objectives leukaemias – all, cll, aml, cml. lymphomas – hodgkin’s vs non-hodgkin’s myeloma
TRANSCRIPT
Haematological MalignancyKim Gibson, F1January 2015
Objectives
• Leukaemias – ALL, CLL, AML, CML.
• Lymphomas– Hodgkin’s vs Non-Hodgkin’s
• Myeloma
Blood Components
Blood Cell Components
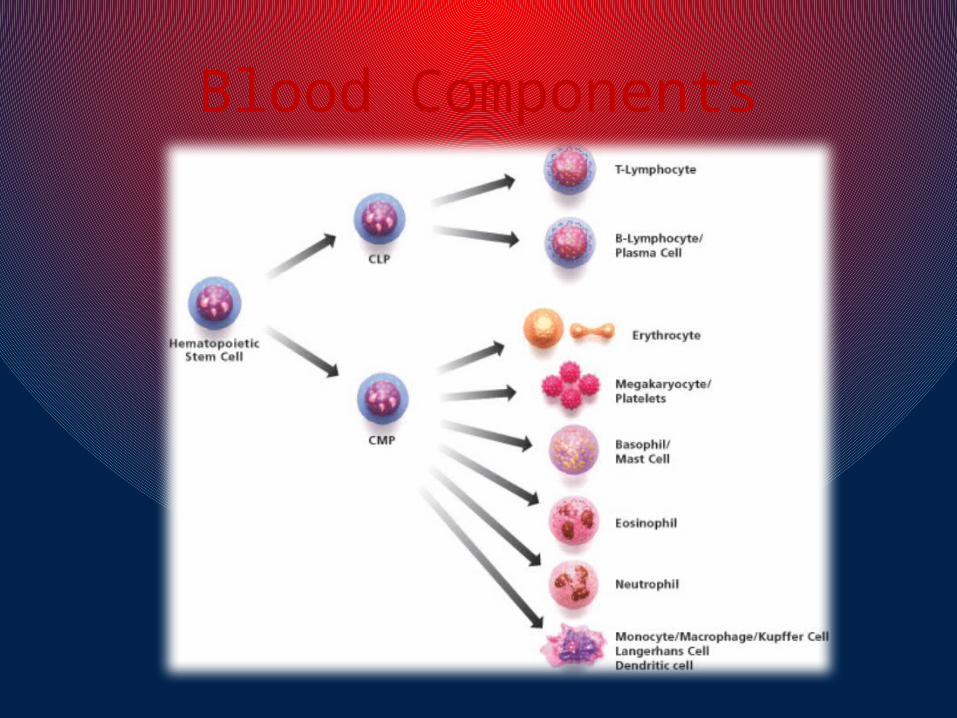
• Lymphocytes form in marrow – T cells mature in the thymus. B and T cells are deposited in lymph organs (e.g. spleen) and circulate in lymphatic system.
• Myeloid cells include all other haematological cell types, which form in bone marrow before release into vascular space.
Leukaemia
• Leukaemic cells (cancerous WBC) infiltrate bone marrow, affecting normal function, i.e. There is inadequate haematopoeisis.
• Aetiology mostly unknown, but viruses/chemicals/drugs/radiation all implicated
Leukaemia
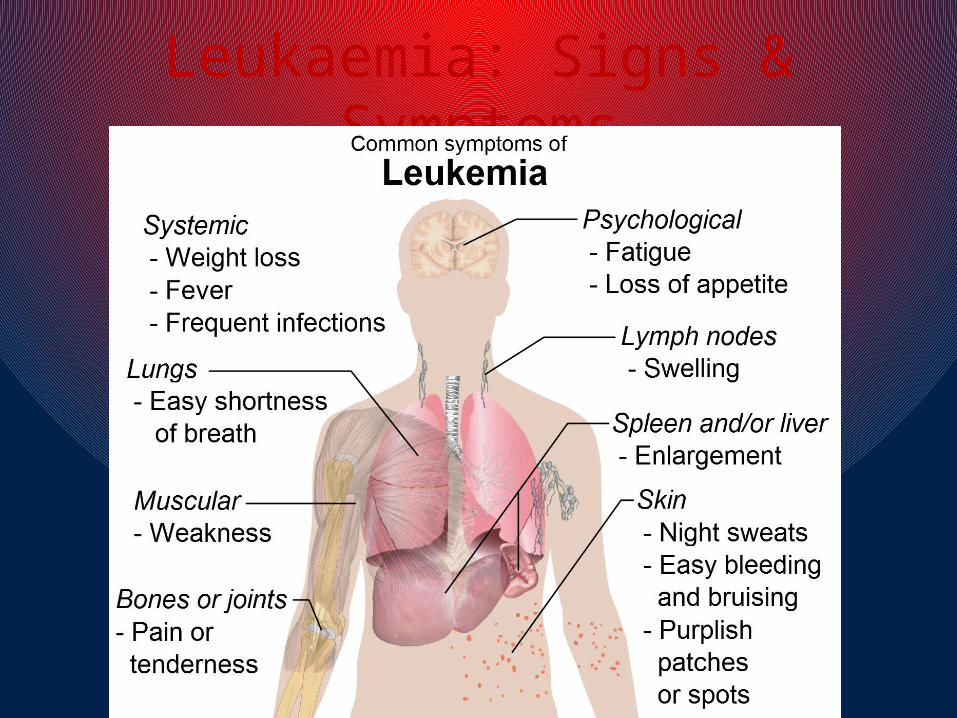
Leukaemia: Signs & Symptoms• Mostly seen in acute leukaemia, late
chronic.
• Due to bone marrow failure – red marrow in central skeleton and proximal long bones
Leukaemia: Investigations
• FBC – Hb low, WBC usually high
• Blood film – shows precursor lymphoblast cells
• Bone Marrow aspirate – increased cellularity, reduced erythropoeisis, reduced megakaryocytes - replaced by blasts
• CXR – why?
• LP for CSF examination in ALL
Leukaemia: Treatment
• Without treatment, acute leukaemia is invariably fatal within months.
• ALL in the young has best chance of cure, AML good chance of cure but secondary AML poorest prognosis.
• Curative treatment carries both morbidity and mortality – Risk vs Benefit
Leukaemia: Treatment
• All need supportive treatment:– Transfusions of red cells and platelets and necessary,
prevention of infection, treatment of infection with antibiotic/antifungal agents as soon as fever develops
• Curative Intent:– Try to return marrow to normal – complete remission
(CR). ‘Induction chemo’ not specific to cancerous cells – major infection risk. Followed by specific ‘consolidation’ regimen – ESSENTIAL or remission will certainly occur.
Acute Myeloid Leukaemia
• Treatment with curative intent if <60
• Risk and prognosis based on bone marrow result
• Bone marrow transplant in some higher risk patients, or if fail 2 cycles chemo
• 75% achieve CR, 50% of those are ‘cured’ (1/3 overall)
Acute Lymphocytic Leukaemia
• ALL commonest childhood malignancy, but can be any age
• CR and consolitation achieved with different agents than in AML
• Early transplant if high risk (older pts, high WCC, >3-4 weeks to achieve CR)
• Major difference is need to treat CNS as soon as CR achieved – intrathecal chemo
• Very high risk may need cranial radiotherapy
• Maintenance Tx for at least 2 years

