neuroimaging findings in patients with aids - clinical infectious
TRANSCRIPT

906
MODERN IMAGING TECHNOLOGY
Neuroimaging Findings in Patients with AIDS
Irwin Walot, Bruce L. Miller, Linda Chang,and C. Mark Mehringer
From the Departments ofRadiology and Neurology, Harbor-UCLAMedical Center, Torrance, and UCLA School ofMedicine,
Los Angeles, California
An increasing number of patients are presenting with central nervous system complications ofhuman immunodeficiency virus infection. New imaging technologies such as magnetic resonanceimaging, magnetic resonance proton spectroscopy, single-photon emission computed tomography,and positron emission tomography are playing an ever-increasing role in the diagnosis of thesecomplications. As therapeutic modes improve, imaging may assume a growing role in monitoringthe responses to therapy among these patients.
Approximately 40%-90% of patients with AIDS will develop CNS manifestations during the courses of their illnesses[1-3]. As a consequence, neuroimaging has come to play animportant role in the treatment of AIDS [4].
Patients with AIDS develop a variety of CNS lesions, andthe diagnosis of these lesions may require the application ofseveral imaging techniques including CT, MRI, single-photonemission computed tomography (SPECT), or magnetic resonance spectroscopy (MRS). Because the sensitivity of MRI issuperior to that of CT and because MRI allows acquisition ofimages in multiple planes, it has become the "gold standard"in neuroimaging.
Patients with AIDS may have CNS lesions due to differentpathological processes that occur synchronously or sequentially; occasionally, more than one pathological process isresponsible for the lesion [1, 5, 6]. In addition, patients whohave developed AIDS as a consequence of intravenous drugaddiction remain at risk for developing CNS diseases common to intravenous drug abusers and may have a higher riskof developing AIDS-related CNS diseases.
In the differential diagnosis of brain diseases in patientswith AIDS, some generalizations about the imaging appearance of CNS lesions are helpful because the clinical presentation of these lesions is often more dependent on their
Received 15 February 1996.Grant support: this work was supported in part by a grant from the U.S.
Public Health Service (PHS 1 R01NS29919-01).Reprints and correspondence: Dr. Irwin Walot, Department of Radiology,
Harbor-UCLA Medical Center, 1000 West Carson Street, Torrance, California90509.
Clinical Infectious Diseases 1996;22:906-19© 1996 by The University of Chicago. All rights reserved.1058-4838/96/2206-0002$02.00
anatomic location than on their etiology. Imaging revealsCNS abnormalities in these patients that can be broadlyclassified into four categories: focal lesions with mass effect; focal lesions without significant mass effect; diffuseglobal CNS abnormalities; and ventriculitis, meningitis,and infarcts.
Focal Lesions with Mass Effect
Focal brain lesions develop in 15%-20% of patients withAIDS. As there are effective therapeutic regimens for most ofthe lesions in this category, they are the most important lesionsto identify. Diagnosis based on imaging can be confoundedby the similarity in appearance of many of the CNS lesionsassociated with AIDS and by alterations in the typical patternsof enhancement and edema that these same lesions would produce in patients who are not immunocompromised.
Contrast enhancement on CT scans or MR images dependson vascularity and disruption of the blood-brain barrier. Theinflammatory response can be weak in patients whose immunestatus is markedly compromised, and there may be correspondingly poor contrast enhancement of infectious lesions thatwould otherwise show intense enhancement in patients withnormal immune responses. However, tumors enhance secondary to an abnormal blood-brain barrier within tumor vesselsor secondary to increased vascularity. In general, tumors thatnormally enhance will continue to enhance despite a severelydysfunctional immune system, but enhancement of infectiousor inflammatory lesions can be variable.
The amount of vasogenic edema surrounding a lesion is alsoinfluenced by the immune response. Both tumors and infectiouslesions are affected, and in the setting of severe immune dysfunction, the amount of adjacent edema and mass effect evoked
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021

eID 1996;22 (June) Neuroimaging in AIDS 907
Figure 1. MR images of the brain of a patient with toxoplasmosis. A, TzW fast spin echo axial MR (300011 02/2) image reveals multiplebilateral high signal-intensity masses (arrows) in the basal ganglia. The lesions elicit considerable surrounding edema, and some of the lesionshave low signal-intensity rims. E, T1W non-contrast-enhanced axial MR (600/10/1) image; the lesions are of low signal intensity, with somelesions having high signal-intensity rims secondary to hemorrhage (arrows). C, Contrast-enhanced T1W (600/10/1) image; the lesions are ringenhancing (arrows). D, CT scan, obtained 2 months after MRI was performed, shows complete resolution of the lesions following the initiationof antitoxoplasmic therapy. TzW = Tz weighted; T,W = T I weighted; numbers in parentheses are repetition time in milliseconds/echo timein milliseconds/excitations.
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021

908 Walot et al. em 1996;22 (June)
Figure 2. MR images of the brain of a patient with toxoplasmosis. A, TzW spin echo axial MR (25001100/.5) image reveals multiplesubcortical focal masses (arrows) and basal ganglia (curved arrows) focal masses. Lesions vary in signal intensity and are surrounded byconsiderable edema. B, TjW non-contrast-enhanced axial (600/10/1) image at the same level shows bright signal in most of the lesions, whichis consistent with the presence of hemorrhage. TzW = T2 weighted; numbers in parentheses are repetition time/echo time/excitations.
in response to either type of lesion can be less than wouldnonnally be expected. The most common focal mass lesionsencountered in patients with AIDS generally induce considerable surrounding edema and enhance on CT and MRI followingthe administration of intravenous contrast agents.
Toxoplasmosis, the most common opportunistic CNS infection in patients with AIDS (this infection occurs in 13.4%-33%of AIDS patients with CNS complications [2, 3]), is caused bythe protozoan Toxoplasma gondii. In the immunologically intacthost, T. gondii generally causes a self-limited infection. Afterthe initial infection, an intact immune system keeps the organismdormant. In the immunocompromised host, the latent organismcan reactivate and cause encephalitis and brain abscesses.
Once the infection is diagnosed, it may be controlled withlifelong drug therapy [7]. Therapy is often begun empiricallyas soon as CT scans or MR images show focal parenchymallesions of any sort because the infection is so common inthis population [7, 8]. Patients who respond to antitoxoplasmicmedications are presumed to have toxoplasmosis. The responseto drug therapy is typically rapid, with noticeable regressionof the lesions apparent on imaging studies within 10 days to 2weeks [8, 9]. Patients who are not compliant or who discontinuetherapy will relapse.
