not for publication or presentation · not for publication or presentation ... john f. dipersio,...
TRANSCRIPT

Not for publication or presentation
A G E N D A CIBMTR WORKING COMMITTEE FOR ACUTE LEUKEMIA Salt Lake City, Utah Saturday, February 16, 2013, 2:45 pm - 4:45 pm
Co-Chair: Donald Bunjes, MD, University Hospital Ulm, Ulm, Germany
Phone: 49-731-500-45532; Fax: 49-731-500-45655; E-mail: [email protected]
Co-Chair: Steven Devine, MD, Ohio State Medical Center - James Cancer Center Phone: 614-293-9868; Fax: 614-293-6690; E-mail: [email protected] Co-Chair: John F. DiPersio, MD, PhD, Washington University School of Medicine Phone: 314-454-8491; Fax: 314-454-8315; E-mail: [email protected] Statisticians: Hailin Wang, MPH, CIBMTR Statistical Center
Phone: 414-805-0647; Fax: 414-805-0714; E-mail: [email protected] Mei-Jie Zhang, PhD, CIBMTR Statistical Center Phone: 414-456-8375; Fax: 414-456-6530; E-mail: [email protected]
Scientific Director: Daniel Weisdorf, MD, University of Minnesota Phone: 612-624-3101; Fax: 612-625-6919; E-mail: [email protected] 1. Introduction
a. 2012 Tandem minutes for approval (Attachment 1) b. Newly appointed chair: Marcos de Lima, MD; University Hospitals Case Medical Center;
E-mail: [email protected] 2. Accrual summary (Attachment 2)
3. Presentations, published or submitted papers
a. LK04-03 Keating A, DaSilva G, Perez WS, Gupta V, Cutler CC, Ballen KK, Cairo MS, Camitta BM, Champlin RE, Gajewski JL, Lazarus HM, Lill M, Marks DI, Nabhan C, Schiller GJ, Socie G, Szer J, Tallman MS, Weisdorf DJ. Autologous blood cell transplantation versus HLA-identical sibling transplantation for acute myeloid leukemia in first complete remission: A registry study from the Center for International Blood and Marrow Transplant Research. Haematologica 2012.
b. LK07-03b Warlick E, Ahn KW, Pedersen TL, Artz A, DeLima M, Pulsipher M, Akpek G, Aljurf M, Cahn JY, Cairo M, Chen YB, Cooper B, Deol A, Giralt S, Gupta V, Khoury HJ, Kohrt H, Lazarus H, Lewis I, Olsson R, Pidala J, Savani B, Seftel M, Socie G, Tallman M, Ustun C, Vij R, Vindel?v L, Weisdorf DJ. RIC is superior to NMA conditioning for older Chronic Myelogenous Leukemia patients undergoing hematopoietic cell transplant during the TKI Era. Blood 2012.
c. R02-05 Foran JM, Pavletic SZ, Logan BR, Agovi-Johnson MA, Pérez WS, Bolwell BJ, Bornhäuser M, Bredeson CN, Cairo MS, Camitta BM, Copelan EA, Dehn J, Gale RP, George B, Gupta V, Hale G, Lazarus HM, Litzow MR, Maharaj D, Marks DI, Martino R, Maziarz RT, Rowe JM, Rowlings PA, Savani BN, Savoie ML, Szer J, Waller EK, Wiernik PH, Weisdorf DJ. Unrelated Donor allogeneic transplantation after failure of autologous transplantation for acute myeloid leukemia: a study from the CIBMTR. Submitted.
d. LK08-02 Koreth J, Pidala J, Pérez WS, Deeg JH, Garcia-Manero G, Malcovati L, Cazzola M, Park S, Itzykson R, Ades L, Fenaux P, Jadersten M, Hellstrom-Lindberg E, Gale RP, Beach CL, Greenberg PL, Tallman MS, DiPersio JF, Bunjes D, Weisdorf DJ, Cutler C. A Decision Analysis of Reduced-Intensity Conditioning Allogeneic Hematopoietic Stem Cell
1

Not for publication or presentation
Transplantation for Older Patients with de-novo Myelodysplastic Syndrome (MDS): Early Transplantation Offers Survival Benefit in Higher-Risk MDS. Submitted.
e. LK08-01 Lee SJ, Storer B, Wang HL, Lazarus HM, Waller E, Isola L, Klumpp T, Savani B, Loren A, Cairo MS, Camitta B, Cutler CC, George B, Khoury J, Marks DI, Rizzieri D, Copelan E, Gupta V, Liesveld J, Litzow MR, Miller A, Shouten H, Gale R, Cahn JY, Weisdorf DJ. Factors significantly associated with leukemia-free survival (LFS) and chronic graft-versus-host disease in adult patients more than 1 year after myeloablative allogeneic transplantation for acute leukemia. Submitted.
f. LK10-02 Warlick ED, Litzow M, Paulson K, Weisdorf DJ. Pre-transplant consolidation chemotherapy does not improve outcomes following reduced intensity conditioning (RIC) hematopoietic cell transplant (HCT) for acute myeloid leukemia (AML) in CR1 (E Warlick/ M Litzow). Presentation at the BMT Tandem Meetings in Salt Lake City, UT, February 2013.Manuscript in preparation.
g. LK10-03 Bachanova V, Marks DI, Zhang MJ, Wang HL, Weisdorf DJ. Older patients with Ph+ acute lymphoblastic leukemia (ALL) in first remission (CR1) have prolonged survival with either myeloablative or reduced intensity conditioning allogeneic transplantation: Impact of imatinib and minimal residual disease (MRD) on outcomes: a CIBMTR matched-pair study (V Bachanova). Presentation at the BMT Tandem Meetings in Salt Lake City, UT, February 2013.Manuscript in preparation.
4. Studies in progress (Attachment 3)
a. R02-09 DLI after relapse (A Loren) Data file preparation b. LK04-01 Allo and auto HCT for APML in CR2
(M Rubinger /M Tallman) Multivariate analysis
c. LK07-03c Allo HCT in older patients with NHL (B McClune) Manuscript Preparation d. LK09-02 Monosomal karyotype and chromosomal 7
abnormalities in allo HCT for AML/MDS (M Pasquini/ M Battiwala)
Protocol Development
e. LK10-02 Pre-HCT consolidation therapy on outcomes of RIC allo for AML in CR1 (E Warlick/M Litzow)
Manuscript preparation
f. LK10-03 Ph+ ALL in adults comparing RIC/MA allo HCT (V Bachanova)
Manuscript preparation
g. LK11-01 Extramedullary disease and outcome in allo HCT for AML (S Goyal/ G Uy)
Protocol development
h. LK12-01 Chemo vs. AlloHCT for Ph- ALL (M Seftel) (Attachment 4)
Draft protocol received
i. LK12-02 Allotx for FLT3/ITD positive AML in CR1 (S Sengsayadeth/ A Deol/ B Savani/ M Jagasia) (Attachment 5)
Draft protocol received FLT3 collaboration ongoing
5. Future/ Proposed studies (Attachment 6 through 13)
AML a. PROP 1012-02 To Determine whether In-vivo T Cell Depletion with Alemtuzumab Affects Outcome after
Myeloablative TBI-based Conditioning in Children and Young Adults who Received Unrelated Donor Transplants for AML (S Samarasinghe/ P Veys/ M Eapen) (Attachment 6)
b. PROP 1112-06 Comparing Autologous to Allogeneic Transplant in APL Patients with Extramedullary Disease who Achieve a Second or Subsequent Complete Remission (CR) (C Ganzel/ M Tallman/ D Douer) (Attachment 7)
c. PROP 1112-10 Comparing Autologous Transplant to Arsenic Trioxide (ATO) for Patients with Acute Promyelocytic Leukemia (APL) in First and Subsequent Relapse (C Ganzel/ M Tallman/ D Douer) (Attachment 8)
2

Not for publication or presentation
ALL d. PROP 1112-38 Allogeneic Transplantation For Older Patients with Acute Lymphoblastic Leukemia:
Impact of Age on Transplant Outcomes (Bachanova V) (Attachment 9) e. PROP 1112-35 Prognostic Significnace of Cytogenetic Abnormalities in Patients with Philadelphia-
negative Acute Lymphoblastic Leukemia undergoing Allogeneic Hematopoietic Stem Cell Transplantation in Complete Remission: A CIBMTR Study (Lazaryan A) (Attachment 10)
f.
PROP 1112-41 Outcomes of Allogeneic Stem Cell Transplantation in T cell Acute Lymphoblastic Leukemia (Rasheed W) (Attachment 11)
ALL LEUKEMIAS g. PROP 0712-04 Allogeneic Transplantation for Acute Biphenotypic Leukemia (ABL): Disease
Characteristics, Complications and Outcomes (R Munker) (Attachment 12) h. PROP 1112-26 The Impact of Peripheral Blood Chimerism on Transplant Outcomes in Patients with
Acute Leukemia and Myelodysplastic Syndrome (Kebriaei P) (Attachment 13)
3

Not for publication or presentation Attachment 1
MINUTES CIBMTR WORKING COMMITTEE FOR ACUTE LEUKEMIA San Diego, California Saturday, February 4, 2013, 12:15 pm - 2:15 pm
Co-Chair: Donald Bunjes, MD, University Hospital Ulm, Ulm, Germany
Phone: 49-731-500-45532; Fax: 49-731-500-45655; E-mail: [email protected]
Co-Chair: Steven Devine, MD, Ohio State Medical Center - James Cancer Center Phone: 614-293-9868; Fax: 614-293-6690; E-mail: [email protected] Co-Chair: John F. DiPersio, MD, PhD, Washington University School of Medicine Phone: 314-454-8491; Fax: 314-454-8315; E-mail: [email protected] Statisticians: Waleska S. Pérez, MPH, CIBMTR Statistical Center
Phone: 414-805-0700; Fax: 414-805-0714; E-mail: [email protected] Mei-Jie Zhang, PhD, CIBMTR Statistical Center Phone: 414-456-8375; Fax: 414-456-6530; E-mail: [email protected]
Scientific Director: Daniel Weisdorf, MD, University of Minnesota Phone: 612-624-3101; Fax: 612-625-6919; E-mail: [email protected]
1. Introduction The CIBMTR Acute Leukemia Working Committee was called to order at 12:20 pm on Saturday, February 4, 2012, by Dr. John DiPersio. The chairs, scientific director and statisticians were presented. Attendees were asked to have their name badges scanned for attendance purposes and to maintain the committee membership roster, and to fill out the Working Committee evaluations and voting sheets for proposals. The CIBMTR new guidelines for voting on proposals were discussed. The new guidelines are based on a scale from 1 to 9; 1= high scientific impact, 9= low scientific impact. The meeting was limited to presentation and discussion of proposals; attendees were asked to review the materials to assess the progress of ongoing studies and the committee’s accomplishments for the past year. Each presentation was limited to 5 minutes (maximum 3-4 overheads) to allow for adequate time for discussion (5 minutes) for the new proposals. The minutes of the February 2011 meeting were approved without modifications.
Dr. Daniel Weisdorf announced the new CIBMTR effort, the Forms Revision Process. All data collection forms are undergoing revision over the next two years, starting with the following: CRID (2804), Pre-TED (2400), Baseline (2000), Infectious Disease Markers (2004), HLA (2005), Infusion (2006), AML (2010/2110), ALL (2011/2111), MDS (2014/2114), JMML (2015/2115), Plasma Cell Disorders (2016/2116), Amyloidosis (2017/2117), Lymphoma (2018/2118) and Waldenstrom's Macroglobulinemia (2019/2119). The revised forms will coincide with the development of the new FormsNet application. Members are encouraged to become a member of the Forms Revision Review Committee in order to capture all the relevant information needed to produce high-quality studies. Suggestions for forms should be forwarded to the Acute Leukemia Working Committee Leadership or Emilie Meissner at [email protected].
4

Not for publication or presentation Attachment 1
2. Accrual summary
Due to the full agenda, the accrual summary of registration and research cases between 1995 and 2011 were not presented to the committee but were available as part of the Working Committee attachments:
Registration only ResearchAML allogeneic 20877 17589ALL allogeneic 11931 9948AML autologous 4588 1191ALL autologous 706 203
3. Presentations, published or submitted papers Due to the full agenda, the 2011 presentations and published papers were mentioned but not presented. Two papers were published; one in press, one submitted and three ASH presentations were given during the past year. These include:
a. LK04-02/GV01-01 Luger SM, Ringdén O, Zhang M-J, Pérez WS, Bishop MR, Bornhauser M,
Bredeson CN, Cairo MS, Copelan EA, Gale RP, Giralt SA, Gulbas Z, Gupta V, Hale GA, Lazarus HM, Lewis VA, Lill MC, McCarthy PL, Weisdorf DJ, Pulsipher MA. Similar outcomes using myeloablative versus reduced intensity allogeneic transplant preparative regimens for Acute Myeloid Leukemia or Myelodysplasia. Bone Marrow Transplantation, 2011.
b. LK06-01 Farag SS, Maharry K, Zhang MJ, Pérez WS, George SL, Mrózek K, Dipersio J, Bunjes DW, Marcucci G, Baer MR, Cairo MS, Copelan EA, Cutler CS, Isola LM, Lazarus HM, Litzow MR, Marks DI, Ringden O, Rizzieri DA, Soiffer RJ, Larson RA, Tallman MS, Bloomfield CD, Weisdorf DJ. Comparison of reduced-intensity allogeneic hematopoietic cell transplantation with chemotherapy in patients aged 60-70 years with acute myeloid leukemia in first remission: A Center for International Blood and Marrow Transplant Research and Cancer and Leukemia Group B study. Biology of Blood & Marrow Transplantation, 2011. Epub ahead of print.
c. LK07-01 Armand P, Kim HT, Zhang MJ, Pérez WS, Cin PD, Klumpp TR, Lazarus HM, Artz AS, Gupta V, Isola LM, Halter J, Rowe JM, Antin JH, Camitta BM, Cairo MS, Sierra J, Stiff PJ, Nabhan C, Jakubowski AA, Devine SM, Maziarz RT, Marks DI, Aljurf MD, Soiffer RJ, Weisdorf DJ. Classifying cytogenetics in patients with AML in complete remission undergoing allogeneic transplantation: a CIBMTR study. Biology of Blood and Marrow Transplantation, 2011. In Press.
d. LK04-03 Keating A, DaSilva G, Pérez WS, Gupta V, Cutler CS, Ballen KK, Cairo MS, Camitta BM, Champlin RE, Gajewski JL, Horan JT, Lazarus HM, Lill M, Marks DI, Nabhan C, Schiller GJ, Socie G, Szer J, Tallman MS, Weisdorf DJ. Autologous blood cell transplantation versus HLA-identical sibling transplantation for Acute Myeloid Leukemia in first complete remission. Submitted.
e. LK07-03b Warlick ED, McClune B, Pedersen TL, Awn KW, Antin JH, Cahn JY, DeLima M, Gupta V, Marks DI, Bunjes D, DiPersio JF, Devine S, Weisdorf DJ. Older adults with chronic myelogenous leukemia (CML), during the tyrosine kinase inhibitor (TKI) era, can be successfully treated with reduced intensity conditioning (RIC) hematopoietic cell transplant (HCT) using sibling or unrelated donors: a Center for International Blood and Marrow Transplant Research (CIBMTR) analysis. Presented at the American Society of Hematology in San Diego, California,
5

Not for publication or presentation Attachment 1
December 2011. Manuscript in preparation.
f. LK07-03b McClune B, Pedersen TL, Ahn KW, Warlick ED, Pidala J, Waller EK, Rizzo JD, Cairo MS, Woolfrey A, Artz A, Lazarus HM, Weisdorf DJ. Reduced intensity or non-ablative hematopoietic cell transplantation in older patients with non-Hodgkin lymphoma (NHL): encouraging survival for patients ≥55 years. Presented at the American Society of Hematology in San Diego, California, December 2011. Manuscript in preparation.
g. LK08-02 Koreth J, Pidala J, Perez WS, Deeg HJ, Garcia-Manero G, Malcovati L, Cazzola M, Park S, Itzykson R, Ades L, Fenaux P, Jädersten M, Hellstrom-Lindberg E, Gale RP, Beach CL, Greenberg PL, Tallman MS, DiPersio JF, Bunjes D, Weisdorf DJ, Cutler CS. A decision analysis of reduced-intensity conditioning allogeneic hematopoietic stem cell transplantation for older patients with de-novo myelodysplastic syndrome (MDS): early transplantation offers survival benefit in higher-risk MDS. Presented at the American Society of Hematology in San Diego, California, December 2011.
4. Studies in progress
The studies which made progress during the past year were not presented in order to provide reasonable time to the new proposals for presentation and discussion. A summary of the progress was provided as an attachment to the committee members. These were: a. R02-05: Unrelated donor stem cell transplantation in AML and all patients who failed an
autologous transplant (J Foran): This study proposes to examine ALL and AML patients receiving URD HCT after relapse from a previous autograft and to identify patients likely to have the best outcome. A draft manuscript is in preparation and it is expected to be submitted after Tandem.
b. R02-09: Evaluation of donor leukocyte infusions to treat relapsed hematologic malignancies after related and unrelated donor myeloablative allogeneic hematopoietic stem cell transplantation (A Loren): The value of related and unrelated donor DLI in treatment of acute leukemia relapsed after allografting will be examined, including the impact of disease status, timing, dose response, and comparative efficacy of the two donor sources. Secondary data collection is required and is underway. The protocol is available for review and secondary data collection is underway.
c. LK04-01: Comparison of autologous and allogeneic hematopoietic stem cell transplantation for patients with acute promyelocytic leukemia (APL)in second complete remission (M Rubinger/M Tallman): This project analyzes outcome of APL in second CR including details of molecular remission prior to transplant. Secondary data collection was completed and the data file preparation is underway.
d. LK07-02: CIBMTR scoring system to predict the outcome after allogeneic transplantation for acute myeloid leukemia (J Sierra): This study proposes to identify the factors that will impact leukemia-free survival after allogeneic HCT following myeloablative conditioning as treatment for primary AML. Based on the factors identified, a scoring system predicting the outcome will be generated. The data file preparation is underway.
e. LK07-03b: Assessment of allogeneic HCT in older patients with Non-Hodgkin Lymphoma and Chronic Myelogenous Leukemia (E Warlick/ B McClune): This study proposes to compare the clinical outcomes of older adults with MDS, de novo AML, AML evolving from preceding MDS,
6

Not for publication or presentation Attachment 1
CML and lymphoma after allogeneic hematopoietic cell transplantation (HCT) to younger adults. The manuscript for the AML and MDS population was published in JCO and the manuscript for Lymphoma and CML are expected to be submitted after Tandem.
f. LK08-01: Using landmark analysis to provide updated relapse and leukemia-free or overall survival estimates to patients (S Lee): This study proposes to provide clinically understandable estimates of the likelihood of future events to patients surviving disease-free after allogeneic transplantation, that are based on the duration of leukemia-free survival already experienced, specifically, to provide estimates of the risks for relapse within the next year, leukemia-free survival for the next 3 and 5 years. Additional factors that impact long-term survival, such as patient age, cytogenetics and whether or not chronic GVHD has developed, will be incorporated into the estimates. The analysis is underway. A draft manuscript is expected to be submitted by July 2012.
g. LK08-02: A decision analysis of reduced intensity conditioning allogeneic stem cell transplantation for older patients with de-novo myelodysplastic syndrome (J Koreth): The purpose of this study is to use decision analysis and the best available databases to determine the optimal role and timing of RIC alloHCT for de-novo MDS patients ≥60 years. The dataset includes data from four patients cohorts: (1) natural history cohort from the IMRAW group at Stanford University and the Pavia group at the University of Pavia medical School in Italy; (2) erythropoiesis agent therapy cohort from the Groupe Francophone des Myelodysplasies (GFM); (3) hypomethylating agent therapy cohort from the AZA-001 Phase III Study of the International Vidaza High-Risk MDS Survival Study Group (IVHMSS) and those receiving decitabine therapy on research studies at M.D. Anderson Cancer Center and (4) transplantation cohort from the CIBMTR, EBMT, DFCI and FHCRC. A draft manuscript is in preparation and it is expected to be submitted by July 2012.
h. LK08-04/ IB08-05: Evaluation of lymphotoxin alpha (LTA) alleles in relation to relapse in AML and CML (P Posch): This is a joint study with the Immunobiology Working Committee and it proposes to determine whether LTA alleles correlate with relapse in AML and CML and to determine if the correlation is associated with high or low LTA production. The study has been deferred for the past year due to outstanding sampling testing which is needed as the basis for the protocol.
i. LK09-02: Impact of monosomal karyotype in the outcome of hematopoietic cell transplantation for Acute Myeloid Leukemia and Myelodysplasia (M Pasquini/ M Battiwala): The purpose of this study is to identify the impact of high risk cytogenetic subsets: specifically chromosome 7 abnormalities (either monosomy7 or del(7q)) and monosomal karyotype in outcomes for AML and MDS after allogeneic HCT and to evaluate the impact of conditioning intensity in the outcome of patients with AML and monosomal karyotype. The data file preparation is underway.
7

Not for publication or presentation Attachment 1
j. LK10-02: Effect of pre-transplant consolidation chemotherapy on outcomes of RIC Allogeneic
transplant for adults with AML in CR1 (E Warlick): The purpose of this study is to (1) compare the outcomes of adults with AML in first remission who have received no consolidation, standard-dose cytarabine consolidation, or high-dose cytarabine consolidation followed by reduced intensity conditioning related or unrelated donor allogeneic stem cell transplantation (HCT) and (2) to determine if there is an exposure threshold (number of cycles of consolidation) that impacts post-transplant outcomes. A draft protocol is available for review.
k. LK10-03: The outcome of adults with philadelphia positive acute lymphoblastic leukemia comparing reduced intensity conditioning and myeloablative conditioning allogeneic stem cell transplantation (V Bachanova): The purpose of this study is to (1) to compare outcomes of adults with Ph+ ALL who received reduced intensity versus myeloablative conditioning followed by sibling or matched unrelated donor HCT; (2) to examine the effect of pre-transplant treatment with tyrosine kinase inhibitors (TKI) on transplant outcomes using RIC and MA conditioning and (3) to examine the prognostic significance of patient, disease and transplant related characteristics on transplant outcomes. Supplemental data collection regarding TKI use is required and funds are available for this purpose. The protocol is available for review and supplemental data collection is underway.
l. LK11-01: Impact of extramedullary disease on the outcome of allogeneic HCT in AML ((S Goyal/ G Uy): The purpose of this proposal is (1) to describe the outcome of patients undergoing alloHSCT for AML with extramedullary involvement and (2) to assess patient, disease and transplant related factors which influence the outcome of alloHSCT in AML. There are 1044 AML patients ≥18 years of age with extramedullary disease prior to HCT reported to the CIBMTR between 1995 and 2008. A draft protocol is available for review.
m. LK11-02: Development of a prognostic scoring system to predict relapse of ALL after allogeneic HCT (R Salit/ M Bishop/ D Porter): The purpose of this proposal is to develop a prognostic scoring system based on patient, disease, and transplant-specific factors that is predictive of relapse after allogeneic hematopoietic stem cell transplantation in patients with ALL and (2) to assess the association of the variables identified within this scoring system with transplantation outcomes and outcomes after relapse. There are 4165 ALL patients ≥ 18 years that underwent an allogeneic transplant and reported to the CIBMTR between 1995 and 2008. A draft protocol is available for review.
8

