nonextraction treatment of an open bite with microscrew...
TRANSCRIPT

CASE REPORT
Nonextraction treatment of an open bite withmicroscrew implant anchorageHyo-Sang Park,a Oh-Won Kwon,b and Jae-Hyun Sungc
Daegu, South Korea
A 16-year-old girl with an anterior open bite was treated with nonextraction therapy that included intrusionof the maxillary and mandibular posterior teeth with microscrew implants. Implants (diameter, 1.2 mm;length, 8 or 6 mm) were placed into alveolar bone near the posterior teeth and used as anchorage for intrusiveforce. To prevent adverse side effects of buccoversion or linguoversion of the posterior teeth during intrusion,a transpalatal bar and a lingual arch were placed. The 3-mm anterior open bite was corrected in 11 monthsof treatment, after intrusion of the maxillary and mandibular posterior teeth and autorotation of the mandible.The posterior intrusion relapsed in the early stage of retention, at 8 months; thereafter, no obvious relapsewas evident in the vertical position of the molars and the FMA. The treatment mechanics of anterior open bitewith posterior intrusion by using microscrew implants were effective but still require a proper retention
protocol. (Am J Orthod Dentofacial Orthop 2006;130:391-402)Open bite malocclusion has long been consid-ered one of the most difficult orthodonticproblems to correct because its etiology is
complicated and multifactorial.1,2 Therapies includemodification of functional or habitual aberrations, or-thopedic treatment, orthognathic surgery, and orth-odontic treatment with extrusion of the anterior teeth orintrusion of the posterior teeth.
Until recently, orthognathic surgery was consideredthe treatment of choice for a severe skeletal open bite.3
The advent of skeletal anchorage has expanded theboundaries of orthodontic treatment.4,5 Skeletal anchor-age can produce treatment outcomes that cannot beobtained by conventional orthodontic treatment butonly from orthognathic surgery. In an earlier report, weshowed that the maxillary incisors can be retracted 14mm against microscrew implants. This is beyond thelimit of orthodontic treatment.6
Molar intrusion was challenging to orthodontistsbefore the development of skeletal anchorage. Skel-etal anchorage, including dental implants,7 surgicalminiplates,5,8 and miniscrew or microscrew im-plants,4,6,9 is now growing in popularity because ofthe ability to provide absolute anchorage. The intru-
From the Department of Orthodontics, School of Dentistry, KyungpookNational University, Daegu, South Korea.aAssociate professor.bProfessor.cHonorary professor.Reprint requests to: Hyo-Sang Park, Department of Orthodontics, School ofDentistry, Kyungpook National University, 101, Dongin-2-Ga, Jung-Gu,Daegu, South Korea 700-422; e-mail, [email protected], March 2005; revised and accepted, July 2005.0889-5406/$32.00Copyright © 2006 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2005.07.014sion of molars with skeletal anchorage produces auto-rotation of the mandible; this resembles the treatmentresults of maxillary surgical impaction.
In terms of surgical procedure and costs, micro-screw implants are superior to dental implants and theminiplate system. Microscrew implants are smallenough to be placed into the alveolar bone, easy toplace and remove surgically, and economical comparedwith other products. These advantages have expandedtheir clinical applications to many clinical situa-tions.9-15 Treatment of anterior open bite after intrusionof molars with miniplates has been reported5,8 but notwith microscrew implants.
This case report describes the treatment mechan-ics for anterior open bite with microscrew implants,treatment planning, treatment procedure, and reten-tion.
