neurological emergencies prof. dr. Çiğdem Özkara
TRANSCRIPT
Neurological EmergenciesNeurological Emergencies
Prof. Dr. Çiğdem ÖzkaraProf. Dr. Çiğdem Özkara

Goal of an emergent Neurological Goal of an emergent Neurological ExaminationExamination
Is there a neurologic condition ?Is there a neurologic condition ?
Where is (are) the lesion(s) located ?Where is (are) the lesion(s) located ?
What are the possible causes?What are the possible causes?
Can the patient discharged from ER safely Can the patient discharged from ER safely or is hospitalisation needed ?or is hospitalisation needed ?

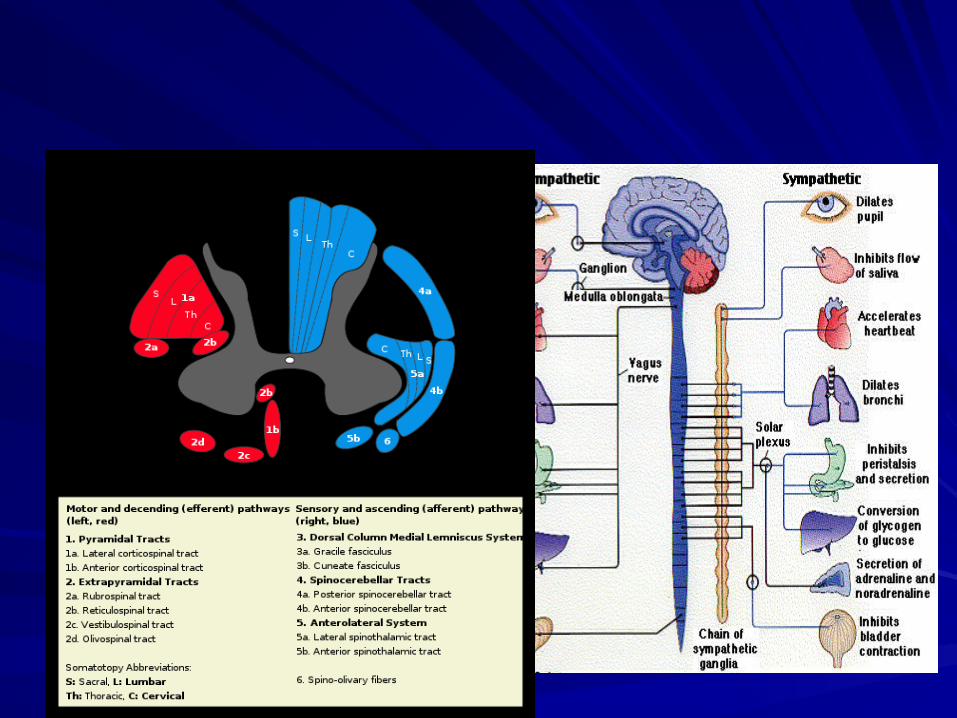
Anatomical basis of NEAnatomical basis of NE
BrainBrain
Brain stemBrain stem
Spinal cordSpinal cord
NervesNerves
MusclesMuscles
Anatomical basis of NEAnatomical basis of NE
BrainBrain– Alteration of thought process or Alteration of thought process or
consciousness, consciousness, – Seizures, involuntary movementsSeizures, involuntary movements– Motor and sensory deficit on the Motor and sensory deficit on the
same sidesame side