Not for publication or presentation Attachment 1
5. Future/ Proposed studies Drs. Bunjes and DiPersio led this section. The proposals were the followings: a. PROP 0911-02 A prognostic risk index for older patients with AML in CR1 undergoing allogeneic
stem cell transplantation (Y-B Chen/S Devine) Dr. Chen presented this proposal. The purpose of this study is to (1) to validate the HCT comorbidity index for older patients with AML in CR1 undergoing alloHCT as well as analyze if several other clinical factors are predictive for non-relapse mortality in RIC HCT; (2) if the HCT-CI does not prove to be predictive of non-relapse mortality, then we will identify the chronic medical conditions and other clinical factors which are important for predicting NRM for older patients with AML in CR1 undergoing RIC HCT. The HCT-CI or a new prognostic index will then be hopefully integrated with clinical, cytogenetic, and molecular data into a scoring system to predict overall survival probabilities for older patients with AML in CR1 undergoing alloHCT. There are 247 myeloablative and 272 RIC/NMA patients ≥50 years of age that underwent an allogeneic for AML within 6 months after achieving a first complete remission reported to the CIBMTR between 2008 and 2010.
b. PROP 1111-02 Allogeneic stem cell transplantation for FLT3/ITD positive AML in CR1 (S Sengsayadeth/B Savani/M Jagasia) and PROP 1111-73 Impact of FLT3-internal tandem duplication (FLT3-ITD) mutation on outcomes of hematopoietic stem cell transplant for cytogenetically normal AML (A Deol) Dr. Sengsayadeth presented this proposal. The purpose of this proposal is (1) to study the prognostic significance of fms-like tyrosine kinase 3/internal tandem mutation (FLT3/ITD) mutation in AML compared to other conventional prognostic markers in patients receiving alloHCT in CR1; (2) to study the impact of FLT3/ITD mutation on incidence of relapse, disease-free survival, and overall survival after allo-SCT in CR1; (3) to study the impact of prior chemotherapy, including the effect of consolidation; and (4) to study the impact of cytogenetics and NPM1 mutation in patients with FLT3/ITD AML. There are 118 patients ≥18 years of age that underwent an HLA-identical sibling or well-matched unrelated transplant for AML FLT-3+ in first complete remission reported to the CIBMTR between 2008 and 2010. It was noted the lack of molecular data and lack of detailed information of FLT3 on the CIBMTR forms. The Acute Leukemia Chairs are communicating with the multicenter FLT3 trials for future collaboration and expansion of the data.
c. PROP 1111-27 Analysis of prognostic significance of persistent cytogenetic and molecular abnormalities at last evaluation prior to allogeneic hematopoietic stem cell transplantation in AML patients in first complete remission (B Oran/ D Weisdorf/ M de Lima) Dr. Weisdorf presented this proposal in Dr. Oran’s absence. The purpose of this proposal is to analyze the prognostic significance of persistent cytogenetic abnormalities at last evaluation prior to allo-HCT on leukemia free survival, overall survival, transplant-related mortality and relapse in AML patients with CR1. There are 146 MRD+ and 1030 MRD- patients ≥18 years of age that underwent an HLA-identical sibling or unrelated donor transplant AML in first complete remission reported to the CIBMTR between 2008 and 2010. Of the 146 MRD+ patients, 21 were in molecular remission, 39 in cytogenetic remission and 19 in molecular and cytogenetic remission. MRD information on the forms is as reported by the center (yes/no). It was suggested to confirm the information of MRD+ although this would require secondary data collection.
9
Not for publication or presentation Attachment 1
d. PROP 1111-29 Chemotherapy versus allogeneic hematopoietic cell transplantation in philadelphia
negative chromosome negative adult ALL (M Seftel) Dr. Seftel presented this proposal. The purpose of this proposal is (1) to compare overall survival, disease-free survival, and treatment-related mortality of young adults with Ph- ALL in first complete remission treated with either alloHCT or with a pediatric style chemotherapy regimen and (2) to identify predictors of OS, DFS, and TRM in this population of adults with ALL. There are 548 patients 18-50 years of age that underwent a bone marrow or peripheral blood myeloablative transplant for Ph- ALL in first complete remission reported to the CIBMTR between 2002 and 2010. The chemotherapy group consists of 100 patients enrolled in the two consecutively conducted Dana-Farber Cancer Institute (DFCI) adult ALL consortium phase II trials between June 1 2002 and December 31 2010 who achieved CR1 (DFCI 01-0175 and 06-254).
e. PROP 1111-14 Interaction between obesity and total body irradiation in allogeneic transplantation for acute leukemia (D Vogl) Dr. Vogl presented this proposal. The purpose of this proposal is (1) to determine whether there is an interaction between body mass index and conditioning regimens containing total body irradiation in determining leukemia-free and overall survival among patients with ALL undergoing alloHCT; (2) to assess whether other factors mediate the relationship between body mass index and conditioning regimen in this population and (3) to determine whether obese patients have worse outcomes in general than normal weight patients in this population. There are 1667 patients (underweight, n=118; normal, n=766, overweight, n=479, obese, n=198, severely obsess, n=52, morbidly obese, n=54) ≥18 years of age who underwent an HLA-identical sibling or matched unrelated donor myeloablative transplant for ALL in first or second complete remission reported to the CIBMTR between 2008 and 2010.
Five additional proposals were submitted to the committee but not presented due to reasons stated below: a. PROP 1111-40 Outcomes of unrelated donor hematopoietic cell transplantation recipients enrolled
in a multicenter clinical trial compared to standard of care (T Kroll/ M Pasquini/ C Bredeson): Overlaps with approved study HS11-01 “Generalizability of BMT CTN 0201 results: prognostic and outcome differences between participants and nonparticipants”.
b. PROP 1111-54 Examining differences in relapse management and response following T-cell replete versus T-cell depleted allogeneic stem cell transplantation in patients with AML or MDS (E Morawa/S Giralt): Not doable due to complexity of data required (multiple steps; evaluations and clinical decision points), cost of secondary data collection and difficulty for centers to provide the needed data.
c. PROP 1111-26 Effect of post-remission chemotherapy before human leukocyte antigen–identical sibling transplantation for AML in first complete remission (A Ghavamzadeh/ K Moghaddam): Overlaps with approved study LK10-02 “Effect of pre-transplant consolidation chemotherapy on outcomes of RIC Allogeneic transplant for adults with AML in CR1”.
d. PROP 1111-49 Impact of a structurally complex karyotype in outcome of stem cell transplantation for AML and MDS (C Dobbelstein/G Göhring/ A Ganser): Overlaps with approved study LK09-02 “Impact of monosomal karyotype in the outcome of hematopoietic cell transplantation for Acute Myeloid Leukemia and Myelodysplasia”.
10

Not for publication or presentation Attachment 1
e. PROP 1111-76 Use of tyrosine kinase inhibitors after allogeneic hematopoietic stem cell transplantation for philadelphia chromosome positive ALL (M Litzow): Overlaps with approved study LK10-03 “The outcome of adults with philadelphia positive acute lymphoblastic leukemia comparing reduced intensity conditioning and myeloablative conditioning allogeneic stem cell transplantation”.
6. Other business
After the new proposals were presented, each participant in the meeting had the opportunity to rate each proposal using paper ballots. Based on the voting results, current scientific merit and the impact of the study on the field the following studies will move forward:
1. LK04-01: SCT for APL 2. LK04-03: Auto PBSC vs. HLA-identical sibling alloHCT for AML-CR1 3. R02-05: URD after failed autologous HCT 4. R02-09: DLI for relapse
5. LK07-03b: Allo HCT in older patients with CML
6. LK07-03c: Allo HCT in older patients with lymphoma
7. LK08-01: Landmark analysis for updated relapse/LFS estimates for patients
8. LK08-02: RIC in alloHCT for older patient with denovo MDS - decision analysis
9. LK09-02: Monosomal karyotype and chromo 7 abnormalities in allo HCT for AML/MDS
10. LK10-02: Pre-HCT consolidation therapy on outcomes of RIC allo for AML in CR1
11. LK10-03: Ph+ ALL in adults comparing RIC/MA allo HCT
12. LK11-01: Extramedullary disease and outcome in allo HCT for AML
13. LK12-01: Chemo vs. AlloHCT for Ph- ALL
14. LK12-02: Allogeneic stem cell transplantation for FLT3/ITD Positive AML in CR1
11
Not for publication or presentation Attachment 1
The following studies and proposals were discontinued due to lack of pertinent data and assessment of lower scientific priority at the time of publication by the Chairs:
LK07-02 Scoring system as predictor in AML after HCT LK08-04/IB08-05 LTA alleles in AML relapse LK11-02 Prognostic scoring system to predict relapse of ALL after allogeneic HCT
PROP 0911-02 A prognostic risk index for older patients with AML in CR1 undergoing allogeneic stem cell transplantation
PROP 1111-27
Analysis of prognostic significance of persistent cytogenetic and molecular abnormalities at last evaluation prior to allogeneic hematopoietic stem cell transplantation in AML patients in first complete remission
PROP 1111-14 Interaction between obesity and total body irradiation in allogeneic transplantation for acute leukemia
PROP 1111-40
Outcomes of unrelated donor hematopoietic cell transplantation recipients enrolled in a multicenter clinical trial compared to standard of care (T Kroll/ M Pasquini/C Bredeson) (overlaps with approved study HS11-01)
PROP 1111-54
Examining differences in relapse management and response following T-cell replete versus T-cell depleted allogeneic stem cell transplantation in patients with AML or MDS (E Morawa/S Giralt) (not doable due to complexity of data required (multiple steps; evaluations and clinical decision points), cost of secondary data collection and difficulty for centers to provide the needed data)
PROP 1111-26
Effect of post-remission chemotherapy before human leukocyte antigen–identical sibling transplantation for AML in first complete remission (overlaps with approved study LK10-02)
PROP 1111-49 Impact of a structurally complex karyotype in outcome of stem cell transplantation for AML and MDS (overlaps with approved study LK09-02)
PROP 1111-76
Use of tyrosine kinase inhibitors after allogeneic hematopoietic stem cell transplantation for philadelphia chromosome positive ALL (overlaps with approved study LK10-03)
Dr. Weisdorf expressed gratitude to the Committee members for their active role and valuable support to the Committee. Without additional comments, the meeting was adjourned at 1:40 pm.
12

Not for publication or presentation Attachment 2
Accrual Summary for Acute Leukemia Working Committee
Characteristics of recipients of allogeneic transplants for AML reported to the CIBMTR between 1995 and 2012
Variable TED only ResearchNumber of patients 22776 19854Number of centers 465 382Median (range) 42 (<1-83) 43 (<1-84)Age in decades <10 1658 ( 7) 1702 ( 9) 10-19 2257 (10) 1973 (10) 20-29 2776 (12) 2340 (12) 30-39 3830 (17) 2786 (14) 40-49 4980 (22) 3760 (19) 50-59 4647 (20) 4172 (21) 60-69 2404 (11) 2804 (14) >=70 208 (<1) 317 (2) Missing 16 (<1) 0Gender Male 12178 (53) 10511 (53) Female 10557 (46) 9341 (47) Missing 41 (<1) 2 (<1)Type of donor Related 17251 (76) 6779 (34) Unrelated 5525 (24) 13075 (66)Graft type Bone marrow 7392 (32) 6592 (33) Peripheral blood 14267 (63) 11192 (56) Cord blood 712 ( 3) 2050 (10) Missing 405 ( 2) 20 (<1)Year of HCT 1995-1996 1454 ( 6) 1639 ( 8) 1997-1998 2055 ( 9) 1457 ( 7) 1999-2000 2537 (11) 1444 ( 7) 2001-2002 2778 (12) 1813 ( 9) 2003-2004 2908 (13) 2124 (11) 2005-2006 2927 (13) 2577 (13) 2007-2008 2451 (11) 2907 (15) 2009-2010 2768 (12) 3473 (17) 2011-2012a 2898 (13) 2420 (12)a Cases continue to be reported in this interval
13
Not for publication or presentation Attachment 2
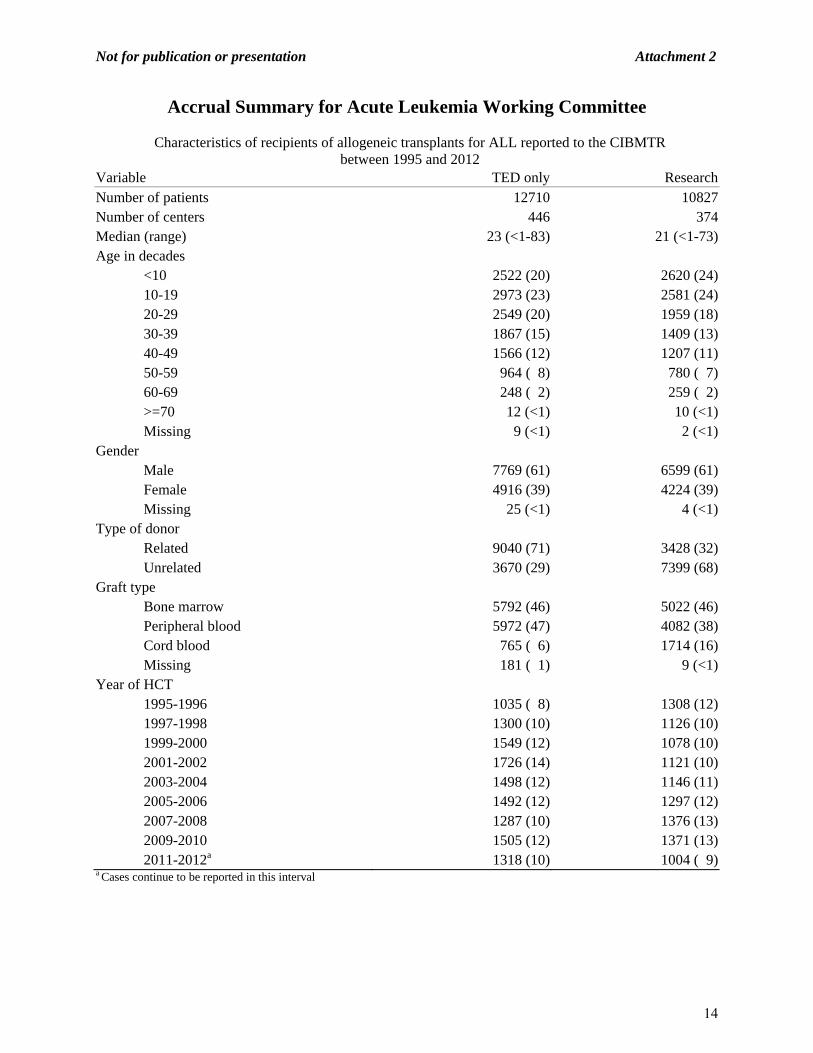
Accrual Summary for Acute Leukemia Working Committee
Characteristics of recipients of allogeneic transplants for ALL reported to the CIBMTR between 1995 and 2012
Variable TED only ResearchNumber of patients 12710 10827Number of centers 446 374Median (range) 23 (<1-83) 21 (<1-73)Age in decades <10 2522 (20) 2620 (24) 10-19 2973 (23) 2581 (24) 20-29 2549 (20) 1959 (18) 30-39 1867 (15) 1409 (13) 40-49 1566 (12) 1207 (11) 50-59 964 ( 8) 780 ( 7) 60-69 248 ( 2) 259 ( 2) >=70 12 (<1) 10 (<1) Missing 9 (<1) 2 (<1)Gender Male 7769 (61) 6599 (61) Female 4916 (39) 4224 (39) Missing 25 (<1) 4 (<1)Type of donor Related 9040 (71) 3428 (32) Unrelated 3670 (29) 7399 (68)Graft type Bone marrow 5792 (46) 5022 (46) Peripheral blood 5972 (47) 4082 (38) Cord blood 765 ( 6) 1714 (16) Missing 181 ( 1) 9 (<1)Year of HCT 1995-1996 1035 ( 8) 1308 (12) 1997-1998 1300 (10) 1126 (10) 1999-2000 1549 (12) 1078 (10) 2001-2002 1726 (14) 1121 (10) 2003-2004 1498 (12) 1146 (11) 2005-2006 1492 (12) 1297 (12) 2007-2008 1287 (10) 1376 (13) 2009-2010 1505 (12) 1371 (13) 2011-2012a 1318 (10) 1004 ( 9)a Cases continue to be reported in this interval
14
Not for publication or presentation Attachment 2
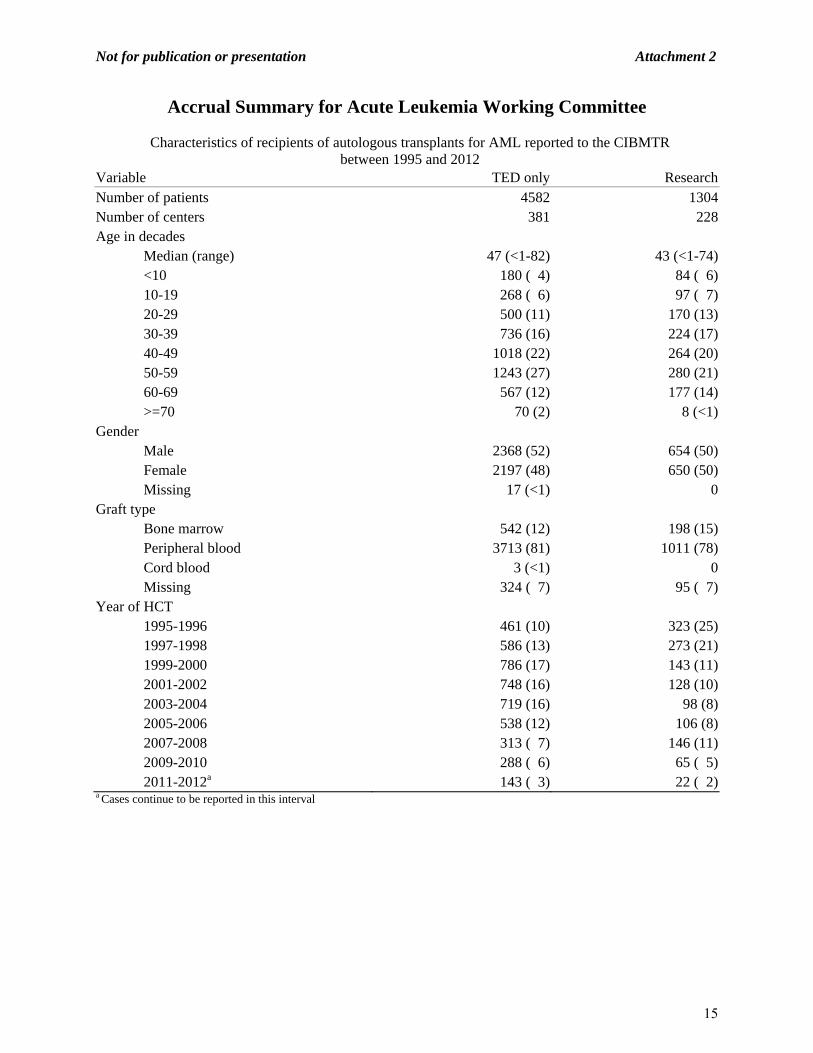
Accrual Summary for Acute Leukemia Working Committee
Characteristics of recipients of autologous transplants for AML reported to the CIBMTR between 1995 and 2012
Variable TED only ResearchNumber of patients 4582 1304Number of centers 381 228Age in decades
Median (range) 47 (<1-82) 43 (<1-74) <10 180 ( 4) 84 ( 6) 10-19 268 ( 6) 97 ( 7) 20-29 500 (11) 170 (13) 30-39 736 (16) 224 (17) 40-49 1018 (22) 264 (20) 50-59 1243 (27) 280 (21) 60-69 567 (12) 177 (14) >=70 70 (2) 8 (<1)Gender Male 2368 (52) 654 (50) Female 2197 (48) 650 (50) Missing 17 (<1) 0Graft type Bone marrow 542 (12) 198 (15) Peripheral blood 3713 (81) 1011 (78) Cord blood 3 (<1) 0 Missing 324 ( 7) 95 ( 7)Year of HCT 1995-1996 461 (10) 323 (25) 1997-1998 586 (13) 273 (21) 1999-2000 786 (17) 143 (11) 2001-2002 748 (16) 128 (10) 2003-2004 719 (16) 98 (8) 2005-2006 538 (12) 106 (8) 2007-2008 313 ( 7) 146 (11) 2009-2010 288 ( 6) 65 ( 5) 2011-2012a 143 ( 3) 22 ( 2)a Cases continue to be reported in this interval
15

Not for publication or presentation Attachment 2
Accrual Summary for Acute Leukemia Working Committee
Characteristics of recipients of autologous transplants for ALL reported to the CIBMTR between 1995 and 2012
Variable TED only ResearchNumber of patients 730 218Number of centers 199 87Age in decades
Median (range) 30 (<1-73) 26 (1-66) <10 63 ( 9) 29 (13) 10-19 118 (16) 44 (20) 20-29 184 (25) 55 (25) 30-39 140 (19) 20 ( 9) 40-49 99 (14) 39 (18) 50-59 93 (13) 24 (11) 60-69 27 ( 4) 7 ( 3) >=70 6 (<1) 0Gender Male 422 (58) 141 (65) Female 308 (42) 77 (35)Graft type Bone marrow 106 (15) 34 (16) Peripheral blood 488 (67) 161 (74) Cord blood 2 (<1) 0 Missing 134 (18) 23 (11)Year of HCT 1995-1996 136 (19) 78 (36) 1997-1998 111 (15) 66 (30) 1999-2000 136 (19) 22 (10) 2001-2002 129 (18) 21 (10) 2003-2004 92 (13) 6 ( 3) 2005-2006 65 ( 9) 11 ( 5) 2007-2008 31 ( 4) 12 ( 6) 2009-2010 21 ( 3) 2 (<1) 2011-2012a 9 ( 1) 0a Cases continue to be reported in this interval
16

Not for publication or presentation Attachment 3
To: Acute Leukemia Working Committee Members
From: Daniel Weisdorf, MD, Scientific Director for the Acute Leukemia WC
RE: 2012-2013 Studies in Progress Summary
Studies in progress R02-09: Evaluation of donor leukocyte infusions to treat relapsed hematologic malignancies after related and unrelated donor myeloablative allogeneic hematopoietic stem cell transplantation (A Loren): The value of related and unrelated donor DLI in treatment of acute leukemia relapsed after allografting will be examined, including the impact of disease status, timing, dose response, and comparative efficacy of the two donor sources. Secondary data collection is required and is underway. The supplemental data collection is finished and data file preparation is underway.
LK04-01: Comparison of autologous and allogeneic hematopoietic stem cell transplantation for patients with acute promyelocytic leukemia (APL)in second complete remission (M Rubinger/M Tallman): This project analyzes outcome of APL in second CR including details of molecular remission prior to transplant. The analysis is finished and currently under manuscript preparation.
LK07-03c: Reduced intensity or non-ablative hematopoietic cell transplantation in older patients with Non-Hodgkin Lymphoma: encouraging survival for patients ≥55 years (B MaClune). This study proposes to analyzes outcome of NHL in older patients who received NMA/RIC conditioning. The draft manuscript has been circulated within writing committee and the PI is currently revising manuscript. LK09-02: Impact of monosomal karyotype in the outcome of hematopoietic cell transplantation for Acute Myeloid Leukemia and Myelodysplasia (M Pasquini/ M Battiwala): The purpose of this study is to identify the impact of high risk cytogenetic subsets: specifically chromosome 7 abnormalities (either monosomy7 or del(7q)) and monosomal karyotype in outcomes for AML and MDS after allogeneic HCT and to evaluate the impact of conditioning intensity in the outcome of patients with AML and monosomal karyotype. The draft protocol is currently being reviewed by PI.
LK10-02: Effect of pre-transplant consolidation chemotherapy on outcomes of RIC Allogeneic transplant for adults with AML in CR1 (E Warlick): The purpose of this study is to (1) compare the outcomes of adults with AML in first remission who have received no consolidation, standard-dose cytarabine consolidation, or high-dose cytarabine consolidation followed by reduced intensity conditioning related or unrelated donor allogeneic stem cell transplantation (HCT) and (2) to determine if there is an exposure threshold (number of cycles of consolidation) that impacts post-transplant outcomes. The draft manuscript has been circulated within WrC and is currently being revised by PI.
17
Not for publication or presentation Attachment 3
LK10-03: The outcome of adults with philadelphia positive acute lymphoblastic leukemia comparing reduced intensity conditioning and myeloablative conditioning allogeneic stem cell transplantation (V Bachanova): The purpose of this study is to (1) to compare outcomes of adults with Ph
+
ALL who received reduced intensity versus myeloablative conditioning followed by sibling or matched unrelated donor HCT; (2) to examine the effect of pre-transplant treatment with tyrosine kinase inhibitors (TKI) on transplant outcomes using RIC and MA conditioning and (3) to examine the prognostic significance of patient, disease and transplant related characteristics on transplant outcomes. Supplemental data collection regarding TKI use is required and funds are available for this purpose. The draft manuscript has been circulated and is currently being revised by PI.
LK11-01: Impact of extramedullary disease on the outcome of allogeneic HCT in AML ((S Goyal/ G Uy): The purpose of this proposal is (1) to describe the outcome of patients undergoing alloHSCT for AML with extramedullary involvement and (2) to assess patient, disease and transplant related factors which influence the outcome of alloHSCT in AML. There are 935 AML patients ≥18 years of age with extramedullary disease prior to HCT reported to the CIBMTR between 1995 and 2010. Protocol development is underway. Studies previously proposed, but not initiated
LK12-01: Chemotherapy versus Allogeneic Hematopoietic Cell Transplantation in Philadelphia negative chromosome negative adult ALL (M Seftel): The purpose of the study is to compare HSCT outcomes of younger adults with Philadelphia chromosome negative (Ph-) Acute Lymphoblastic Leukemia (ALL) in first complete remission (CR1) treated with either allogeneic hematopoietic cell transplantation (alloHCT) or with a pediatric style chemotherapy regimen. LK12-02: FLT3/ITD mutation in acute myeloid leukemia remains a poor prognostic factor compared to conventional cytogenetics with increased risk of relapse and decreased overall survival after allogeneic stem cell transplantation in first complete remission (S Sengsayadeth): The purpose of this study is to (1) To study the prognostic significance of FLT3/ITD mutation in AML in patients receiving allo-HSCT in CR1 and (2) To study the impact of FLT3/ITD mutation on incidence of relapse, disease-free survival (DFS), overall survival (OS) after allo-SCT in CR1.
18

