national healthy cities networks
TRANSCRIPT
National healthy cities networksA powerful force for health and
sustainable development in Europe
Leah Janss Lafond
Zoe Heritage
Jill L. Farrington
Agis D. Tsouros
31497_National.p65 06-10-2003, 08:041
2 . NATIONAL HEALTHY CITIES NETWORKS
Abstract
National healthy cities networks are the backbone of the healthy cities movement in Europe. They providepolitical, strategic and technical support to their members, represent a national resource of experience andexpertise in health development and offer a dynamic platform for public health advocacy at the nationaland international level. Each national network is unique. Each one develops in response to the needs of itsmember cities, according to the resources available and within its own cultural and legal framework. Thepublication has two parts: analysis of the multifaceted work and achievements of national networks acrossEurope and a profile of each network focusing on its special features, successes and aspirations.
Keywords
URBAN HEALTHHEALTHY CITIESCOMMUNITY NETWORKSSUSTAINABILITYEUROPE
ISBN Number 92 890 1087 8
Address requests about publications of the WHO Regional Office to:• by e-mail [email protected] (for copies of publications)
[email protected] (for permission to reproduce them)[email protected] (for permission to translate them)
• by post PublicationsWHO Regional Office for EuropeScherfigsvej 8DK-2100 Copenhagen Ø, Denmark
© World Health Organization 2003
All rights reserved. The Regional Office for Europe of the World Health Organization welcomes requests forpermission to reproduce or translate its publications, in part or in full.
The designations employed and the presentation of the material in this publication do not imply theexpression of any opinion whatsoever on the part of the World Health Organization concerning the legalstatus of any country, territory, city or area or of its authorities, or concerning the delimitation of itsfrontiers or boundaries. Where the designation “country or area” appears in the headings of tables, itcovers countries, territories, cities, or areas. Dotted lines on maps represent approximate border lines forwhich there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they areendorsed or recommended by the World Health Organization in preference to others of a similar naturethat are not mentioned. Errors and omissions excepted, the names of proprietary products are distin-guished by initial capital letters.
The World Health Organization does not warrant that the information contained in this publication iscomplete and correct and shall not be liable for any damages incurred as a result of its use. The viewsexpressed by authors or editors do not necessarily represent the decisions or the stated policy of the WorldHealth Organization.
31497_National.p65 06-10-2003, 08:042

Contents
Preface 5
Introduction 7
1. The development of the WHO Healthy Cities project in Europe 8
2. Organization and leadership of national networks 12
3. Achievements and impact of national networks 16
4. Developing effective national networks for the future 22
5. Profiles of the national healthy cities networks in Europe 27
Annex 1.Resources on healthy cities 86
Annex 2.WHO criteria for accrediting national healthy cities networks 88
Annex 3.Recommended WHO criteria for cities to become members of an accredited national network 90
CONTENTS . 3
31497_National.p65 06-10-2003, 08:043
4 . NATIONAL HEALTHY CITIES NETWORKS
Authors
Leah Janss Lafond
Manager (EU Project), Healthy Cities and Urban Govern-
ance Programme, WHO Regional Office for Europe
Zoe Heritage
Freelance public health trainer, Rennes, France
Jill L. Farrington
Deputy Head, Centre for Urban Health and Deputy Head,
Healthy Cities and Urban Governance Programme, WHO
Regional Office for Europe
Agis D. Tsouros
Head, Centre for Urban Health and Head, Healthy Cities
and Urban Governance Programme, WHO Regional Office
for Europe
Cover design
Fay Stassinopoulou, Athens Greece
Layout and typesetting
Christensen Grafisk ApS, Copenhagen Denmark
31497_National.p65 06-10-2003, 08:044

Prefaceindependent states of the former USSR and severalcountries in south-eastern Europe will therefore bethe focus of our efforts. Existing national net-works will be playing a major role in supportingand mentoring the newcomers.
On behalf of WHO, I would like to thank allthe European national networks and, in particular,the coordinators for providing the valuable infor-mation that comprises the basis for this publica-tion and for their support in finalizing the profilesof the national networks. I would also like tothank the members, past and present, of the Advi-sory Committee on National Healthy Cities Net-works for providing valuable comments on thequestionnaires used to gather the information.Special thanks are also due to Robert Jensen foradministrative support and to David Breuer formeticulous text editing.
Finally I would like to express our gratitude tothe Italian Healthy Cities Network for having gen-erously covered the printing costs of this publica-tion.
Agis D. TsourosHead, Centre for Urban HealthHead, Healthy Cities and Urban GovernanceProgrammeWHO Regional Office for Europe
National networks represent the backbone of thehealthy cities movement in Europe. They repre-sent a rich and diverse resource of public healthknowledge and experience and an effective plat-form for giving visibility to local health issues andconcerns and for supporting countries’ efforts to-wards health development. In line with the spiritand the directions of WHO’s country strategy ofmatching services to new needs, national net-works have the potential and the capacity to sup-port the development and the implementation ofcountry strategies related to health promotion,preventing noncommunicable diseases and envi-ronment and health.
This book provides a fascinating account of themany facets and achievements of national healthycities networks over the last 15 years. It underlinesthe importance of working closely with politiciansand policy-makers and demonstrates with specificexamples why and how national networks repre-sent a valuable resource for innovative publichealth work. The book gives only a glimpse intothe many aspects of the work of national net-works but makes a convincing case for the need tocontinue supporting and strengthening nationalnetworks at the country level and internationally.
One of the main strategic aims of the fourthphase (2003–2007) of the WHO European HealthyCities project is to bring healthy cities to all coun-tries of the WHO European Region. Most of the
PREFACE . 5
31497_National.p65 06-10-2003, 08:045

6 . NATIONAL HEALTHY CITIES NETWORKS
31497_National.p65 06-10-2003, 08:046

IntroductionNational healthy cities networks mobilize and in-spire cities to develop responsive local strategiesfor urban health and sustainable development. Al-though the main objective of national networks isto support cities in implementing the healthy cit-ies approach, many networks have also become asignificant resource for national governments.
The principles of healthy cities have spread rap-idly since the mid–1980s. This publication con-centrates on the development and achievementsof national healthy cities networks in the Euro-pean Region of WHO, but all other WHO regionshave active healthy city initiatives1 and manynetworks that support sustainable urban develop-ment at the national and international levels. Forexample, the European Sustainable Cities & TownsCampaign brings together the WHO EuropeanHealthy Cities Network and nine other Europeanand international networks of local authorities ina major initiative to promote local action for sus-tainable development. This book does not reviewthe contribution of all other public health andsustainable development networks or the develop-ment of healthy cities in other parts of the world.The WHO Regional Office for Europe works di-rectly with the WHO European Healthy CitiesNetwork and with the Network of the EuropeanNational Healthy Cities Networks. This publica-tion focuses on these national networks.
This book has been prepared in close consulta-tion with the coordinators of national networks ofhealthy cities in Europe. It draws on the numer-ous surveys of national networks carried out byWHO since 19972 as well as new material col-lected in late 2002 and early 2003. At the end of2002, the 30 national networks in 29 Europeancountries were asked to provide profiles includingcase studies, a statement by a leading nationalpolitician and evidence of the network’s impact aswell as information on their collaboration withthe national government. They were also asked toprovide statistics and to describe their organiza-tion, resources, major activities, membership crite-ria and partnerships. This basic information is be-ing published on the WHO web site in the form offact sheets for each network3 and is summarizedin the national network profiles in Chapter 5 ofthis book. The initial findings from analysis of
material across the national networks were pre-sented to representatives of the national networksin early 2003.4 The subsequent discussion enableda joint reflection on the strengths and the chal-lenges facing healthy cities networks and the top-ics the representatives would like included in thebook.
This publication has been produced for peoplewho have experience with national networks ofhealthy cities, both politicians and technical staff,and for a wider audience who may be discoveringthe multifaceted healthy cities applications for thefirst time. The book briefly describes the historyand development of national healthy cities net-works in Europe. The following chapters describehow the networks in the European Region are or-ganized and what they have achieved. Althoughthese chapters give an overview, many countriesprovide specific examples. Chapter 4 provides aframework for the future development of nationalnetworks. It includes the criteria for a successfulnational network and some of the challenges anddilemmas currently facing the national networks.Chapter 5 is a compendium of profiles of the na-tional networks in Europe. The profiles explainhow the networks were started, their current ac-tivities at the city, national and sometimes inter-national levels and their future plans.
1 Healthy cities in action: 5 case-studies from Africa, Asia, Middle
East and Latin America. Geneva, World Health Organiza-
tion, 2000 (http://whqlibdoc.who.int/hq/2000/
WHO_SDE_PHE_00.02.pdf, accessed 17 September 2003).2 Farrington J. The state of national networks for healthy cities.
Copenhagen, WHO Regional Office for Europe, 1997 (Cen-
tre for Urban Health).
Rothstein L. The state of national networks for healthy cities.
Copenhagen, WHO Regional Office for Europe, 1999 (Cen-
tre for Urban Health).3 National network fact sheets. Copenhagen, WHO Regional
Office for Europe, 2002 (http://www.euro.who.int/healthy-
cities/CitiesAndNetworks/20020111_5, accessed 17 Septem-
ber 2003).4 Network of European National Healthy Cities Networks. Report
on a WHO business meeting. Copenhagen, Denmark, 28 Febru-
ary–1 March 2003. Copenhagen, WHO Regional Office for
Europe (in press).
INTRODUCTION . 7
31497_National.p65 06-10-2003, 08:047

8 . NATIONAL HEALTHY CITIES NETWORKS
1.The development of the WHO Healthy Cities project in Europe
health for all, health promotion and sustainabledevelopment.2 The concept of healthy cities is
National networks of healthy cities in Europe de-veloped as a spontaneous reaction to great de-mand by cities to participate in the healthy citiesmovement. When WHO launched the HealthyCities project in 1987 with 11 pilot cities, it ex-panded quickly and gained high visibility.1 Today,national healthy cities networks have been estab-lished in 29 countries in the WHO European Re-gion, bringing together about 1300 cities, countiesand organizations across Europe (Fig. 1.1). Thehealthy cities movement is active in every part ofthe world, and all six WHO regional offices sup-port this movement. This chapter reviews the his-torical development of the national healthy citiesnetworks in Europe.
The WHO Healthy Cities project was a direct,local response to a series of global and Europeanpolicy initiatives in the 1970s and 1980s thatchanged how people think about and understandhealth. The project has its roots in the concepts of
Fig. 1.1. National healthy cities networks in the WHO European Region
1 Draper R et al. WHO Healthy Cities project: review of the first
five years (1987–1992): a working tool and reference framework
for evaluating the project. Copenhagen, WHO Regional Of-
fice for Europe, 1993 (EUR/ICP/HSC 644).2 Ottawa Charter for Health Promotion. Copenhagen, WHO Re-
gional Office for Europe, 1986 (http://www.who.dk/
AboutWHO/Policy/20010827_2, accessed 17 September
2003).
Agenda 21 (http://www.un.org/esa/sustdev/
agenda21text.htm). New York, United Nations Division for
Sustainable Development, 1992 (accessed 17 September
2003).
The United Nations Millennium Development Goals. New York,
United Nations, 2000 (http://www.un.org/
millenniumgoals, accessed 17 September 2003).
HEALTH21 – the health for all policy framework for the WHO Eu-
ropean Region. Copenhagen, WHO Regional Office for Eu-
rope, 1999 (http://www.who.dk/InformationSources/Publi-
cations/Catalogue/20020322_1, accessed 17 September
2003).
31497_National.p65 06-10-2003, 08:048

based on the recognition of the importance of thelocal and urban dimension in health action andthe key role of local governments in health andsustainable development.
As the European healthy cities movement hasevolved over time, it has responded to new globalstrategies and priorities, and to changing sociopo-litical, demographic and organizational contexts.Healthy cities is a dynamic concept. Its shape andcontent have been influenced over time by emerg-ing country priorities and new WHO strategies;lessons learned from past experience; advances inscientific knowledge and evidence relating to pub-lic health interventions and the determinants ofhealth; and changes in political, policy and or-ganizational environments. The 15 years of theWHO Healthy Cities project in Europe coincideswith historic political and social changes in east-ern and western Europe and at the global level.The European Region has experienced enormouspolitical and constitutional change in the last dec-ade. Between 1989 and 1996, 27 states in the east-ern part of the Region adopted new constitutions,which often strengthened the role of municipalgovernments. The overall trend in Europe hasbeen towards decentralization, in which munici-pal governments have been delegated morepower, responsibility and autonomy to set priori-ties and decide policies in such areas as education,environment and health, social services, healthservices, social housing, community care, trans-port, urban planning, water supply and wastemanagement.3 In addition, cities provide en-hanced democratic accountability by empoweringcommunities to take part in the decision-makingprocesses that control the factors that influencetheir health.
The WHO Healthy Cities project in Europe hasevolved and been implemented over three 5-yearphases (1988–1992, 1993–1997 and 1998–2002).The fourth phase was launched in 2003. Eachphase has had specific goals, core themes anddeliverables (Box 1.1). Although each phase hassought to expand the strategic scope of theproject, the principles, methods and vision ofhealthy cities have always been linked to fourconstants:
• action to address the determinants of healthand the principles of health for all and sustain-able development;
• action to integrate and promote European andglobal public health priorities;
• action to put health on the social and politicalagendas of cities; and
• action to promote good governance and part-nership-based planning for health.
The goals of the WHO Healthy Cities project areimplemented through a process involving politi-cal commitment to the principles of health for alland sustainable development; institutionalchanges and establishing infrastructure to supportand enable intersectoral collaboration and com-munity involvement; work at the strategic, policyand community levels with specific deliverablesincluding city health development plans andmechanisms that reinforce accountability forhealth; and formal and informal networking lo-cally, nationally and internationally. These areknown as the action elements of the healthy citiesapproach.
The WHO Healthy Cities project in the Euro-pean Region has two main operating vehicles: theWHO European Healthy Cities Network and thenational and subnational healthy cities networks.The WHO European Healthy Cities Network con-sists of designated cities that are fully committedto implementing the goals of each phase. This is akey mechanism for promoting commitment andinnovation and is a source of valuable expertise,
Box 1.1. Phases of development of theWHO European Healthy Cities NetworkPhase I (1988-1992)Thirty-five cities focused on creating newstructures for intersectoral working andmechanisms to manage change.
Phase II (1993-1997)Thirty-nine cities strongly emphasizeddeveloping healthy public policies anddrawing up comprehensive city health plansfocusing on equity and sustainabledevelopment.
Phase III (1998-2002)Fifty-five cities attempted to make a transitionfrom health promotion to integrated cityhealth development plans – creatingpartnership-based policies with a strongemphasis on equity, the social determinantsof health, Local Agenda 21, communitydevelopment and regeneration initiatives.
3 Green G. Health and governance in European cities: a compen-
dium of trends and responsibilities for public health in 46 mem-
ber states of the WHO European Region. London, European
Hospital Management Journal Ltd, 1998.
THE DEVELOPMENT OF THE WHO HEALTHY CITIES PROJECT IN EUROPE . 9
31497_National.p65 06-10-2003, 08:049

10 . NATIONAL HEALTHY CITIES NETWORKS
legitimacy and continuous learning. A new WHOEuropean Network is established to implementthe goals of each phase. To become members, cit-ies formally apply to WHO for designation to theWHO European Healthy Cities Network, which isbased on a set of clear criteria related to the city’scapacity and commitment to implementing a spe-cific programme of work and deliverables.
National networks, in contrast, have developedindependently based on ideas and influences re-sulting from their collaboration with WHO andtheir participation in international meetings. Na-tional networks have enabled wide accessibility tothe concepts and experience of healthy cities tohundreds of cities throughout Europe. Nationalhealthy cities networks involve a wide range ofprofessional, political and community audiences.They provide a flexible response both to theunique needs and opportunities for health andsustainable development within a country. Na-tional networks provide a framework for buildingpolitical commitment and alliances at all levels.
The development of national healthycities networksAlthough national healthy cities networks do notwork according to phases, their development canbe described according to the time frames of thefirst three phases of the WHO European HealthyCities Network.
Responding to great demand (1988–1992)The interest in national networks was so great andthey grew so quickly that the first meeting of na-tional network coordinators was held in Helsinkiin 1988. This meeting brought together six net-works (including two from outside Europe), whichalready linked together 200 cities. In 1989, themovement had grown to include about 350 citiesin seven European national networks. During thistime, several subnational networks (such as inSpain) and language-based networks (such as aFrench-speaking network) had also been estab-lished. At a 1989 meeting in Eindhoven, coordina-tors defined a national healthy cities network asfollows.4
National healthy cities networks can be seen asorganizational structures to inspire and motivatecities to join the healthy cities movement, tohelp them exchange information and experi-ences and to create more favourable social, po-litical, economic and administrative conditionsfor the implementation of healthy cities strate-gies in their countries.
At the same meeting, coordinators proposed es-tablishing a European network of national healthycities networks called EURONET. One of its mainaims was to support the development of healthycities networks in the countries of central andeastern Europe and to facilitate training and re-source development. In 1994, EURONET was offi-cially founded as a legal organization and was ledby network members. An agreement of collabora-tion was signed with WHO, but EURONET lostimpetus a couple of years later.
Strengthening networks (1993–1997)WHO continued to encourage the development ofnational networks by requiring members of theWHO European Healthy Cities Network in its sec-ond phase to support the establishment of na-tional networks in their respective countries. Asthese networks matured, they demonstrated theirpotential to create a legitimate platform forchange and to respond to the diverse needs ofcountries. Cooperation between national net-works during this period focused on strengthen-ing the strategic capacity of national networksthrough exchange and training and supportingthe development of new networks in central andeastern Europe.5
A survey by WHO on national networks in1997 revealed that networks, although theyshared common goals and objectives, variedgreatly in their organization, participation criteriaand their level of access to and support from na-tional governments.6 The preparation for thelaunch of the third phase of the WHO EuropeanHealthy Cities Network in 1998 provided a newimpetus to reflect on the relationship between na-tional healthy cities networks and WHO.7 It wasdecided that WHO and national healthy citiesnetworks would need to collaborate more closelyfor national networks to reach their full potential
4 Goumans M. What about healthy networks? An analysis of
structure and organisation of national healthy cities networks in
Europe. Maastricht, Netherlands, Research for Healthy Cit-
ies Clearing House, 1992 (RHC Monograph Series No. 3).5 National healthy cities networks in Europe. 3rd ed. Copenha-
gen, WHO Regional Office for Europe (Centre for Urban
Health)/EURONET Association, 1997.6 Farrington J. The state of national networks for healthy cities.
Copenhagen, WHO Regional Office for Europe, 1997 (Cen-
tre for Urban Health).7 Goumans M. Strengthening the role of national healthy cities
networks in phase III of the WHO Healthy Cities project (1998–
2002). Discussion paper – Athens International Healthy Cities
Conference 20–23 June 1998. Copenhagen, WHO Regional
Office for Europe, 1998 (Centre for Urban Health).
31497_National.p65 06-10-2003, 08:0410