Toxoplasmic lesions begin as foci of encephalitis thatprogress rapidly to parenchymal abscesses with central necrosis and surrounding inflammation. Toxoplasmosis typically manifests on CT scans and MRls as nodular (smallencephalitis) and/or ring-enhancing (large-abscess) lesionswithin the brain parenchyma. The enhancing ring, whenpresent, may be somewhat thicker and more ill defined thanthat seen in association with a typical bacterial abscess.
The lesions are associated with surrounding edema andtend to be multiple at presentation [9-11]. However, asignificant percentage of patients present with solitary lesions [II]. Toxoplasmic lesions are most often seen in thebasal ganglia [12] and cerebral hemispheres [11] (figure 1).On nonenhanced T,-weighted (T1W) MR images, the lesions are oflow signal intensity, and on Tz weighted (TzW)MR images, the lesions are mildly-to-moderately hyperintense in relation to the brain parenchyma and can be difficult to separate from the surrounding edema. The presenceof small hemorrhages may be a sign of toxoplasmosis (figure 2), and calcifications can occasionally be seen at thesites of treated lesions.
Primary lymphoma of the CNS also occurs frequently inpatients with AIDS [2, 3, 13, 14] and is the most common
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021
eID 1996;22 (June) Neuroimaging in AIDS 909
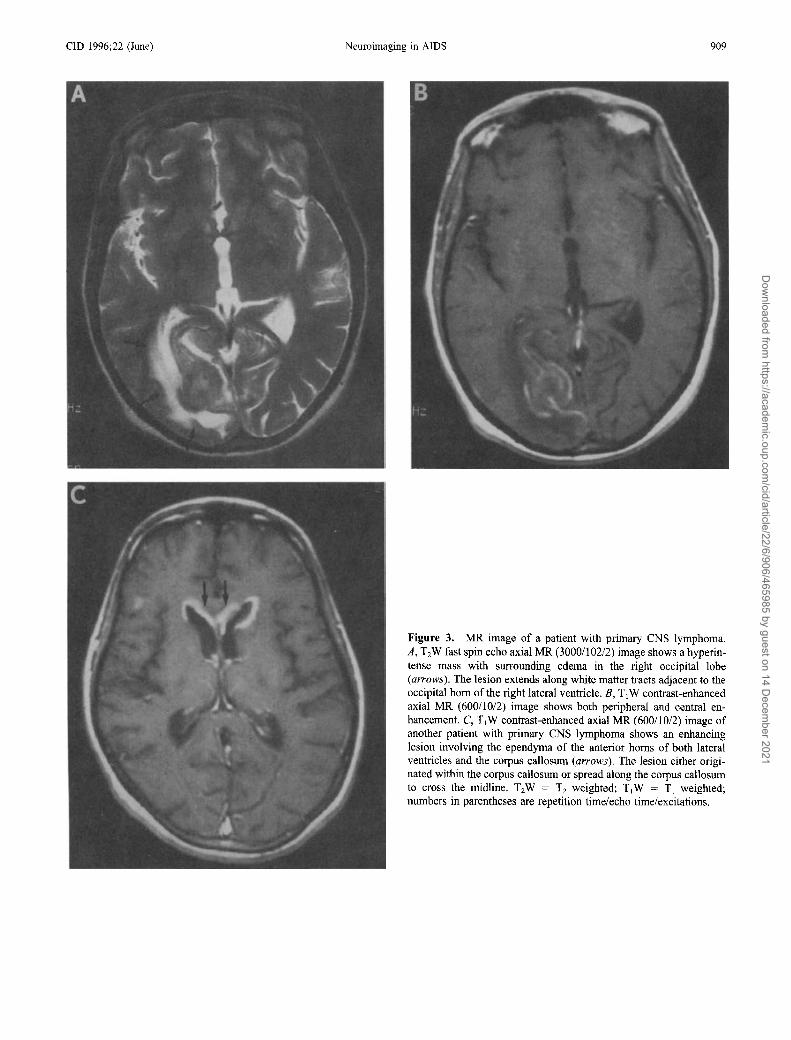
Figure 3. MR image of a patient with primary CNS lymphoma.A, TzW fast spin echo axial MR (3000/102/2) image shows a hyperintense mass with surrounding edema in the right occipital lobe(arrows). The lesion extends along white matter tracts adjacent to theoccipital horn of the right lateral ventricle. E, TIW contrast-enhancedaxial MR (600/10/2) image shows both peripheral and central enhancement. C, TIW contrast-enhanced axial MR (600/10/2) image ofanother patient with primary CNS lymphoma shows an enhancinglesion involving the ependyma of the anterior horns of both lateralventricles and the corpus callosum (arrows). The lesion either originated within the corpus callosum or spread along the corpus callosumto cross the midline. TzW = T2 weighted; TIW = TI weighted;numbers in parentheses are repetition time/echo time/excitations.
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021

910 Walot et al. em 1996;22 (June)
lac and lipidS
lac and lipids
ppm
are of increased attenuation with respect to the brain parenchyma (as is commonly observed in cases of primary CNSlymphoma in patients who do not have AIDS). Lesions thatare of increased attenuation on non-contrast-enhanced CTscans have a high probability of being lymphomas [11] andprobably correspond to the lesions that are hypointense onT2W MR images. Primary CNS lymphoma most often occurs centrally (basal ganglia or corpus callosum) or in theperiventricular white matter, and subependymal spread orventricular encasement is a characteristic finding [11] (figure 3).
The imaging characteristics of lymphoma and toxoplasmosisoverlap to such a significant degree that it is nearly impossibleto differentiate the lesions on the basis of their appearance onCT scans or MR images alone. Patients with a few solid lesionsor ring-enhancing subependymal or periventricular lesions(particularly those with subependymal extension) tend to havelymphomas, whereas patients with multiple ring-enhancing lesions (particularly those that are hemorrhagic) in the basalganglia and cerebral hemispheres are more likely to have toxoplasmosis. The fact that toxoplasmosis and lymphoma mayoccur synchronously in the same patient or even together inthe same lesion further confuses the issue [6]. When patientsare treated empirically for toxoplasmosis, all lesions must bemonitored for therapeutic responses. Differential diagnosis canbe particularly difficult for patients who present with solitarylesions.
Imaging techniques including positron emission tomography (PET), MRS, and SPECT have all been reported as beinghelpful in differentiating primary CNS lymphoma from toxoplasmosis. When SPECT imaging is performed with thallium-201, lymphomas have a propensity to take up the radionuclide tracer, whereas inflammatory lesions do not [20, 21];however, the specificity of SPECT is still unknown [22, 23].On PET scans, lymphomas have a similar propensity to takeup 18F fluorodeoxyg1ucose [24], but PET is not widely available, and its specificity is also unknown. MRS is anothertechnique that can aid in the differential diagnosis of theselesions [25].
