial in Confidence
June 2013
Page 26 of 164

Redacted for Publication - see front cover
Theme What does success look like? What are the conditions for delivering success? Measurement of success Current TargetIncreased energy efficiency Ensuring the design and construction of an energy
efficient buildingAchievement of a stretch target of 35 gigajoules per 100m3 against current guidance of 43 Gigajoules per 100m3
65 Gj per 100m3
35 Gj per 100m3
Elimination of current backlog maintenance at DGRI by disposing of site
SAFR target rate of backlog maintenance of no more than £100 per m2
£850 per m2 £100 per m2
Delivery of improved physical condition Achievement of 90% performance target for Category A or B condition
23% 90%
Delivery of improved functional suitability Achievement of 90% performance target for Category A or B condition
34% 90%
Delivery of improved estate quality Achievement of 90% performance target for Category A or B condition
22% 90%
Delivery of Improved space utilisation 90% ‘fully utilised’ performance target 28% Note: 69% is
catergorised as overcrow ded
90%
Achievement of BREEAM Excellent rating
N/A Excellent
Achievement of E8 HEAT target Achieved Maintained
Estate Performance
Delivery of a new fit for purpose facility
Achievement of SAFR 2020 target
Improved environmental performance and sustainability
Commercial in Confidence
June 2013
Page 27 of 164

Redacted for Publication - see front cover
Theme What does success look like? What are the conditions for delivering success? Measurement of success Current TargetProcurement Programme of 83 weeks achieved
N/a 83 weeks
Project delivered within affordability limits and timescale
N/a £6.7 milliuon as per OBC
Cost-effective and efficient building Ensuring a whole life costing approach is undertaken Energy efficiency targets achieved TBC TBCMeeting financial targets Achievement of CRES targets Continuing to meet the 3 LDP financial
targets of RRL, CRL and cash management
Achievement of Financial
Targets
Achievement of Financial
TargetsRobust Workforce Planning Clarity of Models of Care and workforce implications Delivery of new service models within
redesigned workforce plan.£99.643m per
OBC£106.351m (baseline +
£6.7m additional D&G
investment
Financial Stability
Efficient procurement Implementing conditions prescribed by SFT funding letter
Commercial in Confidence
June 2013
Page 28 of 164

Redacted for Publication - see front cover
4.3 Key Investment Objectives 4.3.1 The investment objectives have been ranked in order of importance and are
summarised below.
Figure 4-2: Investment Objectives
Ref OBC - Key Investment Objectives
1 Clinical Effectiveness & Sustainability: to ensure the Board provides services which are clinically effective and sustainable over the long term e.g. 30+ years.
2 Physical Environment: to facilitate the provision of services in a high quality environment which is ‘fit for purpose’ for staff, patients and visitors.
3 Capacity & Demand: to ensure the Board can respond to the demand for inpatient, day case and outpatient services.
4 Delivering models of care in line with the developing clinical strategy: to ensure that secondary care services facilitate joint planning in the development of patient focussed services, in a primary and community setting.
5 Access: to maximise access to hospital services for the local population.
6 Performance & Efficiency: to ensure the hospital is developed in such a way as to maximise performance and improve efficiency.
7 Recruitment, retention of staff and students: to ensure the Board is able to recruit and retain highly skilled staff to support the delivery of high quality patient care.
4.3.2 The objectives were then further developed and made SMART and now include baseline data against which the planned improvements can be assessed. The more detailed SMART objectives were agreed and are set out in Appendix 2.
4.4 Project Scope 4.4.1 The OBC covers the provision of a new District General Hospital which by
definition incorporates all of the services currently being provided in DGRI with the exception of:
Chronic Renal Services
Ophthalmology Services
A limited range of outpatient services
Commercial in Confidence
June 2013
Page 29 of 164

Redacted for Publication - see front cover
4.5 Existing Arrangements 4.5.1 Services provided from DGRI have changed and developed significantly since
the hospital was commissioned in 1975. That process of change continues and a wide range of departmental refurbishments have been completed.
4.5.2 Key changes have included the addition of a Maternity Wing providing beds and cots and a Day Surgery Unit, procured through a PFI agreement in 2001. The agreement has 19 years left to run. In light of these factors it is fully anticipated that this facility would be retained by the Board as a means of supporting the delivery of clinical services.
4.5.3 During this same time the hospital’s fabric and infrastructure have been subjected to sustained use. Physical condition survey work indicates that the hospital is no longer fit for purpose and would not support delivery of the required models of care.
4.5.4 As the models of service delivery change, with an increased focus on the need to provide person centred, safe and effective healthcare, it is necessary to ensure that the most appropriate treatments, interventions, support and services are provided at the right time to everyone who will benefit. It is therefore essential that the configuration of services supports the optimal patient experience, reduces unnecessary delays and allows resources to be used in the most effective manner. In many instances the current facilities can act as a barrier to ensuring that these requirements are met.
4.5.5 Demographic forecasts indicate that the number of older people in the local population will continue to rise. This will put increased pressure on acute services, particularly unscheduled care, including those for older, physically ill patients who also suffer from confusion or dementia, not only at DGRI but also in community and primary care settings.
4.5.6 As a result of these changes over time, the layout and design of the hospital ward environment inhibits the opportunity to fully deliver the quality ambitions.
4.5.7 It is the aim of NHS Dumfries and Galloway to provide the highest standard of facilities possible for patients and a significantly improved working environment for staff. The case for change section sets out the key drivers for change and explains the rationale for the development of new hospital facilities.
4.6 The Case for Change 4.6.1 The case for change is based on four key issues, namely:
The ambition to deliver National Policy such as 2020 vision, the Quality Strategy and Reshaping Care for Older People and to facilitate the delivery of local initiatives such as Putting You first.
The need to be able to respond to and manage future demographic change. The demographic change impacts on the ageing population, their health needs and the resulting increased demands (including unscheduled care) being placed on the local health system. In parallel, the demographic change also impacts on the workforce availability for the future.
Commercial in Confidence
June 2013
Page 30 of 164

Redacted for Publication - see front cover
Modernisation of services which focus on quality and clinical effectiveness is required.
Backlog maintenance and the lack of functional suitability of current DGRI facilities. There is also the need to improve the patient and staff environment in order to be able to modernise service delivery and meet targets and objectives.
4.6.2 Further details and analysis of each of these is provided below.
National Policy 4.6.3 The Board is committed to achieving the goals set out in key national policy
initiatives as outlined in Section 3.2. Delivering improvements in the way care is provided by implementing new service models which improve the quality of patient care and make more effective use of scarce resources.
4.6.4 In particular the NHS Scotland Quality Strategy places significant emphasis on the need to respect individual needs and values and which demonstrate compassion, continuity, and clear communication and shared decision-making. Furthermore it stresses that there be no avoidable injury or harm to people from the healthcare they receive, and an appropriate, clean and safe environment will be provided for the delivery of healthcare services.
4.6.5 Additionally it emphasises that the most appropriate treatments, interventions, support and services will be provided at the right time to everyone who will benefit, and wasteful or harmful variation will be eradicated.
4.6.6 The current arrangements in terms of service models and physical configuration at the DGRI present significant barriers to ensuring that these requirements are addressed. This significantly impacts on the patient experience, causes delays in treatment and resources to be used ineffectively.
Demographic Change 4.6.7 As outlined in paragraph 2.3 of the OBC, NHS Dumfries and Galloway is facing
some significant challenges in relation to changing demography. Trend data showing anticipated changes in population between 2010 and 2035 from the General Register Office for Scotland (GROS) statistics is shown in the diagram below. This shows that the over 75 population in Dumfries & Galloway is likely to grow by 77% by 2035. Within the over 75 population the number of residents aged 90 years or over is projected to increase from around 1,100 to over 4,400 over the same period. This rise in older age groups has considerable importance when planning future health services.
Commercial in Confidence
June 2013
Page 31 of 164

Redacted for Publication - see front cover
Figure 4-3: GROS population projections 2010 to 2035
4.6.8 A further important impact of the demographic change will be on the working age
population. The working age population (16 to 64) is reducing by 22% from 90,800 in 2010 to 70,608 in 2035. NHS Dumfries and Galloway is a major employer within the region and will compete with other organisations to secure continuity and appropriate staffing levels. It is essential that clinical services are sustainable in the future and that we are able to recruit and retain the skills of our workforce to deliver the high quality range of services to the population.
4.6.9 Looking at our workforce needs and planning for the future has been a central component in developing this OBC. We have recognised that we need to plan career structures that will enable individuals to progress within their chosen field and that we have innovative approaches to career development in Dumfries & Galloway. This will encourage young people to stay in the region to develop a career within the NHS but also to attract and retain staff and skill into the region. Part of our ambition through this OBC is to provide targeted employment opportunities for community benefits throughout Dumfries and Galloway e.g. Modern Apprenticeships.
Modernising Clinical Services 4.6.10 Reviewing the way we deliver clinical services is constantly subject to
reassessment and improvement. This recognises the introduction of new methods of treatment, especially drugs but also the impact that new technology can have in the way healthcare can be delivered. The case for change however, goes beyond the need to respond to new drug regimes or new treatment techniques. It must go to the heart of the population change and the change in the types of care that people will need in the future. It is therefore not appropriate to develop services in a piece meal or incremental fashion but to look at clinical services as a whole and set out a clear strategy for the future.
Commercial in Confidence
June 2013
Page 32 of 164

Redacted for Publication - see front cover
4.6.11 A number of individuals are more likely to have a long term condition which means that the NHS must change the focus of services from episodic care delivered in acute district general hospitals to one of co-ordinated long term care. This involves a move towards integrated care pathways between primary, community and acute care which maximise support for self care and self management whilst developing anticipatory care approaches to prevention and management of these long term conditions. This requires a shift from acute district general hospital care to a greater emphasis on primary and community care.
4.6.12 In addition to acknowledging this shift from episodic care to long term care, it is also important to recognise that those who require inpatient care should receive the best care possible in the most appropriate environment. As part of modernising clinical services there is a clear shift in care provision that supports rehabilitation as locally as possible but allows the experts to work in teams that will support improved outcomes and greater independence for individuals as they return to normal living.
4.6.13 This will require both improved acute hospital facilities and a network of intermediate care facilities (Community and Cottage Hospitals) throughout Dumfries & Galloway that will support local care. These intermediate care facilities will also provide a base for integrated community care teams who will deliver a range of care and support to individuals in their own home and in their own community.
4.6.14 The development of a new District General Hospital will enable the Board to implement a number of new models of care for adult acute emergency care and ambulatory care / 23 hour care. As part of wider system changes it will also support the shifting of care from acute into community and primary care settings with particular focus on improving care for older people. Further details regarding these models are provided within Section 5.
Condition of DGRI Estate
4.6.15 This section of the case for change focuses specifically on the physical condition, energy efficiency, DDA compliance, functional suitability, the quality of the environment and space utilisation of the current hospital facilities.
Physical condition 4.6.16 Commissioned in 1975, DGRI was a purpose built facility on the southern side of
Dumfries town centre. Within the limits of the funding available the accommodation has been well maintained since commissioning. To rectify building and design defects discovered in the 1980s the ward block was strengthened structurally and enclosed in aluminium rain-screen cladding in the early 1990s. New windows were installed in the ward block at the same time.
4.6.17 Most building and engineering services are as fitted in the early 1970s and have reached the end of their useful life.
Commercial in Confidence
June 2013
Page 33 of 164

Redacted for Publication - see front cover
4.6.18 A full physical condition survey was undertaken from November 2003 to January 2004. The results were risk assessed and reviewed in October 2007, and again, more recently, as part of a review of backlog maintenance as part of the development of the Board’s Property and Asset Management Strategy (PAMS).
4.6.19 The most recent assessment of estate condition identifies the majority of the main DGRI site (77%) as falling into category C i.e. poor condition with evidence of major defects. In terms of backlog maintenance the risk profile of the current DGRI estate shows that 44% falls into the high / significant risk category with 37% at medium risk and only some 19% being classified as low risk.
4.6.20 The services in the wards have reached the end of their operational life e.g. nurse call, medical gas systems, electrics, water systems etc.
4.6.21 The existing DGRI is not designed in a way that promotes energy efficiency. The building energy certificate states that the hospital has been assessed and rated as ‘G’ which is the poorest rating
4.6.22 The impact of poor energy performance has resulted in rising energy costs.
Functional suitability, quality of the environment and space utilisation 4.6.23 Since the opening of the DGRI in 1975, there has been a steady growth in the
range and scope of specialist services offered to patients in Dumfries & Galloway. Additional consultants have been appointed in a number of specialities. The range of consultant-managed services provided locally has equally been extended and now includes services such as Oral Surgery, Renal Services and MRI services.
4.6.24 To accommodate some of these services, not all of which use beds intensively, changes have been made to the hospital’s layout and the original 424 inpatient beds at DGRI have been reduced to the present complement (which includes the beds and cots in the Maternity Unit located in the Cresswell Wing of the hospital). Services have been levered into the existing building in pragmatic ways that, despite best efforts, have not always offered the ideal design or clinical adjacencies in which to undertake clinical practice.
4.6.25 Service development has also affected the use of accommodation. Some services have substantially outstripped the space available leaving them to work in cramped conditions whilst changes in clinical practice have also rendered some working spaces functionally unsuitable.
4.6.26 The most recent assessment of functional suitability shows that the vast majority of the main DGRI site falls into category C i.e. not satisfactory (66%). Similarly, the Quality Assessment establishes that 78% of the building falls within Category C.
4.6.27 In terms of space utilisation, only 3% of the building is classed as being underutilised and significantly, 69% is classed as overcrowded.
4.6.28 As clinical services have modernised and developed, they have often had to find additional accommodation to support the service. In a number of specialties this has further fragmented services and clinical adjacencies have been
Commercial in Confidence
June 2013
Page 34 of 164

Redacted for Publication - see front cover
compromised. For example, ICU and HDU are located on different levels. Another example is the remoteness of the Medical Assessment Unit (located on the second floor) in relation to the Emergency Department (which is located on the ground floor of the hospital).
Fragmentation of services 4.6.29 As clinical services have modernised and developed, they have often had to find
additional accommodation to support the service. In a number of specialties this has further fragmented services as the additional space is in a remote location from their current area. This means service provision is fragmented and split between two locations within the hospital. Examples of this include:
Paediatrics – originally located in the main OPD. Following a change in legislation which required separation of adult and children’s services, paediatric outpatients was moved outwith the main OPD and into the paediatric ward. There is however inadequate capacity in the ward to support all clinics so some remain within OPD.
Cardiology - currently Cardiology Services are split, with clinics also taking place in Crichton Royal Hospital.
4.6.30 In addition to departments outgrowing their existing / available accommodation, clinical services have developed and the most appropriate models of care have changed significantly. Clinical adjacencies are poor in many areas. For example, ICU and HDU are located on different levels. Another example is the remoteness of the Medical Assessment Unit (located on the second floor) in relation to the Emergency Department (which is located on the ground floor of the hospital).
Appropriate room sizes 4.6.31 In addition to the above challenges, a significant proportion of the current estate
does not meet minimum Health Building Note (HBN) guidance in terms of recommended minimum room sizes, which means in some areas clinical services are provided in relatively cramped conditions.
4.6.32 The wards were built to the space standards of 30-40 years ago and so no longer meet current space standards. There is insufficient space for the use of lifting aids in bedrooms or bathrooms, nor are there adequate single rooms or isolation facilities. Overall there is much less support accommodation than in comparable modern wards; for example, office space is limited as is storage, interview facilities and staff locker space.
Commercial in Confidence
June 2013
Page 35 of 164

Redacted for Publication - see front cover
Ensuite single inpatient rooms 4.6.33 The existing wards were designed with patient bedrooms organised as 4 bedded
rooms or as single bedrooms. The general arrangement was for 6 single rooms per 30 bedded ward. This gave a proportion of single rooms over the three floors of some 22% at the time when building was originally commissioned.
4.6.34 The single rooms have en-suite facilities that are significantly smaller than current guidance resulting in operational difficulties
4.6.35 The inpatient bed complement has been reconfigured/ adapted over recent years. This has resulted in a reduction in the proportion of single rooms which greatly reduces bed flexibility and has an impact on the Board’s ability to optimally manage outbreaks such as the Norovirus.
4.7 Implications of not providing a new District General Hospital 4.7.1 Modernising health services in Dumfries and Galloway could not be achieved
without investment in a modern, acute facility.
4.7.2 Failure to invest in a new DGH will lead to an inability to:
Fully and efficiently implement the new models of care for Emergency Care, Care of Older People, Theatres and Endoscopy and Critical Care.
Provide improved privacy and dignity for inpatients, and the improved management of HAI, by increasing the number of single en-suite inpatient rooms.
Address the current estate issues of:
The general poor physical condition of the building and engineering services which are at the end of their useful life
Fully complying with the DDA
Improving space utilisation
Improving the functional suitability of accommodation
Improving the quality of the physical environment
Fragmentation of clinical services
Providing improved and more appropriate room sizes for clinical services in line with current and pending future SHBN guidance
Improving energy efficiency
Commercial in Confidence
June 2013
Page 36 of 164

Redacted for Publication - see front cover
4.8 Conclusion 4.8.1 The Conditions for Success have been developed and appropriate measures
identified to ensure their delivery. Within the case for change, there is a requirement to address both the national policy drivers and the local initiatives combined with a changing demography, a changing disease profile and a planned change to the models of care.
4.8.2 The provision of a new DGH will support the Board in the delivery of its Property and Asset Management Strategy and contribute significantly to the achievement of the performance targets set out in the national ‘Annual State of NHS Scotland Assets and Facilities Report’.
Commercial in Confidence
June 2013
Page 37 of 164

Redacted for Publication - see front cover
5 MODEL OF CARE AND SERVICE SPECIFICATION
5.1 Overview 5.1.1 This section of the OBC outlines the work undertaken to develop the proposed
models of care developed as part of the project. The areas presented cover the following:
The scope of service provision
The principles and process for developing the models of care
The proposed model of care for key areas, namely:
Emergency Care, including a Combined Assessment Unit (CAU)
Care of Older People
Theatres / Endoscopy / Day Surgery / 23 Hour Care
Critical Care
5.2 Scope of Service Provision 5.2.1 The services that will be provided from the new District General Hospital
incorporates all of the services currently being provided in DGRI with the exception of:
Chronic Renal Services
Ophthalmology Services
A limited range of outpatient services
5.3 Principles and Process in Developing the Models of Care 5.3.1 The principles applied in developing the models of care focus on the following:
Best clinical practice
Providing care in the most appropriate setting
Co-ordinated delivery of care with partner organisations
Providing seamless patient pathways
Patient quality and experience
5.3.2 In terms of process, clinical briefing documents / operational policies have been developed for each clinical discipline. They describe how services are currently delivered, identify service trends, describe future models of care and outline operational requirements. They are critical to the procurement process since they:
Describe how services are delivered currently, including deficiencies, constraints and future aspirations
Commercial in Confidence
June 2013
Page 38 of 164

Redacted for Publication - see front cover
Identify how services will change between the planning and commissioning phase of the new facility
Describe how services will operate in future (model of care), including changes to workforce requirements
Detail the space required to efficiently deliver new services
Make assumptions about clinical performance and the revenue implications of redesigned clinical services
Incorporate key information that will inform bidders during Competitive Dialogue
5.3.3 The clinical brief/operational policy documentation for the Acute Services Redevelopment Project was developed through a structure, consisting of work streams and work groups.
5.3.4 Between February and May 2012, three meetings of each work stream were held to progress service planning and ensure that future service needs were defined and agreed.
5.3.5 A “cross check” week of meetings in June 2012 ensured integration of workstream plans. Discussions during “cross-check” week generated helpful discussion and a list of issues that required to be clarified as they related to facility planning and workforce matters.
5.3.6 Further meetings of the workstreams took place between October 2012 and February 2013 to refine the clinical briefing documents, develop the proposed models of care and agree the schedules of accommodation.
5.3.7 The development of Acute Services has been a standing item on the agenda of the GP sub-committee, the Primary and Community Care Management Board and the Hospital Management Board. Regular presentations have been made to the Area Partnership Forum, Area Clinical Forum and Performance Committee.
5.3.8 The Board has incorporated comments and advice from primary care in developing plans for the acute hospital.
The Clinical Lead in Primary Care who is a practising GP in the region has been a member of the project team developing the OBC, attending twice weekly meetings.
The Chief Executive and the Medical Director hold regular evening meetings with GPs – held in each of the four localities on a regular basis. These informal meetings, with approximately 12 GPs at a time, provide an effective basis for feedback from GPs.
Commercial in Confidence
June 2013
Page 39 of 164
Redacted for Publication - see front cover
5.4 Proposed Models of Care 5.4.1 Analysis of future demographics illustrates that there will be greater demands on
the social and healthcare systems. There will also be a potentially reduced workforce to provide the traditional models of care. It is important therefore to establish new models of care to address this challenge.
Key areas for redesign have been identified and include:
Emergency Care (Combined Assessment Unit, Emergency Department and Out of Hours)
Care of Older People
Theatres/ Endoscopy/ Day Surgery/ 23 Hour Care
Critical Care
5.4.2 The overarching principle is to reduce the rate of increase in acute hospital admissions while ensuring that those who require admission can be seen, fully investigated and treated as quickly as possible. Clinically necessary services will be available over a 24/7 period and must support a seamless patient pathway across primary and secondary care.
Emergency Care 5.4.3 Currently NHS Dumfries and Galloway emergency services (i.e. Accident and
Emergency; the Medical Admissions Unit (MAU) and the Out of Hours Service operate as three separate units. The majority of GP referrals go directly to the MAU. Some patients are admitted directly to specialty areas during limited hours e.g. stroke unit is restricted to a 09:00 to 17:00 hours of service.
5.4.4 The lack of a surgical assessment unit means that surgical patients presenting in the Emergency Department experience a different pathway and this can result in significant delays.
5.4.5 Throughput and length of stay within MAU is variable and the layout of the unit and the lack of single rooms does not lend itself to person centred care, particularly at periods of peak activity.
5.4.6 The new hospital will create a cohesive Emergency Centre which operates as a “front and back door facility”, with a focus on “decide to admit” rather than “admit to decide”.
5.4.7 There will be increased ambulatory care supported by senior medical review and rapid access to diagnostics. Therefore it is anticipated that a significant percentage of presentations at the CAU will not result in the patient being admitted to the general wards.
5.4.8 The CAU will comprise 32 beds and 10 assessment trolleys. The anticipated length of stay within the unit will be less than 48 hours. The concentration of senior skilled staff in the Combined Assessment Unit will ensure early proactive
Commercial in Confidence
June 2013
Page 40 of 164

Redacted for Publication - see front cover
management of patients which has been shown to reduce average length of stay and improve safety.
5.4.9 The close adjacency of the CAU and Emergency Departments, with co-location of staff, lends itself to much more flexible team working across the Emergency Centre.
5.4.10 Allied Health Professionals and Social Work staff will be based in the Emergency Centre, to contribute to early assessment and support effective discharge planning.
Pathways of Care for Older People 5.4.11 We recognise the pressures that will be created from a rising number of older
patients who will have co-morbidities. The Board in partnership with Social Services is developing rapid response services to maintain older patients at home whenever possible. When admission is required, our aim is to minimise the length of stay as this leads to less functional decline in older patients.
5.4.12 Older people are often admitted to hospital due to lack of adequate alternative services in the community. Dumfries and Galloway is developing an Intermediate Care model which both supports the reduction of avoidable admissions and facilitates timely discharge from acute settings. The development of multi-disciplinary and multi-agency teams across primary and secondary care, working together to bridge the gap, will ensure that the patient’s journey is safe and effective.
5.4.13 Projections predict a significant increase in the proportion of older adults suffering from dementia. Older people with dementia have more functional decline, increased admission to care homes and higher mortality rates. It is also recognised that older people with significant physical disease are at greater risk of co-existent psychiatric morbidity. Future modelling of service provision will ensure improved working between mental health and acute services.
5.4.14 A number of Intermediate Care models are being implemented via the “Putting You First” programme and established work streams. The models are being developed with a focus on ensuring sustainability. An example is the ‘Hub’ initiative in Dumfries which provides a single point of contact to a multi-disciplinary, multi-agency team. This will reduce avoidable admissions to acute services and support earlier discharge. If, on assessment, the individual does not require acute medical care alternative community based services will be provided.
5.4.15 The cottage hospitals within Dumfries and Galloway will provide a greater role in intermediate care. This is being achieved by enhanced medical input to the cottage hospitals, extended training for nursing staff and increased availability of AHP staff. This will increase patient flow through the generic wards in the acute hospital and deliver care within an environment which is closer to the patients’ home.
5.4.16 The development and implementation of intermediate care services is key to the successful delivery of the overall model of care. Without this, we will be unable
Commercial in Confidence
June 2013
Page 41 of 164

Redacted for Publication - see front cover
to address the challenge of increasing demands on health and social care as a result of changing demographics and needs.
Theatres / Endoscopy / Day Surgery / 23-Hour Care 5.4.17 During the planning for Theatres / Endoscopy / Day Surgery / 23-Hour Care
services a wide range of factors were identified which will impact on future requirements. These include but are not restricted to:
The impact of the Bowel Screening Programme increasing demand for colonoscopy
The impact of Joint Advisory Group recommendations regarding endoscopy
Decontamination Guidelines – need for improved decontamination areas Changes to waiting time regimes/targets Increasing day case and 23 hour care activity Changes/developments in technology and clinical practice e.g. increased
interventional radiology in the management of vascular disease Further development of Enhanced Recovery processes after surgery Strategic reviews of a number of services on a supra-regional basis, most
notably vascular surgery Re-patriation of activity from other hospitals e.g. Orthopaedic activity from
the Golden Jubilee Hospital CSSD remaining on the existing site
5.4.18 Services at Dumfries and Galloway Royal Infirmary are currently delivered from six locations:
Main Theatre (6 theatres, including emergency theatre) Ophthalmology Unit (1 theatre) Obstetrics Unit (2 theatres) Day Surgery / Endoscopy Unit Out-patients, where sigmoidoscopies are carried out 23-hour, from Ward 4 (previously an in-patient ward). Ambulatory care is
also delivered from this ward
5.4.19 Within the new hospital all of these services, with the exception of ophthalmology day case, will be provided from one location, thereby increasing efficiency and productivity:
Main Theatre (8 theatres, including emergency and obstetric theatres) Endoscopy (4 suites, with endoscopy decontamination facility) Day Surgery and 23-hour Unit
Commercial in Confidence
June 2013
Page 42 of 164

