advances in the management of non-hodgkin’s lymphomas€¦ · pd dr anastasios stathis, md...
TRANSCRIPT

PD Dr Anastasios Stathis, MDHead-New Drugs Development Unit
Chair-Clinical ResearchOncology Institute of Southern Switzerland
Bellinzona, Switzerland
Advances in the management of non-Hodgkin’s Lymphomas
6th ESO-ESMO Eastern Europe and Balkan RegionMasterclass in Medical Oncology
12/04/2019 - 17/04/2019, Sibenik, Croatia
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Outline
• The different lymphoma subtypes• Diagnosis and staging• Principles of lymphoma therapy• Management of DLBCL: how to tailor
treatment based on clinical and biologicalfactors
ESO-ESMO E
EBR Mas
tercla
ss 20
19

90 entities !!!
The 2016 revision of the 2008 WHO classification
(Swerdlow et al, Blood 2016)
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Incidence and mortality lymphomas
Siegel et al, CA Cancer J Clin. 2019ESO-E
SMO EEBR M
aster
class
2019

Lymphoma Database (Bellinzona and Novara), 2803 patients and 10 yrs follow-up
The most frequent subtypes
ESO-ESMO E
EBR Mas
tercla
ss 20
19
• „Rapidly growing but curable“ (diffuse large B-cell)
• „Rapidly growing and uncurable“ (mantle cell)
• „Cumulative and uncurable“ (follicular)
• „Inflammatory and curable“ (Hodgkin)
To simplify…. a lymphoma can be
ESO-ESMO E
EBR Mas
tercla
ss 20
19
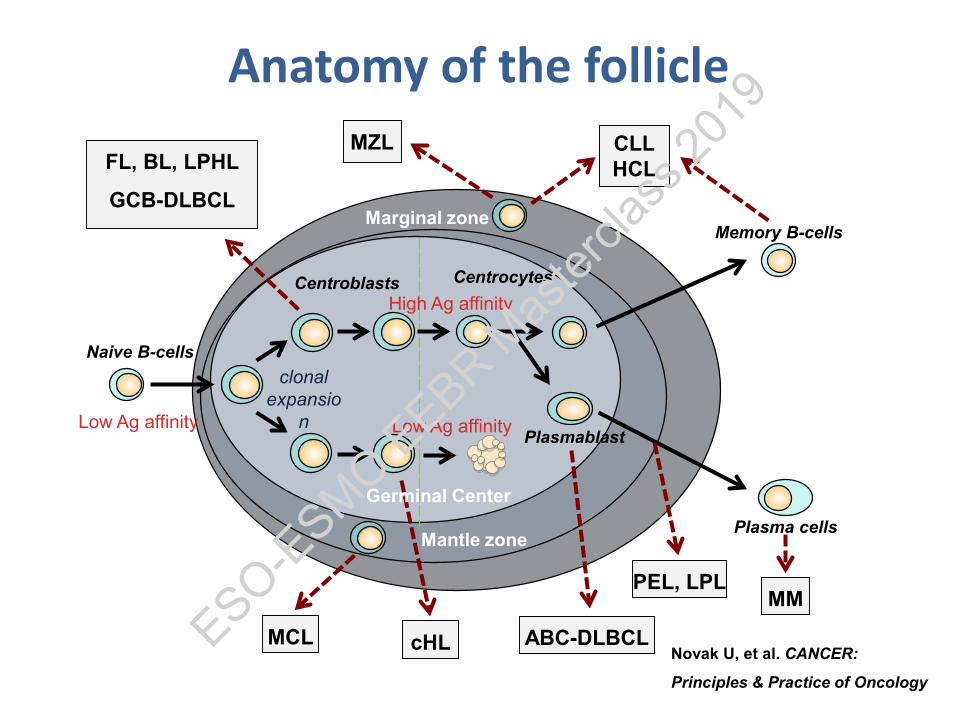
Centroblasts Centrocytes
Memory B-cells
Plasma cells
Naive B-cells
ABC-DLBCL
FL, BL, LPHL
GCB-DLBCL
MZL
MCL
MMPEL, LPL
Marginal zone
Plasmablast
CLLHCL
cHL
Low Ag affinity
High Ag affinity
Germinal Center
Mantle zone
Low Ag affinity
clonal expansio
n
Novak U, et al. CANCER:
Principles & Practice of Oncology
Anatomy of the follicle
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Cb/Cc
Follicular
Diffuse
Images courtesy of Stefano A Pileri, MD
Basic microscopy
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Histologic subtype
CD5 CD23 CD10 BCL6BCL2 Cyclin D1 CD20
CD19
Mantle cell Lymphoma + – – – + +
Follicular Lymphoma – –/+ +/– + – +
Small Lymphocytic Lymphoma/CLL + + – – – +
LymphoplasmacyticLymphoma – – – – – +
Splenic Marginal Zone Lymphoma – – – – – +
Extranodal Marginal Zone Lymphoma (MALT type) – –/+ – – – +
Surface markers of B-cell lymphomas
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Hystological type Translocation Genes involved
MCL t(11;14) BCL1 IgH
FL>DLBCL t(14;18) BCL2 IgH
CLL/SLL t(14;19) BCL3 IgH
DLBCL>FL t(3;14) BCL6 IgH
ALCL t(2,5) NPM ALK
LPL t(9;14) PAX5 IgH
Genetic abnormalities
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Diagnostic work-up
•Medical history •B-symptoms (fever, weight loss, night sweats)•PS and comorbidities •complete physical exam (superficial lymphnodes, Waldeyer ring, liver spleen)•CBC, chemistry, electrophoresis, ESR, LDH, b2-microglobulin, HBV, HCV, HIV
•PET-CT•Bone marrow aspirate and biopsy•Lumbar puncture in high risk aggressive•Cardiac ultrasound when planned to use anthracyclines
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Ann Arbor staging
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Dia
gnos
is Therapy
SurveillanceRelapse
PET PET PET PET
staging early restaging late restaging( interim ) (end therapy)
PET-CT in lymphoma
ESO-ESMO E
EBR Mas
tercla
ss 20
19
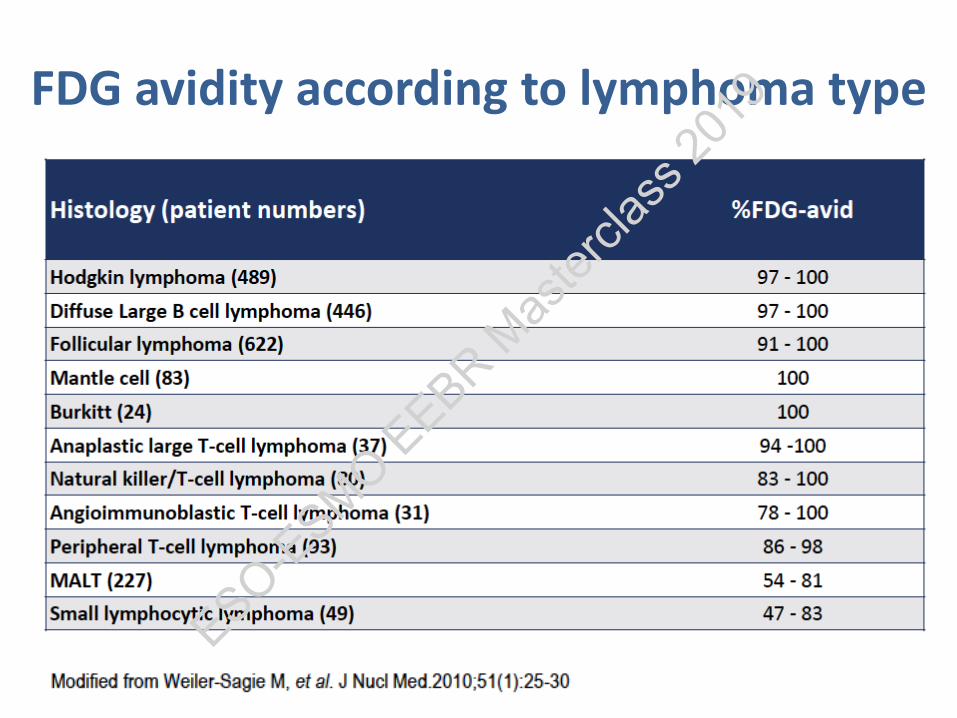
FDG avidity according to lymphoma type
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Bone marrow evaluation
•DLBCL–Biopsy if PET is negative and identifying a discordant histology is important for patient management
•Other subtypes–2 cm unilateral bone marrow biopsy is recommended, along with immunohistochemistry and flow cytometry at screening/baseline
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Response assessment(5-point scale: Deauville criteria)
ESO-ESMO E
EBR Mas
tercla
ss 20
19