Spectra produced by toxoplasmic lesions show that theselesions tend to have markedly elevated lactate and lipid peakswith depletion ofnormal metabolites (figure 4), while the spectra produced by lymphomas show that these lesions tend tohave elevated choline peaks and mildly to moderately elevatedlactate and lipid peaks (figure 4). However, even on MRSthere may be considerable overlap between the spectra of theselesions. We have found that lymphomas with central necrosismay have spectra very much like the spectra of toxoplasmiclesions.
Cryptococcosis, an infection caused by the yeast Cryptococcusneoformans, is also common in patients with AIDS (--5% ofthese patients present with cerebral cryptococcosis [26,27]). Theinitial infection is probably pulmonary, but the organism is neurotropic, and the infection quickly spreads to the CNS. Once in theCNS, the infection can manifest as meningitis, focal encephalitis
toxoplasmosis
lymphoma
CNS neoplasm in these patients. This lymphoma is nearlyalways of the high-grade B-cell type, and the cells containthe Epstein-Barr virus [15, 16] (before the AIDS epidemic,most primary CNS lymphomas were of the T cell variety).Primary CNS lymphoma can present as a solitary lesion,even in patients with AIDS, but it most often presents multifocally [11, 17]. In fact, autopsy studies have shown thatCNS lymphoma is multifocal in 80%-100% of AIDS patients [18].
On CT scans and MR images, lymphoma most commonlymanifests as an enhancing, space-occupying mass with surrounding edema. However, much of the time the lesionsundergo central necrosis and present as ring-enhancingmasses [11]; some studies suggest that most of these lesionsare ring enhancing [17, 19]. On non-contrast-enhanced T1Wimages, typical lesions are isointense in relation to brainparenchyma, while on T2W images the lesions are isointenseto hyperintense.
Occasionally, lesions may be hypointense on T2W images[11]. On nonenhanced CT, a small percentage of the lesions
Figure 4. Representative single voxel MR spectra produced by atoxoplasmic lesion, a primary eNS lymphoma, and an area of normalbrain. Toxoplasmic spectrum has a markedly elevated lactate (lac)and lipid peak and shows diminished peaks of the other metabolites.The lymphoma spectrum has a moderately elevated lactate and lipidpeak and an elevated choline (cho) peak. The remain.ing metabolitessuch as N-acetylaspartate (naa), choline compounds, and myo-inositol(mi) are also diminished.
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021
em 1996;22 (June) Neuroimaging in AiDS 91 I
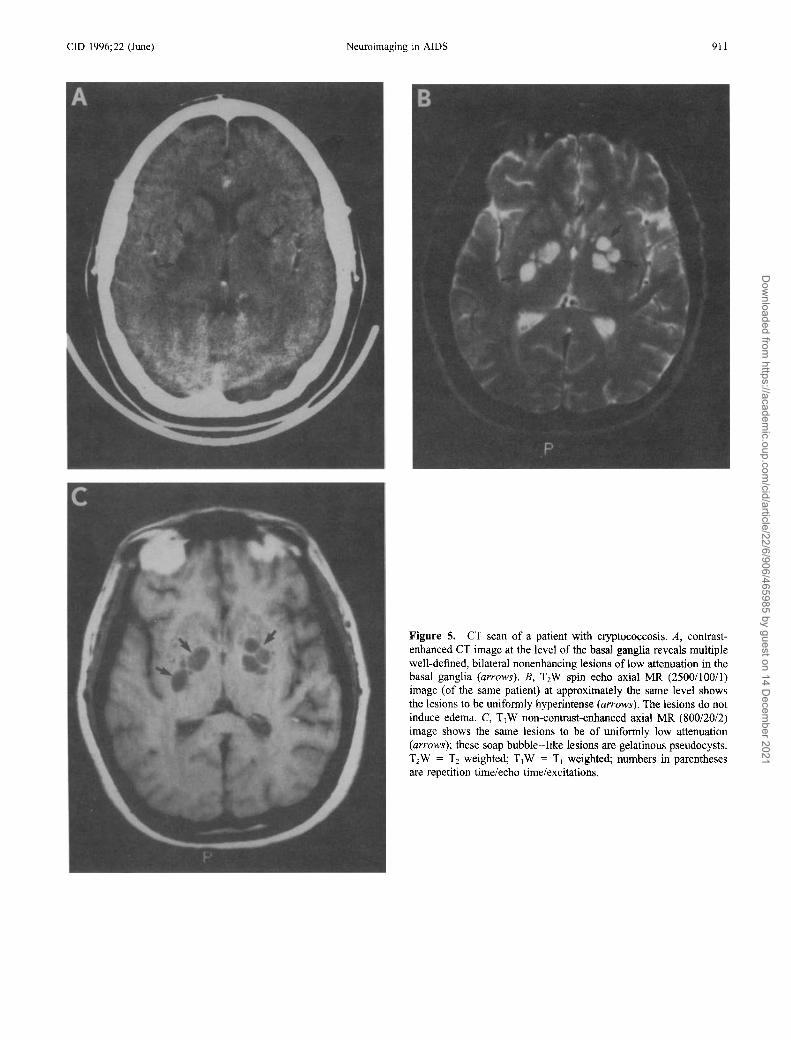
Figure 5. CT scan of a patient with cryptococcosis. A, contrastenhanced CT image at the level of the basal ganglia reveals multiplewell-defined, bilateral nonenhancing lesions oflow attenuation in thebasal ganglia (arrows). B, T2W spin echo axial MR (2500/100/1)image (of the same patient) at approximately the same level showsthe lesions to be unifonnly hyperintense (arrows). The lesions do notinduce edema. C, T\W non-contrast-enhanced axial MR (800/20/2)image shows the same lesions to be of uniformly low attenuation(arrows); these soap bubble-like lesions are gelatinous pseudocysts.T2W = T2 weighted; TIW = TI weighted; numbers in parenthesesare repetition time/echo time/excitations.
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021

912 Walot et al. em 1996;22 (June)
Figure 6. MR image of a patient with a cryptococcal brain abscess. A, T2W fast spin echo axial MR (3000/10212) image at the level of the top ofthe lateral ventricles shows two well-defined lesions of high signal intensity (one in the right frontal lobe adjacent to the right lateral ventricle [an-ow]and another small lesion in the right occipital lobe [curved an-ow]). B, contrast-enhanced TjW MR (600/10/2) image at the same level shows bothlesions to be oflow signal intensity with thin rim enhancement. T2W = T2 weighted; T.W = T) weighted; numbers in parentheses are repetition time/echo time/excitations.