Redacted for Publication - see front cover
5.4.20 All of these will be located to ensure that the overall endoscopy and surgical journey for patients is optimised.
5.4.21 The key principles of our proposed Model of Care are to:
Improve all surgical and associated journeys through a re-design of processes, services, staffing and accommodation. This will be achieved with improved pre-assessment, admission on day of surgery (AODOS) for a minimum of 95% of all surgical and endoscopy admissions. Our BADS (British Association of Day Surgery basket of procedures) day case rates are currently 82%, against the national BADS score of 81.5%; we will be working towards improvement to a local 90% target for all day cases.
Minimise duplication of effort and resources through improved physical adjacencies.
Reduction in journey times within the operating department/endoscopy/support areas and between these and related areas including surgical wards and critical care.
Critical Care 5.4.22 Critical Care Services at Dumfries and Galloway Royal Infirmary are currently
delivered from three locations:
Intensive Care Unit (ICU) - 4 beds level 3 or 6 beds level 2 Surgical High Dependency Unit (SHDU) 4 beds Medical High Dependency Unit (MHDU) - 8 beds
5.4.23 ICU is located on the ground floor next to theatres, with MHDU and SHDU on the 2nd floor. Level 3 patients are cared for in ICU. Level 2 patients are cared for in the High Dependency Units.
5.4.24 Having three separate critical care/high dependency units within DGRI presents challenges in that it reduces nursing flexibility across these areas and is not conducive to team working.
5.4.25 Currently, Level 1 patients are nursed both in HDU and on the general wards. We will develop nursing skills and competencies across the hospital to increase the number of Level 1 patients being cared for in the general wards where appropriate.
5.4.26 The ICU (Level 3) is staffed to a minimum ratio of 1 nurse to 1 patient throughout the 24 hour period and led by Consultant Anaesthetists with intensive care skills. This is a “closed unit” model: admissions are decided by the intensive care team who are the primary care providers with some input from other specialties.
5.4.27 The HDUs (Level 2) have a minimum of 1 nurse to 2 patients throughout the 24 hour period. Patients within HDU remain under the care of their Consultant Surgeon or Physician. The units are supported by anaesthetists as required. This is an “open unit” model.
Commercial in Confidence
June 2013
Page 43 of 164

Redacted for Publication - see front cover
5.4.28 The key principles of our proposed Model of Care are to:
Provide a co-located / combined unit with 17 beds, encompassing ICU, SHDU and MHDU resulting in increased productivity.
Allow considerable pooling of expertise and economies of scale whilst improving quality. This will also maximise use of a scarce workforce.
Implement the preferred closed model, under the management of the anaesthetists in terms of admission and discharge. This model will be vital to ensure equitable use of beds and to provide dedicated medical staff input over the 24-hour period.
Provide shared support areas.
5.5 Service benefits of the new models of care 5.5.1 The anticipated benefits arising from the proposed new models of care include:
Patients will be cared for in the most appropriate place, which may be their own home, by the most appropriate team
Improved person-centred, quality care for all patients tailored to meet identified, individual need
Integrated and adjacent services which span the patient’s pathway Steps within the patient’s pathway are clearly defined Increased efficiency by maximising the potential of all available resources Increased resilience to fluctuating demand in different units Improved clinical outcomes through standardisation and consistency of
practice delivered by dedicated, integrated teams Older people will not be admitted to acute beds unless medically necessary
as there will be greater utilisation of cottage hospitals coupled with the provision of appropriate, proactive, alternative services nearer to or in their own homes
Integration of health and social services will ensure that the associated demographic needs, both from a clinical and care perspective are met within the constraints of combined budgets
Reduction in the number of avoidable admissions and an overall reduction in occupied bed days
5.5.2 We will track the delivery of these benefits by measuring performance against the indicators highlighted in section 4.2 – “Conditions for Success”.
5.6 Clinical and Design Briefs 5.6.1 The clinical brief/operational policy documentation and the resulting models of
care have been used to develop a design brief for the project. This translates the outputs into a set of guidelines that are used to develop the layout of the departments.
5.6.2 This ensures that the principles of the models of care are embedded into the developing proposals for the new facility. These are built around the patient
Commercial in Confidence
June 2013
Page 44 of 164

Redacted for Publication - see front cover
pathway and informed by staff, who will be working within the services, thus ensuring that the process is person centred.
5.6.3 Clinical and design briefs are available on request.
5.7 Conclusion 5.7.1 The changes described above will deliver benefits in patient care, safety and
clinical productivity. The models of care support the delivery of the NHS Board’s vision of shifting the balance of care.
Commercial in Confidence
June 2013
Page 45 of 164

Redacted for Publication - see front cover
6 WORKFORCE PLANNING
6.1 Overview 6.1.1 NHS Dumfries and Galloway utilises the National Framework of the 6 Steps
methodology to support its workforce planning processes. This ensures a consistent, practical approach to the development of workforce plans. The 6 Steps are summarised as follows:
Defining the plan Mapping service change Defining the required workforce Understanding workforce availability Developing an action plan Implementing, monitoring and refreshing the plan
6.1.2 The three key principles within the above steps are affordability, availability and adaptability.
6.1.3 A number of national drivers impact on our approach to workforce planning.
The 20:20 Workforce Vision The Healthcare Quality Strategy for NHS Scotland (2010) Reshaping Care for Older people: a programme of change
6.1.4 Integration of Adult Health and Social Care in Scotland – Consultation Proposals (Scottish Government, 2012).Other significant factors which will shape the workforce in the future include a number of specific regulatory and policy drivers such as the European Working Time Directive and the impact of Modernising Medical Careers and Reshaping the Medical Workforce Project.
6.1.5 The local demographics for Dumfries and Galloway demonstrate that by 2035 the projected population will be 141,500. This is a decrease of 4.5% on the 2010 population. The working age population (16-64) will reduce by 22% from 90,800 in 2010 to 70,608 in 2035. Both the NHS and the Local Authority, as the two largest employers in the region, will be competing for this reduced pool of potential employees.
6.1.6 The integration of Health and Social Care is designed to reduce duplication and make best use of the available workforce.
Commercial in Confidence
June 2013
Page 46 of 164

Redacted for Publication - see front cover
6.2 Current Staffing Position 6.2.1 A summary of the in post establishment is shown below.
Figure 6-1: Current staffing by staff group (WTEs) at Dec 2012
Staff Group DGRI NHS D&G
Administration and Clerical 212.53 549.35
Allied Health Professionals 126.26 247.07
Healthcare Sciences 94.07 98.27
Medical and Dental Support 5.18 15.88
Medical and Dental 223.24 291.81
Nursing and Midwifery 771.70 1758.54
Other Therapeutic 40.22 87.00
Personal Social Care 0.00 19.26
Senior Managers 2.59 23.59
Support Services 234.43 461.21
Totals 1,710.22 3,551.98 Source: 2013/14 Recurring Budget as at Dec12 A number of areas have been apportioned to DGRI as hosted as single service
6.3 Assessing Future Workforce Requirements 6.3.1 Future workforce models will be based on the clinical models described in
Section 5. The revenue costs of these models are outlined within the financial case.
6.3.2 Staffing numbers and skill mix will be adjusted and adapted in line with local workforce plans in the period up to the new hospital being opened.
6.3.3 Workforce development will be a crucial element in delivering new models of care and ensuring a safe, skilled and effective workforce. Future focus will be on the development of integrated team working. Work has already been undertaken to identify the learning and development needs of staff in relation to the models of care. A number of initiatives are currently being tested and trialled through our strategic change programme “Putting You First” such as the Dumfries Health and Social Care Hub. This is a multi-disciplinary/ multi-agency service with a single point of contact to streamline patient care.
Nursing 6.3.4 Current and future nursing workforce modelling has been undertaken and tested
against the National Workforce Planning Tools, the Professional Judgement Tool and significant benchmarking and will be in place well in advance of the opening of the new build. This work will be further supported this year by the
Commercial in Confidence
June 2013
Page 47 of 164

Redacted for Publication - see front cover
implementation of an electronic rostering system to ensure consistency of practice in the effective deployment of staff.
6.3.5 In addition, the implementation of a multi-professional clinical record will be progressed which will reduce duplication of recording and improve communication. A number of electronic devices will be trialled to enable immediate communication between staff and patients within the single rooms.
6.3.6 It is anticipated that there will be a requirement for significant change to practice and to nursing roles over the next five years. A change strategy involving all disciplines will be developed during 2013. Engagement and involvement of all staff will be crucial to the change process. Key changes will be identified and prioritised and staff will be fully supported and developed. Changes to current practice will then be planned and implemented through a staged approach. This will be implemented well before the move to the new build; however the pace of change must be commensurate with staff needs and abilities.
6.3.7 Recognising the complexities of multiple long term conditions, the NHS Board is committed to developing a multidisciplinary, multi-specialty team approach to all patient care and the development of hybrid roles.
6.3.8 Plans have been put in place to further develop the Advanced Nurse Practitioner (ANP) workforce to support and enhance the nursing and medical teams. A five year rolling programme of training of ANPs will commence this year. This will result in 12 additional qualified ANPs in 5 years time and is based on assessment of need in relation to the changing models of care and reductions in the medical workforce. In order to maximise the potential within all available resources, professional boundaries will be crossed and current staff locations will change to meet identified need.
6.3.9 Our future demographic assumptions indicate an increase in the older population and the potential for a significant increase in patients with dementia. In order to meet the needs of these patients and to ensure a safe and appropriate placement of care, Mental Health Nurses and General Registered Nurses will be required to work as one team. Training and development will be progressed and led by the newly-appointed Dementia Nurse Consultant. The introduction of a mental health/acute liaison service will also support this.
6.3.10 Future developments will necessitate a greater input to cottage hospitals and community services from a multidisciplinary/multiagency perspective. Additional training in specific skills has already been given to all staff in the cottage hospitals. Current professional roles will not be eroded in terms of assessment and planning of care, however the delivery of care will be from staff across a range of disciplines and levels of skill. Clinical Nurse Specialists who currently have an acute hospital focus will increase their role into the community as expert adviser/educator. The Emergency Centre will play a pivotal role in managing flows into and out of hospital. This will be staffed by a multidisciplinary/multiagency workforce. It will be crucial to ensure that we have a flexible workforce with the right level of skill and experience to support this facility.
Commercial in Confidence
June 2013
Page 48 of 164

Redacted for Publication - see front cover
Medical 6.3.11 Medical staffing remains a challenging issue for the Board. The changes of
Modernising Medical Careers have led to a reduction in numbers of doctors in training. Their service contribution has been limited by the need to comply with the European Working Time Directive and the requirement to have a more structured training programme away from patient care. In addition we have difficulties recruiting to Dumfries and Galloway and often have unfilled training posts. The locum market has changed significantly and it can sometimes be very difficult to recruit junior and middle grade locum doctors. Within the middle grade rotas we currently have severe problems in paediatrics and some problems in Medicine and in the Emergency Department.
6.3.12 At consultant level, the ability to recruit is variable and is dependent on the specialty concerned: We have had a number of recent successful appointments, but we have remaining challenges in some specialties. The future availability of consultants in different specialties is not currently clear and there may be further pressures in the future.
6.3.13 NHS Dumfries and Galloway remains committed to providing education and training to medical and dental students and post graduate junior and middle grade doctors. We have a high reputation as a centre for training which helps the recruitment of all grades of staff.
6.3.14 The principle changes in the medical workforce include:
Development of ANP’s to replace the reducing numbers of FY1’s from 2017.
Recruitment of two acute physicians to ensure senior decision making in the CAU. These posts are currently being recruited.
Recruitment of one specialty doctor to assist in the CAU and another within CCU to support medical high dependency. These two posts are required now to support the model
Work to achieve full recruitment to current posts Establishment of psychiatric liaison services from Midpark Hospital
Allied Health Professions (AHPs) 6.3.15 AHP services will be developed to fully support the emerging models of care.
These services have historically been limited to Monday to Friday working (except for emergency respiratory and limited orthopaedic work at weekends). Existing resources, across primary and secondary care, will be reconfigured to meet future need.
Patients will be seen at home to prevent admission to hospital where possible. To support this, staff will work between primary and secondary care to follow patients through their care pathway.
Patients will be assessed in the Combined Assessment Unit. If admission to the general wards is not necessary, effective team working and seamless links with primary care will be developed to ensure that the
Commercial in Confidence
June 2013
Page 49 of 164

Redacted for Publication - see front cover
patient can be returned home safely. Timely follow up interventions will be carried in the community to support the patient to maintain (or improve) their existing level of independence.
Seven day a week service will be provided in the wards and in the CAU where this can effectively improve the patient journey and prevent admission or facilitate safe discharge.
Enhanced recovery for major joint surgery will continue to reduce the length of stay.
Flexible working between primary and secondary care AHPs and social services occupational therapy will allow efficiencies and improved patient care.
Role development and ongoing changes to skill mix will, through increasing available capacity, provide for more responsive patient care as part of multi-disciplinary and multi-agency teams.
6.3.16 In other areas where there is physiotherapy input such as 23 hour care there are likely to be changes to working patterns that will require resource planning due to European Working Time Regulations, however any changes to staffing are likely to be minimal.
6.3.17 The impact of the increasing older population will be significant as more responsive AHP services will be required. Increased complexity of case loads requiring increased level of intervention and an enhanced focus on re-ablement to keep people independent where possible will mean that there needs to be a shift in resource from secondary to primary care in line with the aim to avoid admission to hospital where possible.
6.3.18 AHP services, who support the rehabilitation process, are vital to patient care in the field of care for older people. Planning to ensure that AHP services in the future are fit for purpose is directly related to true multi-disciplinary workforce planning. Crucial to this is adopting a person-centred approach with the individual patient and their family at the centre with teams and services designed around them.
Support Services 6.3.19 Under the NPD model all Soft FM services will be retained by NHS Dumfries &
Galloway. The new hospital will necessitate different ways of working across support services. The move to 100% single rooms within the new hospital will result in changes in practice and work is underway with Health Facilities Scotland and Health Protection Scotland to review cleaning techniques and frequencies appropriate for this environment and room configuration.
6.3.20 Different and emerging technologies are also being explored such as vapour sterilisation for single rooms and robotic cleaning for corridors.
6.3.21 The Board have also appraised meal delivery systems and have opted to retain a cook fresh option. This option will require the Board to work with local further education establishments to develop trainee cook packages to ensure continuity of staff. This work is currently underway.
Commercial in Confidence
June 2013
Page 50 of 164

Redacted for Publication - see front cover
6.3.22 The responsibility for Hard FM will fall to Project Co and will result in a small number of staff being subject to TUPE transfer. NHS Dumfries and Galloway will remain responsible for some aspects of the ongoing maintenance of the new build as well as being solely responsible for the remainder of the retained estate.
Administration
6.3.23 Clinical teams (medical, nursing, AHP) will either have access to a workstation adjacent to, or as close to as possible, their own clinical area; a number of these staff will be required to “share” workstations.
6.3.24 Open-plan office accommodation, including “hot-desks”, will be provided for administrative support function to the clinical and non-clinical teams who will require to be located on-site. Arrangements will made for certain staff to work out of hours, moving away from the traditional “9-5” model, in order to maximise the utilisation of the allocated spaces.
6.3.25 All other administrative staff will be based within other NHS Dumfries and Galloway buildings or supported as “home-workers”.
6.4 Management of Workforce Change 6.4.1 There are a number of important elements that will support the NHS Board to
achieve the transition into the new hospital:
Human Resource Implications
Workforce Planning and Development
Organisational Development
Human Resource Implications 6.4.2 In moving forward through the various stages of this process, it will be essential
to ensure full compliance with the Staff Governance Standards (4th Edition) issued in July 2012. NHS Dumfries and Galloway will utilise to the benefit of the project the responsibilities that both staff and management have in the application of the standards as follows:
Well informed
Appropriately trained and developed
Involved in decisions
Treated fairly and consistently, with dignity and respect, in an environment where diversity is valued
Provided with a continuously improving and safe working environment, promoting the health and wellbeing of staff, patients and the wider community
Commercial in Confidence
June 2013
Page 51 of 164

Redacted for Publication - see front cover
6.4.3 These new standards provide staff with a responsibility to:
Keep themselves up to date with developments relevant to their job within the organisation
Commit to continuous personal and professional development
Adherence to the standards set by their regulator bodies
Actively participate in discussions on issues that affect them either directly or indirectly or via their trade union / professional organisation
Treat all staff and patients with dignity and respect while valuing diversity
Ensure that their actions maintain and promote the health and safety and wellbeing of al staff, patients and carers
6.4.4 In terms of the development of the project, information sessions have been held to inform staff at various stages of the process to date to ensure that they are informed of key decisions that have been taken, prior to public announcement.
6.4.5 Information sessions have also been held during the public consultation period whereby staff have been able to access opportunities to provide their thoughts on the various aspects of the project. Steps are being taken to agree with staff what the best methods of keeping them up to date with changes and ensuring that they are involved in contributing their views, ideas and suggestions about proposals as the project goes forward.
6.4.6 NHS Dumfries and Galloway are fully committed to partnership working and staff side colleagues are fully involved in all aspects the project, and have representation on the Project Board and the Project Group. In addition, regular project updates are provided to the Area Partnership Forum to inform progress of the project.
6.4.7 It is fully envisaged that at the appropriate milestones in the project timetable, staff side colleagues will be fully involved in agreeing processes for the transfer of staff to the new hospital and how that will be facilitated for all staff groups.
6.4.8 It will be imperative that these working relationships with staff side colleagues are positive as they will assist with the process of implementing change, supporting staff and ensuring all processes are fair and equitable.
6.4.9 The issues that will be addressed in partnership going forward will include the following:
An open and transparent process for the allocation of staff into posts
Staff communication group
Full and comprehensive training needs analysis
Changes to work patterns / service redesign that impact on staff
Management of redeployment and protection costs and excess travel
Managing vacancies in order to maximise flexibility and opportunities for change including redeployment
Commercial in Confidence
June 2013
Page 52 of 164

Redacted for Publication - see front cover
Management of TUPE implications
Appropriate induction to the new build for all staff
6.5 Workforce Development Plans 6.5.1 In order to assess the workforce impact of moving to a new site, the Project
Board will work in partnership with staff side colleagues to develop comprehensive workforce plans for each work stream to ensure that the model of care developed is aligned to the required workforce,
6.5.2 Detailed workforce plans will be required to identify training and competency needs.
6.5.3 Training plans will be required in line with identified ‘shadow’ structures and staff will need to be prepared for the new models of care and the associated operational policies.
6.6 Organisational Development (OD) Support 6.6.1 The ongoing education and learning of staff will be critical to meeting the
challenges of transitioning into the new build.
6.6.2 A range of opportunities will be available to support staff
Clinical Leadership Programme
Teambuilding and Self Awareness Development Sessions
Leading Better Care and Releasing Time to Care
Annual development reviews, will provide the framework for individual discussions around career development and planning. The identification of associated learning and development activity required to achieve personal and professional career goals will be identified. During 2013/14 the ADR cycle will provide an opportunity to have discussions with all staff about their role in delivering the changes required to implement the new models of care and their individual development.
Supporting staff in the use of new technology.
6.7 Conclusion 6.7.1 The Board has developed a robust process for assessing and managing the
impact of the changes to staffing brought about by implementing the proposals contained within the OBC. This includes an assessment of the following areas:
The factors that affect the workforce plan.
How the Board will identify future staffing requirements.
How the change process will be managed.
Commercial in Confidence
June 2013
Page 53 of 164

Redacted for Publication - see front cover
7 FUTURE SERVICE REQUIREMENTS
7.1 Overview 7.1.1 This section of the business case provides an overview of the estimated future
service requirements based on a 2011 baseline calendar year.
7.2 General Approach to Service Modelling 7.2.1 The overall approach to bed modelling and capacity planning is based on a
number of key assumptions and changes to the future model of service delivery across the Board. These include the following key areas:
Demographic growth: The impact of population change was assessed by applying National Records of Scotland 2010-based population projections for NHS Dumfries and Galloway by age and gender to admitted patient care and outpatients’ data.
Benchmarks: A review of key performance benchmarks was undertaken to compare a range of measures on service utilisation. Data were drawn from the Information Services Division (ISD) Scotland National Scorecard, Better Quality/Better Value, and Navigator indicators. The potential for service change was assessed using comparative data for either large general hospitals or the national standard.
Balance of Care: Through ‘Reshaping Care for Older People’ and ‘Putting You First’ there will be significant changes in the way that we plan and deliver care, with more services being delivered outwith acute hospital settings. To reflect the potential impact of these changes it has been assumed that there will be improved utilisation of cottage hospitals. These changes have been modelled by assuming that there would be a transfer of stroke, fractured hip and care of elderly rehabilitation to community care at specified points in the pathway.
Combined Assessment Unit: As part of the redesign, the Combined Assessment Unit (CAU) will care for patients by providing timely assessments and treatment that is clinically appropriate. Within the CAU there will be an increased focus on the provision of emergency ambulatory and anticipatory care for a range of conditions thus avoiding the need for admission to a hospital bed. It is assumed that these changes would contribute to the overall reduction in length of stay.
Enhanced Critical Care: The number of critical care beds required was modelled by looking at total critical care need. It was assumed that appropriate patients identified as having “level 1 care” requirement, currently treated within the critical care areas, would be accommodated within the general wards in future. It was also assumed that there would be no major vascular or oesophageal surgery in future.
Commercial in Confidence
June 2013
Page 54 of 164

Redacted for Publication - see front cover
Pre-operative stay: The average number of days for elective pre-operative stay was reviewed against Scottish and combined Scottish/English data. It was assumed that pre-operative stay would improve to the Scottish mean in future.
Increased Day Case rate: The current 2011 elective inpatient activity was compared to the British Association of Day Surgery (BADS) procedures and, where activity was currently not performed as day case, it was assumed they would in the future.
Use of 23 hour beds: An analysis of current elective activity, with length of stay <5 days, was compared against BADS activity and other specified procedures determined by clinicians suitable for 23 hour care. These were assumed to be treated in 23 hour beds in the future.
Improvements in Length of Stay (LoS): The current 2011 DGRI LoS by healthcare resource group (HRG) was compared against the average for comparable large general hospitals in Scotland. The results indicate significant reductions in LoS compared to peer sites for certain high volume conditions. Shorter LoS would be achieved through improving patient pathways, increasing community provision and through developing anticipatory approaches to healthcare.
Peaks in Demand: An analysis of the variation in daily admissions and occupied beds for clinical bed pools including combined assessment, palliative care, paediatrics, neonatal and maternity services was undertaken to identify the peaks in demand for these services. It was assumed that these areas require the capacity to operate within 1.5 standard deviations (SD) or 2 SD of the mean value.
7.3 Service Modelling Methodology and Assumptions 7.3.1 A summary of the methodology for modelling inpatient, day case, theatre /
scoping and outpatient requirements is provided in the diagram below.
Commercial in Confidence
June 2013
Page 55 of 164

Redacted for Publication - see front cover
Figure 7-1: Modelling methodology
7.3.2 The planning assumptions for inpatient and daycase provision is outlined in the table below.
Figure 7-2: Planning assumptions – inpatients and day case
Planning area Assumptions
Performance Improved performance based on a review of current DGRI performance, benchmarked against information on comparable peer groups for pre-operative stay, day case rates and length of stay.
Improved utilisation of all cottage hospitals by achieving target 80% average bed occupancy. Transfer in activity modelled using three distinct pathways: fractured hip rehabilitation, stroke rehabilitation and care of the elderly.
Day case patients were assumed to require a trolley/bed for 0.6 of a day. This is based on Royal College of Surgeons recommendation that each day case trolley/bed would on average be used by 1.55 patients per day.
Commercial in Confidence
June 2013
Page 56 of 164

Redacted for Publication - see front cover
Planning area Assumptions
Utilisation / availability
Future capacity planning and bed modelling was based upon the following target bed occupancy rates:
Medical and Surgical 85% Critical Care 75%* Children’s Unit 65% Palliative Care 90% Maternity Inpatients 60% 23 Hour Beds 90%
Bed availability was assumed to be 365 days for inpatients and 252 days for day case patients.
*Intensive Care society guidelines
Bed / trolley requirements
The future beds requirements have been determined using the following formulae:
Total occupied beddays = activity x length of stay
Total beds = occupied bed days / occupancy rate / days beds are available
7.3.3 The planning assumptions for theatre and endoscopy suites is outlined in the table below.
Figure 7-3: Planning assumptions – theatres and endoscopy
Planning area Assumptions
Performance The time per theatre case was taken from National Theatres Implementation Group (NTIG) submissions. These are robust electronic theatre times for each OPCS procedure code including anaesthetic time.
A review of the main operation code was undertaken to identify the current demand for endoscopy. In addition to inpatient and day case scoping there are also a number of flexible sigmoidoscopies currently carried out within outpatients. This is not captured within SMR data, however local information indicates circa 1,000 per annum. These have been added to the overall requirements assuming on average 25 minutes per scope.
Commercial in Confidence
June 2013
Page 57 of 164
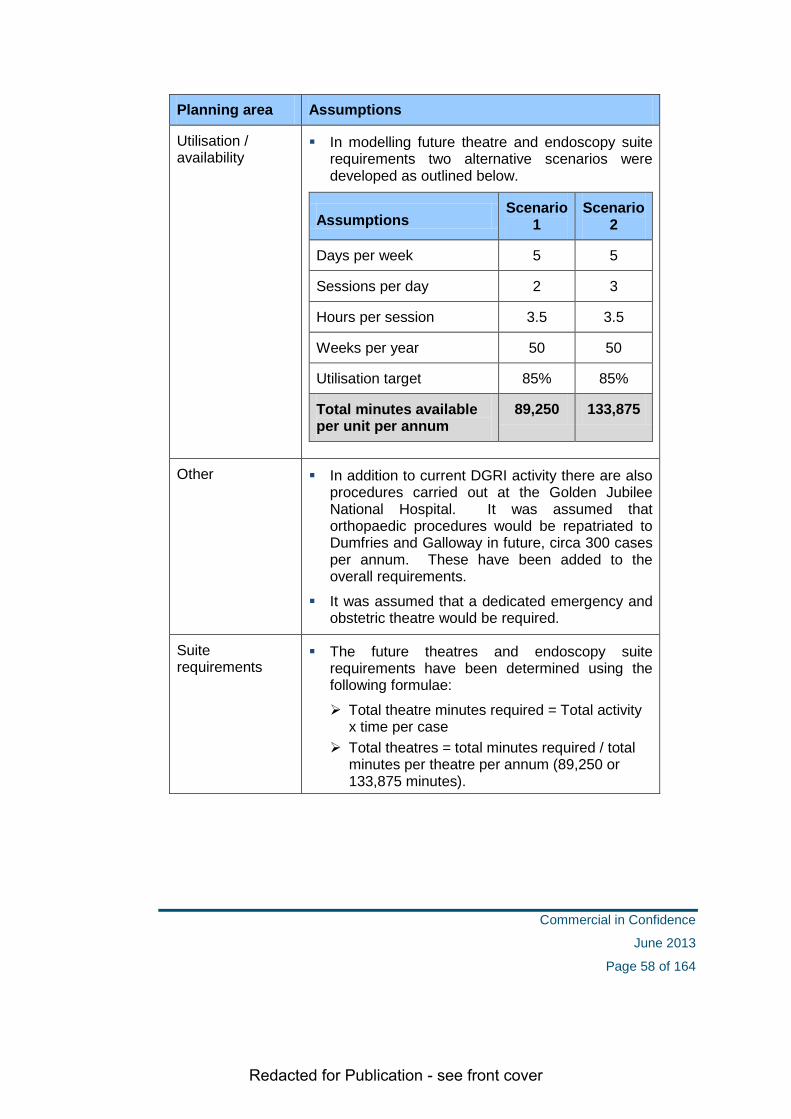
Redacted for Publication - see front cover
Planning area Assumptions
Utilisation / availability
In modelling future theatre and endoscopy suite requirements two alternative scenarios were developed as outlined below.
Assumptions Scenario
1 Scenario
2
Days per week 5 5
Sessions per day 2 3
Hours per session 3.5 3.5
Weeks per year 50 50
Utilisation target 85% 85%
Total minutes available per unit per annum
89,250 133,875
Other In addition to current DGRI activity there are also procedures carried out at the Golden Jubilee National Hospital. It was assumed that orthopaedic procedures would be repatriated to Dumfries and Galloway in future, circa 300 cases per annum. These have been added to the overall requirements.
It was assumed that a dedicated emergency and obstetric theatre would be required.
Suite requirements
The future theatres and endoscopy suite requirements have been determined using the following formulae:
Total theatre minutes required = Total activity x time per case
Total theatres = total minutes required / total minutes per theatre per annum (89,250 or 133,875 minutes).
Commercial in Confidence
June 2013
Page 58 of 164