Not for publication or presentation Attachment 4
LK12-01
CHEMOTHERAPY VERSUS ALLOGENEIC HEMATOPOIETIC CELL TRANSPLATATION
IN PHILIADELPHIA NEGATIVE CHROMOSOME NEGATIVE ADULT ALL
DRAFT PROTOCOL
Study Chair: Matthew Seftel, MD, MPH, MRCP, FRCPC
Associate Professor, Department of Internal Medicine University of Manitoba, Winnipeg, CANADA Phone 204 787 2108 Fax 204 786 0196 Email: [email protected]
1.0 OBJECTIVES:
1.1 To compare the overall survival (OS), disease-free survival (DFS), and treatment-related mortality (TRM) of younger adults with Philadelphia chromosome negative (Ph-) Acute Lymphoblastic Leukemia (ALL) in first complete remission (CR1) treated with either allogeneic hematopoietic cell transplantation (alloHCT) or with a pediatric style chemotherapy regimen.
1.2 To identify predictors of OS, DFS, and TRM in this population of adults with ALL.
2.0 SCIENTIFIC JUSTIFICATION:
In Ph- adult ALL, conventional multi-agent chemotherapy protocols result in high remission rates, but long-term survival can be maintained in only about 40-45% of patients1,2. These results are in contrast to the much more gratifying outcomes seen in children, adolescents and young adults treated within pediatric clinical trials consortia3,4.
In adults who achieve CR1, two major therapeutic strategies have been increasingly used in order to maintain CR and improve long-term survival. Firstly, alloHCT may be offered. AlloHCT in CR1 is thought to offer a survival advantage over ongoing standard chemotherapy. Phase III trials and meta-analyses suggest that related donor alloHCT is a more efficacious, albeit more toxic therapy for adult Ph- ALL in CR11,5. Although the published phase III trials were restricted to related donor (RD) alloHCT, recent observational data suggest that unrelated donor (UD) alloHCT produces similar outcomes to RD alloHCT6,7. Thus, alloHCT in CR1 is likely to be superior to a conventional chemotherapy approach, regardless of whether suitably matched RDs or UDs are used.
The second strategy directed at adult ALL patients is the adoption of pediatric chemotherapy protocols. These “pediatric inspired” regimens are more dose intense than traditional adult chemotherapy approaches, particularly with respect to non-myelosuppressive agents such as corticosteroids, vincristine, and L-asparaginase. Single arm studies suggest that pediatric
19
Not for publication or presentation Attachment 4
regimens offer excellent outcomes in younger adults, with long-term OS in 60-68%8,9. Thus, it is plausible that pediatric inspired chemotherapy regimens are at least as effective, if not superior to alloHCT. However, these two approaches (alloHCT and pediatric style chemotherapy) have never been directly compared to one another. We thus plan to compare outcomes in a cohort of younger adults with Ph- ALL who received alloHCT in CR1 to a similar population of younger adults with ALL who received a uniform, intensive pediatric regimen.
3.0 STUDY POPULATION:
1. All adult patients (aged 18-50) with Ph- ALL in CR1 registered with the CIBMTR who received a myeloablative alloHCT from a related or unrelated donor between June 1, 2002 and December 31, 2010. Recipients of umbilical cord transplants will be excluded.
2. All Ph- patients enrolled in the two consecutively conducted Dana-Farber Cancer Institute
(DFCI) Adult ALL consortium phase II trials between June 1 2002 and December 31 2010 who achieved CR1 (DFCI 01-0175 and 06-254). Patients who received alloHCT in CR1 will be excluded.
4.0 OUTCOMES:
Primary: 4.1 Overall survival: time to death. Patients are censored at time of last follow-up Secondary: 4.2 Disease-free survival: time to treatment failure (death or relapse). Patients are censored
at time of last follow-up. 4.3 Treatment-related mortality: time to death without evidence of leukemia recurrence. 4.4 Relapse: time to onset of leukemia recurrence. Event will be summarized by the
cumulative incidence estimate with treatment related mortality as a competing risk. 4.5 Acute GVHD: Occurrence of grade II, III and/or IV skin, gastrointestinal or liver
abnormalities fulfilling the Consensus criteria of acute GVHD. 4.6 Chronic GVHD: Occurrence of symptoms in any organ system fulfilling the
diagnostic criteria of chronic GVHD
5.0 VARIABLES TO BE ANALYZED: All patients:
- Date of ALL diagnosis - Date of birth - Age at diagnosis: continuous; by decades - Gender: male vs. female - Karnofsky score: <90% vs. ≥90% - FAB classification: T-cell vs. B-cell vs. Unclassified - WBC,x109/L: <30 vs. 30-100 vs. >100 - Time to achieve CR1: <4 weeks vs. 4-8 weeks vs. >8 weeks - Number of chemotherapy cycles required to achieve CR1 (1, 2, >2) - Extramedullary disease at diagnosis: CNS (yes/no), testis (yes/no), other (yes/no) - Cytogenetic abnormalities: t(4;11), hypodiploidy or near triploidy, complex cytogenetics
(>5 abnormalities) vs. none vs. not known vs. other abnormalities
20

Not for publication or presentation Attachment 4
- Cranial or spinal irradiation as part of intial therapy (yes/no) - Date of last follow-up - Date of relapse - Death (yes/no) - Primary cause of death
Specific to HCT cohort:
- Time from diagnosis to transplant, months: <3 vs. >3 - Time from remission to transplant, months: <3 vs. >3 - Conditioning regimen: TBI used; yes vs. no - Type of donor: HLA-identical sibling vs. matched unrelated vs. partially matched
unrelated vs. mismatched unrelated - Donor age: continuous - Donor-recipient gender match: F-M vs. others - Donor-recipient CMV status: -/- vs. others - Source of stem cells: BM vs. PBSC - Year of transplant - GVHD prophylaxis: ex vivo T cell depletion vs. CsA+MTX vs. tacrolimus and
methotrexate vs mycophenolate mofetil + CsA/tacro vs sirolimus - Steroids as GVHD prophylaxis: yes/no - ATG given as part of conditioning regimen or GVHD prophylaxis: no vs. yes - Prior autologous transplant: no vs. yes - Post-transplant therapy: DLI (yes/no); chemotherapy (yes/no); intrathecal
chemotherapy (yes/no) - Reason for DLI: relapse vs. mixed chimerism - Acute GVHD: grade I-IV - Chronic GVHD: maximum grade (limited vs. extensive) and severity (mild; moderate;
severe) Specific to Chemotherapy (DFCI) cohort
- Proportion completing intensification phase (N, %) - Proportion completing maintenance chemotherapy phase (N, %)
6. 0 STUDY DESIGN:
Clinical and disease variables of the two cohorts will be compared by the chi-square statistic or Fisher’s exact test for categorical variables and the Kruskal-Wallis test for continuous variables. Median follow-up time will be calculated utilizing the Kaplan-Meier method. TRM will be defined as death occurring during CR1 as calculated by the cumulative incidence estimate, with relapse as the competing risk. Relapse will be defined as morphologic leukemia recurrence at any site by the cumulative incidence estimate, with death in CR1 as the competing risk. For OS and DFS, patients will be censored at death in CR1 or surviving in continuous CR at last contact. For OS, death from any cause will be considered an event. For DFS, relapse or death will be considered an event.
21
Not for publication or presentation Attachment 4
InthecomparisonofHCTvs.non‐HCTcohorts,adifferenceintimetotreatmentisapotentialsourceofbias.HCTrecipientsmustsurvivelongenoughtoundergoHCT.Thus,HCTrecipientsmayrepresentacohortwithaninherentlybetteroutcome.Toaddressthis,theanalysiswillbelimitedtopatientswhoremainedinCR1foratleastthreemonthsbeforetransplantation10.Toadjustfordifferencesinbaselinecharacteristics,multivariateCoxproportionalhazardsregressionmodelswillbeused.ResultswillbeexpressedashazardratiosofeachoutcomeafterHCTvs.afterchemotherapy.P‐valueswillbe2‐sided.
7.0 REFERENCES:
1. Goldstone AH, Richards SM, Lazarus HM, et al. In adults with standard-risk acute lymphoblastic leukemia, the greatest benefit is achieved from a matched sibling allogeneic transplantation in first complete remission, and an autologous transplantation is less effective than conventional consolidation/maintenance chemotherapy in all patients: final results of the International ALL Trial (MRC UKALL XII/ECOG E2993).Blood. 2008 Feb 15;111(4):1827-33.
2. Thomas DA, O'Brien S, Cortes J, et al. Outcome with the hyper-CVAD regimens in lymphoblastic lymphoma.Blood. 2004 Sep 15;104(6):1624-30.
3. Silverman LB, Stevenson KE, O'Brien JE et al. Long-term results of Dana-Farber Cancer Institute ALL Consortium protocols for children with newly diagnosed acute lymphoblastic leukemia (1985-2000).Leukemia. 2010 Feb;24(2):320-34.
4. Barry E, DeAngelo DJ, Neuberg D, et al. Favorable outcome for adolescents with acute lymphoblastic leukemia treated on Dana-Farber Cancer Institute Acute Lymphoblastic Leukemia Consortium Protocols.J Clin Oncol. 2007 Mar 1;25(7):813-9.
5. Pidala J, Djulbegovic B, Anasetti C, Kharfan-Dabaja M, Kumar A.Cochrane Database Syst Rev. 2011 Oct 5;(10):CD008818.Allogeneic hematopoietic cell transplantation for adult acute lymphoblastic leukemia (ALL) in first complete remission.
6. Oliansky DM, Larson RA, Weisdorf D, Dillon H, Ratko TA, Wall D, McCarthy PL Jr, Hahn T. The Role of Cytotoxic Therapy with Hematopoietic Stem Cell Transplantation in the Treatment of Adult Acute Lymphoblastic Leukemia: Update of the 2006 Evidence-Based Review. Biol Blood Marrow Transplant.2011 Jul 29. [Epub ahead of print]
7. Marks DI, Perez WS, He W et al. Unrelated donor transplants in adults with Philadelphia-negative acute lymphoblastic leukemia in first complete remission. Blood, July 15, 2008; 112(2): 426 - 434.
8. DeAngelo DJ, Dahlberg S, Silverman LB, et al. A Multicenter Phase II Study Using a Dose Intensified Pediatric Regimen in Adults with Untreated Acute Lymphoblastic Leukemia.Blood (ASH Annual Meeting Abstracts), Nov 2007; 110: 587.
9. Huguet F, Leguay T, Raffoux E, et al.Pediatric-inspired therapy in adults with Philadelphia chromosome-negative acute lymphoblastic leukemia: the GRAALL-2003 study.J Clin Oncol. 2009 Feb 20;27(6):911-8.
10. Farag SS, Maharry K, Zhang MJ, Pérez WS, George SL, Mrózek K, Dipersio J, Bunjes DW, Marcucci G, Baer MR, Cairo M, Copelan E, Cutler CS, Isola L, Lazarus HM, Litzow MR, Marks DI, Ringdén O, Rizzieri DA, Soiffer R, Larson RA, Tallman MS, Bloomfield CD, Weisdorf DJ; on behalf of the Acute Leukemia Committee of the Center for International Blood and Marrow Transplant Research and Cancer and Leukemia Group B. Comparison of Reduced-Intensity Hematopoietic Cell Transplantation with Chemotherapy in Patients Age 60-70 Years with Acute Myelogenous Leukemia in First Remission.Biol Blood Marrow Transplant.2011 Jun 21. [Epub ahead of print]
22
Not for publication or presentation Attachment 4
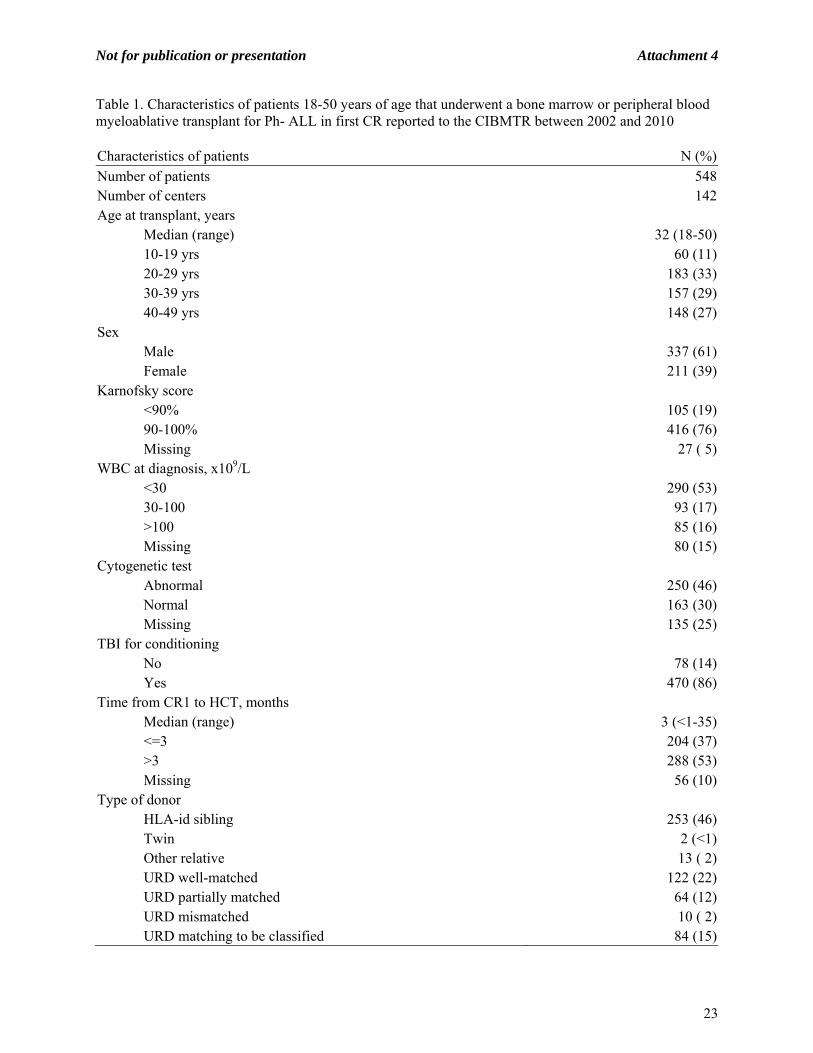
Table 1. Characteristics of patients 18-50 years of age that underwent a bone marrow or peripheral blood myeloablative transplant for Ph- ALL in first CR reported to the CIBMTR between 2002 and 2010 Characteristics of patients N (%)Number of patients 548Number of centers 142Age at transplant, years
Median (range) 32 (18-50)10-19 yrs 60 (11)20-29 yrs 183 (33)30-39 yrs 157 (29)40-49 yrs 148 (27)
Sex Male 337 (61)Female 211 (39)
Karnofsky score <90% 105 (19)90-100% 416 (76)Missing 27 ( 5)
WBC at diagnosis, x109/L <30 290 (53)30-100 93 (17)>100 85 (16)Missing 80 (15)
Cytogenetic test Abnormal 250 (46)Normal 163 (30)Missing 135 (25)
TBI for conditioning No 78 (14)Yes 470 (86)
Time from CR1 to HCT, months Median (range) 3 (<1-35)<=3 204 (37)>3 288 (53)Missing 56 (10)
Type of donor HLA-id sibling 253 (46)Twin 2 (<1)Other relative 13 ( 2)URD well-matched 122 (22)URD partially matched 64 (12)URD mismatched 10 ( 2)URD matching to be classified 84 (15)
23

Not for publication or presentation Attachment 4
Table 1. Continued. Characteristics of patients N (%)D-R sex match
M-M 206 (38)M-F 104 (19)F-M 101 (18)F-F 91 (17)Missing 46 ( 8)
D-R CMV status +/+ 180 (33)+/- 58 (11)-/+ 126 (23)-/- 126 (23)Missing 58 (11)
Graft type Bone marrow 176 (32)Peripheral blood 372 (68)
Year of HCT 2001-2002 57 (10)2003-2004 144 (26)2005-2006 182 (33)2007-2008 105 (19)2009-2010 60 (11)
ATG or Campath ATG alone 94 (17)Campath alone 11 ( 2)No ATG or Campath 443 (81)
GVHD Prophylaxis No GVHD prophylaxis 17 ( 3)Ex vivo T-cell depletion alone 4 ( 1)Ex vivo T-cell depletion + post-tx immune suppression 5 ( 1)CD34 selection +- post-tx immune suppression 6 (1)FK506 + MMF +- others 32 ( 6)FK506 + MTX +- others (except MMF) 189 (34)FK506 + others (except MTX, MMF) 20 ( 4)FK506 alone 3 ( 1)CSA + MMF +- others (except FK506) 10 ( 2)CSA + MTX +- others (except FK506, MMF) 240 (44)CSA + others (except FK506, MTX, MMF) 4 ( 1)CSA alone 11 ( 2)Other GVHD prophylaxis 7 ( 1)
Median (range) FU of survivors, months 41 (3-100)
24

Not for publication or presentation Attachment 4
Time from CR1 to transplant by patient age: Patient age <=3 months >3 months Missing Total10-19 yrs 24 (12) 27 (9) 9 (16) 6020-29 yrs 72 (35) 101 (35) 10 (18) 18330-39 yrs 51 (25) 86 (30) 20 (36) 15740-49 yrs 57 (28) 74 (26) 17 (30) 148Total 204 288 56 548
25

Not for publication or presentation Attachment 5
Figure 1a. DFS
Days
Pro
bab
ility
of
DF
S
0 500 1000 1500 2000 25000
20
40
60
80
100
FLT3/ITD- (2 year 63.5%)
FLT3/ITD+ (2 year 18.7%)
p=0.0027
LK12-02
ALLOGENIC STEM CELL TRANSPLATATION FOR FLT3/ITD POSITIVE ACUTE
MYELOID LUEKEMIA IN CR1
DRAFT PROTOCOL
1. HYPOTHESIS: FLT3/ITD mutation in acute myeloid leukemia remains a poor prognostic factor compared to
conventional cytogenetics with increased risk of relapse and decreased overall survival after allogeneic stem cell transplantation in first complete remission.
2. OBJECTIVES/SPECIFIC AIMS:
2.1 To study the prognostic significance of fms-like tyrosine kinase 3/internal tandem mutation (FLT3/ITD) mutation in acute myeloid leukemia (AML) in patients receiving allogeneic stem cell transplantation (allo-SCT) in complete remission 1 (CR1)
2.2 To study the impact of FLT3/ITD mutation on incidence of relapse, disease-free survival (DFS), overall survival (OS) after allo-SCT in CR1
2.3 To study the impact of prior chemotherapy, including the effect of consolidation 2.4 To study the impact of NPM1 mutation in patients with FLT3/ITD mutation
3. SCIENTIFIC JUSTIFICATION:
Survival of patients with AML, particularly in younger patients, has improved in recent years due to improved understanding of disease biology, post remission therapies, and supportive care. AML, however, remains difficult to treat as many patients will still ultimately relapse and die of their disease. This is particularly true in AML patients with identified FLT3/ITD molecular mutations, which typically confers a poor prognosis. Oftentimes, these patients are referred for early allo-SCT in hopes of overcoming this poor prognostic factor, although the efficacy of this strategy remains unclear. FLT3 is a transmembrane protein that is significant in the survival of hematopoietic stem cells upon activation, and internal tandem duplication, first described in 1996 by Nakao et al, results in constitutive activation of the FLT3 gene in AML patients.1 The FLT3/ITD occurs in about one quarter of all patients diagnosed with AML.2 Although complete remission rates are similar in patients with FLT3/ITD compared to those with FLT3-wild type (WT) with conventional chemotherapy, the risk of relapse has been noted to be markedly higher in FLT3/ITD+ patients when treated with chemotherapy alone.1,3,4 Median survival time after relapse is very poor and
26
Not for publication or presentation Attachment 5
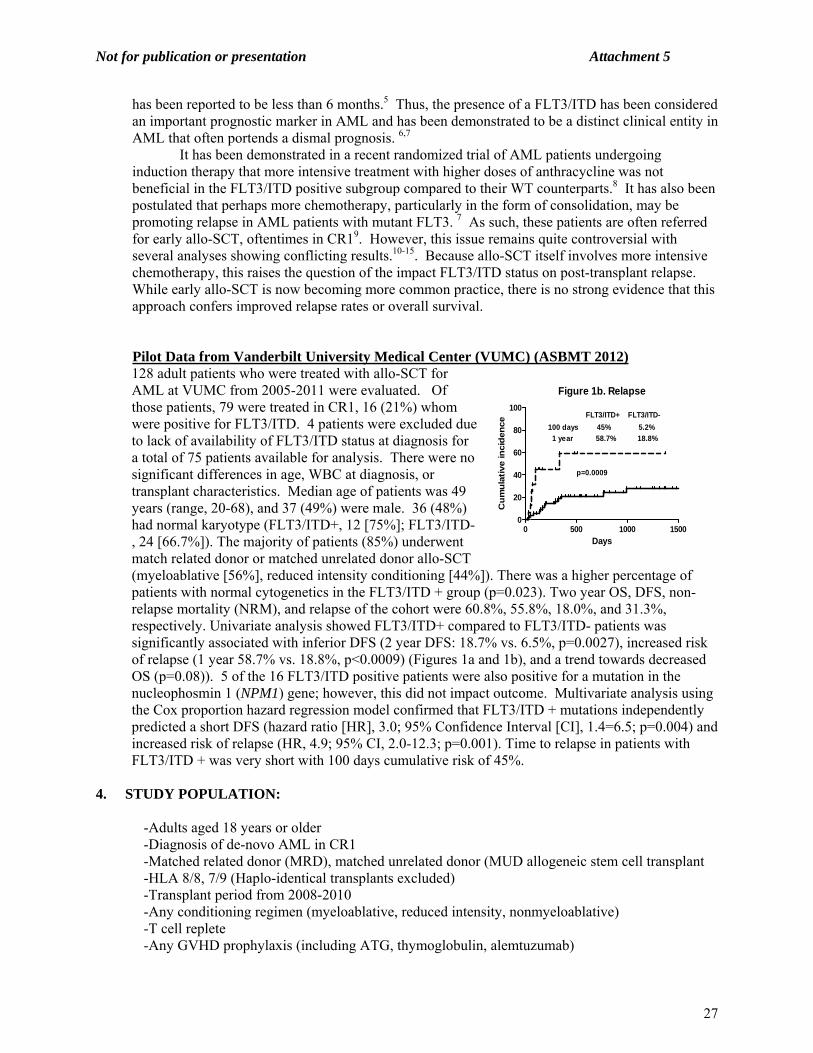
has been reported to be less than 6 months.5 Thus, the presence of a FLT3/ITD has been considered an important prognostic marker in AML and has been demonstrated to be a distinct clinical entity in AML that often portends a dismal prognosis. 6,7 It has been demonstrated in a recent randomized trial of AML patients undergoing induction therapy that more intensive treatment with higher doses of anthracycline was not beneficial in the FLT3/ITD positive subgroup compared to their WT counterparts.8 It has also been postulated that perhaps more chemotherapy, particularly in the form of consolidation, may be promoting relapse in AML patients with mutant FLT3. 7 As such, these patients are often referred for early allo-SCT, oftentimes in CR19. However, this issue remains quite controversial with several analyses showing conflicting results.10-15. Because allo-SCT itself involves more intensive chemotherapy, this raises the question of the impact FLT3/ITD status on post-transplant relapse. While early allo-SCT is now becoming more common practice, there is no strong evidence that this approach confers improved relapse rates or overall survival.
Pilot Data from Vanderbilt University Medical Center (VUMC) (ASBMT 2012) 128 adult patients who were treated with allo-SCT for AML at VUMC from 2005-2011 were evaluated. Of those patients, 79 were treated in CR1, 16 (21%) whom were positive for FLT3/ITD. 4 patients were excluded due to lack of availability of FLT3/ITD status at diagnosis for a total of 75 patients available for analysis. There were no significant differences in age, WBC at diagnosis, or transplant characteristics. Median age of patients was 49 years (range, 20-68), and 37 (49%) were male. 36 (48%) had normal karyotype (FLT3/ITD+, 12 [75%]; FLT3/ITD-, 24 [66.7%]). The majority of patients (85%) underwent match related donor or matched unrelated donor allo-SCT (myeloablative [56%], reduced intensity conditioning [44%]). There was a higher percentage of patients with normal cytogenetics in the FLT3/ITD + group (p=0.023). Two year OS, DFS, non-relapse mortality (NRM), and relapse of the cohort were 60.8%, 55.8%, 18.0%, and 31.3%, respectively. Univariate analysis showed FLT3/ITD+ compared to FLT3/ITD- patients was significantly associated with inferior DFS (2 year DFS: 18.7% vs. 6.5%, p=0.0027), increased risk of relapse (1 year 58.7% vs. 18.8%, p<0.0009) (Figures 1a and 1b), and a trend towards decreased OS (p=0.08)). 5 of the 16 FLT3/ITD positive patients were also positive for a mutation in the nucleophosmin 1 (NPM1) gene; however, this did not impact outcome. Multivariate analysis using the Cox proportion hazard regression model confirmed that FLT3/ITD + mutations independently predicted a short DFS (hazard ratio [HR], 3.0; 95% Confidence Interval [CI], 1.4=6.5; p=0.004) and increased risk of relapse (HR, 4.9; 95% CI, 2.0-12.3; p=0.001). Time to relapse in patients with FLT3/ITD + was very short with 100 days cumulative risk of 45%.
4. STUDY POPULATION: -Adults aged 18 years or older -Diagnosis of de-novo AML in CR1 -Matched related donor (MRD), matched unrelated donor (MUD allogeneic stem cell transplant -HLA 8/8, 7/9 (Haplo-identical transplants excluded) -Transplant period from 2008-2010 -Any conditioning regimen (myeloablative, reduced intensity, nonmyeloablative) -T cell replete -Any GVHD prophylaxis (including ATG, thymoglobulin, alemtuzumab)
Figure 1b. Relapse
Days
Cu
mu
lati
ve in
cid
en
ce
0 500 1000 15000
20
40
60
80
100FLT3/ITD+ FLT3/ITD-
100 days 45% 5.2%
1 year 58.7% 18.8%
p=0.0009
27

Not for publication or presentation Attachment 5
5. OUTCOMES:
5.1 Relapse Incidence: Relapse will be defined as time to onset of recurrent FLT3/ITD AML through morphologic evidence in bone marrow or extramedullary sites. If data is available, time to molecular recurrence will also be evaluated and studied in the context of predicting relapse. Event will be summarized by cumulative incidence (CI) estimate with transplant related mortality (TRM) as a competing risk. 5.2 Disease Free Survival (DFS): DFS will be defined as time to relapse or death from any cause 5.3 Overall Survival (OS): Will be defined as to time of death, with patients censored at last follow-up. 5.4 Transplant related mortality: Will be defined as time to death without evidence of disease presence. Cumulative incidence estimate with relapse will be a competing risk. 5.5 GVHD: Incidence of acute GVHD based on Glucksberg staging of skin, gastrointestinal, and liver disease. Chronic GVHD incidence as well as classification of limited or extensive will also be analyzed.
6. VARIABLES TO BE ANALYZED:
Patient related (at time of transplant): -Age at transplant (continuous) -Gender (Male/Female) -Karnofsky Performance Status: <90% vs. >90% -WBC at diagnosis (continuous) -Transplant Co-morbidity Index Disease related: -FLT3/ITD status at diagnosis -NPM1 status at diagnosis -Prior chemotherapy treatments prior to transplant, including number of consolidation
therapies -Cytogenetics, including monosomal karyotype
Transplant related: -Conditioning regimens: Myeloablative (MA) vs. Others {Reduced intensity conditioning (RIC)
and nonmyeloablative (NMA)} -TBI Yes vs. No
-Donor age (continuous) -Related vs. Unrelated -Donor recipient gender (M-M vs. M-F vs. F-M vs. F-F) -HLA matching and degree of match (8/8, 7/9) -Source of stem cells (bone marrow vs. peripheral blood stem cell -CD34 cell dose X 106/kg -CD3 cell dose X 106/kg -Year of transplant
-GVHD prophylaxis: MTX based vs. Non MTX based -In vivo T cell depletion Yes vs. No
28
Not for publication or presentation Attachment 5
Post-transplant: -Acute GVHD: none vs. II-IV, I-II vs. III-IV -GVHD beyond day 100: late acute, chronic GVHD (limited or extensive) -Relapse: yes/no (molecular, histologic, extra-medullary) -NRM: yes/no
7. DATA COLLECTION:
Data collection will be per standard data collection sheets. Furthermore, given the small number of FLT3/ITD+ AML patients, we may elect to reach out to the individual transplant centers to identify these specific patients to perform more in-depth chart review of the above variables if they are not available in the CIBMTR database.
8. STUDY DESIGN:
All AML patients receiving allo-SCT in CR1 with FLT3/ITD information available in the designated time period will be included in the analysis. Descriptive tables of patient-, disease-, and transplant related factors will be prepared. The tables will list median and range for continuous variables and percent of total for categorical variables. Characteristics of patients will be compared using the chi-square test for categorical variables and the Wilcoxon two-sample test for continuous variables. Outcomes will be defined as above. Comparing the outcomes between FLT3-WT and FLT3/ITD groups transplant groups will require adjustment of baseline patient characteristics. Time to transplant will not need to be adjusted as all patients will be in CR1. To adjust for differences in the baseline characteristics, Cox proportional hazards regression will be used. Probability of DFS and OS will be calculated using the Kaplan-Meier estimator. Comparison of survival curves will be done using the log-rank test.
29