to promote and strengthen urban health acrossEurope. WHO had a major role to play in urgingnational governments to recognize national net-works as important structures and players in ur-ban and public health. This priority was reflectedin a 1998 resolution of the WHO Regional Com-mittee for Europe, which called for Member Statesto support national networks of healthy cities intheir coordinating and capacity-building role.8
Raising standards (1998–2002)Coordinators and political leaders from nationalhealthy cities networks have met together regu-larly and directly cooperated with WHO in a spe-cial European forum for networks.
An important achievement of this cooperationhas been the adoption of a set of standards forboth national healthy cities networks and theirmember cities, which are expressed as criteriawithin the WHO action framework for Europeannational healthy cities networks (Annexes 2, 3).9
This action framework aspires to raise the overallstandards of networks and their constituent cities.The document itself was quite radical at its incep-tion, as many national networks felt that findinga common set of criteria would be impossiblegiven the diversity of national policy contexts andthe resultant organization of networks.
The criteria of the action framework representthe best practices of national networks. The mini-
mum criteria for national networks set a bench-mark and provide guidance for establishing theinfrastructure of a national healthy cities network,and the ideal criteria provide a set of provenstandards for improving and strengthening a net-work.
As of September 2003, 18 networks had beenaccredited (the individual profiles of the nationalnetworks in Chapter 5 indicate whether the net-work was accredited and when). However, not allnetworks that fulfil the minimum criteria of theaction framework have been accredited. Some net-works are using the action framework as an oppor-tunity to create dialogue with new partners and tostrengthen their network structures.
The following chapters explore the organiza-tional factors and some of the key achievementsthat have formed the basis for developing Euro-pean-wide criteria for networks.
8 Healthy Cities. Strengthening action for health for all at local
and city levels in the European Region of WHO. Copenhagen,
WHO Regional Office for Europe, 1998 (http://
www.euro.who.int/AboutWHO/Governance/resolutions/
1998/20030430_4, accessed 17 September 2003).9 Action framework & terms of reference (2000–2002) – Network
of the European National Healthy Cities Networks. Copenha-
gen, WHO Regional Office for Europe, 2000 (http://
www.who.dk/eprise/main/who/progs/hcp/Documentation/
20011106_1, accessed 15 September 2003).
THE DEVELOPMENT OF THE WHO HEALTHY CITIES PROJECT IN EUROPE . 11
31497_National.p65 06-10-2003, 08:0411
12 . NATIONAL HEALTHY CITIES NETWORKS
2.Organization and leadership of national networks
based on statutes. Most networks are independ-ent, legal associations with not-for-profit status.
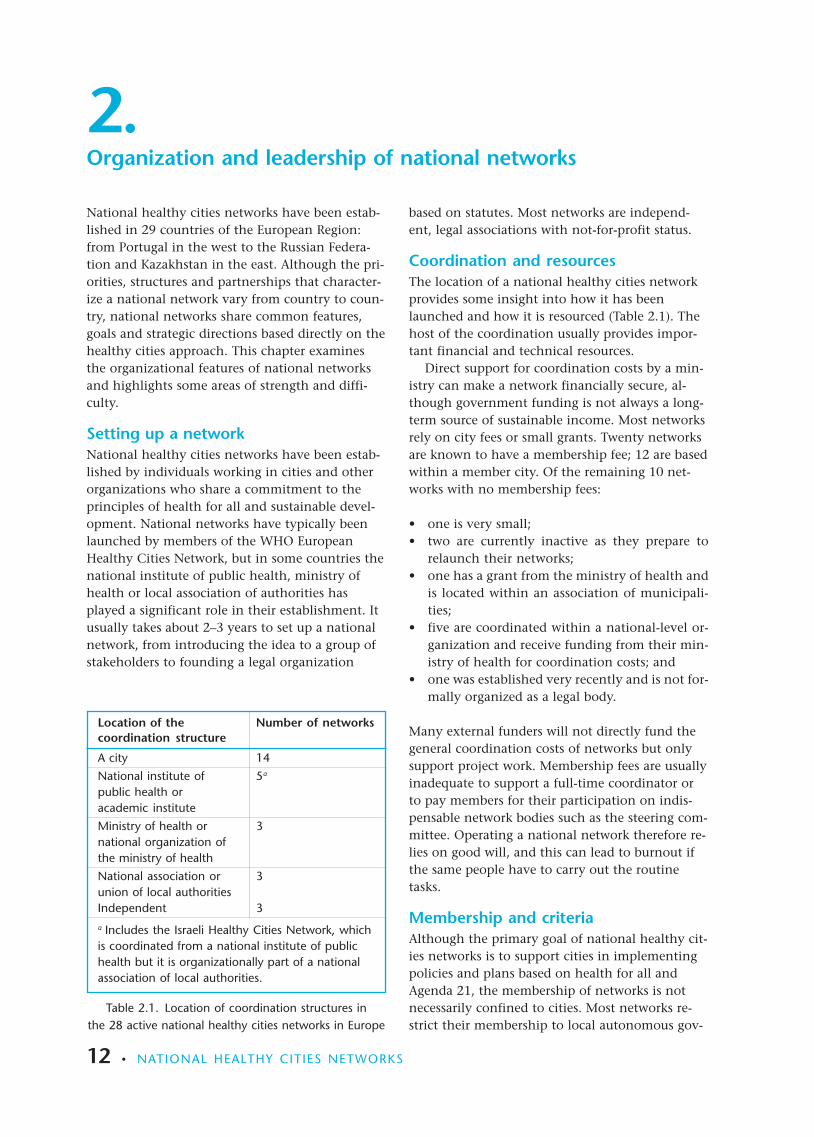
Coordination and resourcesThe location of a national healthy cities networkprovides some insight into how it has beenlaunched and how it is resourced (Table 2.1). Thehost of the coordination usually provides impor-tant financial and technical resources.
Direct support for coordination costs by a min-istry can make a network financially secure, al-though government funding is not always a long-term source of sustainable income. Most networksrely on city fees or small grants. Twenty networksare known to have a membership fee; 12 are basedwithin a member city. Of the remaining 10 net-works with no membership fees:
• one is very small;• two are currently inactive as they prepare to
relaunch their networks;• one has a grant from the ministry of health and
is located within an association of municipali-ties;
• five are coordinated within a national-level or-ganization and receive funding from their min-istry of health for coordination costs; and
• one was established very recently and is not for-mally organized as a legal body.
Many external funders will not directly fund thegeneral coordination costs of networks but onlysupport project work. Membership fees are usuallyinadequate to support a full-time coordinator orto pay members for their participation on indis-pensable network bodies such as the steering com-mittee. Operating a national network therefore re-lies on good will, and this can lead to burnout ifthe same people have to carry out the routinetasks.
Membership and criteriaAlthough the primary goal of national healthy cit-ies networks is to support cities in implementingpolicies and plans based on health for all andAgenda 21, the membership of networks is notnecessarily confined to cities. Most networks re-strict their membership to local autonomous gov-
National healthy cities networks have been estab-lished in 29 countries of the European Region:from Portugal in the west to the Russian Federa-tion and Kazakhstan in the east. Although the pri-orities, structures and partnerships that character-ize a national network vary from country to coun-try, national networks share common features,goals and strategic directions based directly on thehealthy cities approach. This chapter examinesthe organizational features of national networksand highlights some areas of strength and diffi-culty.
Setting up a networkNational healthy cities networks have been estab-lished by individuals working in cities and otherorganizations who share a commitment to theprinciples of health for all and sustainable devel-opment. National networks have typically beenlaunched by members of the WHO EuropeanHealthy Cities Network, but in some countries thenational institute of public health, ministry ofhealth or local association of authorities hasplayed a significant role in their establishment. Itusually takes about 2–3 years to set up a nationalnetwork, from introducing the idea to a group ofstakeholders to founding a legal organization
Table 2.1. Location of coordination structures inthe 28 active national healthy cities networks in Europe
Location of the Number of networkscoordination structure
A city 14
National institute of 5a
public health oracademic institute
Ministry of health or 3national organization ofthe ministry of health
National association or 3union of local authoritiesIndependent 3
a Includes the Israeli Healthy Cities Network, whichis coordinated from a national institute of publichealth but it is organizationally part of a nationalassociation of local authorities.
31497_National.p65 06-10-2003, 08:0412
ernment units (villages, towns, cities and coun-ties), but several networks open their membershipto representatives of ministries, nongovernmentalorganizations, universities, national associationsof cities and other health or sustainable develop-ment networks. For example, the National Assem-bly of Wales is a member of the UK Health for AllNetwork. Nearly all networks have membershipcriteria; only one network does not have any crite-ria as it operates on the principle of a completelyopen network.
Common governing structuresNetworks typically share the same structure ofgoverning bodies, which are often defined by legalrequirements for associations or not-for-profit or-ganizations. The main governing (decision-mak-ing) body is the general assembly, which com-prises the full members of the network. Most net-works require annual meetings of their general as-sembly, but in practice, networks meet more fre-quently. Networks usually elect or appoint mem-bers to a steering committee, which implementsgeneral assembly decisions and further developsthe strategic and technical work of the network.Networks established as legal organizations alsohave other formal offices or bodies such as a treas-urer or an audit committee. The leadership struc-tures of networks are described in greater detaillater.
Political and technical leadershipThe support and involvement of politicians inhealthy cities has been universally accepted as keyto its success. About half the national networksformally involve mayors and other local politi-cians in network structures. This gives a networkincreased legitimacy and a stronger voice at thenational level. Politicians ultimately command re-sources and have the power to make things hap-pen. For example, the enthusiastic and active par-ticipation of politicians in the Norwegian HealthyCities Network resulted in support for a full-timenational network coordinator.
Models of political involvement in networksThe national healthy cities networks in Europehave several models for direct political involve-ment, including a political steering committee, amixed steering committee, political and technicalsteering committees and a political head.
Political steering committee. The network has oneleadership body comprising entirely politicians.This body is supported by technical staff, but
they do not have a formal role or a separatestructure.Mixed steering committee. The network has oneleadership body that brings together both politi-cal and technical representatives.Political and technical steering committees. Thenetwork has two separate structures for politicaland technical leadership. A political steeringcommittee sets the strategic direction and goalsof the network. The technical committee imple-ments the decisions of the political committee.The two bodies typically cooperate closely.Political head. The network chooses a politicianto head the network, independent of his or herinvolvement in other network bodies. This istypically a mayor of a member city.
A couple of networks have gone a step further toinvolve national-level politicians. For example,the Estonian Healthy Cities Network has givenhigh priority to attracting political interest inhealthy cities through a national debate (see theprofile).
Balancing political involvementSome networks emphasize involving politicians inall network structures and activities, whereas oth-ers stress limiting political involvement to key ac-tivities that bring them clear added value – avoid-ing unnecessary demands on their time. Somenetworks struggle to establish mechanisms for ac-tive political involvement, whereas others havenot found the need for such involvement at all.For example, the Finnish Healthy Cities Networkdoes not involve politicians in any formal net-work structure. However, as member cities have toadopt the Network’s criteria and devote resourcesto network activities, politicians in Finland areregularly involved in local level debates onhealthy cities.
Sustaining local political commitmentSustaining local political interest and involvementin healthy cities is an issue for all networks, al-though the means for achieving this varies. Net-works must resolve politicians’ need for short-term results with the long-term vision for healthdevelopment of healthy cities. Coordinating net-work plans with municipal statutory requirements(such as planning and funding cycles) and coordi-nating the appointment of politicians to networksteering committees with election years havehelped some networks to facilitate the consistentinvolvement of politicians (Box 2.1).
ORGANIZATION AND LEADERSHIP OF NATIONAL NETWORKS . 13
31497_National.p65 06-10-2003, 08:0413

14 . NATIONAL HEALTHY CITIES NETWORKS
Box 2.1. Statement by Norway’s Minister for Health
Public health in NorwayNeeds great effortBoth the Norwegian government and thepolitical leadership in the Ministry of Healthare concerned with giving the public healthwork a push. In this context I would like toemphasize that I am not only a Minister forDisease, whose task is to make the curativeactivity more effective; I am also a Minister forPublic Health, who has to observe and haveinfluence across the various sectors of society.The roots of the health issues are not mainlylocated in the health services. I, and everybodywho is interested in public health, shouldtherefore care about how the communityarranges for bicycling and healthier diets; howthe schools deal with harassment and how theprofessional world can be health promotingand not health destructive. This is what I callthe greater health politics.
Needs partnersIn my opinion, it is extremely important to seegovernment and municipalities as partnerswho pull in the same direction in the workwith public health. They should be partnersthat work towards the same goals, but withdifferent roles and responsibilities. I am,however, fully aware of the various challengesattached to the work with public health for themunicipal sector. But there are also uniqueopportunities on the local level. From a central
Networking at many levelsNetworking does not stop with bringing cities to-gether at the national level. Cities cooperatewithin networks on thematic issues, and geo-graphically close cities may cooperate in separateregional networks. National networks frequentlyhave thematic work groups on issues such as acci-dents or healthy housing. Work developed bysmall working groups on thematic areas is thentypically disseminated nationally via network websites or national conferences.
Regional or metropolitan networks in somecountries help smaller cities and towns to becomemore actively involved in healthy cities and createsynergy for work on health issues with a regionaldimension (Box 2.2). These subnational networkscan also help some countries to overcome largegeographical distances that would otherwise pre-vent active networking.
point of view it is important not to putobstacles in the way for the local health workbut to prepare the frameworks and considerwhat kind of support is needed in the efforts atthe local level. The work with public healthcan be a lonely task for many small Norwegianmunicipalities. Knowledge, counselling, supplyof competence, and in some cases, a biggernetwork, is required.
Needs the Norwegian Healthy CitiesNetworkIn this connection we wish to explore thepossibilities of the kind of networking that yourepresent. The government neither shall norshould take over this functional way oforganizing the municipalities, but there areseveral reasons for looking for new forms ofalliances between such networks and thecentral governments.
If we want to see results of the work withpublic health, we must make a joint effort. Iwill surely do my part. I believe that themembers of the Norwegian Network – theleading municipalities on public health – willbe important partners when it is time to putthe politics into life in the coming years.
Dagfinn HøybråthenNorway’s Minister for HealthFebruary 2003
31497_National.p65 06-10-2003, 08:0414

1 Green G. Health and governance in European cities: a compen-
dium of trends and responsibilities for public health in 46 mem-
ber states of the WHO European Region. London, European
Hospital Management Journal Ltd, 1998.
Box 2.2. Regional, metropolitan and language-based healthy cities networks
Regional, metropolitan and language-basednetworks within countries are an interestingfeature of national healthy cities networks.Regional networks help to overcome barriersto participation based on geographicaldistances or language. Regional andmetropolitan networks also enable smallercities, towns or villages with limited resourcesto share expertise and benefits from theinternational experience of the Europeanhealthy cities movement. Importantly, thesenetworks enable cities to work together oncommon local problems that have a regionaldimension.
In Belgium, government is divided intolanguage-based communities and regionalassemblies. The language-based communitieshave directly elected councils responsible forhealth, education and social services. Healthycities networks in Belgium reflect thesestructures and are similarly organized into twolinguistic networks – a Flemish-speakingnetwork (currently inactive) and a French-speaking network.
Spain is divided into 17 autonomousregions with legislative powers and anindependent tax base. Municipalities arejointly responsible with the autonomous
regions for delivering a range of health-relatedservices, such as social welfare.1 Regionalnetworking is therefore a strong feature of theSpanish Healthy Cities Network. The Networkhas active regional networks in Andalusia,Castilla-La Mancha, Catalonia and onemetropolitan network in Madrid.
Germany, a large country, works throughfour regional healthy cities networks as well asat the national level.
Given the vast size of the RussianFederation, the Healthy Cities Support Centreis increasingly emphasizing developingpartnerships with the 89 regions.
Several regional healthy cities networkshave recently been established within theItalian Healthy Cities Network. Regionalhealthy cities networks have been set up inPuglia, Tuscany and Piedmont. These networksare expected to adopt the statutes andstructures of the Italian Healthy CitiesNetwork.
ORGANIZATION AND LEADERSHIP OF NATIONAL NETWORKS . 15
31497_National.p65 06-10-2003, 08:0415

16 . NATIONAL HEALTHY CITIES NETWORKS
3.Achievements and impact of national networks
Each national healthy cities network is unique. Atpresent, no clear pattern is identifiable betweenthe organizational development of networks andhow a country’s political system or health systemis organized. However, the existence or lack ofsupportive national and local policy frameworksfor health for all and sustainable development,and the roles and responsibilities for service deliv-ery among cities, regional structures and thepolicy frameworks of the national government allinfluence network development. Each network de-velops in response to the needs of its member cit-ies, opportunities to obtain financial and humanresources and its own cultural and legal frame-works. As this combination of factors varies enor-mously across the different countries in the Euro-pean Region, what can be defined as a nationalnetwork achievement also varies. What one net-work considers an achievement may not even bean aim for another.
Increasing understanding of the interplay be-tween these factors would provide useful insightfor supporting cities, organizations or individualsthat want to set up or enhance the sustainability ofnational healthy cities networks in the future.Analysis of the profiles of the national networks(available in Chapter 5 of this book) and nationalnetwork fact sheets1 already provides some insightinto the kinds of activities that strengthen net-works, regardless of how they are organized. Thischapter draws on this information and presents theachievements of national networks at the city andnational level to highlight the impact of nationalhealthy city networks. In so doing, the key func-tions of a network are highlighted. Some examplesof international cooperation are also presented.
Achievements at the city levelThe starting-point for a national network is tosupport the development of the healthy citiesmovement at the city level. They have an impor-tant role not only in recruiting new members butalso in continuing to ensure a high level of aware-ness of healthy cities principles among existingcity members. The status of an individual projectcan be enhanced if it is known to implement in-ternationally validated principles or if its successesare shared at a national conference.
Increasing the profile of healthy citiesIncreasing the profile of healthy cities is impor-tant for attracting new members and in ensuringthat resources are made available to the network.Similar to the WHO European Healthy Cities net-work, many national networks require their mem-ber cities to identify a political focal point for theproject. The involvement of politicians, especiallymayors, is vital to ensuring a high profile for ur-ban health within a municipality. For example,when Slovenian cities wish to join a new 5-yearphase of the Slovenian Healthy Cities Network, allthe mayors are invited to a prestigious signing cer-emony presided over by the Minister for Health.
In recent years, several networks have reorgan-ized their structures to strengthen political com-mitment in cities and to the national network.Italy provides an interesting example (see profile).
Sharing best practicesA network has a key role in disseminating newtechniques and supporting best practice amongthe members (Box 3.1).2 Healthy cities networksshare a number of common themes (such as pro-moting systematic planning) and methods of sup-porting cities (such as piloting initiatives through
Box 3.1. Examples of supporting bestpractices in citiesGrants to innovative projects (Poland)Letters of support for cities making grantapplications (Czech Republic)Presentations at prestigious conferencesSite visitsRegular newslettersProviding training and guidance materials
1 National network fact sheets. Copenhagen, WHO Regional
Office for Europe, 2002 (http://www.euro.who.int/healthy-
cities/CitiesAndNetworks/20020111_5, accessed 17 Septem-
ber 2003).2 Schweyer FX, Levasseur G, Pawlikowska T. Créer et piloter un
réseau de santé. Un outil de travail pour les équipes. Rennes,
Éditions de l’École nationale de la santé publique (ENSP),
2002.
31497_National.p65 06-10-2003, 08:0416

thematic groups, publishing manuals or creatingopportunities for exchanging good practice).
Regular business meetings and training coursescreate opportunities for members to formally andinformally exchange experience. Many networksalso use web sites, newsletters and publications toshare best practices. The Dutch Healthy CitiesNetwork sends its newsletter to all municipalities,ministries and other national partners, using it asa publicity tool as well as a method of promotingcommunication between members. The FrenchHealthy Cities Network produces an annual direc-tory that lists the main activities of all city mem-bers.
Many national networks have encouraged citiesto meet together to facilitate learning or to de-velop a joint action plan on a specific topic. Thesethematic networks (known as multi-city actionplans) can be important, as they enable cities toshare good practice. Some have produced valuablepublications. The thematic networks frequentlyappear to have a natural life of a couple of years,as they fulfil their main functions, such as provid-ing a forum for exchange, piloting new methodsand developing guidance.
In other networks, working groups operate on along-term basis. Members of the Danish HealthyCities Network are required to work in at least oneof the Network’s three work groups: health at theworkplace; accident prevention; and diet andphysical activity. The Network has become widelyrecognized for its work in these areas. For exam-ple, the Network has established a National Cen-tre for Workplace Health Promotion, with the sup-port and cooperation of the Ministry of the Inte-rior and Health.
Increasing capacityIncreasing capacity through training strengthensnational networks.3 Virtually all networks provideat least occasional training opportunities: for ex-ample, Latvia has just held a course on writingskills for project proposals. A few networks havegone a stage further and run either regular or ac-credited courses.
In 2002, the Israeli Healthy Cities Network rana course with 15 full-day sessions and two site vis-its. Participating in a longer course has led to thereactivation of the healthy city project in severalinactive cities and two new cities joining the Net-work. The course has lead to the creation of aclose multiethnic support group for the Israeli co-ordinators.
The Polish Healthy Cities Association providestwo types of training: general courses and those
on a specific theme. The general healthy citycourses usually last 1.5 days and are held just be-fore a general assembly. They are open to politi-cians and administrators, which helps to facilitatelasting close collaboration. A number of thematiccourses for specialized staff have been held onphysical activity, cardiovascular disease and othernational priorities.
The Croatian Healthy Cities Network runs a 2-week summer school for an international group ofhealthy city practitioners each year. It is a richsource of exchange of information but also dis-cusses health promotion philosophy. The Networkis also running courses for groups of people at thecounty level to learn how to carry out a participa-tory assessment of health status and how to de-sign a health profile. Half the counties in Croatiahave now attended (see profile).
In Sweden, a course was broadcast to munici-palities by videoconference. This has proven to bea very cost-effective and accessible way of raisingpublic health competencies, especially amongsmall municipalities in northern Sweden that of-ten have difficulty attending longer trainingevents. Sweden’s networks for public health workhave also used field visits to other cities to pro-mote exchange of best practices. They have in-volved approximately 180 professionals from pre-school teachers and school nurses to recreationleaders and environmentalists.
Supporting new working methodsA network has a key role in disseminating newtechniques and ways of working. Almost threequarters of the networks specifically focus on sup-porting cities in developing city profiles and/orplans. These techniques were originally developedin the WHO European Healthy Cities Network. Acity health profile is a quantitative and qualitativeanalysis of health in a city based on social, envi-ronmental and health data as well as the actualexperience of citizens. The profiles provide a basisfor a city to develop an intersectoral plan forhealth with its partners: a city health develop-ment plan. (Further practical information aboutprofiles and planning is available from the re-sources listed in Annex 1.) A criterion for joiningmost national networks is that member cities pro-
3 Reinicke WH et al., eds. Critical choices: the United Nations,
networks and the future of global governance. Ottawa, Interna-
tional Development Research Centre, 2000 (http://
www.gppi.net/cms/public/
a1224f819197be4e797e38bb6b6ba511critical%20choices%20final.pdf,
accessed 17 September 2003).
ACHIEVEMENTS AND IMPACT OF NATIONAL NETWORKS . 17
31497_National.p65 06-10-2003, 08:0417