Acute Leukaemias
• ALL in childhood good prognosis – 80% alive at 5 years
• Overall cure rate for ALL 30%
• In both AML and ALL recurrence usually within 3 years – poor prognosis. Transplant usually considered, despite the risks.

Chronic Myeloid Leukaemia• Peak age 40-60 years.
• Slow, progressive disease. If untreated acute phase (blast crisis) leads to death rapidly.
• Often no symptoms in chronic phase. Symptoms often suggest blast crisis is occurring.
• Philadelphia chromosome associated with 95% cases
• Fluoroscein-in-situ-Hybridisation and reverse-transcriptase PCR helps diagnosis and monitoring response to Tx
CML: Treatment
• Supportive treatment as necessary
• Imatinib is therapy of choice in chronic phase – complete response in 95%, well tolerated, can continue indefinitely
• Acute phase treated in similar way to acute leukaemias to try and return to second chronic phase.
• Stem cell transplant cures 75% where imatinib fails
Chronic Lymphocytic Leukaemia
• Commonest leukaemia, presents mostly >65 years
• Mostly asymptomatic incidental finding
• Median survival approx 10 years
• Diagnosis depends on lymphocyte count >5x 109/L
• Clinical course is variable, difficult to determine prognosis
CLL: Management• Major decision is when to treat – 1/3 never need intervention
• Rai and Binet systems use presence of symptoms and results of investigations to stage – helps determine when to treat
• Treatment (intermittent chemo) can help the symptoms and signs, effect on life expectancy uncertain.
• Supportive treatments as above are important
• Stem cell transplant benefits under Ix in younger patients
• CLL can undergo lymphomatous (Richter’s) transformation (7%) – survival is short.
Lymphomas
• Commoner than leukaemias
• Abnormal proliferation of lymphoid tissue – can occur anywhere lymph tissue found (LNs, spleen, thymus, GI tract...)
• Classifed as Hodgkin’s or Non-Hodgkin’s depending on histology
Hodgkin’s Lymphoma
• Rare, M:F = 1.3:1, 90% in over 16s. Peak incidence in 20s
• Mostly involves LNs
• Definition of HL is presence of Reed-Sternberg cells in lymph tissue on biopsy.