FDG-PET evaluation
ESO-ESMO E
EBR Mas
tercla
ss 20
19
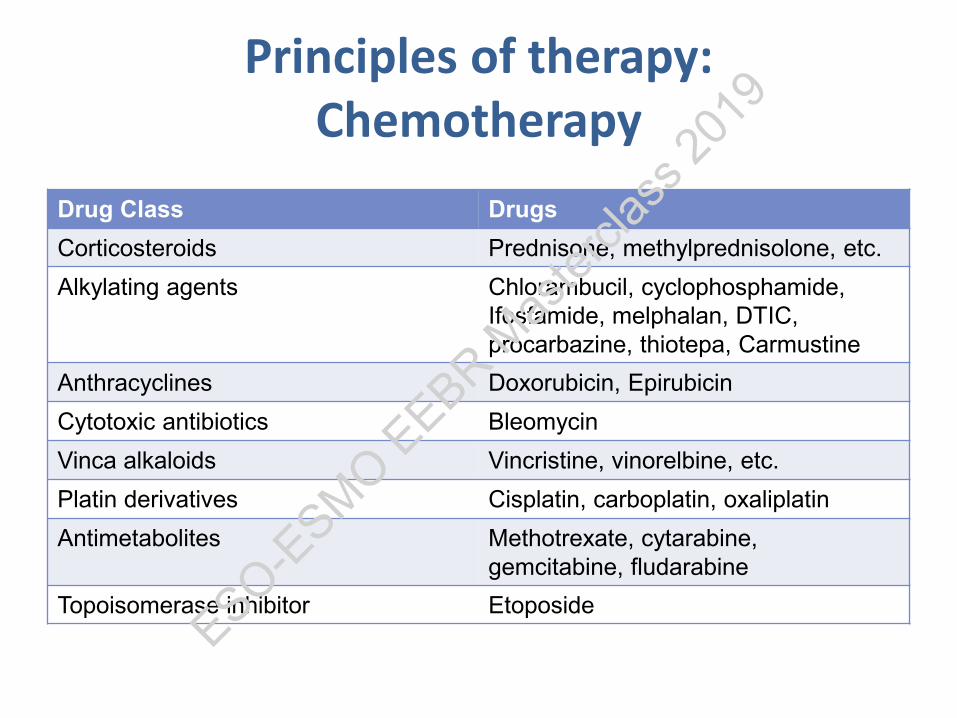
Principles of therapy:Chemotherapy
Drug Class DrugsCorticosteroids Prednisone, methylprednisolone, etc.Alkylating agents Chlorambucil, cyclophosphamide,
Ifosfamide, melphalan, DTIC, procarbazine, thiotepa, Carmustine
Anthracyclines Doxorubicin, EpirubicinCytotoxic antibiotics BleomycinVinca alkaloids Vincristine, vinorelbine, etc.Platin derivatives Cisplatin, carboplatin, oxaliplatinAntimetabolites Methotrexate, cytarabine,
gemcitabine, fludarabineTopoisomerase inhibitor Etoposide
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Principles of therapy:Anti-CD20 moAb Rituximab
Coiffier B, et al. NEJM 2002
OS (N = 399)
Surv
ival
Pro
babi
lity
Yrs
0
0.2
0.4
0.6
0.8
1
0 1 3 5 7 82 4 6
CHOPR-CHOP
P = .0004
Fisher RI, et al. J Clin Oncol. 2005.
DLBCL FL
ESO-ESMO E
EBR Mas
tercla
ss 20
19
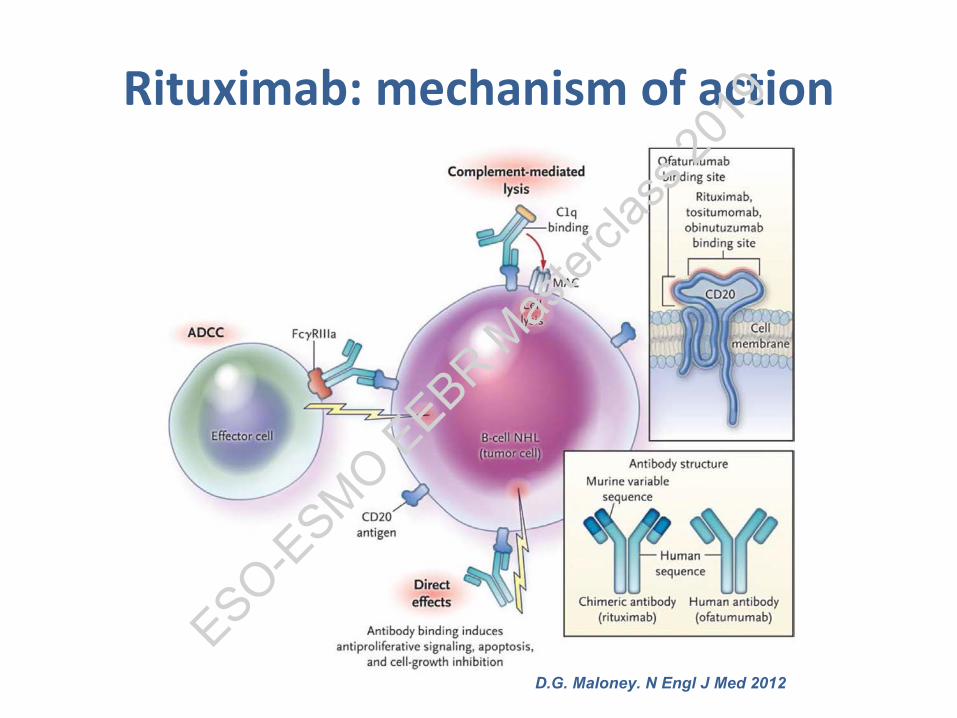
