outbreak management: it takes a village - · pdf fileoutbreak management cycle 1. id team and...
TRANSCRIPT

Outbreak Managementit takes a village….
November 20, 2014 | Linda Stein
Marge Gribogiannis

Objectives • Identification of an outbreak
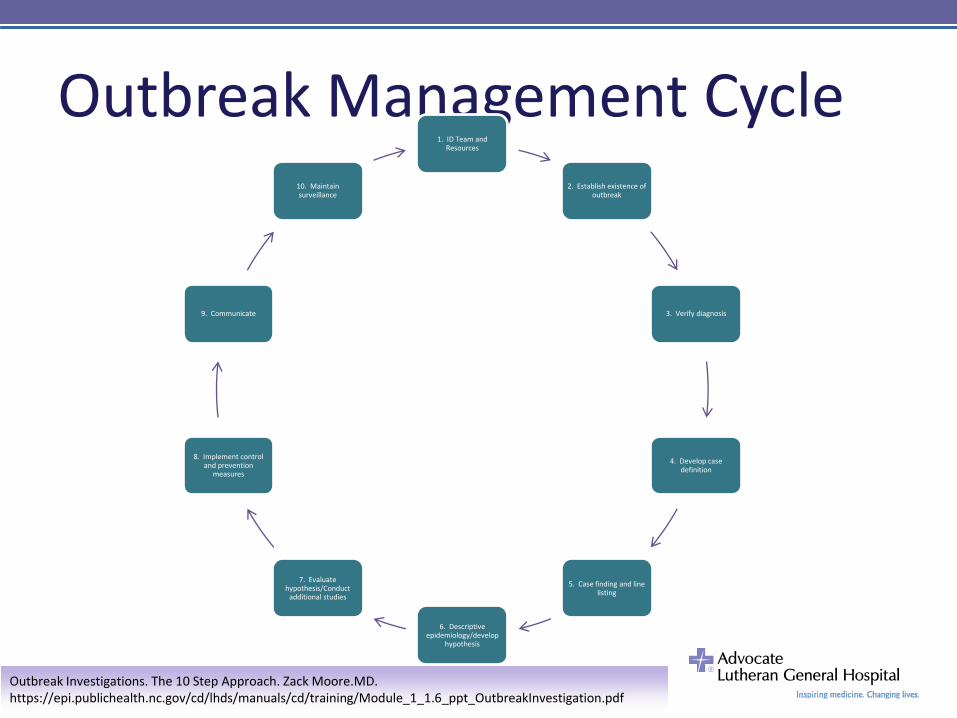
• To be able to perform the outbreak management process1. Identify investigation team and resources
2. Establish existence of outbreak
3. Verify diagnosis
4. Develop case definition
5. Case finding and line listing
6. Descriptive epidemiology/develop hypothesis
7. Evaluate hypothesis/conduct additional studies
8. Implement control and prevention measures
9. Communicate findings
10.Maintain surveillance

Outbreak Investigation
Principles
- Be systematic
- Re-assess
- Coordinate with partners
Outbreak Management Cycle1. ID Team and
Resources
2. Establish existence of outbreak
3. Verify diagnosis
4. Develop case definition
5. Case finding and line listing
6. Descriptive epidemiology/develop
hypothesis
7. Evaluate hypothesis/Conduct
additional studies
8. Implement control and prevention
measures
9. Communicate
10. Maintain surveillance
Outbreak Investigations. The 10 Step Approach. Zack Moore.MD. https://epi.publichealth.nc.gov/cd/lhds/manuals/cd/training/Module_1_1.6_ppt_OutbreakInvestigation.pdf

1. IP Team & Resources
• 638 bed Academic Teaching Center
• Located in the NW suburbs of Chicago
• Infection Prevention Program:
– 5 FTE (including manager position)
– Infection Prevention Physician Chair
– Data-mining software System

2. Establish existence of outbreak
What made this an outbreak?
Over the course of one month:
• 3 readmissions with CRE
• Specimen source varied
• Organism metallo beta-lactamase positive
• Confirmed strain as NDM-1(Epidemiologically
important pathogen)
• Eventually PFGE same

3. Verify the Diagnosis• Background
– Diagnosis
– Not lab error
– Commonality
• Possible cause
• Source spread of disease
4. Develop case definition
• Person, place & time
• Clinical information: characteristics,
location, time
Case finding:
Any patient identified with specimens
positive for Enterobacteriaceae metallo
beta lactamase and/or a readmission
history of GI procedure.