Hodgkin’s Lymphoma: Classification
• Classical HL:– Nodular sclerosing (70%): fibrotic bands and
nodules, usually affects young adults– Lymphocyte-rich HL (5%): infiltration of many
small lymphocytes and R-S cells, peripheral nodes, older age.
– Mixed Cellularity HL (25%): M>F, associated with B symptoms
– Lymphocyte-depleted HL: rare. Numerous R-S cells, advanced B symptoms, associated with HIV.
HL: Signs & Symptoms
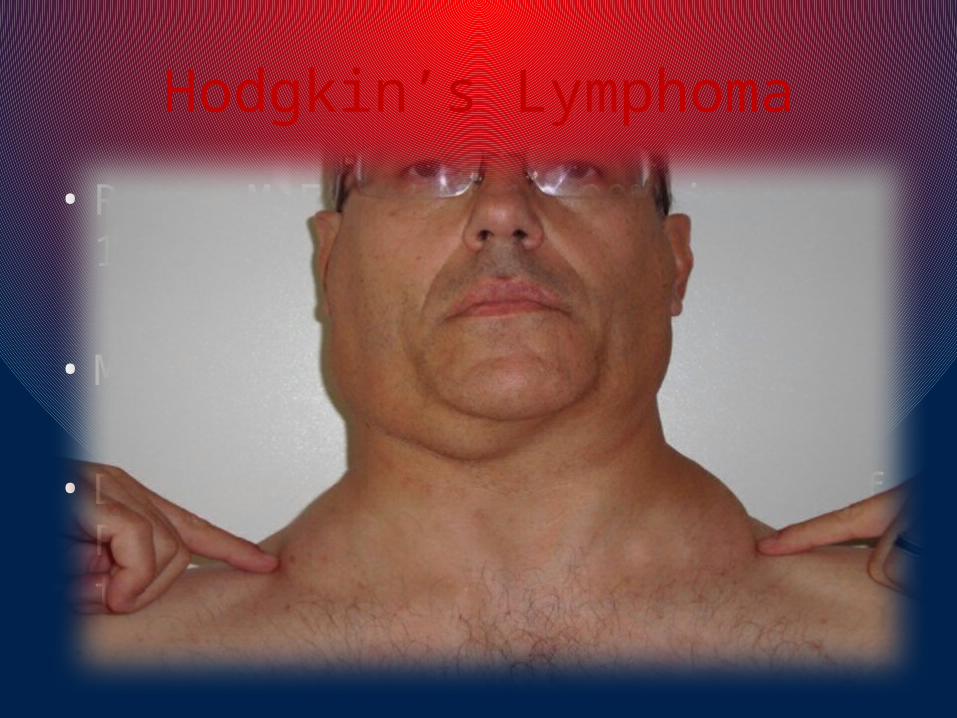
• Lymph node enlargement (usually cervical) – painless and rubbery.
• Enlarged spleen/liver
• Others include pruritis, fatigue, anorexia, alcohol-induced pain at affected LNs.

HL: Investigations & Treatment• LN biopsy.
• FBC – Hb can be normal or low. High lymphocytes. ESR raised, abnormal LFTs.
• CXR and CT, ? PET scan
• Staging by Ann Arbor classification based on number/spread affected nodes and presence of B symptoms which carry a worse prognosis. Fever, drenching night sweats, >10% weight loss in 6/12
• Treatment – curative intent. Chemo and site-specific radiation. Recurrence uncommon, but 2nd/3rd remissions achievable
Non-Hodgkin’s Lymphoma• 70% B cell, 30% T cell
• Viruses including HBV, herpesvirus 8, HIV all implicated
• Malignant proliferation of lymphocytes
• Signs and Symptoms: painless superficial LN enlargement, systemic B symptoms. Extra-nodal involvement inc GIT, lung, brain, testes, thyroid, skin...
• Ix – FBC to look for bone marrow infiltration, ESR raised, U&Es (big nodes obstruct ureters), LFTs, CXR, CT, Bone Marrow Bx, trephine Bx, LN Bx
NHL: Types• Follicular Lymphoma: painless lymphadenopathy.
Remitting/relapsing over ~10 years. Treatment: chemo-immunotherapy, radiotherapy and occasioanlly stem cell transplant. High risk transformation to diffuse large B cell lymphoma
• Lymphoplasmacytic lymphoma: uncommon. Extensive marrow infiltration. Management can be expectant, supportive or chemotx. Survival ~4 years
• Diffuse large B cell lymphoma: commonest. Without Tx fatal in months. >50% younger pts cured. Rapid infiltration of other organs, treated with chemoimmunotherapy.
• Burkitt’s lymphoma – endemic to Africa. Rapid progression. 30% have meningitis at presentation. 60% cure with chemo.