Rituximab: mechanism of action
D.G. Maloney. N Engl J Med 2012
ESO-ESMO E
EBR Mas
tercla
ss 20
19
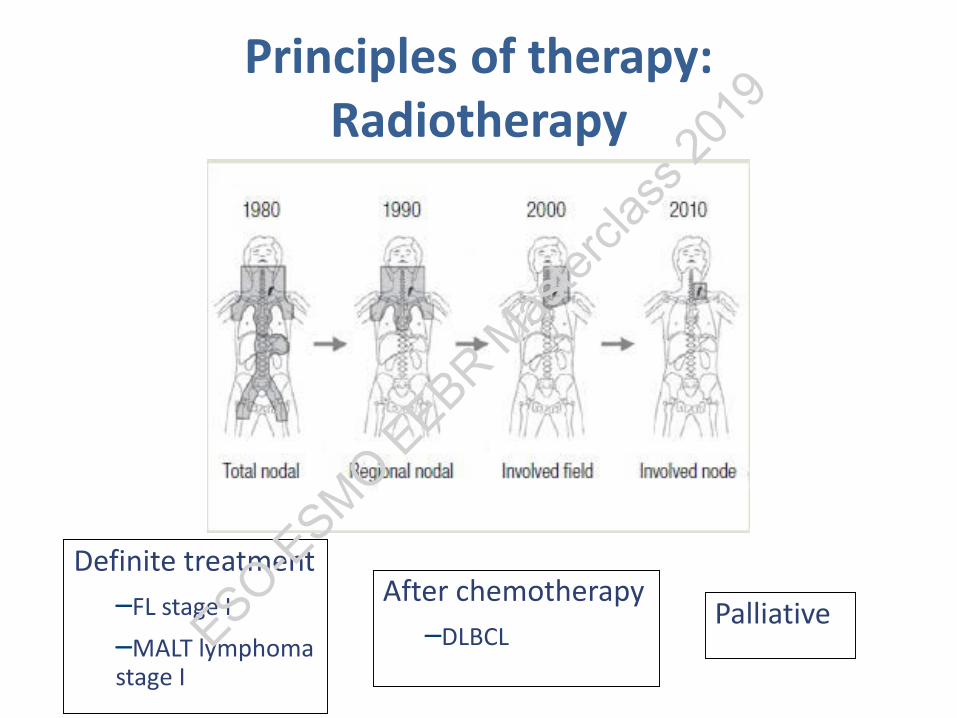
Definite treatment–FL stage I–MALT lymphoma stage I
After chemotherapy –DLBCL
Palliative
Principles of therapy:Radiotherapy
ESO-ESMO E
EBR Mas
tercla
ss 20
19
High dose chemotherapy(autologous transplant)
•Mantle cell lymphoma (1st line)•DLBCL (relapse)
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Chakraverty & MacKinnon, JCO 2011 Khouri et al Blood 2012
Curative potential through graft-versus lymphoma effect• Remission desirable• Reduced-intensity conditioning• Donor lymphocyte infusions
Accepted indications:• MCL >1st relapse/progression• FL >2nd relapse/progression• CLL/SLL >1st relapse/progression after FC-R; • >2nd relapse/progression• DLBCL, PTCL investigational
Allogeneic hematopoietic stem celltransplantation in lymphoma
ESO-ESMO E
EBR Mas
tercla
ss 20
19