Figure 7. cr scans of a patient with a tuberculous brain abscess. A and B, contiguous contrast-enhanced CT scans at the level of the basal gangliareveal a multiloculated lesion of low attenuation with thin rim enhancement in the left temporal lobe (an-ows). The lesion elicits considerable SlUTOundingedema.
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021

CID 1996;22 (June) Neuroimaging in AIDS 913
Figure 8. MR image ofapatient with systemic lymphoma that metastasized to the oculomotor nerves. T1W fat-saturated contrast-enhanced MR(600/15/2) axial image shows enlarged, enhancing third cranial nerves(arrows). Cytological examinations of the CSF were also diagnostic oflymphoma T,W = TI weighted; numbers in parentheses are repetitiontime/echo time/excitations.
or a cerebral mass, or an abscess. However, meningitis is by farthe most common presentation, even in the immunocompetenthost. The immune response is subdued (probably because of themucinous capsule the organism elaborates), and meningeal enhancement on imaging is rare. For AIDS patients who have cerebral cryptococcosis, >70% of CT scan findings are normal orconsist only of generalized atrophy [28].
C. neofonnans can proliferate within the subarachnoid spacesto the point that the perivascular spaces around perforating bloodvessels become filled with organisms and mucoid exudate. Thedilated perivascular spaces appear as nonenhancing cystic masseson CT scans and MR images and are termed "gelatinous pseudocysts." These cyst-like lesions have a predilection for the basalganglia but can be present in the brain stem or in the convexities(figure 5). They appear as areas of low attenuation on CT scans,low signal intensity on TI W images, and high signal intensity onTzW images (these signal characteristics are similar to those forthe CSF).
When C. neoformans infects the brain parenchyma, encephalitis results. The areas of encephalitis may evolve intocryptococcal masses or abscesses (figure 6). However, focalparenchymal masses occur in a relatively small percentageof patients with cerebral cryptococcosis [28] and generallyappear as discrete nodular or ring-enhancing masses on CTscans and MR images.
Although the incidence oftuberculosis is higher among patientswith AIDS [29], the overall incidence of neurotuberculosis still
Figure 9. MR image of a patient with progressive multifocalleukoencephalopathy. A, T2W fast spin echo axial MR (4000/10211) image shows iIIdefined white matter lesions in both frontal lobes (arrows); no mass effect is seen. B, contrast-enhanced T,W axial MR (66/10/1) image at the samelevel shows the lesion to be of low signal intensity with minimal, if any, contrast enhancement.
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021
914 Walot el al. em 1996;22 (June)
appears to be low [4, 30]. Bishburg et al. [30] reported an increased incidence (10 of420 patients in their series) ofneurotuberculosis among IllY-infected patients who were also drug abusers.Neurotuberculosis can present either as meningitis or as focalparenchymal lesions. As has been observed for fungal lesions ofthe CNS, focal neurotuberculosis may present as areas of cerebritis, granulomas (enhancing nodules), caseating granulomas (lesions with irregular ring enhancement), or as a tuberculous abscess(a lesion with thin ring enhancement and mass effect and edema)
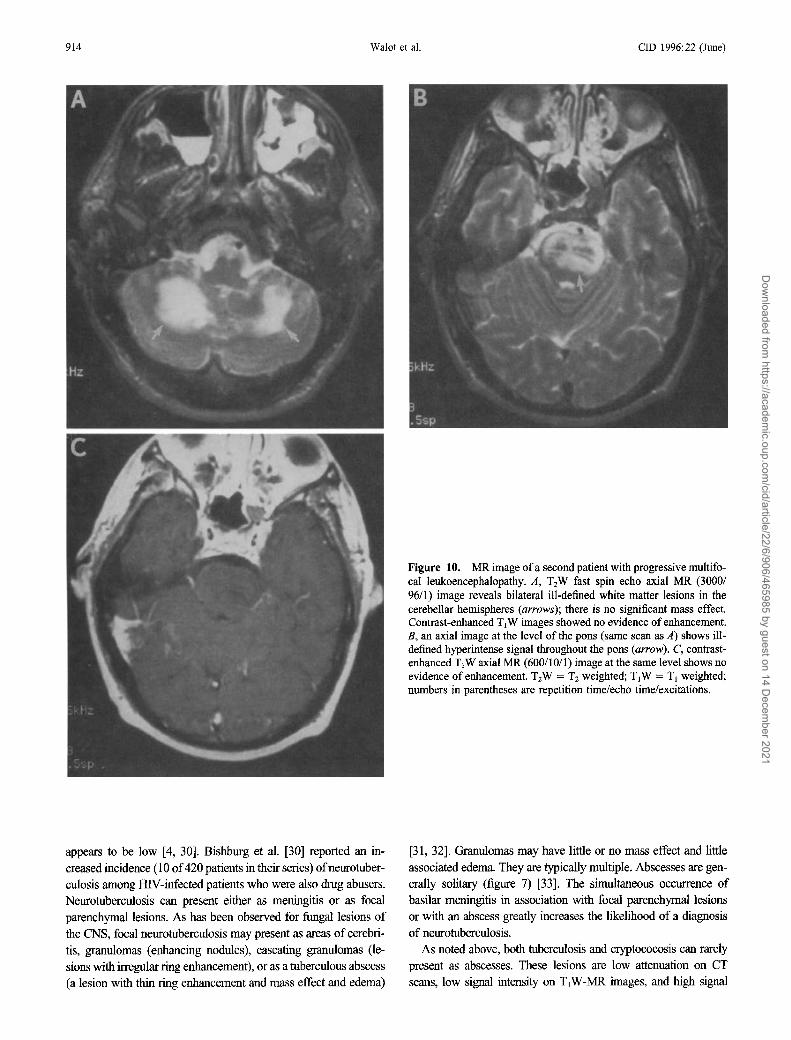
Figure 10. MR image ofa second patient with progressive multifocal leukoencephalopathy. A, TzW fast spin echo axial MR (3000/96/1) image reveals bilateral ill-defined white matter lesions in thecerebellar hemispheres (arrows); there is no significant mass effect.Contrast-enhanced T1W images showed no evidence of enhancement.B, an axial image at the level of the pons (same scan as A) shows i1Idefined hyperintense signal throughout the pons (arrow). C, contrastenhanced T1Waxial MR (600/1 0/ I) image at the same level shows noevidence of enhancement. T2W = T2 weighted; TIW = TI weighted;numbers in parentheses are repetition time/echo time/excitations.