DIAGNOSIS
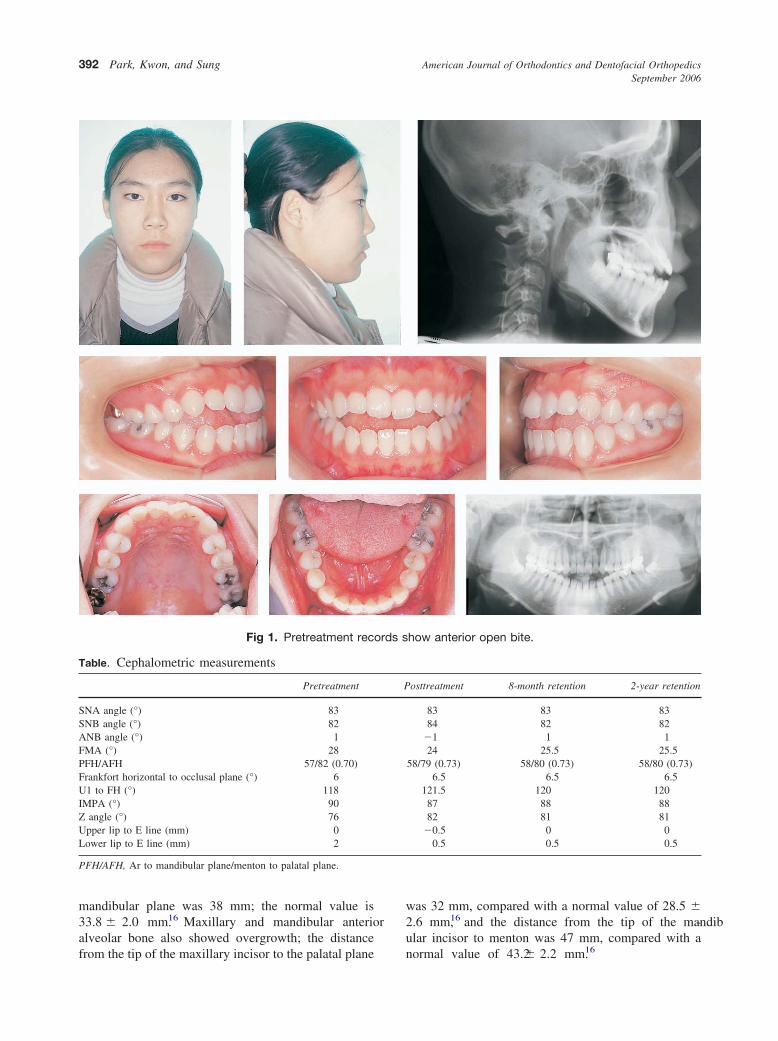
A 16-year-old girl with an anterior open bite and astraight profile came for treatment (Fig 1). Cephalomet-ric analysis showed an ANB angle of 2°, and amandibular plane angle (FMA) of 28° (Table). She had3 mm of overjet and an anterior open bite of –3 mm,and was diagnosed with a skeletal Class I open-bitemalocclusion.
There was no family history of open bite. Theetiology of open bite was assumed to be overgrowth ofthe maxillary and mandibular alveolar bone. The per-pendicular distance from the mesial cusp tip of themaxillary first molar to the palatal plane was 30 mm;the normal value is 24.2 � 1.9 mm for same age groupof Korean girls.16 The perpendicular distance from the
mesial cusp tip of the mandibular first molar to the391
ords s
American Journal of Orthodontics and Dentofacial OrthopedicsSeptember 2006
392 Park, Kwon, and Sung
mandibular plane was 38 mm; the normal value is33.8 � 2.0 mm.16 Maxillary and mandibular anterioralveolar bone also showed overgrowth; the distance
Fig 1. Pretreatment rec
Table. Cephalometric measurements
Pretreatment
SNA angle (°) 83SNB angle (°) 82ANB angle (°) 1FMA (°) 28PFH/AFH 57/82 (0.70)Frankfort horizontal to occlusal plane (°) 6U1 to FH (°) 118IMPA (°) 90Z angle (°) 76Upper lip to E line (mm) 0Lower lip to E line (mm) 2
PFH/AFH, Ar to mandibular plane/menton to palatal plane.
from the tip of the maxillary incisor to the palatal plane
was 32 mm, compared with a normal value of 28.5 �2.6 mm,16 and the distance from the tip of the mandib-ular incisor to menton was 47 mm, compared with a
how anterior open bite.
osttreatment 8-month retention 2-year retention
83 83 8384 82 82
�1 1 124 25.5 25.5
58/79 (0.73) 58/80 (0.73) 58/80 (0.73)6.5 6.5 6.5
121.5 120 12087 88 8882 81 81
�0.5 0 00.5 0.5 0.5
P
normal value of 43.2 � 2.2 mm.16

tment
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 130, Number 3
Park, Kwon, and Sung 393
Intraorally, the patient had Class I canine and molarrelationships (Fig 2). The posterior area had a consid-erable mesial inclination, especially at the mandibularteeth, and there was no occlusal contract from firstpremolar to the other side. Arch-length discrepancies inthe maxillary and mandibular arches were 3 and 0 mm,respectively. The patient had a lowered tongue postureand a flat sound during speech. The tongue was thrustthrough an interincisal gap during swallowing.