BrainstemBrainstem– Cranial nerve deficits in Cranial nerve deficits in
association with motor association with motor and sensory deficitand sensory deficit
– Diplopi, vertigo, dysartria, Diplopi, vertigo, dysartria, dysphagia,disequilibriumdysphagia,disequilibrium
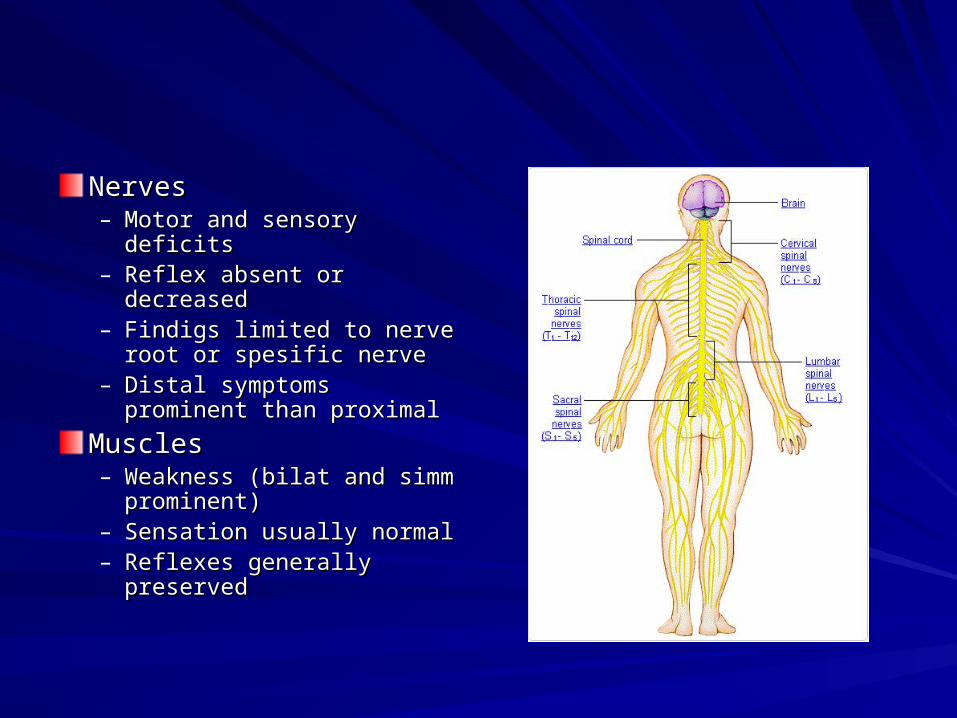
NervesNerves– Motor and sensory deficitsMotor and sensory deficits– Reflex absent or Reflex absent or
decreaseddecreased– Findigs limited to nerve Findigs limited to nerve
root or spesific nerveroot or spesific nerve– Distal symptoms prominent Distal symptoms prominent
than proximalthan proximal
MusclesMuscles– Weakness (bilat and simm Weakness (bilat and simm
prominent)prominent)– Sensation usually normalSensation usually normal– Reflexes generally Reflexes generally
preservedpreserved

Spinal cordSpinal corda)a) Well demarcated level Well demarcated level
sensory or motor. sensory or motor. b)b) Sensory dissociation:Sensory dissociation:
a)a) decreased pain on decreased pain on one side,decreased one side,decreased vibration and position vibration and position on the other sideon the other side;;
b)b) sensory deficit on one sensory deficit on one side, motor deficits on side, motor deficits on the other sidethe other side
a)a) Mixed upper and lower Mixed upper and lower MNMN

Spesific conditions presenting Spesific conditions presenting as emergencyas emergency
CVA (cerebro vascular CVA (cerebro vascular accedant)accedant)
InfectionsInfections
Movement disordersMovement disorders
PNS (polyneuritis) and PNS (polyneuritis) and neuromuscular disordersneuromuscular disorders
Guillain-Barre Synd.Guillain-Barre Synd.
Myastenia GravisMyastenia Gravis
Musculoscletal and Musculoscletal and neurogenic painneurogenic pain
Multiple SclerosisMultiple Sclerosis
Neuro-ophtalmologicalNeuro-ophtalmological
DementiaDementia
Brain tumorsBrain tumors
Increased Intra Cranial Increased Intra Cranial Pressure and herniation synd.Pressure and herniation synd.
Normal pressure Normal pressure hydrocephalushydrocephalus
Nontraumatic spinal cord Nontraumatic spinal cord emergenciesemergencies
Sleep disordersSleep disorders
Common neurological Common neurological PresentationsPresentations
Altered mental statusAltered mental status
HeadacheHeadache
WeaknessWeakness
DizzinessDizziness
SeizuresSeizures
Gait disturbancesGait disturbances
Altered mental statusAltered mental status
CNS dysfunction; global, diffuse, bilateral CNS dysfunction; global, diffuse, bilateral hemispheric, unilateral hemispheric with hemispheric, unilateral hemispheric with brain stem impairment (i.e.compression) brain stem impairment (i.e.compression) or primary brainstem dysfunctionor primary brainstem dysfunction
Function;Function;– decreased: coma, coma like statesdecreased: coma, coma like states– Increased: deliriumIncreased: delirium