CAR-T cells therapy(chimeric antigen receptor)
Kochenderfer and Rosenberg, Nat Rev Clin Oncol, 2013ESO-E
SMO EEBR M
aster
class
2019

CAR Design
S.S. Neelapu. et al, NEJM 2017
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma: ZUMA-1
S.S. Neelapu. et al, NEJM 2017
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Watch and wait strategy in FL (and criteria for treatment start)
Overall survival
Ardeshna K M et al., The Lancet, August 2003
W+W vs. ProMACE-MOPP89 ptsYoung, 1988
W+W vs. Prednimustine130 ptsBrice, 1997
W+W vs. Chlorambucil309 ptsArdeshna, 2003
ESO-ESMO E
EBR Mas
tercla
ss 20
19

1st line management of DLBCL
ESO-ESMO E
EBR Mas
tercla
ss 20
19
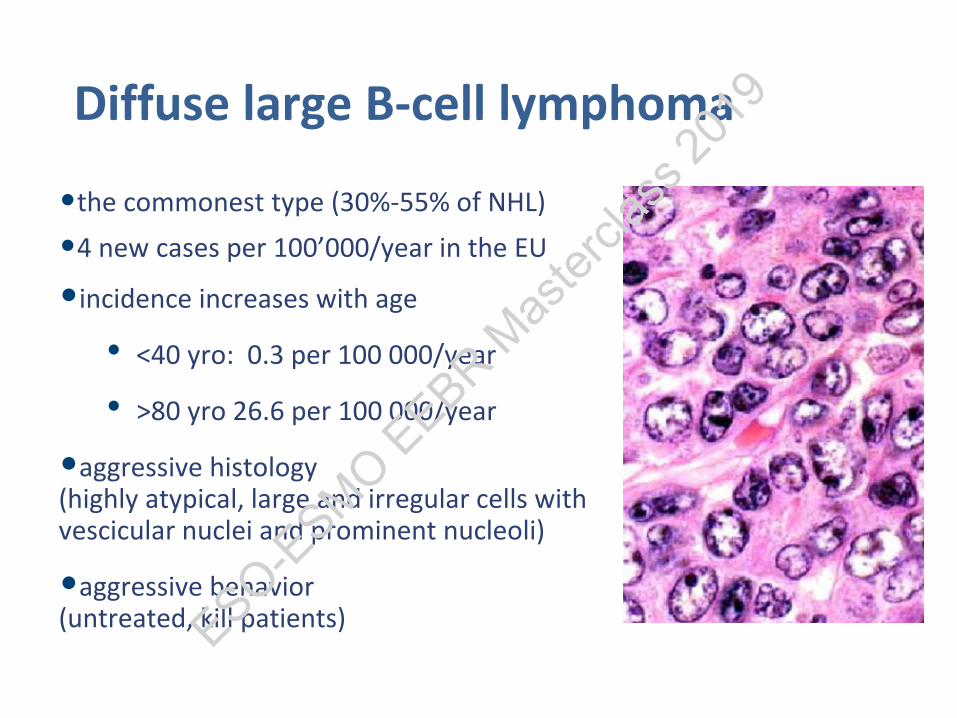
Diffuse large B-cell lymphoma
•the commonest type (30%-55% of NHL)•4 new cases per 100’000/year in the EU
•incidence increases with age
• <40 yro: 0.3 per 100 000/year
• >80 yro 26.6 per 100 000/year
•aggressive histology(highly atypical, large and irregular cells with vescicular nuclei and prominent nucleoli)
•aggressive behavior(untreated, kill patients)ESO-E
SMO EEBR M
aster
class
2019