TREATMENT OBJECTIVES
Six treatment objectives were identified: (1) main-tain facial balance, (2) intrude maxillary and mandib-ular posterior teeth in the alveolar bone which showedexcessive overgrowth, (3) establish ideal overbite andoverjet, (4) resolve crowding, (5) eliminate the tongue-thrust habit, and (6) strengthen masticatory muscle toneto improve retention.
TREATMENT ALTERNATIVES
The first treatment option was to use microscrewimplants to intrude the posterior teeth in both archesand close the anterior open bite. The ease of thesurgical procedure and the expected good treatmenteffects led the patient to choose this option.
The second alternative was multiloop edgewisearchwire therapy. Its treatment effects include extrusionof anterior teeth and uprighting of posterior teeth.2
Because of a tendency for more relapse of extrusionthan intrusion in young patients,17 the complexity ofwire bending, and the requirement for elastics, this
Fig 2. Pretrea
option was declined.
The third alternative was segmental maxillary pos-terior impaction surgery. Surgical segmental impactionof the posterior teeth was necessary to obtain autorota-tion of the mandible and closure of the anterior openbite. Presurgical orthodontic treatment would need toinclude alignment of the crowded anterior teeth andcreation of space between the canines and the premo-lars for surgical osteotomy of the posterior maxilla.
The fourth alternative was total maxillary impac-tion surgery. The superior impaction of the maxillacould also produce autorotation of the mandible andobtain a positive anterior bite. The patient declinedthese 2 alternatives because of the extensive surgicalprocedures.
TREATMENT PLANNING
Because the patient had an acceptable profile andminimal arch-length discrepancies, nonextraction treat-ment was planned. The anterior bite would be closed byintruding the posterior teeth rather than extruding theanterior teeth, because this procedure is reportedlymore prone to relapse.17 In this patient, the anterior andposterior dental heights were excessive compared withKorean norms.16 Intruding the posterior teeth seemedmore rational than extruding the anterior teeth. Micro-screw implants would be placed in the posterior alve-olar bone to provide anchorage to intrude and uprightthe posterior teeth.
To establish a precise treatment plan and to calcu-late the exact amount of tooth movement, mounteddiagnostic casts were used. After mounting the casts on
dental casts.
an articulator, the heights of the cusp tips from the base

r incis
American Journal of Orthodontics and Dentofacial OrthopedicsSeptember 2006
394 Park, Kwon, and Sung
of the articulator were measured (Fig 3). The provi-sional amount of intrusion was marked on the casts.The maxillary posterior tooth segment was cut andpositioned superiorly 2 mm. The next step was upright-ing and slightly intruding the mandibular posteriorteeth. The decision about the amount of intrusion wasmade on the basis of maintaining the cant of theocclusal plane. The alignment of the anterior teeth canbe followed. It was decided that the maxillary anteriorteeth needed to be aligned with a slight labioversion,and the mandibular anterior teeth needed to tip distally.Because the vertical position of the maxillary incisorswas different from that of the canines, the maxillaryincisors were extruded to the level of the occlusalplane.
Biomechanics of open-bite treatment withmicroscrew implants
Treatment planning steps included fabrication ofdiagnostic setup casts with articulator mounting. In the
Fig 3. Diagnostic setup: A, height of cusp meaposterior teeth; C, uprighting and intrusion of manterior teeth and lingual tipping of mandibula
diagnostic setup, the maxillary and mandibular molars
should be intruded until a suitable amount of anterioroverbite is achieved. During molar intrusion, the max-illary and mandibular anterior teeth will come intocontact with each other. To prevent trauma from theocclusal contact and to increase overbite and overjet,the mandibular incisors should be retracted or themaxillary incisors proclined. These procedures can besimplified by grinding off the crowns of the posteriorteeth in the mounted casts. When deciding on theproclination of the maxillary incisor, the facial profileshould be considered. If distal retraction of the maxil-lary anterior teeth is needed to improve the profile,distal force can be applied from the maxillary micro-screw implants to the canines. In this situation, themandibular anterior teeth need more retraction thanplanned distal movement to facilitate the overjet andoverbite increase.