ComaComa
Coma can be described as an eyes closed Coma can be described as an eyes closed unresponsive state. unresponsive state. – Obtundation: a blunting of consciousnessObtundation: a blunting of consciousness– Stupor: a sleep like state from which the Stupor: a sleep like state from which the
patient can be aroused by vigous stimulationpatient can be aroused by vigous stimulation
Delirium: Other end of the spectrum with Delirium: Other end of the spectrum with agitation, hallusinations and excessive agitation, hallusinations and excessive motor and verbal activitymotor and verbal activity

Glasgow Coma Scale Eye Opening
Spontaneous 4
To loud voice 3
To pain 2
None 1
Verbal Response
Oriented 5
Confused, Disoriented 4
Inappropriate words 3
Incomprehensible words 2
None 1
Motor Response
Obeys commands 6
Localizes pain 5
Withdraws from pain 4
Abnormal flexion posturing 3
Extensor posturing 2
None 1
Coma like conditionsComa like conditions
Locked-in state:Locked-in state: patient is alert, lost all patient is alert, lost all voluntary control except for extraoculer voluntary control except for extraoculer eye movements (basis pontis)eye movements (basis pontis)Akinetic mutism:Akinetic mutism: bilateral, deep, medial bilateral, deep, medial frontal lobe disease;awake attentive state frontal lobe disease;awake attentive state devoid of verbal or motor outputdevoid of verbal or motor outputVegetative state:Vegetative state: Chronic state of Chronic state of unresponsiveness, intact sleep-wake unresponsiveness, intact sleep-wake cycles , appear to be awakecycles , appear to be awake
EvaluationEvaluation
Abnormal Vital signs:Abnormal Vital signs: heart rate (atrial fibrill, heart rate (atrial fibrill, ventriculer tachycardias; embolic, ischemic…) ventriculer tachycardias; embolic, ischemic…) blood pressure ( hypertensive encephalopathy, blood pressure ( hypertensive encephalopathy, ICH,stroke), fever (menengitis, encephalitis, heat ICH,stroke), fever (menengitis, encephalitis, heat stroke..)etcstroke..)etc
Respiratory abnormalities: Respiratory abnormalities: – Cheyne- stokes: bi-hemispheric(ischemic, metabolic)Cheyne- stokes: bi-hemispheric(ischemic, metabolic)– Hyperventilation: hypothalamic rostral midbrainHyperventilation: hypothalamic rostral midbrain– Apneustic:mid-lower pontineApneustic:mid-lower pontine– Ataxic: medullaAtaxic: medulla
Focal neurologic findings:Focal neurologic findings:– Brainstem reflexes: Brainstem reflexes:
Pupillary reflexPupillary reflex is resistant to metabolic is resistant to metabolic insult , presence of pupillary dysfunction of insult , presence of pupillary dysfunction of asymmetry distinguish structural from asymmetry distinguish structural from metabolic coma !!!! ( generally small metabolic coma !!!! ( generally small reactive)reactive)
There are pharmacologic agents affective:There are pharmacologic agents affective:
Opiates: pinpoint, poorly reactive pupilsOpiates: pinpoint, poorly reactive pupils
Barbiturates: variaus sized relatively fixed Barbiturates: variaus sized relatively fixed
Third nerve, sympathetic pathwaysThird nerve, sympathetic pathways, .., ..
Ocular reflexes; oculocephalic and Ocular reflexes; oculocephalic and oculovestibuler lie adjacent to oculovestibuler lie adjacent to brainstem areas critical for brainstem areas critical for maintenance of consciousnessmaintenance of consciousness
Motor responseMotor response

Differential diagnosisDifferential diagnosisI.I. Cerebral dysfunction without focal signsCerebral dysfunction without focal signsTraumaTraumaMetabolic encephalopathies Metabolic encephalopathies – electrolyte, glycemia..electrolyte, glycemia..– Organ involvement ; hepatic/ amonnia, renal/urea, Organ involvement ; hepatic/ amonnia, renal/urea,
endocrine/ myxedema, Addison’sendocrine/ myxedema, Addison’s
HypertensiveHypertensiveToxic: CO, alcohol, opioidsToxic: CO, alcohol, opioidsNutritionalNutritionalPostictal (seizures)Postictal (seizures)Anoxic/hypoxicAnoxic/hypoxicEnvironmental (hypo/hypertermia)Environmental (hypo/hypertermia)

