original article temporal branch of the facial nerve and ... filea result of paralysis of the...
TRANSCRIPT

ORIGINAL ARTICLE
Temporal Branch of the Facial Nerveand Its Relationship to Fascial LayersSeda T. Babakurban, MD; Ozcan Cakmak, MD; Simel Kendir, MD;Alaittin Elhan, PhD, MD; Vito C. Quatela, MD
Objectives: To eliminate the inconsistency in the no-menclature, to anatomically and definitively describe thetopographic relationship of the temporal branch of thefacial nerve to the fascial layers and the fat pads, and tocreate an effective algorithm to define the safest ap-proaches and planes for surgical procedures in this area.
Methods: The study was performed using 18 hemifa-cial cadaveric specimens. In 12 hemifacial specimens, thefacial halves were coronally sectioned and dissected. In6 hemifacial specimens, planar dissection was per-formed layer by layer.
Results: The temporal branch of the facial nerve that tra-versed inside the deep layers of the temporoparietal fas-cia and the superficial musculoaponeurotic systemcoursed along the zygomatic arch as 1 (14.3%), 2 (57.1%),
3 (14.3%), and 4 (14.3%) twigs in the specimens. Thetemporoparietal fascia had no attachment to the zygo-matic arch and continued caudally as the superficial mus-culoaponeurotic system. Adhesions were between the tem-poroparietal fascia and the superficial layer of the deeptemporal fascia around the zygomatic arch. In most speci-mens, the superficial layer of the deep temporal fascia con-tinued as the parotideomasseterica fascia, and a deep layerabutted the posterosuperior edge of the zygomatic arch.
Conclusion: An easy and safe surgical approach in thisarea is to elevate the superficial layer deep to the inter-mediate fat pad directly on the deep layer of the deep tem-poral fascia descending to the periosteum along the zy-gomatic arch.
Arch Facial Plast Surg. 2010;12(1):16-23
T HE TEMPORAL BRANCH OF
the facial nerve has be-come of great importancewith advanced techniquesof deep-plane face-lifting,
subperiosteal midface-lifting, endo-scopic forehead-lifting, and interfascial dis-sections in craniofacial and trauma sur-gery. Injury to the temporal branch of thefacial nerve results in cosmetic defects asa result of paralysis of the corrugator su-percilii, frontalis, and orbicularis oculimuscles. Understanding the anatomy ofthis area and the trajectory of the tempo-ral branch of the facial nerve is critical topreserve it from injury. Despite many stud-ies1-29 in the literature, controversy re-mains about the topographic relation-ship of the fascias, the fat pads, and thetemporal branch of the facial nerve and itsnomenclature. The objectives of this studywere to eliminate the inconsistency in thenomenclature, to anatomically and defini-tively describe the topographic relation-ship of the temporal branch of the facialnerve to the fascial layers and the fat pads,and to create an effective algorithm to de-
fine the safest approaches and planes forsurgical procedures in this area.
METHODS
The study was performed using 18 hemifacialspecimens from fixed and fresh cadavers ob-tained from the Department of Anatomy, Fac-ulty of Medicine, Ankara University, Ankara,Turkey. Before dissection, the course of the tem-poral branch of the facial nerve was marked onthe skin of each cadaver’s face. First, the Pit-anguay line (connecting the lobule with one-half the distance between the superior borderof the external auditory canal and the lateralcanthus) was drawn, and the point at whichthat line bisected the zygomatic arch wasmarked. Two other points that were 1.5 cm an-terior and 1.5 cm posterior to the first pointwere marked, depending on the length of thezygomatic arch. Then, second and third linesthat bisected the second and third points sepa-rately were drawn from the temporal region tothe cheek. These 2 coronal strips of tissue wereincised down to the temporal muscle above andto the masseter muscle below, including a coro-nal segment of the zygomatic arch (Figure 1).The 2 sections were en bloc resected, and the
Author Affiliations:Department ofOtorhinolaryngology, Faculty ofMedicine, Baskent University,Ankara (Dr Babakurban);Department ofOtorhinolaryngology, Faculty ofMedicine, Acibadem University,Istanbul (Dr Cakmak), andDepartment of Anatomy,Faculty of Medicine, AnkaraUniversity, Ankara (Drs Kendirand Elhan), Turkey. Dr Quatelais in private practice inRochester, New York.
(REPRINTED) ARCH FACIAL PLAST SURG/ VOL 12 (NO. 1), JAN/FEB 2010 WWW.ARCHFACIAL.COM16
©2010 American Medical Association. All rights reserved.
Downloaded From: https://archfaci.jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/10/2019

anterior and posterior halves of the coronal strips were dis-sected under an operating microscope using magnification of�6 to �40. In 6 hemifacial specimens, planar dissection fromthe skin to the bone was performed layer by layer under theoperating microscope.
The nomenclature in the literature is inconsistent for cer-tain fascias and the fat pads of this region. Therefore, pre-ferred names (given in the Table and in Figure 2) are usedherein to avoid confusion.
RESULTS
FASCIAL LAYERS AND FAT PADS
The temporoparietal fascia and the deep temporal fasciawere identified on the anterior, middle, and posterior partsof each coronal strip. Above the zygomatic arch, the tem-poroparietal fascia was composed of multiple (3-4) lay-ers (Figure 3 and Figure 4) that were integrated withthin fibrous septa immediately deep to the subcutane-ous layer.