Treatment mechanics include intruding and up-righting the posterior teeth. The maxillary microscrewimplants can be placed into palatal alveolar bone
on mounted models; B, intrusion of maxillaryular posterior teeth; D, alignment of maxillary
ors to finalize occlusion.
suredandib
between the first and second molars, and the mandib-

nterio
s clos
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 130, Number 3
Park, Kwon, and Sung 395
ular microscrew implants in the buccal alveolar bone.The intrusion force applied on either the buccal or thepalatal side might produce buccoversion or linguover-sion of the posterior teeth. This movement can beprevented by placing a transpalatal bar or a lingual arch
Fig 4. Biomechancis showing closing of a
Fig 5. A, Placement of microscrew implants imolars. Intrusive force was applied from microto prevent linguoversion of maxillary molars. Bsecond molars from which intrusive force was amolars. C, At 8 months, anterior open bite wa
(Fig 4). The outcomes of intrusion force include intru-
sion of the posterior teeth, which results in passiveclosure of the mandibular plane and correction of theanterior open bite, and the side effects of buccoversionor linguoversion of the posterior teeth. Because adversetooth movement is controlled during intrusion by a
r open bite after intrusion force at molars.
latal alveolar bone between first and secondimplants to hooks on transpalatal bar, placedscrew implants between mandibular first and
d, and lingual arch to prevent buccal tipping ofed.
nto pascrew, Micropplie
transpalatal bar and a lingual arch, the posterior teeth

nt rec
American Journal of Orthodontics and Dentofacial OrthopedicsSeptember 2006
396 Park, Kwon, and Sung
can be intruded even with a light archwire. Therefore,the intrusion of the posterior teeth and the alignment ofthe anterior teeth can be performed at the same timeduring the early stage of treatment.
Intrusion of the posterior teeth induces counter-clockwise autorotation of the mandible, which closesthe anterior open bite. To facilitate this, the microscrewimplants need to be placed into the bone distal to thecenter of resistance of the whole dentition. The intru-sive force distal to the center of resistance effectivelyproduces a clockwise moment on the maxillary denti-tion and a counterclockwise moment on the mandibulardentition. These moments efficiently contribute to clo-sure of the anterior open bite. To prevent traumaticocclusal contact of the anterior teeth, it might benecessary to retract the mandibular dentition distally.This can be performed by applying force from the
Fig 6. Posttreatme
microscrew implants to the mandibular canines or
premolars while the anterior tooth segment is ligatedtogether. This distal movement helps to deepen theanterior overbite.
TREATMENT PROGRESS
A microscrew implant (diameter, 1.2 mm; length, 8mm; Osteomed, Addison, Tex) was placed into thepalatal alveolar bone between the maxillary first andsecond molars on both sides (Fig 5, A) . A mandibularmicroscrew implant (diameter, 1.2 mm; length, 6 mm;Osteomed) was placed into the buccal alveolar bonebetween the mandibular first and second molars (Fig 5, B).Detailed surgical procedures were illustrated and dis-cussed in previous reports.10,11 To prevent linguover-sion of the maxillary posterior teeth during intrusiveforce applied on the palatal side, a transpalatal bar wasplaced. A mandibular lingual arch was used to prevent
ords (11 months).
buccoversion of the mandibular posterior teeth during

American Journal of Orthodontics and Dentofacial OrthopedicsVolume 130, Number 3
Park, Kwon, and Sung 397
intrusive force application. A .022-in fixed preadjustededgewise appliance was banded and bonded, and a .016nickel-titanium archwire was placed. After 1 month oftreatment, an intrusive force of 100 g was applied topalatal hooks that extended from the transpalatal barand to the buccal tube welded on the mandibular firstmolars on each side. At 4 months of treatment, theanterior teeth were aligned and .017 � .025-in beta-titanium alloy archwires were placed. At 6 months oftreatment, .017 � .025-in stainless steel archwires wereplaced, and intrusive forces were applied continuously.At 8 months of treatment, the anterior open bite wasclosed with autorotation of the mandible (Fig 5, C). Theintrusive forces were applied continuously even afterclosing to overcorrect the anterior open bite.
The patient was instructed to clench her posteriorteeth while swallowing and to push her tongueagainst her hard palate. This was to increase masti-catory muscle force and correct her tongue thrusthabit.
After 11 months of treatment, the treatment wasfinished with a normal overbite of the anterior teethand a slight disclusion of the posterior teeth. Thedisclusion in the posterior teeth was created forovercorrection. After treatment, lingual retainerswere bonded from first premolar to first premolar inthe mandibular arch and from canine to canine in themaxillary arch, and an additional maxillary circumferen-
Fig 7. Posttrea
tial retainer was delivered.