Diffuse large B-cell lymphomaR-CHOP-21 Standard treatment today
Coiffier et al Blood 2010
Pfreundschuhet al. Lancet Oncol 2011
ESO-ESMO E
EBR Mas
tercla
ss 20
19
How can we tailor treatment in DLBCL?
CLINICAL FACTORS
Age, comorbidityStage (eg short course
chemo + RT)Extranodal sites (eg CNS
prophylaxis for some sites; different treatment for PCNSL)
ESO-ESMO E
EBR Mas
tercla
ss 20
19

A Predictive Model for Aggressive Non-Hodgkin's LymphomaThe International Non-Hodgkin's Lymphoma Prognostic Factors Project
International Prognostic Index (IPI)
Adverse risk factors:• age ≥60 yr• PS ≥ 2• LDH > normal• Ann Arbor stage III-IV• extranodal sites ≥ 2
1993;329:987-994ESO-E
SMO EEBR M
aster
class
2019

1993;329:987-994
Age-adjusted IPI (aaIPI)
aa IPI
1.Stage > II2. ECOG > 13. LDH > UNV
patients ≤ 60 years
Low 0Low-intermediate 1High-intermediate 2High 3ESO-E
SMO EEBR M
aster
class
2019

Risk of CNS relapseage > 60 y, LDH > N, stage 3 or 4, extranodal sites > 1,
kidney/adrenal gland involvement
Savage KJ et al. (Abs) Blood. 2014ESO-E
SMO EEBR M
aster
class
2019

Treatment based on clinical features
Characteristic TreatmentaaIPI=0 non bulky disease 4x RCHOP +2RaaIPI≥1 and/or bulky disease 6x RCHOP (+RT?)aaIPI=3 6xRCHOP (+auto SCT?)Older and fit patients 6x RCHOP with pre-phaseOlder not-fit 6x R-miniCHOP, or R-CEOP, or
R-Bendamustine
Testis involvement, multiple extranodal sites, close to SNC, ≥4 risk factors of the IPI score
SNC prophylaxis with HD-MTX
ESO-ESMO E
EBR Mas
tercla
ss 20
19
Can we improve over R-CHOP21?
• Shorter treatment intervals • Maintenance rituximab • Intensive 1st line regimen • Front-line autotransplant• Infusional regimens • Replace rituximab with other MoAb
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Can we improve over R-CHOP21?
• Shorter treatment intervals NO• Maintenance rituximab NO• Intensive 1st line regimen YES but..• Front-line autotransplant In selected pts• Infusional regimens NO• Replace rituximab with other MoAb NO
ESO-ESMO E
EBR Mas
tercla
ss 20
19

How can we tailor treatment in DLBCL?
CLINICAL FACTORS
Age, comorbidityStage (eg short course
chemo + RT)Extranodal sites (eg CNS
prophylaxis for some sites; different treatment for PCNSL)
ESO-ESMO E
EBR Mas
tercla
ss 20
19