18 . NATIONAL HEALTHY CITIES NETWORKS
duce a profile and a plan within a given timescale, but this may not always be enforced.
Cities in the Italian Healthy Cities Networkidentified integrated city health plans as a meansfor putting the health and well-being of citizens atthe heart of local decision-making. The first stepwas to produce a profile, and 18 cities had com-pleted theirs by January 2003. The Hungarian As-sociation of Healthy Cities is supporting its mem-ber cities by publishing a manual on city healthplanning. It is moving the focus from illness anddisease to looking at the determinants of health.
Rather than using existing data, the Norwegianand Austrian Healthy Cities Networks have under-taken population surveys in member cities. Thesurveys aim to establish community priorities andviews on health and environmental development.Both Networks undertook this labour-intensivetask, as they wished to generate positive healthdata rather than rely on existing statistics aboutdiseases or death rates.
Achievements at the national levelIncreasing the visibility of healthy citiesNetworks may increase their visibility at the na-tional level through strong political leadership,communication initiatives, high-profile confer-ences and strategic information disseminationthrough a newsletter or a web site. Three quartersof national networks now have web sites. Somenetworks publish attractive versions of their ownmanuals or annual reports. Some organize largeannual conferences open to a wide audience todisseminate the principles of healthy cities, suchas occurs in the United Kingdom.
The Hungarian Association of Healthy Citiesawards an annual prize to the best coverage ofhealthy cities-related activities in various forms ofnational and local mass media- television, radioand newspapers. It is presented by the Minister forHealth. The awards have raised both the qualityand the volume of media coverage on health andenvironmental issues as well as the visibility ofthe healthy cities movement in Hungary. The Por-tuguese Healthy Cities Network has recently or-ganized a similar award. This spreading of an ef-fective means of communication illustrates the
Box 3.2. Statement by Denmark’s Minister for the Interior and Health
A model for cooperation in promoting healthat the local levelAs Minister for the Interior and Health, I findthe Danish Healthy Cities Network very useful.It is both a model for cooperation between thethree political and administrative levels inDenmark (the Government, the regions andthe municipalities) and a vehicle that helps toplace health promotion and diseaseprevention on the political agenda.The healthy cities work has increased politicalattention on and social awareness of the workinvolved in promoting health and preventingdisease in Denmark. The Ministry of theInterior and Health has therefore financiallysupported the activities of the Network formore than 10 years.Overall, the Network has comprised a veryimportant, productive and cooperativeenvironment for developing andimplementing methods of promoting healthand preventing disease and for disseminatinginformation about these methods. Methodsdeveloped through the Network have beenwidely implemented – even in municipalities
that are not members of the Network. Inaddition, efforts to improve health have reallyreached out to the wider population, achievingvery high visibility.Denmark’s Network has great significance forspecific initiatives around the country.Valuable experiences are being incorporatedand useful knowledge is being compiled abouthow best to tackle the issues. It is exciting thatthis is happening within a network,horizontally and with minimal bureaucracy.Through its success in promoting health, theDanish Healthy Cities Network has proved tobe a strong partnership. I would like to takethis opportunity to acknowledge and tocommend the Network’s great contribution tostrengthening the efforts in this field inDenmark.
Lars Løkke RasmussenMinister for the Interior and HealthDenmarkFebruary 2003
31497_National.p65 06-10-2003, 08:0418
one of the benefits of the international network-ing between the national healthy cities networks.
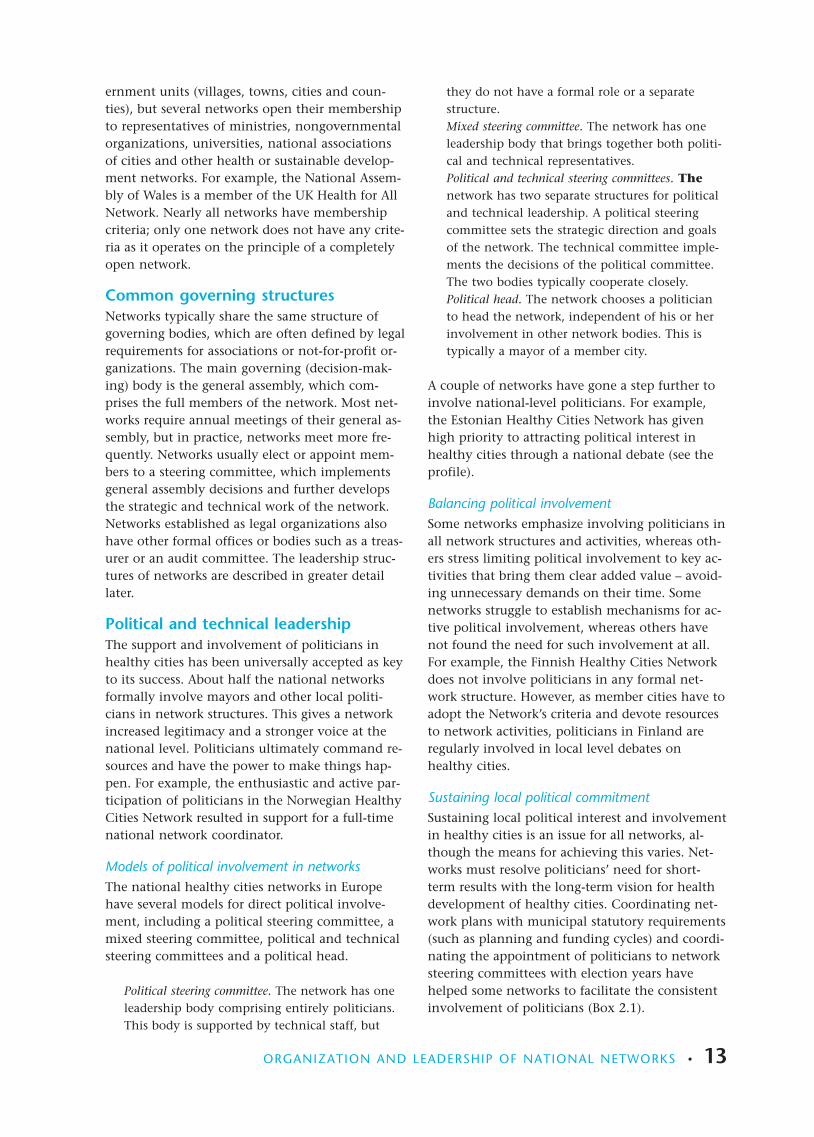
Developing strategic partnershipsIn addition to encouraging cities to collaborate to-gether, a significant role of a national healthy cit-ies network is to link with national partners suchas government ministries (Box 3.2) and institutesof public health. Cooperation with these partnerscan help to place urban health higher on the na-tional agenda and provide the member cities withaccess to expertise. Twenty-five networks reportthat they have a partnership with their ministryof health (Table 3.1). This is a significant achieve-ment, as national networks have consistentlyidentified this as an area of difficulty in the past.4
The nature of network partnerships varies.Some national networks have very close links withnational structures, which may provide coordina-tion support to the network. For example, Tur-key’s Ministry of Health introduced the healthycities initiative in Turkey in 1993 and coordinatesthe network. The Kazakhstan Healthy Cities Net-work reports that it benefits from the support ofthe President and the First Lady and is part of thenational government policy.
Whereas the partnerships between networksand ministries or other national-level bodies usedto be based primarily on funding, in 2003 about85% of networks refer to more strategic workingrelationships with several government bodies – es-pecially ministries responsible for health and theenvironment. For example, the Ministries ofHealth, Environmental Protection, Education andLabour & Welfare are formal members of the Is-raeli Healthy Cities Network. The Network partici-pated in preparing Israel’s national report on theHabitat Agenda, which recognized healthy cities
as a useful vehicle for implementing both theHabitat Agenda5 and Local Agenda 21.
National institutes of public health, universitiesand other research organizations have become in-creasingly important partners for many networks.They can support networks in evaluating theirwork (Box 3.3) and in developing sound meth-odological approaches for core work such as thedevelopment of city health profiles. The HealthyCities Support Centre in the Russian Federation,based within the Institute of Public Health andHealth Care Management of the Sechenov Mos-cow Medical Academy, supported cities in devel-oping a set of 29 qualitative and quantitative indi-cators for use by specialists, decision-makers andcitizens.
An interesting trend among national networksis the establishment of new organizations in col-laboration with national partners. For example,the Association of Healthy Cities of Slovakia hasestablished a Slovak Public Health Association incooperation with national partners.
Influencing national policyAn important aim for national healthy cities net-works is to influence national public healthpolicy. Many networks report a role in influencingnational public health policies by taking part ingovernment advisory groups or national commit-tees. Recognized for its expertise in urban healthand sustainable development, the Hungarian As-sociation of Healthy Cities is a member of a sub-committee of the National Committee on HealthPromotion. The network had responsibilitiesaround the local implementation of Hungary’s na-tional environment and health action plan.
The Government of Slovenia is reorienting thework of the Ministry of Health to increase its fo-cus on health promotion. The Healthy City Cen-tre will be responsible for coordinating this part ofthe national plan – the only part to be coordi-nated outside the National Institute of PublicHealth. All regions in Slovenia will now imple-ment a healthy city approach.
Responding to national prioritiesMany national networks have become importantvehicles for supporting cities in responding to na-
Table 3.1. Partners of the 30 national healthy citiesnetworks in Europe
Type of partner Number of networks
Ministry of health 25
Other ministries orgovernment bodies 14
Unions or associations oflocal authorities 13
National institutes(public health orhealth promotion) 12
Universities orresearch institutes 10
4 Rothstein L. The state of national networks for healthy cities.
Copenhagen, WHO Regional Office for Europe, 1999 (Cen-
tre for Urban Health).5 The Habitat Agenda. Geneva, United Nations Human Settle-
ments Programme, 1996 (http://www.unhabitat.org/unchs/
english/hagenda, accessed 17 September 2003).
ACHIEVEMENTS AND IMPACT OF NATIONAL NETWORKS . 19
31497_National.p65 06-10-2003, 08:0419

20 . NATIONAL HEALTHY CITIES NETWORKS
tional health priorities. Networks provide accessto knowledge and resources that enable and en-courage cities to develop new local initiatives. Forexample, injuries are the third largest cause ofdeath in the Czech Republic and the main causeof death among children and adolescents. Injuryprevention has therefore become a priority forHealthy Cities of the Czech Republic and its part-ners. The network is promoting the principles ofSafe Communities, another WHO network.
The early detection and prevention of breastcancer is a priority for the Poland’s nationalhealth programme and the Polish Healthy CitiesAssociation. Programmes implemented by healthycities include training courses for health profes-sionals, organizing screening examinations, popu-larizing regular breast self-examination and healtheducation for women. The 21 cities involved inthis work cover 2.5 million women. The pro-grammes have become permanent items in citybudgets. Women’s awareness on the subject hasrisen, and their participation has demonstratedsocial demand for these activities.
International collaboration betweennetworksSeveral networks have collaborated outside theformat of WHO business meetings. These contactsare most frequent between networks that share alanguage or a common border (Box 3.4). For ex-ample, the Croatian Healthy Cities Network hasprovided training and support to the recently es-tablished Bosnia and Herzegovina Healthy CitiesNetwork. The networks in the Czech Republic,Slovakia and Hungary are involved in regular ex-change. French-speaking networks (France andBelgium) with representatives from Switzerland,North Africa and Canada organize a biannual in-ternational conference on healthy city practices.
Norway has invited the other Nordic healthycity networks to develop a Nordic Health and En-vironment Profile based on the Norwegian Profile.This is planned to take place in 2004–2005 (seeNorway’s profile).
Box 3.3. Evaluation of national networks
Over one third of national networks haveevaluated the organization and activities ofmember cities.
Seven national networks have gone a stagefurther and have evaluated their ownactivities. The evaluation of national networkactivities can help to highlight the network’ssuccesses (which could support requests forfunding). They can indicate areas of weaknessand suggest responses that could strengthenthe future development of a network. Somenetworks use a simple self-evaluation process,such as Finland, but most prefer an externalinstitution.
An evaluation in Sweden in 2001 lead to aradical restructuring of its national networks.Sweden had two networks: one for large townsand one for medium-sized towns. Theevaluation found that the networks hadprovided valuable support for thedevelopment of local public health inmunicipalities but that they were too looselyassociated, they financially depended on theNational Institute of Public Health and theylacked clear membership criteria. A singlenational network is currently being establishedin Sweden with precise membership criteria.
Ljubljana University evaluates the SlovenianHealthy Cities Network annually. The resultsare presented as part of the Network’s annualreport, which is sent to the Ministry of Health(a main funder of the Network). The lastevaluation included how the Network shouldprovide systematic help for cities in difficultyafter an election creating political change. Italso suggested that associate membership belimited to a period of 6 months, as someassociate member cities did not progress todeveloping city health profiles and otherdeliverables, and this was recognized asnegative for the overall development of theNetwork.
Evaluation of the Danish Healthy CitiesNetwork by the National Institute of PublicHealth has demonstrated that the Network hasinfluenced national-level policies and createdgreater political interest in health.Participation in the Network makesundertaking new activities easier for cities. TheNetwork’s thematic work gives members thespace to develop expertise in certain topics.Members also have a one-stop access point tonational health information.
31497_National.p65 06-10-2003, 08:0420

The influence of national networksAmple evidence from questionnaires and analysescarried out in the European Region, including thesurvey performed for this publication, indicatesthat national networks have important influenceacross Europe.6 The outcomes of long-establishednational healthy cities networks show a clear po-tential:
• to strengthen local institutional effectivenessby supporting cities in adopting good govern-ance approaches based on the principles ofhealth for all and Agenda 21;
• to inform national policy development by crys-tallizing local needs;
• to create a platform for municipalities to sharebest practices and to cooperate with nationalministries, regional-level governments, aca-demic institutes, nongovernmental organiza-tions and other important actors in heath andsustainable development;
• to provide a testing ground for new policies;• to promote best practices by setting standards,
producing guidance and providing training;and
• to generate and disseminate knowledge andnew ideas through exchange, conferences,newsletters, web sites and even by establishingnew organizations.
National networks encourage cities to move awayfrom a culture of organizing single health eventsto a culture of producing strategic health plans inwhich promoting health becomes an aim for allcity departments. National networks can draw onmembers’ individual and joint successes to de-
velop and disseminate innovative practices,thereby attracting more publicity and recognitionof the healthy city movement. This increases thenumber of cities interested in promoting healthycity principles and the quality of work withinmember cities.
At the national level, networks have served as alink between government policy and local action.They have enabled experience gained on theground to be channelled upwards to influence na-tional thinking and have helped to disseminategood practice from national or international poli-cies and research to cities.
In practice, the pooling of practical expertise ofurban health has meant that national healthy citynetworks have become an important national re-source. Not only do they provide valuable supportto their members but they can advise nationalgovernment and other national institutions on ef-fective models of promoting sustainable urbanhealth.
Box 3.4.Cooperation in the Baltic regionThe Baltic Region Healthy Cities Officesupports the development of healthy cities,and especially national healthy citiesnetworks, in the region surrounding theBaltic Sea. It was opened in 2002 and is basedin Turku, Finland. Sixteen national networksattended an international seminar organizedto mark its official launch.
The Office will organize annual meetingsand will provide a web-based informationdatabase on the national healthy citiesnetworks and their activities. The Office willhelp networks to develop training and buildcapacity according to need and to seek
6 Rothstein L. The state of national networks for healthy cities.
Copenhagen, WHO Regional Office for Europe, 1999 (Cen-
tre for Urban Health).
Network of European National Healthy Cities Networks: report
on a WHO business meeting, Brno, Czech Republic, 31 May–2
June 2001. Copenhagen, WHO Regional Office for Europe
(in press).
National network fact sheets. Copenhagen, WHO Regional
Office for Europe, 2002 (http://www.euro.who.int/healthy-
cities/CitiesAndNetworks/20020111_5, accessed 17 Septem-
ber 2003).
ACHIEVEMENTS AND IMPACT OF NATIONAL NETWORKS . 21
31497_National.p65 06-10-2003, 08:0421
22 . NATIONAL HEALTHY CITIES NETWORKS
4.Developing effective national networks for the future
InfrastructureA network should be formally organized under aconstitution or set of statutes. The network shouldhave a central office with technical, administra-tive and financial resources. Depending on thesize of the network, it should have a paid coordi-nator and secretariat or a number of people whoare prepared to take on administrative tasks.
A steering committee should be established tolead and develop the network. Ideally, thereshould be a mechanism to involve a wide range ofstakeholders in the network. Networks shouldnominate a politician to formally represent thenetwork. Chapter 2 described several models fordirect political involvement and leadership.
The network should have clear membership cri-teria for cities, based on the minimum and idealcriteria described in the WHO action frameworkfor European national healthy cities networks (An-nex 3). Network criteria should increase the qual-ity of healthy city work carried out at the locallevel.
Products and outcomesA network should have a clear programme of ac-tivities guided by national and local policy con-texts. Systematic approaches to network activitiesshould allow a network to achieve influence onseveral levels. A network should raise the capacityof cities to implement approaches based on healthfor all and Agenda 21 in response to local and na-tional priorities. It should also synthesize andevaluate this experience to produce case studies,set standards, develop guidelines and inform oradvise policy development at other levels of gov-ernment. Networks should provide clear lines of
The previous chapters have highlighted commonorganizational features, functions and activitiesthat contribute towards enabling networks toachieve sustainable outcomes at many levels. Thischapter draws on these outcomes to make recom-mendations for a successful national healthy citiesnetwork. It is not enough to apply these recom-mendations. Some of the most common chal-lenges and examples of how some networks re-spond to them are described below. This chapterconcludes with a discussion of the future steps fornational networks in Europe.
Criteria for a successful healthy citiesnetworkSeveral surveys and analyses of national networkshave been carried out in the past 5 years.1 Theyhave identified common structural and organiza-tion features and activities that have enabled thesuccessful development of healthy cities in acountry. Based on these findings, the WHO Cen-tre for Urban Health and national healthy citiesnetworks have identified several cross-cutting cri-teria for national networks and their member cit-ies that are consistent with the four action ele-ments of the healthy cities approach described inChapter 1: endorsing principles and strategies, es-tablishing infrastructure, making a commitmentto products and outcomes, and networking. Thecriteria for networks, based on these four actionelements, are described in more detail below.
Endorsement of principles and strategiesA national healthy cities network should fostercommitment to the principles and strategies thatunderpin the healthy cities approach. Ideally, thenational network should be able to demonstratebroad partnerships with a range of partners, in-cluding ministries of health, national associationsof local authorities, national institutes of publichealth and sustainable development organizationsand networks. A national network should strive tostrongly advocate the development of healthy cit-ies in a country and provide a platform for citiesto engage with other government andnongovernmental actors in health and sustainabledevelopment.
1 Rothstein L. The state of national networks for healthy cities.
Copenhagen, WHO Regional Office for Europe, 1999 (Cen-
tre for Urban Health).
Network of European National Healthy Cities Networks: report
on a WHO business meeting, Brno, Czech Republic, 31 May–2
June 2001. Copenhagen, WHO Regional Office for Europe
(in press).
National network fact sheets. Copenhagen, WHO Regional
Office for Europe, 2002 (http://www.euro.who.int/healthy-
cities/CitiesAndNetworks/20020111_5, accessed 17 Septem-
ber 2003).
31497_National.p65 06-10-2003, 08:0422
communication between partners and provide op-portunities for exchange and learning. Many na-tional networks have succeeded in becoming aclearinghouse for information on urban healthdevelopment in their countries and an essentialpartner for national governments.
NetworkingNational healthy cities networks should not onlycreate opportunities for their members to networkat the national level but should also representtheir networks in the European-level healthy citiesmeetings. Ideally, networks should actively pro-mote cooperation and exchange with other net-works and organizations active in health and sus-tainable development at all levels. This book men-tions several examples of international coopera-tion and mentoring.
Challenges and dilemmasNetworks face several dilemmas that make meet-ing the above criteria and goals difficult. The widerange of roles a network should ideally be able tomanage is ultimately influenced by staffing andresources. As most national networks depend on apart-time coordinator and enthusiastic volunteers,they must balance a range of interests and priori-ties.
Quantity versus qualityA dilemma for national networks is to increase thesize of their networks and the impact of healthycities in a country while ensuring that the workcities carry out is of a high standard. This is im-portant for developing criteria for cities. If the cri-teria are too strict, some cities will be excludedfrom participation. Excessively weak criteria mayjeopardize the quality of local work and ulti-mately the legitimacy of the network as a whole.Some networks have solved this problem by creat-ing different categories of membership.
Ultimately, a network’s growth in membershipis limited by its capacity to support its members.As networks grow, new solutions need to be foundto manage the participation of a larger number ofcities. Two possible solutions are developing re-gional support centres and developingsubnational networks.
Maintaining standards in citiesSome cities meet a set of healthy city criteria uponjoining a network but later become inactive, usu-ally because of local political changes or financialcutbacks. Although an inactive city sharing thesame healthy city label as those that are very ac-
tive is not fair, penalizing the city may cause em-barrassment and prevent future cooperation withthe network. Longstanding networks report thatcities tend to have periods of high and low activ-ity and believe that creating a system in which cit-ies would either have their status demoted or beexcluded from the network would not be benefi-cial. This runs contrary to the spirit of nationalhealthy cities networks, which are highly partici-patory and service-minded. Networks exist to sup-port cities, but the sustainability of networks overtime also depends on their capacity to show re-sults and added value.
Networks have responded to this problem inseveral ways. For example, some networks work inphases. Like the WHO European Healthy CitiesNetwork, this allows cities to join a national net-work for a set time period and to exit the networkgracefully, if desired. Requiring cities to reapplyperiodically also offers a network means to main-tain standards of quality. Particular attentionneeds to be paid to facilitating active political par-ticipation in the network. Many network coordi-nators regularly visit and consult with city mayorsand other local politicians to sustain their com-mitment and interest in the network.
Clear criteria for member cities (such as thoseproposed in Annex 3) can also help to support ac-tive participation in a network. Requirements forthe development of new structures to manage thehealthy city process in cities and to dedicate re-sources to this work helps to keep the debate on ahealthy city alive in cities. Most national networksrequire a formal political commitment to the net-work, either in the form of a political statementby the mayor or, more often, a council resolution.Some networks have developed systems for renew-ing this political commitment regularly.
Taking action at the national and local levelsThe support networks offer cities catalyses the de-velopment of local-level expertise, which makes anetwork an interesting partner for national-levelactors. The development of national-level partner-ships and participation in the formulation of pub-lic health policies:• strengthens the legitimacy of the network, both
at the national and local levels;• often increases the network’s access to financial
and technical resources; and• contributes to creating a supportive policy
framework for local healthy city work.
Although the benefits arising from this dual roleare interlinked, work at both the local and the na-
DEVELOPING EFFECTIVE NATIONAL NETWORKS FOR THE FUTURE . 23
31497_National.p65 06-10-2003, 08:0423
24 . NATIONAL HEALTHY CITIES NETWORKS
tional levels requires a substantial time commit-ment, which can be difficult to balance given thelimited technical and financial resources availableto many networks.
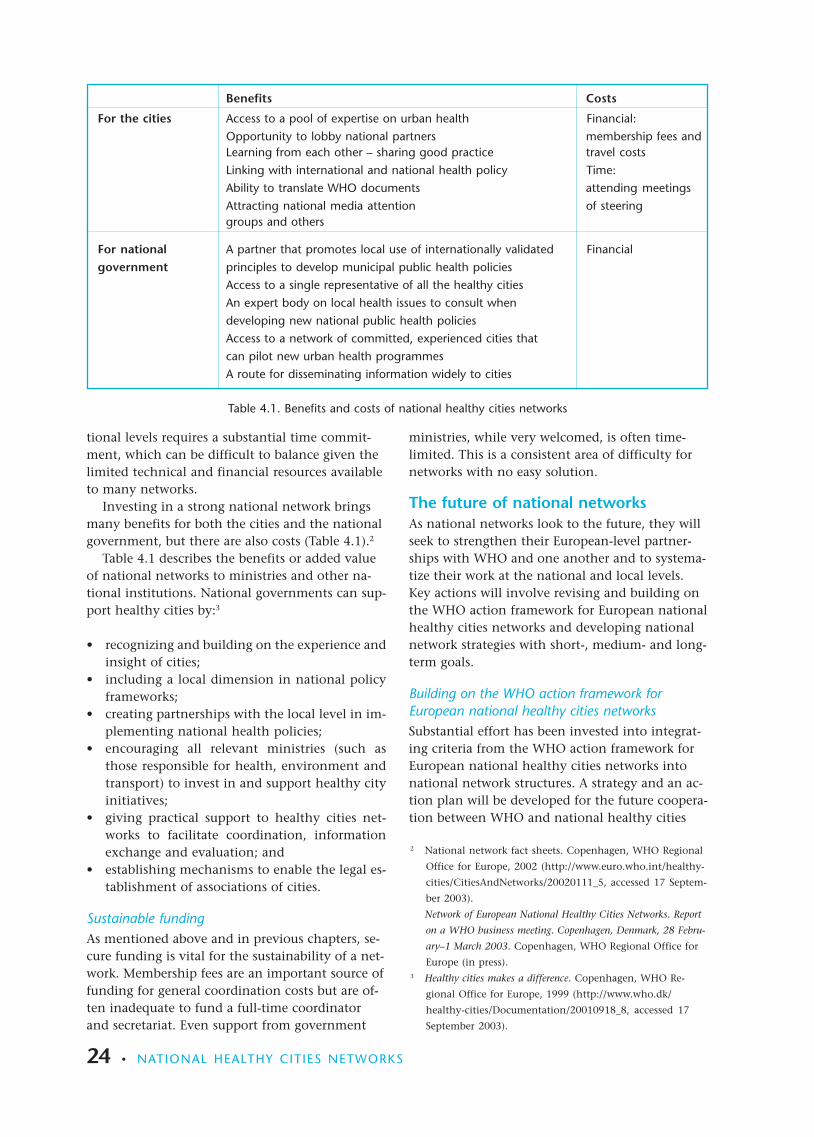
Investing in a strong national network bringsmany benefits for both the cities and the nationalgovernment, but there are also costs (Table 4.1).2
Table 4.1 describes the benefits or added valueof national networks to ministries and other na-tional institutions. National governments can sup-port healthy cities by:3
• recognizing and building on the experience andinsight of cities;
• including a local dimension in national policyframeworks;
• creating partnerships with the local level in im-plementing national health policies;
• encouraging all relevant ministries (such asthose responsible for health, environment andtransport) to invest in and support healthy cityinitiatives;
• giving practical support to healthy cities net-works to facilitate coordination, informationexchange and evaluation; and
• establishing mechanisms to enable the legal es-tablishment of associations of cities.
Sustainable fundingAs mentioned above and in previous chapters, se-cure funding is vital for the sustainability of a net-work. Membership fees are an important source offunding for general coordination costs but are of-ten inadequate to fund a full-time coordinatorand secretariat. Even support from government
ministries, while very welcomed, is often time-limited. This is a consistent area of difficulty fornetworks with no easy solution.
The future of national networksAs national networks look to the future, they willseek to strengthen their European-level partner-ships with WHO and one another and to systema-tize their work at the national and local levels.Key actions will involve revising and building onthe WHO action framework for European nationalhealthy cities networks and developing nationalnetwork strategies with short-, medium- and long-term goals.
Building on the WHO action framework forEuropean national healthy cities networksSubstantial effort has been invested into integrat-ing criteria from the WHO action framework forEuropean national healthy cities networks intonational network structures. A strategy and an ac-tion plan will be developed for the future coopera-tion between WHO and national healthy cities
Benefits Costs
For the cities Access to a pool of expertise on urban health Financial:Opportunity to lobby national partners membership fees andLearning from each other – sharing good practice travel costsLinking with international and national health policy Time:Ability to translate WHO documents attending meetingsAttracting national media attention of steeringgroups and others
For national A partner that promotes local use of internationally validated Financialgovernment principles to develop municipal public health policies
Access to a single representative of all the healthy citiesAn expert body on local health issues to consult whendeveloping new national public health policiesAccess to a network of committed, experienced cities thatcan pilot new urban health programmesA route for disseminating information widely to cities
Table 4.1. Benefits and costs of national healthy cities networks
2 National network fact sheets. Copenhagen, WHO Regional
Office for Europe, 2002 (http://www.euro.who.int/healthy-
cities/CitiesAndNetworks/20020111_5, accessed 17 Septem-
ber 2003).
Network of European National Healthy Cities Networks. Report
on a WHO business meeting. Copenhagen, Denmark, 28 Febru-
ary–1 March 2003. Copenhagen, WHO Regional Office for
Europe (in press).3 Healthy cities makes a difference. Copenhagen, WHO Re-
gional Office for Europe, 1999 (http://www.who.dk/
healthy-cities/Documentation/20010918_8, accessed 17
September 2003).
31497_National.p65 06-10-2003, 08:0424
networks based on the action framework and onthe lessons learned in the past 5 years. This strat-egy will be strongly linked to the fourth phase ofthe WHO European Healthy Cities Network.4 Thefourth phase will include work on the followingcore developmental themes:
• partnership-based plans for health and sustain-able development
• healthy urban planning• health impact assessment• healthy ageing.
Developing national network strategiesAt a February 2002 business meeting in Newcastle,United Kingdom, participants discussed the futureof national healthy cities networks. An importantoutcome was a decision that networks should es-tablish national network strategies. As a follow-upto this decision, WHO presented a definition anda framework for national network strategies at thenext meeting.5
A national network strategy was defined as fol-lows.
A national network strategy sets out the strategicgoals and the expected results of the work of thenetwork within a fixed time framework. It pro-vides the rationale for the directions and actionschosen and indicators to judge progress. The na-tional network strategy is a tool for systematicthinking and action and a basis for partnership-building and transparency.
The structure of a national network strategyshould incorporate common European goals butbe flexible enough to respond to diverse nationaland local policy contexts. The strategies will in-clude explicit goals and objectives and mark ashift from ad hoc to systematic planning. The keycomponents of such a plan include a descriptionof a network’s vision, goals and objectives and acontext for a set of actions, structures and re-sources, and it should define a time frame.
A national network strategy should combinethree main levels of action (local, national and in-ternational) guided by the principles and strate-gies of health for all and Agenda 21. The strategieswill address promoting the mission and objectivesof the network; making friends, joining forces andbecoming a credible policy actor; supporting deci-sion-making; sustaining and increasing member-ship; and carrying out key functions.
Promoting the mission and objectives of the net-work. The national network strategy should posi-
tion the network within the national and localpolicy context, taking into account the interac-tion between different levels of government andtheir health-related responsibilities. Networksshould think through the implications and oppor-tunities arising from this vision.
Making friends, joining forces and becoming a cred-ible policy actor. National networks should buildpartnerships with national government ministries,nongovernmental organizations and other impor-tant actors in health and sustainable develop-ment. Networks should provide a platform for cit-ies to engage with other actors as a resource to alllevels of government, creating an enabling envi-ronment. National networks should not only lookto the national level for resources but also aim tosupport national governments. At the interna-tional level, established national networks shouldtake on a mentoring role to support the 23 coun-tries in the WHO European Region that have yetto establish healthy cities networks.
Supporting decision-making. Network strategiesmust clearly define the political dimension of itswork. The technical development of the networkshould aim to support decision-makers in devel-oping the capacity to manage change.
Sustaining and increasing membership. An impor-tant role of networks is to both support and en-able existing members and to attract new cities tothe healthy cities movement.
Carrying out key functions. Some of the key func-tions networks need to carry out to fulfil their ob-jectives include training and capacity-building, in-formation exchange and dissemination, consulta-tion and advice, advocacy and communication,evaluation and reporting and resource develop-ment. Networks should assess urban health needsto become a centre for knowledge on the urbanhealth, social and environmental situation incountries.
Looking towards the futureNational networks of healthy cities represent apowerful force for health and sustainable develop-ment in Europe. They are a national resource ofurban health expertise, provide a platform for
4 Network of European National Healthy Cities Networks: report
on a WHO business meeting, Copenhagen, Denmark, 28 Febru-
ary–1 March 2003. Copenhagen, WHO Regional Office for
Europe (in press).5 Network of European National Healthy Cities Networks: report
on a WHO business meeting, Copenhagen, Denmark, 28 Febru-
ary–1 March 2003. Copenhagen, WHO Regional Office for
Europe (in press).
DEVELOPING EFFECTIVE NATIONAL NETWORKS FOR THE FUTURE . 25
31497_National.p65 06-10-2003, 08:0425