5. Case finding & line listing• Identification, clinical info, time, demographics,
location, risk factors, possible causes– Patient
– Sex
– Age
– Admit diagnosis
– Admit date
– Patient location
– Previous admissions and room locations
– Medical history (surgery, immuno-compromised)
– Risk Factors (e.g. prior nursing home stay, roommate of other CRE patient,
procedure, equipment)
– Culture and date of collection
– Treatment
– Discharge status

6. Descriptive epidemiology/develop hypothesis
• Three patients were identified with specimens
(e.g. ,urine, sputum,) positive for E. coli, New
Delhi metallo beta-lactamase and history of
GI lab procedure.
• Could this be related to specific procedure?
ERCP?

6. Descriptive Epidemiology/Timeline

IP and CCDPH Epi Review• Patient :88 years old female from Niles IL
• History of travel outside of the United States: None
• Potential Risk factors: Dementia, multiple antibiotic treatments due to
frequent UTI s
• Transmission source: No roommates during ALGH admissions
Location In Date Out Date Comment
Nursing home A 3/30/2013 Present Contact Precautions
ALGH Unit 15 W 3/26/2013 3/30/2013 Discharged to Nursing home A
ALGH Unit ER admit from home
2/25/2013 3/26/2013 Admit with UTI ,E.coli MBL
Nursing home A 2/22/2013 2/25/2013 UTI with VRE
ALGH 5 TWR (Admit from home /had 24 hr caregiver)
1/28/2013 2/2/2013 Admit for UTI

Epi-linked surveillance• Point prevalence surveillance for unrecognized
CRE cases and ongoing transmission.
• Conduct AST of patients with epidemiologic links to
a patient with CRE infection (i.e. patients in the
same unit).
• Partner with:
– Risk management
– Clinical unit
– Physicians
– Patient educationCDC Guidance for Control of Carbapenem-Resistant Enterobacteriaceae (CRE) 2012 CRE
Toolkit.

Evaluating the hypothesis
Step 8. Infection prevention measures:
• Review department policy & procedure
• Observation practice
- ERCP procedure (pre & post)
- High level disinfection
• Bring in equipment manufacturers
• Review & observe Environmental Services procedure
• Environmental surveillance (transmission source)
• Education
• Epi-linked surveillance (unit-based surveillance)

Cleaning and disinfection of Procedure Rooms: Including but not limited CATEGORY EQUIPMENT/ITEMS and FREQUENCY OF CLEANING PERSON WHO CLEANS
EQUIPMENT
Environment (items that do not touch the patient)
Daily, discharge cleaningO2 regulator, Suction regulatorHigh dusting Green Cord Organizer CoverC arm exterior & High dusting monitor screensPhones ,Chairs, Trash cansExterior of sharps containers, Windowsills*Suction compartment on floor near ERBE machineBumper guards, Top of supply cabinet Countertops (Gi lab to remove books, etc.)Floor: wet mop w/ H25 daily in evening
Environmental Services
Radiology Daily or when visibly soiledC arm and ESP-Cine, Instruments, cablesTechnician table, RBE cautery cartLead aprons
Radiology Tech
Laboratory After each use or when visibly soiledMicroscope stage; adjustment knobs; objectives; revolving nosepiece; armPlastic cover over Microscope when not in use
Histology tech
Nursing After each use or when visibly soiledEndo cart** Nurse Serve supply cartBlood pressure cuffsDaily Keyboards , Massimo leads, IV poles
Nursing
Intubation StationAnd Anesthesia Cart
After each use or when visibly soiledWork station areaAlaris IV pump; Propofol Infusion pumpWeeklyData Ohmeda monitor and cordsExterior of cart including wheels
Anesthesia
Epi-linked Active Surveillance Testing
• Develop ―detect and protect‖ screening
protocol– Engage your IP partners.(i.e. Nursing, IS, Physicians)-
– Conduct bed-trace of patients
– Provide education on CRE to both physicians and healthcare
associates including specimen collection.
– Provide patient education (SHEA MDRO FAQ)
– Connect with Laboratory about testing
– Follow up for any positive CRE screen results
– Performed on various nursing units, & Epi-link ECF