II.Cerebral dysfunction with focal signsII.Cerebral dysfunction with focal signs
StrokeStroke
Seizure Seizure – PostictalPostictal– Nonconvulsive SE Nonconvulsive SE
TraumaTrauma
Intra Cranial infectionsIntra Cranial infections
Intoxications Intoxications

32 yrs man32 yrs manSudden severe headache, vomiting, Sudden severe headache, vomiting, GTC seizure on the way to the hospitalGTC seizure on the way to the hospitalPE: tachicardia, fever, sweatingPE: tachicardia, fever, sweatingNE: Confused, agitated, meningeal irritation NE: Confused, agitated, meningeal irritation signs: +signs: +What is this?What is this?Where can be the lesion?Where can be the lesion?What to do?What to do?

PearlsPearls
Evaluation and management will go on at Evaluation and management will go on at the same timethe same time
Focal localising signs were described in Focal localising signs were described in drug overdoses and metabolic coma !!!drug overdoses and metabolic coma !!!

Common neurological Common neurological PresentationsPresentations
Altered mental statusAltered mental status
HeadacheHeadache
WeaknessWeakness
DizzinessDizziness
SeizuresSeizures
Gait disturbancesGait disturbances
Headache: Headache: Nasty NineNasty Nine1.1. First/ new , severe headacheFirst/ new , severe headache
2.2. Abrupt onsetAbrupt onset
3.3. Progressive and changing patternProgressive and changing pattern
4.4. Headache with neurologic symptoms>1hrHeadache with neurologic symptoms>1hr
5.5. Abnormal neurological findingsAbnormal neurological findings
6.6. Headache with syncope and seizuresHeadache with syncope and seizures
7.7. New headaches in children <5yr,>50 yrNew headaches in children <5yr,>50 yr
8.8. New headaches in pregnancy, with cancer, New headaches in pregnancy, with cancer, immunosuppressionimmunosuppression
9.9. Headaches worsening with exertion, sex, Headaches worsening with exertion, sex, Valsalva maneuverValsalva maneuver

Primary headache syndromesPrimary headache syndromes
tension-typetension-type
ClusterCluster
migrainemigraine
Secondary headache Secondary headache syndromessyndromes
SAHSAHMenengitisMenengitisIntracranial mass lesionsIntracranial mass lesionsCerebro Vascular DiseaseCerebro Vascular DiseaseInflammatory disordersInflammatory disordersDisorders of CSF volume and flow Disorders of CSF volume and flow (hydrocephalus, pseudotumor cerebri, (hydrocephalus, pseudotumor cerebri, intracranial hypotension)intracranial hypotension)

PearlsPearls
Focus on the Focus on the newnew or or differentdifferent headaches headaches not merely the worstnot merely the worst
Suspected SAH needs CT and LPSuspected SAH needs CT and LP
New or different headaches over 50 , New or different headaches over 50 , suspect temporal arteritis, investigate suspect temporal arteritis, investigate sedimentation ratesedimentation rate
Common neurological Common neurological PresentationsPresentations
Altered mental statusAltered mental status
HeadacheHeadache
WeaknessWeakness
DizzinessDizziness
SeizuresSeizures
Gait disturbancesGait disturbances

Evaluation of WeaknessEvaluation of WeaknessOnset: Onset: – Acute; initial manifestation of newly onset disease,Acute; initial manifestation of newly onset disease,– Exacerbation of a known progressive; Myastenia GravisExacerbation of a known progressive; Myastenia Gravis– Slowly progressive; Amyotrophic Lateral Sclerosis Slowly progressive; Amyotrophic Lateral Sclerosis
LocationLocation– ProximalProximal– DistalDistal– CranialCranial
Associated symptoms: pain, cramp, GIS(intox: bot)Associated symptoms: pain, cramp, GIS(intox: bot)
Medical historyMedical history
Muscle weaknessMuscle weakness
Cerebral hemispheric lesions: stroke,tmCerebral hemispheric lesions: stroke,tm
Spinal cord disordes: tm, inf, disc,Spinal cord disordes: tm, inf, disc,
Anterior horn cell disorders: ALSAnterior horn cell disorders: ALS
Nerve root disorders: Guillain-Barre S.Nerve root disorders: Guillain-Barre S.
Neuromuscular junction disorders: MG, Neuromuscular junction disorders: MG, botbot
Myopathies: Myopathies:

The most serious presentation of The most serious presentation of severe muscle weaknesssevere muscle weakness
““Acute Neuromuscular respiratory Acute Neuromuscular respiratory failurefailure””
Form of restrictive pulmonary diseaseForm of restrictive pulmonary disease
Myastenia gravisMyastenia gravis
Guillain-Barre syndromeGuillain-Barre syndrome
Amyotrophic lateral sclerosisAmyotrophic lateral sclerosis

65 yrs old woman65 yrs old womanDeveloped R hemiparesisDeveloped R hemiparesisMedical history: hypertensionMedical history: hypertensionFE: 170/95mmHg, 115 /min pulse rateFE: 170/95mmHg, 115 /min pulse rateNE: R central facial paresis, motor 2/5, 4/5NE: R central facial paresis, motor 2/5, 4/5What is this?What is this?Where can be the lesion?Where can be the lesion?What to do?What to do?

Common neurological Common neurological PresentationsPresentations
Altered mental statusAltered mental status
HeadacheHeadache
WeaknessWeakness
DizzinessDizziness
Gait disturbancesGait disturbances
SeizuresSeizures

DizzinessDizziness : the disturbed sense of well : the disturbed sense of well being usually perceived as an altered being usually perceived as an altered orientation in spaceorientation in space
VertigoVertigo: illusion of movement of oneself : illusion of movement of oneself or one’s surroundingsor one’s surroundings

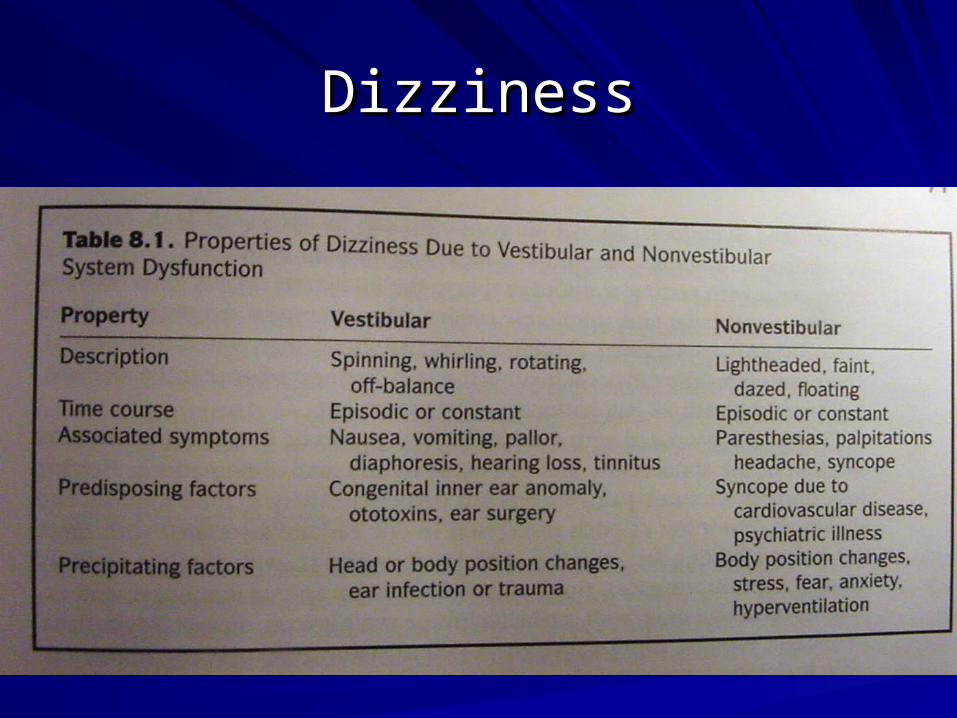
DizzinessDizziness
VestibulerVestibulerPeripheral (inner ear sensory organs, Peripheral (inner ear sensory organs,
afferents and brainstem efferents,) afferents and brainstem efferents,) Central (vestibuler nuclei, CNS connections)Central (vestibuler nuclei, CNS connections)
NonvestibulerNonvestibuler
DizzinessDizziness

VertigoVertigo

Important vestibuler system Important vestibuler system disordersdisorders
Benign positionel vertigoBenign positionel vertigo
Vestibuler neuritisVestibuler neuritis
LbyrinthitisLbyrinthitis
Meniere’s diseaseMeniere’s disease
Cerebello pontine angle tumorsCerebello pontine angle tumors
Vascular diseaseVascular disease