[31,32]. Granulomas may have little or no mass effect and littleassociated edema. They are typically multiple. Abscesses are generally solitary (figure 7) [33]. The simultaneous occurrence ofbasilar meningitis in association with focal parenchymal lesionsor with an abscess greatly increases the likelihood of a diagnosisof neurotuberculosis.
As noted above, both tuberculosis and cryptococosis can rarelypresent as abscesses. These lesions are low attenuation on CTscans, low signal intensity on T1W-MR images, and high signal
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021

em 1996;22 (June) Neuroimaging in AIDS 915
Figure 11. MR image ofa patient with HIV encephalopathy. T2Wfast spin echo axial MR (3000/10212) image at the superior aspect ofthe lateral ventricles reveals diffuse, ill-defined, abnormally increasedsignal intensity in the white matter (arrows). T2W = T2 weighted;numbers in parentheses are repetition time/echo time/excitations.
intensity on T2W-MR images. They have thin enhancing rims,
usually induce considerable surrounding edema, and can be identi
cal in appearance to pyogenic abscesses. Although infection with
HIV-I does not predispose to pyogenic abscess formation, a con
siderable percentage of HIV-infected patients have acquired theinfection through drug abuse, and those patients who continue toabuse intravenous drugs are at risk for the development ofpyogenicabscesses.
Neurosyphilis, which has been reported to occur in 1.5%1.8% of patients with AIDS [34, 35], can rarely present asfocal syphilitic lesions (gummas). Berger et al. [36] havereported two such lesions in HIV-infected patients, andBrightbill et al. [37] recently reported that among their pa
tients with neurosyphilis, 2 (6%) of 35 had gummas. Find
ings on imaging are nonspecific, with lesions presenting as
nodular, enhancing masses in the cortex or dura. The lesions
have mass effect and elicit surrounding edema [36-38]. Me
tastases from systemic lymphomas may present as enhancing
focal masses, dura-based masses, or infiltrative lesions of
cranial nerves (figure 8).
Focal Lesions Without Significant Mass Effect
The lesions in this category generally involve only whitematter, do not induce significant edema, and generally do not
enhance. Focal lesions in the white matter are characteristically
of decreased attenuation on CT images, low signal intensity
on T1W MR images, and high signal intensity on T2W images,
and they appear nonspecific. Similar-appearing lesions are seen
in patients with multiple sclerosis and postviral demyelinatingsyndromes (such as acute disseminated encephalomyelitis) and
in aging patients. Aside from these more typical etiologies,
white matter lesions in patients with AIDS may result from a
number of other pathological processes.
Progressive multifocal leukoencephalopathy is the most seri
ous focal lesion without significant mass effect. Astrom et al.
[39] first described it in 1958 among patients with lymphoma.
It is now known to be caused by the IC virus, a papovavirus.
Eighty percent of adults are seropositive for antibodies to the
IC virus; however, like T gondii, this virus causes few problems
in the immunocompetent host. In 1%-3.8% of patients with
AIDS, immune system failure allows reactivation of the virus.
CNS manifestations are caused by infection and destruction of
oligodendrocytes, resulting in secondary demyelinization. Thelesions tend to be mulifocal at presentation, primarily involvethe white matter, and progress in size and number. The lesions
cause focal neurological deficits, and there is no proven therapy.
Death usually occurs within months of reactivation of the virus,
but remission can occur if the patient's immune status improves.
On CT, the lesions have low attenuation. On MRI, they are of
low signal intensity on T IW images and high signal intensity on
T2W images. They exhibit little or no mass effect. Although ring
enhancement has been reported [40], these lesions generally do
not enhance on CT or MRI. They often occur at the interfacebetween the gray matter and the white matter and have a scalloped
contour secondary to involvement of peripheral U fibers (figure9). The parietal lobe is predominantly affected, but these lesions
also occur in the periventricular white matter, posterior fossa,
brain stem, spinal cord, and even the basal ganglia (where travers
ing white-matter tracts are thought to be involved). In our experi
ence, two thirds oflesions have occurred in an occipital or subtentorial location (figure 10). MR proton spectroscopy may also beuseful in distinguishing progressive multifocalleukoencephalopathy from other focal brain lesions [25].
Similar-appearing lesions have also been attributed to directinfection of the CNS with herpes simplex virus and cytomegalovirus (CMV). As well, similar lesions may be seen in patientswith neurosyphilis [37].
Diffuse Global eNS Abnormalities
In our practice, the most common imaging manifestation of
HIV infection is global atrophy. This condition manifests as
dilated, prominent subarachnoid spaces, basilar cisterns, and
ventricular enlargement that is out of proportion in relation to
the patient's stated age (hydrocephalus ex vacuo). It is seen onboth CT scans and MR images. The finding of diffuse cerebralatrophy can be accompanied by diffuse, confluent, ill-definedareas of abnormally increased signal intensity on T2W MRimages of the periventricular white matter (figure 11) and ab-
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021
916 Walot et al. cm 1996;22 (June)
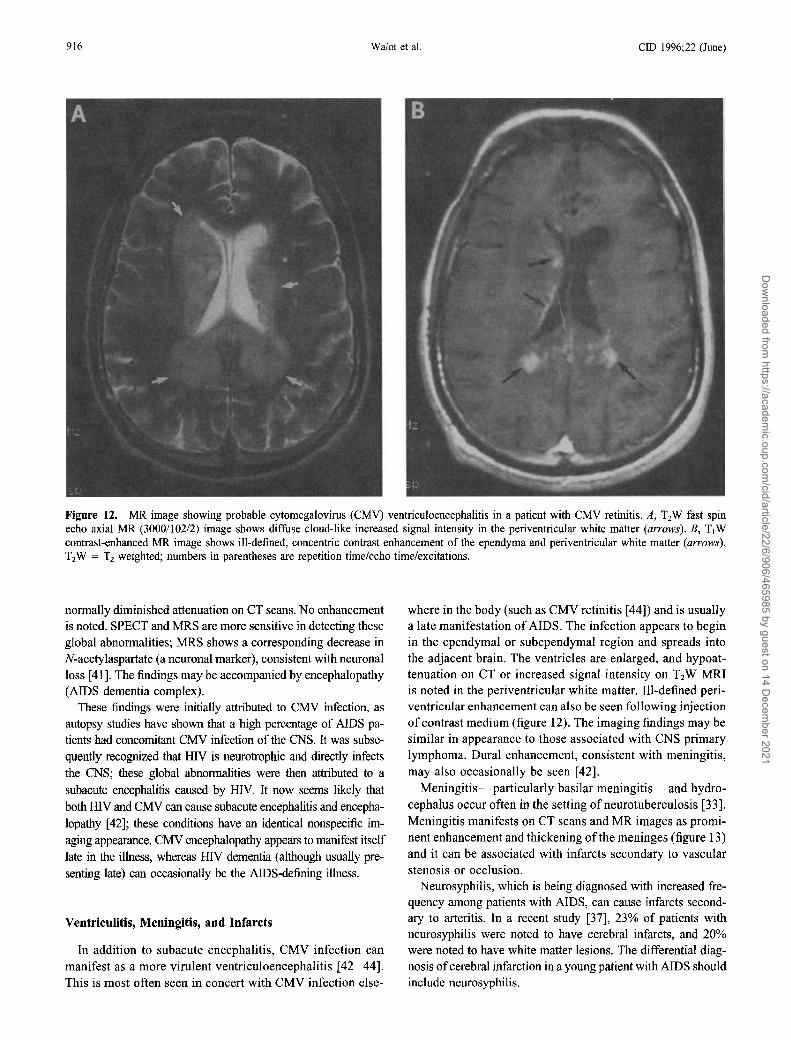
Figure 12. MR image showing probable cytomegalovirus (CMV) ventriculoencephalitis in a patient with CMV retinitis. A, TzW fast spinecho axial MR (3000/102/2) image shows diffuse cloud-like increased signal intensity in the periventricular white matter (arrows). B, T1Wcontrast-enhanced MR image shows ill-defined, concentric contrast enhancement of the ependyma and periventricular white matter (arrows).TzW = Tz weighted; numbers in parentheses are repetition time/echo time/excitations.