How can we tailor treatment in DLBCL?
CLINICAL FACTORS
Age, comorbidityStage (eg short course
chemo + RT)Extranodal sites (eg CNS
prophylaxis for some sites; different treatment for PCNSL)
BIOLOGICAL FACTORS??
COO (ABC vs GCB)Myc , BCL2, BCL6
translocationsMYC/BCL2 IHC double
expression (DE)
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Myc, Bcl-2 and Bcl-6
Rosenthal and Younes, Blood Reviews 2016
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Myc, Bcl-2 and Bcl-6
• MYC is a transcription factor which regulates the expression of several target genes involved in the cell cycle, DNA damage repair, metabolism, protein synthesis, and response to stress– MYC translocation can be detected in approximately 10% of DLBCL
(range 4% to 14%)
• BCL2 normally serves an anti-apoptotic function– BCL2 translocations are found in 20–30% of de novo DLBCL and the
vast majority of cases are observed in the GCB subtype
• BCL6 is expressed in normal mature germinal center B-cells and acts as a transcription repressor
ESO-ESMO E
EBR Mas
tercla
ss 20
19
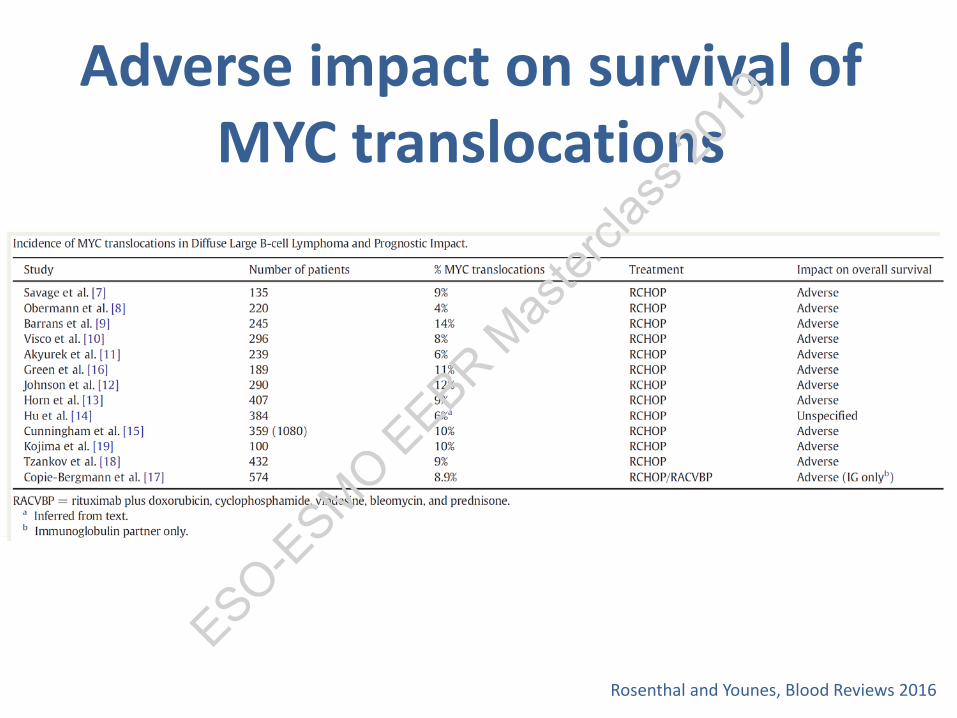
Adverse impact on survival of MYC translocations
Rosenthal and Younes, Blood Reviews 2016
ESO-ESMO E
EBR Mas
tercla
ss 20
19
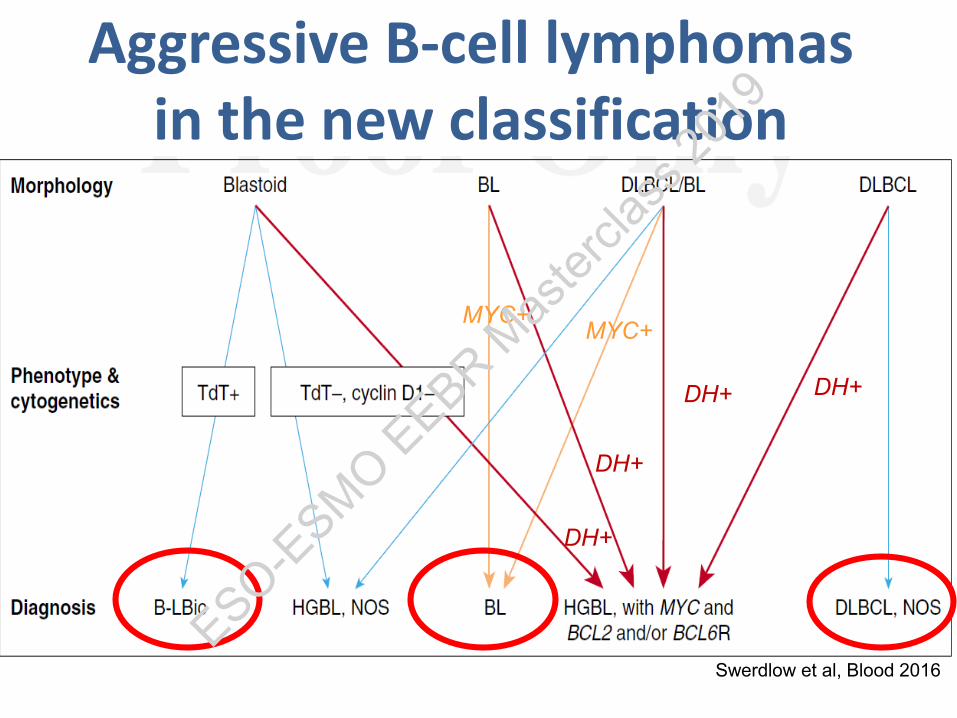
Swerdlow et al, Blood 2016
MYC+MYC+
DH+
DH+
DH+ DH+
Aggressive B-cell lymphomas in the new classification
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Landsburg DJ. Et al, J Clin Oncol, 2017
MYC +/- BCL2 +/- BCL6 rearrangements(role of intensive 1st line R-chemo)
RFS OS
ESO-ESMO E
EBR Mas
tercla
ss 20
19
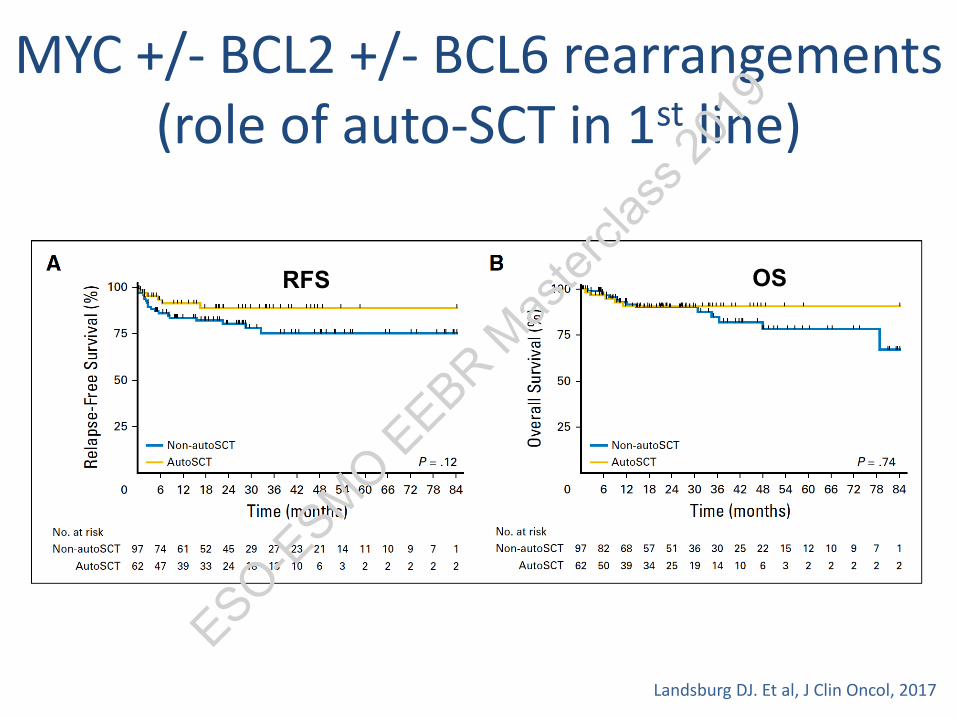
MYC +/- BCL2 +/- BCL6 rearrangements(role of auto-SCT in 1st line)
Landsburg DJ. Et al, J Clin Oncol, 2017
RFS OS
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Double-expressor lymphoma
19-34% of cases
IHC expression(40% MYC)(50% BCL2)
Rosenthal and Younes, Blood Reviews 2016
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Coexpression of MYC and BCL2 considered new prognostic marker (double-expressor lymphoma)
Hu et al, Blood 2013ESO-E
SMO EEBR M
aster
class
2019