CRE Active Screening (AST)
Informing the patientA patient on the same unit you have been on has recently received diagnoses
of a very rare bacterial infection. The bacteria that caused this type of infection
have been seen in only 4% of US Hospitals. It is unclear at this time how this
individual became infected but we believe that this individual already had the
bacteria when they came into the hospital. Since this bacteria is resistant to
many antibiotics, we have notified the Illinois Department of Public Health.
Normally we would not do anything further but to better understand this rare
organism and for the safety of our patients, The Illinois Department of Public
Health has instructed the hospital to conduct a screening test on selected
patients. The screening test consists of an external swabbing of the rectum
using a QTip. The screening test will be done at no cost to you or your
insurance company. The results of the screening test will be shared with the
Illinois Department of Public Health and your physician.

Unit based AST• Conducted over various time frames of the
investigation:
– March , April, May, July
– All hospital epi-linked cultures were reported as
negative for CRE.

Environmental Surveillance• Vital part of investigation.
• Partner with laboratory
• Challenge of collecting cultures from various
surfaces, mechanical parts, liquids.
• Used E-swab, brush tips, sponge stick, TSB

Laboratory-Clinical Microbiology• Follow Clinical and Laboratory
Standards Institute guidelines
for susceptibility testing.
• Establish a protocol for detection of carbapenemase
production (e.g. modified Hodge test)
• Use e-swab for collection. Lab will place swab in TSB
broth with ertapenem and plate onto chromagar with
meropenem. This will identify any CRE. Additional
identification required to determine if CRE isolates are
NDM-1 strain.
• Establish system to ensure prompt notification of IP staff
of all CREs.CDC Vital Signs. Making Health Care Safer. Stop Infections from Lethal CRE Germs Now. March 2013.

Environmental Areas Sampled
7.Evaluate hypothesis & conduct additional studies
• Environmental culture found positive for
E.coli,NDM-1 (ERCP Scope, specifically at the
elevator platform)
• Epi-linked AST – negative (No unit based
transmission)
• Additional studies identified ―rugged‖ surface
inside ERCP scope elevator platform.

New Hypothesis*(4) NDM and (3) KPC patient cases were
identified from varied specimens (e.g. blood,
urine, sputum, wound)
and readmission history of GI lab procedure,
specifically same ERCP scope.
*Elevator section with possible platform defect.

8. (R) Implement control & prevention measures
• Re-reviewed department policies
-ERCP procedure
- High level disinfection
• Review manufacturer recommendations.
• Repeat audit of Environmental Services cleaning
process
• Engage manufacturers to audit associates performing
process.
• Additional environment culture ( Clean room & Storage
unit)
• Epi-linked AST
• Education

Additional studiesInside elevator platformActions taken:
• Scope A removed from service
• ALGH filed complaint with the FDA (SMDA)
• Initiated EPI-AID from the CCDPH/IDPH
• CDC arrival-August 2013
• Scope manufacturer notified of potential ―defect‖
• Scope A sent to CDC for investigation
• CDC partnering with(FDA)for guidance &recommendation
• Complete high level disinfection process reviewed.
• Retrospective review and direct observation of endoscope reprocessing did
not identify lapses in protocol.
Prevention steps taken:
New scope purchased to replace scope A
Next steps:
Continue investigation- how & why related to the scope
CDC Partners • Initial CDC findings:
PFGE results of Cluster : genetically related.
• Suggesting that Hospital 1 was the source of
transmission for many of the patients with
subsequent transmission at ECF between
two roommates.
• Scope A sent to CDC for further analysis and
was confirmed as positive for NDM isolate.