26 . NATIONAL HEALTHY CITIES NETWORKS
wide participation and exchange between citiesand can promote solidarity within and betweencountries. Networks can facilitate effective localresponses to national priorities and bring togetherlocal needs and experiences to better informpolicy development at all levels. National networkstrategies provide a basis for strengthening the ac-tion and outcomes of national networks in the fu-ture by building on the best practices described inthis book. The large number of international
agencies, European institutions and internationalnetworks focusing on urban sustainable develop-ment present exciting opportunities for nationalhealthy cities networks to expand their partner-ships and take forward the strategic agenda ofhealthy cities. In the future, WHO will continueto work in partnership with European nationalhealthy cities networks and support them inreaching their full potential.
31497_National.p65 06-10-2003, 08:0426
5.Profiles of the national healthy cities networks in Europe
31497_National.p65 06-10-2003, 08:0427

28 . NATIONAL HEALTHY CITIES NETWORKS
AustriaCountry factsPopulation: 8.1 millionUrban population: 65%Population living in network cities: 43%
Network factsAccredited: 2001Established: 1992Members: 31Organization: associationWeb site: http://staedtebund.wien.at(click on “Ausschüsse”)
BackgroundThe Austrian Healthy Cities Network was estab-lished in 1992 as a committee of the Austrian Fed-eration of Cities. Today, the Network is a legal as-sociation of 31 cities and towns. The Network isled by an 11-member political board, includingmayors, vice-mayors and local councillors and theSecretary-General of the Austrian Association ofCities and Towns.
Advancing health promotion in citiesA critical assessment of the Austrian Healthy Cit-ies Network carried out by external experts work-ing in scientific institutions and similar agenciesin 2000 demonstrated that health promotion hadbeen further developed in member cities as a di-rect result of their participation in the Network.This was measured in terms of resource allocation,personnel and infrastructures. Today, health pro-motion in Network member cities is a fixed itemin city budgets. Local politicians and official rep-resentatives have significantly increased their in-terest in health by participating in the Network.
A new model for reporting healthIn 2000, the Network developed a new, standard-ized model for a comprehensive municipal healthreport with the support of the Fund for a HealthyAustria. Austrian cities had already produced mu-nicipal health reports in the 1980s and 1990s, butthese had mainly been carried out by health au-thorities and focused on traditional health data,such as mortality, morbidity and hospitalizationdata. The Austrian healthy cities model, buildingon WHO’s broad definition of health, includes in-formation on:
• lifestyles• nutrition• exercise• the environment• workplaces• social factors.
This information is obtained through a householdsurvey of citizens (see below), which is an integralpart of the Network’s municipal health report. Inthe future, municipal health reports are expectedto yield valuable data for evaluating and compar-ing progress in cities.
Moving forwardThe Network’s 5-year action plan (2001–2005) setsout the following objectives for the Network:• All cities should prepare a health report.• All cities should take on at least 10 health for all
targets.• The Network should increase its membership.• The Network should support cities in involving
citizens.The Network also aims to strengthen its coopera-tion and exchange with other national healthycities networks in Europe.
Health comes into being where people live and work. The city, as living space for more and morepeople, is exactly the place where health can be developed whenever the conditions allow. Healthycities are trying to create these conditions, and the last 10 years since the foundation of our Networkshow that we are on the right track. Our efforts are concentrated currently on municipal healthreports, participation of citizens, local health report conferences and health promotion for women.Beyond this, our healthy cities try to implement the HEALTH21 policy of the WHO, and in my city, Linz,this programme is the basis for a 10-year running health promotion plan.
Christiana Dolezal, City Councillor, Linz, Chair, Austrian Healthy Cities Network
31497_National.p65 06-10-2003, 08:0428
For more information, contact:Peter LüfteneggerNetzwerk Gesunde Städte ÖsterreichsSchottenring 24A-1010 ViennaAustria
Spotlight on AustriaPerceptions of health and well-being. A person’ssense of health and well-being are closelylinked, but only about half the people whofelt perfectly healthy also felt perfectly happy.The survey found that happiness required notonly health and affluence – it requires bal-ance, personal relationships, finding meaningin one’s life and a favourable social environ-ment.
Older and happier. The analysis found that peo-ple’s perception of health takes a characteris-tic course, depending on age. People olderthan 50 years felt happier – or at least said sowhen questioned. Is the generation of thetough years of the last century more easily sat-isfied? Do people have to learn happiness fordecades? Does the new generation fall into ahistorical gap of insecurity?
Education. The analysis could not conclusivelyaccount for the link between education andbetter health. It is a mystery why educatedpeople are healthier. It is not just the knowl-edge, nor is it just the higher income – on topof that it is probably also autonomy and asense of self-worth, better access to informa-tion and an alternative culture. Perhaps nowa-days education pays more in terms of healththan of money.
Taking action. The survey is to be repeated af-ter 3 years to demonstrate whether the newhealth measures adopted in the three townshave been successful in remedying the weakpoints in the population’s health. Policy-mak-ers have welcomed the municipal health re-port, as it has raised public interest in healthissues and the steps the city will take to bringabout health improvements. The populationis involved in this process where possible.
Citizens’ perception of health and well-beingHousehold surveysHousehold surveys were first piloted in lateautumn 2000 in three cities of comparablesize and structure – St Pölten, Villach andWels. The surveys were published in localnewspapers and were delivered to all house-holds. The mayors of the towns encouragedall citizens to participate.
The Network commissioned the Office forthe Organization of Applied Social Research(BOAS) to scientifically analyse the citizen sur-veys within the framework of municipal sta-tistics. Municipal-level experts discussed theresults of the household surveys, which had a10% response rate. This resulted in a new fo-cus on municipal health policies.
FindingsThe findings presented below and in Box 5.1are based on analysis of 5441 usable repliesfrom the three towns.
Box 5.1. Snapshot of findings fromhousehold surveys in St Pölten, Villachand Wels
• After the age of 50 years, only half thepopulation felt totally healthy.
• Up to the age of 50 years, women sufferfrom impaired health more than men.
• After age 50 years, men’s and women’shealth did not differ significantly.
• Higher levels of education correlated withbetter health after the age of 35 years.
• People with a university degree are healthierat age 60 years than people with only basiceducation at age 40 years.
• Hardly any young people describethemselves as happy – people older than 50years felt happiest.
Tel.: +43 1 5311476099Fax: +43 1 531149976175E-mail: [email protected]
AUSTRIA . 29
31497_National.p65 06-10-2003, 08:0429

30 . NATIONAL HEALTHY CITIES NETWORKS
BelgiumCountry factsFrench-speaking population:4.1 millionTotal population:10.3 millionLiving in network cities(of the French-speakingcommunity): 57%
Network factsEstablished: 1 January 2002Members: six (one region, one province,four cities)Organization: non-statutorynetworkBackground
BackgroundThe constitution recognizes three cultural com-munities: French-, Flemish- and German-speaking.These communities are responsible for many ar-eas: culture, support for young children andhealth promotion. The constitution also recog-nizes three separate regions that are essentially re-sponsible for economic development but alsomanage some aspects of health care.
Within this structure of government, it has notbeen ideal to form one national healthy cities net-work, as cities within each language communityhave a different set of partners and a uniquepolicy context. The healthy cities movement inBelgium has to be part of a government structure,and it chose to align itself to decentralized federallevels that are closer to the citizens. Two separateregional healthy cities networks were therefore es-tablished in 1992 – the Belgian Flemish-speakingHealthy Cities Network (Box 5.2) and the BelgianFrench-speaking Healthy Cities Network (de-scribed below). Belgium is unique in this respect.
Promoting health for allThe main goal of the Belgian French-speakingHealthy Cities Network is to promote the WHOhealth for all strategy and its targets as widely aspossible. The Network encourages its members todevelop core products of the WHO EuropeanHealthy Cities Project, including the city healthprofile and the city health development plan. Italso shares the important principle of thinking
globally and acting locally. The Network organizesjoint activities for World Health Day, World No-Tobacco Day and World AIDS Day and has initi-ated a series of round-table meetings on healthand the environment, attracting about 600 par-ticipants to each event.
Support and exchangeThe Network’s Coordination Centre is based inLiège Province Santé (Liège Healthy Province),which offers administrative support and facilitatesthe exchange of information. The CoordinationCentre acts as a contact relay, supplying WHO in-formation and guidelines to members. As a mem-ber of the WHO European Healthy Cities Net-work, Liège Province Santé supports cities in theBelgian French-speaking Healthy Cities Networkin developing healthy city infrastructures and inimplementing the approach. Training on how toestablish a healthy city project and healthy citiesnetwork took place in May 2003.
International partnershipsThe Network has established close links with theFrench Healthy Cities Network and takes part insome important joint activities. For example, Bel-gian member cities participate in an internationalFrench-speaking Healthy Cities network.
For more information on the Belgian French-speaking Healthy Cities Network, contact:Jacqueline TrinonNational Network and Healthy City CoordinatorMaison de la Qualité de la VieSecteur Provincial de Promotion de la SantéBoulevard de la Constitution 19B-4020 Liège, BelgiumTel.: +32 4 3495133, Fax: +32 4 3495135E-mail: [email protected]
Box 5.2. The Flemish-speaking HealthyCities NetworkWhen the City of Mechelen was designated tothe first phase of the WHO European HealthyCities Network in 1991, it led the developmentof a network in Flanders. Six cities cametogether to form a Flemish-speaking networkand worked actively in health promotion. Thisresulted in the establishment of local healthplatforms that covered the entire region ofFlanders. In the absence of a city linked to theWHO European Network, and in the wake ofpolitical changes, the Flemish-speakingNetwork is inactive. It is hoped that it will berelaunched in 2004.
31497_National.p65 06-10-2003, 08:0430
After working intensely to promote the WHOstrategy for health for all at the local level, wehave really been able to measure the addedvalue of the recommendations of the WHOEuropean Healthy Cities project. This is thereason why, as a member of the WHO EuropeanNetwork of Healthy Cities and as the Presidentof the Belgian French-speaking Healthy CitiesNetwork, we are ready to address thedifficulties inherent in our country’s structuresto persuade many cities, provinces, regionsand other local powers to rally the movement.We are sure that this will be the best solutionto improve the health of each citizen and theentire population. I am convinced that workingin a network and sharing information,procedures, successes and mistakes is themain way to make progress in the field ofhealth and environment today and tomorrow.
Georges PireMember of Provincial GovernmentProvince of LiègePresident, Belgian French-speaking HealthyCities Network
I have long-established contacts with LiègeProvince Santé.
Through these, I have had the opportunity toappreciate the value of the health for allstrategy in the 21st century. The holistic senseof health (of which environment is a great part)constitutes a considerable value.
The Belgian French-speaking Healthy CitiesNetwork is a very interesting tool for bringingabout a new way of thinking and acting forpromoting health and a sustainableenvironment.
I am ready to support the Network in thefuture.
Michel ForetMinister of Environment and DevelopmentPlanningWalloon RegionBelgium
Spotlight on the Belgian French-speakingHealthy Cities Network
shows. The young people were introduced tothe goals and significance of WHO’s healthfor all strategy and Healthy Cities project. Af-terwards, participants joined round-tablemeetings with experts and politicians to dis-cuss health and the environment.
The event also proved that a healthy life-style need not be boring. In the evening, par-ticipants danced to the reggae music of a bandcomprising eight people 17-22 years old fromdifferent cultures.
The event provided a pleasant and relaxedatmosphere to raise awareness of health, toshare the goals and experience of the healthycities movement and to give the 250 youngpeople a wonderful day on which to lookback.
Raising awareness among tomorrow’sdecision-makersThe Network brought together 250 youngpeople from member cities on a boat trip fromHuy to Liège on the river Meuse. The objec-tive was to raise awareness of health and toengage the decision-makers of today and oftomorrow in dialogue. Politicians and expertson health and environmental issues partici-pated in this event, which received wide cov-erage from local radio stations and other massmedia.
Georges Pire, President of the Networkand a member of the Provincial Governmentof Liège, welcomed participants. A full pro-gramme of activities was organized on theboat to raise awareness of health issuesthrough theatre, film, exhibitions, video and
BELGIUM . 31
31497_National.p65 06-10-2003, 08:0431