DLBCL heterogeneityGene expression profiling results
Alizadeh AA et al., Nature 2000;403:503-11
GC B like
Activated B like
Different cell of origin
ESO-ESMO E
EBR Mas
tercla
ss 20
19

DLBCL heterogeneityGene expression profiling results
Rosenwald et al, NEJM, 2002ESO-E
SMO EEBR M
aster
class
2019

Immunohistochemistry as a surrogate
Hans CP et al., Blood 2004;103:275-82
Discordances with cDNA: 20%
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Biological differences between GCB and ABC
GCB ABCBCR/NFkB signalling
Histone modification
Blocks to terminal differentiation
Cell cycle
Signalling cascade
EZH2 mutations
BCL6 expression
MYC and BCL2 translocations
PTEN del/loss(PI3k/AKT/mTORactivation)
CD79A, CARD11, MYD88mutationsTNFAIP3 (A20) deletions
PRDM1 loss/mutations
MYC and BCL2 proteinoverexpression
JAK-STAT pathway activationSehn and Gascoyne, Blood 2015
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Drugable genetic alterationsGCB ABC
BCR/NFkB signalling
Histone modification
Blocks to terminal differentiation
Cell cycle
Signalling cascade
EZH2 mutations
BCL6 expression
MYC and BCL2 translocations
PTEN del/loss(PI3k/AKT/mTORactivation)
CD79A, CARD11, MYD88mutationsTNFAIP3 (A20) deletions
PRDM1 loss/mutations
MYC and BCL2 proteinoverexpression
JAK-STAT pathway activationSehn and Gascoyne, Blood 2015
Inhibitors of the signalling
cascade
BCL6 inhibitors
EZH2 inhibitors
BCL2 inhibitors
Inhibitors of BCR/NFkBsignalling
JAK inhibitors
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Phase III studies based on COO
• Phase III studies in ABC (non-GCB)– R-CHOP +/- bortezomib– R-CHOP +/- ibrutinib– R-CHOP +/- lenalidomide
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Phase III studies based on COO
• Phase III studies in ABC (non-GCB)– R-CHOP +/- bortezomib NEGATIVE– R-CHOP +/- ibrutinib NEGATIVE– R-CHOP +/- lenalidomide NO RESULTS YET
ESO-ESMO E
EBR Mas
tercla
ss 20
19