Redacted for Publication - see front cover
7.3.4 The planning assumptions for outpatient clinic requirements are outlined in the table below.
Figure 7-4: Planning assumptions – outpatients
Planning area Assumptions
Performance Improved performance based on a review of current DGRI specialty return to new ratios, benchmarked against Scottish and combined Scottish/English data. It was assumed that DGRI return to new ratios would improve to the combined mean in future.
A reduction in pre-operative stay will be achieved by pre-assessment for all planned procedures; therefore it is assumed that there will be increased demand for these clinics in future.
Outpatient clinics for a number of services including paediatrics, obstetrics and gynaecology will be conducted in the specialist departments; therefore it is assumed that these services do not require clinic room space within the general outpatient area.
To determine the clinic minutes required the current time scheduled per attendance for each specialty was assumed. The average time for a new appointment is 25 minutes (range 10 minutes to 45 minutes) and the average time for a return appointment is 15 minutes (range 10 minutes to 20 minutes).
Commercial in Confidence
June 2013
Page 59 of 164

Redacted for Publication - see front cover
Planning area Assumptions
Utilisation / availability
In modelling future outpatient clinic room requirements two alternative scenarios were developed as outlined below.
Assumptions Scenario
1 Scenario
2
Days per week 5 5
Sessions per day 2 3
Hours per session 3.5 3.5
Weeks per year 50 50
Utilisation target 85% 85%
Total minutes available per room per annum
89,250 133,875
Clinic requirements
The future clinics have been determined using the following formulae:
Total clinic minutes required = Total activity x time per attendance
Total clinics = total minutes required / total minutes per clinic per annum (89,250 or 133,875 minutes)
Commercial in Confidence
June 2013
Page 60 of 164
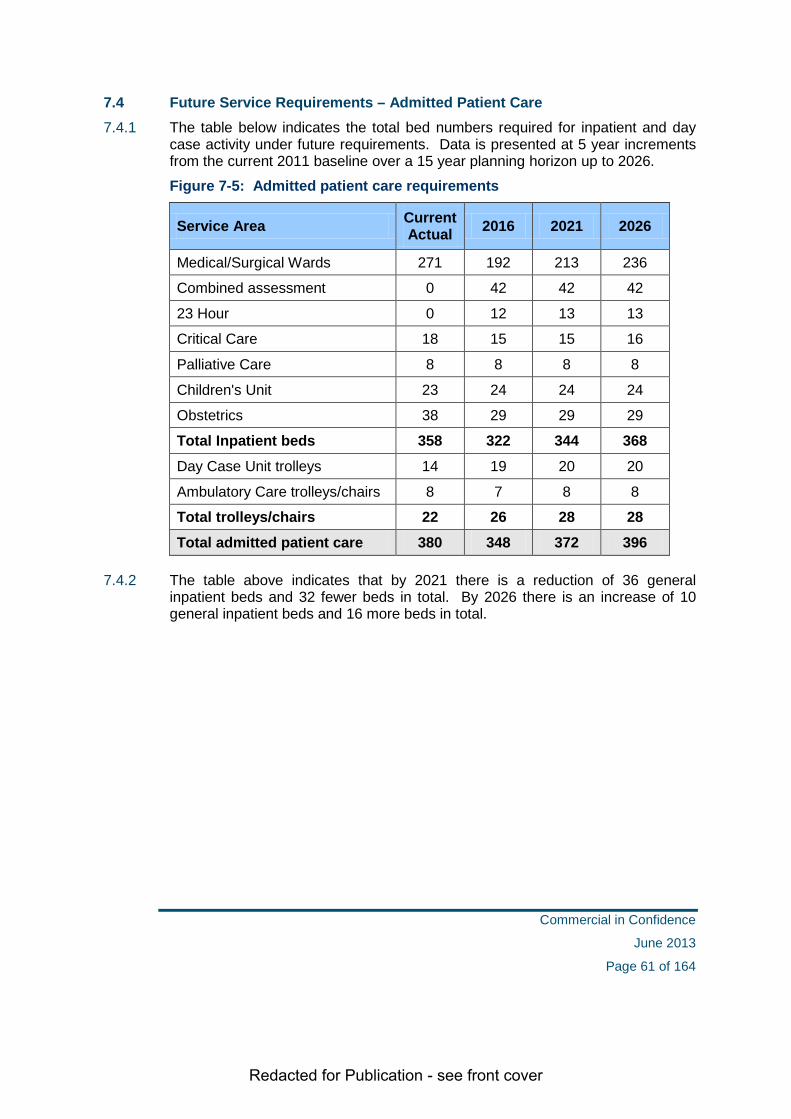
Redacted for Publication - see front cover
7.4 Future Service Requirements – Admitted Patient Care 7.4.1 The table below indicates the total bed numbers required for inpatient and day
case activity under future requirements. Data is presented at 5 year increments from the current 2011 baseline over a 15 year planning horizon up to 2026.
Figure 7-5: Admitted patient care requirements
Service Area Current Actual 2016 2021 2026
Medical/Surgical Wards 271 192 213 236
Combined assessment 0 42 42 42
23 Hour 0 12 13 13
Critical Care 18 15 15 16
Palliative Care 8 8 8 8
Children's Unit 23 24 24 24
Obstetrics 38 29 29 29
Total Inpatient beds 358 322 344 368 Day Case Unit trolleys 14 19 20 20
Ambulatory Care trolleys/chairs 8 7 8 8
Total trolleys/chairs 22 26 28 28 Total admitted patient care 380 348 372 396
7.4.2 The table above indicates that by 2021 there is a reduction of 36 general inpatient beds and 32 fewer beds in total. By 2026 there is an increase of 10 general inpatient beds and 16 more beds in total.
Commercial in Confidence
June 2013
Page 61 of 164

Redacted for Publication - see front cover
7.4.3 An analysis of general inpatient beds based upon 2.5% increments in bed occupancy and length of stay improvement is shown in the table below. The grid demonstrates the sensitivity of the bed modelling to a range of planning assumptions. The median number of beds is 214 which aligns with the modelled requirement for 2021.
Figure 7-6: Analysis of general inpatient beds by bed occupancy and LoS
Bed Occupancy and Planning Year
Length of stay reduction
2016 2021 2026
80% 82.5% 85% 80% 82.5% 85% 80% 82.5% 85%
2.5% 220 212 204 243 234 226 268 259 250
5.0% 213 205 198 236 227 219 261 251 243
7.5% 207 199 192 229 221 213 253 244 236
10.0% 200 193 186 222 214 206 245 237 228
12.5% 193 186 179 215 207 199 238 229 221
15.0% 187 180 173 208 200 193 230 222 214
17.5% 180 173 167 200 193 186 222 214 207
Commercial in Confidence
June 2013
Page 62 of 164

Redacted for Publication - see front cover
7.5 Future Service Requirements – Theatres and Endoscopy Theatres
7.5.1 The table below indicates the results under each availability scenario. It was assumed that a dedicated emergency and obstetric theatre would be required.
Figure 7-7: Theatre requirements
Sessions per day 2016 2021 2026
Scenario 1 – 2 Sessions per day 7.9 8.0 8.1
Scenario 2 – 3 Sessions per day 6.3 6.4 6.4
7.5.2 The table suggests that, using 2026 as the planning period, 9 theatres (including 1 ophthalmology theatre) will be required under 2 session working and 7 theatres under 3 session working.
7.5.3 We currently have 9 theatres on the DGRI site and are planning for 8 theatres in the New Build and an Ophthalmology Theatre in the refurbished Cresswell. The Outline Business Case refers to the use of the operating theatres (x 6 elective) on 2 sessions per day over 5 days.......Monday to Friday am & pm. The remaining 2 theatres are the emergency and obstetric theatres.
7.5.4 NHS Dumfries and Galloway plan to significantly change the way these services are currently delivered, through a whole scale review and redesign of processes, services, staffing and accommodation. The key changes will be:
• To continue development of ERAS – enhanced recovery after surgery.
• To improve and enhance all existing surgical and associated journeys
• To ensure that patients are always cared for in the most appropriate locations, at the most convenient time for patients, by the most appropriate staff groups
• to minimise non-value adding process steps through ensuring that patients only access staff, services and process elements if they will benefit from them
• To minimise duplication of effort and resources whilst ensuring longer-term sustainability through optimising and consolidating physical accommodation
7.5.5 To continue disinvestment in procedures of limited value
7.5.6 To achieve the above we will need to completely review the way in which our theatre sessions are scheduled, to ensure that the surgeons from the various specialties are given access to theatres at times that will ensure the greatest efficiency and maximise productivity. The current theatre timetabling is out
Commercial in Confidence
June 2013
Page 63 of 164

Redacted for Publication - see front cover
dated. This review will be challenging as it will require us to fundamentally change the current specialty timetables/ job plans and start afresh.
7.5.7 We have already implemented evening and weekend operating in a number of elective theatres to enable us meet the TTG (Treatment Time Guarantee) demand placed on our operative services, however on an ad hoc basis. This is an expensive arrangement given the additional cost of out of hours working, with payment of premium rates to the groups of staff involved. Also this can be difficult to sustain given that our hospital elective services have traditionally been Monday to Friday and any additional theatre activity out with this time involves fairly significant change to a number of other services e.g. anaesthetic, ward nursing, administrative, diagnostic, ancillary services.
7.5.8 Notwithstanding the above, given the increased pressure on our theatre services, and our strategy to repatriate certain activity (e.g. major joint surgery from tertiary centres), it is likely we wil have to extend the number of operating days and theatre operating times to meet demand. We have commenced an efficiency and productivity review of our elective theatres to improve capacity which will be recommending that we extend our operating times, with morning sessions starting at 8.30am and the afternoon sessions finishing at 6.00pm. Improvements in theatre productivity have already been made in a number of areas; one successful change has been in Orthopaedics where the number of hip replacements is being increased from 2 to 4 per day.
7.5.9 Our ability to deliver the appropriate staffing model and the consequent affordability is vital to the achievement of our repatriation strategy. Not only are we aiming to improve the quality of our services, we also are planning to deliver savings from these changes.
7.5.10 In conclusion,
• We will be making cost effective use of 8 theatres avoiding premium out of hours payments for staff.
• We will continue weekend operating and extend am/pm operating times.
• We will continue increasing day case rates (evening sessions not appropriate).
• The capacity planned will allow for repatriation and anticipated growth in demand.
Commercial in Confidence
June 2013
Page 64 of 164

Redacted for Publication - see front cover
Endoscopy Suites 7.5.11 The table below indicates the future requirements for endoscopy under either 2
session or 3 session working.
Figure 7-8: Endoscopy suite requirements
Sessions per day 2016 2021 2026
Scenario 1 – 2 Sessions per day 1.8 1.9 2.1
Scenario 2 – 3 Sessions per day 1.2 1.3 1.4
7.5.12 The table above suggests, under the 2026 planning period, a total of 3 endoscopy suites will be required under 2 session working and 2 suites with 3 session working.
7.5.13 As is the case with theatres, the Board’s formal position is to operate a 2 session working day in light of the workforce and financial implications associated with three session working.
Outpatient Clinics 7.5.14 The table below indicates the future requirements for outpatient clinic rooms
under either 2 session or 3 session working.
Figure 7-9: Clinic room requirements Session per day Functional Area 2016 2021 2026
2 sessions
General Outpatients (excluding orthodontics)
22 23 23
Orthopaedic Outpatients (including Out of Hours)
5 5 6
Pre-assessment 4 4 4
Total 31 32 33
3 sessions
General Outpatients 15 15 16
Orthopaedic Outpatients 3 4 4
Pre-assessment 2 3 3
Total 20 22 23
Commercial in Confidence
June 2013
Page 65 of 164

Redacted for Publication - see front cover
7.5.15 The clinic room modelling suggests that by 2021, 32 clinic rooms are required under 2 session working and 22 under 3 session working. By 2026 the numbers increase to 33 clinic rooms under 2 session working and 23 under 3 session working.
7.5.16 As is the case with theatres and scoping suites, the Board’s formal position is to operate a 2 session working day in light of the workforce and financial implications associated with three session working.
Commercial in Confidence
June 2013
Page 66 of 164

Redacted for Publication - see front cover
7.6 Summary of Current and Future Requirements The table below summaries the future capacity requirements for 2026. This year was chosen as a realistic timeframe (approx.10 years post completion) that would reflect essential components of demographic change. It is assumed that 2 session working will be in place within theatres, scoping suites and outpatient clinics. Figure 7-10: Summary of requirements by service area to 2026
Facility Current Actual
Future Service
Requirements
Actual number provided in
new development
Medical/Surgical Wards 2711 214 2102
Combined Assessment 0 42 423
23 Hour 0 14 14
Critical Care 18 16 17
Palliative Care 8 8 8
Children's Unit 234 24 245
Obstetrics 386 29 297
Total inpatient beds 358 347 344
Day Case Unit trolleys 148 20 208
Ambulatory Care trolleys/chairs 8 10 10
Total trolleys/chairs 22 30 30
Theatres 99 9 810
Scoping suites 3 3 411
Outpatient consulting rooms 2712 33 33 1. includes 8 medical assessment beds and 12 23-hour beds 2. includes both medical and surgical beds 3. includes 10 assessment trolleys 4. includes 19 beds and 4 assessment beds 5. includes 12 beds, 4 assessment beds and 8 day unit beds 6. includes 18 maternity inpatients, 9 birthing suite and 11 neonatal cots 7. includes 12 maternity inpatients, 6 birthing suite, 2 assessment beds and 9 neonatal
cots 8. excludes stage 1 recovery 9. includes ophthalmic (x1) and maternity (x2) theatres embedded in departments 10. excludes ophthalmic theatre (for daycases) which will be located in Cresswell build
however, access will be required to theatre in the new build for inpatients 11. will include ’oscopy’ activity currently carried out in OPD procedure room 12. includes outpatient activity carried out in both General and Orthopaedic Outpatient
departments. This does not include outpatient activity carried out in other clinical areas of DGRI
Commercial in Confidence
June 2013
Page 67 of 164

Redacted for Publication - see front cover
7.7 Conclusion 7.7.1 This chapter provides an overview of the service model methodology and
assumptions. In particular it provides the following:
General approach to modelling the future service requirements
Capacity planning methodology and assumptions
Future service requirements - including beds, theatres and outpatient clinic rooms
Comparison of current and future requirements
Commercial in Confidence
June 2013
Page 68 of 164

Redacted for Publication - see front cover
ECONOMIC CASE
Commercial in Confidence
June 2013
Page 69 of 164

Redacted for Publication - see front cover
8 OPTION OVERVIEW
8.1 Overview 8.1.1 This section of the OBC sets out the process for option appraisal. The primary
aim is to demonstrate which option offers best value for money by considering the benefits, costs and risks.
8.1.2 The case will clearly highlight the preferred option which can demonstrate the optimal balance across the core elements. The table below highlights the steps taken in reaching the preferred option:
Figure 8-1: Development of economic case
Long List of Options
Preferred Option
Opt
ion
Iden
tific
atio
n
Acute Services Redevelopment Project – Economic Case
Non Financial Benefits
Economic Appraisal
Non Financial
Risks
Option Appraisal of Short Listed Options
Short List of Options
Commercial in Confidence
June 2013
Page 70 of 164

Redacted for Publication - see front cover
9 OPTION IDENTIFICATION
9.1 Overview 9.1.1 This section of the OBC sets out the options considered as part of the option
appraisal process and describes further the options shortlisted and taken forward to the option appraisal described in the next section.
9.2 Long List of Options 9.2.1 An initial list of options were fully considered and tested to identify if they could
deliver at a high level the Investment Objectives set out in the Strategic Case. The list of options and the reason for discounting a number of the options are shown below:
Figure 9-1: Long list of options
Description /x Reason for discounting
1 Redevelopment, including additional ward block to provide single room accomodation (100%)
2 Constructing a new DGH on current site
3 Constructing a new DGH on a new site
4 Do nothing Limited or no ability to respond to National Policy
5 Do minimum, backlog maintenance Limited or no ability to respond to future Demographics
6 Minimal refurbishment of existing ward accomodation, increase in number of single rooms available to 36%
Limited or no ability to moderniseservives
7 Redevelopment, including additional ward block to provide single room accomodation (50%)
Backlog maintenance notaddressed or significantly difficultto achieve
8 Constructing a new DGH on a new site, with additional office accomodation
x Additional office space not apriority
x
9.2.2 The remaining three options were agreed to be taken forward to the next stage.
Commercial in Confidence
June 2013
Page 71 of 164
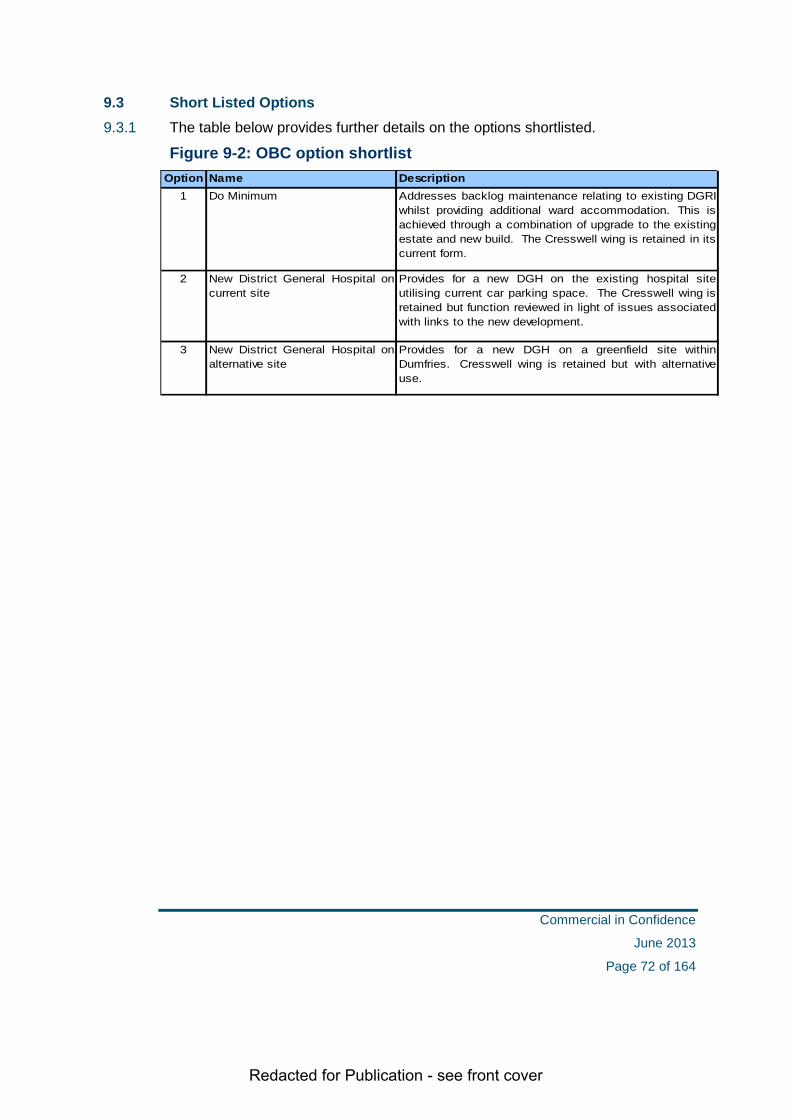
Redacted for Publication - see front cover
9.3 Short Listed Options 9.3.1 The table below provides further details on the options shortlisted.
Figure 9-2: OBC option shortlist Option Name Description
1 Do Minimum Addresses backlog maintenance relating to existing DGRIwhilst providing additional ward accommodation. This isachieved through a combination of upgrade to the existingestate and new build. The Cresswell wing is retained in itscurrent form.
2 New District General Hospital oncurrent site
Provides for a new DGH on the existing hospital siteutilising current car parking space. The Cresswell wing isretained but function reviewed in light of issues associatedwith links to the new development.
3 New District General Hospital onalternative site
Provides for a new DGH on a greenfield site withinDumfries. Cresswell wing is retained but with alternativeuse.
Commercial in Confidence
June 2013
Page 72 of 164

Redacted for Publication - see front cover
10 OPTION APPRAISAL
10.1 Overview 10.1.1 The following section sets out the process followed and the outputs collected for
each of the three core elements
• Non financial benefits
• Non financial risks
• Economic appraisal (Net Present Value)
10.2 Non financial Benefits 10.2.1 Non financial benefits are those benefits which cannot be measured in monetary
terms; they include improvements across services that can be measured using non financial performance indicators.
10.2.2 The Board has developed a range of benefits which will underpin the delivery of the investment objectives set out within the Strategic Case. By assessing each of the short listed options, the strategic alignment can be considered and a differentiation made between alternative solutions.
10.2.3 Details of the benefit criteria and their mapping to the investment objectives are provided in the table below. Further details of the features associated with each benefit criteria are provided at Appendix 3.
Figure 10-1: OBC benefit criteria and links to investment objectives Criteria Map to Investment Objective
Clinical Effectiveness and Sustainability Capacity and Demand Delivering models of care in line with the clinical strategy Access Performance and efficiency Clinical Effectiveness and Sustainability Capacity and Demand Clinical Effectiveness and Sustainability Physical Environment Capacity and Demand Delivering models of care in line with the clinical strategy Performance and efficiency
Appropriate numbers of adequately trained staff Recruitment, retention of staff and students Physical environment Access Clinical Effectiveness and Sustainability Physical Environment
Clinical effectiveness and Integration of service
Sustainability and Safety of Services
Quality of Patient Care
Quality of physical environment
Timing, Phasing and Disruption
10.2.4 To ensure that the importance of each criteria relative to each other is appropriate the Board, in partnership with a wider stakeholder group, ranked and
Commercial in Confidence
June 2013
Page 73 of 164

Redacted for Publication - see front cover
weighted the criteria prior to scoring each of the options. The group agreed that the quality of patient care was the most important non financial benefit and therefore it received the largest share of the weighting. Timing, phasing and disruption were considered the least important in terms of non financial benefits and the weighting reflected this.
10.2.5 The results of the scoring exercise are detailed in the table below.
Figure 10-2: Benefit scores for shortlisted options
Option 1
Option 2
Option 3
1 Quality of patient care 21.50% 116.10 182.70 200.002 Clinical effectiveness, integration of service 20.50% 98.40 164.00 178.303 Sustainability and safety of services 19.50% 83.90 159.90 167.704 Appropriate numbers of adequately trained staff 17.50% 87.50 148.80 148.805 Quality of physical environment 14.00% 57.40 126.00 128.806 Timing, phasing and disruption 7.00% 19.60 35.00 66.50
100.00% 462.90 816.40 890.103 2 1
Benefit CriteriaWeight
%
Weighted Score
Total ScoreRank
10.2.6 The results of the scoring show that the off-site option produce the highest score in terms of non financial benefits.
10.2.7 Whilst the option of developing a new hospital on the current site scores well it does not deliver as high a score as the offsite option in areas such as Quality and Clinical Effectiveness. This results largely from the challenges in linking the new development to the Cresswell wing. It is also significantly more disruptive during the construction phase than Option 3.
10.2.8 Unsurprisingly the do minimum option returns a poor score. Whilst it does address backlog maintenance it does not improve key adjacencies nor provide for expansion / reconfiguration in a number of areas. It is also highly disruptive and involves an extended programme of development.
10.2.9 In terms of non-financial benefits it is clear that the new build, off site option offers the optimal solution.
10.2.10 As a result of the significant reliance that is placed on the outcome of the benefit criteria exercise it is important to consider how sensitive the results are to changes in key variables. By running a series of sensitivity models it can be demonstrated that the outcome is reliable. The following table sets out the sensitivities modelled and the outcomes.
Commercial in Confidence
June 2013
Page 74 of 164