Not for publication or presentation Attachment 5
REFERENCES:
1. Nakao M, Yakota S, Iwai T. Internal tandem duplication of the flt3 gene found in acute myeloid leukemia. Leukemia. 1996;10:1911-1918.
2. Levis M, Small D. FLT3: ITDoes matter in leukemia. Leukemia. 2003;17(9):1738-1752. 3. Yanada M, Matsuo K, Suzuki T, Kiyoi H, Naoe T. Prognostic significance of FLT3 internal
tandem duplication and tyrosine kinase domain mutations for acute myeloid leukemia: a meta-analysis. Leukemia. 2005;19(8):1345-1349.
4. Frohling S, Schlenk RF, Breitruck J, et al. Prognostic significance of activating FLT3 mutations in younger adults (16 to 60 years) with acute myeloid leukemia and normal cytogenetics: a study of the AML Study Group Ulm. Blood. 2002;100(13):4372-4380.
5. Ravandi F, Kantarjian H, Faderl S, et al. Outcome of patients with FLT3-mutated acute myeloid leukemia in first relapse. Leuk Res. 2010;34(6):752-756.
6. Kottaridis PD, Gale RE, Frew ME, et al. The presence of a FLT3 internal tandem duplication in patients with acute myeloid leukemia (AML) adds important prognostic information to cytogenetic risk group and response to the first cycle of chemotherapy: analysis of 854 patients from the United Kingdom Medical Research Council AML 10 and 12 trials. Blood. 2001;98(6):1752-1759.
7. Levis M. FLT3/ITD AML and the law of unintended consequences. Blood. 2011;117(26):6987-6990.
8. Fernandez HF, Sun Z, Yao X, et al. Anthracycline dose intensification in acute myeloid leukemia. N Engl J Med. 2009;361(13):1249-1259.
9. Savani BN. Transplantation in AML CR1. Blood. 2010;116(11):1822-1823. 10. Bornhauser M, Illmer T, Schaich M, Soucek S, Ehninger G, Thiede C. Improved outcome after
stem-cell transplantation in FLT3/ITD-positive AML. Blood. 2007;109(5):2264-2265; author reply 2265.
11. Meshinchi S, Arceci RJ, Sanders JE, et al. Role of allogeneic stem cell transplantation in FLT3/ITD-positive AML. Blood. 2006;108(1):400; author reply 400-401.
12. Meshinchi S, Alonzo TA, Stirewalt DL, et al. Clinical implications of FLT3 mutations in pediatric AML. Blood. 2006;108(12):3654-3661.
13. Gale RE, Hills R, Kottaridis PD, et al. No evidence that FLT3 status should be considered as an indicator for transplantation in acute myeloid leukemia (AML): an analysis of 1135 patients, excluding acute promyelocytic leukemia, from the UK MRC AML10 and 12 trials. Blood. 2005;106(10):3658-3665.
14. Koreth J, Schlenk R, Kopecky KJ, et al. Allogeneic stem cell transplantation for acute myeloid leukemia in first complete remission: systematic review and meta-analysis of prospective clinical trials. JAMA. 2009;301(22):2349-2361.
15. Schlenk RF, Dohner K, Krauter J, et al. Mutations and treatment outcome in cytogenetically normal acute myeloid leukemia. N Engl J Med. 2008;358(18):1909-1918.
16. Dezern AE, Sung A, Kim S, et al. Role of Allogeneic Transplantation for FLT3/ITD Acute Myeloid Leukemia: Outcomes from 133 Consecutive Newly Diagnosed Patients from a Single Institution. Biol Blood Marrow Transplant. 2011.
30

Not for publication or presentation Attachment 5
Table 1. Characteristics of patients ≥18 years of age that underwent an HLA-identical sibling or well-matched unrelated transplant for AML FLT-3+ in first complete remission reported to the CIBMTR between 2008 and 2010 Characteristics of patients N (%)
Number of patients 118
Number of centers 50
Age at transplant, years
Median (range) 48 (18-71)
10-19 yrs 4 ( 3)
20-29 yrs 13 (11)
30-39 yrs 13 (11)
40-49 yrs 36 (31)
50-59 yrs 40 (34)
>=60 yrs 12 (10)
Sex
Male 59 (50)
Female 59 (50)
Karnofsky score
<90% 39 (33)
90-100% 72 (61)
Missing 7 ( 6)
Comorbidity index
0 54 (46)
1 13 (11)
2 22 (19)
3 10 ( 8)
4 9 ( 8)
5 4 ( 3)
6 3 ( 3)
7 3 ( 3)
31

Not for publication or presentation Attachment 5
Table 1. Continued.
Characteristics of patients N (%)
Type of AML
denovo AML 106 (90)
secondary AML 12 (10)
WBC at diagnosis, x109/L
<30 49 (42)
30-100 43 (36)
>100 21 (18)
Missing 5 ( 4)
Cytogenetic test
Abnormal 36 (31)
Normal 78 (66)
Missing 4 ( 3)
Conditioning regimen
MA 94 (80)
RIC 18 (15)
NMA 4 ( 3)
TBD 2 ( 2)
TBI for conditioning
No 66 (56)
Yes 52 (44)
Type of donor
HLA-id sibling 58 (49)
URD well-matched 60 (51)
D-R sex match
M-M 17 (14)
M-F 25 (21)
F-M 10 ( 8)
F-F 8 ( 7)
Missing 58 (49)
D-R CMV status
+/+ 19 (16)
+/- 8 ( 7)
-/+ 19 (16)
-/- 15 (13)
Missing 57 (48)
32

Not for publication or presentation Attachment 5
Table 1. Continued
Characteristics of patients N (%)
Graft type
Bone marrow 14 (12)
Peripheral blood 103 (87)
Cord blood 1 ( 1)
Year of HCT
2008 34 (29)
2009 34 (29)
2010 50 (42)
ATG or Campath
ATG alone 26 (22)
Campath alone 2 ( 2)
No ATG or Campath 90 (76)
GVHD Prophylaxis
No GVHD prophylaxis 2 ( 2)
CD34 selection + post-tx immune supression 1 ( 1)
FK506 + MMF +- others 20 (17)
FK506 + MTX +- others (except MMF) 74 (63)
FK506 + others (except MTX, MMF) 8 ( 7)
FK506 alone 4 ( 3)
CSA + MMF +- others (except FK506) 6 ( 5)
CSA + MTX +- others (except FK506, MMF) 3 ( 3)
Median (range) FU of survivors, months 13 (5-38)* There are an additional 32 unrelated donor patients where the D-R HLA matching needs to be classified: The matched URD patients from this group will be added to the above study population. * 409/1133 (36%) patients are missing FLT3 information.
Frequency | FLT3- | FLT3+ |Missing | Total | | | | -----------------+--------+--------+--------+ HLA-id sibling | 262 | 58 | 163 | 483 -----------------+--------+--------+--------+ URD well-matched | 186 | 60 | 133 | 379 -----------------+--------+--------+--------+ URD matching to | 126 | 32 | 113 | 271 be classified | | | | -----------------+--------+--------+--------+ Total 574 150 409 1133
33
Not for publication or presentation Attachment 6
Study Proposal 1012-02 Study Title: To determine whether in vivo T cell depletion with Alemtuzumab affects outcome after myeloablative TBI- based conditioning in children and young adults who received unrelated donor transplants for acute myeloid leukaemia (AML). Sujith Samarasinghe, PhD, FRCPath, Paediatric Haematology, Newcastle Upon Tyne, UK, [email protected] Paul Veys, FRCPCH, FRCPath, Paediatric BMT, Great Ormond Street Hospital, London, UK, [email protected] Mary Eapen, MD,MS, CIBMTR, Wisconsin, Milwaukee, WI, [email protected] Primary Hypothesis: Children and adolescents/young adults (AYA) who have undergone myeloablative unrelated donor HSCT for AML have reduced GVHD especially chronic GVHD with in vivo T cell depletion with Alemtuzumab compared to T cell replete or ATG based regimens without affecting leukaemia free survival (LFS) or non relapse mortality (NRM). Specific Aims:
1. To compare in children and AYA who have undergone a myeloablative HSCT for AML, the incidence of acute GVHD and chronic GVHD between regimens with in vivo T cell depletion using Alemtuzumab/ATG or T cell replete.
2. To compare in children and AYA who have undergone a myeloablative HSCT for AML overall survival (OS) and LFS between regimens with in vivo T cell depletion using Alemtuzumab/ATG or T cell replete.
3. To compare in children and AYA who have undergone a myeloablative HSCT for AML, haematopoeitic recovery and day 100 / 1 year transplant related mortality (TRM) between regimens containing in vivo T cell depletion using Alemtuzumab/ATG or T cell replete.
4. To compare in children and AYA who have undergone a myeloablative HSCT for AML, the incidence of viral infections between regimens containing in vivo T cell depletion using alemtuzumab/ATG or T cell replete.
5. To determine transplant outcomes for AYA who have undergone a myeloablative unrelated HSCT for AML.
Scientific Justification: The optimal conditioning strategy in children and AYA undergoing a myeloablative unrelated donor HSCT for AML is unknown. Controversy exists on the optimal conditioning regimen as well as the effectiveness of in vivo T cell depletion strategies. Both TBI and non TBI based conditioning regimens are currently used in paediatric and AYA AML. A recent CIBMTR analysis showed similar outcomes after TBI and non TBI based myeloablative T cell replete unrelated donor HSCT for myeloid malignancies (1) However, GVHD rates were high after myeloablative T cell replete unrelated donor HSCT using TBI based regimens; rates of grade 2-4 acute were approximately 50-60 % and chronic GVHD were 40-50 % (1). GVHD in particular chronic GVHD significantly impacts on long term morbidity and mortality. One approach to counter this, involves in vivo T cell depletion with alemtuzumab or ATG. Whilst this is very effective at reducing GVHD rates, there remains the concern that in vivo T cell depletion leads to an increased risk of relapse and infectious mortality. Prospective and retrospective studies have shown mixed results regarding the efficacy of in vivo T cell depletion. Two prospective randomised studies comparing ATG versus T cell replete in myeloablative unrelated donor HSCT, demonstrated reduced acute and chronic GVHD with in vivo T cell depletion without affecting LFS (2-4). However, there was no difference in OS in part due to an increase in
34

Not for publication or presentation Attachment 6
infectious mortality in the ATG arm (4). Similarly a retrospective analysis comparing in vivo T cell deplete (either ATG or Alemtuzumab) with T cell replete myeloablative unrelated donor HSCT for paediatric ALL demonstrated reduced acute and chronic GVHD with in vivo T depletion (5). Chronic GVHD was lowest with alemtuzumab, but again there was no difference in LFS and OS between the three arms. In contrast, retrospective analyses suggest that reduced intensity conditioning (RIC) incorporating in vivo T cell depletion, whilst reducing acute and chronic GVHD, do so at the expense of an increase in relapse risk (6). A preliminary EBMT retrospective analysis comparing ATG versus alemtuzumab for adult AML in RIC HSCTs also showed worse LFS and OS wIth alemtuzumab. (7) These studies suggest that the efficacy and safety of in vivo T cell depletion in unrelated donor HSCT for AML depend on the intensity of the preparative regimen. The aim of this retrospective combined CIBMTR/BSBMT analysis is to determine whether incorporation of in vivo T cell depletion with alemtuzumab affects outcome for paediatric and AYA AML after myeloablative conditioning, compared to T cell replete and ATG based regimens. A secondary aim of the analysis is to determine the outcome of the AYA population following unrelated donor HSCT for AML. Outcomes for the AYA population in AML are often incorporated into larger group analyses and thus little specific information for this group has been published. The definition of an AYA varies, but for the purpose this study will be between 15-39 years as defined by the Adolescent and Young Adult Oncology Peer Review Group (15-21 older adolescent, 22-39 young adult).(8,9)
Patient Eligibility Population:
Inclusion Criteria Age: 0-39.99 years AML: primary or secondary Year of Transplant between 1997-2010 First Allogeneic Transplant Matched Unrelated donor (8/8 HLA match) or mismatched unrelated donor (7/8 HLA
match) Myeloablative conditioning regimen with TBI and Cyclophosphamide Graft Source: Bone Marrow, Peripheral Blood, umbilical cord
Exclusion Criteria
Prior Allogeneic Transplant Ex vivo T cell depletion CD34 selected PBSCs grafts Haploidentical related donors, matched sibling or family donors
Data Requirements: Variables to be included:
Patient Age (0-15, 15-21, 22-39 years) Donor-recipient gender match (female donor and male recipient vs. other) Donor-recipient HLA match (matched vs. mismatched) Stem cell source Year of Transplantation (1997-2003 vs. 2004-2010) Performance Status (Lansky if < 16 years , Karnofsky if ≥ 16 years) GVHD prophylaxis
35

Not for publication or presentation Attachment 6
Donor-recipient CMV serostatus (donor and recipient negative vs. donor positive/recipient negative vs. donor negative/recipient positive vs. donor and recipient positive )
Type of ATG ( Horse vs. Rabbit) Disease Characteristics Disease Status at Transplantation (CR1 vs. CR2 vs. Refractory) Risk Stratification (Favourable, Adverse and Intermediate as per MRC and COG criteria)
(10-12) Favourable t(15;17), t(8;21)(q22;q22), inv(16)p13.1q22) or t(16:16)(p13.1;q22), Adverse –7, -5 or del(5q), complex, t(6;9)(p23;q34), over 15% blasts after course 1, inv
(3)(q21q26.2) or t(3:3)(q21:q26.2), 12p abnormality, FLT3-ITD high allelic ratio Intermediate all others
Outcomes of Interest: TRM at 100 days and 1 year Overall and leukaemia free survival Acute and chronic GVHD Infections: Viral (CMV, EBV, Adenovirus), Fungal (invasive) Time to neutrophil recovery (≥0.5 x 109/L for 3 consecutive days) and platelet recovery
(≥ 20 x 109/L unsupported by transfusion for 7 days) Data Collection Forms: 2000 (Recipient Baseline Data), 2010 (AML pre HSCT Data), 2100 (100 day Post-HSCT data), 2200 (six months to two years post HSCT), 2300 (Yearly follow up for greater than 2 years Post-HSCT data), 2110 (AML post-HSCT data).
Sample Requirements: We request input from statisticians.
Study Design: Multicentre Retrospective analysis involving CIBMTR and BSBMT registries.
References: 1. Uberti JP, Agovi MA, Tarima S, et al. Comparative analysis of BU and CY versus CY and TBI in
full intensity unrelated marrow donor transplantation for AML, CML and myelodysplasia. Bone Marrow Transplant. 2011;46(1):34-43.
2. Finke J, Bethge WA, Schmoor C, et al. Standard graft versus host disease prophylaxis with or without ant-T-cell globulin in haematopoeitic cell transplantation from matched unrelated donors: a randomized, open label, multicentre phase 3 trial. Lancet Oncol 2009; 10 (9): 855-864.
3. Socie G, Schmoor C, Bethge WA et al. Chronic graft versus host disease: long term results from a randomized trial on graft-versus-host disease prophylaxis with or without anti-T-cell globulin ATG-Fresenius. Blood 2011, 117 (23): 6375-6382.
4. Bacigalupo A, Lamparelli T, Bruzzi P, et al. Antithymocyte globulin for graft-versus-host disease prophylaxis in transplants from unrelated donors: 2 randomised studies from the Gruppo Italiano Trapianti Midollo Osses (GIMTO). Blood. 2001, 98 (10): 2942-2947.
5. Veys P, Wynn R, Eapen M et al. Impact of Immune modulation with in vivo T cell depletion and myeloablative total body irradiation conditioning regimen on outcomes after unrelated donor transplantation for acute lymphoblastic leukaemia in children. Blood. 2012. doi:10.1182/blood-2012-01-405795.
6. Soiffer RJ, Rademacher J, Ho V et al. Impact of immune modulation with anti-T cell antibodies on the outcome of reduced intensity allogeneic hematopoeitic stem cell transplantation for hematologic malignancies. Blood. 2011; 117 (25): 6963-6970.
36

Not for publication or presentation Attachment 6
7. Baron F, Labopin G, Mufti R, Craddock C et al. Impact of alemtuzumab versus anti-thymocyte globulin after unrelated allogeneic stem cell transplantation with reduced-intensity conditioning as treatment for AML in CR1:a survey from the Acute Leukaemia Working Party of the EBMT. Bone Marrow Transplantation. 2012; 47; S75-S76 (0347).
8. Adolescent and Young Adult Oncology Progress Peer Review Group. Closing the Gap: Research and care imperatives for adolescents and young adults with cancer-Report of the Adolescent and Young Adult Oncology Progress Review Group. Bethesda, MD. National Cancer Institute; 2006. Report.
9. Nakano T, Hunger S. Therapeutic Strategy and complications in the adolescent and young adult with acute lymphoblastic leukemia. Blood. 2012. 119 (19):4372-4374.
10. Harrison C, Hills R, Webb D, Burnett A, Gibson B, et al. Journal of Clinical Oncology. 2010: 28 (16) 2674-2681.
11. Stevens R, Hann I, Wheatley K, et al. British Journal of Haematology. 1998 101: 130-140. 12. Winter S. Pediatric Acute Leukemia Therapies Informed by Molecular Analysis of High-Risk
Disease. Hematology Am Soc Hematol Educ Program. 2011;2011:366-73.
37

Not for publication or presentation Attachment 6
Selection criteria The below selection criteria was applied Excluded Included
INCLUSION:
1st allo HCT for AML between 1997 and 2010 after CAP modeling 14123
Age < 40 7677 6446
Unrelated donor 2461 3985
BM, PB or UCB graft 5 3980
7/8 or 8/8 antigen level HLA match 1178 2802
Myeloablative conditioning 324 2478
Patient with at least 100-day comprehensive research form 19 2459
Patient consented for research 6 2453
EXCLUSION:
Ex vivo T cell depletion 195 2258
CD34 selected PBSC grafts 33 2225
Characteristics of patients who were under 40 years old and had 1st allo unrelated donor translant
with myeloablative conditioning between 1997 and 2010, excluding ex vivo T cell depletion and CD34 selected PBSC grafts.
Variable Children AYA
Number of patients 614 1611
Number of centers 118 208
Patient age
Median (range) 7 (<1-15) 28 (15-40)
0-15 614 0
16-21 0 323 (20)
22-39 0 1288 (80)
Karnofsky/Lansky score
<90 93 (15) 445 (28)
90-100 475 (77) 1065 (66)
Missing 46 (7) 101 ( 6)
Donor/recipient gender match
Female donor and male recipient 122 (20) 259 (16)
Other 487 (79) 1335 (83)
Missing 5 (<1) 17 ( 1)
38

Not for publication or presentation Attachment 6
Continued.
Variable Children AYA
Donor/recipient CMV match
-/- 162 (26) 427 (27)
-/+ 152 (25) 488 (30)
+/- 78 (13) 204 (13)
+/+ 114 (19) 414 (26)
5 108 (18) 78 ( 5)
Antigen level HLA matching
Matched (8/8) 401 (65) 1252 (78)
Mismatched (7/8) 213 (35) 359 (22)
Cytogenetic abnormalities
Normal 61 (10) 234 (15)
Favorable 51 (8) 125 ( 8)
Intermediate 70 (11) 178 (11)
Poor 127 (21) 343 (21)
TBD (need review) 158 (26) 274 (17)
Missing 147 (24) 457 (28)
Disease status prior to HCT
Primary induction failure 52 (8) 202 (13)
CR1 227 (37) 636 (39)
CR2 233 (38) 453 (28)
>=CR3 10 (2) 36 ( 2)
Relapse 89 (14) 279 (17)
Missing 3 (<1) 5 (<1)
Graft type
Bone marrow 347 (57) 747 (46)
Peripheral blood 81 (13) 814 (51)
Umbilical cord blood 186 (30) 50 ( 3)
ATG or campath
ATG alone 276 (45) 465 (29)
CAMPATH alone 34 (6) 46 ( 3)
No ATG or CAMPATH 304 (50) 1097 (68)
Missing 0 3 (<1)
39
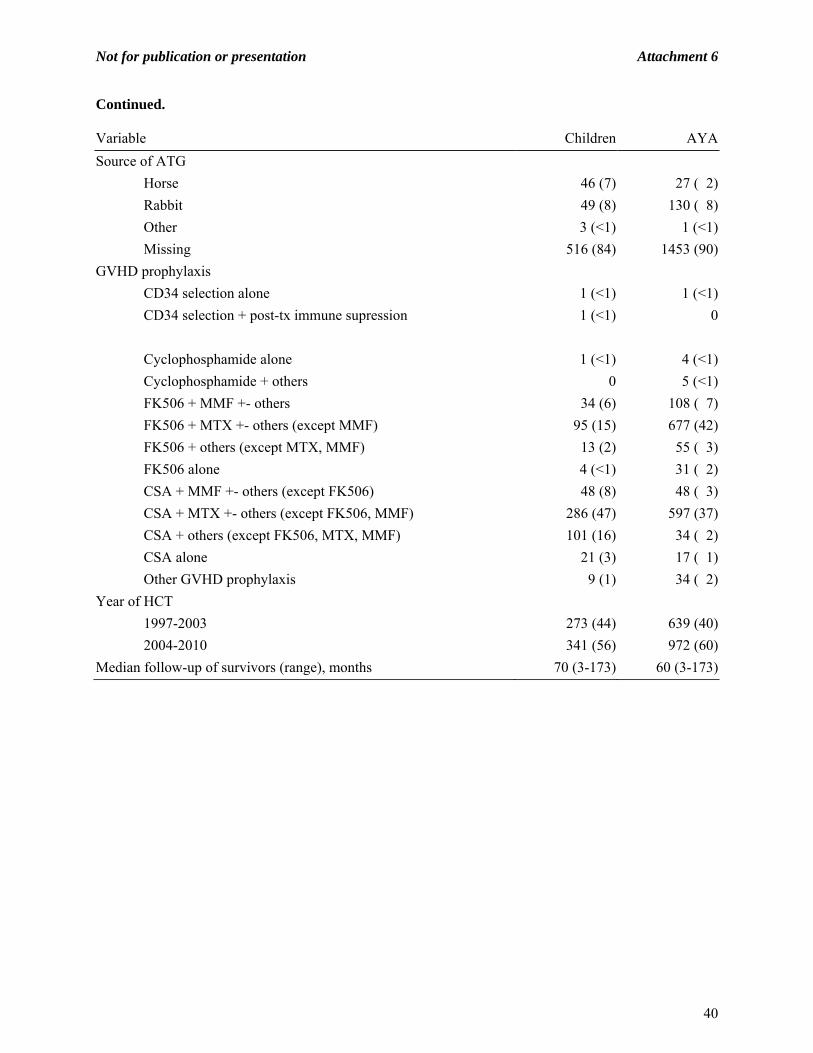
Not for publication or presentation Attachment 6
Continued.
Variable Children AYA
Source of ATG
Horse 46 (7) 27 ( 2)
Rabbit 49 (8) 130 ( 8)
Other 3 (<1) 1 (<1)
Missing 516 (84) 1453 (90)
GVHD prophylaxis
CD34 selection alone 1 (<1) 1 (<1)
CD34 selection + post-tx immune supression 1 (<1) 0
Cyclophosphamide alone 1 (<1) 4 (<1)
Cyclophosphamide + others 0 5 (<1)
FK506 + MMF +- others 34 (6) 108 ( 7)
FK506 + MTX +- others (except MMF) 95 (15) 677 (42)
FK506 + others (except MTX, MMF) 13 (2) 55 ( 3)
FK506 alone 4 (<1) 31 ( 2)
CSA + MMF +- others (except FK506) 48 (8) 48 ( 3)
CSA + MTX +- others (except FK506, MMF) 286 (47) 597 (37)
CSA + others (except FK506, MTX, MMF) 101 (16) 34 ( 2)
CSA alone 21 (3) 17 ( 1)
Other GVHD prophylaxis 9 (1) 34 ( 2)
Year of HCT
1997-2003 273 (44) 639 (40)
2004-2010 341 (56) 972 (60)
Median follow-up of survivors (range), months 70 (3-173) 60 (3-173)
40