Phase III studies with new drugs in 1st line DLBCL
Iacoboni G et al, Ann Oncol, 2018
ESO-ESMO E
EBR Mas
tercla
ss 20
19
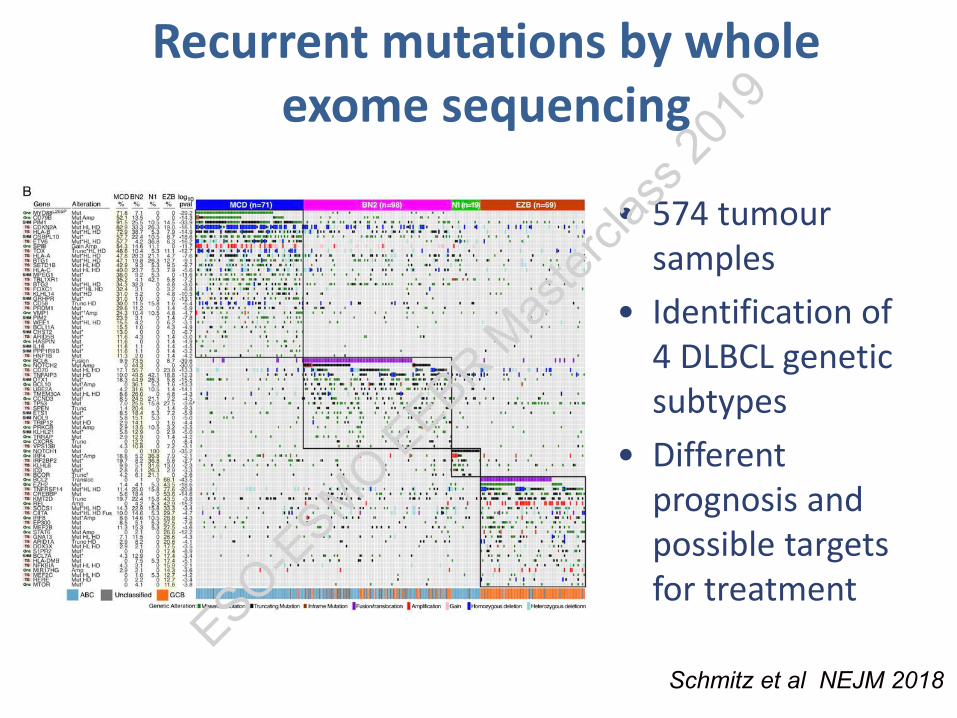
Recurrent mutations by whole exome sequencing
Schmitz et al NEJM 2018
• 574 tumour samples
• Identification of 4 DLBCL genetic subtypes
• Different prognosis and possible targets for treatment
ESO-ESMO E
EBR Mas
tercla
ss 20
19
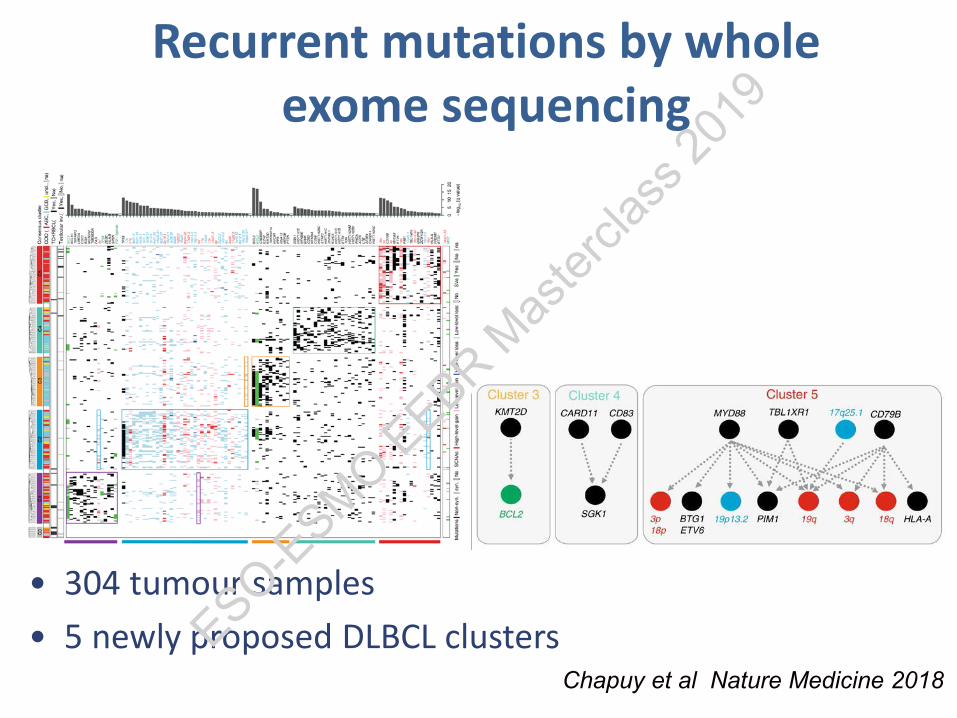
Recurrent mutations by whole exome sequencing
Chapuy et al Nature Medicine 2018
• 304 tumour samples• 5 newly proposed DLBCL clustersESO-E
SMO EEBR M
aster
class
2019

How I treat DLBCL
• R-CHOP remains the standard of care• Consolidation with ASCT in selected young high IPI• R-CHOP + CNS prophylaxis based on CNS risk factors• No data to support MTAs added to R-CHOP based on
COO• Intensified treatment and CNS prophylaxis in HGBL
with MYC +/- BCL2 +/- BCL6 rearrangements
ESO-ESMO E
EBR Mas
tercla
ss 20
19
In conclusion
• Treatment outcomes improved for many different lymphomas
• In DLBCL RCHOP remains the standard of care• All phase III trials have failed to imrpove treatment
outcomes in 1st line• CARTs have shown great activity in r/r DLBCL patients
(problem of costs!!!)• Need to direct treatment to specific genetic
alterationsESO-E
SMO EEBR M
aster
class
2019

Thank you for your attention
ESO-ESMO E
EBR Mas
tercla
ss 20
19