normally diminished attenuation on CT scans. No enhancementis noted. SPECT and MRS are more sensitive in detecting theseglobal abnormalities; MRS shows a corresponding decrease inN-acetylaspartate (a neuronal marker), consistent with neuronalloss [41]. The findings may be accompanied by encephalopathy(AIDS dementia complex).
These findings were initially attributed to CMV infection, asautopsy studies have shown that a high percentage of AIDS patients had concomitant CMV infection of the CNS. It was subsequently recognized that HIV is neurotrophic and directly infects
the CNS; these global abnormalities were then attributed to asubacute encephalitis caused by illV. It now seems likely that
both H1V and CMV can cause subacute encephalitis and encephalopathy [42]; these conditions have an identical nonspecific imaging appearance. CMV encephalopathy appears to manifest itself
late in the illness, whereas H1V dementia (although usually presenting late) can occasionally be the AIDS-defining illness.
Ventriculitis, Meningitis, and Infarcts
In addition to subacute encephalitis, CMV infection canmanifest as a more virulent ventriculoencephalitis [42-44].This is most often seen in concert with CMV infection else-
where in the body (such as CMV retinitis [44]) and is usuallya late manifestation of AIDS. The infection appears to beginin the ependymal or subependymal region and spreads intothe adjacent brain. The ventricles are enlarged, and hypoattenuation on CT or increased signal intensity on T2W MRIis noted in the periventricular white matter. Bl-defined periventricular enhancement can also be seen following injectionof contrast medium (figure 12). The imaging findings may besimilar in appearance to those associated with CNS primarylymphoma. Dural enhancement, consistent with meningitis,may also occasionally be seen [42].
Meningitis-particularly basilar meningitis-and hydrocephalus occur often in the setting of neurotuberculosis [33].Meningitis manifests on CT scans and MR images as prominent enhancement and thickening ofthe meninges (figure 13)and it can be associated with infarcts secondary to vascularstenosis or occlusion.
Neurosyphilis, which is being diagnosed with increased frequency among patients with AIDS, can cause infarcts secondary to arteritis. In a recent study [37], 23% of patients withneurosyphilis were noted to have cerebral infarcts, and 20%were noted to have white matter lesions. The differential diagnosis ofcerebral infarction in a young patient with AIDS shouldinclude neurosyphilis.
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021
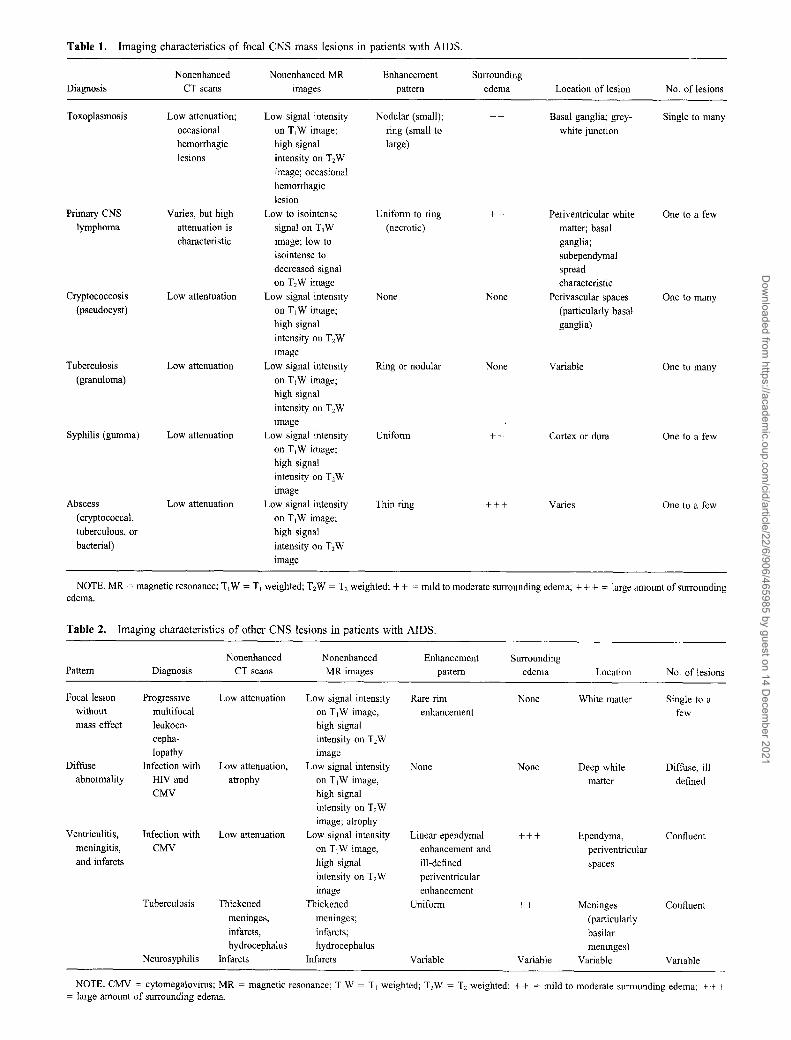
Table 1. Imaging characteristics of focal CNS mass lesions in patients with AIDS.