The temporoparietal fascia could be easily dissectedfrom the superficial layer of the deep temporal fascia abovethe zygomatic arch (Figures 5, 6, 7, and 8). Descend-ing to the zygomatic arch, a discrete fatty layer called thesuperficial fat pad was encountered between the super-ficial layer of the deep temporal fascia and the temporo-parietal fascia (Figures 3 and 5). This fat pad disap-peared below the middle level of the zygomatic arch. Thesuperficial fat pad was encountered in middle parts ofall specimens. However, this fatty layer was not visiblein 27.3% of posterior parts and 9.1% of anterior parts ofspecimens. The mean vertical lengths of the superficialtemporal fat pad were 14, 20, and 25 mm, respectively,
in posterior, middle, and anterior parts of specimens. Al-though this layer was thin (�2 to �3 mm) in 36.3% ofposterior, 36.4% of middle, and 27.3% of anterior partsof specimens, it was too thin (�1 to �2 mm) in 27.3%of posterior, 27.3% of middle, and 27.3% of anterior partsof specimens, and was thick (�3 to �4 mm) in 9.1% ofposterior, 36.3% of middle, and 36.3% of anterior partsof specimens.
The temporoparietal fascia had no attachment to thezygomatic arch (Figures 3, 4, and 5). The temporopari-etal fascia descending to the zygomatic arch lost its fas-cial layers and became a foamy tissue (Figures 3 and 6).The level of change varied and was observed at approxi-
1 2
Figure 1. Lines of the 2 coronal strips of tissue.
Table. Naming of the Fascias and the Fat Padsin the Literature
Anatomic Name Synonyms Preferred Name
Fascia superficialis,1
superficialtemporal fascia, ortemporoparietalfascia15
Superficial temporalfascia,3,7,10,12,16,17,25,26
temporoparietalfascia,2-4,9,12,19 epicranialaponeurosis,14 galea,20
aponeurotic fascia,11
subgaleal fascia,13,28
or superficialmusculoaponeuroticsystem7
Temporoparietalfascia
Fascia temporalis1 ortemporal fascia15
Temporal fascia,14,15,19,21
deep temporalfascia,3,9-11,16,17,22,26
superficial temporalfascia,20,25 or temporalismuscle fascia11
Deep temporalfascia
Fascia temporalis(laminasuperficialis),1
temporal fascia, orsuperficiallaminae15
Innominate fascia,3,12
superficial layerof deep temporalfascia,3,9,11,14,16,17,19,21
intermediate temporalfascia,7,25 or superficialtemporal fascia8
Superficial layerof deeptemporalfascia
Fascia temporalis(lamina profunda),1
temporal fascia, ordeep laminae15
Deep layer ofdeep temporalfascia3,9,11,14,16,17,19,21
or deep temporalfascia7,8,12,25
Deep layer ofdeeptemporalfascia
Temporoparietal fatpad15
Suprafascial fat pad,8
subaponeuroticplane,3,9,26 loose areolarplane,3 loose areolartissue,10,14 innominatefascia,27 superficial fatpad,7,11,17,20 or subgalealfat pad20
Superficial fatpad
Superficial fat pad15 Interfascial fat pad,8,20
superficial fat pad,3,9,14,16
intrafascial fat pad,20
intermediate fatpad,7,10,11,17 middle fatpad,11 or temporal fatpad29
Intermediate fatpad
Corpus adiposumbuccae1
Subfascial fat pad,8 deepfat pad,3,7,9-11,14,16,17 orbuccal fat pad29
Deep fat pad
Temporal branch ofthe facial nerve15 ornervus facialis(rami temporales)1
Frontal branch,3,7,8,11,12,16-19
temporalbranch,8,10,11,14,18,20,23-25
or frontotemporalbranch9,14,21
Temporalbranch
(REPRINTED) ARCH FACIAL PLAST SURG/ VOL 12 (NO. 1), JAN/FEB 2010 WWW.ARCHFACIAL.COM17
©2010 American Medical Association. All rights reserved.
Downloaded From: https://archfaci.jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/10/2019
mately 1 cm above the zygomatic arch in 18% of speci-mens (6 of 33 sides of 11 specimens), in the upper levelof the zygomatic arch in 64% (21 of 33 sides of 11 speci-mens), and in the middle of the zygomatic arch in 18%(6 of 33 sides of 11 specimens). The fascia continued as asuperficial musculoaponeurotic system (SMAS) below thezygomatic arch (Figure 3 and Figure 9). Beginning froma level between the upper edge and the middle of the zy-gomatic arch, tight adhesions were observed between thetemporoparietal fascia and the superficial layer of the deeptemporal fascia, which covered the zygomatic arch, the mas-seter muscle, and the parotid gland (Figure 9 andFigure10). Below this level, the plane could only be foundusing sharp dissection between these layers (Figure 9).However, at the level of the parotid gland, fibrous inden-tations were observed from the temporoparietal fascia intothe superficial layer of the deep temporal fascia coveringthe parotid gland (Figure 6), and no dissection plane wasnoted among the SMAS, the superficial layer of the deeptemporal fascia, and the parotid fascia (Figure 9).