Redacted for Publication - see front cover
Figure 10-3: Result of benefits sensitivity testing Scenario Description Option 1 Option 2 Option 3
462.90 816.40 890.103 2 1
346.80 633.70 690.103 2 1
440.13 786.83 896.893 2 1
Original As per original weighting and scoring
1 Exclude the top weighted benefit to ensure overall scores are not skewed by one dominant benefit
2 Weighting all benefits equally to test for robustness of scoring options
10.2.11 The result of the sensitivity testing demonstrates that Option 3 would continue to produce the highest score in terms of non financial benefits.
10.3 Non financial Risks 10.3.1 Non financial risks are those risks which are likely to have a non financial impact,
there may also be associated costs however the consideration in this section are the non financial implications. For example it may include the impact on the service if the building failed to deliver the level of quality anticipated or cannot provide future flexibility or access
10.3.2 The Board has identified a range of development and service risks. Development risks are assumed to relate to the design and construction phase of the project and service risks to the commissioning and operational phases.
10.3.3 By assessing each of the short listed options against these the level of risk can be considered and a differentiation made between alternative solutions.
10.3.4 The options were scored on the severity of the consequence and the likelihood of occurrence using a simple 1-5 scoring scale for. The risk was then scored low to very high using the following table:
Figure 10-4: Analysis of qualitative risk levels figure
1 Negligible 1 2 3 4 5 1-3 Low
2 Minor 2 4 6 8 10 4 - 9 Medium
3 Moderate 3 6 9 12 15 10 - 14 High
4 Major 4 8 12 16 20 15 - 25 Very High
5 Extreme 5 10 15 20 25
KeySeverity of consequence
Likelihood of occurrence
1 Rare
2 Unlikely
3 Possible
4 Likely
5 Almost certain
Commercial in Confidence
June 2013
Page 75 of 164
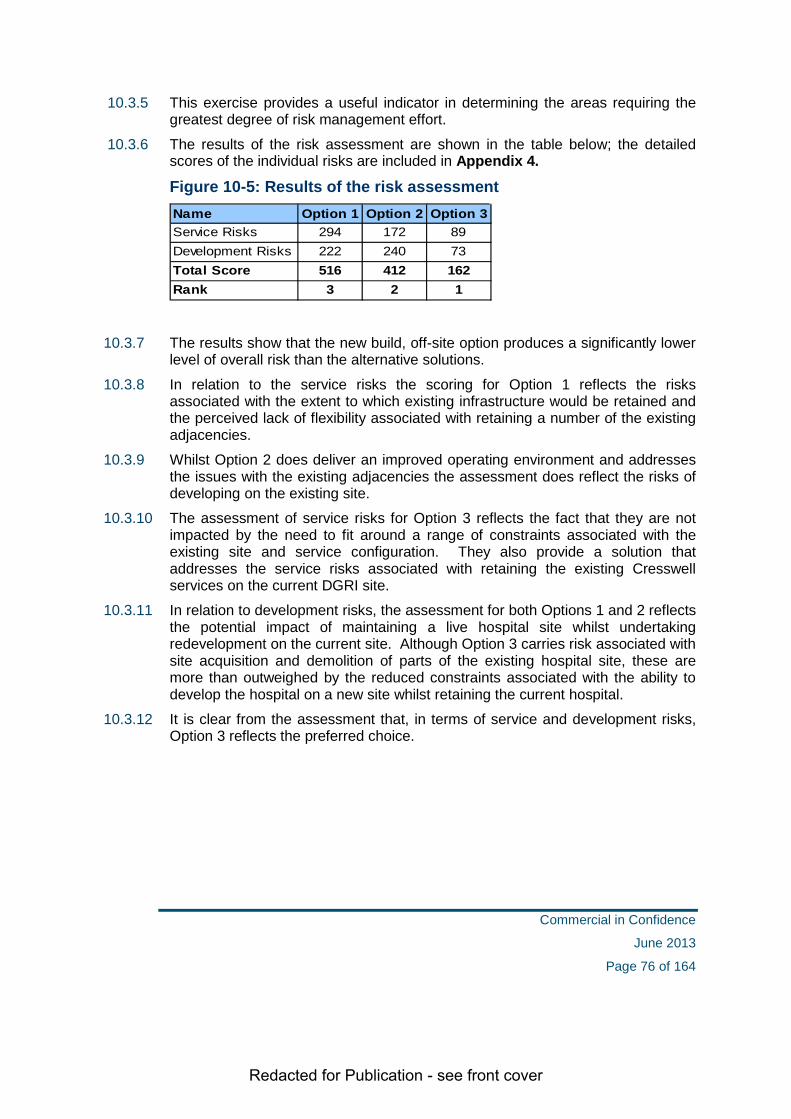
Redacted for Publication - see front cover
10.3.5 This exercise provides a useful indicator in determining the areas requiring the greatest degree of risk management effort.
10.3.6 The results of the risk assessment are shown in the table below; the detailed scores of the individual risks are included in Appendix 4.
Figure 10-5: Results of the risk assessment Name Option 1 Option 2 Option 3Service Risks 294 172 89Development Risks 222 240 73Total Score 516 412 162Rank 3 2 1
10.3.7 The results show that the new build, off-site option produces a significantly lower level of overall risk than the alternative solutions.
10.3.8 In relation to the service risks the scoring for Option 1 reflects the risks associated with the extent to which existing infrastructure would be retained and the perceived lack of flexibility associated with retaining a number of the existing adjacencies.
10.3.9 Whilst Option 2 does deliver an improved operating environment and addresses the issues with the existing adjacencies the assessment does reflect the risks of developing on the existing site.
10.3.10 The assessment of service risks for Option 3 reflects the fact that they are not impacted by the need to fit around a range of constraints associated with the existing site and service configuration. They also provide a solution that addresses the service risks associated with retaining the existing Cresswell services on the current DGRI site.
10.3.11 In relation to development risks, the assessment for both Options 1 and 2 reflects the potential impact of maintaining a live hospital site whilst undertaking redevelopment on the current site. Although Option 3 carries risk associated with site acquisition and demolition of parts of the existing hospital site, these are more than outweighed by the reduced constraints associated with the ability to develop the hospital on a new site whilst retaining the current hospital.
10.3.12 It is clear from the assessment that, in terms of service and development risks, Option 3 reflects the preferred choice.
Commercial in Confidence
June 2013
Page 76 of 164

Redacted for Publication - see front cover
10.4 Economic Appraisal 10.4.1 The Board has identified a range of costs which relate to the project over the next
30 years which include both capital and revenue costs. Examples of costs included within this calculation would be unitary charge, capital build costs, baseline running costs and any additional service running costs identified.
10.4.2 The combined cost is referred to as the Net Present Value (NPV) and is calculated by removing any inflationary cost increases over the 30 year period and presenting the costs at current day prices.
10.4.3 To allow comparability between the three options the cost information which has been used to calculate the NPV is based on technical costing previously provided by external advisors on the three options. This information has been reviewed and updated to reflect current pricing information.
10.4.4 The results of the analysis are presented in the table below and the detailed schedules are included within Appendix 5.
Figure 10-6: Results of the economic appraisal £000
Option 1 Option 2 Option 3
NPV over appraisal period
Ranking 1 3 2
10.4.5 The table above indicates that using the previously available costing information Option 1 has the lowest NPV. This is due to the lower level of capital expenditure within this option as it not a full rebuild. Option 2 and 3 both being new build NPD options are higher.
10.4.6 There is a relatively small differential between Option 2 and 3, with the costs of Option 2 only needing to decrease marginally to switch the ranking of these options.
10.4.7 As a result of the significant reliance that is placed on the outcome of the economic appraisal it is important to consider how sensitive the results are to changes in key variables. The following table sets out the sensitivities modelled and the outcomes.
Commercial in Confidence
June 2013
Page 77 of 164

Redacted for Publication - see front cover
Figure 10-7: Results of NPV sensitivity analysis Scenario Description Option 1 Option 2 Option 3
1 3 2
1 3 2
1 2 3
Original As per original weighting and scoring
1 Replace Option 3 with the more recent costed information available (per Tech Cost 2)
2 Use Option 3 as a benchmark for Option 2 based on Tech Cost 2
The results show that by replacing the original cost used to calculate Option 3 with the latest Tech Cost 2 information the ranking remains consistent. In Sensitivity Scenario 2, Option 2 has been restated on a similar basis as Tech Cost 2. The impact of this is marginal on the NPV calculation.
10.5 Option Appraisal Results 10.5.1 The following table summarises the results of the benefits appraisal, qualitative
risk assessment and economic appraisal presented above.
Figure 10-8: Results of the option appraisal Option appraisal measure Option 1 Option 2 Option 3
Benefit Points 462.90 816.40 890.10
Net Present Value (£000)
Risk Assessment 516 412 162
10.5.2 To assess the relative value for money a comparison of the Net Present Value per benefit point has been undertaken and is shown below. This is calculated by dividing the NPV by the benefit score for each option to provide a comparable cost per benefit point.
Figure 10-9: Results of the cost per benefit point Option 1 Option 2 Option 3
NPV over appraisal period (£000)
Benefits Appraisal (points) 462.90 816.40 890.10
NPV per Benefit Point (£000) 4,381 2,769 2,519
Ranking 3 2 1
10.5.3 The results show that when comparing the relative costs and benefits of the alternative solutions, Option 3 has the lowest overall cost per benefit point indicating this option delivers the best value for money of the short listed options.
Commercial in Confidence
June 2013
Page 78 of 164
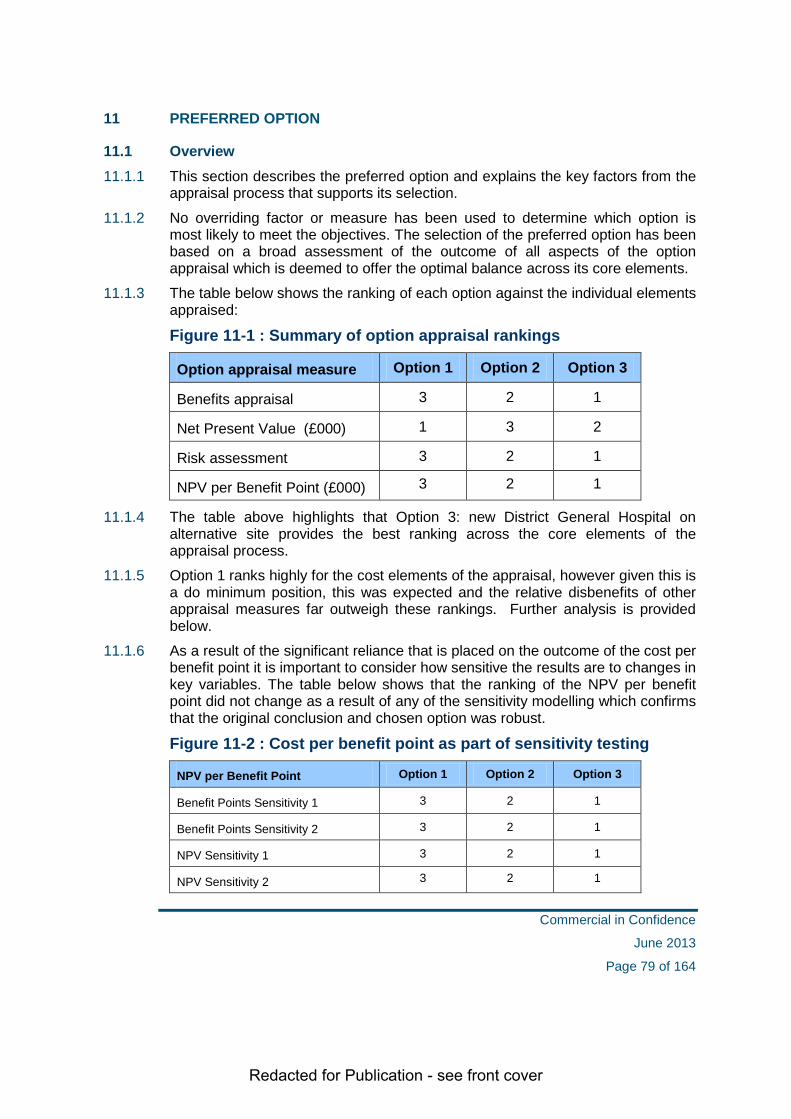
Redacted for Publication - see front cover
11 PREFERRED OPTION
11.1 Overview 11.1.1 This section describes the preferred option and explains the key factors from the
appraisal process that supports its selection.
11.1.2 No overriding factor or measure has been used to determine which option is most likely to meet the objectives. The selection of the preferred option has been based on a broad assessment of the outcome of all aspects of the option appraisal which is deemed to offer the optimal balance across its core elements.
11.1.3 The table below shows the ranking of each option against the individual elements appraised:
Figure 11-1 : Summary of option appraisal rankings
Option appraisal measure Option 1 Option 2 Option 3
Benefits appraisal 3 2 1
Net Present Value (£000) 1 3 2
Risk assessment 3 2 1
NPV per Benefit Point (£000) 3 2 1
11.1.4 The table above highlights that Option 3: new District General Hospital on alternative site provides the best ranking across the core elements of the appraisal process.
11.1.5 Option 1 ranks highly for the cost elements of the appraisal, however given this is a do minimum position, this was expected and the relative disbenefits of other appraisal measures far outweigh these rankings. Further analysis is provided below.
11.1.6 As a result of the significant reliance that is placed on the outcome of the cost per benefit point it is important to consider how sensitive the results are to changes in key variables. The table below shows that the ranking of the NPV per benefit point did not change as a result of any of the sensitivity modelling which confirms that the original conclusion and chosen option was robust.
Figure 11-2 : Cost per benefit point as part of sensitivity testing
NPV per Benefit Point Option 1 Option 2 Option 3
Benefit Points Sensitivity 1 3 2 1
Benefit Points Sensitivity 2 3 2 1
NPV Sensitivity 1 3 2 1
NPV Sensitivity 2 3 2 1
Commercial in Confidence
June 2013
Page 79 of 164

Redacted for Publication - see front cover
11.2 Analysis of the Option Appraisal Results
Option 1
11.2.1 This option should be discounted as although it addresses the backlog maintenance requirements and provides some clinical and functional enhancements, it does not fully support the key requirements of the models of care and required improvements to clinical service delivery.
11.2.2 The prolonged programme, multiple phases and extensive decant facilities required compromises the overall value for money. This is reflected in the poor level of benefits offered and the high degree of qualitative risk.
Option 2
11.2.3 This option delivers a higher level of benefits and lower level of risk than Option 1 but poorer overall value for money than Option 3.
11.2.4 It delivers the full range of clinical requirements and infrastructure enhancements whilst addressing all of the backlog maintenance issues associated with the existing site. This is reflected in the benefits score against key criteria such as quality, clinical effectiveness, safety and quality of environment.
11.2.5 The qualitative risk analysis shows that Option 2 is an option which carries significantly increased risk due to the existing site constraints and service disruption during the build programme.
11.2.6 It would clearly be possible to deliver this option, however, site constraints and topography would compromise the final solution. As well as the parking issues, access to mortuary, CSSD and supplies department would be difficult to maintain.
11.2.7 The use of the Cresswell wing would have to be changed to allow for improved clinical adjacencies. Whilst this could be achieved the site constraints would result in a less efficient building with increased communication space, which would result in increased recurring costs.
11.2.8 Current access problems would not be resolved by building on the existing site. This is obviously a critical success factor for the preferred solution.
Commercial in Confidence
June 2013
Page 80 of 164
Redacted for Publication - see front cover
Option 3
11.2.9 This option is the second most expensive in terms of initial investment; however it scores best in Benefits Appraisal and Risk Assessment. As with Option 2 it delivers the full range of clinical requirements and infrastructure enhancements whilst addressing all of the backlog maintenance issues associated with the existing site. It does however have the added advantage of being less disruptive than Option 2 which is reflected both in terms of benefits and risks.
11.2.10 Located within the Dumfries by-pass, will result in reduced congestion issues through the town and improving access to the hospital. Journey times for staff, patients and visitors from outlying areas would be reduced.
11.2.11 The site has fewer constraints on the design, and would deliver efficiencies by providing a more compact building, improving clinical adjacencies and reducing travel time within the building.
11.2.12 As is the case with Option 2 the use of the Cresswell wing would have to be changed, however, this is likely to require some service reconfiguration so that day surgery and maternity services can be accommodated within the new hospital.
Conclusion For the reasons outlined above, Option 3, the development of a new District General Hospital on a greenfield site is the option that will be taken forward and included in the reference design process.
The selection process for a new Greenfield site is outlined in Chapter 14
Commercial in Confidence
June 2013
Page 81 of 164

Redacted for Publication - see front cover
Commercial in Confidence
June 2013
Page 82 of 164

Redacted for Publication - see front cover
REFERENCE DESIGN
Commercial in Confidence
June 2013
Page 83 of 164

Redacted for Publication - see front cover
12 REFERENCE DESIGN PROCESS
12.1 Summary 12.1.1 The Board has, in conjunction with our experienced advisors, undertaken a
significant amount of work to develop a reference design for the Project. Planning permission in principle was received from Dumfries and Galloway Council Planning Department on 26 April, 2013 and confirmed by letter on 9th May 2013
12.1.2 The reference design includes the following:-
• A new hospital building, of low rise design of no more than four stories in height, to accommodate some 350 in-patient beds, with an internal floor space of approx 53,500sqm;
• formation of new access from an enlarged A75 / Garroch roundabout and realignment of the Glen Road; separate dedicated emergency entrance, and secondary goods and services access;
• 980 car parking spaces and 80 cycle parking spaces;
• a helipad;
• staff residences;
• a dedicated energy centre;
• landscaping, including extensive cut and fill operations to level the site, with retention /re-use of all material along eastern site boundary;
• provision of Sustainable Urban Drainage scheme; & off-site road infrastructure improvement works.
• Outline drawings and adjacencies can be found at Appendix 6.
12.2 Hospital Building 12.2.1 The proposed hospital building would contain the following key departments;
A&E, Out of Hours GP, Out-Patients Department, Orthopaedics, Combined Assessment Unit, Imaging, Palliative Care, Oncology, Short Stay Unit, Theatres and Endoscopy, Critical Care Unit, Women's Services (containing Maternity, Birthing, etc), and eight generic wards. The remaining services are due to be accommodated in the existing Cresswell Maternity Unit, refurbishment of which is due to be completed by summer 2019.
12.2.2 The reference design of the hospital building has been reached as a result of the individual department floor space requirements and the clinical adjacencies of these departments. This has resulted in a 'radial' or 'sundial' layout, containing three key zones or elements. The first element is the Treatment and Diagnostic Block, containing the main entrance, A&E, Out-Patients Dept, Theatres, Imaging, etc. This is broadly rectangular in footprint, punctuated with lightwells, and orientated with principal elevation to the north- east site entrance. This block is
Commercial in Confidence
June 2013
Page 84 of 164

Redacted for Publication - see front cover
mostly arranged over three floors, with smaller areas of lower ground service accommodation, and variable height monopitch roofs of approximately 19m in height. The second element is the In-Patient Accommodation Block, comprising the generic wards that radiate out from the core building around a central enclosed courtyard. Each arm is rectangular in form, and three storeys in height, with pitched roofs of approximately 20m in height. These units are stepped down into the sloping ground, such that the ridge height would be some 3m lower than the Treatment and Diagnostic Block. The third element is the Women and Children's Block, which is appended to the principal elevation of the main block, and based around its own internal courtyard. It would be two storeys in height with pitched roofs.
12.3 Ward Layout 12.3.1 The layout of the generic ward aims to provide as much natural light and
ventilation as possible whilst delivering care efficiently and effectively.
12.3.2 The large light wells in the middle of the ward create a feeling of spaciousness and increase visibility for both staff and patients across the ward area. The 4 walk-through passageways provide ready access to all rooms and reduce travel distance.
12.3.3 The 8 single rooms at the far end of the ward facilitate a high level of observation due to the proximity of, and design of, the main nurses’ station.
12.3.4 All single rooms have a panoramic window out to the surrounding countryside and large glass panels in the door and into the ward area. This provides both a high level of observation into the room and enables the patient to observe and feel part of the general ward activity. Staff bases will be decentralised with 6 multidisciplinary, touchdown areas positioned throughout the ward enabling observation and interaction with patients.
12.3.5 The Information Technology department is proactively involved in the project and we are currently exploring future technological advances to enhance communication and the delivery of care. It is anticipated for example that the use of telemetry will improve the overall monitoring of patients, alert systems will be put in place for patients at risk of deterioration and/or falling and the recording and access to patient information will be readily available in the patient’s room.
12.3.6 Benchmarking other hospitals with single rooms has shown that when a separate room for socialising is provided this is rarely used. However there is evidence to support the fact that an open plan socialising area is used by patients. The generic ward has a socialising area with a large panoramic window in the middle of the ward which gives equal access for all patients.
12.3.7 Isolation has been cited as a potential negative outcome from the introduction of single rooms. The following key points will ensure that patients do not feel isolated:
• Staff will actively promote the socialising area
Commercial in Confidence
June 2013
Page 85 of 164

Redacted for Publication - see front cover
• Flexible visiting with the potential for overnight stay will ensure that patients have the optimum support from family and friends.
• Large glazed areas into and out of the room enables the occupant to interact with staff, other people and their environment
• Touchdown areas will ensure that staff are positioned throughout the ward
• Improved technology will improve enhance communication for patients
12.3.8 It is worthy of note the average length of stay will be short - circa 3.5 days. Early transfer to Cottage Hospitals will be the norm for rehabilitation/reablement
12.3.9 A socialisation space will be provided to promote interaction between patients and extended visiting will promote better opportunities to interact with family and friends (thereby reducing the feelings of isolation)
12.4 Ensuite single inpatient rooms 12.4.1 When considering the room sizings for inpatient rooms the Board have taken into
account the current review of Scottish Health Planning Note (SHPN) guidance as set out in SHPN 04/01 (October 2010). They have ensured that the clinical room sizes adopted are as a minimum in line with the recommended SHPN sizings and that all rooms will provide an appropriate environment for the single inpatient rooms as well as the five discrete activity zones you would expect to see:
Core bed space
Bed head services
Sanitary facilities
Clinical support
Family support
12.4.2 As a result of significant research nationally, new guidance contained in CEL 27 (2010) regarding the minimal acceptable levels of single inpatient rooms has been issued, requiring that there should be a presumption of 100% inpatient single room provision in future hospital development.
12.4.3 100% single rooms provision will greatly enhance privacy, dignity and confidentiality for patients. The majority of care will be delivered within the patient’s own room and discussions with Health Professionals will take place in private.
12.4.4 Single room provision lessens the risk of cross infection from airborne viruses. Patients with unrecognised infection or carriers of infection are separable from other patients on admission.
12.4.5 All single rooms will be generic and able to manage any specialist function. Exceptions will be Critical Care, Paediatrics etc. Generic single rooms enables flexibility to meet peaks in activity.
Commercial in Confidence
June 2013
Page 86 of 164

Redacted for Publication - see front cover
12.4.6 Private toilet facilities are more effective in containing C Diff and Norovirus. In addition the generic ward layout means that sections of the ward can be segregated during an outbreak rather than the whole ward.
12.4.7 Movement of patients within the ward will be greatly reduced, as the need to make a 4 bedded room gender specific will be removed.
12.4.8 Single rooms will facilitate flexible visiting, thereby enabling relatives to play a more supportive role in the patient’s care. The size of the single room will enable relatives to stay overnight with the patient where appropriate. In addition, communication between relatives and the multidisciplinary team will be improved with close relatives able to, for example, be with the patient during ward rounds.
12.4.9 Noise will be greatly reduced from the patient’s perspective and they will not be disturbed during the night whilst staff are attending to other patients. A good night’s sleep aids recovery and improves wellbeing.
12.4.10 In summary, by increasing the number of single rooms, patients will have increased privacy and dignity and a reduced risk of acquiring an infection during their stay in hospital. There will also be an added advantage of increased flexibility of use in beds to reflect changes in gender mix and peaks in demand.
12.5 Access, parking and helipad 12.5.1 The existing A75 Garroch roundabout is proposed to be improved to
accommodate a new spur to serve the hospital and the U347n Glen Road. The improvements involve the diameter of the roundabout being enlarged and the geometry of the existing three main spurs being adjusted. The existing route of the Glen Road would be realigned to a more southerly position, connecting to the new southern spur of the roundabout.
12.5.2 The site is proposed to be served by three vehicular accesses. The main access to the site would be via the A75 Garroch roundabout, leading by internal road network to main entrance drop-off and bus stop/s. A secondary and separate access is also proposed for blue light traffic and A&E drop-off direct from the Glen Road at the north-western corner of the site. A further secondary access is proposed for service and delivery vehicles, via the U350n Garroch Business Park public road, which would be managed to prevent regular use by non-authorised traffic. A total of 980 car parking spaces would be provided to serve the development.
12.5.3 A helipad is proposed to the north-western corner of the site, sited to be within close proximity of the A&E department.
12.6 Staff residences 12.6.1 The indicative proposal is to construct 104 single bedrooms for use by individual
clinical (predominantly medical) staff.
Commercial in Confidence
June 2013
Page 87 of 164

Redacted for Publication - see front cover
12.7 Energy centre 12.7.1 The development would be served by a stand-alone energy centre, to be located
to the south-east of the site and adjacent to the proposed secondary service access. The details of this building have not been provided at this stage, nor has any further information been provided on the proposed generating source. However, it should be assumed for the purposes of this planning permission in principle that there will be an associated chimney (this could be as much as 20m in height).
12.8 Landscaping 12.8.1 The existing site is characterised topographically by the hillock to the north of the
site, and the proposed layout intends to utilise site levels to accommodate split levels between the Treatment and Diagnostics Block and the In-Patient Accommodation. The Main Entrance would sit at an indicative level of +20m, with this level being largely maintained to the south of the site (+19m). The finished ground levels would slope down elsewhere, with indicative levels of +14m on the western boundary, +14.5m at the helipad, and +13m at the Garroch roundabout.
12.8.2 Four key landscaped areas are indicated; firstly, the waste material / spoil extracted from the levelling of the site would be used to form a landscaping bund along the eastern boundary; secondly, at the main entrance with a focal landscaping area to assist with wayfinding; thirdly, landscaped gardens between the three blocks of the In-Patient Accommodation Block; and finally, therapeutic gardens within the various internal courtyards. Extensive tree planting is shown across the site as part of the overall landscaping proposal.
12.9 Sustainable Urban Drainage System 12.9.1 An indicative SUDS pond feature is proposed for the south-western corner of the
site (the lowest part of the site) adjacent to the In-Patient Accommodation Block. This pond is proposed to provide attenuation before discharging into an existing outfall from the site to the adjacent Terraughtie Burn.
12.10 Design Development 12.10.1 The reference design has been progressed to RIBA stage C and incorporates the
following
• Design concept diagrams • 1:1250 Site layout plans • 1:500 Departmental plans and sections • 1:200 Plans, sections and elevations • 3D computer generated visuals • Whole project ADB room data sheets covering all areas • Standard 1:50 room layout drawings. • Planning and stakeholder consultation statements
Commercial in Confidence
June 2013
Page 88 of 164

Redacted for Publication - see front cover
• AEDET report and design vision statement • ACOP 2007 CDM hazard identification. • Design reports relating to Architectural and Engineering elements
Commercial in Confidence
June 2013
Page 89 of 164

Redacted for Publication - see front cover
12.11 Costing Methodology 12.11.1 The reference design information has informed the estimation of the build cost for
the project. The following paragraphs set out the methodology adopted.
12.11.2 The Schedule of Drawn Accommodation has been priced on a room by room and a department by department basis. The individual rooms within each department were allocated to one of three Functional Area Types:
• Public • Staff • Clinical/Delivery
12.11.3 The Health Planning Cost Guides (HPCG) identifies a rate to apply to each of the Functional Area Types and these rates vary on a department by department basis. The rates also include a 5% contingency to deal with design risk given that the rates are being applied to costs associated with a project that is not fully designed at this stage.
12.11.4 The Schedule of Accommodation also identifies the gross floor area included within each department, including space occupied by internal partitions etc.
12.11.5 In addition to pricing the Schedule of Accommodation, the technical advisers also assessed the cost impact of the unique items and Site/Design Premiums associated with the Reference Design. This process of cost adjustment and their incorporation within the Technical Cost assists in developing a budget which more appropriately reflects the specific design proposals for the development.
12.11.6 Technical Cost 3, on which the financial case is based, reflects the key design features of the Reference Design proposed for the new hospital, these include:
• Wall to floor ratios associated with the hub and spoke design • The incorporation of light wells in ward blocks • The requirement for 19m2 single occupancy bedrooms • Proposed roof details, including the provision of “Green roof” • Site specific works associated with ground conditions and topography • The inclusion of residential accommodation for staff
12.11.7 In recognition that there are aspects of the Reference Design which are departures from the benchmark data used to formulate the HPCG departmental rates, the advisers incorporated Site/Design Premiums within Technical Cost 3.
12.11.8 The site/design premiums include the following:
• Piled Hybrid Foundations • Cut & Fill • Increased lifts allowance • Contemplation space design • Roof and Canopies
12.11.9 The above has resulted in a forecast construction cost that is outlined further in the Financial Section
Commercial in Confidence
June 2013
Page 90 of 164