All microscrew implants stayed firm throughout thetreatment. After treatment, they were removed byunscrewing without anesthesia.
TREATMENT RESULTS
A 1.5-mm overbite was obtained after intrusion ofthe maxillary and mandibular molars (Figs 6 and 7).The mandible showed autorotational closure; accord-ingly, the FMA was reduced from 28° to 24°. Theocclusal plane showed little change, but it steepenedslightly (0.5°) after more intrusion of the maxillarymolars than the mandibular molars. The posterior teethshowed disclusion at debonding; this was left to over-come the expected relapse of the posterior intrusion.The facial profile changes were not conspicuous. ClassI canine and molar relationships were obtained. Therewas no obvious evidence of root resorption.
To prevent relapse of the intruded posterior teeth, avertical chincap was provided, and chewing exerciseswere prescribed to strengthen the masticatory muscles.Lingual retainers were bonded canine to canine in themaxillary arch and first premolar to first premolar in themandibular arch.
In the retention process, the disclusion on theposterior teeth settled down quickly after 2 months ofretention. At 8 months of retention, there was a loss ofanterior tooth contact—a minimal amount of relapse(Fig 8). To obtain the anterior contact, lingual buttons
t dental casts.
tmenwere bonded to the maxillary central incisors and

American Journal of Orthodontics and Dentofacial OrthopedicsSeptember 2006
398 Park, Kwon, and Sung
canines and the mandibular canines and first premolars,and vertical elastics were used to obtain best fit of theocclusion. Because of the lingual bonded retainers,there were no obvious side effects. After a month ofelastic use, the buttons were removed. To maintain theangulation of the canines, labial fixed retainers werebonded between the canines and the premolars in themaxillary arch. Tongue exercises were prescribed dur-ing the retention period. Two-year retention recordsshowed good retention without obvious relapse (Figs 9and 10).
The pretreatment and posttreatment cephalomet-ric superimposition (Fig 11) showed the uprightingand intrusion of the posterior teeth and resultantautorotational closure of the mandible. The maxillaryincisors showed slight labioversion, and the mandib-
Fig 8. Retention
ular incisors were tipped lingually. The intruded
posterior teeth showed a slight relapse in the super-imposition between posttreatment and 8-month re-tention (Fig 12). The reason for this might be loss ofocclusal contact between the maxillary and mandib-ular posterior teeth or a relapse tendency of theintrusion. Accordingly, the mandibular plane showeda slight opening during the first 8 months of reten-tion. After that, there was no change in the FMA andvertical position of the posterior teeth between the8-month and the 2-year retention superimpositions(Fig 13).
DISCUSSION
The bite closed rapidly with progressive intrusionof the posterior teeth in both arches. It took only 8months to obtain a positive overbite. The application of
ds at 8 months.
recoran intrusive force distal to the center of resistance of the

ar ret
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 130, Number 3
Park, Kwon, and Sung 399
dentition produced a clockwise moment at the maxil-lary dentition and a counterclockwise moment at themandibular dentition. These movements were effectivein closing the anterior open bite. Small vertical changesat the posterior teeth can produce profound changes inthe anterior area. Only 1 mm intrusion at the posteriorteeth can produce 3 to 4 mm forward and upwardmovement of the chin.18
Passive anterosuperior movement of the anteriorteeth during autorotation was predicted on the assump-
Fig 9. Two-year re
Fig 10. Two-ye
tion that the center of the condyle was the rotational
axis of the mandibular autorotation. The rotational axisof the mandible has been reported as variable inmaxillary surgical impaction.19 Therefore, the amountof passive anterior movement of the mandibular inci-sors during autorotation can differ from patient topatient. It is impossible to predict these changes intreatment planning; decisions must be made duringtreatment to accommodate them. If there is moreforward movement of the mandibular incisors duringautorotation than expected, they should be retracted
n intraoral photos.
ention models.
tentio
more, or the maxillary incisors should be moved

American Journal of Orthodontics and Dentofacial OrthopedicsSeptember 2006
400 Park, Kwon, and Sung
forward; the facial profile should be considered whendeciding between the 2.