The deep temporal fascia lay under the superficial fatpad and covered the temporal muscle. The thick singlelayer of the upper part of the deep temporal fascia sepa-rated into the superficial layer and the deep layer as it
descended to the zygomatic arch, and a fibrofatty tissuecalled the intermediate fat pad filled the space betweenthese layers (Figures 3, 4, and 7 and Figure 11). Thedeep layer of the deep temporal fascia could be easily dis-sected from the intermediate fat pad (Figure 11). How-ever, dissection of the superficial layer of the deep tem-poral fascia from the intermediate fat pad was moredifficult because of extensions of a fibrous network of thefat pad and arteriovenous perforators. In 10 specimens,the layers of the deep temporal fascia did not fuse above
S
SFP
SMAS
PMF
TPF
DTF
D-DTF
S-DTF
TM
IFP
DFP
ZA
MM
PG
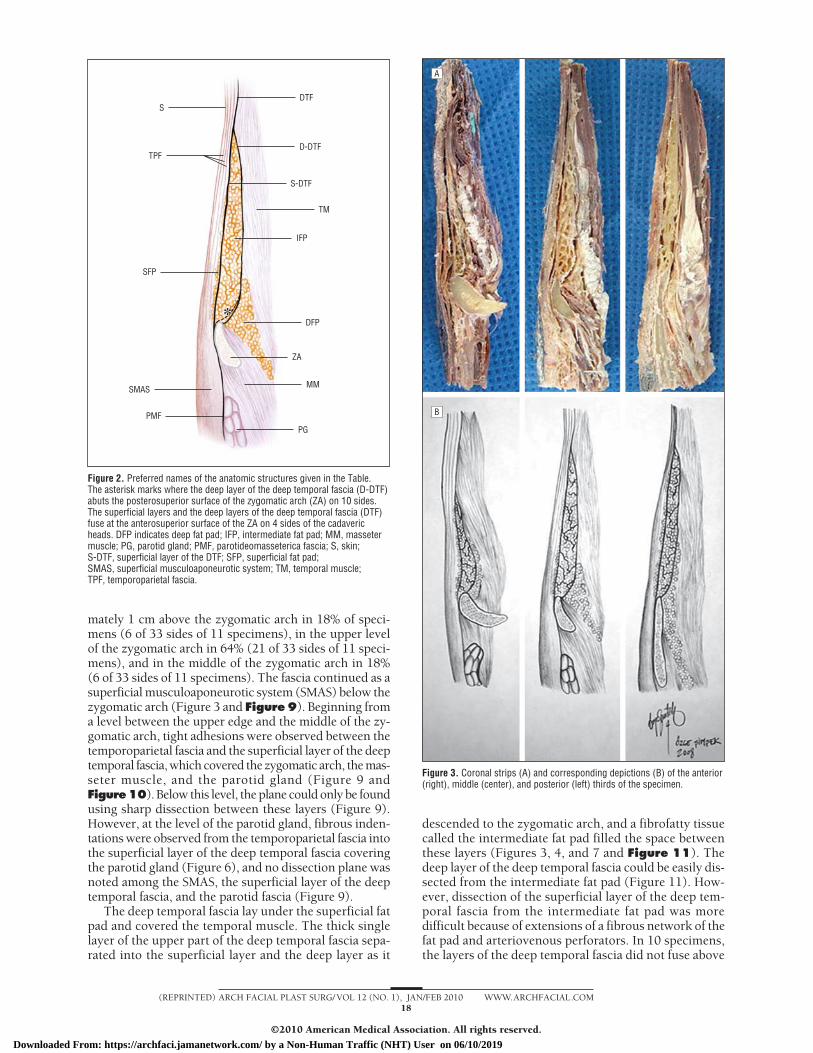
Figure 2. Preferred names of the anatomic structures given in the Table.The asterisk marks where the deep layer of the deep temporal fascia (D-DTF)abuts the posterosuperior surface of the zygomatic arch (ZA) on 10 sides.The superficial layers and the deep layers of the deep temporal fascia (DTF)fuse at the anterosuperior surface of the ZA on 4 sides of the cadavericheads. DFP indicates deep fat pad; IFP, intermediate fat pad; MM, massetermuscle; PG, parotid gland; PMF, parotideomasseterica fascia; S, skin;S-DTF, superficial layer of the DTF; SFP, superficial fat pad;SMAS, superficial musculoaponeurotic system; TM, temporal muscle;TPF, temporoparietal fascia.
A
B
Figure 3. Coronal strips (A) and corresponding depictions (B) of the anterior(right), middle (center), and posterior (left) thirds of the specimen.
(REPRINTED) ARCH FACIAL PLAST SURG/ VOL 12 (NO. 1), JAN/FEB 2010 WWW.ARCHFACIAL.COM18
©2010 American Medical Association. All rights reserved.
Downloaded From: https://archfaci.jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/10/2019

the zygomatic arch. In these specimens, the deep layerabutted the periosteum of the posterosuperior edge of thezygomatic arch (Figure 3), and the superficial layer de-scended through the anterior surface of the zygomaticarch to form the parotideomasseterica fascia inferiorly(Figure 5). However, on 4 sides of the cadaveric heads,the superficial layer and the deep layer of the deep tem-poral fascia fused at the anterosuperior edge of the zy-gomatic arch and continued inferiorly as a single layerto form the parotideomasseterica fascia (Figure 2).
The mean vertical lengths of the intermediate fat padwere 23, 24, and 37 mm, respectively, in posterior, middle,and anterior parts of specimens. The intermediate fat layerwas divided into several lobules by a fibrous network(Figure 3). There were arteries (1-2 mm in diameter) andveins (2-3 mm in diameter) in the fat pad (Figure 11).Although small vessels were common, several larger ves-sels were also encountered in each coronal strip at 5 to24 mm from the zygomatic arch.