ERCP Specimen CollectionNON-DESTRUCTIVE RECOVERY OF ENTERIC BACTERIA FROM DUODENOSCOPE
Equipment Materials and Reagents
ERCP scope, post ETO sterilization Sterile gloves
E-swab (green top)
Plastic specimen transport bag
Method
Note: Due to the length of the device, it is recommended that this sampling procedure be performed by
two persons, with one holding the endoscope steady while the other manipulates it.
• Don sterile gloves.
• Using the endoscope controls, manipulate the last 1.5-2 inches of the tip several times.
• Swab the endoscope channel tip, and the elevator channel repeatedly with the E-swab, moving
back and forth 15 times.
• Place swab in E-swab container. Label container accordingly.
• Complete lab requisition.
• Transport in plastic bag to laboratory. Hand-off to Microbiology Tech.
•

Elevator mechanism - distal tip

PFGE results

9. Communication
• Patient Notification of all who had ERCP
procedures with Scope A
• IP Resources: Administration, Risk
Management, Public Relations,
CCDPH,IDPH, CDC
– Weekly conference calls
• Deliver consistent message to public
• Ensure any patients screened positive are
informed, verbally and in writing.

Patient Notification LetterName
Address
Chicago, IL
Dear (Insert Patient Name):
Advocate Lutheran General Hospital values the trust you place in us to provide you with the safest and highest quality of care. As a healing ministry, we want
you to know that the safety of our patients and the communities we serve is our top priority. As a valued patient, you are receiving this letter because you
underwent a procedure at the hospital between (x and x timeframe) and we want you to be aware of a potential concern we are investigating.
Your procedure involved the use of a piece of medical equipment called an endoscope. We recently learned that microscopic bacteria may have been present
on the endoscope used during your procedure. It is out of an abundance of caution we are requesting that you schedule an appointment to come in for a free
screening in our outpatient clinic to ensure that you were not exposed.
Please call our GI Lab at (847) 723-6800 between the hours of 8 a.m. and 4 p.m., Monday through Friday to schedule your screening at a time that is
convenient for you.
We recognize that this may be upsetting to you and cause you some concern. Should you have any immediate questions that you would like answered prior to
your screening, please dial the same GI Lab number above and ask to leave a message for Dr. Dean Silas who serves as Medical Director of our GI Lab. He
will respond to your inquiry within 24 hours.
Sincerely,
President
President, Medical Staff

Patient Notification Line ListMRN/Name
ADDRESS PHONE GI MD INPT/OUT PCP
MD
Notification
Requested
Screening
date
Notification
date Results

CRE Positive Screen LetterName
Address
City
Dear ________,
This letter is in follow-up to the recent phone conversation regarding your test results.
The results of your screening test indicate that you have been identified as having a positive carbapenem-resistant Enterobacteriaceae (CRE)
screen result. This positive CRE screening result means that you have been colonized with the CRE germ. CRE colonization means that the
organism can be found on the body but may not cause any symptoms or disease.
If you have already granted us approval to share these results with your Primary Care Physician, a copy of these results will be mailed to your \
doctor’s office. If you so choose, you may want to discuss these results with your physician. If you have additional questions, please feel free to
contact Manager of Infectious Disease Prevention at (847) 723-6353 or, Director, Division of
Infectious Diseases at (847) 723-7638.
Advocate Lutheran General Hospital values the trust you place in us to provide you with the safest and highest quality of care. As a healing
ministry, we want you to know that the safety of our patients and the communities we serve is our top priority.
Sincerely,
Chief Operating Officer Director, Division of Infectious Disease