Open bite is a difficult malocclusion correction toretain. To minimize relapse in this patient, the posteriorteeth were intruded to an overcorrected vertical posi-tion. The overcorrected intrusion, however, quickly
Fig 11. Pretreatment and posttre
Fig 12. Posttreatment and 8-month
settled because of lack of occlusal contact. This might
be explained by the absence of occlusal contact in theposterior segment after treatment or the relapse ten-dency of intruded molars in the early stage of retention.
When evaluating the treatment results retrospec-tively, if we retract the mandibular dentition moredistally, we can obtain greater overjet and overbite.
t cephalometric superimposition.
tion cephalometric superimposition.
atmen
reten
This might help minimize clinical relapse in overbite

American Journal of Orthodontics and Dentofacial OrthopedicsVolume 130, Number 3
Park, Kwon, and Sung 401
treatment. As we mentioned before, the posterior teethhad settled at 2 months of retention. Even after meetingthe opposing teeth, the posterior teeth had a slightadditional relapse until the FMA was opened by 1.5° at8 months of retention. The FMA’s initial 28° wasreduced to 24° by autorotation of the mandible afterposterior intrusion, and it rebounded to 25.5° during 8months of retention. After that, there was no change inthe vertical position of the posterior teeth or the FMA.A report by Sugawara et al20 showed that one third ofmandibular molar intrusions relapse during the firstyear of retention. They suggested that overcorrectionmight be a way to overcome relapse. Because of theshort treatment time, there was no time for retention ofthe posterior intrusion during treatment. A prolongedtreatment time might be helpful. Maintaining the mi-croscrew implants for a while after treatment might berecommended. Not only during treatment, but alsoduring retention, muscle exercises should be prescribedto equalize the functional force. The development of aproper retention protocol for molar intrusion in open-bite treatment is a task for the future.
A reason for placing the microscrew implants intobuccal alveolar bone in the mandibular arch is toprovide better accessibility. Furthermore, the possibil-ity of tongue irritation with lingually placed micro-screw implants supports their placement into the buccalalveolar bone. The mandibular buccal alveolar bone ismore than 3 mm thick and is thus a good site formicroscrew implant placement.21,22 Three-millimeter
Fig 13. Eight-month and 2-year re
thick alveolar cortical bone and a 10° to 20° angular
placement of the microscrew implant were determinedto be important factors for preventing root damage. Byplacing the microimplants with angulations, clinicianscan increase the implant surface area that is in contactwith cortical bone. Six-millimeter microscrew implantscan be placed in the cortical bone.
The distance between roots of the maxillary firstand second molars is much smaller on the buccal sidethan on the palatal, 22 because the molars have 2buccal roots and 1 palatal root. Additionally, the firmmasticatory palatal mucosa, which has a strongresistance to inflammation, might support microim-plants placed into the palatal alveolar bone. The softtissue is thick in the palate and varies from site tosite. The thickness of the soft tissue should bemeasured, and the length of the microimplantsshould be selected to compensate for soft-tissue thick-ness and to provide a suitable length of bone contact.The new microimplants designed for palatal placementare longer than those designed for buccal placement.23
The implants used in this study were surgicalmicroscrews that do not have a special attachment onthe head for elastic materials. A ligature wire hook wastwisted onto the neck of the screw and bent to form a hookto connect the elastics. The new microimplant system hasa button on the head for attaching elastics, which providebetter versatility for orthodontic treatment.23
The forces applied from the buccal and palatal sidesproduce third-order problems in the posterior toothsegment. A transpalatal bar and a lingual arch were
n cephalometric superimposition.
tentioplaced to prevent torque problems. There were differ-

American Journal of Orthodontics and Dentofacial OrthopedicsSeptember 2006
402 Park, Kwon, and Sung
ences in third-order forces between the maxillary firstand second molars during treatment, because the sec-ond molars were not connected to the transpalatal bar,and the palatal intrusive force was transmitted buccallythrough the archwire to the second molars. This forceproduced buccal tipping of the second molars. The firstmolars connected with the transpalatal bar did not tipduring intrusion. To correct torque differences betweenthe first and second molars, lingual cleats were attachedon the palatal surface of the second molars, and anintrusion force was applied from the microscrew im-plants. To minimize torque discrepancy in the posteriorteeth, the transpalatal bar and the lingual arch can beextended from the first to the second molars (Fig 4).