Not for publication or presentation Attachment 7
Study Proposal 1112-06 Study Title: Comparing Autologous to Allogeneic Transplant in APL Patients with Extramedullary Disease who Achieve a Second or Subsequent Complete Remission (CR) Chezi Ganzel, MD, Memorial Sloan-Kettering Cancer Center, New York, NY, [email protected] Martin S. Tallman, MD, Memorial Sloan-Kettering Cancer Center, New York, NY, [email protected] Dan Douer, MD, Memorial Sloan-Kettering Cancer Center, New York, NY, [email protected] Specific Aims:
1. To compare the OS, DFS, TRM after autologous and allogeneic transplant in APL patients with extramedullary disease.
2. To determine the frequency and outcome of extramedullary disease in APL over time. 3. To compare different groups of patients with extramedullary disease, according to: sites of
involvement (CNS, skin etc.) and different types of relapse (extramedullary only vs. extramedullary plus bone marrow, molecular vs. hematologic bone marrow relapse).
Scientific Justification: Currently, in the all trans retinoic acid (ATRA) and arsenic trioxide (ATO) era, the complete remission (CR) rate of acute promyelocytic leukemia (APL) patients is very high, at approximately 90%. Despite this success, there are about 10-20% of patients who relapse1,2. The common practice in these patients is to induce a second CR and then to proceed to autologous hematopoietic stem cell transplantation (HSCT). Extramedullary disease (EMD) in AML patients was described decades ago. It was recognized that the incidence of this phenomenon varies between the different types of the disease. While in AML patients with t(8;21), EMD is not uncommon3, in APL it was considered to be a very rare phenomenon4,5. Several case reports described EMD in APL patients6 in different sites (such as CNS, skin, gingiva, optic nerve and mediastinum) and in different time points (presentation and relapse) but the general impression is that its appearance is very unusual. Due to its rarity, the prognostic impact of this event in APL patients is undetermined7,8. Recently, there are several reports of increasing numbers of EMD in APL patients, particularly at time of relapse7,9. Several authors tried to relate this new increment to the major therapeutic change in APL which took place with the introducing of ATRA. The rationale for such a relationship could be that by prolonging survival, ATRA creates enough time for the dormant cells in sanctuary sites to grow8. Alternatively, it may be that ATRA itself encourages the leukemic cells to migrate from the blood vessels to extramedullary sites perhaps by perturbing adhesion molecules10. Despite all of these descriptions and explanations, still the real incidence of EMD in APL patients is unknown and more importantly, the prognostic implication of this phenomenon is uncertain. The prognostic question can be divided into cases of sole EMD and those with a combination of both EMD and concurrent bone marrow relapse. It could also be that different extramedullary sites have different prognostic impact. Due to the fact that almost all extramedullary APL cases are in the setting of relapsed disease, the practical question is whether it is sufficient for such patients to undergo autologous HSCT, such as is routine practice for patients in second CR after bone marrow relapse, or are they better treated with more aggressive therapy such as allogeneic HSCT. Due to the major differences in both morbidity and mortality between the two types of transplant, this question is of critical importance. In this study we will examine whether there is a change in the incidence of diagnosis of extramedullary relapse throughout the years. We will compare retrospectively the prognosis and toxicity of autologous versus allogeneic HSCT in this kind of patients. We will also try to divide all these patients into
41

Not for publication or presentation Attachment 7
subgroups according to different extramedullary sites and according to the presence of bone marrow involvement in addition to the extramedullary one. It should be noticed that there is other CIBMTR project, led by Dr Morel Rubinger, dealing the all big issue of comparing allogeneic to autologous HSCT in relapsed APL patients. We already have been reassured that Rubinger’s study is not going to address EMD in any detailed way so that there is no major overlap. Patient Eligibility Population: Every APL patient registered in CIBMTR, who had EMD and underwent a transplant. Data Requirements:
The CIBMTR forms that will be needed are: - Recipient baseline data - Acute myelogenous leukemia pre-HSCT data - Selective post-transplant essential data No requirement for collection of supplemental data. Variables from the existing CIBMTR data collection forms that need to be analyzed:
1. ID, age, sex, ethnic. 2. At diagnosis: Diagnosis date, pathology (regular APL / M3v), cytogenetics, FISH, molecular
(including: PML-RARA break point), WBC, ANC, Hb, Plt, PT, PTT, fibrinogen, D-Dimer, extramedullary (y/n), extramedullary site/s, if several – number of sites, extramedullary type of involvement (biopsy proven, molecular only, clinical only)
3. Induction: date of beginning treatment, protocol, antracyclins (y/n), ARA-C (y/n), ATRA (y/n), ATO, intrathecal (y/n), radiation (site/n), hematologic complete remission (y/n), molecular complete remission (y/n), differentiation syndrome (y/n)
4. Consolidation: antracyclins (y/n), ARA-C (y/n), ATRA (y/n), ATO, number of cycles 5. Maintenance: maintenance therapy (y/n), ATRA (y/n), 6MP (y/n), MTX (y/n) 6. 1st relapse: date, time from remission to relapse ,bone marrow involvement (y/n), BM relapse
type (hematologic / molecular), extramedullary (y/n), extramedullary site/s, if several – number of sites, extramedullary type of involvement (biopsy proven, molecular only, clinical only), clonal evolution, salvage therapy, intrathecal (y/n), radiation (site/n)
7. Autologous transplant: date, BM/PB, conditioning, CD 34+/per Kg, hematologic complete remission (y/n), molecular complete remission (y/n), extramedullary complete remission (y/n), transplant related complications (hematological/ infectious/ cardiovascular/ arrhythmias / neurological), transplant related mortality (TRM) (y/n)
8. 2nd relapse: date, time from remission to relapse , relapse type (hematologic / molecular), extramedullary (y/n), extramedullary site/s, if several – number of sites, extramedullary type of involvement (biopsy proven, molecular only, clinical only), clonal evolution, salvage therapy, intrathecal (y/n), radiation (site/n)
9. Autologous transplant: date, BM/PB, conditioning, CD 34+/per Kg, hematologic complete remission (y/n), molecular complete remission (y/n), extramedullary complete remission (y/n), transplant related complications (hematological/ infectious/ cardiovascular/ arrhythmias / neurological), transplant related mortality (y/n)
10. 3rd relapse: date, time from remission to relapse 11. Prognosis: new malignancy (y/n), new malignancy type, alive (y/n), date last seen or death
Desired outcome variables: DFS, OS and transplant related toxicity. The toxicity includes: hematological, infectious, cardiovascular, arrhythmias and neurological complications, as well as transplant related mortality.
42

Not for publication or presentation Attachment 7
Sample Requirements: Not required. Study Design: We will collect the above data from the CIBMTR database of all APL patients with extramedullary disease who underwent any type of HSC transplant. We will examine the change in the frequency (absolute number and percentage of relapse) of extramedullary disease throughout the years. We will perform a detailed comparison between those who underwent autologous vs. allogeneic HSCT. It will include patients characteristics, toxicity aspects as wells as TRM, DFS and OS. We will try to look at different sites of EMD, or associated with bone marrow involvement, and to check if every subgroup does the same. Statistical Methodology: Input from CIBMTR is needed for appropriate methodology statistical design. References:
1. Burnett AK, Grimwade D, Solomon E, Wheatley K, Goldstone AH. Presenting white blood cell count and kinetics of molecular remission predict prognosis in acute promyelocytic leukemia treated with all-trans retinoic acid: result of the Randomized MRC Trial. Blood 1999;93:4131-4143.
2. Ades L, Sanz MA, Chevret S, et al. Treatment of newly diagnosed acute promyelocytic leukemia (APL): a comparison of French-Belgian-Swiss and PETHEMA results. Blood 2008;111:1078-1084.
3. Tallman MS, Hakimian D, Shaw JM, Lissner GS, Russell EJ, Variakojis D. Granulocytic sarcoma is associated with the 8;21 translocation in acute myeloid leukemia. J Clin Oncol 1993;11:690-697.
4. Marra R, Stori S, Pagano L, et al. Central nervous system acute promyelocytic leukaemia: a report of three cases. Haematologia (Budap) 1989;22:195-199.
5. Byrd JC, Edenfield WJ, Shields DJ, Dawson NA. Extramedullary myeloid cell tumors in acute nonlymphocytic leukemia: a clinical review. J Clin Oncol 1995;13:1800-1816.
6. Wiernik PH, De Bellis R, Muxi P, Dutcher JP. Extramedullary acute promyelocytic leukemia. Cancer 1996;78:2510-2514.
7. Specchia G, Lo Coco F, Vignetti M, et al. Extramedullary involvement at relapse in acute promyelocytic leukemia patients treated or not with all-trans retinoic acid: a report by the Gruppo Italiano Malattie Ematologiche dell'Adulto. J Clin Oncol 2001;19:4023-4028.
8. de Botton S, Sanz MA, Chevret S, et al. Extramedullary relapse in acute promyelocytic leukemia treated with all-trans retinoic acid and chemotherapy. Leukemia 2006;20:35-41.
9. Vega-Ruiz A, Faderl S, Estrov Z, et al. Incidence of extramedullary disease in patients with acute promyelocytic leukemia: a single-institution experience. Int J Hematol 2009;89:489-496.
10. Evans GD, Grimwade DJ. Extramedullary disease in acute promyelocytic leukemia. Leuk Lymphoma 1999;33:219-229.
43

Not for publication or presentation Attachment 7
Selection Criteria
The below selection criteria was applied # excluded N
INCLUSION:
1st HCT for APL, auto (n=249) and allo (n=1206) after CAP modeling 1455
Extramedullary involvement any time prior to HCT 1326 129
EXCLUSION
Alive patient with less than 100 day follow up 0 129
Patient do not consent 0 129
Characteristics Table Variable Allogeneic Autologous
Number of patients 106 23
Number of centers 75 19
Median (range) 22 (2-64) 23 (3-69)
Age at transplant, years
<10 19 (18) 4 (17)
10-19 26 (25) 6 (26)
20-29 27 (25) 3 (13)
30-39 17 (16) 6 (26)
40-49 10 ( 9) 2 ( 9)
50-59 6 ( 6) 1 ( 4)
>=60 1 (<1) 1 ( 4)
Sex
Male 61 (58) 15 (65)
Female 45 (42) 8 (35)
Karnofsky score
<90% 34 (32) 2 ( 9)
>=90% 70 (66) 19 (83)
Missing 2 ( 2) 2 ( 9)
44

Not for publication or presentation Attachment 7
Continued.
Variable Allogeneic Autologous
White blood count at dx, x10^9/L
Median (range) 9 (<1-220) 8 (1-163)
<= 10 52 (49) 12 (52)
10 - 100 35 (33) 5 (22)
> 100 8 ( 8) 1 ( 4)
Missing 11 (10) 5 (22)
t(15;17) at diagnosis
Negative 9 ( 8) 4 (17)
Positive 46 (43) 11 (48)
Not tested or unknown 51 (48) 8 (35)
Cytogenetic abnormalities (SWOG)
Normal 13 (12) 6 (26)
Favorable 49 (46) 11 (48)
Intermediate 3 ( 3) 1 ( 4)
Poor 2 ( 2) 0
TBD (need review) 5 ( 5) 2 ( 9)
Missing 34 (32) 3 (13)
Time from CR1 to 1st relapse, months
Median (range) 8 (<1-33) 12 (3-41)
<12 39 (37) 5 (22)
>=12 19 (18) 6 (26)
Missing 48 (45) 12 (52)
Time from CR2 to transplant, months
Median (range) 2 (<1-12) 2 (<1-8)
<6 89 (84) 22 (96)
>=6 9 ( 8) 1 ( 4)
Missing 8 ( 8) 0
ATRA as induction therapy
Yes 22 (21) 11 (48)
Missing 84 (79) 12 (52)
ATRA as consolidation therapy
Yes 6 ( 6) 4 (17)
Missing 100 (94) 19 (83)
45

Not for publication or presentation Attachment 7
Continued. Variable Allogeneic AutologousType of first relapse
Medullary 21 (20) 1 ( 4)
Extramedullary 18 (17) 9 (39)
Medullary and extramedullary 23 (22) 8 (35)
Missing 44 (42) 5 (22)
Conditioning regimen intensity
Myeloablative 103 (97) 0
RIC 2 ( 2) 0
Non-myeloablative 1 (<1) 0
Not applicable 0 23
TBI for conditioning
Non-TBI 46 (43) 13 (57)
TBI based 60 (57) 10 (43)
Type of donor
HLA-identical sibling 82 (77) 0
URD well/partially matched 2 ( 2) 0
Other related and URD combined 22 (21) 0
Auto, not applicable 0 23
Graft type
Bone marrow 88 (83) 9 (39)
Peripheral blood 18 (17) 14 (61)
Year of transplant
<=1995 69 (65) 11 (48)
1996-2000 17 (16) 5 (22)
2001-2005 18 (17) 3 (13)
2006-2010 2 ( 2) 4 (17)
ATG or campath
No 99 (93) 23
Yes 7 ( 7) 0
46

Not for publication or presentation Attachment 7
Continued.
Variable Allogeneic Autologous
GVHD prophylaxis
No GVHd prophylaxis 3 ( 3) 0
Ex vivo t-cell depletion +- post-tx immune supression 11 (10) 0
CD34 selection +- post-tx immune supression 1 (<1) 0
FK506 +- MMF/MTX +- others 6 ( 6) 0
CSA +- MMF/MTX +- others 58 (55) 0
Other 27 (25) 0
Not applicable 0 23
Acute GVHD, N (%)
No aGVHD 49 (46) 23
I 18 (17) 0
II 19 (18) 0
III 13 (12) 0
IV 7 ( 7) 0
Median follow-up of survivors (range), months 110 (3-284) 85 (35-217)
47

Not for publication or presentation Attachment 8
Study Proposal 1112-10 Study Title: Comparing Autologous Transplant to Arsenic Trioxide (ATO) for Patients with Acute Promyelocytic Leukemia (APL) in First and Subsequent Relapse Chezi Ganzel, MD, Memorial Sloan Kettering Cancer Center, New York, NY, [email protected] Martin S. Tallman, MD, Memorial Sloan Kettering Cancer Center - Peds, New York, NY, [email protected] Dan Douer, MD, Memorial Sloan Kettering Cancer Center, New York, NY, [email protected] Specific Aims:
1. To compare the overall survival (OS) and disease-free survival (DFS) between autologous hematopoietic stem cell transplantation (HSCT) and arsenic trioxide (ATO)-based treatment in relapsed APL patients, using large databases.
2. To compare the toxicity between autologous HSCT and ATO-based treatment in relapsed APL patients, using large databases. The relevant toxicity includes: treatment-related mortality (TRM), hematological toxicity, infectious diseases, cardiovascular events, arrhythmias, neurologic events and APL differentiation syndrome.
3. To identify patient characteristics that can predict a favorable outcome with ATO-based treatment alone without transplant.
Scientific Justification: The treatment of APL patients was revolutionized in the past 20 years with the introduction of all trans retinoic acid (ATRA) and ATO which have fundamentally changed the standard of care and dramatically improved the outcome. However approximately 10-20% of APL patients relapse1,2. The common practice in the western world is to treat relapsed APL with ATO and after achieving molecular CR, to consolidate with autologous transplantation3-6. The long-term leukemia-free survival after HSCT in these patients has been reported as between 50%6 to 79%7, provided that the transplanted cells are PCR negative for the PML/RAR fusion transcript. Taking into consideration the well-known morbidity and mortality risks of HSCT, the question whether this approach is justified in every patient is raised. Furthermore, not all patients can undergo HSCT due to age, co-morbidities, fertility issues, financial limitations or their choice. Arsenic trioxide is an extremely active single agent in APL8 and therefore could be considered in relapsed patients, as an alternative post remission treatment. In several countries ATO is more widely used, including as post remission treatment in relapsed patients. However, the reported data from these countries are limited. A study from Iran9 reported 31 relapsed patients with 2-year DFS of 54% and a study from India10 reported only 19 patients with 5-year estimate EFS of about 35%. Given these limitations, a direct comparison between the two approaches could not be done. Furthermore, it is highly unlikely that a randomized trial would ever be carried out. In addition, it is possible that some patients have characteristics, for which multiple cycles of ATO may lead to as favorable an outcome or even more favorable, less toxic and less expensive as that of autologous HSCT. Defining the effectiveness of ATO consolidation in relapsed APL patients and identifying characterization of those patients who appear to respond well would provide physicians an alternative to HSCT. It might be that in the future not every relapsed APL patient will require autologous HSCT, but some with specific characteristics will be treated more effectively by ATO.
48

Not for publication or presentation Attachment 8
Patient Eligibility Population: The CIBMTR patients = transplanted patients:
- Patients with relapsed APL (molecular or hematologic) - Underwent autologous HSCT - Registered on CIBMTR.
Foreign databases = ATO based therapy: - Patients with relapsed APL (molecular or hematologic) - Did not undergo HSCT. - Included in databases of the Indian and/or the Iranian groups
Data Requirements:
The CIBMTR forms that will be needed are: - Recipient baseline data - Acute myelogenous leukemia pre-HSCT data - Selective post-transplant essential data
The study will combine CIBMTR data with data from databases of the Indian and/or the Iranian groups. The selection criteria for patients from these groups will be: every relapsed (molecular or hematologic) APL patient who was treated by ATO based therapy and didn’t undergo HSCT.
Variables from the existing CIBMTR data collection forms that need to be analyzed: 1. ID, age, sex, ethnic 2. At diagnosis: Diagnosis date, pathology (regular APL / M3v), cytogenetics, FISH,
molecular (including: PML-RARA break point), WBC, ANC, Hb, Plt, PT, PTT, fibrinogen, D-Dimer, extramedullary (y/n), extramedullary site
3. Induction: date of beginning treatment, protocol, antracyclins (y/n), ARA-C (y/n), ATRA (y/n), ATO, intrathecal (y/n), radiation (y/n), hematologic complete remission (y/n), molecular complete remission (y/n), differentiation syndrome (y/n)
4. Consolidation: antracyclins (y/n), ARA-C (y/n), ATRA (y/n), ATO, number of cycles 5. Maintenance: maintenance therapy (y/n), ATRA (y/n), 6MP (y/n), MTX (y/n) 6. 1st relapse: date, time from remission to relapse , relapse type (hematologic / molecular),
extramedullary (y/n), extramedullary site, clonal evolution, salvage therapy, intrathecal (y/n), radiation (y/n)
7. Autologous transplant: date, BM/PB, conditioning, CD 34+/per Kg, hematologic complete remission (y/n), molecular complete remission (y/n), transplant related complications (hematological/ infectious/ cardiovascular/ arrhythmias/ neurological), transplant related mortality (y/n)
8. 2nd relapse: date, time from remission to relapse , relapse type (hematologic / molecular), extramedullary (y/n), extramedullary site, clonal evolution, salvage therapy, intrathecal (y/n), radiation (y/n)
9. Autologous transplant: date, BM/PB, conditioning, CD 34+/per Kg, hematologic complete remission (y/n), molecular complete remission (y/n), transplant related complications (hematological/ infectious/ cardiovascular/ arrhythmias/ neurological), transplant related mortality (y/n)
10. 3rd relapse: date, time from remission to relapse 11. Prognosis: new malignancy (y/n), new malignancy type, alive (y/n), date last seen or
death Desired outcome variables: DFS, OS and transplant related toxicity. The toxicity includes:
hematological, infectious, cardiovascular, arrhythmias and neurological complications, as well as transplant related mortality.
49

Not for publication or presentation Attachment 8
Sample Requirements: Not required. Study Design: In this study we will collect information from the CIBMTR data base and 1or 2 ATO-only database for relapse APL patients. We will compare the data between the groups for demographics, details of disease presentation, induction therapy, remission rate, and the characteristics of the relapse. After identification of the common and different characteristics of the two groups, we will list side by side the prognostic factor, including treatment related morbidity (TRM), and OS of each group. Finally within the ATO-only group we will analyze the patient characteristics in relation to their outcome including TRM, OS and DFS. Statistical Methodology: Input from CIBMTR is needed for appropriate methodology statistical design. References:
1. Burnett AK, Grimwade D, Solomon E, Wheatley K, Goldstone AH. Presenting white blood cell count and kinetics of molecular remission predict prognosis in acute promyelocytic leukemia treated with all-trans retinoic acid: result of the Randomized MRC Trial. Blood 1999;93:4131-43.
2. Ades L, Sanz MA, Chevret S, et al. Treatment of newly diagnosed acute promyelocytic leukemia (APL): a comparison of French-Belgian-Swiss and PETHEMA results. Blood 2008;111:1078-84.
3. Mandelli F, Labopin M, Granena A, et al. European survey of bone marrow transplantation in acute promyelocytic leukemia (M3). Working Party on Acute Leukemia of the European Cooperative Group for Bone Marrow Transplantation (EMBT). Bone Marrow Transplant 1994;14:293-8.
4. Kamimura T, Miyamoto T, Nagafuji K, et al. Role of autotransplantation in the treatment of acute promyelocytic leukemia patients in remission: Fukuoka BMT Group observations and a literature review. Bone Marrow Transplant 2011;46:820-6.
5. Nabhan C, Mehta J, Tallman MS. The role of bone marrow transplantation in acute promyelocytic leukemia. Bone Marrow Transplant 2001;28:219-26.
6. Sanz MA, Labopin M, Gorin NC, et al. Hematopoietic stem cell transplantation for adults with acute promyelocytic leukemia in the ATRA era: a survey of the European Cooperative Group for Blood and Marrow Transplantation. Bone Marrow Transplant 2007;39:461-9.
7. de Botton S, Fawaz A, Chevret S, et al. Autologous and allogeneic stem-cell transplantation as salvage treatment of acute promyelocytic leukemia initially treated with all-trans-retinoic acid: a retrospective analysis of the European acute promyelocytic leukemia group. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2005;23:120-6.
8. Douer D, Tallman MS. Arsenic trioxide: new clinical experience with an old medication in hematologic malignancies. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2005;23:2396-410.
9. Alimoghaddam K, Ghavamzadeh A, Jahani M, et al. Treatment of relapsed acute promyelocytic leukemia by arsenic trioxide in Iran. Arch Iran Med 2011;14:167-9.
10. Thirugnanam R, George B, Chendamarai E, et al. Comparison of clinical outcomes of patients with relapsed acute promyelocytic leukemia induced with arsenic trioxide and consolidated with either an autologous stem cell transplant or an arsenic trioxide-based regimen. Biol Blood Marrow Transplant 2009;15:1479-84.
50
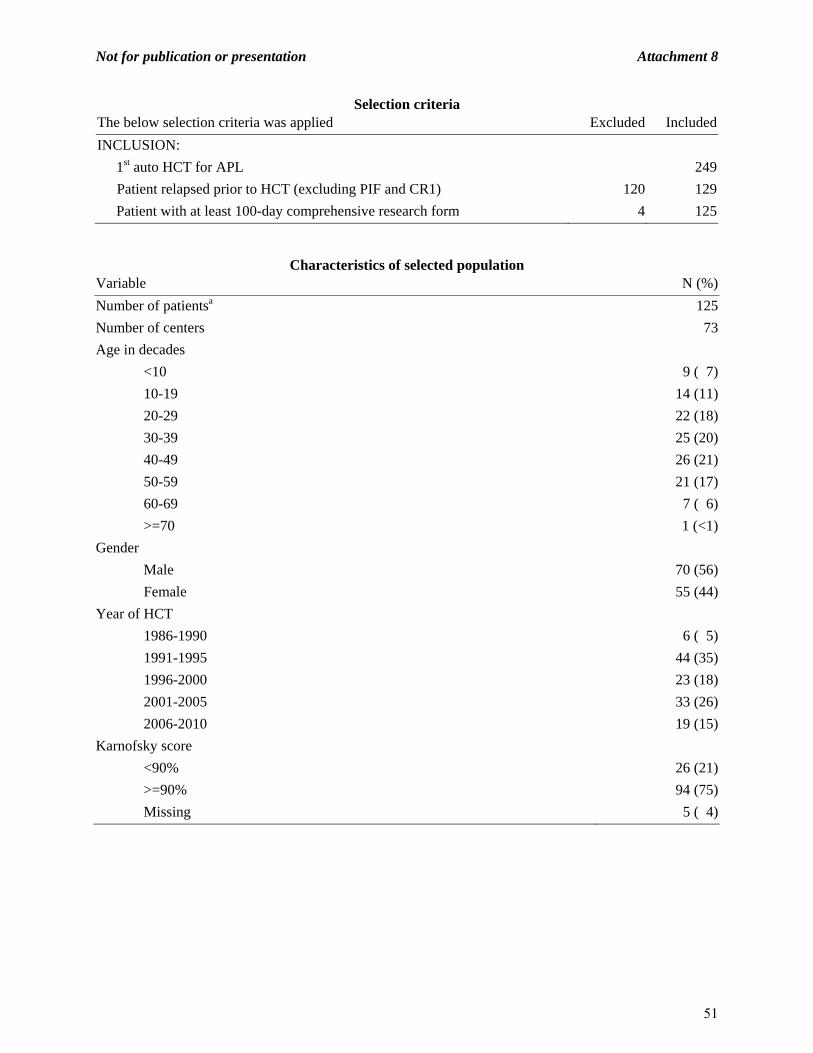
Not for publication or presentation Attachment 8
Selection criteria The below selection criteria was applied Excluded Included
INCLUSION:
1st auto HCT for APL 249
Patient relapsed prior to HCT (excluding PIF and CR1) 120 129
Patient with at least 100-day comprehensive research form 4 125
Characteristics of selected population Variable N (%)
Number of patientsa 125
Number of centers 73
Age in decades
<10 9 ( 7)
10-19 14 (11)
20-29 22 (18)
30-39 25 (20)
40-49 26 (21)
50-59 21 (17)
60-69 7 ( 6)
>=70 1 (<1)
Gender
Male 70 (56)
Female 55 (44)
Year of HCT
1986-1990 6 ( 5)
1991-1995 44 (35)
1996-2000 23 (18)
2001-2005 33 (26)
2006-2010 19 (15)
Karnofsky score
<90% 26 (21)
>=90% 94 (75)
Missing 5 ( 4)
51