Negative Screen LetterInsert Date
Insert Name
Address
City, State Zip
Dear ___________,
The purpose of this letter is to inform you of your results from your recent screening test at Advocate Lutheran General Hospital.
The results of your screening test indicate that you have a negative carbapenem-resistant Enterobacteriaceae (CRE) screen
result. This means that the CRE germ was not present at the time of screening. At this time there is no further action you need to
take.
We apologize for any inconvenience and anxiety this may have caused you. At Advocate Lutheran General Hospital we value the
trust you place in us to provide you with the safest and highest quality of care. As a healing ministry, we want you to know that the
safety of our patients and the communities we serve is our top priority.
Sincerely,
Chief Operating Officer Director, Division of Infectious Disease

Public Relations• Lutheran General has recently been investigating a cluster of patients who have presented to ALGH with an
organism of significance (New Delhi Metallo Beta-Lactamase) or NDM-1.
• It falls under the class of CRE, which stands for Carbapenem-resistant Enterobacteriaceae, which are part (or
subgroup) of Enterobacteriaceae that are difficult to treat because they are resistant to commonly used antibiotics.
Occasionally CRE are completely resistant to all available antibiotics. CRE are an important threat to public health.
• I am not sure if it would get any media attention, but since some of our area skilled nursing facilities are also
working with the Health Department, I wanted to make sure you were aware of the situation. I have also notified
Donna Currie & Dr. Malow (Oakbrook Support Center-Patient Safety/Infection Prevention)
• Talking bullets:
• Identified several cases of New Delhi Metallo Beta-Lactamase (CRE- E.Coli) from the community
• Working with the Cook County Health Department & the Illinois Dept of Public Health
• Implemented all health dept recommendations, as well as the CDC recommendations ( CRE Tool kit)
http://www.cdc.gov/hai/organisms/cre/cre-toolkit/
• No evidence of hospital transmission identified
• The weblink above may also have media related Q&A.
• Any additional questions please feel free to contact me

Community Outreach
• Transparency
• Contacting patients/outreach to patients in
ECFs
• IP resources included Post Acute Network,
CCDPH to follow up on screening patients
discharged to LTCFs.
• Additional mailings to patients who did not
respond with first letter sent by certified mail.

Reaching out to associatesMEMORANDUM
Friday,
TO: All Associates
FROM: Barb Weber, Interim President, COO, Advocate Lutheran General Hospital
SUBJECT: Patient Safety
As an associate of Advocate Lutheran General Hospital, you know that providing the safest and highest quality care to those we are privileged to serve is our top priority.
Regrettably, I’m writing to inform you about an issue that affected a small number of our patients.
These patients were exposed to carbapenem-resistant Enterobacteriaceae (CRE), while undergoing a specific endoscopic procedure here at our hospital. CRE are a family of
germs that are highly-resistant to antibiotic treatment and are most likely to affect people with compromised immune systems.
Out of an abundance of caution, we decided to notify every patient who underwent this endoscopic procedure here at the hospital between January and September of this year to
ask that they return to the hospital for a free screening to test for the presence of the bacteria.
While we understand the anxiety this may cause patients, our number one goal is to ensure the well-being of those who have entrusted us with their care.
As part of our investigation into this incident, we have been working closely with the Centers for Disease Control and Prevention (CDC), the Federal Drug Administration (FDA),
the Illinois Department of Public Health (IDPH) and Cook County’s Department of Public Health. With their partnership and guidance, we feel confident that we have taken the
appropriate steps to ensure no other patients are at risk and that this does not happen again.
Given our ongoing commitment to building a strong culture of patient safety and transparency in care, we have decided to proactively share our story with the local media. We
hope that the lessons we have learned and the steps we have taken to remedy this matter can serve as a learning opportunity for other hospital care settings.
We have established a hotline to handle any calls regarding this matter, should you receive any calls, please direct them to our Infection Prevention Department at 847.723.6353.
And as always, should you have any additional questions, please do not hesitate to contact a member of our senior leadership team.