Common neurological Common neurological PresentationsPresentations
Altered mental statusAltered mental status
HeadacheHeadache
WeaknessWeakness
DizzinessDizziness
Gait disturbancesGait disturbances
SeizuresSeizures

Gait disturbancesGait disturbances
HemipareticHemipareticAtaxic: dorsal column, cerebellum, peripheral Ataxic: dorsal column, cerebellum, peripheral nervenerveSteppage: foot drop; L5 radiculopathy, peroneal Steppage: foot drop; L5 radiculopathy, peroneal HystericalHystericalSpastic Spastic Parkinsonian conditionsParkinsonian conditionsEarly gait apraxia: elderly, small uncertain stepsEarly gait apraxia: elderly, small uncertain stepsLate gait apraxia: dementia; small hesitant stepsLate gait apraxia: dementia; small hesitant stepsWaddling Waddling
Common neurological Common neurological PresentationsPresentations
Altered mental statusAltered mental status
HeadacheHeadache
WeaknessWeakness
DizzinessDizziness
Gait disturbancesGait disturbances
SeizuresSeizures
STATUS EPILEPTICUS is recurrent STATUS EPILEPTICUS is recurrent seizures without complete recovery of seizures without complete recovery of consciousness between attacks or consciousness between attacks or continuous seizure activity for more than continuous seizure activity for more than 30 minutes with or without impaired 30 minutes with or without impaired consciousness.consciousness.
Do not start medication unless the seizure Do not start medication unless the seizure is SE !!is SE !!

Causative factorsCausative factors
TraumaTrauma
TumorTumor
CVACVA
IC inf.IC inf.
Acute metab. disorderAcute metab. disorder
Intoxication Intoxication
Drugs (ciprofloxacin, baclofen, flumazenil..)Drugs (ciprofloxacin, baclofen, flumazenil..)
Mycoplazmosis pneumonia, cat scratch disease Mycoplazmosis pneumonia, cat scratch disease encephalitis, HSV6, AIDS, dural metastasis)encephalitis, HSV6, AIDS, dural metastasis)
Types of SETypes of SE
Generalized convulsive SEGeneralized convulsive SE
Epilepsia partialis continuaEpilepsia partialis continua
Myoclonic status in comaMyoclonic status in coma
Nonconvulsive SENonconvulsive SE– Complex Partial seizuresComplex Partial seizures– AbsenceAbsence

Tonic clonic SE Tonic clonic SE pathophysiologypathophysiology
Motor activityMotor activityEEGEEGPhysiological changesPhysiological changes– 1. phase: Compensation: SEizure activity increases 1. phase: Compensation: SEizure activity increases
cerebral metabolism,blood flow increases to cerebral metabolism,blood flow increases to compansate the situation. compansate the situation.
– Blood pressure increase, cardiac output and rate Blood pressure increase, cardiac output and rate increase, autonomic features (sweating, hypertermia, increase, autonomic features (sweating, hypertermia, bronchial secretion, salivation,vomit ) Hyperglicemiabronchial secretion, salivation,vomit ) Hyperglicemia
Phase 2Phase 2
Decompansation: cerebral autoregulation Decompansation: cerebral autoregulation progressively worsen, cerebral blood flow (CBF) progressively worsen, cerebral blood flow (CBF) depends on systemic blood pressure and depends on systemic blood pressure and hypotension occur, (IV AED HypoTA hypotension occur, (IV AED HypoTA ))Systemic and cerebral hypoxia, pulmonary Systemic and cerebral hypoxia, pulmonary hyperTA, eodema, cardiagenic arrytmia very hyperTA, eodema, cardiagenic arrytmia very oftenoftenleft vent cont left vent cont card outputcard output Cardiac failure Cardiac failureIC pressure syst pre CBF impair EODEMAIC pressure syst pre CBF impair EODEMA

Metabolic and endocrinologic changesMetabolic and endocrinologic changes
Lactic acidosisLactic acidosisHypoglicemiaHypoglicemiaHypo/hyperkalemiaHypo/hyperkalemiaHyponatremiaHyponatremiaMyoglobunuriaMyoglobunuria or dehydratation or dehydratation acute tubuler necrosis, acute tubuler necrosis, fulminan renal and fulminan renal and hepatic failurehepatic failureRabdomyolisis is prevented by artificial Rabdomyolisis is prevented by artificial ventilation and muscle paralysisventilation and muscle paralysisNorAdr and adrenaline release NorAdr and adrenaline release