Not for publication or presentation Attachment 8
Continued.
Variable N (%)
White blood count at diagnosis
<= 30 77 (62)
30 - 100 10 ( 8)
> 100 3 ( 2)
Missing 35 (28)
Disease status prior to HCTb
CR2 104 (83)
>=CR3 4 ( 3)
Relapse 17 (14)
Time from diagnosis to HCT
<6 months 2 ( 2)
6 - 12 months 10 ( 8)
>12 months 113 (90)
Conditioning regimen intensity
Myeloablative 112 (90)
RIC 8 ( 6)
Non-myeloablative 1 (<1)
TBD (regimens under review) 4 ( 3)
Total body irradiation
No 95 (76)
Yes 30 (24)
Graft type
Bone marrow 41 (33)
Peripheral blood 84 (67)
Cause of death
Still alive 81 (65)
Primary disease 21 (17)
New malignancy 3 ( 2)
Idipathic pneumonia syndrome 3 ( 2)
Infection 5 ( 4)
Organ failure 5 ( 4)
Others 5 ( 4)
Missing 2 ( 2)
Median follow-up of survivors (range), months 73 (3-242)a Only patients with consent and complete post-HCT 100 day forms are selected b patients with primary induction failure and CR1 are excluded
52
Not for publication or presentation Attachment 9
Study Proposal 1112-38 Study Title: Allogeneic transplantation for older patients with acute lymphoblastic leukemiareported to the CIBMTR and EBMT: impact of age on transplant outcomes. Ashley Rosko, MD, University Hospitals Case Medical Center, Cleveland, OH, [email protected] Marcos de Lima, MD, University Hospitals Case Medical Center, Cleveland, OH, [email protected] Mohamad Mohty, MD, Service d’Hematologie Clinique, CHU Hotel Dieu, Universite de Nantes, Nantes, France, [email protected] Daniel Weisdorf, MD, Bone and Marrow Transplant Program, University of Minnesota, Minneapolis, MN, [email protected] Veronika Bachanova MD, PhD, Bone and Marrow Transplant Program, University of Minnesota, Minneapolis, MN, [email protected] Specific Aims:
1. To analyze outcomes of allogeneic donor transplantation for older patients with acute lymphoblastic leukemia comparing 3 age groups: 40-50, 51-60 and ≥61 years of age.
2. To define the prognostic factors (patient, disease and transplant related [including graft choice and conditioning regimen intensity]) impacting on mortality, relapse and survival.
Scientific Justification: Elderly ALL is the largest ALL subset for which advances in treatment failed to deliver satisfactory results(1). It is estimated that 30% of patients diagnosed with ALL are over 60 years of age. Among suggested reasons to explain worse outcomes are some biological disease characteristics (Ph+ chromosome or high risk cytogenetics are present in almost 50% of patients older than 55) and enhanced susceptibility of older patients to organ-toxic side effects of chemotherapy (2). Non-transplant studies:
Prospective MRC UKALL XII/ECOG study on 100 subjects between ages 55-65 reported 73% complete remission rate and 20% 5-year overall survival (3). None of these patients underwent stem cell transplantation. Relapse remains the leading cause of death for those who attained remission with induction chemotherapy.
CALGB ALL chemotherapy trials enrolled 166 patients older patients and reported a complete remission rate of 57% and 5 year OS rate only 12% (2).
Transplant studies: In high risk ALL, the allogeneic donor transplant can be curative for selected eligible patients
of all ages with acceptable organ function and performance status. Over the past decade, the increased the availability of the alternative donor pool and advances in supportive care lead to increasing use of allograft in ALL (4-6). Alternative graft sources maybe particularly relevant for aging population of patients and therefore included in this proposal.
Increasing age has been recognized as a major risk for transplant related mortality (TRM), with age limit being above 35 years in recent prospective MRCUKALL XII/ECOG trial (7). Increased TRM was associated with lack of survival advantage of MA HCT for “older” patients.
53
Not for publication or presentation Attachment 9
The use of reduced intensity conditioning (RIC) has allowed for allografting in older patients and resulted into similar survival compared to myeloablative HCT(8-10). Some studies demonstrated lower TRM of RIC HCT in ALL performed in CR1 (11). CIBMTR study compared efficacy of RIC HCT in 92 patients with Philadelphia negative ALL in CR1,CR2 to full intensity HCT and showed similar TRM (33% vs 32%), relapse rate (35% vs 26%) and 3-years OS (43% vs 38%) (12). In that study, age did not impact on relapse whereas TRM of patients over 30 was higher compare to younger than 30; however no dramatic differences were seen between those 40-49 and over 50 years of age (HR 1.49 and 1.88). Notably allografts have been curative for a selected older patients even in 6th decade.
Large registries such as CIBMTR and EBMT are needed to perform the analysis of elderly ALL transplants since there are only few patients per single institution. These data may help us to understand how patient, transplant variables, donor source and ALL related factors in various age groups (middle-aged, older, oldest) impact tolerance to transplant procedure and what are the types of post-transplant complications in these age groups. The potency and durability of GVL effect and impact of age on relapse and survival will be better understood.
The goal is to identify those subsets among elderly ALL 1) who substantially benefit from early consolidation with allogeneic HCT or 2) in whom HCT should be not be performed and alternative therapies needs to be applied. These results may offer an important insight to guide the development of eligibility criteria and selection definition for prospective RIC HCT protocol for older ALL patients.
Patient Eligibility Population: Patients aged 40 years and above with ALL who received an allogeneic donor stem cell transplantation in complete remission. Included are all patients (CR1 CR2 and active disease) from any graft source transplanted between 1/2000-6/2011.
Outcomes:
1 and 2 year treatment-related mortality: Time to death without evidence of leukemia recurrence.
1 and 2 year Relapse incidence: Time to onset of leukemia recurrence. Recurrence is defined as morphologic marrow or clinical extramedullary relapse.
3 years Leukemia-free survival: Time to treatment failure (death or relapse). 3 years Overall survival: Time to death. Acute GVHD: Grade II, III and/or IV skin, gastrointestinal or liver abnormalities
(Consensus criteria of acute GVHD). Chronic GVHD: Occurrence of symptoms in any organ system (diagnostic criteria of
chronic GVHD). Variables to be Analyzed: Patient-related:
Age: by 3 decade groups: 40-49 vs 50-59 vs 60+ Gender: male vs. female Coexistent disease or organ impairment – specify organ involved or as available HCT-CI: - Cardiac - Pulmonary - Diabetes - Depression - Hypertension
54

Not for publication or presentation Attachment 9
- Obesity - Renal insufficiency - Concomitant anticoagulant therapy Prior fungal infections (yes or no) Karnofsky score: <80 vs 80-90 vs 100%
Disease-related: Cytogenetics: t(9:22) vs other high risk vs other WBCx109/L at diagnosis: <30 vs. 30-100 vs. >100 Extramedullary disease prior to HCT: CNS (yes/no), other (yes/no) Time to achieve CR1: <4 weeks vs. 4-8 weeks vs. >8 weeks Duration of CR1 (in CR2 patients) Induction chemotherapy
Treatment-related:
Time from dx to transplant Time from remission to transplant Conditioning regimen:
- MA - Specific RIC regimen( grouped by alkylating –agent based regimen vs. low-dose TBI
200 cGy-based vs. other) Type of donor:
- HLA-identical sibling - Matched unrelated (8/8) - Partially matched unrelated (7/8) - Mismatched URD (<7/8) - UCB
Donor-recipient gender match: F-M vs. M-F vs. M-M vs. F-F Donor age : continuous median (range) in 3 cohorts Donor-recipient CMV status: -/- vs. others Source of stem cells: BM vs. PBSC Year of transplant 2000-2005 vs 2006-2011 GVHD prophylaxis: CsA/tacrolimus +MTX vs. CSA/tacrolimus + MMF +/-other vs
other Use of ATG/campath: yes vs no In vitro T cell depletion yes vs no Central nervous system prophylaxis Donor lymphocyte infusion (as part of planned therapy) Maintenance therapy Date of relapse (if applicable) Date of death or last known contact Cause of death (if known)
55

Not for publication or presentation Attachment 9
Study Design: Our goal is to compare the outcomes of adults with ALL among three age cohorts: 40-50 vs 51-60 vs >61 years utilizing retrospectively detailed information on patient’s clinical characteristics and outcomes utilizing the CIBMTR and EBMT registries. Patient and transplant related variables will be compared using Chi-square test for categorical variables and Mann-Whitney test for continuous variables. Kaplan-Meier curves will be used to estimate the probability of OS and LFS, cumulative incidence will be used to estimate probability of neutrophil recovery, TRM, GVHD and relapse. Relapse will be summarized by the cumulative incidence estimate with treatment related mortality as a competing risk. For LFS and OS patients will be censored at the time of last follow-up. Age groups will be compared using Cox proportional hazard regression model for aGVHD, cGHVD and neutrophil recovery. The proportional hazards assumption for all other variables. For OS, DFS, TRM and relapse, a forward stepwise method was used to build regression models. Other specifics TBD by CIBMTR statistician. Since the age groups are the main interest of this study, the risk factor of age will be included in all steps of model building procedure. The risk factors with significant level of p < 0.05 will be included in the model. The potential interaction between main effect of conditioning regimen and all significant covariates will be examined. Adjusted probability of leukemia-free survival and overall survival will be computed based on final Cox regression model, stratified by treatment groups, and weighted by the pooled sample proportion value for all significant risk factors. These adjusted probabilities estimate likelihood of outcomes in populations with similar prognostic factors. SAS programs will be used in all the analyses. References:
1. Pulte D, Gondos A, Brenner H. Improvement in survival in younger patients with acute lymphoblastic leukemia from the 1980s to the early 21st century. Blood 2009; 113: 1408-1411.
2. Larson RA. Management of acute lymphoblastic leukemia in older patients. Semin Hematol 2006; 43: 126-133.
3. Sive JI, Buck G, Fielding A, Lazarus HM, Litzow MR, Luger S, et al. Outcomes in older adults with acute lymphoblastic leukaemia (ALL): results from the international MRC UKALL XII/ECOG2993 trial. Br J Haematol 2012; 157: 463-471.
4. Marks DI, Aversa F, Lazarus HM. Alternative donor transplants for adult acute lymphoblastic leukaemia: a comparison of the three major options. Bone Marrow Transplant 2006; 38: 467-475.
5. Tomblyn MB, Arora M, Baker KS, Blazar BR, Brunstein CG, Burns LJ, et al. Myeloablative hematopoietic cell transplantation for acute lymphoblastic leukemia: analysis of graft sources and long-term outcome. J Clin Oncol 2009; 27: 3634-3641.
6. Bachanova V, Weisdorf D. Unrelated donor allogeneic transplantation for adult acute lymphoblastic leukemia: a review. Bone Marrow Transplant 2008; 41: 455-464.
7. Goldstone AH, Richards SM, Lazarus HM, Tallman MS, Buck G, Fielding AK, et al. In adults with standard-risk acute lymphoblastic leukemia, the greatest benefit is achieved from a matched sibling allogeneic transplantation in first complete remission, and an autologous transplantation is less effective than conventional consolidation/maintenance chemotherapy in all patients: final results of the International ALL Trial (MRC UKALL XII/ECOG E2993). Blood 2008; 111: 1827-1833.
8. Mohty M, Labopin M, Volin L, Gratwohl A, Socie G, Esteve J, et al. Reduced-intensity versus conventional myeloablative conditioning allogeneic stem cell transplantation for patients with acute lymphoblastic leukemia: a retrospective study from the European Group for Blood and Marrow Transplantation. Blood 2010; 116: 4439-4443.
56

Not for publication or presentation Attachment 9
9. Ram R, Storb R, Sandmaier BM, Maloney DG, Woolfrey A, Flowers ME, et al. Non-myeloablative conditioning with allogeneic hematopoietic cell transplantation for the treatment of high-risk acute lymphoblastic leukemia. Haematologica 2011; 96: 1113-1120.
10. Stein AS, Palmer JM, O'Donnell MR, Kogut NM, Spielberger RT, Slovak ML, et al. Reduced-intensity conditioning followed by peripheral blood stem cell transplantation for adult patients with high-risk acute lymphoblastic leukemia. Biol Blood Marrow Transplant 2009; 15: 1407-1414.
11. Bachanova V, Verneris MR, DeFor T, Brunstein CG, Weisdorf DJ. Prolonged survival in adults with acute lymphoblastic leukemia after reduced-intensity conditioning with cord blood or sibling donor transplantation. Blood 2009; 113: 2902-2905.
12. Marks DI, Wang T, Perez WS, Antin JH, Copelan E, Gale RP, et al. The outcome of full-intensity and reduced-intensity conditioning matched sibling or unrelated donor transplantation in adults with Philadelphia chromosome-negative acute lymphoblastic leukemia in first and second complete remission. Blood 2010; 116: 366-374.
57

Not for publication or presentation Attachment 9
Selection criteria
The below selection criteria was applied Excluded Included1st allo HCT for ALL after CAP modeling 14526Age >=40 12487 2039Year of HCT between 01/01/2000 and 06/30/2011 667 1372Patient with at least 100-day comprehensive research form 138 1234Patient consent 18 1216
Characteristics of study population Variable N (%)Number of patients 1216Number of centers 179Age in decades 40-49 640 (53) 50-59 456 (38) 60-69 119 (10) >=70 1 (<1)Gender Male 625 (51) Female 591 (49)Recipient race Caucasian 975 (80) African-American 54 ( 4) Asian 115 ( 9)
Pacific Islander 1 (<1) Native American 5 (<1) Other 22 ( 2) Unknown 44 ( 4)Year of HCT 2000-2005 659 (54) 2006-2011 557 (46)Karnofsky score < 80 106 ( 9) 80 - 90 292 (24) 90 - 100 754 (62) Missing 64 ( 5)Prior fungal infections No 1076 (88) Yes 124 (10) Missing 16 ( 1)
58

Not for publication or presentation Attachment 9
Continued. Variable N (%)Cytogenetics T(9:22) only 220 (18) T(9:22) and other 217 (18) Other 267 (22) Missing 512 (42)White blood count at diagnosis <= 30 654 (54) 30 - 100 149 (12) > 100 140 (12) Missing 273 (22)Disease status prior to HCT Primary induction failure 85 ( 7) CR1 713 (59) CR2 217 (18) >=CR3 31 ( 3) Relapse 167 (14) Missing 3 (<1)Extramedullary disease at diagnosis No 1028 (85) Yes 176 (14) Missing 12 (<1)EMD at CNS at diagnosis No 1134 (93) Yes 70 ( 6) Missing 12 (<1)EMD at other site at diagnosis No 1091 (90) Yes 113 ( 9) Missing 12 (<1)Time to achieve CR1 <4 weeks 149 (12) 4-8 weeks 419 (34) >8 weeks 444 (37) Missing 204 (17)Duration of CR1 <6 months 46 ( 4) 6-12 months 38 ( 3) >12 months 85 ( 7) Missing 999 (82) Patient not in CR2 48 ( 4)
59

Not for publication or presentation Attachment 9
Continued. Variable N (%)Time from diagnosis to HCT <6 months 511 (42) 6 - 12 months 396 (33) >12 months 305 (25) Missing 4 (<1)Conditioning regimen intensity Myeloablative 924 (76) RIC 176 (14) Non-myeloablative 95 ( 8) TBD (regimens under review) 7 (<1) Missing 14 (1)Total body irradiation No 330 (27) Yes 872 (72) Missing 14 ( 1)GVHD prophylaxis Ex vivo T-cell depletion alone 20 ( 2) Ex vivo T-cell depletion + post-tx immune supression 16 ( 1) CD34 selection alone 8 (<1) CD34 selection + post-tx immune supression 19 ( 2) Cyclophosphamide alone 6 (<1) Cyclophosphamide + others 5 (<1) FK506 + MMF +- others 127 (10) FK506 + MTX +- others (except MMF) 399 (33) FK506 + others (except MTX, MMF) 47 ( 4) FK506 alone 23 ( 2) CSA + MMF +- others (except FK506) 104 ( 9) CSA + MTX +- others (except FK506, MMF) 333 (27) CSA + others (except FK506, MTX, MMF) 27 ( 2) CSA alone 51 ( 4) Other GVHD prophylaxis 31 ( 3)ATG or campath ATG alone 230 (19) CAMPATH alone 34 ( 3) No ATG or CAMPATH 938 (77) Missing 14 ( 1)Graft type Bone marrow 297 (24) Peripheral blood 827 (68) Umbilical cord blood 90 ( 7) PB + UCB 2 (<1)
60
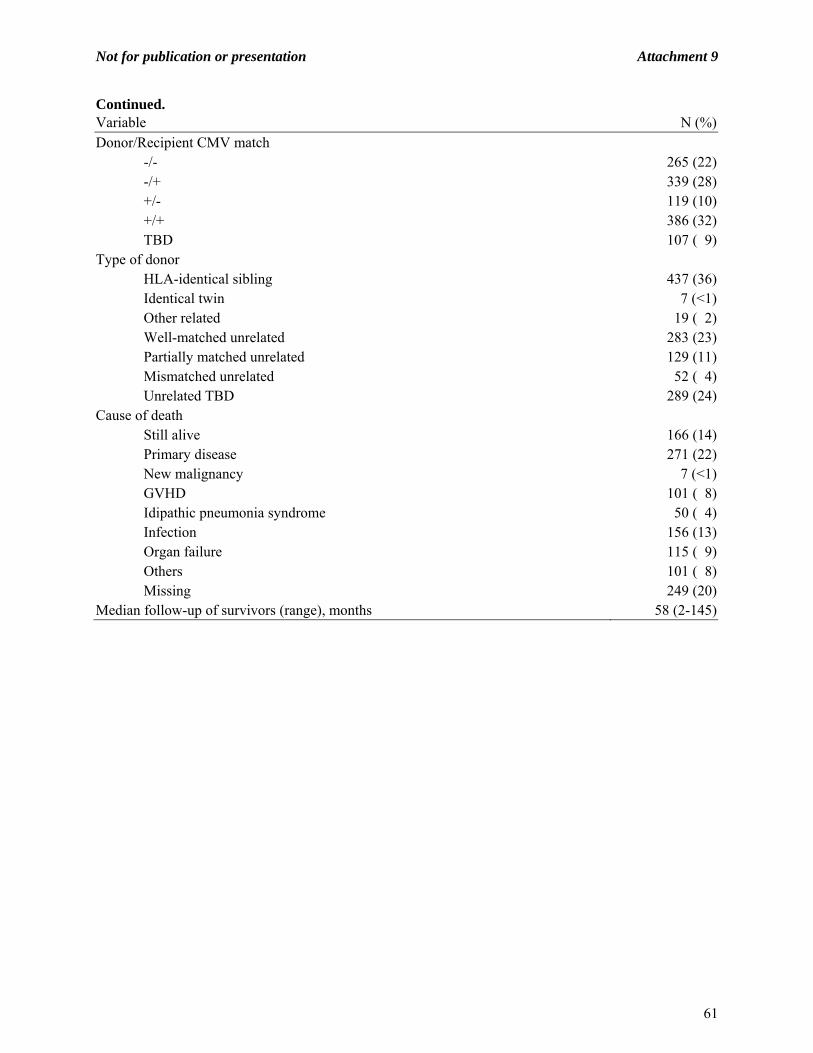
Not for publication or presentation Attachment 9
Continued. Variable N (%)Donor/Recipient CMV match -/- 265 (22) -/+ 339 (28) +/- 119 (10) +/+ 386 (32) TBD 107 ( 9)Type of donor HLA-identical sibling 437 (36) Identical twin 7 (<1) Other related 19 ( 2) Well-matched unrelated 283 (23) Partially matched unrelated 129 (11) Mismatched unrelated 52 ( 4) Unrelated TBD 289 (24)Cause of death Still alive 166 (14) Primary disease 271 (22) New malignancy 7 (<1) GVHD 101 ( 8) Idipathic pneumonia syndrome 50 ( 4) Infection 156 (13) Organ failure 115 ( 9) Others 101 ( 8) Missing 249 (20)Median follow-up of survivors (range), months 58 (2-145)
61

Not for publication or presentation Attachment 10
Study Proposal 1112-35 Study Title: Prognostic significance of cytogenetic abnormalities in patients with Philadelphia‐negative acute lymphoblastic leukemia undergoing allogeneic hematopoietic stem cell transplantation (allo‐HCT) in complete remission: A Center for International Blood and Marrow Transplant Research Study Aleksandr Lazaryan, MD, MPH, PhD, University of Minnesota Medical Center, Fairview, Minneapolis, MN, [email protected] Veronika Bachanova, MD, PhD, University of Minnesota Medical Center, Fairview, Minneapolis, MN, [email protected] Daniel Weisdorf, MD, University of Minnesota Medical Center, Fairview, Minneapolis, MN, [email protected] Specific Aims:
1. To develop a novel HCT‐specific cytogenetic classification scheme for prognostication of relapse and survival outcomes following allo‐HCT in patients with Philadelphia‐negative ALL
2. To validate major existing cytogenetic groupings of Ph‐ALL among the recipients of allo‐HCT from multicenter cohort of CIBMTR patients
3. To compare the performance of novel and existing classification schemes in an independent cohort of HCT patients from CIBMTR patient database
Scientific Justification: Allogeneic hematopoietic stem cell transplantation (allo‐HCT) is a potent life‐saving therapy for a subset of patients with ALL particularly for those with high risk disease. Definitions of high risk ALL vary from study to study and generally include a combination of demographic (age), clinical (WBC, response to induction, minimal residual disease), pathologic (B‐or T‐cell lineage), and cytogenetic characteristics. Cytogenetic abnormalities have been consistently shown to be highly prognostic of outcomes in adult ALL (1, 2). In particular, the presence of Philadelphia chromosome portends poor prognosis and warrants allo‐HCT in first complete remission (CR1) (3, 4). The use of tyrosine kinase inhibitors has revolutionized therapy of Philadelphia‐positive (Ph+) ALL that subsequently evolved into distinct disease entity (5). The rest of adult ALL patients constitute a diverse group of Philadelphia‐negative (Ph‐) diseasestratified into distinct cytogenetic risk categories based on their prognostic significance across several studies summarized in Supplementary Table 1. Due to low frequencies of individual Ph‐chromosomal abnormalities, only few of these studies were able to construct prognostic models based on cytogenetic abnormalities of Ph‐adult ALL patients (1, 2). The most commonly used cytogenetic categorieshave been developed based on the mix of patients treated with either conventional chemotherapy or transplant (autologous or allogeneic). MLL translocations at 11q23 including t(4;11), complex karyotype, t(8;14), low hypodiploidy or near triploidy consistently prognosticated poor clinical outcomes in MRC/ECOG and SWOG phase III clinical trials, which included a subset of allo‐HCT recipients (1, 2). The potential benefit of allo‐HCT largely depends on immune‐mediated graft‐vs‐leukemia effect which compared to conventional chemotherapy may have a completely different impact on a given cytogenetic abnormality. Although MRC/ECOG and SWOG data favored prognostic relevance of cytogenetics for related‐donor recipients of allo‐HCT, the existing classification schemes are largely based on chemotherapy treated ALL patients hence may not be most optimal for the transplant recipients.
62
Not for publication or presentation Attachment 10
To date, there has been no validated HCT‐specific cytogenetic classification of Ph‐ALL. The knowledge of cytogenetic abnormalities and their significance in predicting outcomes after allo‐HCT could contribute to a stratified biological classification of adult Ph‐ALL patients undergoing transplant based on cytogenetics, much like in AML (6). With overall rarity of adult ALL and its individual chromosomal abnormalities it becomes necessary to study very large cohorts of patients with data on cytogenetics readily available. CIBMTR has one of the largest data on adult ALL recipients of allo‐HCT including information on cytogenetic abnormalities. This creates a unique research opportunity for developing a cytogenetic classification scheme for prognostication of ALL relapse and survival outcomes following allo‐HCT which is often a critical part of the decision to pursue allo‐HCT. In addition, this study will provide a novel classification scheme for stratifying adult patients entering clinical trials of allo‐HCT for Ph‐ALL. Patient Eligibility Population:
Adult Ph‐ALL patients age 16 years or older who underwent allo‐HCT in first complete remission (CR1) or second complete remission (CR2) at participating CIBMTR centers between 1995 and 2010 and for whom cytogenetic information is available prior to allo‐HCT.
Patients with L3 ALL and those with inadequate post‐transplant follow‐up will not be eligible to participate.
Data Requirements:
All necessary study data are available for extraction from the ALL‐specific CIBMTR data collectionforms(http://www.cibmtr.org/DataManagement/DataCollectionForms/Documents/2011/Rev2.0/combine‐2011%20ALL%20r2.pdf)
Demographic (age, gender, race), clinical (date of diagnosis, WBC, KPS, blast % (bone marrow and circulating) at diagnosis, presence/site of extramedullary disease, disease status prior to transplant [CR1 vs. CR2], number of prior therapies, type of allo‐HCT [myeloablative vs. reduced intensity; matched related vs. unrelated donor];donor‐recipient gender match; donor‐recipient CMV status; cell source [bone marrow vs. PBSC]; GVHD prophylaxis; year of HCT [1995‐2010 grouped by 5‐year increments]; TBI vs. non‐TBI conditioning; date of relapse or death), and biologic (B‐or T‐lineage; cytogenetic and molecular abnormalities) characteristics will be abstracted from the CIBMTR data forms.
Sample Requirements: N/A Study Design: We propose an observational retrospective cohort study of Ph‐adult ALL recipients of allo‐HCT. Eligible subjects will have their cytogenetic abnormalities characterized and recorded at diagnosis and/or prior to allo‐HCT. Ph‐negative cytogenetic abnormalitiesfrom the CIBMTR data forms include A. Monosomy [¬7] B. Trisomies [+4, +8, +17, +21] C. Translocations [t(1;19), t(2;8), t(4;11), t(5;17), t(8;14), t(8;22), 9p, t(10;14), t(11;14), t(v;11q23), t(12;21), 12p D. Deletions [del6q/6q‐, del9p/9p‐, del12p/12p‐] E. Addition [add(14q)] F. Other [hyperdiploid (>50), hypodiploid (<46), complex (≥3 distinct abnormalities), other]. Available primary cytogenetics reports will be carefully reviewed to enable validation analysis of established cytogenetic groupings within CIBMTR database as well as their
63