32 . NATIONAL HEALTHY CITIES NETWORKS
Bosnia and HerzegovinaCountry factsPopulation: 4.1 millionUrban population: 43%
Network factsEstablished: 2001Members: 13Organization: nonstatutory network
The healthy cities movement in Bosnia andHerzegovina was initiated by the InternationalCommittee of the Red Cross (ICRC) in partnershipwith local governments, the Ministries of Healthof both entities of Bosnia and Herzegovina, WHOand nongovernmental organizations in 1998. Anumber of members of the WHO EuropeanHealthy Cities Network and national networkshave supported the development of healthy citiesin Bosnia and Herzegovina. In 2001, 13 citiesacross the country founded the Bosnia andHerzegovina Healthy Cities Network. Mayors ofthese cities launched the Network by signing astatement that reflected a common understandingof the necessity to advocate cooperation betweencities and communities on issues that transcendpolitical boundaries. The Network has adoptedstatutes and is now seeking to establish itself as alegal organization. The overall objectives of thenetwork are to sustain voluntary self-help advo-cacy, to involve more cities and to develop part-nerships at all levels. The Network still has manyobstacles to overcome, but it has learned how tobring about change (Box 5.3).
Healthy cities – a courier of peace andchangeThe ICRC recognized that building communityself-reliance for health was vital in a countrywhere government funds for health services arelikely to be limited for the foreseeable future.Healthy cities offered a transparent, bottom-upapproach built on mutual cooperation and trustand a process for taking action where the greatestneeds are – in communities. The Healthy Citiesproject in Bosnia and Herzegovina has providedan excellent example of how to involve local ac-tors in defining needs and priorities and in de-signing and implementing projects. The projecthas promoted fundamental values for building
civil society and has supported the process of de-mocratization. It has helped communities and lo-cal governments to work in partnership to definea clear vision for the future, set priorities and in-crease competence in planning and implementingprojects. At the same time, the healthy citiesmovement complements and supports the coun-try’s strategy for public health.
Towards democracyA key issue of concern for the Network is develop-ing the concept of democracy among young peo-ple. As young people are growing up in segregatedsocieties, the Network fears that young people willlearn to mistrust one another. In response to thisconcern, the Network is now developing a schooldemocracy project in partnership with the Norwe-gian Healthy Cities Network and Croatian HealthyCities Network. The democracy project was con-ceived by Sandnes (Norway), a member of theWHO European Healthy Cities Network, in 1996. Itinvolves setting up model parliaments in primaryand secondary schools, with the aim of bringingabout change in society by educating youth indemocratic processes. Student assemblies discussand propose solutions to health-related problemssuch as the availability of drugs, playground safetyor how to support children with special needs.
For more information, contact:Suada TukaTechnical Secretary, National NetworkAdema Buca 20, 88000 MostarBosnia and HerzegovinaTel.: +387 63 314970, Fax: +387 36 853929E-mail: [email protected]
Box 5.3. Lessons learned implementingthe healthy cities approach• Forget the status quo and go for innovation.• Find people who can motivate others.• Plan the process, but involve communities as
early as possible.• Test ideas with pilot groups.• Learn from your experience and expand to
the city and national levels.• Do not expect the process to be smooth or
easy.• Realize that everything requires trial and error.
31497_National.p65 06-10-2003, 08:0432

Spotlight on Bosnia and HerzegovinaA network built on communitiesHealthy cities in Bosnia and Herzegovina is basedon a grassroots community project called HealthyCommunities. The ICRC’s primary health careteam launched this project in 1998. As the namesuggests, this work was first initiated in a numberof communities (geographical areas). Later, whenthe initiative spread to the city level, the termHealthy Cities project was adopted. Mayors, localgovernment heads, the Ministries of Health,nongovernmental organizations and institutes ofpublic health were partners of the project. TheICRC provided funding for three communityfacilitators to work in three pilot cities.
Getting supportCommunity facilitators presented the project to lo-cal people by going door-to-door and explainingthe project and using personal contacts and refer-rals to reach a critical mass of people. This processwas important for building trust and respect. Com-munity members were invited to a meeting wherethey were asked to participate more formally in acommunity health group. The meetings also pro-vided the opportunity for community members todiscuss local issues with mayors. Each communityhealth group comprised about 12-15 volunteers.
Building community self-reliance for healthOver a period of 1 year, training was provided forcommunity health group members, politicians andinstitutes of public health (Box 5.4). The CroatianHealthy Cities Network led some of the first train-ing sessions for Bosnia and Herzegovina HealthyCommunities. Community facilitators identifiedtraining needs for the community health groups inthe beginning of the project, and communityhealth groups began to identify their own trainingneeds after about 6 months. The early trainingworkshops were organized at the national level, asfew communities were involved in the project atthat point. Through these events, communitymembers of different ethnic origin came to see thatthey faced similar problems and saw that theycould work together to find common solutions. Forthe participants in these sessions, this representedsome of the first steps towards down a difficult pathtowards ethnic reconciliation.
Assessing community needsCommunity health groups assessed communityhealth needs through door-to-door surveys andgroup interviews. The most commonly identifiedhealth problems were discussed in a public work-shop. Priorities for action were set using criteriathat took into account cost and the percentage ofthe population that would benefit. Each commu-nity had seed money from the ICRC with whichto implement projects. Community task groupsled the implementation of the projects in partner-ship with local governments, municipal enter-prises and local contractors, who often helped toraise extra funds. Projects included health educa-tion, employment projects, building renovationand improvement of services such as water supplyand sewerage.
ConclusionThe Healthy Communities project in Bosnia andHerzegovina helped to introduce a new definitionof health based on a social model. The commu-nity health needs assessment was important formotivating people to participate, which helped toestablish links among community members anddevelop their skills in joint problem-solving.Transparent, accountable decision-making andcommunity leadership characterized this project,which was undertaken in partnership with localgovernments. In this way, Healthy Communitiesalso provided a positive experience of local de-mocracy.
We wholeheartedly support the principles of health and sustainable development through our commitment toWHO’s HEALTH21 policy and the Athens Declaration for Healthy Cities. We pledge our support to implementing ac-tions for health in our cities that will be based on partnerships with different city departments and sectors andwith the active involvement of our citizens ... . We will strive to ensure that our Network will have the necessaryresources for coordination, capacity building and technical support. We are eager to cooperate with cities andnetworks of the European healthy cities movement in a spirit of solidarity, mutual respect and shared vision towork for the health and the well-being of our people.
Excerpt of the Founding Statement of the Bosnia and Herzegovina Healthy Cities Network signed by 13 mayors
Box 5.4.Training topics for building capacityfor community self-management• Introduction to health• Communication and group work• Advocacy and lobbying• Participatory assessment of health needs• Project planning• Fundraising• Evaluation and monitoring• Training the trainers
BOSNIA AND HERZEGOVINA . 33
31497_National.p65 06-10-2003, 08:0433

34 . NATIONAL HEALTHY CITIES NETWORKS
CroatiaCountry factsPopulation: 4.3 millionUrban population: 57%Living in national network cities: 40%
Network factsAccredited: 2000Established: 1992Members: 22 (full) and 28 (associated)Organization: nongovernmental organizationWeb site:http://zdravi-gradovi.com.hr/eng/index.htm
The most important issues for the CroatianHealthy Cities Network stem from the direct con-sequences of war and economic transition on hu-man health (Box 5.5). Healthy cities has provideda testing ground for applying new strategies andmethods for addressing these issues in Croatia.The Network supports cities through educationand training, information dissemination and part-nership building. While full members of the Net-work must meet a set of criteria consistent withthe WHO action framework for European nationalhealthy cities networks (Annexes 2, 3), allCroatian cities have equal assess to the Network’sresources and events. The Network also supportscities in neighbouring countries.
and public health experts, as it legitimated theiraccess to the key players in the city, includingpoliticians, administrators, professionals, institu-tions, citizen representatives and nongovernmen-tal organizations. Dialogue was opened amongdifferent interest groups through involvement in acommunity health needs assessment, which re-sulted in joint action plans based on intersectoralalliances (rapid health needs assessment). Thisrepresented the first time since the war that com-munities were able to see themselves as capable ofidentifying and solving health problems.
Motovun Summer School of HealthPromotionAn important event for spreading healthy citiespractice is the Motovun Summer School of HealthPromotion. The Summer School is organized bythe Andrija Stampar School of Public Health,which is also the base for coordinating the Net-work. The aim of this initiative is to establish ameeting-point for people working in health pro-motion locally, regionally, nationally and interna-tionally. The Summer School links the academiccommunity and centres of excellence with localpractitioners, enabling an exchange of knowledge,skills and experience. This 2-week event includesconferences and workshops specifically for profes-sionals involved in the healthy cities movement.A number of courses are run in English for inter-national participants.
The 10th Summer School in Motovun was heldin 2003. Over the past 10 years, thousands haveparticipated in the Summer School – about 250people per year from 22 European countries andthe United States.
EvaluationDuring 2001, the Network began developing anevaluation tool to assist member cities in assessingtheir achievements. Two groups were establishedwith the following objectives:• to reach a national consensus on a set of indica-
tors for all cities to monitor and evaluate proc-esses and outcomes annually; and
• to develop a more comprehensive instrumentto be used for a 5-year project evaluation to beused by cities that have undertaken a rapidhealth needs assessment and produced cityhealth profiles and plans.
National network cities worked in groups to de-velop indicators based on those used by the WHOEuropean Healthy Cities Network. The groups alsodeveloped a number of additional process indica-
Box 5.5. Health challenges in Croatia• Mental health, including posttraumatic
disorders• Family health• Community empowerment• Unemployment, especially among young and
mid-career workers• Unmet needs of vulnerable groups• Rebuilding human settlements and
infrastructure• Alcohol, tobacco and substance abuse
Renewing public healthThe second phase of the WHO European HealthyCities project (1993–1997) had important effectson the healthy cities movement in Croatia. Thisphase promoted a process for developing and im-plementing strategic city health documents (cityhealth profiles and city health plans) – integratingthe issues of health, community participation anddevelopment. This helped project coordinators
31497_National.p65 06-10-2003, 08:0434
tors. Coordinators of all members of the CroatianHealthy Cities Network then consultedstakeholders in their respective cities, and a re-vised set of indicators for the Network wasadopted in 2003. Cities will use these annually.Public health experts developed the 5-year evalua-tion instrument and piloted it in Rijeka in 2003.As a result, the Network has adopted this methodfor monitoring project achievements, comparingresults between cities and reporting on results.
For more information, contact:Selma SogoricNational Network CoordinatorCroatian Healthy Cities NetworkAndrija Stampar School of Public HealthMedical SchoolUniversity of ZagrebRockefellerova 4, 10000 ZagrebCroatiaTel.: +385 1 4590100, Fax: +385 1 4684213E-mail: [email protected]
Spotlight on CroatiaHealth – Plan for It: a training programmefor countiesBackgroundExperts at the Andrija Stampar School of PublicHealth, supported by colleagues from the UnitedStates Centers for Disease Control and Prevention,developed a training programme for counties. It in-troduced the Healthy City philosophy and practiceto the county level. Health – Plan for It providesguidance to counties as they develop a county healthprofile and a county plan for health (Box 5.6).
Stakeholders and participantsCounty councils and governors were particularly ea-ger to learn how to effectively manage scarce re-sources. The Network was pleased to have an oppor-tunity to influence health decision-making at thecounty level through participation in county trainingteams. The Ministry of Health and the Ministry ofLabor and Social Welfare expressed support and paidthe trainers, making the course free of charge for theparticipants.
Between March 2002 and May 2003, three groupsof counties completed 4 months of intensive train-ing. This included 9 of Croatia’s 20 counties. Eachcounty team was composed of at least nine peopleincluding political, technical and community repre-sentatives. Healthy city coordinators were includedin technical or community parts of the team – de-pending on the formal structure of the local healthycity project.
A process of learning by doingThe programme consisted of four modules that ena-bled county health plans to be developed based ona step-by-step approach.
1. County teams learned how to carry out a partici-patory assessment of health needs and how todesign a county health profile.
2. The teams were introduced to decision-makingtechniques to set five priorities reflecting com-munity health needs (Box 5.7). They identifiedhealth stakeholders and consulted them on thesepriorities.
3. County teams were guided through the healthplanning process. In a second round of consulta-tions, county expert panels advised the countyteams on feasible policies and programmes.
4. County teams worked on a draft version of acounty health plan, which included monitoringand quality assurance mechanisms and evalua-tion plans.
Three months following this training, county teamspresented their county health profiles and plans totheir respective county councils. The county coun-cils later accepted the plans.
ResultsMost of the counties’ priority areas (Box 5.7) over-lapped priorities identified by cities and reflectednational concerns. As a result, these priorities havebeen considered as a basis for formulating a na-tional health policy. The results from the trainingprogramme have been presented nationally as wellas to other counties. Anticipated benefits includeimproved financial resource management, betterdelivery of health and social care services and ashift away from a “one-size-fits-all” approach tohealth policy. The training programme is currentlybeing tested in The former Yugoslav Republic ofMacedonia.
Box 5.6. Health – Plan for ItA training course for counties covering:• Public health management – providing
appropriate, high-quality services• Organizational and human resource management• Collaboration and community participation
Box 5.7. Common health priorities incounties in Croatia• Unemployment• Quality of life among elderly people• Mental health• Alcoholism• Cardiovascular diseases• Malignant diseases• Allergies
CROATIA . 35
31497_National.p65 06-10-2003, 08:0435

36 . NATIONAL HEALTHY CITIES NETWORKS
Czech RepublicCountry factsPopulation: 10.3 millionUrban population: 75%Population living in network cities: 11%
Network factsAccredited: 2001Established: 1994Members: 31 cities and towns; 2 micro-regions;1 region; 1 nongovernmental organizationOrganization: associationWeb site: http://www.gate.cz
BackgroundHealthy city networking in the Czech Republicstarted in 1992 through the initiative of threetowns (Brno, Sumperk and Trebon) and the sup-port of the Czech Ministry of Health. In 1994,Healthy Cities of the Czech Republic was estab-lished as a legal association of 11 cities and towns.Full and associate membership is open to regions,towns, districts, municipalities and micro-regions(voluntary local associations of municipalities).Full members make a commitment to implementintegrated local strategies for health, sustainabledevelopment and the quality of life, based on:• WHO’s HEALTH21 policy• Agenda 21 of the United Nations• the national environment and health action
plan.
New Gate 21The network’s method for the local implementa-tion of international and national strategies forhealth and sustainable development is based onthe WHO Healthy Cities approach. New Gate 21was developed in 1998 through cooperation withthe network’s main partners – WHO, the UnitedNations Development Programme, ministries ofthe Czech Republic and Charles University inPrague. Its central features include:• collecting and disseminating information• developing guidelines, manuals and case studies• a dynamic web site, called eGate.
The New Gate 21 method was selected as a world-wide project for EXPO 2000 in Hanover, Germanyand was made part of the Czech Exposition. Since2002, the network has been working with the
Ministry of Environment to develop a nationalmethod for the implementation of Local Agenda21.
Supporting citiesA major objective of the network is to support lo-cal authorities in implementing local health forall and Agenda 21 strategies. As of May 2003, 17members had produced city health developmentplans – a key priority for members of the WHOEuropean Healthy Cities Network in its thirdphase (1998–2002). The network’s particular areaof strength has been its ability to support cities ininvolving citizens in the city health developmentplans. The network has also facilitated systematiccooperation with national ministries, WHO andother expert partners.
Exchanging and promoting new ideasThe network’s Internet-based information systemis called eGate. The eGate web site provides clearlyarranged and continuously updated informationon a wide range of areas. The web site aims to as-sist professionals in public administration, localpoliticians, nongovernmental organizations,schools and businesses. eGate offers 11 e-mailconferences on specialized topics – health, Agenda21 and the environment being the most popular.The conferences are accessed via an automated,online registration system and have no time limit.Between 150 and 200 people from all over theCzech Republic participate in each conference.The site is freely accessible to everyone, and someinformation is available in English.
Mass media coverageThe network receives nationwide mass media cov-erage. Since 2001, Czech Radio 2 has been broad-casting monthly 1-hour programmes on healthycities, featuring the achievements of the network,individual cities and the viewpoints of ministries,expert partners and academics. The network hasalso been presented several times on national tel-evision. Further, specialized journals for munici-palities regularly feature articles on healthy cities.
31497_National.p65 06-10-2003, 08:0436
Future goalsThe network is actively working to fulfil WHO’shealth for all target calling for at least 50% of cit-ies, urban areas and communities to become ac-tive members of a healthy city or healthy commu-nity network by 2015.
For more information, please contact:Petr SvecNational Network CoordinatorHealthy Cities of the Czech Republic (HCCZ)Srobarova 48CZ-100 42 Prague 10Czech RepublicTel.: +420 602 500639E-mail: [email protected]
Spotlight on the Czech RepublicKromeriz – a safe communityInjuries are the leading cause of death among chil-dren and young people in the Czech Republic. In-jury prevention is therefore a priority for the net-work and its partners. Kromeriz began its work as asafe community early in 2000. The city hadstepped forward when the Prague Centre for Epide-miology and Injury Prevention expressed an inter-est in cooperating with a network member thatwould be ready to act as a model city in WHO’sSafe Communities network.
A city becomes a safe community by meeting aset of criteria (Box 5.8) that demonstrate that a cityhas the structures, partnerships and programmes inplace that will enable it to become safe. Commu-nity involvement is an important element of theapproach.
Kromeriz, a member of Healthy Cities of theCzech Republic since 1996, agreed to apply for des-ignation. A city council resolution provided thepolitical commitment for participation in SafeCommunities. The Safe Communities criteria wereconsidered consistent with the healthy cities ap-proach and the city’s local priorities on injury pre-vention.
By virtue of meeting the criteria of the nationalhealthy cities network, Kromeriz was immediatelyable to satisfy many of the Safe Communities crite-ria. For example, Kromeriz already had anintersectoral steering group, broad partnerships forhealth and experience developing strategic, healthfor all-based policies and plans, all of which are anintegral part of the city health development plan.
In 2003, Kromeriz is expected become the firstCzech city to be designated to the WHO Safe Com-munities Network. A full description of how it meetsthe Safe Communities criteria is available at http://www.phs.ki.se/csp/safecom/kromeriz.htm (accessed15 September 2003).
Box 5.8. Indicators for International SafeCommunitiesSafe Communities have:1. an infrastructure based on partnership and col-
laborations, governed by a cross-sectional groupthat is responsible for safety promotion in theircommunity;
2. long-term, sustainable programs covering bothgenders and all ages, environments, and situa-tions;
3. programs that target high-risk groups and envi-ronments, and programs that promote safety forvulnerable groups;
4. programs that document the frequency andcauses of injuries;
5. evaluation measures to assess their programs,processes and the effects of change; and
6. ongoing participation in national and interna-tional Safe Communities networks.
Source: WHO Collaborating Centre on CommunitySafety Promotion, Karolinska Institute (http://www.phs.ki.se/csp/indicators.htm, accessed 15 Sep-tember 2003).
The manuals for establishing and developing a healthy city have been tried and tested to such an extent thatthe new members can start realizing their vision of a healthy city right away.Ladislav Ambrozek, Deputy Mayor of Hodonin, Chair, Healthy Cities of the Czech Republic
I see the project as a space where politicians and the city authorities’ staff meet with the people who want toactively work for their city. The project can have a magical effect – it can turn many passive clients into activepartners.Marie Cerna, Deputy Chair, Vysocina Region
Owing to mutual contacts within both national and European healthy cities networks, we can draw upon theexperience of others and not reinvent the wheel where others have already tested a particular solution inpractice.Rostislav Slavotinek, First Deputy Mayor and Councillor, Brno
CZECH REPUBLIC . 37
31497_National.p65 06-10-2003, 08:0437