Another fat pad (called the deep fat pad) was ob-served between the deep temporal fascia and the tempo-
ral muscle. This layer (called the buccal fat pad) contin-ued between the masseter muscle and the temporal muscleinferiorly (Figures 4, 7, and 11).
TM
DFP
IFP
TPF
ZA
MM
Figure 4. Dissection of the middle third of the coronal strip. Thetemporoparietal fascia (TPF) is composed of multiple layers. DFP indicatesdeep fat pad; IFP, intermediate fat pad; MM, masseter muscle; TM, temporalmuscle; ZA, zygomatic arch.
TB-FN
TPF
SFP
PMF
S-DTF
ZA
Figure 5. Dissection of the hemiface of a cadaver. The superficial layer of thedeep temporal fascia (S-DTF) continues as the parotideomasseterica fascia(PMF). SFP indicates superficial fat pad; TB-FN, temporal branch of the facialnerve; TPF, temporoparietal fascia; ZA, zygomatic arch.
TB-FN
TFA
ZA
TM
S-DTF
PG
TPF
Figure 6. Dissection of the posterior third of the coronal strip. There arefibrous indentations from the temporoparietal fascia (TPF) into thesuperficial layer of the deep temporal fascia (S-DTF) covering the parotidgland (PG). TB-FN indicates temporal branch of the facial nerve;TFA, transverse fascial artery; TM, temporal muscle; ZA, zygomatic arch.
TM
D-DTF
S-DTF
TB-FN
IFP
DFP
ZA
TPF
Figure 7. The topographic relationship of the temporoparietal fascia (TPF) tothe temporal branch of the facial nerve (TB-FN). The temporal branch twigsof the facial nerve course within the TPF. D-DTF indicates deep layer of thedeep temporal fascia; DFP, deep fat pad; IFP, intermediate fat pad;S-DTF, superficial layer of the DTF; TM, temporal muscle;ZA, zygomatic arch.
(REPRINTED) ARCH FACIAL PLAST SURG/ VOL 12 (NO. 1), JAN/FEB 2010 WWW.ARCHFACIAL.COM19
©2010 American Medical Association. All rights reserved.
Downloaded From: https://archfaci.jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/10/2019

TEMPORAL BRANCH OF THE FACIAL NERVE
Division of the temporal branch of the facial nerve oc-curred in the parotid gland. The temporal branch of thefacial nerve emerged from the parotid gland below thezygomatic arch (Figures 6 and 10) and traversed insidethe temporoparietal fascia over the zygomatic arch(Figures 5 and 7) following the Pitanguay line. The num-
bers of temporal branch twigs passing over the zygo-matic arch were 1 (14.3%), 2 (57.1%), 3 (14.3%), or 4(14.3%) in the specimens (Figure 8). There was approxi-mately 3 mm between the frontal nerve and the bone overthe zygomatic arch in the fresh cadaver specimens(Figure 10). Although the frontal nerve traversed insidethe deep layers of the SMAS and the temporoparietal fas-cia (Figure 7), no obvious dissection plane was encoun-tered between the superficial layer of the deep temporalfascia and either the SMAS or the temporoparietal fasciasurrounding the temporal branch twigs over the zygo-matic arch. Above the zygomatic arch, a fat layer calledthe superficial fat pad was observed between the tempo-roparietal fascia and the deep temporal fascia, and a thin
S-DTF
PG
TB-FN
TPF
Figure 8. The temporal branch twigs of the facial nerve. The facial nervetraverses along the zygomatic arch as multiple twigs. PG indicates parotidgland; S-DTF, superficial layer of the deep temporal fascia; TB-FN, temporalbranch of the facial nerve; TPF, temporoparietal fascia.
SFP
PG
TPF
SMAS
IFP
S-DTF
ZA
MM
Figure 9. Dissection of the middle third of the coronal strip in a freshcadaver specimen. The superficial layer of the deep temporal fascia (S-DTF)continues across the zygomatic arch (ZA) as the parotideomassetericafascia. The temporoparietal fascia (TPF) continues as the superficialmusculoaponeurotic system (SMAS). IFP indicates intermediate fat pad;MM, masseter muscle; PG, parotid gland; SFP, superficial fat pad.
TB-FN
ZA
Figure 10. The topographic relationship of the temporal branch of the facialnerve (TB-FN) to the zygomatic arch (ZA). The distance between the ZA andthe TB-FN piercing the fascia is 3 mm. The asterisk marks where the tissuewas horizontally cut to show the relationship.
TPF
S-DTF
SFP
ZA
DTF
TM
D-DTF
V
A
IFP
DFP
MM
A B
1
23
Figure 11. Dissection of the layers of the deep temporal fascia (DTF) andschematic view of surgical approaches to reach the zygomatic arch (ZA)through the intermediate fat pad (IFP). A, The deep layer of the DTF (D-DTF)can be easily dissected from the IFP. B, Three possible approaches indicatedby numbers 1, 2, and 3 (see the last paragraph of the “Comment” section fora discussion). The asterisk marks the subgaleal dissection plane. A indicatesartery; DFP, deep fat pad; MM, masseter muscle; S-DTF, superficial layer ofthe DTF; SFP, superficial fat pad; TM, temporal muscle; TPF, temporoparietalfascia; V, vein.