CONCLUSIONS
Microscrew implants can provide suitable anchor-age for intrusion of the maxillary and mandibularposterior segment. This produces rapid closure of ananterior open bite along with mandibular autorotation.The treatment mechanics for correcting anterior openbite with microscrew implants are effective. However,even with overcorrection and several methods of reten-tion, there is still concern about retention, and a properretention protocol should be developed.
REFERENCES
1. Speidel TM, Isaacson RJ, Worms FW. Tongue-thrust therapyand anterior dental openbite. Am J Orthod 1972;62:287-95.
2. Kim YH. Anterior openbite and its treatment with multiloopedgewise archwire. Angle Orthod 1987;57:290-321.
3. Epker BN, Fish LC. Surgical-orthodontic correction of open-bitedeformity. Am J Orthod 1977;71:278-99.
4. Creekmore TD. The possibility of skeletal anchorage. J ClinOrthod 1983;17:266-9.
5. Umemori M, Sugawara J, Mitani H, Nagasaka H, Kawamura H.Skeletal anchorage system for open bite correction. Am J OrthodDentofacial Orthop 1999;115:166-74.
6. Park HS, Kwon TG. Sliding mechanics with microscrew implantanchorage. Angle Orthod 2004;74:703-10.
7. Shapiro PA, Kokich VG. Uses of implants in orthodontics. Dent
Clin North Am 1988;32:539-50.8. Sherwood KH, Burch JG, Thompson WJ. Closing anterior openbites by intruding molars with titanium miniplate anchorage.Am J Orthod Dentofacial Orthop 2002;122:593-600.
9. Costa A, Raffini M, Melsen B. Miniscrews as orthodonticanchorage. Int J Adult Orthod Orthognath Surg 1998;13:201-9.
10. Park HS, Bae SM, Kyung HM, Sung JH. Micro-implant anchor-age for treatment of skeletal Class I bialveolar protrusion. J ClinOrthod 2001;35:417-22.
11. Park HS, Bae SM, Kyung HM, Sung JH. Simultaneous incisorretraction and distal molar movement with microimplant anchor-age. World J Orthod 2004;5:164-71.
12. Park HS, Kyung HM, Sung JH. A simple method of molaruprighting with micro-implant anchorage. J Clin Orthod 2002;36:592-6.
13. Park YC, Lee SY, Kim DH, Lee SH. Intrusion of posterior teethusing mini-screw implants. Am J Orthod Dentofacial Orthop2003;123:690-4.
14. Park HS, Kwon OW, Sung JH. Uprighting second molars withmicro-implant anchorage. J Clin Orthod 2004;38:100-3.
15. Park HS, Kwon OW, Sung JH. Micro-implant anchorage forforced eruption of impacted canine. J Clin Orthod 2004;5:297-302.
16. Sung JH, Kwon OH, Kyung HM, Park KD. Longitudianl data ofcraniofacial growth from lateral cephalometrics in Koreans withnormal occlusion. Seoul: Jung-Won; 2001. p. 105-52.
17. Reitan K, Rygh P. Biomechanical principles and reactions. In:Graber TM, Vanarsdall RL, editors. Orthodontics—current prin-ciples and techniques. 2nd ed. St Louis: Mosby; 1994. p. 168-9.
18. Kuhn RJ. Control of anterior vertical dimension and properselection of extraoral anchorage. Angle Orthod 1958;38:340-9.
19. Rekow ED, Speidel TM, Koenig RA. Location of the mandibularcenter of autorotation in maxillary impaction surgery. Am JOrthod Dentofacial Orthop 1993;103:530-6.
20. Sugawara J, Baik UB, Umemori M, Takahashi I, Nagasaka H,Kawamura H, et al. Treatment and posttreatment dentoalveolarchanges following intrusion of mandibular molars with applica-tion of a skeletal anchorage system (SAS) for open bite correc-tion. Int J Adult Orthod Orthognath Surg 2002;17:243-53.
21. Champy M, Pape H, Gerlach KL, Lodde JP. Mandibular fracture.In: Kruger E, Schilli W, editors. Oral and maxillofacial trauma-tology. Vol 2. Chicago: Quintessence; 1986. p. 19-43.
22. Park HS. An anatomical study using CT images for the implan-tation of micro-implants. Korean J Orthod 2002;32:435-41.
23. Kyung HM, Park HS, Bae SM, Sung JH, Kim IB. Developmentof orthodontic micro-implants for intraoral anchorage. J Clin
Orthod 2003;37:321-8.