Nonenhanced Nonenhanced MR Enhancement Surrounding
Diagnosis CT scans images pattern edema Location of lesion No. of lesions
Toxoplasmosis Low attenuation; Low signal intensity Nodular (small); ++ Basal ganglia; grey- Single to many
occasional on T1W image; ring (small to white junction
hemorrhagic high signal large)
lesions intensity on T2W
image; occasionalhemorrhagic
lesion
Primary CNS Varies, but high Low to isointense Uniform to ring ++ Periventricular white One to a few
lymphoma attenuation is signal on T1W (necrotic) matter; basal
characteristic image; low to ganglia;isointense to subependymaldecreased signal spreadon T2W image characteristic
Cryptococcosis Low attentuation Low signal intensity None None Perivascular spaces One to many
(pseudocyst) on T1W image; (particularly basalhigh signal ganglia)
intensity on T2W
image
Tuberculosis Low attenuation Low signal intensity Ring or nodular None Variable One to many
(granuloma) on TjW image;high signal
intensity on T2Wimage
Syphilis (gumma) Low attenuation Low signal intensity Uniform ++ Cortex or dura One to a fewon T1W image;high signal
intensity on T2Wimage
Abscess Low attenuation Low signal intensity Thin ring +++ Varies One to a few(cryptococcal, on T1W image;
tuberculous, or high signal
bacterial) intensity on T2W
image
NOTE. MR = magnetic resonance; T1W = T I weighted; T2W = T2 weighted; + + = mild to moderate surrounding edema; + + + = large amount of surroundingedema.
Table 2. Imaging characteristics of other CNS lesions in patients with AIDS.
Nonenhanced Nonenhanced Enhancement SurroundingPattern Diagnosis CT scans MR images pattern edema Location No. of lesions
Focal lesion Progressive Low attenuation Low signal intensity Rare rim None White matter Single to awithout multifocal on T1W image, enhancement fewmass effect leukoen- high signal
cepha- intensity on T2Wlopathy image
Diffuse Infection with Low attenuation, Low signal intensity None None Deep white Diffuse, illabnormality HIVand atrophy on T1W image, matter defined
CMV high signal
intensity on T2Wimage; atrophy
Ventriculitis, Infection with Low attenuation Low signal intensity Linear ependymal +++ Ependyma, Confluentmeningitis, CMV on T1W image, enhancement and periventricularand infarcts high signal ill-defined spaces
intensity on T2W periventricular
image enhancementTuberculosis Thickened Thickened Uniform ++ Meninges Confluent
meninges, meninges; (particularlyinfarcts, infarcts; basilarhydrocephalus hydrocephalus meninges)
Neurosyphilis Infarcts Infarcts Variable Variable Variable Variable
NOTE. CMV = cytomegalovirus; MR = magnetic resonance; TjW = T1weighted; T2W = T2 weighted; ++ = mild to moderate surrounding edema; +++= large amount of surrounding edema.
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021

918 Walo! et al. CID 1996;22 (June)
~ . '"fl .,) , -J '~/", 'I Y \ \
i '\ A~ i\ I
\ /I'
I
" /
"
Figure 13. MR image of a patient with tuberculous meningitis and
hydrocephalus. T,W contrast-enhanced axial MR (600/2012) image
reveals thickened enhancing meninges surrounding the brainstem
(arrows) and dilated temporal horns of the lateral ventricles (largearrows). An arachnoid cyst in the left middle fossa (curved arrows)is an incidental finding. T,W = T I weighted; numbers in parentheses
are repetition time/echo time/excitations.
Tables I and 2 summarize the CT and MRl findings with
respect to brain abnormalities in patients with AIDS.
Diagnostic imaging studies serve as an adjunct to clinical
acumen and laboratory studies in the management of AIDS.
Future research in the areas of functional neuroimaging
(SPECT and PET) and MRS will result in improved diagnostic
specificity and will impact positively on patient care.
Acknowledgment
The authors thank Thomas Ernst, Ph.D., for providing the proton
spectra used in figure 4.
References
1. Comford ME, Holden JK, Boyd MC, Berry K, Vioters HV. Neuropathol
ogy of the acquired immune deficiency syndrome (AIDS): report of 39
autopsies from Vancouver, British Columbia. Can J Neurol Sci 1992;
19:442-52.
2. Anders KH, Guerra WF, Tomiyasu U, Verity MA, Vinters HV. The neuro
pathology of AIDS: UCLA experience and review. Am J Pathol 1986;
124:537-57.
3. Levy RM, Bredesen DE, Rosenblum ML. Neurological manifestations of
the acquired immunodeficiency syndrome (AIDS): experience at UCSF
and review of the literature. J Neurosurg 1985;62:475-95.
4. Levy RM, Mills CM, Posin JP, Moore SG, Rosenblum ML, Bredesen DE.
The efficacy and clinical impact of brain imaging in neurologically
symptomatic AIDS patients: a prospective CT/MRI study. J Acquir
Immune Defic Syndr 1990;3:461-71.
5. Gray F, ed. Atlas of the neuropathology of HIV infection. New York:
Oxford University Press, 1993:162-72.
6. Chang L, Cornford ME, Chiang FL, Ernst TM, Sun NCJ, Miller BL.
Radiologic-pathologic correlation. Cerebral toxoplasmosis and lym
phoma in AIDS. AJNR Am J Neuroradiol 1995; 16:1653-63.
7. Porter SB, Sande MA. Toxoplasmosis of the central nervous system in
the acquired immunodeficiency syndrome. N Engl J Med 1992;327:
1643-8.
8. Luft BJ, Remington JS. AIDS commentary. Toxoplasmic encephalitis. J
Infect Dis 1987; 157:[-6.
9. Navia BA, Petitio CK, Gold JWM, Cho ES, Jordan BD, Price RW. Cere
bral toxoplasmosis complicating the acquired immune deficiency syn
drome: clinical and neuropathological findings in 27 patients. Ann Neu
rol 1986; 19:224- 38.
10. Weisberg LA, Greenberg J, Stazio A. Computed tomographic findings in
cerebral toxoplasmosis in adults. Comput Med Imaging Graph 1988;
12:379-83.
II. Dina TS. Primary central nervous system lymphoma versus toxoplasmosis
in AIDS. Radiology 1991; 179:823-8.
12. Levy RM, Rosenbloom S, Perrett LV. Neuroradiologic findings in AIDS:
A review of 200 cases. AIR Am J Roentgeno[ 1986; 147:977-83.
13. Bantz S, Iglesias-Rozas J, Jautzke G, Adler T. Cerebral lymphomas in
AIDS [abstract]. Clin NeuropathoI1989;8:219.