Redacted for Publication - see front cover
COMMERCIAL CASE
Commercial in Confidence
June 2013
Page 91 of 164

Redacted for Publication - see front cover
13 PROCUREMENT ROUTE ASSESSMENT
13.1 Overview 13.1.1 As part of the Scottish Government budget announcement on 17 November
2010, £2.5bn of revenue funded investment pipeline was identified of which £750m related to NHS Scotland projects. Specific provision was incorporated to support the delivery of the Dumfries and Galloway hospital project utilising the Non Profit Distributing (NPD) programme supported by the Scottish Futures Trust (SFT). The project is also incorporated within the Scottish Government Infrastructure Investment Plan published on 4 February 2013.
13.1.2 The Board has worked closely with SFT during the OBC development stage of the project so that it can clearly understand their requirements in considering the merits and practicalities of an NPD procurement.
13.1.3 Other aspects of the project procurement process are outlined in the next section of the OBC
13.2 Key Features of the Assessment 13.2.1 The guidance sets out a 3 stage process covering:
Stage 1 – Programme Level Assessment
Stage 2 – Project Level Assessment
Stage 3 – Procurement Level Assessment
13.2.2 For the projects identified as revenue funded at Scottish Government level, a quantitative comparison of value for money between traditional capital procurement (i.e. using the Conventionally Procured Assessment Model) and revenue funding routes is no longer required nor is the associated technical guidance.
13.2.3 It sets out general guidance to value for money appraisal and its demonstration through business cases. For the purposes of health projects this is established within the Scottish Capital Investment Manual (SCIM) and supported by further guidance from SFT.
13.2.4 For health projects at OBC stage the guidance specifically requires Boards to qualitatively consider procurement options, and as part of this evaluation, complete the VfM checklist set out within Appendix 7.
13.3 Proposed Procurement Route 13.3.1 Having considered the requirements of the SFT guidance and completed the
qualitative evaluation, the Board considers that the Non Profit Distribution (NPD) procurement route is the appropriate procurement approach for the project.
13.3.2 The key factors influencing the selection of this approach are:
Optimises risk allocation via the use of performance based payment incentives enshrined in the project agreement
Commercial in Confidence
June 2013
Page 92 of 164

Redacted for Publication - see front cover
There will be few if any anticipated derogations required from the standard NPD contract
There has been a strong focus on ensuring adequate flexibility as part of the development of clinical requirements
The level of design work undertaken to date provides for further innovation across the procurement phase of the project
Acquisition of the proposed site is well progressed ensuring that this will not cause a delay to the project
The Board has established a sound governance and management structure for the project
The Board has already appointed technical, financial and legal advisers to augment its own resources and has appointed a Project director with recent experience of successfully delivering PPP procurement in health
The scale of the project ensures that transaction costs will be justifiable
It is anticipated that there will be significant market interest in the project
The enhanced stakeholder involvement and public interest representation in the management of the project via the Public Interest Director.
13.4 Procurement Strategy and Process 13.4.1 The procurement strategy has been developed in conjunction with the
Commercial Workstream associated with the project and includes inputs from the Board’s Technical Advisors, Legal Advisors and Financial Advisors. A full copy of the strategy is provided at Appendix 8.
13.4.2 The key aims of the procurement strategy are to:
Ensure a robust and explicit procurement process and carry out appropriate and rigorous evaluation of the bidders technical, legal and financial proposals throughout to understand the basis of the bids.
To demonstrate, as a condition for success, adherence to UK best practice combined in ISO10845 and BS 8534 to the need for cost effectiveness of the process; competition between bidders; transparency of process and equitability of evaluation
Comply with the requirements of Competitive Dialogue.
Ensure the maximisation of benefits associated with having a well developed reference design for the new facility
Promote community benefits
13.4.3 The document covers the key stages associated with the procurement process including:
Use of a Prior Information Notice (PIN)
Publication of OJEU notice
Commercial in Confidence
June 2013
Page 93 of 164

Redacted for Publication - see front cover
Development and application of Pre-Qualification Questionnaire (PQQ) and associated Information Memorandum (IM)
Development and application of Invitation To Participate in Dialogue (ITPD) and associated tender documents
Tender evaluation to select preferred bidder
Activity to achieve financial close
13.4.4 The main requirements identified within the procurement strategy are:
The initial pre-qualification process should shortlist 3 bidders for the Competitive Dialogue (CD) process. This is in line with recognised practice as noted in the document.
All shortlisted bidders will be provided with the final tender template as part of the Invitation To Participate in Dialogue pack. This will confirm evaluation criteria and will be used to inform discussions throughout the CD process to help bidders shape compliant tenders.
The CD process will be split into 4 stages with a review process associated with each stage.
At the end of stage 2 a formal evaluation is proposed of bidders solutions developed to date. Dependant on the outcome of this review, one of the shortlisted bidders may be dropped from the process and the remaining 2 bidders taken forward to stage 3.
At the end of stage 3 the remaining bidders will prepare and submit a draft of their final tenders. This will be reviewed for compliance by the board’s evaluation team whilst dialogue is still open.
During stage 4 feedback will be given to bidders on their draft tenders. Dialogue will formally close when the Authority is satisfied that all bidders are in a position to submit fully compliant tenders. Only then will bidders be invited to submit their final tenders.
Sets of evaluation criteria are being developed by the project team and the Board’s advisors taking into account available SFT and other guidance and the specific context of the project stages. These cover the pre-qualification, interim and final bid stages. Details of these evaluation criteria are set out in the procurement strategy and ITPD documentation. Particular attention has been given to the evaluation of community benefits.
Commercial in Confidence
June 2013
Page 94 of 164

Redacted for Publication - see front cover
13.4.5 The procurement process formally commences with publication of the OJEU notice a draft copy of which is provided at Appendix 9. At this point the fully developed PQQ and IM documents will be provided to organisations applying to participate.
13.4.6 The ITPD is also in preparation. The timing of OJEU publication is driven by approval of planning in principle and approval of the Outline Business Case by CIG. Both these milestones are expected to be achieved in spring 2013 with OJEU publication currently programmed for June 2013.
13.5 Community Benefits 13.5.1 NHS Dumfries and Galloway seek to maximise potential Community Benefits
arising from the Acute Services Redevelopment Project and to ensure that such benefits are seen as a 'golden thread' within our procurement strategy linked to our overarching objectives in relation to sustainability and benefits realisation plan. Within the procurement strategy Community Benefits will be emphasised as a key bidder evaluation criteria at the interim and final bid evaluation stages.
13.5.2 Bidders will be required to submit details of their proposals to actively promote and sustain such benefits, by, for example how their own business and employment policies will promote local employment, training and business opportunities with small and medium sized enterprises (SMEs). Bidders will be required to set out their proposals on how they will collaborate with established community benefit initiatives (e.g. existing local authority frameworks, trade associations and other similar organisations operating in Dumfries and Galloway).
13.5.3 Underpinning such initiatives, the Board will seek to incorporate ‘social clauses’, compliant with current EU procurement legislation, in the form of contract performance conditions into the Project Agreement with the bidders in relation to jobs, training and business opportunities. This approach, described as ‘targeted recruitment and training’ (TRT) will be actively used by the Board to actually monitor the bidder’s performance in realising such benefits post award of the contract during the construction and operational phases. At the prequalification stage, bidders past performance in the area of using and engaging with SMEs will be scrutinised and evaluated. The relative weighting of such criteria will feature prominently within context of the proposed strategic and management approach category. Such criteria will also feature in the evaluation of bidders interim and final proposals as a key consideration in the assessment of the most economically advantageous tender.
13.5.4 The Board will also seek to promote the profile and awareness of such benefits by engaging with capacity building intermediaries such as the Construction Skills Council to obtain advice on communications, setting of targets and training and development schemes. The Board will also be considering owing to our geographical location and social deprivation characteristics, potential linkages and advantages of using the European Investment Bank as a source of funding:
Commercial in Confidence
June 2013
Page 95 of 164

Redacted for Publication - see front cover
having a well developed and articulated strategic approach to Community Benefits will enhance our abilities to attract such funds
13.6 Conclusion 13.6.1 The NPD model has been identified as the preferred procurement route for the
project in the Scottish Government’s document ‘Scottish Spending Plans and Draft Budget 2011-12’. This is supported by the VFM assessment and by a number of key factors such as significant market interest in the project and that the project is viable, desirable and achievable.
Commercial in Confidence
June 2013
Page 96 of 164

Redacted for Publication - see front cover
14 OTHER PROCUREMENT ISSUES
14.1 Overview 14.1.1 In addition to evaluating the merits and practicalities of the NPD procurement, the
Board has also spent time considering a range of other commercial issues associated with the project, but falling outwith the scope of the NPD arrangements, these include:
The future use of the Cresswell wing
Acquisition of the new hospital site
Enabling works on the new site
Demolition of the existing hospital and disposal of the remaining site
14.1.2 The current status and commercial considerations for each is outlined below.
14.2 Cresswell Wing 14.2.1 Located on the existing DGRI site, the Cresswell wing is provided through a
Private Finance Initiative (PFI) project agreement with Dumfries Facilities Ltd. The agreement was signed in 1999 and the building became operational in 2002.
14.2.2 The building was designed and constructed to provide maternity and day case surgery services and has fulfilled these functions since it commenced in use. The term of the Project Agreement is 30 years from the completion of the facilities i.e. until 2032.
14.2.3 The annual unitary charge paid to Dumfries Facilities for the building is approximately £2m. Unusually for a PFI agreement, the hard facilities management services are provided by the Board via a sub-contract with Dumfries Facilities Ltd’s facilities management contractor, FES Ltd. Soft facilities management services are provided directly by the Board but out with the PFI Project Agreement.
14.2.4 The future use of Cresswell requires further work on the financial and economic case, currently being developed in conjunction with the production of this OBC. Following such work and any negotiation with Dumfries Facilities (DF) with regard to what options are deliverable, and work is being performed on ascertaining more accurate costs associated with the different options along with appropriate accounting treatment considerations. It is the Board’s intention to perform an economic appraisal using NPV cash flows for each option to look at the different uses for Cresswell, along with qualitative considerations, and elect a preferred way forward. The details of this assessment and its outcome will be detailed outwith this OBC document.
14.2.5 In considering the provision of a new District General Hospital on a new site, the Board has therefore sought to establish which services to accommodate within the Cresswell wing on the basis that it is retained.
Commercial in Confidence
June 2013
Page 97 of 164

Redacted for Publication - see front cover
14.2.6 A range options were considered for the future use of Cresswell and submitted to NHS Dumfries and Galloway Project Board in September 2012. This was the culmination of work on future use that had taken place throughout 2012.
14.2.7 The criteria for including services in Cresswell were agreed as follows:
• Are clinically appropriate to be in a facility remote from services of a district general hospital
• Require to be in a highly serviced building originally designed for acute clinical services
• Have a coherence with other clinical services to be housed in Cresswell
• Reduces the amount of new build as part of the new hospital development
• Are in line with Board’s property strategy to concentrate on four site within Dumfries
14.2.8 Following extensive discussions several services were identified as being suitable for location within Cresswell and a number of option appraisals were performed.
14.2.9 Following the detailed option appraisals outlined above, concerned with the future of the existing Cresswell facilities, the Board’s confirmed preferred option is to transfer existing day surgery and maternity services into the proposed new build on the grounds of patient safety
14.2.10 Having considered a range of options for the provision of services within the Creswell (on the premise that day surgery and maternity services would be part of the new hospital build) the Board has concluded that the optimal clinical configuration is to house Renal and Ophthalmology services on the ground floor with a range of mainly out-patient services on the first floor and lower ground floor. In this option integrated non-acute Children’s Services would be accommodated at another facility.
14.2.11 The Cresswell wing is fully integrated into the DGRI such that heating; medical gases, oxygen, electricity and fire alarms are routed through the DGRI. For the building to continue to function after the DGRI has moved to a new site, these services will have to be provided in an alternative to enable the building to function independently.
14.2.12 In considering the future function of the Cresswell wing the Board have identified a number of key risks which include:
Completion of negotiations with Dumfries Facilities Ltd - it proves not to be possible to reach an agreement with Dumfries Facilities for a change to the PFI Project Agreement or negotiations with Dumfries Facilities proves to be more difficult than expected resulting in an extended timescale delays.
Increases in costs of remodelling Cresswell - the costs of remodelling the Cresswell wing internally and/or of providing services to the Cresswell wing to
Commercial in Confidence
June 2013
Page 98 of 164

Redacted for Publication - see front cover
enable it to function independently of the DGRI, exceed the estimated costs identified in this paper.
Availability of Capital on the basis that changes would be funded through capital, the level of funding needed to enable the Cresswell to function independently of the DGRI and to allow the remodelling of Cresswell, is not available.
14.2.13 The works would potentially be delivered using the Frameworks Scotland 2 procurement arrangements.
14.2.14 Negotiations have commenced with Dumfries Facilities Limited on the change of use of the Cresswell wing and the impact this may have on the existing PFI agreement.
14.3 Selection and Acquisition of New Hospital Site 14.3.1 In recognising that the preferred solution for the provision of a new District
General Hospital proposed an offsite solution, the Board appointed property advisors to carry out a search for an alternative site in the Dumfries area and thereafter enter into negotiations to acquire the most suitable site.
14.3.2 The process followed involved four key stages as detailed below.
Stage 1: Strategic assessment of potential sites – this involved undertaking a detailed site search within the agreed geographical boundary and provided a list of sites with information in terms of ownership, planning use, infrastructure information, as well as technical and environmental considerations. This produced 22 potential sites.
Stage 2:Initial site evaluation and shortlisting – the Board used a scoring matrix to evaluated the 22 sites identified in the initial search, the list was reduced to 5 potential sites, in addition to the existing DGRI site which were shortlisted for further detailed scrutiny and investigation. At this stage the Board also undertook community consultation on the shortlisted sites.
Stage 3: Final shortlisting – the Board made a final decision to two of the sites taking due account of all of the technical issues and the community responses. The two shortlisted sites were Garroch Loaning and Summerfield.
Stage 4: Negotiations with land owners – On the instructions of the Board the property advisors entered into negotiations with the land owners / land agents to obtain the best terms for the purchase of the sites on the basis that no payment or deposit would be made until planning consent had been granted and the OBC approved.
14.4 Partnership Approach to Planning and Other Issues 14.4.1 NHS Dumfries and Galloway works closely with their Public Sector partner
Dumfries and Galloway Council in many aspects of delivering region wide services. As part of this close partnership working it was decided that the Council
Commercial in Confidence
June 2013
Page 99 of 164

Redacted for Publication - see front cover
should be represented at Project Board level when planning a region wide facility of this magnitude.
14.4.2 The Council’s Head of Planning and Environment was appointed to the Project Board and worked closely with NHS officers during the site selection process and assigned members of his staff to assist in the development of the reference design and the compilation of the Planning in Principle application.
14.4.3 The basis of this relationship was set out in a Planning Partnership Protocol which detailed roles, responsibilities and a programme for the delivery of the Planning in Principle approval.
14.4.4 Throughout the site selection process assistance was provided in identifying a long list of sites and in gathering relevant information to inform the selection of a short list. Planning officers advised on compatibility of sites with Local plan designation.
14.4.5 The Head of Planning and Environment attended the site selection meetings when parties from various groups came together to assess the shortlisted sites and recommend a preferred site to Project Board. The Head of Planning was able to assist the selection process by clarifying regional policy on a number of matters being discussed.
14.4.6 A Senior Planner from the Council was appointed to the Reference Design Working Group and was able to observe and contribute to discussion as the reference design was being developed. This meant that Council Officials were fully aware of how the proposed design was evolving well in advance of any formal submission. It also ensured that there was no abortive work being carried out as Planning requirements and restrictions influenced the design at the earliest stage.
14.4.7 This close working relationship has resulted in a very smooth approval process which received the minimum of objections from the general public and none from statutory consultees.
Commercial in Confidence
June 2013
Page 100 of 164

Redacted for Publication - see front cover
14.5 Site Option Appraisal 14.5.1 Between October and December 2011, NHS Dumfries and Galloway carried out
a public engagement and option appraisal process on its plans to build a new acute hospital to replace the existing Dumfries and Galloway Royal Infirmary. The Board’s preferred option is to build the new hospital on a new site, but it agreed to proceed to formal consultation with five options, i.e. four new site options and the existing site. Formal consultation took place between 11 January 2012 and 11 April 2012. The consultation covered five sites in total, four new sites on the outskirts of Dumfries and the existing hospital site.
14.5.2 The sites consulted on were;
Site A – Garroch
Site B – Summerfield
Site C – Heathhall
Site D – Locharbriggs/ Tinwald Downs
Site E – Existing hospital site
14.5.3 Extensive public consultation on the suitability of the sites was undertaken. The quality of the consultation was reviewed by the Scottish Health Council.
14.5.4 A variety of methods were used to engage and consult with the population of Dumfries and Galloway including;
display stands
information leaflet, map and individual topic information sheets
advertising via posters, press advertisements, website and Twitter
Participatory Appraisal which included street work, through existing Building Healthy Communities groups, which engaged with 928 people
12 ‘drop-in’ sessions were held at venues across the Board area and open to all which were attended by 203 people
NHS staff attended 31 “Invite Us” sessions, which were pre-arranged meetings of a variety of groups covering older people, young people, disability groups, faith groups and community councils, where the Board spoke with 779 people.
14.5.5 The Board worked with its partners including Dumfries and Galloway Council (for example by working with the Planning Department to identify the -site locations for a new hospital) and the Scottish Ambulance Service (by analysis of the impact on Scottish Ambulance Service operations if the new build was off-site).
14.5.6 Selecting a preferred site involved both a qualitative and a quantitative assessment. The method chosen to identify the Preferred Site was to agree a number of Benefit Criteria, to agree the weighting to be given to each Benefit
Commercial in Confidence
June 2013
Page 101 of 164

Redacted for Publication - see front cover
Criteria and then to score the Benefit Criteria. This approach covered the qualitative element of the overall assessment.
14.5.7 The quantitative element of the assessment included the likely purchase price of the site, estimated enabling costs such as road alterations and utility provision.
14.5.8 At its 18th April meeting the Project Board agreed that the qualitative criteria should account for 75% of the score and the quantitative criteria for the remaining 25%. This significant difference reflects the fact that the cost of site purchase and enabling works, although estimated to be several million pounds, is a very small proportion of the overall project cost. The Project Board felt, therefore, that it did not wish the choice of site to be heavily influenced by cost. This view was supported by the Scottish Government and Scottish Futures Trust (SFT) representatives on the Project Board.
14.5.9 The various options were then scored at a workshop attended by a range of stakeholders representing patients, staff and other groups including Scottish Futures Trust and Dumfries and Galloway Council
14.5.10 The site with the overall highest score was Garroch Farm. The Garroch site scored highest even after a range of sensitivities were taken into account. The Garroch site was approved by the NHS Dumfries & Galloway Board in May 2012.
14.6 Acquisition of Garroch Farm Site 14.6.1 Negotiations took place with the parties representing the respective land owners
and a stage reached at which each party had finally proposed best terms.
14.6.2 In line with the requirements of the NHS Scotland Property Transactions Handbook, the property advisers subsequently entered into discussions with the land agent for the site to establish Heads of Terms and the commence legal negotiations.
14.6.3 A contract for the purchase of 18.3 Hectares of land forming part of Garroch Farm was signed on 18 January 2013.
14.6.4 The missives included two suspensive conditions, namely:
The acquisition by the purchaser of all rights in respect of third party land interests (whether by way of purchase or servitude or otherwise) considered by the purchaser at its sole decision and discretion to be necessary for the full and successful conclusion of the proposed development of the property and that on terms satisfactory to the purchaser at its sole decision and discretion.
The grant of formal approval by the Scottish Government Capital Investment Group of the Outline Business Case for the proposed development of the property (for the avoidance of doubt, such approval will require inter alia the prior grant of Planning Permission in Principle for the proposed development of the property).
14.6.5 A target date for purification of the suspensive conditions is 30 June 2013 following consideration of the Outline Business Case by the Health Department
Commercial in Confidence
June 2013
Page 102 of 164

Redacted for Publication - see front cover
Capital Investment Group in May 2013. A long stop date for purification of missives is 30 September 2013. Interest on the agreed purchase price will be payable at from 1 July 2013 up to settlement date or at a rate of from the date of purification of suspensive conditions.
14.7 Enabling Works on the New Hospital Site 14.7.1 This will include the provision of services to the new site (terminating at the
proposed location for the new energy centre) as well as road infrastructure changes to secure appropriate site access / egress.
14.7.2 A Section 69 agreement has been signed and the responsibility to deliver local road alterations has passed to D&G Council. The Council has general powers to make agreements under Section 69 of the Local Government (Scotland) Act 1973. This gives the Council power “to do anything (whether or not involving the expenditure, borrowing or lending of money or the acquisition or disposal of any property or rights) which is calculated to facilitate, or is conducive or incidental to, the discharge of their functions”. The hospital will not be delayed even if the Council fail to maintain the agreed schedule for delivery.
14.7.3 Discussions with Transport Scotland, the agency with responsibility for alterations to the trunk road network are well underway and it is hoped that these discussions will be complete within the next six weeks. These are likely to be secured through service utility providers and other contractors. There will be Transport Scotland and Local Authority input into the proposed road infrastructure changes.
14.8 Disposal of Current Hospital Site 14.8.1 A draft masterplan outlining the proposals for disposing of the surplus
components of the existing DGRI site has been developed by the Board. The key aspects of the masterplan are summarised below.
Timeframe for disposal is financial year 2021/22
The Board will retain the Cresswell building and Dental Centre along with parking and access provisions to support this, all other parts of the site will be disposed of. The refurbishment work on Cresswell cannot commence until the new hospital is operational in 2018. The refurbishment of Cresswell will take 12/14 months to complete before any demolition work can commence.
Technical issues that impact on value include demolition costs, site servicing costs, planning permission, planning gain, road infrastructure improvements.
Commercial in Confidence
June 2013
Page 103 of 164
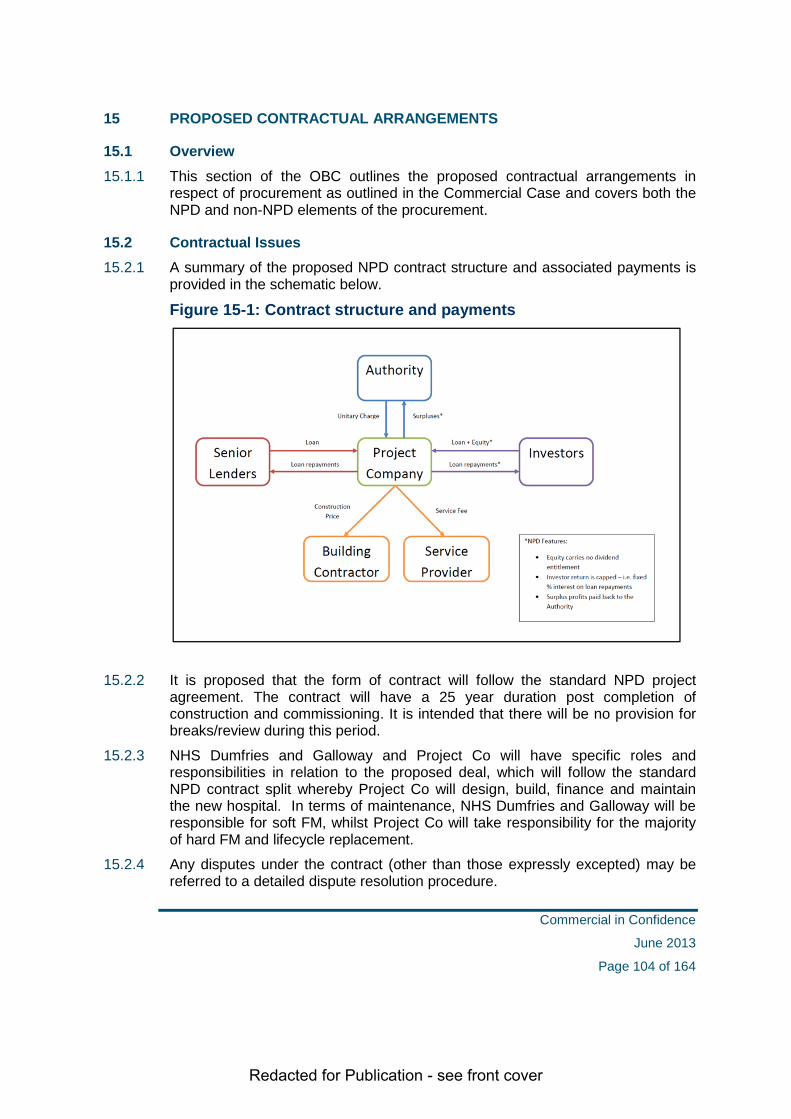
Redacted for Publication - see front cover
15 PROPOSED CONTRACTUAL ARRANGEMENTS
15.1 Overview 15.1.1 This section of the OBC outlines the proposed contractual arrangements in
respect of procurement as outlined in the Commercial Case and covers both the NPD and non-NPD elements of the procurement.
15.2 Contractual Issues 15.2.1 A summary of the proposed NPD contract structure and associated payments is
provided in the schematic below.
Figure 15-1: Contract structure and payments
15.2.2 It is proposed that the form of contract will follow the standard NPD project agreement. The contract will have a 25 year duration post completion of construction and commissioning. It is intended that there will be no provision for breaks/review during this period.
15.2.3 NHS Dumfries and Galloway and Project Co will have specific roles and responsibilities in relation to the proposed deal, which will follow the standard NPD contract split whereby Project Co will design, build, finance and maintain the new hospital. In terms of maintenance, NHS Dumfries and Galloway will be responsible for soft FM, whilst Project Co will take responsibility for the majority of hard FM and lifecycle replacement.
15.2.4 Any disputes under the contract (other than those expressly excepted) may be referred to a detailed dispute resolution procedure.
Commercial in Confidence
June 2013
Page 104 of 164