Findings: Patient Screening • Patient screening indentified link to additional
ERCP scopes.
• CDC confirmed their Environmental
Surveillance cultures were negative.
• Additional Epi-linked surveillance was negative
(no unit based transmission identified)

Evaluate hypothesis*• A patient who had an ERCP with scope ―C‖ had a positive culture
for E.coli MBL (metallo beta lactamase). This was the second case
identified with the same source scope.
• There was a one month period of no discernible transmission
between cluster 1 associated with scope ―A‖ and cluster 2
associated with scope ―B‖.
* New Hypothesis:We have a repeated instance of another new scope associated with
E.coli MBL, this would imply the source of the biofilm may be located
within the integral components of the AER (automated endoscope
reprocessor) which functions to wash and disinfect the scopes.

Epi Curve- Scopes
NewDelhi Metallo-β-Lactamase–Producing Carbapenem-Resistant Escherichia coli ssociated With Exposure to Duodenoscopes. Lauren Epstein ,MD., et al. JAMA. 2014;312(14):1447-1455.

8. (R)Infection Control Measures• Manufacturer product evaluation of our AER equipment.
• Review manufactures recommendation of products (detergent,
disinfectant)
• AER bay’s were bleached.
• Detergent and alcohol lines bleached.
• Performed environmental surveillance cultures of AER reservoir
holding tanks and filters.
• Patient notification for those who had ERCP with Scope C.
• Moved from HLD to sterilization with ETO (ethylene oxide).
• ERCP scopes post sterilization were cultured.
• Repeat audit of ERCP patient procedure (pre, during and post)
• Repeat audit of Environmental Services protocol.
• Prior to ERCP procedure, conduct AST CRE screening.

Findings:
• Scope B identified as Epi-link to an infected
patient per CDC review.
• Hospital filed additional SDMA forms for
Scopes B and C.
• Patient notification-expanded to include all
patients that received ERCP during defined
timeframe.
• Environmental cultures negative.
• No AER deficits identified.

CRE Network Diagram
NewDelhi Metallo-β-Lactamase–Producing Carbapenem-Resistant Escherichia coli Associated With Exposure to Duodenoscopes. Lauren Epstein ,MD., et al. JAMA. 2014;312(14):1447-1455
Final Hypothesis*
• Inability to effectively High Level Disinfect
ERCP scopes.
• Challenges of equipment design
impacting the cleaning and disinfection process.
Service, maintenance, length of time device kept
in service.
• Options for alternative methodologies to ensure
equipment is safe for patients.
10. Maintain Surveillance• Surveillance –(CRE alert using data mining system)
• Quality Control Plan: GI Lab
– On a monthly basis, each ERCP endoscope will be cultured
specifically for CRE
– Follow the method described in obtaining samples for
culture using the E-swab.
– (2) swabs from each ERCP & EUS scope (Elevator up &
down position)
– GI lab to maintain record of results

GI Lab IP Plan 2014Prevention Strategies Action Item
(time line)
Accountable Person(s) Intervention
evaluation
(supporting data)
Date of Completed
Screening process 8/7/13 - ongoing Linda Stein Send certified letter to all remaining
unscreened patients.
2/15/14
Sterilization
Follow-up recommendations:Monthly CRE cultures
CDC did not give a recommendation for ongoing environmental or scope culturing
Surveillance cultures of ERCP scopes
GI Lab
Lloyd Hendrick
GI Lab
Last know procedure using HLD was on 10/08/13 that resulted in positive result.
ETO sterilization Process began::
Add scope serial # to CPD tracking system
Monthly culturing
Monthly culture (2) per scope. Elevator in up & down position. Any positive results should be communicated to infection prevention.
10/7/13 Monday
10/8/13 Tuesday
4/1/14
Process began: 2/25/14
On-going
No positives to date 4/23/14
Misc items: Process moving
forward
1. Portable phone
2. Outpatient #365 screening
3. Open financial accts
Recommend closing cluster
investigation
Beth Quinones(Outpatient)
Chad Calabria (Pt intake)
Cori Taylor(Communications)
Presented at Infection
Prevention Committee
Close all open accounts
Return phone to
communications
4/10/14
Cluster investigation officially
closed
4/23/14
All open accts will be closed.