Not for publication or presentation Attachment 10
comparison with transplant‐based grouping that will be derived from this study. The latest available karyotype (i.e. at diagnosis for patients in CR1 and at relapse for patients in CR2 when available) will be analyzed in this study, as it is likely to be the best determinant of post‐transplant outcomes. The primary outcome will be an overall survival (OS) following allo‐HCT calculated from the time of transplant to death or date of last follow up at which point the subjects are censored. Secondary endpoints will include event‐free survival (EFS), non‐relapse mortality (NRM) and cumulative incidence of relapse. EFS will be estimated as the time from transplant to death or disease relapse with survivors being free of disease at the time of last follow up (i.e. censored observation). Both EFS and OS will be estimated by Kaplan‐Meier method and compared using log‐rank test. Cumulative incidence of NRM and relapse will be compared between cytogenetic groups using Gray test with disease relapse treated as a competing risk in NRM analysis. Clustering analysis of proportional hazards of individual cytogenetic abnormalities will be used for establishing the new CIBMTR‐based cytogenetics classification of Ph‐ALL. Performance of various classification schemes will be compared by using Akaike information criterion (AIC) derived from the full proportional hazards model and a model that does not incorporate cytogenetics.
64

Not for publication or presentation Attachment 10
Supplementary Table 1. Karyotype‐based risk stratificationofPhiladelphia‐negative (Ph‐) ALL
Studies/Publications Risk groups Cytogenetic abnormalities
MRC (Moorman, Blood 2007)
Poor t(4;11), t(8;14)*, complex* (≥5 abnormalities w/o translocations), low hypodiploidy (30‐39)/near triploidy (60‐78)*
Other all other karyotypes Good high hyperdiploidy (>50), del9p
Modified MRC** (Pullarkat, Blood 2008)
Very high t(4;11), t(8;14), complex (≥5 abnormalities w/o translocations), low hypodiploidy (30‐39)/near triploidy (60‐78)
High other 11q23/MLL, ‐7§, del7p, +8§, t(1;19) or t(17;19), t(5;14)
Intermediate normal diploid, low hyperdiploidy (47‐50), abnormal 11q (not MLL), del6qǂ, del17p, del9p, del12p, del13q, t14q32, t(10;14), tetraploidy (>80), or any karyotypic changes not identified with a different risk group
Standard high hyperdiploidy (>50)
SWOG (Pullarkat, Blood 2008)
Other unfavorable
‐7, +8, and 11q23/MLL gene rearrangements
Miscellaneous
any karyotypic changes not identified with a different risk group
Normal normal karyotype
NILG‐ALL (Bassan, Blood 2009)
Adverse t(4;11) and/or MLL‐AF4, +8, near triploidy, lowhypodiploidy, complex (≥3 abnormalities), del6q, t(8;14)
Non‐adverse t(1;19) and/or E2A‐PBX1, hyperdiploid, other karyotypic changes not identified with a different risk group
Normal normal karyotype
North UK (Moorman, Blood 2010)
Poor t(4;11), t(8;14), t(14;18), complex (≥5 abnormalities w/o translocations), low hypodiploidy (30‐39)/near triploidy (60‐78)
Standard all other karyotypes
GIMEMA 0496 (Mancini, Blood 2005)
High t(4;11), t(1;19) Intermediate del6q and other karyotypes Standard normal karyotype, del9p
*Independent predictors**Combined based on similar OS estimates §Identified as unfavorable by CALGB (7) ǂIdentified as intermediate risk (8)
65

Not for publication or presentation Attachment 10
References: 1. Pullarkat V, Slovak ML, Kopecky KJ, Forman SJ, Appelbaum FR. Impact of cytogenetics on the
outcome of adult acute lymphoblastic leukemia: results of Southwest Oncology Group 9400 study. Blood 2008;111(5):2563‐72.
2. Moorman AV, Harrison CJ, Buck GA, et al. Karyotype is an independent prognostic factor in adult acute lymphoblastic leukemia (ALL): analysis of cytogenetic data from patients treated on the Medical Research Council (MRC) UKALLXII/Eastern Cooperative Oncology Group (ECOG) 2993 trial. Blood 2007;109(8):3189‐97.
3. Fielding AK, Rowe JM, Richards SM, et al. Prospective outcome data on 267 unselected adult patients with Philadelphia chromosome‐positive acute lymphoblastic leukemia confirms superiority of allogeneic transplantation over chemotherapy in the pre‐imatinib era: results from the International ALL Trial MRC UKALLXII/ECOG2993. Blood 2009;113(19):4489‐96.
4. Laport GG, Alvarnas JC, Palmer JM, et al. Long‐term remission of Philadelphia chromosome‐positive acute lymphoblastic leukemia after allogeneic hematopoietic cell transplantation from matched sibling donors: a 20‐year experience with the fractionated total body irradiation‐etoposide regimen. Blood 2008;112(3):903‐9.
5. Liu‐Dumlao T, Kantarjian H, Thomas DA, O'Brien S, Ravandi F. Philadelphia‐positive acute lymphoblastic leukemia: current treatment options. Curr Oncol Rep;14(5):387‐94.
6. Armand P, Kim HT, Zhang MJ, et al. Classifying cytogenetics in patients with acute myelogenous leukemia in complete remission undergoing allogeneic transplantation: a Center for International Blood and Marrow Transplant Research study. Biol Blood Marrow Transplant;18(2):280‐8.
7. Wetzler M, Dodge RK, Mrozek K, et al. Prospective karyotype analysis in adult acute lymphoblastic leukemia: the cancer and leukemia Group B experience. Blood 1999;93(11):3983‐93.
8. Mancini M, Scappaticci D, Cimino G, et al. A comprehensive genetic classification of adult acute lymphoblastic leukemia (ALL): analysis of the GIMEMA 0496 protocol. Blood 2005;105(9):3434‐41.
66

Not for publication or presentation Attachment 10
Selection criteria
The below selection criteria was applied Excluded Included
1st allo HCT for ALL after CAP modeling 14564
Age >=16 6028 8536
Year of HCT between 1995 to 2010 3355 5181
Philadelphia negative and non-L3 380 4801
Patient in CR1 or CR2 prior to HCT 1412 3389
BM or PB graft 220 3169
Patient with at least 100-day comprehensive research form 69 3100
Patient consent 37 3063
EXCLUSION:
Missing gender 1 3062
Characteristics of study population
Cytogenetics prior to HCT
Variable Normal Abnormal Unknown
Number of patients 276 2195 591
Number of centers 118 270 172
Age in decades
10-19 49 (18) 394 (18) 104 (18)
20-29 89 (32) 582 (27) 205 (35)
30-39 56 (20) 500 (23) 127 (21)
40-49 48 (17) 394 (18) 98 (17)
50-59 26 ( 9) 269 (12) 48 ( 8)
60-69 8 ( 3) 56 ( 3) 8 ( 1)
>=70 0 0 1 (<1)
Gender
Male 175 (63) 1333 (61) 344 (58)
Female 101 (37) 862 (39) 247 (42)
67

Not for publication or presentation Attachment 10
Continued.
Variable Normal Abnormal Unknown
Recipient race
Caucasian 206 (75) 1788 (81) 476 (81)
African-American 8 ( 3) 54 ( 2) 17 ( 3)
Asian 45 (16) 195 ( 9) 49 ( 8)
Pacific islander 1 (<1) 1 (<1) 2 (<1)
Native American 0 7 (<1) 2 (<1)
Other 5 ( 2) 66 ( 3) 19 ( 3)
Unknown 11 ( 4) 84 ( 4) 26 ( 4)
Year of HCT
1995-2000 65 (24) 722 (33) 263 (45)
2001-2005 81 (29) 883 (40) 211 (36)
2006-2010 130 (47) 590 (27) 117 (20)
Karnofsky score
<90% 61 (22) 550 (25) 141 (24)
>=90% 210 (76) 1555 (71) 425 (72)
Missing 5 ( 2) 90 ( 4) 25 ( 4)
White blood count at diagnosis
<= 10 129 (47) 790 (36) 211 (36)
10 - 100 74 (27) 807 (37) 153 (26)
> 100 26 ( 9) 303 (14) 60 (10)
Missing 47 (17) 295 (13) 167 (28)
Disease status prior to HCT
CR1 164 (59) 1494 (68) 297 (50)
CR2 112 (41) 701 (32) 294 (50)
Cytogenetic test details available
No 270 (98) 588 (27) 587 (99)
Yes 6 ( 2) 1607 (73) 4 (<1)
Extramedullary disease at diagnosis
No 220 (80) 1842 (84) 476 (81)
Yes 55 (20) 340 (15) 101 (17)
Missing 1 (<1) 13 (<1) 14 ( 2)
EMD at CNS at diagnosis
No 256 (93) 2070 (94) 541 (92)
Yes 19 ( 7) 112 ( 5) 36 ( 6)
Missing 1 (<1) 13 (<1) 14 ( 2)
68

Not for publication or presentation Attachment 10
Continued.
Variable Normal Abnormal Unknown
EMD at other site at diagnosis
No 238 (86) 1942 (88) 506 (86)
Yes 37 (13) 240 (11) 71 (12)
Missing 1 (<1) 13 (<1) 14 ( 2)
Time from diagnosis to HCT
<6 months 96 (35) 940 (43) 149 (25)
6 - 12 months 82 (30) 645 (29) 150 (25)
>12 months 97 (35) 608 (28) 292 (49)
Missing 1 (<1) 2 (<1) 0
Conditioning regimen intensity
Myeloablative 238 (86) 1955 (89) 540 (91)
RIC 16 ( 6) 127 ( 6) 33 ( 6)
Non-myeloablative 10 ( 4) 77 ( 4) 13 ( 2)
TBD (regimens under review) 1 (<1) 16 (<1) 4 (<1)
Missing 11 (4) 20 (<1) 1 (<1)
Total body irradiation
No 50 (18) 441 (20) 149 (25)
Yes 216 (78) 1731 (79) 442 (75)
Missing 10 (4) 23 ( 1) 0
GVHD prophylaxis
Ex vivo T-cell depletion alone 4 ( 1) 50 ( 2) 16 ( 3)
Ex vivo T-cell depletion + post-tx immune suppression 5 ( 2) 80 ( 4) 23 ( 4)
CD34 selection alone 0 11 (<1) 4 (<1)
CD34 selection + post-tx immune suppression 1 (<1) 32 (1) 14 ( 2)
Cyclophosphamide alone 0 4 (<1) 0
Cyclophosphamide + others 1 (<1) 6 (<1) 1 (<1)
FK506 + MMF +- others 20 ( 7) 118 ( 5) 19 ( 3)
FK506 + MTX +- others (except MMF) 67 (24) 517 (24) 121 (20)
FK506 + others (except MTX, MMF) 5 ( 2) 46 ( 2) 11 ( 2)
FK506 alone 4 ( 1) 24 ( 1) 6 ( 1)
CSA + MMF +- others (except FK506) 6 ( 2) 58 ( 3) 16 ( 3)
CSA + MTX +- others (except FK506, MMF) 138 (50) 1060 (48) 305 (52)
CSA + others (except FK506, MTX, MMF) 5 ( 2) 40 ( 2) 15 ( 3)
CSA alone 10 ( 4) 68 ( 3) 23 ( 4)
Other GVHD prophylaxis 10 ( 4) 81 ( 4) 17 ( 3)
69

Not for publication or presentation Attachment 10
Continued.
Variable Normal Abnormal Unknown
ATG or campath
ATG + CAMPATH 0 0 1 (<1)
ATG alone 38 (14) 388 (18) 110 (19)
CAMPATH alone 3 ( 1) 63 ( 3) 9 ( 2)
No ATG or CAMPATH 225 (82) 1721 (78) 470 (80)
Missing 10 ( 4) 23 ( 1) 1 (<1)
Graft type
Bone marrow 118 (43) 1034 (47) 321 (54)
Peripheral blood 158 (57) 1161 (53) 270 (46)
Donor/Recipient CMV match
-/- 65 (24) 613 (28) 176 (30)
-/+ 47 (17) 494 (23) 126 (21)
+/- 34 (12) 253 (12) 73 (12)
+/+ 114 (41) 698 (32) 160 (27)
TBD 16 ( 6) 137 ( 6) 56 ( 9)
Type of donor
HLA-identical sibling 177 (64) 943 (43) 232 (39)
Identical twin 3 ( 1) 11 (<1) 0
Other related 8 ( 3) 47 ( 2) 13 ( 2)
Well-matched unrelated 3 ( 1) 450 (21) 136 (23)
Partially matched unrelated 1 (<1) 241 (11) 100 (17)
Mismatched unrelated 1 (<1) 90 ( 4) 37 (6)
Unrelated TBD 81 (29) 411 (19) 73 (12)
Missing 2 (<1) 2 (<1) 0
Cause of death
Still alive 91 (33) 547 (25) 137 (23)
Primary disease 59 (21) 438 (20) 114 (19)
New malignancy 1 (<1) 18 (<1) 1 (<1)
GVHD 11 ( 4) 169 ( 8) 40 ( 7)
Idipathic pneumonia syndrome 8 ( 3) 122 ( 6) 35 ( 6)
Infection 20 ( 7) 217 (10) 69 (12)
Organ failure 17 ( 6) 145 ( 7) 45 ( 8)
Others 18 ( 7) 144 ( 7) 52 ( 9)
Missing 51 (18) 395 (18) 98 (17)
Median follow-up of survivors (range), months 50 (2-192) 70 (1-194) 70 (2-194)
70

Not for publication or presentation Attachment 11
Study Proposal 1112-41
Study Title: Outcomes of Allogeneic Stem Cell Transplantation in T cell Acute Lymphoblastic Leukemia Walid Rasheed, MD. King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia, [email protected] Richard Maziarz, MD, Oregon Health and Science University, Portland, OR, [email protected] Mahmoud Aljurf, MD, MPH, King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia, [email protected] Specific Aims: To analyze outcomes of allogeneic stem cell transplantation (Allo-SCT) in adult patients with T-Cell Acute Lymphoblastic Leukemia (T-ALL) including overall survival (OS), disease-free survival (DFS) and non-relapse mortality (NRM). Scientific Justification: T-ALL accounts for approximately 20-25% of adult patients with ALL (1). T-ALL has clinical, immunologic, cytogenetic, and molecular features that are distinct from those of B-ALL (2, 3). Recent studies suggest improved outcome with the use of intensive treatment and T-ALL was associated with a better 5-year overall survival (OS) than B-ALL (48% vs. 41%, P 0.001) (4). However the long term outcome of adult patients with T-ALL remains unsatisfactory with 5-year OS of 30% -50% (4-6). Furthermore, the outcome of relapsing patients is very poor with 5-year OS of 5% (7). While Allo-SCT is usually recommended for adult patients in second or later complete remission (≥CR2), it has been also offered as post-remission therapy for some patients in CR1, especially those with high-risk features (8). The most widely used risk factors include: age, white blood cell count, immunophenotype, cytogenetics, time to CR, extra-medullary disease, and more recently minimal residual disease (9-12). The literature is deficient in prospective studies focusing on T-ALL due to its relative rarity. Reports of Allo-SCT outcome in T-ALL are even more limited. Furthermore, many prospective ALL trials have reported the outcomes of T-cell subtypes as part of subgroup analysis, which makes precise comparison of outcomes in different studies difficult due to differences in patient’s characteristics and treatment protocols and relatively small no. of patients.
Marks et al (13) have reported the description and outcome of a large cohort of adults with T-ALL treated in this prospective trial with “biological assignment”. The donor group in this study included patients with and without high risk features and the median age was 29 years. OS at 5 years was 61% for the donor group compared with 46% for those without available donor (P 0.02). However, this observation is limited by the donor versus no donor assignment.
In a recent report of Allo-SCT in high risk T-ALL patients, OS and DFS at 5 years were 43.5% and 41.8%, respectively. Patients who underwent Allo-SCT in CR1 had a 5-year OS of 53.5% (95% CI 34.5-72.5) and DFS of 52% (95% CI 33-71), compared with 31.9% (95% CI 9-54.8) and 29.4% (95% CI 7.6-51.2) respectively for those transplanted in ≥CR2. Grade II-IV acute GVHD was significantly associated with a lower OS (P 0.006) and DFS (P 0.01),(14).
We are proposing to analyze CIBMTR data covering the period of 1990 – 2010 in order to assess the outcome of this group of patients and to define factors predicting the outcome after Allo-SCT. This would likely include a significantly large cohort of patients with adequate follow up. The analysis is likely to include patients with reduced intensity transplant with an opportunity to study the efficacy of less intensive conditioning regimens (with lower TRM) in this disease.
71

Not for publication or presentation Attachment 11
Patient Eligibility Population: Study period: 1990 to 2010. Patients aged =/> 16 years with a diagnosis of T-ALL who underwent allogeneic stem cell transplantation. Include sibling and unrelated donor, as well as myeloablative & non-myeloablative transplants. No restriction on type of pre transplant therapy or conditioning regimen used. Patients who underwent more than one transplantation procedure (autologous or allogeneic) are to be excluded. Data Collection:
Patient related: age, sex, performance status at transplant. Disease related: CNS involvement, Cytogenetics, extra-medullary involvement. Initial therapy related: type of chemotherapy, response to chemotherapy, use of
radiotherapy, no. of therapy lines prior to transplant. Transplant related: disease status at transplant (CR1, CR2, relapse, primary refractory),
conditioning regimen, donor type, graft source and year of transplant. Outcome related: Overall survival, Disease free survival, time to treatment
failure/relapse, incidence of acute and chronic GVHD (and its grade), non –relapse mortality.
Study Design (Scientific Plan): Analyze the overall outcome (overall survival, disease free survival, and non-relapse
mortality) of patients with T-ALL who underwent allogeneic stem cell transplantation. Analyze potential prognostic factors; stratifying outcomes according to age, cytogenetics,
disease status, conditioning regimen type, donor type (sibling vs. unrelated) and stem cell source type (BM vs. PBSC vs. Cord).
Survival and disease free survival analysis to be performed according to Kaplan – Meier methods. Log-rank test will be used to analyze outcome differences between various subgroups.
References:
1. Vitale A, Guarini A, Ariola C, et al. Adult T-cell acute lymphoblastic leukemia: biologic profile at presentation and correlation with response to induction treatment in patients enrolled in the GIMEMA LAL 0496 protocol. Blood 2006;107:473-479.
2. Schneider NR, Carroll AJ, Shuster JJ, et al. New recurring cytogenetic abnormalities and association of blast cell karyotypes with prognosis in childhood T-cell acute lymphoblastic leukemia: a pediatric oncology group report of 343 cases. Blood 2000;96:2543-2549.
3. Chiaretti S, Li X, Gentleman R, et al. Gene expression profile of adult T-cell acute lymphocytic leukemia identifies distinct subsets of patients with different response to therapy and survival. Blood 2004;103:2771-2778.
4. Rowe JM, Buck G, Burnett AK, et al. Induction therapy for adults with acute lymphoblastic leukemia: results of more than 1500 patients from the international ALL trial: MRC UKALL XII/ECOG E2993. Blood 2005;106:3760-3767.
5. Thomas X, Boiron JM, Huguet F, et al. Outcome of treatment in adults with acute lymphoblastic leukemia: analysis of the LALA-94 trial. J Clin Oncol 2004;22:4075-4086.
6. Kantarjian H, Thomas D, O'Brien S, et al. Long-term follow-up results of hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (Hyper-CVAD), a dose-intensive regimen, in adult acute lymphocytic leukemia. Cancer 2004;101:2788-2801.
7. Fielding AK, Richards SM, Chopra R, et al. Outcome of 609 adults after relapse of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study. Blood 2007;109:944-950.
72