38 . NATIONAL HEALTHY CITIES NETWORKS
DenmarkCountry factsPopulation: 5.3 millionUrban population: 85%Population living in network cities: 52%
Network factsAccredited: 2000Established: 1991Members: 15Organization: politically binding networkWeb site: http://www.sund-by-net.dk
BackgroundThe Danish Healthy Cities Network was estab-lished in 1991 with the aim of developing meth-ods and materials in health promotion and dis-ease prevention and anchoring this work locally.In practice, this means that Network memberstake part in both developing and putting Networkmethods into day-to-day practice, serving as mod-els for all counties and municipalities. Member-ship fees finance the costs of the Network. TheMinistry of the Interior and Health financiallysupports the Network’s project work.
Meeting high standardsCities and counties join the Network by passing acouncil resolution binding them to the Network’saccession document. These criteria include theminimum criteria set out in the WHO actionframework for European national healthy citiesnetworks (Annexes 2, 3), the government policyon public health and the principles, objectivesand targets of HEALTH21 and the Ottawa Charterfor Health Promotion. This political commitment
to a set of quality standards is an important sourceof strength for the Network.
Three areas of expertiseThe Network’s three priority themes are health atthe workplace, accident prevention and diet andphysical activity. Every member is required tocarry out joint work on one theme and to partici-pate in the corresponding work group. TheNational Board of Health and the National Insti-tute of Public Health provide technical support tothe work groups. The Network crystallizes the lo-cal experience and expertise gained in these areasby producing and testing materials and manuals(Box 5.9). These manuals are disseminated nation-ally.
National influenceThe expertise of the network has become a na-tional resource. For example, a National Centrefor Health Promotion at the Workplace has beenestablished through the collaboration of the Cityof Copenhagen and Sønderjylland County, withthe support of the Ministry of the Interior andHealth. The Centre disseminates the knowledgedeveloped by the Network to the counties and tooccupational health services. It also organizescourses, conferences and meetings and providessupport for local interventions.
The Network’s added valueThree external evaluations of the Network havedemonstrated that both politicians and coordina-tors find that Network membership provides sig-nificant added value (Box 5.10). Access to train-ing, guidance materials and exchange has madeinnovating, planning and testing new ideas easierfor cities and counties. Learning has taken placethrough summer schools, courses, conferencesand work groups organized by the Network. Thecommitment to developing local health strategiesand plans has resulted in increased political inter-est and investment in health, with a special focuson community participation. As a result of theNetwork’s focus on accident prevention, fourmember cities have been designated to the WHOSafe Communities network.
Cities and counties have stated that their mem-bership of the Danish Healthy Cities Network hasput them at the forefront of health developmentin the Network’s priority areas. However, theadded value of the Danish Network extends be-yond what it gives to its members. The Networkhas made Danish and European expertise avail-able to all municipalities and counties in Den-
Box 5.9. Handbooks and manualsavailable (in Danish)• Falls in the nursing home• Falls in the hospital• Falls in the home• Good ideas on how to make a health profile of
a workplace• Good advice for health planning• A good trick (manual and video for staff in can-
teens)• The Danish Healthy Cities Network toolbox• Preventing accidents among children 0–6 years• Preventing accidents in school and recreation
facilities (children 6–15 years)
31497_National.p65 06-10-2003, 08:0438
FutureIn 2001, politicians expressed a number of objec-tives for the future of the Network (see Spotlighton Denmark):• The work should continue to be made more
professional by making health promotion partof the daily work and part of policy.
• International contacts and activity should bestrengthened.
• A comprehensive Network database should bedeveloped to document health promotion ac-tivities.
• Membership should be increased.The Network is now working to fulfil these aspira-tions. The Network has contacted political leadersacross Denmark with the aim of attracting newmembers, and it is actively involved in the Net-work of European National Healthy Cities Net-works. The Network is also developing a NordicHealth and Environment Profile in partnershipwith the Norwegian and Swedish healthy citiesnetworks. By documenting the impact of healthpromotion activities, the Network hopes to facili-tate increased investment in health promotion atthe local level.
Denmark’s Network has great significance for specific initiatives around the country. Valuable experiences arebeing incorporated and useful knowledge is being compiled about how best to tackle the issues. It is excitingthat this is happening within a network, horizontally and with minimal bureaucracy.Lars Løkke RasmussenMinister for the Interior and Health(See Box 3.2 for the full text of the statement)
Spotlight on DenmarkPoliticians affirm the value of the DanishHealthy Cities NetworkOn 26 February 2001, the Danish Healthy CitiesNetwork celebrated its tenth anniversary at Co-penhagen City Hall. Politicians, leading officials,Network coordinators, national partners (includ-ing the National Board of Health, Ministry ofHealth and the National Institute of PublicHealth) and representatives of WHO and otherNordic and Danish networks participated.On the occasion of this event, the Network pub-lished a book featuring interviews with politi-cians from each member county and municipal-ity and the Minister for Health at the time, ArneRolighed. Each responded to the following ques-tions.
• Has the Danish Healthy Cities Networkbrought added value to the local level?• What is expected of the Danish Healthy Cit-ies Network in the future?Politicians generally agreed that membership ofthe Network had helped to increase local aware-ness of the importance of health promotion anddisease prevention. The rich and high-qualityexchange through the Network has made it pos-sible for cities and counties to move forward to-gether rather than continuously reinventing thewheel. The event and the publication helped tostrengthen political support for the Network aswell as the focus on health in cities and coun-ties.The Ministry of Health financed the publicationand the event.
Box 5.10. The added value of the DanishHealthy Cities Network according to themembers• Greater political commitment for health promo-
tion and disease prevention• Support for the development of local health pro-
files and plans• Increased capacity to involve citizens• One-stop access to information on local and na-
tional initiatives, best practices and exchange• Opportunities to influence national-level policy• Increased access to resources through participa-
tion in large developmental projects• Professional training and development
Source: Denmark’s network of healthy cities. Annualreport 2000. Copenhagen, National Institute ofPublic Health, 2001 (http://www.si-folkesundhed.dk/udgivelser/web/sundby-beret2000uk.htm, accessed 22 August 2003).
mark by disseminating guidelines and translatingWHO information and publications and throughits web site.
DENMARK . 39
31497_National.p65 06-10-2003, 08:0439
40 . NATIONAL HEALTHY CITIES NETWORKS
EstoniaCountry factsPopulation: 1.4 millionUrban population: 68%Living in national network cities: 20%
Network factsEstonian Healthy Cities NetworkEstablished: 2002Members: 15Organization: not-for-profit associationWeb site: http://www.kuressaare.ee/tervis
BackgroundThe city of Kuressaare hosted a conference in 1999to introduce the idea of setting up a healthy citiesnetwork in Estonia. The value of networking be-came clear over the following 3 years, as localpoliticians, professionals and the public gained ac-cess to new ideas and the confidence to put theminto action. The Estonian Healthy Cities Networkwas legally established as a not-for-profit associa-tion of local authorities in 2002. The Network’smain goal is to improve the status of public healthand the environment in Estonia’s cities and townsthrough approaches based on health for all andAgenda 21. Today, political leaders in one third ofEstonia’s towns have acknowledged that local au-thorities have both the potential and a responsi-bility to promote health by making a formal com-mitment to the Network.
Broadening the health agendaDuring Estonia’s transitional period, health fellinto the background as emphasis was placed onbuilding economic and physical infrastructure.Little attention was paid to how these sectors af-fect health and well-being. Today, as new evidenceon the determinants of health emerges, the tide ischanging. A major objective of the Network is topromote broad understanding of the determinantsof health, including living and working condi-tions, social and community influences, indi-vidual lifestyle factors and the quality of the envi-ronment.
Getting on the right trackCities and towns are concerned about whetherthey are perceived as being healthy places to liveand work. Towns with large-scale industrial facili-
ties and a poor physical environment are usuallyperceived as less healthy. The Network has beenespecially important for these towns, as it offersthem a framework for ultimately improving theliving conditions and well-being of citizens. Thisframework is based on the proven methods, toolsand recommendations developed by the WHO Eu-ropean Healthy Cities project over the past 15years. Estonia’s towns can now make use of thisinternational experience without reinventing thewheel.
Building capacity through exchangeAs the Network is young, considerable energy hasbeen devoted to raising the capacity of city coor-dinators to work with healthy cities approachesthrough conferences, seminars and workshops.This training has also focused on building skills tocommunicate health messages via the mass me-dia. Kuressaare and Pärnu, members of the WHOEuropean Healthy Cities Network, have played animportant role in sharing their experiences andproviding leadership.
Documenting changeFollowing the key steps of the healthy cities ap-proach, the Network’s top priority is to lay thefoundation for systematic and comprehensivehealth data collection and analysis by producingcity health profiles. Estonia’s towns have not pre-viously produced extensive profiles, and data fromdifferent sectors have been collected in isolation.Achieving an overview of the pattern of changesin cities and towns has therefore been difficult.The city health profiles will make visible how vari-ous sectors influence health outcomes and will en-able cities to set targets and measure changes.
31497_National.p65 06-10-2003, 08:0440
Looking forwardThe next phase of the Network’s development willemphasize strengthening the Network’s structuresand programmes. Although attracting new townsto the healthy cities movement will be vital, en-suring high standards of activities and producingresults that are clear and visible to citizens andpoliticians will be essential. As political commit-ment underpins the Network, a special effort willbe made to ensure that healthy cities conceptsand principles are brought to new leaders follow-ing local elections. In 5 years, the Network expectsthat decision-makers and the population will be
familiar with the healthy cities movement. TheNetwork will aim to encourage people to activelyparticipate in promoting and sustaining theirhealth and well-being.
For more information, contact:Ingrid TiltsCoordinatorKuressaare Town GovernmentTallinna 10EE-93813 KuressaareEstoniaE-mail: [email protected]
Spotlight on Estonia
Being part of an initiative launched by WHO provides [Estonia’s cities] with confidence and the reliabil-ity of moving in line with developments in Europe.
Jaanus Tamkivi, Mayor, KuressaareChair, Board of the Association of Estonian Cities
A political debate on healthIn April 2002, the Estonian Healthy CitiesNetwork and its partners organized a politicaldebate. The debate, the first of its kind in Es-tonia, brought together representatives of sixof the eight major political parties to discusshow political decision-making had positivelyor negatively influenced health trends in re-cent years.
Remarkably, the debate concluded thatthe decisions with the most destructive im-pact on health were those not made. The par-ticipants generally agreed that the key to thepublic’s health lay outside the health care sys-tem. The group recognized that high unem-ployment combined with low social benefitshad led to the critical problem of alcoholism.Alcohol-related mortality rates are more thanthree times the average for men in the Euro-pean Union and about twice the average forwomen. Following further debate on measuresfor reducing alcohol consumption, three keypolicy directions emerged.
These included the need for:• legal restrictions on the sale, advertise-
ment and accessibility of alcohol toyouth;
• measures to counteract the illegal trade inalcohol;
• social improvements such as increasingemployment opportunities, social benefitsand social activities for youths; and
• education to bring about behaviouralchanges.Representatives of the political parties rec-
ognized that national legislation was notbased on promoting health and that few re-sources had been allocated to preventive ac-tivities. On a positive note, it was stated thatthe National Health Protection Inspectorate’ssystem was well structured. The health insur-ance fund had laid a solid base for financingthe public health system and public healthprojects. The healthy cities movement wasidentified as an important mechanism forsupporting cities and towns in promotinghealth.
Although the debate focused more onproblems than solutions, the political partiesvoiced consensus for the need to raise healthhigher on the national agenda. It was agreedthat integrated policies based on a long-termvision for health should be developed. Widemass media coverage of the event brought theissues to the wider public.
ESTONIA . 41
31497_National.p65 06-10-2003, 08:0441

42 . NATIONAL HEALTHY CITIES NETWORKS
FinlandCountry factsPopulation: 5.2 millionUrban population: 60%Population living in network cities: 29%
Network factsAccredited: 2000Established: 1996Members: 14 (including 29 municipalities and 2 counties)Organization: networkWeb site: http://www.stakes.fi/hyvinvointi/ted/TKverkosto/index.html
Welfare and Health) coordinates the Network, andrepresentatives of the Ministry of Health and So-cial Affairs participate in the Network’s manage-ment board. Similarly, representatives of the Net-work have been appointed to the Ministry’s Na-tional Public Health Committee and its subcom-mittees. This cooperation has opened an impor-tant channel of communication between the na-tional and local levels.
A testing ground for new ideasThe Network’s 3-year action plan is concernedwith devising and testing methods for health pro-motion on a national scale. For example, the Net-work supports the local implementation of thegovernment resolution on the Health 2015 publichealth programme by providing training andmodels. With the support of STAKES, Network cit-ies have also initiated pilot projects on health im-pact assessment. The pilot projects are being car-ried out, together with local polytechnics, to de-velop training programmes to strengthen local ex-pertise in health impact assessment.
Welfare in schoolsThe Network provides a forum for comparativelearning between schools and for evaluatingmechanisms to support well-being in school com-munities. The Network’s ongoing Welfare inSchools project develops tools and methods formapping, describing and dealing with well-beingissues. Over the long term, the aim is tostrengthen the structures and the strategic think-ing on promoting well-being in schools. Webpages on each member municipality are being de-veloped as a resource to municipalities outside theNetwork.
BackgroundSeven municipalities established the FinnishHealthy Cities Network in 1996. These munici-palities came together as part of a project thatsupported the local implementation of Finland’shealth for all 2000 policy. Although the projecthad produced interesting results, it had left manyquestions unresolved. It was still unclear as tohow to promote and share responsibilities forhealth across sectors. The Network was launchedto provide cities with an arena to exchange expe-rience and to develop new public policy ap-proaches. This coincided with a period in whichhealth promotion and disease prevention were in-creasingly viewed as being essential to health be-cause economic recession had demonstrated theinadequacy of the resources devoted to healthcare.
Membership and criteriaMembers of the Network must meet a set of crite-ria consistent with the standards set by the WHOaction framework for European national healthycities networks (Annex 3). Membership is fixed for4 years. At the end of this period, an assessment ismade as to the whether the municipality stillmeets the membership criteria. The membershipterm also gives cities an opportunity to opt out ofthe Network. This approach has helped to ensurethat cities remain active and allows the Networkto be assessed from both sides at fixed intervals.
Healthy cities at the heart of developmentThe Network’s strong, national-level partnershipshas placed the healthy cities movement in Fin-land at the heart of development. STAKES (theNational Research and Development Agency for
31497_National.p65 06-10-2003, 08:0442
Peer evaluationCities in the Network work together on jointprojects and share their experiences at regularmeetings. Part of the process of learning isachieved through the peer evaluation. This takesthe form of assessment by municipalities of oneanother’s strategies for well-being. The advantageof this approach has been that municipalities gainfrom having their projects assessed by their peerswhile learning an effective method for self-assess-ment.
A vision of the Network’s futureThe Network is quite well known among Finland’smunicipalities. Interest in membership is growingfrom the support the Network can provide deci-sion-makers on local and regional health promo-tion work. In the future, the Network aims:• to facilitate a controlled expansion of its mem-
bership, with a focus on maintaining highstandards of participation;
• to complete its current projects with the aim ofsupporting national health policy;
• to build greater nationwide awareness of theNetwork;
• to create an arena in which local and nationalactors can meet and assess health policy devel-opment; and
• to establish greater visibility for the Networkthrough extensive international cooperation.
For more information, contact:Kerttu PerttiläDevelopment ManagerMunicipal Strategies for Health PromotionSTAKES (National Research and DevelopmentAgency for Welfare and Health)Lintulahden kuja 4, P.O. Box 220FIN-00531 HelsinkiFinlandTel.: +358 9 39672318Fax: +358 9 39672496E-mail: [email protected]
Spotlight on FinlandNeighbourhood houses – new premisesfor a healthy cityAs Helsinki moved towards a healthy citiesmodel of multisectoral cooperation, it en-countered difficulties in getting citizens in-volved in health promotion. As a response tothis problem, Helsinki set up a network ofneighbourhood houses around the city. Theseare neighbourhood living rooms, local meet-ing-places and action centres run by volun-teers. Many houses have a coordinator whogets a small salary.
Social inclusionHalf of Helsinki’s population lives in one-member households, and the cold climatelimits opportunities for getting to know otherpeople outdoors. People need an indoor meet-ing-place to share ideas and interests or get in-volved in the development of their neigh-bourhoods. The houses bring together enthu-siastic people of different ages and ethnicbackgrounds who take part in developing cul-tural, social and physical activities.
A healthy future for local youthAlmost all neighbourhood houses focus onproviding a healthy future for local youngpeople. Rising crime rates have opened a de-bate on the decline in moral and social values,and the solution is considered to be local andsocial, at least in part. Neighbourhood houseshave worked to develop relationships betweenyoung people and adults to pass on valuesand to reduce antisocial behaviour such asdrug use. Success depends on the ability to seeyouth as the great hope of our cities, ratherthan a threat, and to offer them a better fu-ture.
Future challengesNeighbourhood houses are one response totoday’s urban challenges. After 10 years, 30houses have been established and there is ademand for more. The houses offer an oppor-tunity to bridge what sometimes seems like asubstantial gap between the municipality andthe people and can make a real local differ-ence in the sense of community.
FINLAND . 43
31497_National.p65 06-10-2003, 08:0443

44 . NATIONAL HEALTHY CITIES NETWORKS
FranceCountry factsPopulation: 60.2 millionUrban population: 75%Living in national network cities: 9%
Network factsAccredited: 2003Established: 1987 (1990 as a legal association)Members: 45Organization: AssociationWeb site: http://www.villes-sante.com
The French Healthy Cities Network was establishedin 1987 with the involvement of eight cities. Fourof these cities took on the role of relay cities, whichinvolved leading the development of the healthycities in their respective regions. In 1990, the Net-work founded a legal association with 14 membercities. The main aims of the Network are to supportcities in implementing WHO’s policy for health forall locally and to facilitate exchange between cities.The Network has especially focused on reducing in-equality in health and on the social and environ-mental determinants of health.
A Network built on political commitmentA distinguishing feature of the Network is the di-rect leadership of politicians. Each city nominatestwo councillors to represent the city in the Net-work’s General Assembly. These politicians like-wise assume direct responsibility for healthy citieslocally. A 13-member steering committee, compris-ing only local politicians, provides the Network’sstrategic leadership. Cities and not individual peo-ple are elected to the steering committee.
Partnership with the Ministry of HealthThe Network signed a 3-year contract with theMinistry of Health in December 2002. Over thecoming years, the Network will work in partner-ship with Ministry representatives to develop localresponses to national public health priorities.Steering groups of cities will work in partnershipwith Ministry committees to take forward thethree themes of the project:• local implementation of national programmes
on cancer and on nutrition;• development of a health profile tool related to
the social determinants of health; and• communication.
The Network will serve as a testing ground for thedevelopment of new types of partnerships with lo-cal, regional and national organizations. The con-tract enables the Network to be seen as a legiti-mate, established partner at all levels. The Ministryof Health will provide financial support for thiswork through a system of decentralized funding.
Multi-level exchangeThe Network has sought to promote exchangethrough the creative use of online tools, publica-tions, twinning and regional networking. The Net-work has established a number of thematic workgroups in response to its work agreement with theMinistry (Box 5.11). Regional groups have beenestablished in Paris (Île de France), Rhône-Alpesand Nancy-Mulhouse to work on common prob-lems such as mental health, preventing drugabuse and the health of immigrants.
Box 5.11. Thematic work groups in theNetwork• Agenda 21• Cancer• Nutrition• Health profiles and indicators
International networkingThe Network has played a leading role in the es-tablishment of an international French-speakingnetwork involving countries from Europe, NorthAmerica and Africa. The French and Tunisian net-works and the French-speaking networks fromBelgium, Switzerland and Canada constitute theorganizational committee. To date, there havebeen six international symposia, each lasting 4days, with participants from three continents.Electronic exchangeThe Network has sought to overcome geographi-cal barriers to municipal exchange through thecreative use of online tools and publications. Cit-ies and towns use the Network’s web site to inter-act and stay informed. A web-based version of theNetwork’s directory allows cities to learn aboutone another through geographical or theme-basedsearches (see spotlight on France). The Networkalso produces a brief monthly bulletin calledINFODOC (information and documentation) thatprovides a wide range of online resources, docu-ments and publications from France and WHO,conference details, Network news and a calendar.An interesting feature of INFODOC is questionsfrom city to city. This enables cities to raise issues
31497_National.p65 06-10-2003, 08:0444

and get answers to questions such as “What is thestatus of your action against AIDS?”.
Next stepsThe work agreement with the Ministry of Healthwill guide the priorities of the Network over thenext 3 years. With the increased visibility and le-gitimacy gained through this partnership, the Net-work hopes to attract a large number of new cities.In addition, the Network aims to support cities tostrengthen local action on health and Agenda 21.At the same time, the Network will seek to buildnew partnerships with national-level organiza-
tions to raise awareness of the role of health inthis domain.
For more information, contact:Valérie Lévy-JurinPresidentRéseau Français des Villes-Santé de l’OMSHotel de VillePlace Stanislas, F-54035 Nancy cedexFranceTel.: +33 (0)3 86850338, Fax: +33 (0)3 83390351E-mail: [email protected]
The national government recognizes the legitimacy of local authorities becoming involved in health and how thishas become a reality for many cities, especially those in the French Healthy Cities Network. Although municipali-ties have little legal responsibility for providing curative health care, they can make a considerable contributionto improving health in their cities, especially by ensuring access to health care and disease prevention initiativesfor vulnerable people and by conducting campaigns to reduce avoidable premature death. In addition, the volun-tary endorsement by local authorities of the principles underlying the WHO European Healthy Cities Networkdemonstrates their interest in participatory approaches based on partnership, in which is considered both ameans and an ultimate objective of social development at the local level. In this way, municipalities can help toreduce social and geographical inequality in health and, even more so, the causes of a possible widening of thisinequality, in a setting of local democracy.Excerpt from the preamble to the Agreement between the Ministry of Health and the French Healthy Cities Net-work, 11 December 2002Bernard BassetDeputy Director for HealthMinistry of Health
In 1989, Nancy was designated as a “healthy city” by WHO. The continuation of Nancy Healthy City [in the WHOEuropean Healthy Cities Network] has not occurred by accident. It underlines the active commitment of the mu-nicipality to develop local public health policies and a partnership in line with the recommendations from WHOand, especially, the Ottawa Charter for Health Promotion.
Health promotion is not only the responsibility of the health care sector. It is wider than simply healthy life-styles; it aims at improving well-being. We know that health promotion concerns us all. Healthy cities is an effec-tive way to ensure change.The French Healthy Cities Network provides valuable support to all its member cities.André RossinotMayor of Nancy
Spotlight on FranceHealthy cities in action – a tool for pro-moting exchangeEvery 2 years, the Network produces a directorythat gives a broad overview of activities in everymember city. The directory begins with briefoverview of the principles of healthy cities andthe criteria for joining the Network. Then themajor activities of each member city are con-cisely presented. This information includes con-tact information, the city’s population and a de-scription of key activities organized by themeand population group.
In a country the size of France, the directory isa powerful tool for facilitating city-to-city ex-changes, because it allows users to search for in-formation by geographical location, theme,population group and key words.
Published in hard copy and on the Network’sweb site, the directory documents the diverse ac-tions carried out throughout France. It is an es-sential resource for supporting local action andpromoting the work of the Network to nationaland international partners.
FRANCE . 45
31497_National.p65 06-10-2003, 08:0445