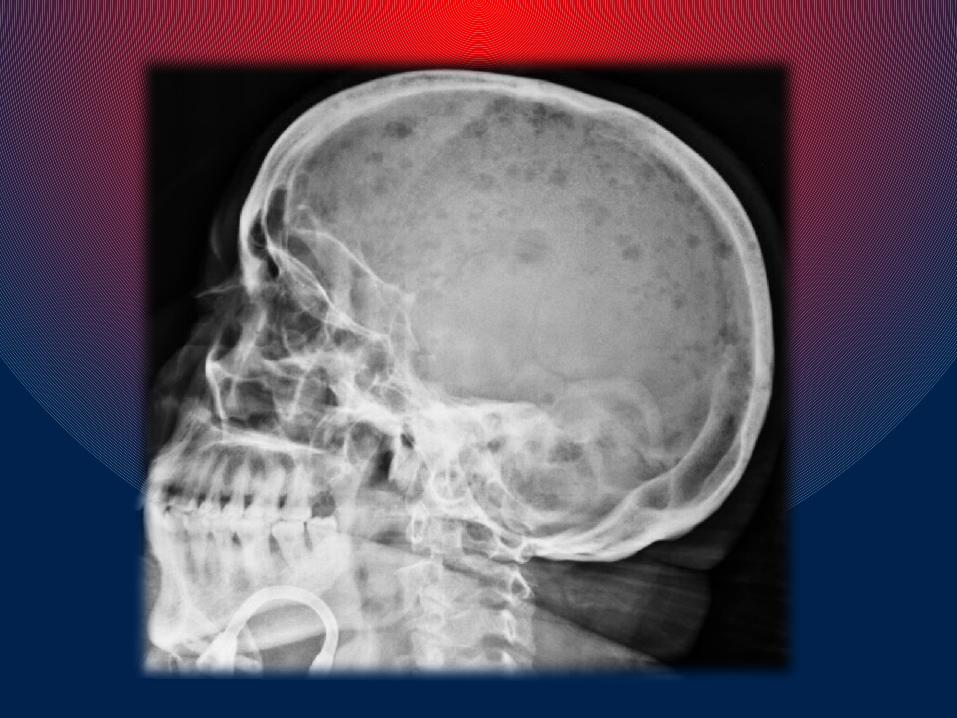
Multiple Myeloma
• Malignancy of plasma (B!) cells within bone marrow
• Clonal expansion of abnormal proliferative plasma cells paraproteinaemia and excretion of light chains in urine (Bence Jones protein)
• Disease of elderly, commoner in men
Multiple Myeloma Features
• Bone destruction (vertebral or long bones, can cord compression). Pain and/or pathological fractures
• Hypercalcaemia
• Bone marrow infiltration (anaemia, neutropenia, thrombocytopenia)
• Renal impairment from light chain deposition in tubules
• Recurrent infections (healthy immunoglobulins reduced)
C alcium
R enal failure
A naemia
B one problemsIf you see back pain and renal failure, think MYELOMA
Multiple Myeloma: Investigations• FBC – suggestive of marrow infiltration
• ESR and CRP possibly raised
• U&Es (renal failure) and uric acid
• Blood film
• Serum calcium
• Serum free light chain assay
• Urinary Bence-Jones protein
• Bone Marrow aspirate
• Skeletal Survey
AKA: MYELOMA SCREEN
Multiple Myeloma: Treatment
• Survival is 5-10 years if treatment of complications is successful. Chemo and steroids
• There is no ‘cure’ for multiple myeloma
• Supportive therapy as before
• Orthopaedic involvement in pathological fractures

Conclusion
• Haematological malignancies are COMPLICATED
• Lots of overlap
• Symptoms are non-specific and often insidious
• Easier to learn if you break it down into different classifications

ANY QUESTIONS?
THANK YOU!