Redacted for Publication - see front cover
15.2.5 At the end of the contract the facility will be handed back in accordance with the contract’s comprehensive Handback Procedure. This covers the condition of the facilities at the end of the contract, with provision for inspection and completion of any subsequent works required.
15.3 Required Services 15.3.1 A summary of the technical scope of works associated with the design,
construction and maintenance of the new hospital facilities at Garroch Loaning is provided at Appendix 10. It describes the split of the works that will be delivered through the NPD contract and those that will be delivered outwith the NPD contract.
15.4 Proposals for Risk Transfer 15.4.1 As part of the risk workshops undertaken during the OBC stage, a risk register
has been prepared covering all risks relevant to the project. This outlines the proposed allocation of risks between NHS Dumfries and Galloway and the private sector.
15.4.2 The standard PPP Risk Allocation Matrix within the SCIM was used to determine which risks were potentially acceptable to transfer and which were likely to be retained by the Board.
15.4.3 Risks associated with the NPD procurement aspects of the project will follow the standard allocation for an NPD project.
15.4.4 NHS Dumfries and Galloway will, via the Project Agreement, transfer the relevant risks to the private sector. As part of the ITPD documentation, potential bidders will be required to confirm their agreement to the proposed risk allocation.
15.4.5 A copy of the project risk register is included as Appendix 11. Details of the proposals to manage risks is outlined within the Project Management Case.
15.4.6 The proposed changes to the use of the Creswell wing are not anticipated to impact on the level of risk or its apportionment between the Board and Dumfries Facilities Ltd.
15.5 Proposed NPD Payment Mechanism 15.5.1 This section describes the charging mechanism that will govern the payments
made by NHS Dumfries & Galloway to the NPD operator.
15.5.2 Such arrangements are controlled under NPD and similar projects by a payment mechanism that forms part of the contractual documentation. SFT have provided a standard form payment mechanism, the use of which will form part of the conditions of the provision of revenue support for NPD projects. The NPD Standard will, therefore, form the basis of the mechanism to be used in this project. However, the NPD standard has been designed on a generic basis for any type of accommodation project and will need to be amended for use in an acute NHS scheme.
Commercial in Confidence
June 2013
Page 105 of 164

Redacted for Publication - see front cover
15.5.3 The mechanism calculates the amount per month that will be paid to the operator, based on the annual unitary charge, indexed as agreed in the contract, converted to a monthly sum from which various deductions may be made if applicable.
15.5.4 Deductions are made where the operator fails to perform services as specified in the contract documents, these being a fixed amount per failure based on the severity of the failure.
15.5.5 Deductions are made where an area of the facility is deemed to be unavailable, or unsuitable for use in terms of, for example, temperature, health and safety or lighting. The size of the deduction is dependent on the importance placed on the area in question, with the facility being divided up into areas each of which is given its own weighting. At a certain threshold it is possible for the Board to make a deduction for the entire facility.
15.5.6 The operator is given a period of time to rectify the problem before a deduction is made, and deductions escalate if there is a repeated occurrence.
15.5.7 The NPD mechanism differs in two key areas to those used in previous NHS mechanisms.
The NPD standard assumes that the Facilities will not be required to be available 24/7 and operates Deductions on the basis of whole days rather than several sessions within a day. This is unlikely to be workable in an operational hospital that is in use constantly;
The large number of rooms in a major healthcare facility and the fact that they are generally in constant use means that calculated deductions are likely to be very small. In the NHS Standard, the mechanism uses a concept of ‘gearing’ that increases the value of a calculated deduction by a factor of, for example, three in order to ensure that the deduction acts as sufficient incentive to restore availability as quickly as possible.
15.5.8 It is proposed that the NPD Standard be amended to include drafting adopted from the NHS Standard to address the above issues. Such amendments have been agreed with SFT on other NHS NPD projects and so should form acceptable derogations from the NPD Standard.
15.6 Non NPD Contractual Issues 15.6.1 The contractual issues relating to the elements of the project to be procured
outwith the main NPD contract include:
Site acquisition
Enabling works (new site)
Enabling works Creswell
Changes to the Creswell PFI contract
Commercial in Confidence
June 2013
Page 106 of 164
Redacted for Publication - see front cover
Site Acquisition 15.6.2 The agreed Heads of Terms are subject to two suspensive conditions:
The acquisition by the purchaser of all rights in respect of third party land interests (whether by way of purchase or servitude or otherwise) considered by the purchaser at its sole decision and discretion to be necessary for the full and successful conclusion of the proposed development of the property and that on terms satisfactory to the purchaser at its sole decision and discretion.
The grant of formal approval by the Scottish Government Capital Investment Group of the Outline Business Case for the proposed development of the property (for the avoidance of doubt, such approval will require inter alia the prior grant of Planning Permission in Principle for the proposed development of the property).
Enabling works 15.6.3 New site enabling works relating to services will be secured through appropriate
contractual arrangements direct with utility companies. Road and access improvements will likely be secured through a combination of grants to Dumfries and Galloway Council and Transport Scotland framework agreements.
15.6.4 It is anticipated that the proposed changes to the Creswell wing will be procured through the Frameworks Scotland 2 arrangements. As such, from a contractual perspective, these will be covered by the provisions of the NEC3 contract.
Changes to the Creswell Contract 15.6.5 It is anticipated that any required changes to the Creswell contract will be
secured by way of a Supplemental Agreement to the Project Agreement held with Dumfries Facilities Ltd (DFL). This will effectively incorporate a formal contract variation which outlines the impact on services provided and will form an annex to the original agreement.
15.6.6 The contract variation is in progress and will be issued in June 2013 to Dumfries Facilities for their response. A Cost Tech 1 is currently in preparation to support the Schedule of Accommodation for the Cresswell revision. Dumfries Facilities are required to respond whether it is a project that they would wish to take forward and seek funding. DFL, in early discussions, have advised that they are content that the Project is taken forward and funded by the Board. The work on Cresswell will not commence until post 2018 and will not delay or impact on moving the main NPD project forward
15.7 Personnel Implications 15.7.1 NHS Dumfries & Galloway staff will transfer to the new hospital under
organisational change arrangements.
15.7.2 For hard FM services to be delivered by the NPD contractor there will be an opportunity for relevant NHS Dumfries & Galloway staff to transfer under the
Commercial in Confidence
June 2013
Page 107 of 164

Redacted for Publication - see front cover
TUPE regulations. Staff in these services who choose to remain employed by NHS Dumfries & Galloway will be treated in accordance with employment and organisational change policies.
15.7.3 Where staff do not wish to TUPE, redeployment within NHS Dumfries & Galloway would be supported.
15.8 Accountancy Treatment 15.8.1 Further details of the proposed accountancy treatment associated with the
project is provided within the Financial Case.
Commercial in Confidence
June 2013
Page 108 of 164

Redacted for Publication - see front cover
FINANCIAL CASE
Commercial in Confidence
June 2013
Page 109 of 164

Redacted for Publication - see front cover
16 FINANCIAL APPRAISAL
16.1 Overview 16.1.1 This section of the OBC sets out the financial impact of the preferred option. The
primary aim is to demonstrate the overall affordability position for both NHS Dumfries and Galloway and Scottish Government.
16.1.2 The case will clearly highlight the impact of the following: Recurring revenue costs
Capital costs
Non-recurring costs
The associated accountancy treatment
16.1.3 The following case will describe where additional costs are expected, what type of costs these are classified as, the clarity on the source of funding and ultimately demonstrate affordability, the diagram below demonstrates this.
Figure 16-1: Financial framework
Site acquisition
Hospital development
Equipment Gp2,3 and 4
Off site capital works
SG Project Specific Capital
Allocation
NHS Board Revenue
Enabling works
Pay and Non Pay costs
SG Revenue contribution
Sources of funding
Sour
ces o
f inp
uts
Acute Services Redevelopment Project – Financial Framework
Transition & Commissioning
Project Running Costs
Capital
Non Recurring Revenue
Recurring Revenue
Types of Cost
Commercial in Confidence
June 2013
Page 110 of 164
Redacted for Publication - see front cover
16.1.4 All costs have been identified using assumptions generated from the input of external advisors as well as the senior management team at NHS Dumfries & Galloway.
16.1.5 The cost models described will continue to be reviewed and refined as further detailed work is undertaken.
16.2 NPD Funding Model Overview 16.2.1 This project is being taken forward under the Non Profit Distributing funding
model (NPD); this is a revenue funded scheme unlike the traditional capital funded route most commonly used in recent NHS Dumfries & Galloway projects.
16.2.2 The NPD model was developed and introduced as an alternative to and has since superseded the traditional Private Finance Initiative (PFI) model in Scotland.
16.2.3 The NPD model is defined by the following broad principles:
No dividends are payable to shareholders
Capped private sector returns
Surpluses are returned to the public sector
Enhanced stakeholder involvement in the management of projects
16.2.4 The NPD model aims to eliminate uncapped equity returns and limit these returns to a reasonable rate set through competition. The NPD model is not a “not for profit” model – contractors and lenders are expected to earn a normal market rate of return. It aims to retain the benefits of equity-based PPP structures such as:
Optimum risk allocation
Whole-life costing
Maximised design efficiencies
Robust programme of lifecycle maintenance and facilities management
Performance-based payments to the private sector
Single point delivery system
Improved service provision
Commercial in Confidence
June 2013
Page 111 of 164

Redacted for Publication - see front cover
16.2.5 In practice this means that instead of paying at point of construction for the building, NHS Dumfries and Galloway will enter a contract with an NPD provider who will design, build, finance and maintain the building for a period of 25 years. Once the building has formally been handed over to NHS Dumfries & Galloway a monthly fee becomes chargeable; this is referred to as the unitary charge and is subject to deductions for availability and performance failures on a monthly basis. No charge is payable until the building is handed over unlike in a traditional capital construction where payments are being made through the duration of the construction phase.
16.2.6 At the end of the 25 year contract the building ownership is retained in full by NHS Dumfries & Galloway and the unitary charge is no longer payable. The Board would then be required to make a decision about the continued maintenance of that building.
16.2.7 In terms of the funding arrangements the SGHSCD letter of 22 March 2011 set out the agreed levels of revenue support which will be made available towards the unitary charge, this is set out below.
Figure 16-2: NPD unitary charge funding arrangements
16.2.8 The conditions attached to the funding include amongst other elements the construction cap that will apply to the project. This is the expected construction cost including the cost of the building, IT infrastructure, Group1 (supply and installation) and 2 (Installation only) equipment and private sector design fees post financial close that the project must deliver within. The Board is expected to deliver the project within the project scope presented.
Commercial in Confidence
June 2013
Page 112 of 164

Redacted for Publication - see front cover
17 RECURRING REVENUE
17.1 Overview 17.1.1 Recurring revenue expenditure are those costs which NHS Dumfries and
Galloway incur on an ongoing basis to provide health services. They continue to recur year on year until a change is instigated which will remove or reallocate these costs. These are unlike non-recurring costs which are one off and are discussed later in the case.
17.1.2 When considering the recurring revenue implications of this project it is useful to understand the financial context within which it sits. The following table gives an indication of the 2012/13 recurring budgets for the existing DGRI hospital including Cresswell.
Figure 17-1: DGRI baseline budget
Directorate
WTE Budget
£'000 Recurring
Acute Services Directorate 915.19 55,828£ Diagnostics Directorate 175.30 11,360£ Operational Services Directorate 231.33 10,424£ Womens & Childrens Directorate 164.01 9,018£ All ied Health Professionals 102.73 4,922£ Pharmacy 42.82 2,062£ Patient Administration 64.30 1,468£ Education Centre 6.05 210£ Infection Control 8.50 333£
1710.22 95,625£ Depreciation 0.00 2,115£ Cresswell Unitary Charge & Depn 0.00 1,723£
0.00 3,838£ Total direct DGRI costs 1710.22 99,463£
This is 2012/13 total recurring budget including pays, non pays and income as at Dec12 identified as being associated with DGRI. Does not include overheads
Commercial in Confidence
June 2013
Page 113 of 164

Redacted for Publication - see front cover
17.1.3 Given the existing level of investment within the current DGRI it is not possible to do a full costing exercise at this time. The recurring revenue section will focus on the areas where the most significant additional costs are anticipated.
17.1.4 The underlying assumption is therefore that existing budgets for all areas not included in this review will be sufficient to allow any service redesign which is required as well as continuing to deliver Cash Releasing Efficiency Savings (CRES).
17.1.5 Any changes to this assumption will require to be supported by future financial plans.
17.1.6 As will be seen the recurring revenue implications for the project are largely attributable to the NPD unitary charge however there are a number of other costs elements which need considered as part of the overall affordability of the project. These are illustrated below.
Figure 17-2: Affordability cost elements
17.1.7 The areas identified will now be considered in turn identifying the additional investment required and the sources of funding available to deliver this.
Commercial in Confidence
June 2013
Page 114 of 164

Redacted for Publication - see front cover
17.2 Unitary Charge Payment 17.2.1 The unitary charge is the estimated monthly cost which will be payable for the
design, build, finance and maintenance of the new hospital over the life of the contract.
17.2.2 The Board’s appointed financial advisors prepared a Shadow Bid Model. This is a model which aims to estimate the unitary charge the private sector provider is likely to seek.
17.2.3 The following information has been used to produce this model:
Estimated capital construction costs from Technical Cost 3 which has been produced by the Technical Advisors (Appendix 12 );
Estimated lifecycle and hard facilities management costs also identified in Technical Cost 3;
The value of risks which the NPD bidders may include in their submission prior to mitigation which was calculated as part of the quantification of the risk register at
Programme information as currently forecast reflected in the Management Case.
Funding assumptions provided by SFT (Appendix 13 );
Commercial in Confidence
June 2013
Page 115 of 164

Redacted for Publication - see front cover
17.2.4 The table below shows the key input costs used in the model.
Figure 17-3: Input costs
17.2.5 The construction cap is estimated to be circa £180m based on the information
presented above. This is the expected construction cost including the cost of the building, IT infrastructure, Group1 (supply and installation) and 2 (Installation only) equipment and private sector design fees post financial close.
17.2.6 Inflation which is presented above is an estimate of the price movement from current day prices Q2 2013 to mid point of construction estimated to be Q3 2016. This has been calculated using the most up to date Building Cost Information Service all-in tender price index. The implied inflation allowance is % giving rise to a current estimate of £ m; however this will continue to be reviewed as the project moves through the procurement process.
17.2.7 Using the inputs and assumptions described the model produces a unitary charge payment in the first full year (2018/19) of £ m rising to an estimated £ m in Year 25 giving a total cost of £ m over the lifetime of the contract.
UNITARY CHARGE INPUTS
Element m2 £ per m2 % rate Indicative CostBase Building Costs 53,694 £ £ Stand Alone Energy Centre 975 £ £ External Works 199,068 £ £ 104 Doctors Accomodation 3,120 £ £ Targeted Value Engineering -£ Assumed Competitive Reduction -£ -£
£ Design Fees £
£ Risk £ Anticipated construction cap £ Inflation from Q2 2013 - Q3 2016 £
£ Cost including estimatedinflation 199,890,000£
Lifecycle Costs per m2FM Cost per m2
Base Bulding Cost calculated using baseline HPCGs Q1 2010 209Base Bulding Cost indexed to current day using Forecast BCIS index Q2 2013 224Inflation Mid Point of Construction using Forecast BCIS Index Q3 2016 249
Construction Start 01/04/15Construction Completion 30/06/17Building Handover 22/12/17
Source:
Model Input
Prepared from information received from Mott McDonald on Technical Costing 3 dated 1/5/13. This is re-presented to show construction cap. Mott McDonald Techinical Costing 3 as received is included as Appendix 11
Other Input Information
Commercial in Confidence
June 2013
Page 116 of 164

Redacted for Publication - see front cover
Using the HM treasury real discount rate of 3.5% the net present value (NPV) or cost at current day values is £ m.
17.2.8 The unitary charge rises year on year because the maintenance elements (lifecycle and facilities management costs) as well as the NPD providers’ operational running costs are increased annually based on the Retail Price Index (RPI). The balance of the charge remains flat throughout the duration.
17.2.9 Further detail on the unitary charge estimate per annum is included in Appendix 14.
17.2.10 The following table show the unitary charge and anticipated funding assumptions at current day prices.
Figure 17-4: Unitary charge analysis
17.2.11 Given the significant importance being placed on the unitary charge value to
identify both the funding that NHS Dumfries and Galloway will receive to support this project and the funding NHS Dumfries and Galloway will require to identify to support this development it is important that the level of variability and therefore inherent risk within these figures is carefully considered.
17.2.12 A range of sensitivities have been applied to the unitary charge model by the external advisors some of which would present an additional cost to NHS Dumfries and Galloway, some as an additional cost to Scottish Government and some cost to both parties. Appendix 15 sets out the full range of sensitivities run.
17.2.13 The table below identifies the key variables that would have most significant impact on NHS Dumfries and Galloway recurring revenue consequences.
Anticipated Cost £'000Real Terms Unitary Charge
Funding Assumption
NHS Dumfries and GallowayScottish Government
Commercial in Confidence
June 2013
Page 117 of 164

Redacted for Publication - see front cover
Figure 17-5: Unitary charge sensitivity 1
17.2.14 A number of key variables have a direct impact on the amount of funding which
the Scottish Government will be required to support; the table below identifies the key variables that would have most significant impact on Scottish Government recurring revenue consequences.
Figure 17-6: Unitary charge sensitivity 2
17.2.15 The challenge for NHS Dumfries and Galloway will be to continue to test all of
the design elements to ensure that maximum value for money is delivered for both NHS Dumfries and Galloway and Scottish Government as the sensitivities highlighted above are of significant financial risk to both parties.
Change Sensitivity
NHS D&G Impact per annum
Lifecycle and Hard FM rates are more or less than current estimate
+ 10%/-10%
Increase in construction costs as a direct result of a Board change of scope or project delay resulting in timetable impact (this does not include the potential increase in l ifecycle and hard FM costs)
+ 10%
Change Sensitivity SGHSCD Impact
Swap rate is different to anticipated at financial close
+ 1%/-1%- per annum
Index used in updating HPCGs uses last fixed index rather than forecast
Move from Q2 2013 Forecast (224) to Q4 2012 Fixed (230)
additonal on construction cap
Assumed Competitive reduction not achievedadditional
construction costadditional on construction cap
Commercial in Confidence
June 2013
Page 118 of 164

Redacted for Publication - see front cover
17.3 Depreciation 17.3.1 Depreciation reflects the impact of capital expenditure over its useful life.
17.3.2 The costs described in the later capital section will require to be recorded as assets and therefore the depreciation impact of each requires to be considered.
17.3.3 In addition, the accounting treatment described later highlights that NHS Dumfries and Galloway will be required to record the NPD asset constructed on its balance sheet. Depreciation will therefore be chargeable on this asset also.
17.3.4 The current assumptions being used for depreciation are shown below.
Figure 17-7: Depreciation analysis
17.3.5 As highlighted in the capital section of this case further work is required on the
values in relation to equipment. The final value chargeable for depreciation will depend on two elements: the value of equipment finally procured and the life that is considered appropriate to be applied to that asset. This variable is significant, by increasing the average life by 1 year on current estimates would reduce costs by £ however reducing the life by 1 year can increase costs by k. This
Future Anticipated Charges Current Revised ChangeExisting DGRI - BuildingsExisitng DGRI - ResidenciesCapital Costs - Site AcquisitionCapital Costs - External Enabling WorksCapital Costs - Off Site Capital WorksCapital Costs - Site Clearance CostsCapital Costs - Equipment Group 2&3Accounting Treatment - NPD On B/SheetTOTAL INCREASE IN DEPRECIATIONFunding Assumption Current Revised ChangeNHS Dumfries & GallowayScottish GovernmentTOTAL FUNDING CHANGES
Notes1. No depreciation charges are assumed for the following capital works:
2. The revised equipment estimate is based on an average 8 year l ife
a. Site Acquisiton - no depreciation charged on landb. External Enabling Works - assumed to be either land enhancement or paid as a capital grant therefore no depreciation chargeablec. Site Clearance Costs - no depreciation charged on costs incurred on asset being prepared for sale
3. NPD On balance sheet is estimated to have a post impairment value of £ , depreciation estimate from current valuers
4. Any additional depreciation as a result of an increased asset valuation of Cresswell wil l be require to be supported by NHS D&G, this is included within off site capital works
Commercial in Confidence
June 2013
Page 119 of 164
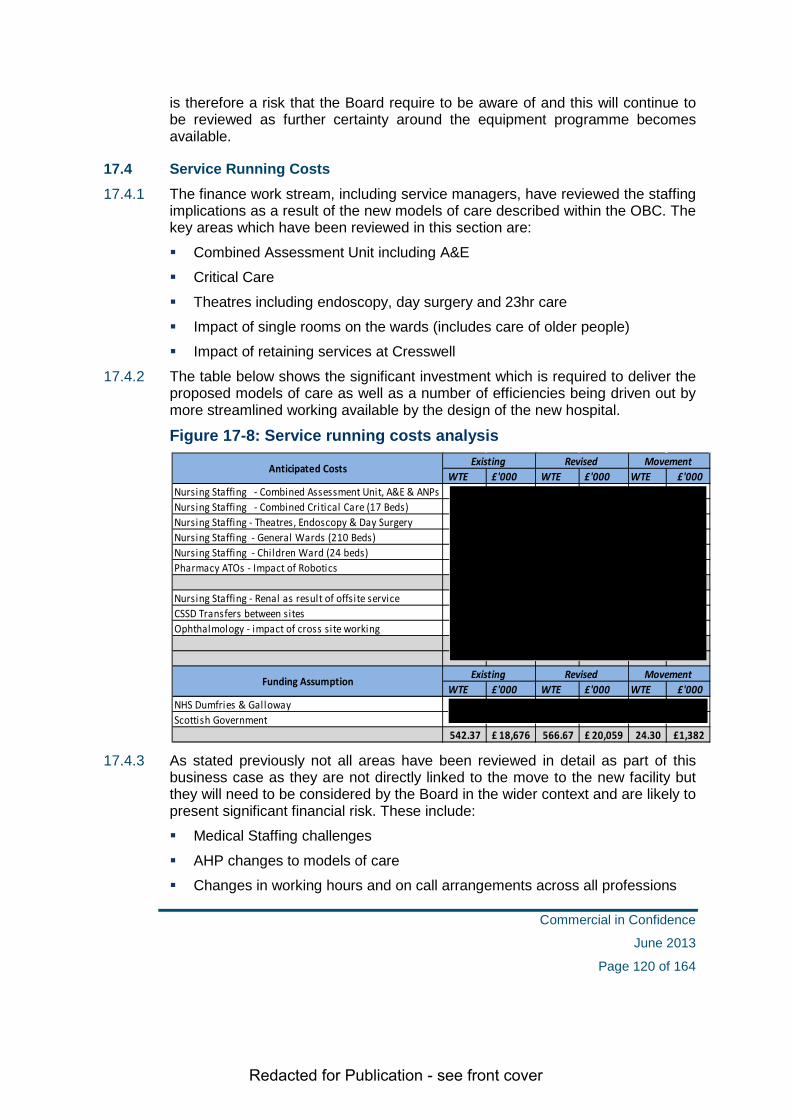
Redacted for Publication - see front cover
is therefore a risk that the Board require to be aware of and this will continue to be reviewed as further certainty around the equipment programme becomes available.
17.4 Service Running Costs 17.4.1 The finance work stream, including service managers, have reviewed the staffing
implications as a result of the new models of care described within the OBC. The key areas which have been reviewed in this section are:
Combined Assessment Unit including A&E
Critical Care
Theatres including endoscopy, day surgery and 23hr care
Impact of single rooms on the wards (includes care of older people)
Impact of retaining services at Cresswell
17.4.2 The table below shows the significant investment which is required to deliver the proposed models of care as well as a number of efficiencies being driven out by more streamlined working available by the design of the new hospital.
Figure 17-8: Service running costs analysis
17.4.3 As stated previously not all areas have been reviewed in detail as part of this
business case as they are not directly linked to the move to the new facility but they will need to be considered by the Board in the wider context and are likely to present significant financial risk. These include:
Medical Staffing challenges
AHP changes to models of care
Changes in working hours and on call arrangements across all professions
WTE £'000 WTE £'000 WTE £'000
Nursing Staffing - Combined Assessment Unit, A&E & ANPsNursing Staffing - Combined Critical Care (17 Beds)Nursing Staffing - Theatres, Endoscopy & Day SurgeryNursing Staffing - General Wards (210 Beds)Nursing Staffing - Children Ward (24 beds)Pharmacy ATOs - Impact of Robotics
Nursing Staffing - Renal as result of offsite serviceCSSD Transfers between sitesOphthalmology - impact of cross site working
WTE £'000 WTE £'000 WTE £'000NHS Dumfries & GallowayScottish Government
542.37 18,676£ 566.67 20,059£ 24.30 1,382£
Anticipated Costs Existing Revised Movement
Funding Assumption Existing Revised Movement
Commercial in Confidence
June 2013
Page 120 of 164

Redacted for Publication - see front cover
Impact of Health & Social Care Integration
Impact of service redesign through PYF programme and strategic change programme
Changes required in community & cottage hospitals
Local workforce demographics
Any increase to the Cresswell unitary charge as a result of the proposed refurbishment
17.5 Facilities Management Services 17.5.1 A matrix of all FM services has been developed by the project FM work stream.
The current assumptions are that Soft FM services (domestics, catering, and portering) will continue to be provided by NHS Dumfries and Galloway and the majority of hard FM services (property maintenance, lifecycle) will be delivered by the Project Co.
17.5.2 As a result of the increased floor area and provision of single rooms at the new facility costs are anticipated to increase for domestic services. An additional cost has been calculated using current average costs and assumptions on estimated cleaned area. Further innovative solutions are anticipated in this area as work progresses which are likely to reduce the anticipated costs currently identified of
m.
17.5.3 No increase in running costs for the provision of catering are anticipated at this time, however it is recognised that to continue to have access to fully trained hospital catering staff to deliver the cook fresh option as approved by the Board, a sustainable training programme is required, an allowance has been made to release staff to support this.
17.5.4 The service delivery model for porters, laundry services and mail room services are being reviewed however costs are not expected to increase.
17.5.5 Hard FM services will be carried out by the Project Co. and charged as part of the annual unitary charge fee. It is assumed that the budgets associated with providing these services currently can be released.
Commercial in Confidence
June 2013
Page 121 of 164