46 . NATIONAL HEALTHY CITIES NETWORKS
GermanyCountry factsPopulation: 82.0 millionUrban population: 88%Living in national network cities: 27%
Network factsEstablished: 1989Members: 58Organization: associationWeb site: http://www.gesunde-staedte-netzwerk.de
Promoting exchangeA primary goal of the Network is to share experi-ences of healthy cities approaches through:• a newsletter available online and disseminated
3–4 times annually;• a healthy cities web site;• a healthy cities award (established in 1999) for
models of excellence in intersectoral collabora-tion;
• the documentation of models of good practice;• working groups on issues such as health promo-
tion in the workplace;• workshops on issues such as health assessment
or citizen participation;• international healthy cities symposia;• work in four regional networks; and• disseminating models of good practice at work-
shops, conferences, etc.
PartnershipsMember cities of the Network cooperate withhealth-promoting schools, health-promoting hos-pitals, health-promoting companies and Agenda21 activities. The Network also places high valueon citizen participation and partnerships withcommunities. For example, local self-help groupsand citizen action committees have been repre-sented at the Network’s general meeting. Coopera-tion between the Network and the German Asso-ciation of Cities and Towns on health and socialissues resulted in the 1999 Declaration of Co-logne, which promotes commitment to equal op-portunities.
At the international level, the Network has co-operated with the Austrian Healthy Cities Net-work and Slovenian Healthy Cities Network since1996.
Eleven cities founded the German Healthy CitiesNetwork in 1989 in Frankfurt am Main to facili-tate exchange. Today, the Network includes 58member cities that cover about 22 million inhab-itants. The major cities of Germany, includingBerlin, Hamburg, Munich, Cologne, Dresden andDüsseldorf, are part of the Network. Importantaims of the Network are to strengthen politicalcommitment to healthy cities and to demonstratethe competence of member cities. The Networkfunctions as a self-help organization of cities. Acondition for membership is accepting the Net-work’s nine-point programme (Box 5.12) througha formal council resolution. This programme hasbeen continually updated to reflect member expe-riences and changing conditions.
Box 5.12.A nine-point programme of action1. Agree to join the Network by a council
resolution2. Found a healthy cities office locally3. Develop intersectoral health promotion
policies4. Carry out health impact assessment5. Involve communities6. Report on health7. Participate in Network activities8. Exchange information9. Report experiences and successes to the
Network every 4 years
The Network secretariat is based in the health au-thority of Hamburg. The Network’s General As-sembly elects an executive board composed of fivepolitical representatives and five members of self-help groups within member cities.
31497_National.p65 06-10-2003, 08:0446
Network achievementsThe Network’s achievements include the follow-ing.• Nearly every important city in Germany is a
member of the Network.• Cities have established healthy city structures.• After 12 years, the Network has become an im-
portant agency for advancing health promotionin Germany.
• The Network is an important partner for manyother institutions in health promotion.
• Member cities have excelled in the fields ofhealth promotion and public health.
The futureThe Network aims to establish an alliance to in-crease the impact of health promotion in Ger-many by working more closely with institutions
active in this field, such as the Federal Centre forHealth Education, the Federal Association forHealth, medical associations, public health or-ganizations and environmental groups.
For more information, contact:Klaus-Peter StenderNational Network CoordinatorGerman Healthy Cities Network Secretariatc/o Labour Health and Social Issues AuthorityTesdorpfstrasse 8D-20148 HamburgGermanyTel.: +49 40 428482216Fax: +49 40 428482604E-mail: [email protected]
Spotlight on GermanyHealthy city competence centresEstablishing the healthy city competence cen-tres has been a successful strategy of the Net-work. The Network has eight healthy citycompetence centres organized by seven mem-ber cities:• healthy district development – Halle
(Saale);• health of children and youth- Stuttgart;• health promotion and health reporting for
children and youth – Kreis Neuss;• migration and public health – Frankfurt am
Main and Friedrichshain-Kreuzberg vonBerlin;
• health conferences – Herne;• local health management – Kreis Unna; and• consumer protection – Kreis Unna.
The tasks of these centres are to transfer spe-cialist knowledge to other cities. Developingthese centres is a goal of the Network’s actionplan for the next 6 years.
These cities have special knowledge on real-izing the idea of a healthy city. They are per-suasive examples of how to organize the localhealth process. Healthy city competence cen-tres will have a significant role in the future ofthe Network, because they will improve thequality of the work of all members.
GERMANY . 47
31497_National.p65 06-10-2003, 08:0447

48 . NATIONAL HEALTHY CITIES NETWORKS
GreeceCountry factsPopulation: 10.5 millionUrban population: 60%
Network factsAccredited: 2001Established: 1991Members: 52Organization: not-for-profit organization
BackgroundThe Hellenic Healthy Cities Network was first es-tablished in 1991 and was registered as a legal or-ganization in 1994. The Network has had threemajor reorganizations, each serving to make theNetwork more robust. Today, the Network is anot-for-profit organization with 52 municipalmembers. About one third of these members arelocated in the Athens metropolitan area and par-ticipate in a special metropolitan network, asubnetwork of the Network.
A range of activitiesConsiderable effort has been put to campaigningfor the healthy city project, so as to gain wider ac-ceptance both at the local and central governmentlevel as well as in institutes and agencies. The Net-work develops links, promotes partnerships andsecure funds for healthy city projects, includingthe production of health profiles and plans.
Main aims of the Network1. Support the development of a city health plan
in each city in accordance with WHO’s healthfor all policy.
2. Facilitate the sharing of experiences and goodpractices between cities.
3. Provide information to the cities on health pro-motion and disease prevention.
4. Improve health and the quality of life in the cit-ies through health promotion activities.
5. Organize events and seminars based on theneeds expressed by the member cities.
ActivitiesRecent activities in support of this goal includethe following:
Children and the healthy cityThe Ministry of Education funded this project,which it was carried out in secondary schools. Itaimed: 1) to record the children’s views of theirsurroundings and their knowledge about healthand environmental protection; 2) to empower thechildren to identify potential problems and thinkthrough the options through a series of discus-sions and creative exercises; and 3) to create strat-egies for action and take a stand. Seminars forteachers were also carried out, and a semi-interac-tive CD-ROM that can be used at any upper pri-mary or secondary school is currently being pro-duced.
Recording the social identity of and identificationof socially excluded groups in DodecaneseThe completion of this study, in which the Net-work acted as a partner of the National Centre forSocial Research, resulted in the development ofhealth profiles for the four municipalities in Do-decanese.
Social exclusion profiles at the city level –development of initiatives and social inclusionmechanismsThe Network worked on this research projectfunded by the European Union, completed during2001, as a partner of the National Centre for So-cial Research. This project’s aims included estab-lishing a system for monitoring social exclusioncapable of identifying changes in and the determi-nants of social exclusion at the city level, to en-courage the development of a city network fortransferring and sharing social exclusion data andto draw recommendations from the experience ofmunicipalities.
31497_National.p65 06-10-2003, 08:0448

City health planningThe strategic plan of the Network is to advocate,support and assist the development of health ac-tion plans in all city members, and to establish arelated documentation centre for the Network.The strategic plan includes the following steps:• developing the city health profile, which evalu-
ates the health status of the population and de-scribes the environmental conditions and fac-tors affecting citizens’ health;
• measuring and continuously monitoringhealthy city indicators, a series of socioeco-nomic, environmental and demographic indi-cators;
• at the local level, synthesizing these findings inintegrated local action plans submitted to localcouncils; and
• at the national level, developing a database forcollecting, comparing and analysing indicatorsand profiles from the cities.
The Network is focusing on meeting the primaryhealth care needs of people who fall out of theumbrella of the national plan. It is envisaged thatthe development of local health action plans incities will motivate the introduction of new insti-tutional mechanisms in cities for designing, devel-oping and realizing health and social policy at thecity level and for facilitating comparison betweencities at the national and European levels.
Responding to national prioritiesThe Network aims to respond to the challengesstemming from the National Health Plan (2000–2006), which includes:• improving primary health care services;• completing a national health map;• decentralizing the administration – each prefec-
ture should have its own local health plan;• implementing independent hospital manage-
ment;
• implementing a new organization for the ad-ministration of health resources; and
• operating hospitals after-hours.In conjunction with this, statutory bodies are alsoin a slow process of decentralizing responsibilityto municipalities for environment and health. TheNetwork sees itself as having a special role in fa-cilitating intersectoral partnerships. Municipalitieshave a good track record of collaboration and ef-fectively using resources. The Network will buildon this experience to respond effectively to thegovernment’s new health agenda.
PartnershipsThe key partners of the Network include the Min-istries of Health, Environment and Housing. Forexample, the Network has worked with the Minis-try of Housing in a project that brings togetherthe indicators work of healthy cities and LocalAgenda 21. The activities described above illus-trate the Network’s partnership with the NationalCentre for Social Research. The Network also haslinks with a national programme for promotingcommunity involvement in formal education, anintersectoral forum for community developmentand a national forum for preventing smoking.
For more information, contact:Yannis PapatheocharisHead of SecretariatHellenic Healthy Cities NetworkAgiou Georgiou 56P.O. Box 65125GT-15410 AthensGreeceTel.: +30 1067 70547Fax: +30 1067 22859E-mail: [email protected]
GREECE . 49
31497_National.p65 06-10-2003, 08:0449

50 . NATIONAL HEALTHY CITIES NETWORKS
HungaryCountry factsPopulation: 10.0 millionUrban population: 63%Living in national network cities: 10%
Network factsAccredited: 2000Established: 1989Members: 23Organization: association (nongovernmental organization)Web site: http://www.hahc.hu
work’s secretariat is based in the Pécs Healthy Cit-ies office and is supported financially by the city.Membership fees fund network activities.
Recognition of high standardsThe network has limited its growth to three newmembers a year, preferring quality to quantity.Over the past 15 years, this focus on quality hasmade the Hungarian network a strong and reliablepartner in the eyes of national actors. Since 1990the network has been invited to participate onvarious national boards and bodies such as the Na-tional Committee on Health Promotion and theNational Environmental Health Committee. Inthis context, the network has also been asked torepresent the local dimension in the planning andimplementation of various national programmes.The next section describes an example of suchwork. The Ministry of Health provides funds forsome of the network’s programmes and nationalactivities. The network also receives a small grantfrom the Civic Fund of the Hungarian Parliament.
Planning guidance: building links between healthand the environmentProducing city health development plans is an on-going priority of the network. In recognition of itsexperience of integrated health planning, the net-work was invited to participate on a subcommit-tee of the National Health Promotion Committeein 1995. The network’s role on the committee wasto develop a strategy for the local implementationof Hungary’s national environment and health ac-tion plan. Six member cities piloted local environ-ment and health action plans. These cities foundthe framework of city health development plansto be a useful tool for developing local environ-
BackgroundAfter becoming one of the first WHO project cit-ies, Pécs initiated collaboration on healthy citiesin Hungary. In 1989, an informal network of fivecities was established. As the network grew, thecities decided to create more formal links and ob-ligations by setting up a legal association in 1992.Today, the Hungarian Association of Healthy Cit-ies brings together 23 cities under a solid frame-work of quality standards, consistent with theWHO action framework for European nationalhealthy cities networks (Annexes 2, 3).
Political leadership and network managementMayors represent cities in the network’s GeneralAssembly, and they set the strategic direction ofthe network. The General Assembly elects a presi-dent (the network’s political head) annually fromamong its members. The General Assembly electsa seven-member board, which meets 3–4 times ayear to take decisions on common network pro-grammes and initiatives. The network has made anumber of recommendations for cities to securestable political support for local projects (Box5.13). The network’s General Secretary (the coor-dinator of the network) and local coordinators areresponsible for day-to-day operations. The net-
Box 5.13. Recommendations forsustaining political support• Create a strong organization, with
community support, to ensure continuityduring political changes
• Give local politicians a role in projects• Set up an independent budget for the
healthy city project
31497_National.p65 06-10-2003, 08:0450
ment and health action plans. Based on their ex-perience, the network produced a guidebook onthe preparation of local health and environmentaction plans in 1998. The guidebook focuses onaddressing the broad determinants of health tobridge health and environmental concerns.
EvaluationThe network evaluated its members and publishedit in Yearbook 2000 (http://www.hahc.hu, accessed
13 August 2003). Eighteen of 21 cities respondedto a questionnaire on:• organizational structures;• local commitment to develop a health plan and
work on specific themes; and• networking.The evaluation gives insight into the location ofthe project in the city structures, membership ofsteering committees, human resources and localdecision-making processes and key local and na-tional partners (Box 5.14). The most importantcommon activities included the elaboration ofcity health profiles and plans, the organization ofhealth days and weeks, peer teaching related topreventing drug abuse and the eradication ofragweed.
For more information, contact:Antonio de BlasioNational Network CoordinatorHungarian Healthy Cities NetworkWHO Egészséges Városért AlapitványVaradi Antal u. 11, H-7621 PécsHungaryTel.: +36 72 312965, Fax: +36 72 515861E-mail: [email protected]
Box 5.13. Priorities of members of thenetwork• City health plans and profiles• Drug prevention programmes• Anti-smoking programmes• Health promotion in schools• Advice on healthy lifestyles• Environment and health action plans• Mental health• Screening programmes• Health behaviour research
Source: de Blasio A, ed. Yearbook 2000. Pécs,Hungarian Association of Healthy Cities, 2001(http://www.hahc.hu, accessed 13 August 2003).
Spotlight on HungaryNational Healthy Cities Media AwardBackgroundThe issue of health communication in the massmedia has long been an important discussiontopic among health promotion experts and envi-ronmentalists. In response to this issue, the net-work carried out a joint training session forproject coordinators and local media profession-als based in member cities. Building on the suc-cess of this first step, the idea of creating an an-nual mass media award for coverage of thehealthy cities movement in Hungary was born.The first award was granted in 2001.
ImplementationThe basic idea of the award is to give higher vis-ibility to health and environmental issuesthrough coverage of healthy city activities invarious forms of national and local media. TheNational Healthy Cities Media Award is grantedin three categories – television, radio and writtenmedia. Local city coordinators announce theaward to their mass media partners, and a call forentries is published in professional periodicalsand in some daily newspapers. The board of the
network dedicated EUR 4060 to the award in2001 and 2002 respectively. Each year there weremore than 40 entries, demonstrating strong in-terest among mass media professionals.Representatives of the Ministries of Health,Sport, Environment and Education sit on a jurywith respected mass media, public relations andhealth experts to determine the best piece ineach category. For example, an award wasgranted to a journalist in 2002 for a newspaperseries on local healthy city activities in Paks. Thejury also selects the recipients of a special prizefrom the Ministries of Sport, Education and theEnvironment. The Minister for Health presentsthe National Healthy Cities Media Award to thewinners.
ConclusionThe National Healthy Cities Media Award hasproven to be a good tool for creating strongerpartnerships between the member cities and themass media. It has raised both the quality andthe amount of media coverage on health and en-vironmental issues as well as the visibility of thehealthy cities movement in Hungary.
HUNGARY . 51
31497_National.p65 06-10-2003, 08:0451