Other complicationsOther complications
Acute pancreatitisAcute pancreatitis
FracturesFractures
Infections (lung, skin and urinary system)Infections (lung, skin and urinary system)
TromboflebitisTromboflebitis
DehydratationDehydratation
DICDIC
Cerebral venous trombosisCerebral venous trombosis
Cerebral infarct or hemarrogeCerebral infarct or hemarroge

General approachGeneral approachA) 1. step (0-10.min): cardiorespiratory, A) 1. step (0-10.min): cardiorespiratory, airway, O2airway, O2B) 2. step: (1-60 min): B) 2. step: (1-60 min): – 1)follow the neurological status, heart rate, blood 1)follow the neurological status, heart rate, blood
pressure, fewer, blood gases, pH, coagulation, pressure, fewer, blood gases, pH, coagulation, haematologyhaematology
– 2)IV AED2)IV AED– 3)IV NaCl 0.9, don’t mix up the drugs, venous 3)IV NaCl 0.9, don’t mix up the drugs, venous
lines used for AEDs (trombosis, flebitis..)lines used for AEDs (trombosis, flebitis..)– Glucos, blood gas, renal and hepatic functions and Glucos, blood gas, renal and hepatic functions and
Ca, Mg,haematology, coagulation, AED levelsCa, Mg,haematology, coagulation, AED levels– 50ml %50 glucose (hypoglisemi), alcoholism, 50ml %50 glucose (hypoglisemi), alcoholism,
nutritional disorders. Thiamin 250mg IVnutritional disorders. Thiamin 250mg IV

3. Step (1-60/90 min) 3. Step (1-60/90 min) – Etiological investigation ie, AED stopped ? Etiological investigation ie, AED stopped ? – To treat physiological abnormalities and To treat physiological abnormalities and
complications : hypoxia, ICB increase, pulmoner complications : hypoxia, ICB increase, pulmoner eodema and hyperTA, arrytmia, cardiac failure, eodema and hyperTA, arrytmia, cardiac failure, lactic asidosis, hyperpirexia, hypoglisemia, lactic asidosis, hyperpirexia, hypoglisemia, elektrolit imbalance, renal or hepatic failure, DIC, elektrolit imbalance, renal or hepatic failure, DIC, rabdomyolisisrabdomyolisis
– HypoTA : pressor treatment: dopamin 2-5 HypoTA : pressor treatment: dopamin 2-5 micgr/kg/min, IV monitormicgr/kg/min, IV monitor
4. Step (30-90.min): ICU4. Step (30-90.min): ICU
AED administrationAED administrationA) prodromal phase: diazepam (10mg IV,2-A) prodromal phase: diazepam (10mg IV,2-5mg/min,repeat after 15 min, rectal), 5mg/min,repeat after 15 min, rectal), midozolam, paraldehid, clonozepammidozolam, paraldehid, clonozepam
B) early SE: (0-30min) diazepam, B) early SE: (0-30min) diazepam, midozolam,clonazepam (1mg/30sn)midozolam,clonazepam (1mg/30sn)
C)persistance SE(30min<): physiological C)persistance SE(30min<): physiological decompensation, phenobarbitone 10mg/kg decompensation, phenobarbitone 10mg/kg 100mg/min and/or 100mg/min and/or
Pht 15-20mg/kg 50mg/minPht 15-20mg/kg 50mg/min
D) Refractory SE(60-90min): anestesiaD) Refractory SE(60-90min): anestesia
Management of a patient during a Management of a patient during a seizureseizure
Bend towards left sideBend towards left side
Avoid to injure himselfAvoid to injure himself
Touch gentlyTouch gently
Never place anything in his mouth unless Never place anything in his mouth unless you see them in the beginningyou see them in the beginning
Stay with him until he recoversStay with him until he recovers
17 yrs old girl17 yrs old girlGTC Seizure on awakeningGTC Seizure on awakeningConfused at ERConfused at ERNo focal signsNo focal signsHistory: Birthday party until late nightHistory: Birthday party until late nightWhat is this?What is this?Where can be the lesion?Where can be the lesion?What to do?What to do?