(REPRINTED) ARCH FACIAL PLAST SURG/ VOL 12 (NO. 1), JAN/FEB 2010 WWW.ARCHFACIAL.COM20
©2010 American Medical Association. All rights reserved.
Downloaded From: https://archfaci.jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/10/2019

layer of the temporoparietal fascia covered the temporalbranch of the facial nerve medially in all specimens(Figure 5).
COMMENT
Despite many studies, controversy remains about the to-pography of the temporoparietal fascia, which com-prises a fascial layer just under the subcutaneous tissuein the temporal region extending to the parietal region.1
After description of the SMAS of the face by Mitz and Pey-ronie,2 the temporoparietal fascia was recognized as im-portant to the temporal branch of the facial nerve. Theseauthors stated that the SMAS was a fibromuscular net-work located between the facial muscles and the der-mis. According to their observations, the SMAS “crossesin front of the zygomatic arch and belongs to the tem-porozygomatic SMAS”2(p85) and is independent of the pa-rotid fascia. In 1988, Hing et al3 noted that the tempo-roparietal fascia was attached to the zygomatic arch. In1989, Stuzin et al4 demonstrated in cadaver dissectionsthat the temporoparietal fascia continued as the SMASacross the zygomatic arch but was not in anatomic con-tinuity with the periosteum of the zygomatic arch. How-ever, Gosain et al5 claimed that the SMAS was not in ana-tomic continuity with the temporoparietal fascia. Gassneret al6 supported the finding by Gosain et al and statedthat the SMAS and the temporoparietal fascia were in cor-responding anatomic layers but lost their anatomic con-tinuity when they fused with the zygomatic arch. In con-trast, Campiglio and Candiani7 and Coscarella et al8
claimed that the temporoparietal fascia abutted the zy-gomatic arch and comprised the parotideomasseterica fas-cia below the zygomatic arch. Our results agree with theobservation by Stuzin et al4 that the temporoparietal fas-cia had no attachment to the zygomatic arch. Our find-ings are consistent with most studies4,9-11 in the litera-ture reporting that the temporoparietal fascia continuesas the SMAS below the zygomatic arch. However, we dem-onstrate herein that the temporoparietal fascia becomesa foamy tissue between the upper level of the zygomaticarch and approximately 1 cm above the zygomatic arch.We also show that there are adhesions between the tem-poroparietal fascia and the superficial layer of the deeptemporal fascia between the upper and middle levels ofthe zygomatic arch. Because of the fusion, elevation re-quires sharp dissection between these layers; this couldendanger the temporal branch of the facial nerve, whichis protected by only a thin layer of spongiosis-type tem-poroparietal fascia or SMAS over the zygomatic arch. How-ever, we observed fibrous indentations from the SMASinto the superficial layer of the deep temporal fascia cov-ering the parotid gland, which could reflect fusion of theSMAS and the parotid fascia to form a single layer.
Tellioglu et al12 reported that the temporoparietal fas-cia was composed of inner and outer parts. They statedthat the outer layer extended as the SMAS below the zy-gomatic arch. The inner layer blended with the superfi-cial layer of the deep temporal fascia on the zygomaticarch and continued to the masseteric fascia. Hata13 dis-agreed with their findings, arguing that the outer layer
of the fascia was “temporoparietalis” and that the innerpart of the fascia was the “loose areolar layer” or the “sub-galeal fascia.” Beheiry and Abdel-Hamid10 demon-strated that the temporoparietal fascia splits into the su-perficial layer and the deep layer and that the superficiallayer splits into 2 other layers in the lower half of the tem-poral muscle. We show herein that the temporoparietalfascia is composed of multiple fascial layers that are in-tegrated with thin fibrous septa.
The deep temporal fascia is a dense uniform aponeu-rotic layer covering the temporal muscle.1 There is agree-ment that the deep temporal fascia is a single layer at-tached along the length of the superotemporal line, whereit blends with the periosteum14,15 and splits into the su-perficial and deep lamina above the level of the zygo-matic arch.4,7,8,10,11,14,16-20 However, it is controversial wherethe deep temporal fascia splits and where and if its lay-ers abut the zygomatic arch or continue as the masse-teric fascia over the zygomatic arch. Yasargil et al21 dem-onstrated that the deep temporal fascia is divided into 2layers at the orbital level. According to them, the super-ficial layer and the deep layer of the fascia that are at-tached to the lateral and medial borders of the zygo-matic arch are separated by an intermediate fat layer.Stuzin et al4 subsequently showed that the deep tempo-ral fascia splits into 2 layers below the supero-orbital mar-gin. They documented that the superficial layer of thedeep temporal fascia is attached to the superior marginof the zygomatic arch, overlies the periosteum of the zy-gomatic arch, and blends with the parotideomassetericafascia. Salas et al9 argued that the deep layer of the deeptemporal fascia is attached to the posterosuperior mar-gin of the zygomatic arch, continues along the deep sur-face of the zygomatic arch, and blends with the “pos-teromasseteric fascia.” Ramirez et al19 found that the deeplayer and the superficial layer of the deep temporal fas-cia fuse at 1 cm above the zygomatic arch and are at-tached to the superficial surface of the zygomatic arch,blending with the attachment to the fascia of the masse-ter muscle. Ammirati et al20 reported that 2 layers of thisfascia are attached to the anterior portion of the zygo-matic arch and continue with the parotideomassetericafascia below the zygomatic arch. Campiglio and Candi-ani7 noted that the temporal muscle fascia split into 2sheets at 5 cm above the zygomatic arch, with the su-perficial sheet abutting the anterior surface of the zygo-matic arch and the deep sheet abutting the posterior sur-face of the zygomatic arch. These 2 fascial layers werefused in the anterior and posterior thirds of the zygo-matic arch but were separated by a fat pad in the middle.Similarly, Hwang and Kim22 demonstrated that the su-perficial layer and the deep layer of the deep temporalfascia fused and abutted the superior margin of the zy-gomatic arch in 18 dissections (56%) and abutted the su-perolateral surface in 14 dissections (44%). Coscarellaet al8 and Beheiry and Abdel-Hamid10 reported that thefascia of the temporal muscle split into 2 layers at 1 to 2cm above the zygomatic arch or over the lower half ofthe temporal muscle, and the superficial fascia attachedto the lateral side of the zygomatic arch. The deep fasciaabutted the medial side of the zygomatic arch. In con-trast, Accioli de Vasconcellos et al11 found that the deep
(REPRINTED) ARCH FACIAL PLAST SURG/ VOL 12 (NO. 1), JAN/FEB 2010 WWW.ARCHFACIAL.COM21
©2010 American Medical Association. All rights reserved.