Redacted for Publication - see front cover
17.5.6 There are a number of services which can fall within the scope of either hard or soft FM such as grounds maintenance, landscaping, floor coverings and wall decoration, the current assumption is that these will be retained by NHS Dumfries and Galloway therefore a budget to provide these services requires to be retained.
Figure 17-9: FM running costs analysis
17.6 Building Running Costs 17.6.1 There are also a number of building related costs which will continue to be
payable by NHS Dumfries and Galloway. For the purposes of the OBC traditional solutions have been used as the baseline, as alternative solutions are considered further efficiencies are expected to be generated.
17.6.2 Utilities will be delivered through the NPD provider with access to the national negotiated NHS tariffs. The costs will then flow back to NHS Dumfries and Galloway as a pass through arrangement. As it is intended to include this as part of the contractual agreement a VAT saving has been identified as a result of the different procurement route for these services.
17.6.3 The existing budget for utilities is releasable to offset the cost of the new facility. At this time the assumption for gas, electric and biomass is that the increased consumption as a direct result of the building footprint will be offset by the much increased efficiency of a new build.
17.6.4 Water consumption is anticipated to increase as a result of flushing requirement associated with the increased number of bathrooms. Indicative costs have been established with input from the technical advisors and the estates and property service department.
17.6.5 Rates for a modern fit for purpose single bedroom building are higher than the current building which receives relief elements for age and functional obsolescence. For the purposes of the OBC indicative costs have been provided by the local valuation office, these will require to be refined as the reference
WTE £'000 WTE £'000 WTE £'000
Maintenance including PPM and GroundsBacklog Maintenance/Statutory ComplianceDomesticsCateringPorteringLaundryClinical WasteTelephone Switchboard
WTE £'000 WTE £'000 WTE £'000NHS Dumfries & GallowayScottish Government
Anticipated Cost Existing Revised Movement
Funding Assumption Existing Revised Movement
Commercial in Confidence
June 2013
Page 122 of 164

Redacted for Publication - see front cover
design develops. The k increase is significant and fall directly to NHS Dumfries and Galloway.
Figure 17-10: Building running costs analysis
17.7 Other Associated Costs 17.7.1 A number of other costs have been identified as part of this review in relation to
transport. To provide a comparable level of bus access to the new hospital site a 20 minute daytime frequency is required. It is considered that initial usage would be lower and a subsidy will therefore be required. In addition a provision has been included to provide some form of cross site travel arrangement for staff. These are summarised in the table below.
Figure 17-11: Other associated costs analysis
17.8 Summary of Affordability 17.8.1 As described earlier the Scottish Government will be required to support the
majority of the unitary charge subject to a number of conditions. NHS Dumfries and Galloway are therefore required to support all the other additional costs
17.8.2 The Board’s commitment to a sustainable future has been mirrored in the pro active approach to financial planning over the last number of years. In
Existing Anticipated Movement£'000 £'000 £'000
Rates £ Council Tax £ Water £ Energy £ Fibre Link £
£ Existing Anticipated Movement
£'000 £'000 £'000NHS Dumfries & Galloway £ Scottish Government £
£
Anticipated Costs
Funding Assumption
Existing Anticipated Movement£'000 £'000 £'000
Subsidised Bus Route -£ Transport Links between sites -£
-£ Existing Anticipated Movement£'000 £'000 £'000
NHS Dumfries & Galloway -£ Scottish Government -£
-£
Anticipated Costs
Funding Assumption
Commercial in Confidence
June 2013
Page 123 of 164

Redacted for Publication - see front cover
anticipation for the change in service delivery the financial plan has recognised the need to release funding on a recurring basis to support this.
17.8.3 The current financial plan has released £3.8m to date and this has been ring fenced specifically as a contribution towards the recurring revenue costs. The future financial plans will address any recurring costs over and above the identified source of funds. This will also be reviewed for annual uplifts to match inflationary movements.
17.8.4 The following table sets out the total overall source and application of revenue.
Figure 17-12: Revenue costs summary
17.8.5 The above table indicates that the recurring cost to NHS Dumfries and Galloway
will be £ m which is made up of a combination of Unitary Charge, depreciation, facility and revised service model costs. The Board has ring fenced £3.8m to offset the additional cost of the new build project. The estimated revenue gap of £ m will need to be secured through a dual approach of reducing the identified increased cost areas as described in the revenue section and also by releasing additional funding from the Board’s Five Year Financial Plan. This will be a challenging task; however, the latest iteration of the Board’s Financial Plan has made provision to fund this gap.
NHS D&G SGHSCD TotalWTE £'000 WTE £'000 WTE £'000 £'000 £'000 £'000
Unitary ChargeDepreciationService Running CostsFacil l ities ManagementBuilding Running CostsOther Costs
NoteThese costs are presented at 2012/13 prices both source and application will require to be indexed
REVENUE COSTS Existing Revised Movement
Commercial in Confidence
June 2013
Page 124 of 164

Redacted for Publication - see front cover
17.9 Conclusion 17.9.1 The Board has a strong commitment to supporting the development of a new
Acute Hospital for the population of Dumfries and Galloway and has support from both the Scottish Government and community planning partners including the Local Authority.
17.9.2 Based on the information presented above an increase of £ m at current day prices is required to take forward this project, this equates to an additional investment of m for NHS Dumfries and Galloway and a £ m contribution from Scottish Government.
17.9.3 The financial case presents an affordable model for NHS Dumfries and Galloway however given the significant financial implications of this service change considerable financial rigour will need to be maintained to ensure the level of review and challenge continues to close the recurring revenue gap.
17.9.4 The Scottish Government have already identified a share of the NPD revenue budget to support the new build project. The challenge for NHS Dumfries and Galloway will be to continue to test all of the service and physical design elements to ensure that maximum value for money is delivered.
Commercial in Confidence
June 2013
Page 125 of 164

Redacted for Publication - see front cover
18 CAPITAL
18.1 Overview 18.1.1 NHS Dumfries and Galloway will receive a formula allocation from Scottish
Government of £3.1m for 2013-14 rising to £3.6m in 2014-15. This is used to support rolling programmes in statutory compliance, equipment and IT; in addition this fund also supports the Boards overall estates and property strategy.
18.1.2 As demonstrated in the revenue case earlier the substantial part of this project is covered by the revenue financing model however there are a number of different capital works which will require to be completed to deliver the project that sit out with the scope of the NPD model. Given the level of capital funding available locally support is required from the SGHSCD to fund these capital elements.
18.1.3 The following section sets out the various elements which require capital funding to complete the project, the timeline of investment required and the anticipated funding source.
18.1.4 The total estimated capital requirement is £53m and further details of the individual elements are set out below.
Figure 18-1: Capital cost elements
Capital Costs
Site Acquisition
External Enabling
Works
Off Site Capital Works
Site Clearance
Equipment Grp 2&3
Commercial in Confidence
June 2013
Page 126 of 164

Redacted for Publication - see front cover
18.2 Site Acquisition 18.2.1 The site purchase includes the agreed sum payable for the main hospital site and
in addition an estimate for land acquisitions in connection with the secondary access which is being progressed and a further piece of land required for road enabling works.
18.3 External Enabling Works 18.3.1 A number of work packages that fall outwith the scope of the NPD element of the
project are required to be taken forward to deliver this project on the acquired site. These are costs out with the ‘red line’ perimeter of the site and include road upgrades, electric, water, gas and telecommunication service provision to site. In addition improved walking and cycling routes are also included.
18.3.2 The individual work packages are costed and are being progressed with the relevant organisation therefore there is a good degree of certainty in the majority of these costs at this time.
18.4 Off site Capital Works 18.4.1 To maximise the use of the retained estate and therefore minimise the unitary
charge on the new build a number of offsite capital works are required.
18.4.2 The existing Cresswell Unit is a building which will be retained on the existing site currently has 19 years remaining in an existing PFI agreement. It is therefore important that this building is fully utilised and transfer only those services which require being in an acute hospital setting. A capital refurbishment programme is required to allow the building to be used differently, services have been identified and an estimate provided by the Project technical advisors has been included.
18.4.3 An energy centre servicing the Cresswell Unit is required to allow the building to function as a standalone building. An estimate provided by the Project technical advisors has been included.
18.4.4 A capital estimate has been included to reflect the need to run existing services in the old hospital until such time that Cresswell is commissioned.
18.4.5 The Dumfries Dental Centre which will remain on the existing site is currently being investigated as a solution to provide the Orthodontic service. A contribution towards the capital sum estimate to reconfigure the building has been included.
Commercial in Confidence
June 2013
Page 127 of 164

Redacted for Publication - see front cover
18.5 Site Clearance Costs 18.5.1 The current working assumption is that the existing site will be cleared and
disposed off. A number of buildings will remain on the existing and adjoining CRH site, at present these buildings are serviced directly through the DGRI. As well as the demolition costs which have been included a number of services including gas, electric, water and telecoms are required to be re-provided to clear the DGRI site.
18.6 Equipment Group 2 & 3 18.6.1 Group 2 equipment is normally equipment which is fixed to the building fabric
and/or attached to or forming part of the building services, kitchen equipment, laboratory refrigerators for example. Group 3 equipment tends to be free standing and/or mobile equipment, ventilators and anaesthetics machines for example.
18.6.2 The current planning assumption for equipment is based on 20% of capital construction costs as per Technical Costing 2; this assumes that Group 1 equipment is included within the NPD cost model. Where practical and feasible all moveable equipment, medical and non medical which has not reached the end of its useful life will be transferred and therefore it is further assumed that at least 15% of this gross value will be transferred.
18.6.3 An initial review carried out by Health Facilities Scotland (HFS) indicates a similar value of equipment purchases however a fully costed model will be developed with HFS along with the designated work streams, the general managers, and the local Capital Investment Group supported by the project team to identify the actual equipment needs.
18.6.4 This will also take account of transfers envisaged and any impact of managed service contracts and lease arrangements. Further consideration of subsequent revenue implications on capital charges, service contracts, consumables and staffing will be considered in the revenue case.
18.6.5 Further equipment requirements have also been included for the offsite capital works at Cresswell and as a result of retaining CSSD in its current location.
Commercial in Confidence
June 2013
Page 128 of 164

Redacted for Publication - see front cover
18.7 Capital Cost Summary 18.7.1 A summary of the total non NPD capital requirements is shown below.
Figure 18-2: Capital cost requirements
CAPITAL COSTS
TOTAL ESTIMATE
Land - Main SiteLand - Secondary AccessLand - Transport ScotlandSite AcquisitionTransportation: Works to Dumfries Road NetworkTransportation: Works to Trunk Road NetworkTransportation: Works to secondary accessAccessibil ity: Walking and cyclingAccessibil ity: SignageSite Connection: Foul SewerageSite Connection: Water Supply (Mains)Site Connection: ElectricitySite Connection: GasSite Connection: Fibre optic l inksExternal Enabling WorksCresswell: Reconfiguration for servicesCresswell: Energy CentreDental Centre: Contribution to reconfiguration for OrthodonticsDGRI: Reconfiguration to allow service provision in current DGRIOff Site Enabling WorksReprovide Electric, Gas, Water, Fibre, Telecoms, FireSite DemolitionSite Clearance CostsNew Build: Group 2 & 3 EquipmentCresswell: Group 2 & 3 EquipmentCSSD: Increased Equipment for offsite optionEquipmentTotal Capital Cost including indexation, fees & VAT
Commercial in Confidence
June 2013
Page 129 of 164

Redacted for Publication - see front cover
18.7.2 Capital costs have been prepared at current day prices (Quarter 4 2012) however as these works will not be carried out until future years the baseline costs have been adjusted to recognise the anticipated movement in prices to this time. The Building Cost Information Services (BCIS) forecast indices are the recognised indices used in preparing business cases of this nature. It is important to highlight that these are forecast indices for the purposes of modelling and are likely to change as work packages are tendered for actual delivered prices nearer the time.
18.7.3 VAT at 20% has been included on all elements with the exception of the land purchase where it is not applicable and professional fees where it is currently recoverable.
18.7.4 Professional fees have also been included at the relevant rate advised by the project technical advisors.
18.7.5 The full schedule of capital costs which includes indexation, fee and VAT rates applied to the individual elements along with underlying assumptions is included in Appendix 16.
18.8 Optimism Bias 18.8.1 Optimism bias refers to the tendency when evaluating publicly funded projects to
overestimate the benefits and underestimate the costs. Evidence indicates that public sector procurement options typically suffer from optimistic bias in the estimation of costs and benefits.
18.8.2 Given the differing levels of cost certainty at this point in the project, the standard methodology on optimism bias has been applied to all capital costs described above.
18.8.3 A summary of the total capital requirements including Optimism Bias is shown in the table below.
Figure 18-3: Total capital requirements
CAPITAL COSTS
Capital Cost inc VAT & Fees
Optimism Bias % applied
Optimism Bias
Capital Cost inc VAT, Fees & OB
Site AcquisitionExternal Enabling WorksOff Site Capital WorksSite Clearance CostsEquipmentTotal Capital Cost inc VAT & Fees
Commercial in Confidence
June 2013
Page 130 of 164

Redacted for Publication - see front cover
18.9 Summary of Capital Affordability 18.9.1 The table below highlights when capital funding is likely to be needed in order to
carry out the capital works and the associated funding assumptions.
18.9.2 As previously highlighted NHS Dumfries and Galloway do not have sufficient capital formula allocation to support this level of expenditure it is therefore assumed that project specific funding will be allocated from Scottish Government. This assumption will be reflected in the Board’s five year capital plan which will be submitted as part of the LDP process.
Figure 18-4: Capital costs summary
18.9.3 A capital receipt from the sale of the existing site has not been included in the
capital costs as an offset.
18.9.4 Under the current accounting treatment the receipt would be returned centrally, this is estimated for receipt in 2021/22 or thereafter. Further work is required to firm up on this value for FBC.
18.10 Conclusion 18.10.1 The Board has developed a robust capital model which identifies all likely capital
expenditure which is out with the NPD model. The estimated cost of £ m is anticipated to be funded by Scottish Government as project specific funding.
2013/14 2014/15 2015/16 2016/17 2017/18 2018/19 2019/20 2020/21 TOTAL£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Site AcquisitionExternal Enabling WorksOff Site Capital WorksSite Clearance CostsEquipmentCapital Cost inc VAT & Fees
2013/14 2014/15 2015/16 2016/17 2017/18 2018/19 2019/20 2020/21 TOTAL£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
NHS Dumfries & GallowayScottish GovernmentCapital Cost inc VAT & Fees
Anticipated Costs
Funding Assumption
Commercial in Confidence
June 2013
Page 131 of 164

Redacted for Publication - see front cover
19 NON RECURRING REVENUE EXPENDITURE
19.1 Project Running Costs 19.1.1 Costs associated with the in house project team have been included and also
professional fees including technical, legal and financial advisors which cannot be capitalised. These costs have been estimated through to the operational phase.
19.2 Commissioning 19.2.1 Non recurring expenditure will be incurred as the new building is commissioned;
services transferred and become fully operational. This will include initial cleaning costs, removal and transport costs, patient transport and double running for staff familiarisation, induction and equipment training as well as double running for staff as services operate on a dual site while the transfer is in operation.
19.3 Building Double Running Costs 19.3.1 During the commissioning period essentially two buildings will be operating,
charges for rates, gas, biomass, electric, water and depreciation for example will be payable on two sites for this period of time.
19.3.2 Following the transfer of patients and services to the new building, the work to refurbish Cresswell will get underway; as a result a number of services will remain in the existing DGRI building for around a year. Double running for building costs will continue for this period. Work is continuing to identify the level of reduction that may apply to these elements during this period.
19.3.3 Further cost will be incurred on the decommissioning of the existing site once all services have been relocated in preparation for the site disposal this will include security.
19.4 Group 4 Equipment 19.4.1 It is recognised that some of the equipment required for the new hospital will be
below the capital threshold of £5k. The current assumption within the OBC is that the capital sum identified includes all equipment including those items less than £5k. When room schedules are developed further an appropriate split of capital and revenue will be more readily identifiable.
19.5 Excess Travel Costs 19.5.1 The excess travel policy allows staff to claim excess travel between old and new
base of work. This will apply for 4 years and is paid at the public transport rate which is currently 24p however anticipated to rise to 27p in future years.
Commercial in Confidence
June 2013
Page 132 of 164

Redacted for Publication - see front cover
19.6 Summary of Affordability 19.6.1 The following table identifies the anticipated costs and the funding available to
support these.
Figure 19-1: Non recurring revenue costs summary
19.6.2 As indicated much more detailed work is required to assess total cost
requirements however at this stage early indications show at least a further £1m will be required.
19.6.3 No funding for these costs will be supported centrally therefore any shortfall will need to be identified by the Board and banked with Scottish Government in advance of 2017/18.
19.7 Conclusion 19.7.1 A high level review of non recurring costs has been carried out which indicates
that as a minimum £ m will be required to cover these costs. The Board are in a good financial position with regards to supporting these costs having already identified within future financial plans and having banked m in 2012/13 with the Scottish Government towards these future costs. The final shortfall identified will require to be delivered through the identification of non recurring sources in advance of 2017/18.
2013/14 2014/15 2015/16 2016/17 2017/18
Between 18/19 & 21/22 Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000Project Team & External Advisors £ All other non recurring costs £ Total Non Recurring Revenue Costs £
2013/14 2014/15 2015/16 2016/17 2017/18
Between 18/19 & 21/22 Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000Currently within Financial Plan £ Currently banked with SGHSCD £Total Non Recurring Revenue Costs £
NON RECURRING COSTS
NON RECURRING FUNDING
Commercial in Confidence
June 2013
Page 133 of 164

Redacted for Publication - see front cover
20 ACCOUNTANCY TREATMENT
20.1 Overview 20.1.1 This section of the OBC sets out the technical accounting issues that arise as a
result of this project. The table below highlights the areas which need considered as part of this case:
Figure 20-1: Accounting Treatment elements
20.1.2 A summary of each element is provided below, further details are provided in Appendix 17. Work is ongoing with the Boards appointed external auditors to confirm the assumptions included.
20.2 Assets within the scope of NPD contract 20.2.1 As highlighted earlier within the financial case this project is being taken forward
under the Non Profit Distributing funding model (NPD), this is a revenue funded scheme unlike the traditional capital funded route most commonly used in recent NHS Dumfries and Galloway projects. As a result of this the accounting treatment for both NHS Dumfries and Galloway and Scottish Government requires to be considered closely.
•Capital Purchases
•Capital Grants
•Exisiting DGRI•New Build DGRI•Cresswell
•NHS D&G Accounts
•National Accounts
•NHS D&G Accounts
•National Accounts
Assets within scope of NPD
contract
Existing PFI arrangement for Cresswell
Capital additionsImpairments
Commercial in Confidence
June 2013
Page 134 of 164

Redacted for Publication - see front cover
NHS Dumfries & Galloway Accounts
20.2.2 NHS Dumfries and Galloway are required to prepare annual accounts based on International Financial Reporting Standards (IFRS). An NPD funded project specifically requires to be tested against the guidance set out on Service Concessions (IFRIC12).
20.2.3 Having considered the guidance the current assumption is that the new hospital will need to be treated as a service concession. This means that the Board will be required to record this as an asset on the balance sheet. National Accounts
20.2.4 Scottish Government is required to prepare annual accounts based on National Accounting Standards as set out in the Manual of Government Deficit and Debt (MGDD). An NPD funded project specifically requires to be tested against the guidance to consider if the hospital would require to be treated as a Government asset.
20.2.5 Having considered the guidance the current assumption is that the new hospital will not be treated as a Government asset and would be considered as similar to an operating lease. This means that the Scottish Government will not be required to record this as an asset on the government balance sheet.
20.3 Existing PFI arrangement at Cresswell 20.3.1 The Cresswell Unit is an existing PFI agreement which NHS Dumfries and
Galloway have with 19 years remaining. As highlighted in the Commercial Case negotiations on a change of use have commenced with the provider to understand the potential impact on the existing PFI agreement. . As a result of this the accounting treatment for both NHS Dumfries and Galloway and Scottish Government requires to be considered closely. NHS Dumfries & Galloway Accounts
20.3.2 Under IFRS the Cresswell building is currently treated as a service concession and is recorded as an asset on the Boards balance sheet.
20.3.3 The assumption is that any amendment to the PFI agreement as a result of the refurbishment will have no impact on the current treatment. The Board will continue to record the asset on the balance sheet. National Accounts
20.3.4 Under MGDD the Cresswell building is currently treated as an operating lease and is not recorded as an asset on the government balance sheet.
20.3.5 The assumption is that any amendment to the PFI agreement as a result of the refurbishment will have no impact on the current treatment. The Government will continue to record the asset as similar to an operating lease.
20.4 Capital Additions 20.4.1 As described in the capital section of the Finance Case a number of different
capital costs will be incurred to support the project.
Commercial in Confidence
June 2013
Page 135 of 164

Redacted for Publication - see front cover
20.4.2 NHS Dumfries and Galloway will be required to record these on the balance sheet as assets with the exception of any expenditure which is to be treated as a capital grant. For example the purchase of land and equipment will be recorded as an asset on Boards balance sheet however the works required to the road network both locally and nationally will not and should be treated as an asset on the balance sheet of the organisation where it is currently recognised.
20.5 Impairments 20.5.1 Under IFRS an asset must be impaired in the Boards accounts if the value it is
recorded at is higher than it is now valued to be worth. The current assumption is that the following impairments will require to be recognised:
• The existing DGRI
• The new District General Hospital
• Cresswell following refurbishment
20.5.2 The table below gives an indicative view on values and the assumptions around funding however these will require to be refined as the external auditors’ opinion becomes available and the most current valuations are available.
Figure 20-2: Impairments
20.6 Conclusion
The accounting treatment contains a number of working assumptions which are currently being considered by the Boards external auditors.
It is assumed that the new DGH will be on balance sheet for NHS Dumfries and Galloway purposes however off balance sheet for national accounting purposes. It is further assumed that Cresswell will have no impact on the existing accounting treatment and that capital additions will be treated in accordance with current guidance.
Further work with external auditors and independent valuers is required to firm up values and timing of impairments.
Impairment TimingFinancial Year
Estimate £m
Funding Source
Existing DGRI Financial Close 2014-15 £ SGHSCD as part of Annually Managed Expenditure (AME)New DGH Formal Handover 2017-18 £ SGHSCD as part of Annually Managed Expenditure (AME)Cresswell Formal Handover 2019-20 £ SGHSCD as part of IFRS Non Core Allocation
£
Note: These values require to be firmed upwith the professional external advisor once further clarity is available
Commercial in Confidence
June 2013
Page 136 of 164

Redacted for Publication - see front cover
MANAGEMENT CASE
Commercial in Confidence
June 2013
Page 137 of 164

Redacted for Publication - see front cover
21 PROJECT MANAGEMENT & PROJECT IMPLEMENTATION TIMETABLE
21.1 Overview 21.1.1 This section of the OBC sets out the arrangements in place to manage the
project to successful delivery. The areas covered include:
Project management strategy and methodology
The project framework
Project roles and responsibilities
The project plan, showing the high level timetable for the project
Project communication and reporting arrangements
Arrangements for independent project assurance through the Key Stage Review process
21.2 Project Management Strategy and Methodology 21.2.1 This project supports the principles of project and programme management to
ensure that the project is successfully delivered. The Acute Services Redevelopment Project sits within a range of wider changes to the health system within Dumfries and Galloway.
21.2.2 Clear and appropriate project governance arrangements are fundamental to the success of the project. The governance arrangements adopted, taken together with the procurement strategy and the resources deployed to support the project, must ensure that NHS Dumfries and Galloway is able to procure the new hospital facilities in an efficient and effective manner, whilst also allowing adequate scrutiny at key decision points.
21.2.3 It is the responsibility of NHS Dumfries and Galloway to ensure that an appropriate and robust governance structure is put in place for the project. Project governance arrangements have recently been reviewed within the wider context of the Board’s overall governance framework to ensure that they are fully aligned to the proposed procurement strategy.
21.2.4 The governance structure must be fully reflective of the revenue financed NPD procurement route being followed in relation to the new hospital and should also recognise that the Board will be identifying a private sector partner with which it will engage on a daily basis for the next 25 years as a minimum.
21.3 The Project Framework 21.3.1 This project has its own Project Board which reports to:
The Board of NHS Dumfries and Galloway which has overall responsibility for this project
The Performance Committee, who are responsible for scrutiny of the work of the Project Board.
Commercial in Confidence
June 2013
Page 138 of 164

Redacted for Publication - see front cover
21.3.2 The diagram below sets out:
The overall programme structure
How the Project Board and the Project Team for the Acute Services Redevelopment Project fit into this structure
The key roles for Acute Services Redevelopment Project including the Project Sponsor and Project Director
The key supporting mechanisms
Figure 21-1: Project structure
21.4 Project Roles and Responsibilities 21.4.1 The detailed roles and responsibilities within the project structure are set out
below covering:
Structures within the project
Individual roles within the project structure
External advisers
Investment Decision Maker (IDM) Dumfries and Galloway NHS Board
Performance Committee
Project Owner – NHS Dumfries and Galloway
Chief Executive
Project Director – Acute Services Redevelopment
Project Manager
Project Board
Project Team -Redevelopment led by
Project Manager
Stakeholder Groups
Project Group
Project Sponsor NHS Dumfries and Galloway Chief Operating Officer
External Advisors
Commercial in Confidence
June 2013
Page 139 of 164

Redacted for Publication - see front cover
Structures within the Project 21.4.2 The detailed roles and responsibilities of the Boards and Teams within the
project structure are set out in the table below.
Figure 21-2: Project roles and responsibilities
Team or Group Role and Responsibilities
Dumfries and Galloway NHS Board - The Investment Decision Maker (IDM)
It is essential that there is a clearly identified body with responsibility for approving the investment. The NHS Dumfries and Galloway Board will be the Investment Decision Maker (IDM) for the project and as part of this will be responsible for deciding what financial and other resources to invest in the project. The Board must consider whether the project fits with the strategic direction that it is developing, particularly around the use of cottage hospitals.
The Board also needs to be satisfied that the project is affordable throughout its life. The Board should also be satisfied that the project represents value for money in the context of the available funding. Ultimately the Board will be accountable for the successful delivery of the project. The Board should ensure that an appropriate governance structure is put in place, and that adequate resources have been deployed including appointing the Project Sponsor.
The Board should approve a formal Scheme of Delegation that will allow certain of its responsibilities to be exercised at other levels within the organisation. The Scheme of Delegation has been drawn up for this project and therefore reflects the NPD procurement process and the key decision making points that are required.
A vital part of the Board’s role as Investment Decision maker, and which will not be delegated, will be to approve the selection of the Private Sector Partner at the conclusion of the bidding exercise. The Private Sector Partner will be responsible for the design (to completion), construction, finance, maintenance and life cycle replacement of the new hospital building over a period of at least 25 years.
Commercial in Confidence
June 2013
Page 140 of 164