Not for publication or presentation Attachment 11
8. Hahn T, Wall D, Camitta B, et al. The role of cytotoxic therapy with hematopoietic stem cell transplantation in the therapy of acute lymphoblastic leukemia in adults: an evidence-based review. Biol Blood Marrow Transplant 2006;12:1-30.
9. Chessells JM, Hall E, Prentice HG, Durrant J, Bailey CC, Richards SM. The impact of age on outcome in lymphoblastic leukaemia; MRC UKALL X and XA compared: a report from the MRC Paediatric and Adult Working Parties. Leukemia 1998;12:463-473.
10. Hoelzer D, Gokbuget N. New approaches to acute lymphoblastic leukemia in adults: where do we go? Semin Oncol 2000;27:540-559.
11. Moorman AV, Harrison CJ, Buck GA, et al. Karyotype is an independent prognostic factor in adult acute lymphoblastic leukemia (ALL): analysis of cytogenetic data from patients treated on the Medical Research Council (MRC) UKALLXII/Eastern Cooperative Oncology Group (ECOG) 2993 trial. Blood 2007;109:3189-3197.
12. Szczepanski T. Why and how to quantify minimal residual disease in acute lymphoblastic leukemia? Leukemia 2007;21:622-626.
13. Marks DI, Paietta EM, Moorman AV, et al. T-cell acute lymphoblastic leukemia in adults: clinical features, immunophenotype, cytogenetics, and outcome from the large randomized prospective trial (UKALL XII/ECOG 2993). Blood 2009;114:5136-5145.
14. Bakr M, Rasheed W, Mohamed SY, Al-Mohareb F, Chaudhri N, Al-Sharif F, Al-Zahrani H, Al-Dawsari G, Saleh AJ, Nassar A, Ahmed S, Elghazaly A, Ahmed SO, Ibrahim K, Chebbo W, El Gohary GM, Al Mahayni MH, Hussain F, Nurgat Z, Elhassan TA, Walter CU, Aljurf M. Allogeneic hematopoietic stem cell transplantation in adolescent and adult patients with high-risk T cell acute lymphoblastic leukemia. Biol Blood Marrow Transplant. 2012 Dec;18(12):1897-904. doi: 10.1016/j.bbmt.2012.07.011.
73
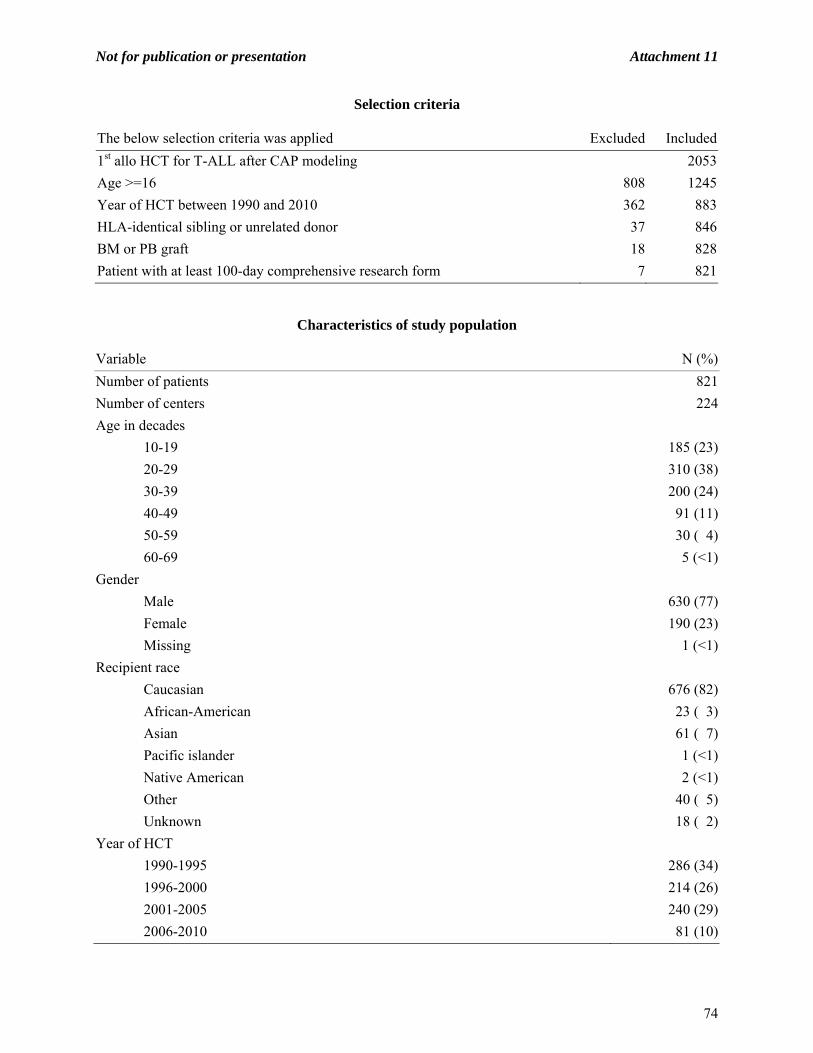
Not for publication or presentation Attachment 11
Selection criteria
The below selection criteria was applied Excluded Included
1st allo HCT for T-ALL after CAP modeling 2053
Age >=16 808 1245
Year of HCT between 1990 and 2010 362 883
HLA-identical sibling or unrelated donor 37 846
BM or PB graft 18 828
Patient with at least 100-day comprehensive research form 7 821
Characteristics of study population
Variable N (%)
Number of patients 821
Number of centers 224
Age in decades
10-19 185 (23)
20-29 310 (38)
30-39 200 (24)
40-49 91 (11)
50-59 30 ( 4)
60-69 5 (<1)
Gender
Male 630 (77)
Female 190 (23)
Missing 1 (<1)
Recipient race
Caucasian 676 (82)
African-American 23 ( 3)
Asian 61 ( 7)
Pacific islander 1 (<1)
Native American 2 (<1)
Other 40 ( 5)
Unknown 18 ( 2)
Year of HCT
1990-1995 286 (34)
1996-2000 214 (26)
2001-2005 240 (29)
2006-2010 81 (10)
74
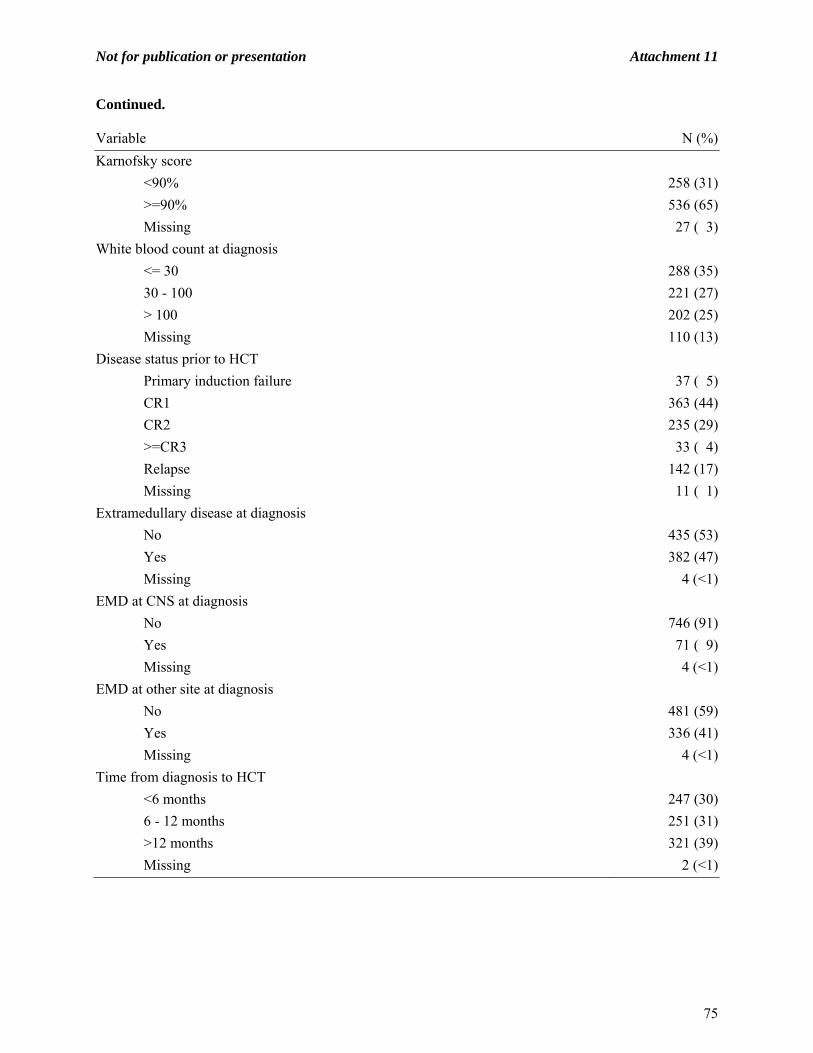
Not for publication or presentation Attachment 11
Continued.
Variable N (%)
Karnofsky score
<90% 258 (31)
>=90% 536 (65)
Missing 27 ( 3)
White blood count at diagnosis
<= 30 288 (35)
30 - 100 221 (27)
> 100 202 (25)
Missing 110 (13)
Disease status prior to HCT
Primary induction failure 37 ( 5)
CR1 363 (44)
CR2 235 (29)
>=CR3 33 ( 4)
Relapse 142 (17)
Missing 11 ( 1)
Extramedullary disease at diagnosis
No 435 (53)
Yes 382 (47)
Missing 4 (<1)
EMD at CNS at diagnosis
No 746 (91)
Yes 71 ( 9)
Missing 4 (<1)
EMD at other site at diagnosis
No 481 (59)
Yes 336 (41)
Missing 4 (<1)
Time from diagnosis to HCT
<6 months 247 (30)
6 - 12 months 251 (31)
>12 months 321 (39)
Missing 2 (<1)
75
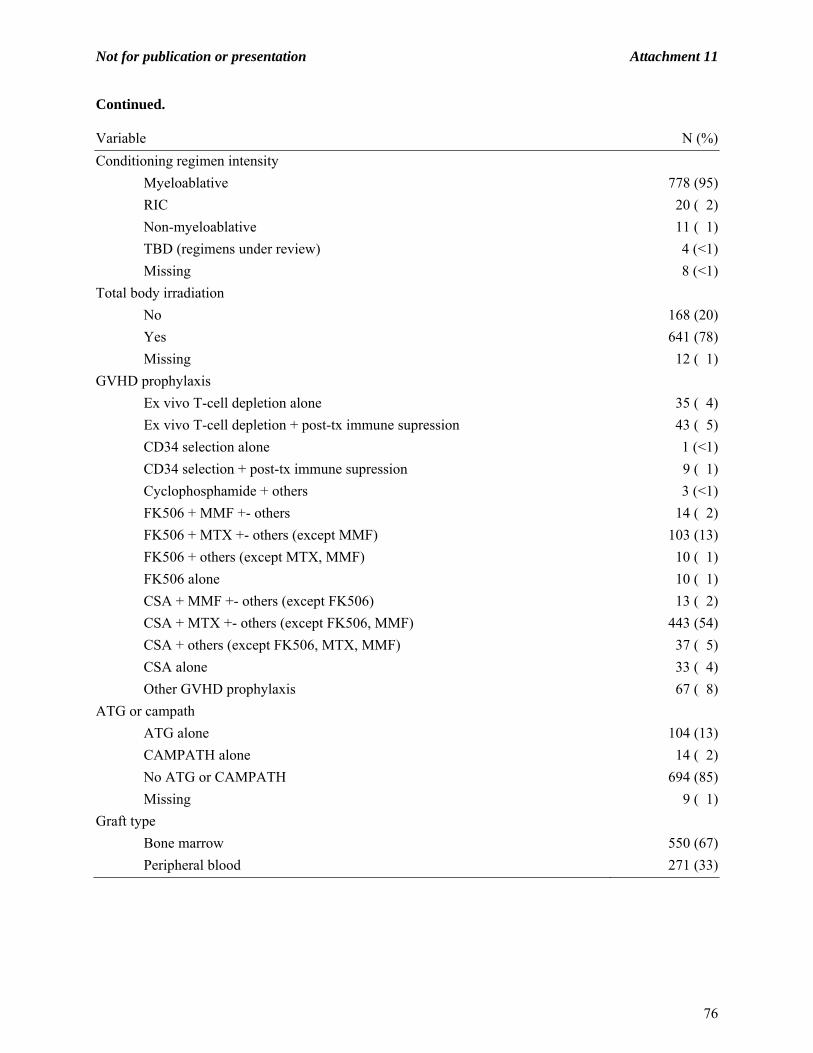
Not for publication or presentation Attachment 11
Continued.
Variable N (%)
Conditioning regimen intensity
Myeloablative 778 (95)
RIC 20 ( 2)
Non-myeloablative 11 ( 1)
TBD (regimens under review) 4 (<1)
Missing 8 (<1)
Total body irradiation
No 168 (20)
Yes 641 (78)
Missing 12 ( 1)
GVHD prophylaxis
Ex vivo T-cell depletion alone 35 ( 4)
Ex vivo T-cell depletion + post-tx immune supression 43 ( 5)
CD34 selection alone 1 (<1)
CD34 selection + post-tx immune supression 9 ( 1)
Cyclophosphamide + others 3 (<1)
FK506 + MMF +- others 14 ( 2)
FK506 + MTX +- others (except MMF) 103 (13)
FK506 + others (except MTX, MMF) 10 ( 1)
FK506 alone 10 ( 1)
CSA + MMF +- others (except FK506) 13 ( 2)
CSA + MTX +- others (except FK506, MMF) 443 (54)
CSA + others (except FK506, MTX, MMF) 37 ( 5)
CSA alone 33 ( 4)
Other GVHD prophylaxis 67 ( 8)
ATG or campath
ATG alone 104 (13)
CAMPATH alone 14 ( 2)
No ATG or CAMPATH 694 (85)
Missing 9 ( 1)
Graft type
Bone marrow 550 (67)
Peripheral blood 271 (33)
76

Not for publication or presentation Attachment 11
Continued.
Variable N (%)
Donor/Recipient CMV match
-/- 214 (26)
-/+ 194 (24)
+/- 102 (12)
+/+ 258 (31)
TBD 53 ( 6)
Type of donor
HLA-identical sibling 475 (58)
Unrelated TBD 346 (42)
Cause of death
Still alive 230 (28)
Primary disease 227 (28)
New malignancy 3 (<1)
GVHD 40 ( 5)
Idipathic pneumonia syndrome 64 ( 8)
Infection 79 (10)
Organ failure 64 ( 8)
Others 55 ( 7)
Missing 59 ( 7)
Median follow-up of survivors (range), months 84 (2-263)
77

Not for publication or presentation Attachment 12
Study Proposal 0712-04 Study Title: Allogeneic Transplantation for Acute Biphenotypic Leukemia (ABL): Disease Characteristics, Complications and Outcomes Reinhold Munker, MD, Louisiana State University Health Sciences Center-Shreveport, Shreveport, LA, [email protected] Specific Aims:
Describe frequency of allogeneic transplant for ABL, demographics and disease characteristics before transplant, describe outcomes of transplant for ABL
Scientific Justification: Over the last 35 years, the diagnosis and treatment of acute leukemias have made significant progress. Acute leukemias bearing markers of both myeloid and lymphoid origin were recognized many years ago (1). These leukemias are rare (2- 5% of all acute leukemias) and are considered as “puzzling” both with regard to their cell of origin as well as to the optimal treatment approach (2,3). In 1995, the European Group for the Immunologic Characterization of Leukemias (EGIL) established criteria for ABL where points were assigned to specific markers of B lymphoid, T lymphoid and myeloid origin. If a patient received more than 2 points from 2 different lineages, the diagnosis of ABL could be made (4). In 2008, the World Health Organization revised the criteria for lineage assignment and introduced the term of “mixed phenotype acute leukemia” (5). In the WHO classification, cases are excluded which could be classified under other cytogenetic or clinical categories. With the current refinements of molecular diagnostics all acute leukemias including ABL may ultimately be classified according to their molecular profile (6,7). In the pediatric age group, the prognosis of ABL is considered to be closer to acute myelogenous leukemia (AML) than to acute lymphoblastic leukemia (ALL) (8) or comparable with high-risk ALL (9) or intermediate between ALL and AML (10). In adults, only small case series were reported (11-17) with most but not all (15) cases having a poor prognosis. As far as allogeneic transplant is concerned, only a small series with pediatric patients has been published (18). Among adult patients, only sporadic cases treated with an allogeneic transplant were included in the references cited (11, 12, 13, 16, 17). There is an urgent need to define the role of allogeneic transplant for pediatric and adult ABL. Such a retrospective study will guide patients and physicians who benefits most from a transplant. Patient Eligibility Population:
All patients undergoing an allogeneic transplant between 1996 and 2012 with the primary diagnosis of acute biphenotyic leukemia (ABL) or a similar diagnosis (also described as acute leukemias of mixed phenotype and ambiguous origin)
Age limits: 0- 69 Transplant type: all allogeneic transplants, reduced or full intensity, bone marrow, peripheral
blood, cord blood, related, unrelated, radiation nor radiation-based conditioning regimens
78

Not for publication or presentation Attachment 12
Data Requirements: Data collection forms: “other acute leukemias “, supplementary data: to be determined. Type of chemotherapy given before transplant, disease status before transplant, exact marker and
genetic profile of ABL. Timing of SCT/ BMT, type of transplant. Outcome of transplant (overall survival, leukemia-free survival). Graft-versus host reactions, complications. Donor lymphocyte infusions (if applicable).
Sample Requirements: Not applicable at present. Study Design (Scientific Plan):
Describe the disease characteristics of ABL before transplant (WBC, marker profile, genetic profile if available, presence or absence of CNS involvement, mediastinal mass)
Will assess overall survival and survival free from disease Will assess complications of transplant including CNS relapse Will compare outcome with ALL and AML cohorts and develop statistical methods in
collaboration with CIBMTR biostatisticians
Variables to be Analyzed: Age: by decades Gender, ethnicity, performance score, graft source, conditioning regimen Year of transplant: 1996- 2001, 2002- 2007, 2008- present HLA-identity: HLA-identical family member, unrelated fully matched, partially matched
References:
1. Smith LJ, Curtis JE, Messner HA, et al. Lineage infidelity in acute leukemia. Blood 1983; 61: 1138- 45.
2. Weinberg OK and Arber DA. Mixed-phenotype acute leukemia: historical overview and a new definition. Leukemia 2010; 24: 1844- 51.
3. Steensma DP Oddballs: Acute leukemias of mixed phenotype and ambiguous origin.Hematol Oncol Clin N Am 2011; 25: 1235- 53.
4. Bene MC, Castoldi G, Knapp W et al. Proposals for the immunologic characterization of acute leukemias. European Group for the Immunologic Characterization of Leukemias (EGIL). Leukemia 1995; 9: 1783- 6.
5. Borowitz MJ, Bene MC, Harris NL, et al Acute leukaemias of ambiguous lineage. In Swerdlow SH, Campo E, Harris NL, et al. eds. World Health Organization (WHO) Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th Ed. Lyon (France): International Agency for Research on Cancer (IARC Press; 2008; p150- 5.
6. Zhao XF, Gojo I, York T et al. Diagnostics of biphenotypic acute leukemia: a paradigmatic approach. Int J Clin Exp Pathol 2010; 3: 75- 86.
7. Patel JP, Gönen M, Figueroa ME, et al. Prognostic relevance of integrated genetic profiling in acute myeloid leukemia. N Engl J Med 2012, 366: 1079- 89.
8. Rubnitz JE, Onciu M, Pounds S, et al. Acute mixed lineage leukemia in children: the experience of St Jude Children’s Research Hospital. Blood 2009; 113: 5083- 9.
9. Al-Seraihy AS, Owaidah TM, Ayas M, et al. Clinical characteristics and outcome of children with biphenotypic acute leukemia. 2009; 94: 1682- 90.
10. Gerr H, Zimmermann M, Schrappe M, et al. Acute leukaemias of ambiguous lineage in children: characterization, prognosis and therapy recommendations. Br J Haematol 2010; 149: 84- 92.
79

Not for publication or presentation Attachment 12
11. Legrand O, Perrot J-Y, Simonin G, et al. Adult biphenotypic acute leukaemia: an entity with poor prognosis which is related to unfavourable cytogenetics and P-glycoprotein over-expression. Br J Haematol 1998; 100:147- 55.
12. Killick S, Matutes E, Powles RL et al. Outcome of biphenotypic acute leukemia. Haematologica 1999; 84: 699- 706.
13. Rubio MT, Dhedin N, Boucheix C, et al. Adult T-biphenotypic acute leukaemia: clinical and biological features and outcome. Br J Haematol 2003; 123: 842- 9.
14. Weir EG, Al Ansari-Lari M, Batista DAS, et al. Acute bilineal leukemia: a rare disease with a poor outcome. Leukemia 2007; 21: 2264- 70.
15. Aribi A, Bueso-Ramos C, Estey E, et al. Biphenotypic acute leukaemia: a case series. Br J Haematol 2007; 138: 213- 6.
16. Mikulic M, Batinic D, Sucic M, et al. Biological features and outcome of biphenotypic acute leukemia: a case series. Hematol Oncol Stem Cell Ther 2008; 1: 225- 30.
17. Xu XQ, Wang JM, Lǚ SQ, et al. Clinical and biological characteristics of adult biphenotypic acute leukemia in comparison with that of acute myeloid leukemia and acute lymphoblastic leukemia: a case series of a Chinese population. Haematologica 2009; 94: 919- 27.
18. Park JA, Ghim TT, Bae KW, et al. Stem cell transplant in the treatment of childhood biphenotypic acute leukemia. Pediatr Blood Cancer 2009; 53: 444- 52.
80

Not for publication or presentation Attachment 12
Selection table The below selection criteria was applied # excluded NINCLUSION: 1st allo HCT for mixed-phenotype acute leukemia after CAP modeling 674Year range 1996-current 217 457Age <70 1 456Patient with at least 100-day comprehensive research form 175 281Patient consented for research 2 279EXCLUSION: Identical twin 1 278
Characteristics of patients who are under 70 years old and received 1st allogeneic transplant for mixed-phenotype acute leukemia after 1996
Variable N (%)Number of patients 278Number of centers 122Age
Median (range) 22 (1-68) <10 46 (17) 10-19 80 (29) 20-29 52 (19) 30-39 35 (13) 40-49 32 (12) 50-59 24 ( 9) 60-69 9 ( 3)Gender Male 159 (57) Female 119 (43)Ethnicity Hispanic or Latino 32 (12) Non-Hispanic or Non-Latino 122 (44) Non-resident of the U.S. 109 (39) Missing 15 ( 5)Karnofsky score <90% 64 (23) >=90% 206 (74) Missing 8 ( 3)
81

Not for publication or presentation Attachment 12
Continued. Variable N (%)Disease status prior to HCT Primary induction failure 19 ( 7) CR1 193 (69) CR2 37 (13) >=CR3 4 ( 1) Relapse 21 ( 8) Missing 4 ( 1)Time from diagnosis to HCT, median (range) 5 (<1-276)Graft Type Bone Marrow 112 (40) Peripheral blood 104 (37) Cord blood 62 (22)Type of donor HLA-identical sibling 133 (48) Other related 16 ( 6) Unrelated TBD 128 (46) Missing 1 (<1)Total body irradiation No 92 (33) Yes 185 (67) Missing 1 (<1)Conditioning regimen intensity Myeloablative 246 (88) RIC 16 ( 6) Non-myeloablative 13 ( 5) TBD (regimens under review) 2 (<1) Missing 1 (<1)Year of HCT 1996-2000 67 (24) 2001-2005 92 (33) 2006-2010 109 (39) 2011-current 10 ( 4)Median follow-up of survivors (range), months 48 (2-160)
82

Not for publication or presentation Attachment 13
Study Proposal 1112-26 Study Title: The impact of peripheral blood chimerism on transplant outcomes in patients with acute leukemia and myelodysplastic syndrome Partow Kebriaei, MD, M.D. Anderson Cancer Center, Houston, TX, [email protected] Richard Champlin, MD, M.D. Anderson Cancer Center, Houston, TX, [email protected] Specific Aims: Primary:
Assess the impact of persistent mixed chimerism at 3 months following allogeneic hematopoietic stem cell transplantation (SCT) on the rate of relapse post SCT
Assess the impact of persistent mixed chimerism on the rate of graft versus host disease (GVHD)
Secondary: Describe the kinetics of donor chimerism in the first year following transplant
Scientific Justification: The association of mixed chimerism and disease relapse following allogeneic SCT remains unclear with some studies suggesting increased of risk of relapse (1-3), and others not (4-6). The disease type, transplant conditioning, and kinetics of the mixed chimerism likely contribute to the disparate study results. A better understanding of the impact of mixed chimerism is key as we continue to try to identify groups of patients who may benefit from early intervention to minimize the risk for relapse following SCT. Using the registry database with large patient numbers may allow us to better delineate the independent effects of variables, such as SCT conditioning intensity, which is not feasible in small single center reports. Patient Eligibility Population: Patients with AML, MDS, ALL who received a T cell replete allograft with peripheral blood or bone marrow cells with available chimerism data at 3 months post SCT. Data Requirements: Data collected from standard chimerism forms. Peripheral blood T-lineage and myeloid chimerism analysis at 30 days (+/- 2 weeks), 3 months (+/- 1 month), 6 months (+/- 1 month) and 12 months (+/-1 month) following allogeneic SCT. Sample Requirements: None
Study Design: Primary outcomes: chimerism at 3 months, engraftment, incidence of acute and chronic
GVHD, progression, death. Secondary outcomes: chimerism data at 30 days, 6 months and 12 months post SCT
Study Variables: Patient:
Age at SCT, gender, diagnosis, disease status at SCT, cytogenetic risk (high vs. intermediate vs. low) CMV status prior to SCT.
Donor: Stem cell source, total nucleated cell count (TNC), CD34, degree of HLA match, CMV
status.
83

Not for publication or presentation Attachment 13
Transplant: Myeloablative / nonmyeloablative / RIC, GVHD prophylaxis regimen
Study Design: Univariate and multivariate analysis comparing outcomes of patients with mixed donor chimerism at 3 months versus those that do not with respect to engraftment, rates of GVHD, and relapse. We will look at mixed chimerism as a discrete variable at 3months, as well as a continuous variable within the first year following transplant. References:
1. Bader P, Kreyenberg H, Hoelle W, Dueckers G, Kremens B, Dilloo D et al. Increasing mixed chimerism defines a high-risk group of childhood acute myelogenous leukemia patients after allogeneic stem cell transplantation where pre-emptive immunotherapy may be effective. Bone marrow transplant 2004; 33: 815–821. | Article | PubMed | ISI | CAS |
2. Bader P, Kreyenberg H, Hoelle W, Dueckers G, Handgretinger R, Lang P et al. Increasing mixed chimerism is an important prognostic factor for unfavorable outcome in children with acute lymphoblastic leukemia after allogeneic stem-cell transplantation: possible role for pre-emptive immunotherapy? J Clin Oncol 2004; 22: 1696–1705.
3. Hans C. Lee, MD, Rima M. Saliba, Ph.D., Gabriela Rondon, MD, Julianne Chen, Yasmeen Charafeddine, L. Jeffrey Medeiros, MD, Marcos De Lima, MD, Borje S Andersson, MD, PhD, Partow Kebriaei, M.D., Betul Oran, MD, MS and Richard E. Champlin. Early Mixed T-Lymphocyte and Myeloid Chimerism Is Predictive of Disease Recurrence Following Allogeneic Stem Cell Transplantation for AML/MDS, ASH 2012, Atlanta, Georgia.
4. van Besien K, Dew A, Lin S, Joseph L, Godley LA, Larson RA, Odenike T, Rich E, Stock W, Wickrema A, Artz AS. Patterns and kinetics of T-cell chimerism after allo transplant with alemtuzumab-based conditioning: mixed chimerism protects from GVHD, but does not portend disease recurrence. Leuk Lymphoma. 2009 Nov;50(11):1809-17.
5. Alimoghaddam K, Ghaffari H, Foroughi F, Chardouli B, Sanaat Z, Bahar B, Mousavi A, Iravani M, Ghavamzadeh A. Effects of chimerism on graft-versus-host disease, disease recurrence, and survival after HLA-identical marrow transplantation in Iran. Arch Iran Med. 2006 Apr;9(2):99-103.
6. Prognostic value of hematopoietic chimerism in patients with acute leukemia after allogeneic bone marrow transplantation: a prospective study. Choi SJ, Lee KH, Lee JH, Kim S, Chung HJ, Lee JS, Kim SH, Park CJ, Chi HS, Kim WK. Bone Marrow Transplant. 2000 Aug;26(3):327-32.
84

Not for publication or presentation Attachment 13
Selection criteria
The following selection criteria was applied Excluded Included
INCLUSION:
1st allo HCT for AML/ALL/MDS with BM/PB graft, after CAP modeling 41069
T-cell replete graft 3431 37638
Patient consent 1310 36328
Patient with at least 100-day comprehensive research form 212 36116
EXCLUSION:
Legacy patients (chimerism data not available) 29854 6262
Characteristics of study population Variable N (%)
Number of patients 6262
Number of centers 223
Age
<10 286 ( 5)
10-19 436 ( 7)
20-29 650 (10)
30-39 665 (11)
40-49 1159 (19)
50-59 1764 (28)
60-69 1181 (19)
>=70 120 ( 2)
Missing 1 (<1)
Gender
Male 3491 (56)
Female 2768 (44)
Missing 3 (<1)
Karnofsky score
<90% 1973 (32)
>=90% 4006 (64)
Missing 283 ( 5)
Disease at diagnosis
AML 3704 (59)
ALL 963 (15)
MDS 1595 (25)
85

Not for publication or presentation Attachment 13
Continued. Variable N (%)
Disease status (for acute leukemias/CML/MDS/LYM)
Early 3125 (50)
Intermediate 1096 (18)
Advanced 1661 (27)
Unknown 380 ( 6)
Chimerism tested
single donor test date 0-100 days
No 1588 (25)
Yes 4674 (75)
single donor test date 100 days-6 mos
No 3492 (56)
Yes 2770 (44)
single donor test date 6-12 mos
No 3732 (60)
Yes 2530 (40)
single donor test date 12-24 mos
No 4440 (71)
Yes 1822 (29)
single donor test date > 24 mos
No 5857 (94)
Yes 405 ( 6)
Cytogenetic abnormalities
Normal 1537 (25)
Favorable 242 ( 4)
Intermediate 624 (10)
Poor 1458 (23)
TBD (need review) 659 (11)
Missing (not available for ALL patients) 1742 (28)
Graft Type
Bone Marrow 1355 (22)
Peripheral blood 4907 (78)
86

Not for publication or presentation Attachment 13
Continued.
Variable N (%)
Type of donor
HLA-identical sibling 2095 (33)
Identical twin 4 (<1)
Other related 95 ( 2)
Unrelated TBD 4012 (64)
Missing 56 (<1)
Donor/recipient CMV match
-/- 1675 (27)
-/+ 1803 (29)
+/- 699 (11)
+/+ 1741 (28)
TBD 344 ( 5)
Conditioning regimen intensity
Myeloablative 4024 (64)
RIC 1495 (24)
Non-myeloablative 532 ( 8)
TBD (regimens under review) 176 ( 3)
Missing 35 (<1)
GVHD prophylaxis
CD34 selection alone 37 (<1)
CD34 selection + post-tx immune supression 51 (<1)
Cyclophosphamide alone 31 (<1)
Cyclophosphamide + others 37 (<1)
FK506 + MMF +- others 864 (14)
FK506 + MTX +- others (except MMF) 3099 (49)
FK506 + others (except MTX, MMF) 354 ( 6)
FK506 alone 132 ( 2)
CSA + MMF +- others (except FK506) 400 ( 6)
CSA + MTX +- others (except FK506, MMF) 945 (15)
CSA + others (except FK506, MTX, MMF) 68 ( 1)
CSA alone 101 ( 2)
Other GVHD prophylaxis 143 ( 2)
87

Not for publication or presentation Attachment 13
Continued.
Variable N (%)
Year of HCT
2007 1659 (26)
2008 1584 (25)
2009 1445 (23)
2010 997 (16)
2011 491 ( 8)
2012 86 ( 1)
Median follow-up of survivors (range), months 36 (<1-67)
88