Lessons Learned
• Keep a log/diary of investigation (timeline)
• Senior leadership is essential (resource allocation)
• Challenges in using sterilization as a method to ensure
safety of scopes
• Become familiar with endoscopic design (e.g. ERCP,
EUS).
• Annual competency & education
• System-wide standardization of products versus
manufacturer recommendations
• Renewed respect for associates dedicated to doing this
job, every day.

Looking towards the future• Review and update of current guidelines for
cleaning and disinfection of endoscopes
• More options from manufacturers
• Is sterilization the way?
• Biofilm and in-vitro interaction with equipment

IP Outbreak Resources “Village”
Hospital Administration
Risk Management
Nursing Units
ID Physicians
Environmental Services
Laboratory Services
Professional Associations
Biomedical Engineering
Materials Management
Vendors/Manufacturers
Quality Management
Central Processing/Sterilizati
on
Medical Records/Information
services
Regulatory/CCDPH/IDPH/CDC/FDA
Data Mining Services
Public Relations/Media
Other HCF/ECF
Our “Village”

Acknowledgments to our “Village”
Lidia Raslau/Norah Connelly/Dr. Dean Silas
GI Lab Chad Calabria Patient Registration
Dusanka Bjelan/Evangheline Feldiorean
GI Lab Beth Hickey Finance
Lynn Guibourdanche, Sinead Forkan Kelly
Infection Prevention Valarie Diaz/Beth Quinones Outpatient Dept
Joanna Werling/Victoria Marriott
Administrative assistance
Michael Wiegel Risk Management
Dr. Robert Citronberg Infectious Disease Marcel Trutza Biomedical Engineering
Dr. Leo Kelly VP Medical Management (EMT)
Michael Costello/Janet Havel ACL Lab
Barb Weber COO (EMT) Michael Vernon/Mabel Frias CCDPH
Cindy Mahal-VanBrenk Director ,Surgery Allison Arwady/Judy Conway/Craig Conover
IDPH
Pamela Hyziak Clinical Excellence Drs. Lauren Epstein/Jennifer Hunter/Alice Guh
CDC
Trent Knanishu Environmental Services
Joyce Welton Supply Chain Management

JAMA October 8, 2014 Volume 312, Number 14

References• Brief report: Early identification and control of carbapenemase-producing Klebsiella
pneumoniae, originating from contaminated endoscopic equipment. Sally F. Alrabaa
MD, et. al, American Journal of Infection Control 41 (2013): 562-4.
• CDC Guidance for Control of Carbapenem-Resistant Enterobacteriaceae (CRE) 2012
CRE Toolkit.
• CDC Vital Signs. Making Health Care Safer. Stop Infections from Lethal CRE Germs
Now. March 2013.
• EIS Conference Abstract. Cluster of New Delhi Metallo-β-Lactamase-Producing
Carbapenem-Resistant Enterobacteriaceae at a Hospital — Illinois, 2013. April, 2014
• Notes from the Field: Hospital Outbreak of Carbapenem-Resistant Klebsiella
pneumoniae Producing New Delhi Metallo-Beta-Lactamase- Denver, Colorado, 2012.
MMWR, February 15,2013, vol. 62, no.6, p. 108.
• Notes from the Field: New Delhi Metallo-β-Lactamase–Producing Escherichia coli
Associated with Endoscopic Retrograde Cholangiopancreatography — Illinois, 2013.
MMWR, January 3, 2014, vol 62, no. 51, p.1051-1051.
• Outbreak Investigations. The 10 Step Approach. Zack Moore.MD.
https://epi.publichealth.nc.gov/cd/lhds/manuals/cd/training/Module_1_1.6_ppt_Outbre
akInvestigation.pdf