14. So YI, Beckstead ill, Davis RL. Primary central nervous system
lymphoma in acquired immune deficiency syndrome: a clinical and
pathological study. Ann Neurol 1986;20:566-72.
15. Rosenberg NL, Hochberg FH, Miller G, Kleinschmidt-DeMasters BK.
Primary central nervous system lymphoma related to Epstein-Barr virus
in a patient with acquired immune deficiency syndrome. Ann Neurol
1986;20:98-102.
16. Levine AM. Acquired immunodeficiency syndrome-related lymphoma.Blood 1992;80:8-20.
17. Ciricillo SF, Rosenblum ML. Use ofCT and MR imaging to distinguish
intracranial lesions and to define the need for biopsy in AIDS patients.
J Neurosurg 1990;73:720-4.
18. Morgello S, Petitio CK, Mouradian JA. Central nervous system lymphoma
in the acquired immunodeficiency syndrome. Clin Neuropathol 1990;
9:205-15.
19. Poon T, Matoso I, Tchertkoff V, Weitzner I Jr, Gade M. CT features of
primary cerebral lymphoma in AIDS and non-AIDS patients. J Comput
Assist Tomogr 1989; 13:6-9.
20. Vanarthos WJ, Ganz WI, Vanarthos JC, Serafini AN, Tehranzadeh J.
Diagnostic uses of nuclear medicine in AIDS. Radiographies 1992; 12:
731-49.
21. Ruiz A, Ganz I, Post MID, Camp A, et al. Use of thallium-201 brain
SPECI to differentiate cerebral lymphoma from toxoplasma encephali
tis in AIDS patients. AJNR Am J Neuroradiol 1994; 15:1885-94.
22. 0 Malley JP, Ziessman HA, Kumar PN, Harkness SA, Tall JG, Pierce
PF. Diagnosis of intracranial lymphoma in patients with AIDS: value
of 20'n single-photon emission computed tomography. Am J Roent
genol 1994; 163:417-21.
23. Dierckx RA, Martin JJ, Dobbeleir A, Crois R, Neetens I, De Deyn PP.
Sensitivity and specificity of thallium-201 single-photon emission to
mography in the functional detection and differential diagnosis of brain
tumors. Eur J Nuel Med 1994;21:621-33.
24. Hoffinan IM, Waskin HA, Schifter T, et al. FOG-PET in differentiating
lymphoma from nonmalignant central nervous system lesions in patients
with AIDS. J Nucl Med 1993; 34:567- 75.
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021

CID 1996;22 (June) Neuroimaging in AIDS 919
25. Chang L, Miller BL, McBride D, et a1. Brain lesions in patients withAIDS-H-l MR spectroscopy. Radiology 1995; 197:525-31.
26. Zugar A, Louie E, Holzman RS, Simberkoff MS, Rahal J1. Cryptococcaldisease in patients with the acquired immunodeficiency syndrome. Diagnostic features and outcome of treatment. Ann Intern Med 1986; 104:234-40.
27. Eng RHK, Bishburg E, Smith SM, Kapila R. Cryptococcal infections inpatients with acquired immune deficiency syndrome. Am J Med 1986;81:19-23.
28. Popovich MJ, Arthur RH, Helmer E. CT of intracranial cryptococcosis.AJR Am J Roentgenoll990; 154:603-6.
29. Raymond CA. Increase in AIDS-associated illnesses focuses new attentionon an old nemesis. JAMA 1986;256:3323-4.
30. Bishburg E, Sunderam G, Reichman LB, Kapila R. Central nervous systemtuberculosis with the acquired immunodeficiency syndrome and its related complex. Ann Intern Med 1986; 105:210-3.
31. Watson IDG, Shnier RC, Seale JP. Central nervous system tuberculosisin Australia: a report of 22 cases. Med J Aust 1993; 158:408-13.
32. De Castro CC, Hesselink JR. Tuberculosis. Neuroimaging Clinics ofNorthAmerica 1991; 1:119-39.
33. Whiteman M, Expinoza L, Post MJD, Bell MD, Falcone S. Central nervoussystem tuberculosis in HIV-infected patients: clinical and radiographicfindings. AJNR Am J Neuroradioll995; 16:1319-27.
34. Katz DA, Berger JR. Neurosyphilis in acquired immunodeficiency syndrome. Arch NeuroI1989;46:895-8.
35. Berger JR. Neurosyphilis in human immunodeficiency virus type I-seropositive individuals. A prospective study. Arch Neurol 1991; 48:700-2.
36. Berger JR, Waskin H, Pall L, Hensley G, Ihmedian I, Post MJD. Syphiliticcerebral gumma with HIV infection. Neurology 1992;42:1282-7.
37. Brightbill TC, Ihmeidan IH, Donovan Post MID, Berger JR, Katz DA.
Neurosyphilis in HIV-positive and HIV-negative patients: neuroimaging
findings. AJNR Am J Neuroradiol 1995; 16:703-11.
38. Agrons GA, Han SS, Husson MA, Simeone F. MR imaging of cerebralgumma. AJNR Am J Neuroradiol 1991; 12:80-1.
39. Astrom KE, Mancall EL, Richardson EP Jr. Progressive multifocal leuko
encephalopathy: a hitherto unrecognized complication of chronic lym
phatic leukemia and Hodgkins disease. Brain 1958; 81:93 -Ill.
40. Wheeler AL, Truwit CL, Kleinschmidt-DeMasters BK, Byrne WR, Han
non RN. Progressive multifocalleukoencephalopathy: contrast enhance
ment on CT scans and MR images. AJR Am J RoentgenoI 1993; 161 :1049-51.
41. McConnell JR, Swindells S, Ong CS, et al. Prospective utility of cerebral
proton magnetic resonance spectroscopy in monitoring HIV infectionand its associated neurological impairment. AIDS Res Hum Retrovi
ruses 1994; 10:977-82.
42. Holland NR, Power C, Mathews VP, Glass ID, Forman M, McArthur Jc.
Cytomegalovirus encephalitis in acquired immunodeficiency syndrome
(AIDS). Neurology 1994;44:507-14.
43. Salazar A, Podzamczer D, Rene R, et al. Cytomegalovirus ventricu
loencephalitis in AIDS patients. Scand J Infect Dis 1995;27:165-9.
44. Berman SM, Kim RC. The development of cytomegalovirus encephali
tis in AIDS patients receiving ganciclovir. Am J Med 1994;96:415-9.
Dow
nloaded from https://academ
ic.oup.com/cid/article/22/6/906/465985 by guest on 14 D
ecember 2021