Downloaded From: https://archfaci.jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/10/2019

temporal fascia was independent of the zygomatic arch(like the temporoparietal fascia) and continued cau-dally as the masseter muscle fascia. Our results are inagreement with the observations of all of these studiesthat the deep temporal fascia splits into the superficiallayer and the deep layer. However, our findings demon-strate that the point where the fascia splits differs at theanterior, middle, and posterior portions of the zygo-matic arch because of the fat pad between the layers ofthe fascia. We also show that the layers of the deep tem-poral fascia do not fuse above the zygomatic arch, butthe 2 layers could be seen as a single layer if a cross-section was obtained near the lateral orbital rim. In mostof our specimens, the superficial layer continues as theparotideomasseterica fascia, and the deep layer abuts theposterosuperior edge of the zygomatic arch. However, thesuperficial layer and the deep layer of the deep temporalfascia continued together across the zygomatic arch asthe parotideomasseterica fascia in 27% of specimens (9of 33 sides of 11 specimens).
Kim and Matic16 observed that a fibrous network di-vides the intermediate fat pad into lobules and that thereis a dual arterial supply to the intermediate fat pad fromperforators originating from the middle and deep tem-poral arteries, which pierce the superficial layer and thedeep layer of the deep temporal fascia. Our study con-firms that the intermediate fat pad is divided into sev-eral lobules by a fibrous network and that there are ves-sels inside the fat pad, especially at 5 to 24 mm from thezygomatic arch. We also show that perforators are morecommon between the intermediate fat pad and the su-perficial layer and the deep layer of the deep temporalfascia.
Researchers have called attention to the number of tem-poral branch twigs at the level of the zygomatic arch. Go-sain et al23 demonstrated that 2 to 4 rami of the temporalbranch of the facial nerve cross the zygomatic arch. Zaniet al24 noted that the temporal branch of the facial nerveis composed of 1 twig in 28% of cases, 2 twigs in 32% ofcases, 3 twigs in 16% of cases, and 4 twigs in 4% of casesat the level of the zygomatic arch. Ammirati et al20 showedthat the temporal branch of the facial nerve is divided intoanterior, middle, and posterior rami after piercing the pa-rotideomasseterica fascia. In our study, the temporal branchof the facial nerve traversed along the zygomatic arch as 1twig in 14.3%, as 2 twigs in 57.1%, as 3 twigs in 14.3%,and as 4 twigs in 14.3% of specimens.
Various approaches have been described for a safe sur-gical dissection around the temporal branch of the fa-cial nerve and the zygomatic arch. Researchers7,8,11,14,20
have observed that the temporal branch of the facial nervecourses within the superficial fat pad. Because of this find-ing, Coscarella et al8 proposed submuscular dissection(deep to the temporal muscle) or subfascial dissection(deep to the deep temporal fascia layer). In contrast, otherauthors4,9,12,18 have noted the temporal branch of the fa-cial nerve in the deepest temporoparietal fascia above thezygomatic arch. Beheiry and Abdel-Hamid10 reported thatthe temporal branch of the facial nerve coursed first be-tween the layers of the superficial lamina of the tempo-roparietal fascia and then coursed between the deep layerand the superficial layer of the temporoparietal fascia. Con-
sistent with these findings, Salas et al9 and Yasargil et al21
recommended interfascial dissection. Ammirati et al20
showed that terminal twigs of the temporal branch of thefacial nerve penetrated the temporoparietal fascia at dif-ferent levels. They cautioned against mistaking the su-perficial fat pad for the intermediate fat pad and endan-gering the temporal branch of the facial nerve by interfacialdissection and instead recommended deeper dissectionto preserve the facial nerve. In contrast, Stuzin et al4
claimed that a safe surgical plane is ensured by begin-ning dissection in the superficial fat pad of the temporalregion and by deepening the dissection at 2 cm above thezygomatic arch into the intermediate temporal fat padto expose the zygomatic arch. Ramirez et al19 reportedin 1991 that there was no structure between the perios-teum of the zygomatic arch and the temporoparietal fas-cia. Therefore, they suggested that subgaleal dissectionshould be deepened through the layers of the deep tem-poral fascia at about 3 cm above the zygomatic arch andthat subperiosteal dissection should be performed at thelevel of and along the entire length of the zygomatic arch.In 2002, Ramirez25 described some changes in his sur-gical technique, noting that the zygomatic arch could beentered at 2 to 3 mm above the superior border of thezygomatic arch. As part of their midface-lift technique,Quatela and Olney published the recommendation “toelevate deep to the intermediate fat pad directly on thedeep layer of the deep temporal fascia and then deep tothe periosteum.”17(p217) Krayenbühl et al14 suggested thatsubgaleal fascia dissection can be performed up to theadhesions between the temporoparietal fascia and the deeptemporal fascia and that interfacial or interlaminar dis-section (between the 2 lamina of the deep temporal fas-cia) or subfascial dissection could then be performed toprotect the facial nerve.