Redacted for Publication - see front cover
Team or Group Role and Responsibilities
Performance Committee
Whilst the NHS Board will be the Investment Decision Maker and as such retain responsibility for the most major decisions, more detailed scrutiny will be undertaken by the Board’s Performance Committee. The committee will make recommendations to the Board on key issues such as the appointment of a Preferred Bidder and the approval of the Project Agreement. The Scheme of Delegation must make clear what authority is being delegated to the committee.
This arrangement will also limit the time needed for detailed project scrutiny at NHS Dumfries and Galloway Board meetings and therefore allow the normal business of the Board to continue without the meetings being dominated by discussion about the project. Detailed scrutiny of issues at the Performance Committee should give the full NHS Dumfries and Galloway Board confidence in the progress of the project.
It is essential that Project Sponsor is represented on the Performance Committee. The chair will be one of the non-executive members of the Board.
The frequency and timing of Performance Committee meetings would normally be expected to match that of Board meetings. On occasions, however, the procurement timescale of the project will require that meetings are held more frequently and additional meetings are therefore very likely to have to be called at crucial stages in the project and possibly at short notice.
Project Board The Project Board will take decisions in areas delegated to it through the Scheme of Delegation and will make recommendations to the Board or Board committee, on other issues where it does not have delegated authority.
The Project Board has a wide range of senior membership from a variety of stakeholders in the new hospital, including management with responsibility for the services and clinicians providing the services.
Project Board membership has been agreed by the Project Sponsor and includes the Project Director. Some of the stakeholders represented may be external to NHS Dumfries and Galloway such as the local authority, Scottish Government and SFT.
The Project Board are responsible for reviewing the risk register at regular meetings taking due consideration of the red risks highlighted along with the proposed mitigating
Commercial in Confidence
June 2013
Page 141 of 164

Redacted for Publication - see front cover
Team or Group Role and Responsibilities actions.
The Project Director brings a high level report on project progress to each meeting. This report will clearly identify issues where decisions are required and those issues that are delaying progress on the project.
The Project Board must ensure that the role of external advisers is clear and that their involvement in the project is appropriate and complementary to that of the Board’s own staff resources and that their involvement does not result in them taking on a leadership role.
The remit of the Project Board covers the entire range of issues that will need to be addressed in the project.
The Project Board is chaired by the Project Owner and meets monthly with more frequent meetings where required.
Commercial in Confidence
June 2013
Page 142 of 164

Redacted for Publication - see front cover
Team or Group Role and Responsibilities
Project Group The primary role of the Project Group is to act as an stakeholder reference group specifically for NHS Dumfries and Galloway clinical; non-clinical and operational end-users and drawn from acute and primary services.
Members of this group include identified Workstream Leads; and the corresponding Workstream General Manager and Clinical Director together with Estates and Facilities Lead and other specialist leads whose function spans across the Workstreams (e.g. Infection Control, Human Resources and Information Technology leads).
The members of the Project Group provide the primary interface with the Project Team’s appointed Technical Advisors and in particular with the Healthcare Planners and Design Team members (e.g. Architects). This interface has enabled the Board’s Model of Care to be developed along with other fundamental considerations such as the Bed Model and Schedule of Accommodation, Reference Design and Clinical and Operational Policies.
The role of the Project Group will flex and evolve as the project progresses beyond the development of the Reference Design and Outline Business Case towards procurement. During procurement members of the Bid Evaluation Team drawn from the Project Group will continue to liaise with the other Project Group members to provide feedback and progress reports. The Project Group will also continue, by working in parallel with the procurement process, to develop and implement the Board’s Clinical Strategy in readiness for the transfer of services into the new build and plans for changes to the community and cottage hospitals so as to be fully aligned with the proposed model of care as set out in the Outline Business Case.
The Project Group meets on a regular basis with members of the Project Team to review the progress of the project; deal with any issues that require escalation from the Workstreams and to provide reports on the progress of the Board’s Clinical Strategy and plans for changes to the community and cottage hospitals.
Project Team The Project Team’s role is to ensure that the Acute Services Redevelopment Project is managed successfully throughout all stages of the project so that all project objectives are met and all benefits are realised.
Commercial in Confidence
June 2013
Page 143 of 164

Redacted for Publication - see front cover
Team or Group Role and Responsibilities
The Project Team is directed under the leadership of the Project Director and on a day-to-day basis by the Project Manager. In addition to their specific functional roles and specialism, as defined in the project team structure, members of the Project Team have an overarching responsibility to ensure that all relevant stakeholders (e.g. members of the Project Group) are fully engaged in the project through the delivery of change plans and an agreed strategy for:
• communication; • project governance; • risk management; • change control; • quality assurance; • planning; • business case development, • programming; • design; • procurement; • construction; • commissioning and • post occupancy evaluation activities.
The Project Team is represented at the Project Board by the Project Director supported by the Project Manager.
Commercial in Confidence
June 2013
Page 144 of 164

Redacted for Publication - see front cover
Individual roles within the Project Structure 21.4.7 The detailed roles and responsibilities of the key individuals within the project
structure are set out in the table below.
Figure 21-3: Individual roles and responsibilities
Individual Role and Responsibilities
Project Owner
The Project Owner represents the NHS Dumfries and Galloway Board and has responsibility at a strategic level for the successful delivery of the project. The Project Owner may need to have delegated authority in some areas. The Project Sponsor provides direction and strategic leadership for the project and as such is accountable to the NHS Dumfries and Galloway Board.
The Project Owner’s involvement in the project, whilst not on a full time basis, should not be split or shared amongst a number of individuals. There must be no ambiguity about who is fulfilling the role of Project Owner.
The Project Owner will ensure that the Board receives regular reports on project progress and is alerted to issues that risk blowing the project off course. The Project Owner is responsible for alerting the Board if the project is likely to be delayed or has other major difficulties, such as additional demands on NHS Dumfries and Galloway finance. The Project Owner will also chair the Project board.
Notwithstanding the involvement of others at a senior level in the project, the Project Owner retains personal responsibility for the success of the project.
It is the responsibility of the Project Owner to appoint a suitably senior and named individual as Project Sponsor.
Owing to the project’s magnitude and scale, the Board’s Chief Executive has been identified as the Project Owner for the project.
Project Sponsor
Recognising the scale and complexity of this project it requires a Project Sponsor, who is appointed by and reports direct to the Project Owner. The Project Sponsor must be able to provide more direct input to the project than can be expected of the Project Owner and should ensure that the project is sufficiently resourced.
Although the input of the Project Sponsor will sometimes be on a part time basis, an important responsibility of the Project Sponsor will be to provide support to the Project Director.
It is not necessary for the Project Sponsor to be technically qualified, as they will be supported by a Project Director working full time on the project with in depth knowledge of the NPD and
Commercial in Confidence
June 2013
Page 145 of 164

Redacted for Publication - see front cover
Individual Role and Responsibilities wider procurement issues. The Project Sponsor role should not be split or shared between individuals.
The Board’s Chief Operating Officer has been identified as the Project Sponsor.
Project Director
Appointed by the Project Sponsor this is a full time role with a considerable degree of authority and responsibility for driving the project forward on a day to day basis by providing the project with visible leadership.
In light of the proposed procurement arrangements for the project the Project Director must have experience of procuring revenue funded projects i.e. PPP/PFI/NPD. It is very important that NPD skills are not provided exclusively by advisers.
The Project Director is the senior individual working on the project on a full time basis and must have adequate support from a team of individuals working on the project either on a full- time or part-time basis.
The Project Director brings reports on project progress and issues requiring decision to the Project Board.
Commercial in Confidence
June 2013
Page 146 of 164

Redacted for Publication - see front cover
External advisers 21.4.8 The Project team is supported by external advisers providing technical, financial
and legal advice to the project.
21.4.9 Following a formal procurement process the following appointments have been made:
Technical advisers – Mott MacDonald
Financial advisers – Ernst and Young LLP
Legal advisers – Shepherd and Wedderburn
21.4.10 Mott MacDonald’s role is initially focussed on assisting with the preparation of the reference design but will also provide support throughout the NPD procurement, process.
21.4.11 In undertaking this role they are supported through sub-consultancy agreements to comprise the Technical Advisory Team. The respective roles and responsibilities and organisations involved are:
Client and lead Technical Adviser – Mott MacDonald
Architects – Keppie Design
M&E / C&S Engineering – Mott MacDonald
Cost Consultants – Franklin Andrews
Healthcare Planners – Buchan and Associates
21.4.12 Ernst & Young are the Board’s Financial Advisers, responsible for the preparation of the shadow bid model, financial modelling and project finance advice up to and including financial close.
21.4.13 Shepherd and Wedderburn are the Board’s legal advisers, responsible for legal advice in relation to the NPD procurement up to and including financial close as well as support in relation to changes associated with the Cresswell wing.
21.4.14 As noted earlier in the OBC the Board are working in partnership with Dumfries and Galloway Council to ensure that all planning issues are considered and addressed at an early stage. Planning in Principle was agreed at the Planning Committee meeting held on 24th April 2013 and confirmed on 9th May 2013. Since that time Section 69 agreements have been completed in order to progress some of the planning issues.
Commercial in Confidence
June 2013
Page 147 of 164

Redacted for Publication - see front cover
21.5 Project Plan 21.5.1 A summary of the key milestones for the project is provided in the table covering
the period from OBC submission through to commissioning and operation of the new hospital. A full programme is provided at Appendix 18.
Figure 21-4: Key project milestones
Milestone Expected Date
OBC approved by NHS Dumfries and Galloway Board 08/04/2013
OBC submission to SGHD Capital Investment Group 16/04/2013
OBC approved by SGHD Capital Investment Group 21/05/2013
Commencement of new site enabling works 21/05/2013
NPD OJEU notice published 24/06/2013
NPD PQQ responses evaluated 24/09/2013
Issue of NPD ITPD 25/09/2013
Conclude NPD Competitive Dialogue 09/06/2014
Final NPD tender evaluation complete 05/09/2014
Selection of NPD Preferred Bidder 05/09/2014
NPD Financial Close 06/02/2015
New hospital construction start 01/04/2015
New hospital construction completion 30/06/2017
New hospital contractor’s commissioning and handover 22/12/2017
Completion of service migration to new hospital 02/03/2018
First patients at new hospital 05/03/2018
Commencement of Cresswell adaptations 01/05/2018
Cresswell handover with adaptations 30/04/2019
Commercial in Confidence
June 2013
Page 148 of 164

Redacted for Publication - see front cover
21.6 Project Communication and Reporting Arrangements 21.6.1 The Board has developed a formal Communication Strategy which clearly sets
out Acute Services Redevelopment Project’s aims and objectives for all aspects of communications, both internal and external and key actions to achieve these. A copy of the strategy is provided at Appendix 19.
21.7 Key Stage Reviews 21.7.1 In line with the Scottish Government communication issued on 6 July 2012 for
projects being delivered either through the hub Initiative or via NPD the Key Stage Review (KSR) processes will be used to assess these projects going forward.
21.7.2 All projects in the revenue funded programme are, in addition to any existing project approvals processes, externally validated by the Scottish Futures Trust (SFT). SFT undertakes validation by carrying out Key Stage Reviews (KSRs) of projects at key stages of the procurement. A summary of the review process is provided in the diagram below.
Figure 21-5: NPD procurement journey and KSRs
21.7.3 The Key Stage Review process requires five standard reviews at the following stages:
KSR1 – Pre-issue of OJEU
KSR2 – Pre Issue of ITPD
KSR3 – Pre-Invitation to Submit Final Tenders
KSR4 – Pre-Appointment of Preferred Bidder
KSR5 – Pre Financial Close and Contract Award
Commercial in Confidence
June 2013
Page 149 of 164

Redacted for Publication - see front cover
21.7.4 Where it becomes apparent that projects are not developed enough to receive a full sign off following a standard KSR, additional follow-up reviews may need to be carried out in advance of:
Pre-issue of Invitation to Participate in Dialogue; and/or
Pre- appointment of Preferred Bidder
21.7.5 In addition to the formal KSR’s, in advance of OBC approval a Design Review has been undertaken to establish the value for money offered through the reference design for the project. In line with the requirements of the Scottish Capital Investment Manual (SCIM), formal Post Project Evaluation will also be required (further details are provided within Section 22 of the OBC.
Commercial in Confidence
June 2013
Page 150 of 164

Redacted for Publication - see front cover
22 MANAGING SUCCESSFUL DELIVERY
22.1 Overview 22.1.1 This section of the OBC is primarily focussed on demonstrating how the Board
anticipates managing the successful delivery of the Acute Services Redevelopment project. Specifically it outlines the strategy, framework and plans relating to:
Proposals for the management of change
Benefits realisation planning
Proposals for managing key project risks
Arrangements for post project evaluation
22.2 Change Management Plan Change management philosophy
22.2.1 The provision of a new District General Hospital presents a significant change point for the Board. The change to the physical infrastructure is simply an enabler to a more fundamental change in the way that healthcare will be delivered across NHS Dumfries and Galloway.
22.2.2 The impact of the change will be fundamental. The table below summarises some of the main impacts of the changes across four areas
Figure 22-1: Impact of change
Area Impact Culture The Board’s Clinical Change Strategy ‘PYF’ is intended
to shift the balance of care from a focus on acute services to the development of seamless patient pathways which span the spectrum of prevention, primary care, acute care and social care services. The drive to ensure person centred care will lead to further enhancements of both the patient and staff experience. The culture of the organisation will shift accordingly.
Systems Systems will be more responsive and geared to supporting the new models of care, both within the hospital and across acute and primary care. In particular more emphasis will be placed on electronic forms of communication and effective handover between acute and primary care to make the patient experience seamless e.g. Single Electronic Clinical Records and Order Communications for the ordering of diagnostic tests.
Commercial in Confidence
June 2013
Page 151 of 164

Redacted for Publication - see front cover
22.2.3 In the light of the impact of these changes, the Board’s change management
philosophy is to:
Recognise the significance of the change
Take the opportunity to improve the quality of healthcare
Implement the change in a structured and well managed way
Change management principles 22.2.4 The Board is developing a series of principles that will underpin the change
process. .
22.2.5 The principles established to date are to:
Recognise the need to maximise the benefits of the change for patients, who are at the heart of the changes made
Take advantage of the time available to complete the new build to start the change process and thereby avoid risks related to a ‘big bang’ approach
Test and prove the changes through careful piloting of any aspects of the new models and processes that can be implemented before the new facility is finally commissioned
The change management philosophy and principles will be communicated to all staff.
Work in partnership with staff and other stakeholders both within and outside the hospital to engage all those involved in the delivery of care in the change process
Focus on staff skills and development required so staff are both capable and empowered to deliver healthcare effectively and to a high quality standard in the new facility through new models of care
Processes The proposed models of care will introduce new clinical processes. The new physical environment will facilitate improvements in the patient experience which cannot be achieved within the existing building.
People There will be changes to roles and responsibilities, particularly for clinical staff. Some of this will arise from the changes in clinical processes within the hospital, whereas other changes in roles will come from the way the focus of care will shift from acute to pathway based care.
Commercial in Confidence
June 2013
Page 152 of 164

Redacted for Publication - see front cover
22.3 Approach to change management 22.3.1 The process will be led by the project sponsor, who will responsible for leading,
managing and implementing the Change Management Programme.
22.4 Benefits Realisation Planning 22.4.1 Benefits management is the overarching process which incorporates the Benefits
Realisation Plan (BRP) as part of a process of continuous improvement. It takes due account of changes in the project during the delivery phase which impact on, or alter the anticipated benefits.
22.4.2 As such the benefits management approach is a cycle of selection, planning, execution and review as illustrated below.
Figure 22-2: Benefits Management approach
22.4.3 In developing the BRP the Board has sought to ensure that stakeholders are at the centre of the benefits realisation process. In this regard a workshop was held in December 2012 involving members of the Project Team as well as wider clinical and non-clinical stakeholders.
22.4.4 As part of the workshop activities a number of stages were identified in the development of the BRP process, namely:
• How benefits will contribute to the Board’s local strategies and to National Strategies
• How benefits will be delivered
• The owners roles and responsibilities for defining, realising and managing benefits
• The mechanism for monitoring benefits and identify corrective actions, if required
• The arrangements for transition to the operational phase
Commercial in Confidence
June 2013
Page 153 of 164

Redacted for Publication - see front cover
• The schedule for benefit reviews and identification of further benefits
22.4.5 As part of the further development of BRP the Board will agree baseline measures reflecting the current status of each benefit area and the timeline for attaining the anticipated full realisation of the benefits. This will also be linked to the Change Management Plan to provide assurance on delivery.
22.5 Risk Management Plan 22.5.1 This section of the OBC sets out Dumfries and Galloway’s approach to the
management of risks associated with the project incorporating:
Risk management philosophy
Risk identification and quantification
The approach to risk management
Risk management philosophy 22.5.2 The Board’s philosophy for managing risks considers effective risk management
to be a positive way of achieving the project’s wider aims, rather than a mechanistic exercise, to comply with guidance. Inadequate risk management would reduce the potential benefits to be gained from the project.
22.5.3 The Board recognises the value of an effective risk management framework to systematically identify, actively manage and minimise the impact of risk. This is done by:
Having strong decision making processes supported by a clear and effective framework of risk analysis and evaluation
Identifying possible risks before they crystallise and putting processes in place to minimise the likelihood of them materialising with adverse effects on the project;
Putting in place robust processes to monitor risks and report on the impact of planned mitigating actions;
Implement the right level of control to address the adverse consequences of the risks if they materialise;
Commercial in Confidence
June 2013
Page 154 of 164

Redacted for Publication - see front cover
Risk identification and quantification 22.5.4 A series of risk workshops were undertaken incorporating, members of the
Project Team, the external advisers as well as a cross section of NHS Dumfries and Galloway staff.
22.5.5 The initial activities focused on establishing a range of project risks reflecting the scope of the project as well as the likely procurement route. Primary risks were identified across a range of categories incorporating:
Clinical risks
Contractual risks
Design risks
Enabling works risks
Equipping risks
FM risks
Land acquisition risks
Legal risks
Procurement risks
Project management risks
22.5.6 These risks were further allocated across a range of categories depending on where these risks would apply within the overall structure of the project. These include:
The phase of the project to which they apply
Those that would have a major impact on the cost of the project
The ownership of the risks including those which can be transferred to the NPD contractor
22.5.7 Each risks has subsequently been assessed for its probability and impact, and where relevant its expected value. Where risks have been valued this has resulted in the following key outputs:
A risk value of million is attached to risks transferred to the NPD operator via the standard form NPD contract. These risks will be priced by the bidders involved in the procurement process and would form part of their overall financial proposals. This value is included, therefore, within the input costs used to derive the shadow unitary charge as described within the Financial Case.
A risk value of million is attached to risks retained by the public sector a proportion of which would result in an increased cost of the project.
22.5.8 The risk register is maintained as a dynamic document and updated at key milestones or as the need arises with the risk profile for the project kept under
Commercial in Confidence
June 2013
Page 155 of 164

Redacted for Publication - see front cover
constant review. The top risks are reported to the Project Board on a bi-monthly basis and to the Audit Committee every 6 months.
22.5.9 A copy of the full Risk Register is provided at Appendix 20.
Risk management 22.5.10 The risk register incorporates details of risk owners and appropriate counter
measures to manage the Board’s exposure to the risks and this will be maintained and updated throughout the procurement process.
22.5.11 A risk sub-group has been established with responsibility for the management of the risk process including ongoing assessment and quantification of risks. The group will also review and develop the management strategies associated with the risks. This group will comprise members of the Project Team as well as the Board’s Technical and Financial Advisors.
22.6 Proposals for Post Project Evaluation 22.6.1 The Board is committed to ensuring that a thorough and robust post-project
evaluation is undertaken at key stages in the process to ensure that positive lessons can be learnt from the project.
22.6.2 Scottish Government has published guidance on PPE, which supplements that incorporated within the Scottish Capital Investment Manual (SCIM). The key stages applicable for this project are set out in the table below:
Figure 22-3: The four stages of PPE
Stage Evaluation undertaken When undertaken
1 Plan and cost the scope of the PPE work at the project appraisal stage. This should be summarised in an Evaluation Plan.
Plan at OBC, fully costed at FBC stage
2 Monitor progress and evaluate the project outputs
On completion of the facility
3 Initial post-project evaluation of the service outcomes
Six months after the facility has been commissioned
Commercial in Confidence
June 2013
Page 156 of 164

Redacted for Publication - see front cover
Stage Evaluation undertaken When undertaken
4 Follow-up post-project evaluation (or post occupancy evaluation - POE) to assess longer-term service outcomes after the facility has been commissioned. Beyond this period, outcomes should continue to be monitored. It may be appropriate to draw on this monitoring information to undertake further evaluation after each market testing or benchmarking exercise
Two years after the facilities have been commissioned
22.6.3 Within each stage, the following issues will be considered:
The extent to which relevant project objectives have been achieved
The extent to which the has progressed against plan
Where the plan was not followed, what were the reasons
Where relevant how plans for the future projects should be adjusted
22.6.4 The Project Owner will be responsible for ensuring that the arrangements have all been put in place and that the requirements for PPE are fully delivered. The Project Director will be responsible for day to day oversight of the PPE process, reporting to the Project Owner and Project Board.
22.6.5 The Project Owner and the Project Director will set up an Evaluation Steering Group (ESG), which will:
Represent interests of all relevant stakeholders
Have access to, professional advisers who have appropriate expertise for advising on all aspects of the project.
22.6.6 The Project Manager will coordinate and oversee the evaluation. The key principle is that the evaluation is objective.
22.6.7 The Evaluation Team will be multi-disciplinary and include the following professional groups, although the list is not exhaustive:
Clinicians, including consultants, nursing staff, clinical support staff and Allied Health Professionals
Healthcare Planners, Estates professionals and other specialists that have an expertise on facilities
Accountants and finance specialists, IM&T professionals, plus representatives from any other relevant technical or professional grouping
Patients and/or representatives from patient and public group
Commercial in Confidence
June 2013
Page 157 of 164

Redacted for Publication - see front cover
Commercial in Confidence
June 2013
Page 158 of 164

Redacted for Publication - see front cover
GLOSSARY OF TERMS
Commercial in Confidence
June 2013
Page 159 of 164

Redacted for Publication - see front cover
24/7 Twenty four hours a day seven days a week
A&E Accident & Emergency
ADR Annual Development Review
AEDET Achieving Excellence – Design Evaluation Toolkit
AHP Allied Health Professional
ANP Advanced Nurse Practioner
AODOS Admission on Day of Surgery
ASB Accounting Standards Board
AVLOS Average Length of Stay
BADS British Association of Day Surgery
BCR Board’s Construction Requirements
BEAM Building Environment Assessment Methodology
BREEAM Building Research Establishment Environmental Assessment Method
BRP Benefits Realisation Plan
CAA Civil Aviation Authority
CAU Combined Assessment Unit
CCTV Closed-circuit television
CCU Critical Care Unit
CD Competitive Dialogue
CDM Construction (Design & Management) Regulations
CEL Chief Executive Letter
CfS Conditions for Success
CHP Combined Heat & Power
CIBSE Chartered Institution of Building Services Engineers
CIG Capital Investment Group
Council Dumfries and Galloway Council
Commercial in Confidence
June 2013
Page 160 of 164

Redacted for Publication - see front cover
COSHH Control of Substances Hazardous to Health
CRES Cash Releasing Efficiency Savings
CRL Capital Resource Limit
CSSD Central Sterile Supplies Department
CT Computed Tomography
DoE Department of the Environment
DDA Disability Discrimination Act 2005
DDI Direct Dial In
DFL Dumfries Facilities Limited
DGH District General Hospital
DGRI Dumfries and Galloway Royal Infirmary
DNA Did Not Attend
ED Emergency Department
EMS Environmental Management System
EPC Energy Performance Certificate
ETT Exercise Tolerance Testing
EU ETS European Union Emission Trading System
EWTD European Working Time Directive
FBC Full Business Case
FM Facilities Management
FRS Financial Reporting Standard
FY1 Foundation Year 1 (Doctor Training)
FY2 Foundation Year 2 (Doctor Training)
GP General Practioner
GROS General Registrars of Scotland
HAI Healthcare Associated Infection
HBN Health Building Notes
HDL Health Department Letter
Commercial in Confidence
June 2013
Page 161 of 164

Redacted for Publication - see front cover
HDU High Dependency Unit
HEAT Health, Efficiency Access and Treatment
HFN Health Facilities Notes
HFS Health Facilities Scotland
HGN Health Guidance Notes
HSE Health & Safety Executive
HTM Health Technical Memoranda
HVAC Heating Ventilation & Air Conditioning
HWS Hot Water Supply
IA Initial Agreement
ICU Intensive Care Unit
IFRS International Financial Reporting Standards
IM Information Memorandum
IM&T Information Management & Technology
ISD Information Services Division ( of Scottish Government)
IT Information Technology
ITPD Invitation to Participate in Dialogue
KPI Key Performance Indicator
LAN Local Area Network
LDP Local Development Plan
LOS Length of Stay
LPS Loss Prevention Standard
MAU Medical Assessment Unit
MEL Management Executive Letter (now known as Chief Executive Letter CEL)
MEWS Modified Early Warning System
MRI Magnetic Resonance Imaging
NEAT NHS Environmental Assessment Tool
Commercial in Confidence
June 2013
Page 162 of 164

Redacted for Publication - see front cover
NHBC National House Building Council
NHS D&G NHS Dumfries and Galloway
NHSIA National Health Service Information Authority
NPC Net Present Cost
NPD Non Profit Distributing
NPV Net Present Value
OBC Outline Business Case
OCS Office Communicator System
OD Organisational Development
OJEU Official Journal of the European Union
OOH Out of Hours
OPD Outpatient Department
PA Public Address system
PAMS Property and Asset Management Strategy
PBX Private Branch Exchange
PFI Private Finance Imitative
PIN Prior Information Notice
PPE
PPM
Post Project Evaluation
Planned Preventative Maintenance
PPP Public Private Partnership
PQQ Pre-Qualification Questionnaire
PYF Putting You First
QIS Quality Improvement Scotland
RDD Reviewable Design Data
RDS Room Data Sheets
RPI Retail Price Index
RRL Revenue Resource Limit
RTT Referral to Treatment
Commercial in Confidence
June 2013
Page 163 of 164
Redacted for Publication - see front cover
SoA Schedule of Accommodation
SbD Secured by Design
SCIEH Scottish Centre for Infection and Environmental Health
SCIM Scottish Government Capital Investment Manual
SEPA Scottish Environment Protection Agency
SFPN Scottish Fire Practice Notes
SFT Scottish Futures Trust
SGHD Scottish Government Health Directorate
SHFN Scottish Health Facilities Notes
SHGN Scottish Health Guidance Notes
SHPN Scottish Health Planning Notes
SHS Scottish Healthcare Supplies
SHTM Scottish Health Technical Memorandum
SHTN Scottish Hospital Technical Notes
SMART Specific, Measurable, Achievable, Realistic, Timely
SRO Senior Responsible Owner
SUDS Sustainable Urban Drainage System
TPO Tree Preservation Order
TUPE Transfer of Undertakings (Protection of Employment) Regulations
UC Unitary Charge
UP Unitary Payment
UPS Un-interruptible Power Supplies
VDU Visual Display Unit
VfM Value for Money
VoIP Voice over Internet Protocol (or Voice Over IP)
WTE Whole Time Equivalent
Commercial in Confidence
June 2013
Page 164 of 164