In light of our findings and the results of the studiesreviewed herein, 3 approaches may be used to reach thezygomatic arch through the intermediate fat pad. The dis-section plane is incised down to the periosteum (sub-periosteal) on the zygomatic arch in all 3 approaches(Figure 11). The first approach is a subgaleal dissection(superficial to the superficial layer of the deep temporalfascia), deepening into the intermediate fat pad just abovethe zygomatic arch. Our study demonstrates that the tem-poral branch of the facial nerve is covered by a thin layerof the temporoparietal fascia above the zygomatic archand that there is a superficial fat pad between the tem-poroparietal fascia and the superficial layer of the deeptemporal fascia. However, our study also shows that thisfat pad disappears and that adhesions are observed at thedissection plane beyond the upper edge of the zygo-matic arch. Our findings suggest that continuous dissec-tion on the subgaleal plane to the upper edge of the zy-gomatic arch is safe and easy. Beyond this level, subgalealdissection carries the risk of injury to the temporal branchof the facial nerve. Therefore, the surgeon will need tocontinue deep dissection to at least a few millimeters abovethe zygomatic arch. The second approach begins with sub-galeal dissection as in the first approach but deepens intothe intermediate fat pad at 1 to 2 cm above the zygo-matic arch. Our study shows that there are widespreadvessels in the intermediate fat pad located 5 to 24 mm
(REPRINTED) ARCH FACIAL PLAST SURG/ VOL 12 (NO. 1), JAN/FEB 2010 WWW.ARCHFACIAL.COM22
©2010 American Medical Association. All rights reserved.
Downloaded From: https://archfaci.jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/10/2019

from the zygomatic arch. Although dissection using thisapproach would be safer than the first approach, morebleeding may occur. The third approach is to dissect thedeep layer of the deep temporal fascia (deep to the in-termediate fat pad) beginning from the division point ofthe layers of the deep temporal fascia. Our study showsthat the intermediate fat pad can be easily dissected fromthe deep layer of the deep temporal fascia and that onlya few small vessels are encountered along the dissectionplane. Our results suggest that this approach is as safeas the second approach in terms of injury to the tempo-ral branch of the facial nerve but that less bleeding anddisruption of the fat pad occur compared with the sec-ond approach.
Accepted for Publication: July 14, 2009.Correspondence: Ozcan Cakmak, MD, Acibadem Uni-versity, Department of Otorhinolaryngology, AcibademKadikoy Hospital, Tekin Sokak, No. 8, Acibadem, Kadi-koy, Istanbul, Turkey 34718 ([email protected]).Author Contributions: All authors had full access to allthe data in the study and take responsibility for the in-tegrity of the data and the accuracy of the data analysis.Study concept and design: Babakurban, Cakmak, and Qua-tela. Acquisition of data: Babakurban, Cakmak, Kendir,and Elhan. Analysis and interpretation of data: Babakur-ban, Cakmak, Kendir, and Quatela. Drafting of the manu-script: Babakurban, Cakmak, Kendir, and Elhan. Criti-cal revision of the manuscript for important intellectualcontent: Cakmak, Kendir, and Quatela. Statistical analy-sis: Babakurban. Administrative, technical, and material sup-port: Cakmak, Elhan, and Quatela. Study supervision: Cak-mak, Elhan, and Quatela.Financial Disclosure: None reported.Previous Presentation: This study was presented andawarded the best poster in the field of facial plastic sur-gery at the First Meeting of the European Academy ofOtorhinolaryngology & Head and Neck Surgery in Col-laboration With the European Federation of Oto-Rhino-Laryngological Societies; June, 28, 2009; Mannheim, Ger-many.
REFERENCES
1. Arinci K, Elhan A. Anatomi. Vol 1. 2nd ed. Ankara, Turkey: Günes Kitabevi LtdSÈti; 2006.
2. Mitz V, Peyronie M. The superficial musculo-aponeurotic system (SMAS) in theparotid and cheek area. Plast Reconstr Surg. 1976;58(1):80-88.
3. Hing DN, Buncke H, Alpert BS. Use of the temporoparietal free fascial flap in theupper extremity. Plast Reconstr Surg. 1988;81(4):534-544.
4. Stuzin JM, Wagstrom L, Kawamoto HK, Wolfe SA. Anatomy of the frontal branchof the facial nerve: the significance of the temporal fat pad. Plast Reconstr Surg.1989;83(2):265-271.
5. Gosain AK, Yousif NJ, Madiedo G, Larson DL, Matloub HS, Sanger JR. Surgical
anatomy of the SMAS: a reinvestigation. Plast Reconstr Surg. 1993;92(7):1254-1265.
6. Gassner HG, Rafii A, Young A, Murakami C, Moe KS, Larrabee WF Jr. Surgicalanatomy of the face: implications for modern face-lift techniques. Arch FacialPlast Surg. 2008;10(1):9-19.
7. Campiglio GL, Candiani P. Anatomical study on the temporal fascial layers and theirrelationships with the facial nerve. Aesthetic Plast Surg. 1997;21(2):69-74.
8. Coscarella E, Vishteh AG, Spetzler RF, Seoane E, Zabramski JM. Subfascial andsubmuscular methods of temporal muscle dissection and their relationship tothe frontal branch of the facial nerve: technical note. J Neurosurg. 2000;92(5):877-880.
9. Salas E, Ziyal IM, Bejjani GK, Sekhar LN. Anatomy of the frontotemporal branchof the facial nerve and indications for interfascial dissection. Neurosurgery. 1998;43(3):563-569.
10. Beheiry EE, Abdel-Hamid FA. An anatomical study of the temporal fascia and re-lated temporal pads of fat. Plast Reconstr Surg. 2007;119(1):136-144.
11. Accioli de Vasconcellos JJ, Britto JA, Henin D, Vacher C. The fascial planes ofthe temple and face: an en-bloc anatomical study and a plea for consistency. BrJ Plast Surg. 2003;56(7):623-629.
12. Tellioglu AT, Tekdemir I, Erdemli EA, Tüccar E, Ulusoy G. Temporoparietal fas-cia: an anatomic and histologic reinvestigation with new potential clinicalapplications. Plast Reconstr Surg. 2000;105(1):40-45.
13. Hata Y. Is it true that the temporoparietal fascia has two layered structures? PlastReconstr Surg. 2001;107(5):1309-1310.
14. Krayenbühl N, Isolan GR, Hafez A, Yasargil MG. The relationship of the fronto-temporal branches of the facial nerve to the fascias of the temporal region: a lit-erature review applied to practical anatomical dissection. Neurosurg Rev. 2007;30(1):8-15.
15. Standring S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 39th ed.Edinburgh, Scotland: Elsevier Churchill Livingstone; 2008.
16. Kim S, Matic DB. The anatomy of temporal hollowing: the superficial temporalfat pad. J Craniofac Surg. 2005;16(5):760-763.
17. Quatela VC, Olney DR. Management of the midface. Facial Plast Surg Clin NorthAm. 2006;14(3):213-220.
18. Sabini P, Wayne I, Quatela VC. Anatomical guides to precisely localize the fron-tal branch of the facial nerve. Arch Facial Plast Surg. 2003;5(2):150-152.
19. Ramirez OM, Maillard GF, Musolas A. The extended subperiosteal face lift: a de-finitive soft-tissue remodeling for facial rejuvenation. Plast Reconstr Surg. 1991;88(2):227-238.
20. Ammirati M, Spallone A, Ma J, Cheatham M, Becker D. An anatomicosurgicalstudy of the temporal branch of the facial nerve. Neurosurgery. 1993;33(6):1038-1044.
21. Yasargil MG, Reichman MV, Kubik S. Preservation of the frontotemporal branchof the facial nerve using the interfascial temporalis flap for pterional craniotomy:technical article. J Neurosurg. 1987;67(3):463-466.
22. Hwang K, Kim DJ. Attachment of the deep temporal fascia to the zygomatic arch:an anatomic study. J Craniofac Surg. 1999;10(4):342-345.
23. Gosain AK, Sewall SR, Yousif NJ. The temporal branch of the facial nerve: howreliably can we predict its path? Plast Reconstr Surg. 1997;99(5):1224-1236.
24. Zani R, Fadul R Jr, Da Rocha MA, Santos RA, Alves MC, Ferreira LM. Facial nervein rhytidoplasty: anatomic study of its trajectory in the overlying skin and themost common sites of injury. Ann Plast Surg. 2003;51(3):236-242.
25. Ramirez OM. Three-dimensional endoscopic midface enhancement: a personal questfor the ideal cheek rejuvenation. Plast Reconstr Surg. 2002;109(1):329-349.
26. Abul-Hassan HS, von Drasek Ascher G, Acland RD. Surgical anatomy and bloodsupply of the fascial layers of the temporal region. Plast Reconstr Surg. 1986;77(1):17-28.
27. Casanova R, Cavalcante D, Grotting JC, Vasconez LO, Psillakis JM. Anatomic ba-sis for vascularised outer-table calvarial bone flaps. Plast Reconstr Surg. 1986;78(3):300-308.
28. Tolhurst DE, Carstens M, Greco R, Hurwitz D. The surgical anatomy of the scalp.Plast Reconstr Surg. 1991;87(4):603-614.
29. Wen HT, de Oliveira E, Tedeschi H, Andrade FC Jr, Rhoton AL. The pterional ap-proach: surgical anatomy, operative technique, and rationale. Oper Tech Neurosurg.2001;4(2):60-72. doi:10.1053/otns.2001.25567.
(REPRINTED) ARCH FACIAL PLAST SURG/ VOL 12 (NO. 1), JAN/FEB 2010 WWW.ARCHFACIAL.COM23
©2010 American Medical Association. All rights reserved.
Downloaded From: https://archfaci.jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/10/2019