52 . NATIONAL HEALTHY CITIES NETWORKS
IsraelCountry factsPopulation: 6.5 millionUrban population: 91%Population living in network cities: 43%
Network factsAccredited: 2000Established: 1990Members: 57Organization: association
BackgroundThe Israeli Healthy Cities Network was founded in1990 by four cities and the Ministry of Health.The Network was launched by a political declara-tion, which made an explicit commitment tohealth for all and the Ottawa Charter for HealthPromotion. In 1997, the Network became a legalassociation and a supported unit within Israel’sUnion of Local Authorities. Today the Network in-volves 36 cities, 4 ministries, a school of publichealth and a number of nongovernmental organi-zations and individuals.
Network objectivesThe aim of the Network is to promote the adop-tion of healthy cities as a method. The Networkencourages cities to integrate healthy cities princi-ples into their local organizational structures andstrategic plans. To facilitate this outcome, the Net-work has a strategic plan with objectives to:
• disseminate knowledge of healthy cities andAgenda 21;
• call upon politicians and academics to widelysupport healthy cities;
• develop partnerships with government, public,private and international organizations;
• provide training and support to member cities;and
• increase the status of healthy cities as a main-stream policy movement.
Promoting action for equityThe Network challenges local politicians to makea formal commitment to take action for equity inhealth. The idea began when mayors of the mem-bers of the WHO European Healthy Cities Net-work signed a statement on action for equity in
Europe on 10 June 2000 in Horsens, Denmark.This statement included a pledge to develop sys-tematic approaches to address equity issuesthrough a number of key actions. The Networktranslated the statement into Hebrew and held aconference on the subject in May 2001. As a re-sult, six mayors signed the statement. The Net-work took this concept of a formal political com-mitment forward by adopting a Healthy CityCharter. The Charter has two versions: one formayors of Network members to sign after theirelection (new and incumbent) and another aimedat political candidates before elections. The firstpoint of the Charter is a commitment to act forequity. Other points relate to the principles andstrategies for health for all and Local Agenda 21.
A workbook on city health profilesThe Network began working with indicators andcity health profiles in 1992. Maale Adumim, aNetwork member, carried out a city health profilein 1993, which served as a lever for developing atool for the Network. The Network set up a healthprofile task group and developed a workbook onthe preparation of a city health profile (availablein English). The workbook defines a number of in-dicators and a step-by-step process for collectingand analysing data derived from official sourcesand population surveys. The Network facilitatesthe task of data collection by providing eachmember city with relevant national-level data ontheir city, together with national averages. Theworkbook also gives advice on how to present anddiscuss findings with mayors and local steeringcommittees.
Integrating health and sustainabledevelopmentIn 2001, the Network was part of a national steer-ing committee responsible for preparing Israel’snational report on the Habitat Agenda. The aim ofthe Habitat Agenda is to promote socially and en-vironmentally sustainable towns and cities withthe goal of providing adequate shelter for all. Par-ticipants on the national committee agreed thathealthy cities embraced the principles of bothAgenda 21 and the Habitat Agenda. The resultingnational report challenged healthy cities to act asmodels for the implementation of the HabitatAgenda – making use of the Network’s city healthprofiling tool to measure progress over time. In re-sponse, the Network undertook a comparativeanalysis of indicators based on health for all, LocalAgenda 21 and Habitat targets. It updated itsworkbook on city health profiles in 2001, bring-
31497_National.p65 06-10-2003, 08:0452
ing together the three agendas. Today, the toolprovides a solid basis for developing local healthand sustainable development strategies.
Mutual support and trainingNetworking between cities started with periodicmeetings to facilitate exchange. Today coordina-tors network naturally – regularly consulting oneanother on planning and maintaining activities.The Network now has several senior coordinatorslocated in four regions who provide regional sup-port to new colleagues. New cities visit more expe-rienced cities to learn by seeing a healthy city inaction. The Network gives high priority to provid-ing intensive training for coordinators. For more information, contact:
Milka DonchinNational Network CoordinatorIsraeli Healthy Cities NetworkDepartment of Social MedicineHadassah School of Public Health and Commu-nity MedicineP.O. Box 12000Jerusalem 91120IsraelTel.: +972 2 6777538Fax: +972 2 6439730E-mail: [email protected]
Box 5.14. Aims of the trainingprogramme• To develop skills in leadership,
management, teamwork, leadingintersectoral steering committees anddeveloping partnerships
• To gain knowledge in health promotionand sustainable development
• To gain knowledge in collecting andanalysing data and planning interventionsto meet defined needs and aspirations
Box 5.15. Topics covered by the course• Inequalities in health• The Israeli health system• The national service of community work• Healthy urban planning• Green spaces in a healthy city• The health effects of physical activity• Oral health• Leisure activities for elderly people
• Individual versus community rights• Not-for-profit organizations
Spotlight on IsraelA training course for healthy city coor-dinatorsThe Israeli Healthy Cities Network recentlycarried out a 120-hour training programme,which enabled participants to obtain continu-ing education credit. The programme aimedto give coordinators the core set of skills theywould need to lead and manage a healthy city(Box 5.14). However, municipal employees,politicians, ministry representatives and pro-fessionals active in health promotion and en-vironmental protection were also invited toattend.The course introduced the key principles ofhealthy cities and sustainable development –
building knowledge in areas such as healthsettings, data collection and analysis, strategicplanning, participatory leadership, communi-cations and evaluation (Box 5.15).Twenty participants took part in this course,which ran from January to July 2002. TheMinistry of Health funded 60% of the partici-pation fee, which covered lectures, teachingmaterials, field visits and meals.As a result of their participation in the course,several cities re-established the coordinatorrole in their city and two new cities joined theNetwork. An unexpected outcome of thecourse was the creation of a supportive groupof friends.
ISRAEL . 53
31497_National.p65 06-10-2003, 08:0453
54 . NATIONAL HEALTHY CITIES NETWORKS
ItalyCountry factsPopulation: 56.8 millionUrban population: (67%)Population living in network cities: 16%
Network factsAccredited: 2003Established: 1995; relaunched in 2001Members: 115Organization: not-for-profit associationWeb site: http://www.comune.bologna.it/cittasane-oms
The healthy cities movement in Italy began infor-mally in 1989. A network was officially estab-lished in 1995 when 40 cities signed a joint politi-cal agreement. Today, the Italian Healthy CitiesNetwork brings together some of Italy’s largest cit-ies, including Rome and Milan, in implementingthe principles of health for all and Agenda 21. TheNetwork cooperates and facilitates exchange onAgenda 21. Cities pay an annual membership fee.
A network re-launchedUntil 2001, cities joined the Network by signing aletter of intent, accepting the Network’s Pro-gramme Charter. Although this required a politi-cal commitment to health for all principles, theProgramme Charter did not set out criteria linkedto regular activities. Following political changesafter local elections, city administrations wouldoften be unaware of previous commitments to theNetwork. As a result, many cities became inactive.
To remedy this situation, the Network put for-ward a proposal for a new Network structure tobolster local political commitment to healthy cit-ies in 2000. Four national meetings were held toestablish new statutes stipulating out the structure
and criteria of the Network. In 2001, the Networkwas re-launched as a not-for-profit association. TheNetwork’s criteria (Box 5.16) require cities to makean annual political commitment to healthy cities.
Political steering committeeThe Network places high priority on involvingpoliticians. The Network’s main governing body,the General Assembly, is comprised of politicians(mayors, aldermen and municipal advisers). TheGeneral Assembly elects a President, who is thepolitical head of the Network, and a steering com-mittee from among its members. The Presidentappoints a national coordinator, who directlyleads and manages a technical committee. Thetechnical committee acts according to the politi-cians’ recommendations. The technical committeecomprises city coordinators of members of theWHO European Healthy Cities Network and anumber of other city coordinators elected by theGeneral Assembly.
City health profilesMembers of the Network have made a commit-ment to developing integrated city health plans.The first step has been the development of cityhealth profiles. Cities identified the need for thistool, as a means of putting the health and well-be-ing of citizens at the heart of local decision-mak-ing. By January 2003, 18 cities had produced pro-files: Bologna, Udine, Barletta (BA), Bari, Mesagne(BR), Arezzo, Maniago (PN), Ancona, Modena, Son-drio, Conegliano (TV), Vercelli, Milan, Siena, Mol-fetta (BA), Padua, Venice and Vittorio Veneto (TV).
Information and exchangeThe Network is extremely active. Since 2000, therehave been 12 meetings of the technical commit-
Box 5.16. Criteria for membership of theItalian Healthy Cities Network• An annual membership fee• Dedication of municipal funds and
organizational resources to local healthy cityactivities
• Nomination of a local technical coordinator• Consistent activity on healthy city projects• Participation of politicians at national
meetings• Local contribution to the Network’s national
report
31497_National.p65 06-10-2003, 08:0454
tee, 5 national meetings of politicians on themanagement of the Network, 4 national assem-blies and 2 national conventions. In 2003 the Net-work held a training seminar for new members.The Network has brought European experience toItaly’s cities by translating core documents of theWHO European Healthy Cities project. The Net-work is also developing a practical manual forpoliticians and professionals on how to imple-ment the healthy cities approach. The manualdraws upon WHO documents and global strate-gies for health and sustainable development. Themanual will be presented at the next nationalconvention in Potenza in March 2004.
A national methodThe Network is currently producing its second na-tional report. The report aims to promote a na-tional method for healthy cities, by sharing theevaluation of local action. It provides case studieson the practical application of healthy city princi-ples, with examples from the most active citieshighlighting new ideas. The report will also iden-tify a number of subjects of national concern aswell as approaches and activities that characterizethe Network.
Regional networkingRegional networking is an interesting area of de-velopment in the Network (Box 5.17). A regionalnetwork was recently established in Puglie in De-cember 2002, which brings together 13 cities.Other regional networks have been set up in Tus-cany and Piedmont. The national political steer-ing committee discussed with representatives ofeach regional network about how regional net-works could formally be included as members ofthe Network association. It is foreseen that the re-gional networks will adopt the Network’s statutesand structures, recognizing the national President,Coordinator and the organization of the national-level association.
Multi-city action plansThe Network has established a number of multi-city action plans, which bring groups of cities to-gether to work on issues of common concern.Current multi-city action plans are working withthe issues of alcohol, tobacco and mental health.Previous work on multi-city action plans pro-duced interesting connections with the EuropeanNetwork of Health Promoting Schools and the Eu-ropean Network of Health Promoting Hospitals.
FutureThe Network intends to build on its successes topromote:• better integration among the national health
networks;• an efficient policy on governance; and• wider involvement of citizens.
For more information, contact:Fulvia SignaniNational Network and Healthy City CoordinatorItalian Healthy Cities Networkc/o Assessorato alla Sanità ed AmbienteSettore Salute e Qualità della Vita Comunedi BolognaVia Libia 57, I-40138 Bologna, ItalyTel.: +39 051 4293470–50, Fax: +39 051 4293451E-mail: [email protected] [email protected]
Box 5.17. Regional healthy citynetworkingRegional networks provide meeting points forgeographically close cities. The immediate valueof these networks is their capacity to:• Strengthen healthy city approaches• Facilitate local benchmarking• Share human capital (experts and
technicians)• Exchange methods and ideas
Our specific aim is now to disseminate the WHO Healthy Cities philosophy, to achieve good results on evalua-tion and to devote continuous attention to equity in health.Excerpt from a presentation of the Network’s Activity Programme, 2002–2004Gian Paolo Salvioli, President, Italian Healthy Cities Network AssociationBologna Health and Environment Alderman
We can say that the task of drawing the health profile of a city is a noble and complex commitment ... Thehealth profile, which has brought together different institutions such as schools, political forces and the vol-untary movement, has become a consultation tool to evaluate indicators on the quality of life in Barletta. ...The most important outcome will be to live in a healthier city.Francesco Salerno, Mayor of Barletta
ITALY . 55
31497_National.p65 06-10-2003, 08:0455
56 . NATIONAL HEALTHY CITIES NETWORKS
KazakhstanCountry factsPopulation: 16.0 millionUrban population: 46%Population living in cities: 24%
Network factsAccredited: 2002Established: 1999Members: 10Organization: coordinated by the NationalCentre for Healthy Lifestyles Development
The Kazakhstan Healthy Cities Network is coordi-nated by the National Centre for Healthy Life-styles Development. The Network is thus wellplaced, as the Centre is responsible for coordinat-ing all Kazakhstan’s settings programmes. TheCentre’s regional, urban and local health promo-tion centres are also involved in the Network.
National partnershipsThe Network has developed formal partnerships,based on cooperation agreements, with a numberof national-level bodies (Box 5.18). The Networkalso enjoys support from the President and theFirst Lady of Kazakhstan and as well as deputies ofParliament. The National Centre for Healthy Life-styles also mobilizes its partnerships with agenciesof the United Nations (including UNICEF,UNESCO, UNFPA, UNDP and United Nations Vol-unteers), the United States Agency for Interna-tional Development, the Soros Fund, foreign uni-versities and private companies in support of theNetwork.
Political commitmentThe Network places high priority on the activerole of mayors (akims) in the project. Mayors areresponsible for the health and quality of life of in-habitants and the socioeconomic situation in thecity. They have authority over all health, educa-tion and social programmes. They are also in regu-lar contact with citizens. Mayors present at leastone speech a month on local television and havea telephone hotline for citizens. Several mayorsorganize meetings with citizens 2–3 times per yearon key issues of concern.
In 2003, the Network coordinator visited themayors of all Network cities, who confirmed theircommitment to the project. The coordinatorshared with them the progress of other Networkcities and provided methodological materials forprogress in urban health. The Network coordina-tor has also met with a member of Parliamentwho has proposed the creation of a national coor-dination council. This would fall under the aus-pices of the government and would represent lo-cal healthy city interests at the national level.
Action and prioritiesThe overall goals of the Network are to mobilizelocal, national and international actors to supportlocal policies aimed at improving health, the qual-ity of life and the environment in cities. A keyachievement of the Network has been the adop-tion of healthy cities as a government policy inKazakhstan. Network cities work on both com-mon as well as locally defined priorities (Box5.19).
In 2003, the Network launched a Healthy Vil-lages project, following WHO guidelines.1 Thisproject supports the development of healthy com-
Box 5.18.Key partners of the Network
• Ministry of Public Health• Ministry of Education and Science• Ministry of Culture, Information and Public
Accord• Agency of Tourism and Sport• Ministry of Internal Affairs• Ministry of Defense• Ministry of Labour and Social Protection of
the Population• Ministry of Natural Resources and
Environment Protection
31497_National.p65 06-10-2003, 08:0456
munities by supporting community leaders in as-sessing problems and setting priorities amonghealth interventions. The Network will work withHealthy Villages to disseminate the healthy citiesapproach and to promote the exchange of experi-ence between adjacent villages. Healthy Villages isa response to the President’s announcement that2003–2005 will be Years of Support for Villages.
Raising public awareness of health promotionAll Network cities organize 12 large-scale healthpromotion events annually. These typically in-clude the participation of at least 60–70% of thepopulation of these cities. The events are usuallylinked to health education and the quality of life.
For example, the programme called Torch forHealth brought together 30 000 participants in sixregions of the country. As part of the event, atorch was passed between people identified asleading healthy lifestyles. An exhibition on thetheme of women’s health attracted 50 000 partici-pants. The Network’s annual Festival of Health is aresponse to the national social strategy,Kazakhstan 2030. The Network plans to launchnew joint initiatives to support orphans and topromote good nutrition for pupils.
For more information, contact:Tamara GermanyukNational Network CoordinatorKazakhstan Healthy Cities NetworkNational Centre for Healthy Lifestyles Develop-ment, Prophylactic Programmes86 Kunaev Str480100 AlmatyKazakhstanTel.: +7 3272 918415Fax: +7 3272 911083E-mail: [email protected]
1 Healthy villages: a guide for communities and community
health workers. Geneva, World Health Organization, 2002
(http://www.who.int/docstore/water_sanitation_health/
Healthyvil/HVtoc.htm, accessed 22 August 2003).
Box 5.19.Health priorities in cities in Kazakhstan
• Behavioural risk factors (alcohol and drugabuse, smoking, etc.)
• Family health• Healthy nutrition• Health of children, adolescents and young
adults• Environment• Water quality• Health-promoting schools• Healthy universities
Spotlight on KazakhstanHealthy environments for childrenWorld Health Day takes place every year on 7April. The theme in 2003 was Shape the Fu-ture of Life: Healthy Environments for Chil-dren, focusing on the leading causes ofchronic illness in childhood that are relatedto environmental hazards. The Networkplanned a wide range of activities in themonth leading up to World Health Day. TheNetwork also encouraged all cities inKazakhstan to organize such activities and toinvolve citizens.
Key activities in Network cities that markedthe event included:• healthy workplaces, study places and city
spaces;• training and lectures for children at
schools and preschools and for universitystudents;
• training for parents in life skills atworkplaces;
• greening of city spaces (more than 2000saplings were planted in each Networkcity); and
• children’s artwork on the theme was exhib-ited in all Network cities.
Mayors of Network cities made speeches onlocal television and radio stations and partici-pated in round-table discussions. School psy-chologists also took part in these actions.They worked not only with the children butwith the parents and teachers. The WorldHealth Day events were further supported by520 health-promoting schools, 30 healthyuniversities, 25 health-promoting hospitalsand 27 healthy workplaces.
KAZAKHSTAN . 57
31497_National.p65 06-10-2003, 08:0457

58 . NATIONAL HEALTHY CITIES NETWORKS
LatviaCountry factsPopulation: 2.3 millionUrban population: 67%Population Living in network cities: 61%
Network factsEstablished: 2002Members: 15Organization: nongovernmental organization
Latvia’s network for healthy cities was establishedin 2002, following several years of awareness-rais-ing efforts. The network’s formal title is LatvianHealth Promoting Municipalities. Members in-clude cities, towns and rural districts with the sta-tus of a municipality. Municipalities join the net-work by passing a council resolution in support ofmembership. The network works closely with theMinistry of Health, the WHO Liaison Office, theNational Association of Local Authorities and theEuropean Network of Health Promoting Schools.Activities are funded through membership fees.
ExchangeThe network holds two meetings a year. These fo-cus on exchanging experience on actions thatsupport the city hosting the meeting and address-ing a range of common priorities. Past meetingshave addressed issues ranging from substanceabuse to the specific challenges of implementingthe healthy cities approach. These challenges in-clude establishing infrastructures for health pro-motion work in municipalities and how to workin partnership with regional coordinators fromthe National Health Promotion Centre.
PartnershipsThe Network has partnerships with the WHO Liai-son Office in Latvia, the Ministry of Welfare, theNational Health Promotion Centre and the BalticRegion Healthy Cities Office. The network con-tributed to the development of Latvia’s publichealth strategy in 2001 through participation innational work groups. In accordance with WHO’sHEALTH21 policy, the national policy has 21 tar-gets. Target 13 on settings for health promotionstates that, by 2010, the people of Latvia shouldhave greater opportunities to live in healthy
physical and social environments at home, atschool, at work and in the local community. Thestrategy calls for developing a nationwide networkof healthy cities and communities to reach the ob-jectives of this target. Health Promoting Munici-palities also works in close partnership with theLatvian Network of Health Promoting Schools. To-gether they develop local activities, projects andseminars.
Regional cooperationThe National Health Promotion Centre has initi-ated a new health promotion model that involvesthe implementation of programmes at the re-gional level. Nine regional coordinators, who arebased in municipalities, are responsible for imple-menting regional projects. The network is workingin partnership with these regional coordinators tofacilitate effective cooperation with municipalitieswhile developing local-level capacity and supportfor health promotion. This relationship is en-hanced by the fact that most of the regional coor-dinators are based in network cities.
Bridging health care and healthpromotionAlthough Latvia’s municipalities are responsiblefor primary health care services, they have no di-rect responsibility for health promotion. As thehealth care sector is currently inadequatelyfunded, municipalities have been reluctant toshift resources to health promotion. Recently,members of the network have responded to thissituation by developing strategic municipal healthpromotion plans. Municipalities have establishedwork groups with the aim of clarifying their rolein the field of health promotion. They have alsoworked to develop mechanisms to involve general
31497_National.p65 06-10-2003, 08:0458
practitioners in healthy city initiatives. The net-work has developed an 8-hour training pro-gramme for general practitioners on Health Pro-moting Municipalities and its activities. It ishoped that cooperation with general practitionerswill lead to support for increased investment inhealth promotion activities.
For more information, contact:Ina BehmaneNational Network CoordinatorLatvian Healthy Cities NetworkAvotu iela 123800 SaldusLatviaTel.: +371 3807903Fax: +371 3807910E-mail: [email protected]
Spotlight on Latvia
I was very pleased to see Riga incorporated into the WHO Healthy Cities movement at the end of 2002. Thecity of Riga now has to strive to reach the goals set by the WHO Healthy Cities movement. It is easier for Rigato implement these goals in cooperation with WHO and other healthy cities.In March 2001 the Ministers of Latvia adopted a public health strategy. The main goal of this strategy is to im-prove public health, and it is modelled based on the WHO European regional strategy for health for all in the21st century. One of the main principles of the strategy is to involve society as much as possible. I believethat the Latvian Healthy Cities project, working with the Riga City Environment Centre Agenda 21, can be-come one of the main tools for implementing the goals of the Latvian public health strategy at the municipallevel.Good practices and examples from the healthy cities will help to put health on the agenda!
Aivars Guntis KreitussDeputy Mayor, City of Riga
cooperation between physicians, social work-ers and the public.In Ventspils, several programmes have beencarried out to limit the distribution of drugs.Children from deprived areas or disadvan-taged families are given discounts to attendsporting and cultural events sponsored in thecity. Day care centres for children have alsobeen set up. These provide after-school carefor pupils aged 7–18 years.The two most important conclusions of theproject were that explicit political commit-ment for funded projects is essential and thatthere must be cooperation across sectors.As a result of this activity, five network citieshave developed new drug and alcohol preven-tion programmes and seven cities have suc-cessfully applied for project funding.
Preventing substance abuseIn 2002, the network carried out a 5-monthproject funded by Latvia PAV (a programme toprevent drug and alcohol abuse) to supportcities in developing plans to limit the use ofpsychoactive (mood-altering) substance abuse.Cities exchanged experience on initiatives inthis area, and coordinators developed skills inwriting project proposals.In Jelgava, citizens established anongovernmental organization called Parentsfor Jelgava. Parents involved in this organiza-tion take an active role in enforcing restric-tions on the sale of alcohol and tobacco toyoung people by monitoring venues wherethese substances are sold and used. This ap-proach is now being used in three other citiesin the network. Jelgava shared its positive ex-perience of treating addiction by promoting
LATVIA . 59
31497_National.p65 06-10-2003, 08:0459
60 . NATIONAL HEALTHY CITIES NETWORKS
LithuaniaCountry factsPopulation: 3.7 millionUrban population: 68%Population living in network cities: 41%
Network factsEstablished: 1994Members: 8Organization: not-for-profit organization
Background and overviewThe main activities of the Lithuanian Healthy Cit-ies Network focus on supporting municipalities indeveloping and implementing broad local healthpolicies. The Network gives priority to work oncity health profiles, improving the environmentand sustainable development, and social needs.Member cities have developed local public healthstrategies, environmental policies and social poli-cies.
The Network has a number of other nationaland international partners drawn from academe,international and national organizations and not-for-profit organizations.
Organization and resourcesThe main organs of the Network are the GeneralAssembly and the Board (Steering Committee).The Board consists of the coordinators from eachmember city (or region). The role of the Board isto• propose strategies for Network activities• define the direction of Network development• exchange information and coordinate activities
with other organizations• coordinate activities with other WHO initia-
tives.
Membership fees fund the Network, and the Cityof Kaunas hosts the coordinating office.
MembersThe Network is open to municipalities and regions.Eight municipalities, covering 41% of the Lithua-nian population, are members of the Network. Tobecome a member of the Network, municipalitieshave to formally accept the health for all principlesand to agree to develop and implement city pro-files and plans based on health for all.
Network thematic areasThe Network implemented a number of pro-grammes in 2002 related to environmental im-provement, health promotion and social needs,including work on:• city health profiles• education for municipal staff• courses for coordinators• healthy kindergartens• healthy schools.
The Network gives priority to involving citizens inall healthy city activities.
Municipal-level activitiesThe Network has organized a number of meetingsand conferences to support municipal-level workon health and the environment and sustainabledevelopment. The Network has also carried outconsultations with city coordinators, which haveyielded proposals for environmental improvementand health promotion in cities. The local councilsof member cities have adopted local public healthstrategies, environmental policies and social poli-cies.
National partnershipsThe Network contributes to developing nationalpolicy by cooperating with the Ministries ofHealth, Environment and Education. For example,through participation in the Health Care ReformBureau, the Network has had the opportunity toinfluence and put forward proposals on:• national debates• the preparation of the country’s public health
law and public health strategy• the development of training for health care spe-
cialists.
31497_National.p65 06-10-2003, 08:0460
This forum is responsible for developing healthpromotion and health care structures in cities andtraining.
The Network has also made proposals at the na-tional level related to the national environmentand health action plan and to the use of healthycity indicators. National environment and healthaction plans are government documents that ad-dress environmental health problems in a com-prehensive, holistic and intersectoral way. Healthand environment ministers across the WHO Euro-pean Region endorsed and strongly supported theimplementation of national environment andhealth action plans in the London Declaration ofthe WHO Third Ministerial Conference on Envi-ronment and Health in 1999.
The Network also participates on the NationalHealth Board and defines the programme of ac-tivities of the National Healthy Cities Institute.
International partnershipsBeyond its partnerships with the national govern-ment, the Network has a range of partners, includ-ing:
• Baltic Region Healthy Cities Office• Danish Healthy Cities Network• Polish Healthy Cities Association• United Nations Development Programme
• Regional Environmental Center for Central andEastern Europe
• Lithuanian Association of Municipalities• not-for-profit organizations• Kaunas Medical University• Vytautas Magnus University.
Future plansPlanned activities for 2003–2005 include imple-menting a healthy society policy and creatingpublic primary health care functions and institu-tions.
The Network also plans to build on its cityhealth profile work. Data collected by Networkcities will be used to develop a planning systemfor municipal health policies and strategies, basedon intersectoral cooperation.
For further information, contact:Juozas KameneckasNational Network CoordinatorLithuanian Healthy Cities NetworkKaunas Healthy City Project OfficeDonelaicio 75a-11LT-3000 KaunasLithuaniaTel.: +370 686 11815Fax: +370 7 209130E-mail: [email protected]
LITHUANIA . 61
31497_National.p65 06-10-2003, 08:0461
62 . NATIONAL HEALTHY CITIES NETWORKS
NetherlandsCountry factsPopulation: 16.0 millionUrban population: 90%Population living in network cities: about 50%
Network factsEstablished: 1989Members: 25Organization: Open membership
BackgroundEindhoven, one of the first members of the WHOEuropean Healthy Cities Network, initiated thedevelopment of the Dutch Healthy Cities Networkin the late 1980s. The Network is open to all citiesand has no specific criteria or fees. A support of-fice within the Association of Municipalities coor-dinates the Network. A working group comprisedof civil servants from municipalities and advisersfrom national health promotion organizationsand universities manages it. The Network receivesfunding from the Ministry of Health.
Supporting citiesThe overall goal of the Network is to support citiesin developing healthy urban policies. The Net-work also strives to influence ministries, especiallythe Ministry of Health, to adopt healthy cities ap-proaches and to set up mechanisms forinterministerial cooperation on health. The Net-work has produced 10 booklets on healthy citytopics and produces a quarterly newsletter distrib-uted to all municipalities and to the Network’spartners in ministries, national institutes and uni-versities. The Network has established cooperationwith the Ministry of Spatial Planning, Housingand Environmental Protection on healthy build-ing (see related section below). The Network hasalso influenced the Ministry of Health’s decisionto require municipalities to produce a local healthplan every 4 years.
Thematic work groupsThematic work groups are a key feature of the Net-work. Municipalities identify work group themesat Network meetings (Box 5.20). The aim of workgroups is to disseminate new ideas and to stimu-late action in cities by developing methods andpolicies based on local best practices. Work groups
remain active for as long as it takes to achievetheir objectives. Work group results are publishedand sent to the mayors of health of all municipali-ties. National conferences are often organized onwork group themes.
Healthy building and livingIn 1996, the Rotterdam City Council approved aresolution stating that major city developmentprogrammes would only be considered followingadvice from the health department on potentialhealth effects. In response, the Healthy City Officedeveloped a list of points to be considered such asthe needs of elderly people, the use of buildingmaterials, the effects of ventilation and lightingand a building’s connection to the environmentand community. Rotterdam cooperated inten-sively with the Departments of Building andTransport, learning valuable lessons on how tobring about positive health effects (Box 5.21). Forthis cooperation to be effective, the Healthy CityOffice had to understand the planning processesof these departments and provide relevant adviceat the appropriate time.
Rotterdam’s experience was shared at Network
Box 5.20. Thematic work groups in theNetworkThe Network has had work groups in the fol-lowing areas:• youth health promotion policy• healthy building and living• intersectoral cooperation• social safety problems• healthy neighbourhoods• local health policy• health and Agenda 21• local policies on chronic diseases
31497_National.p65 06-10-2003, 08:0462

meetings; as a result, a work group was establishedon healthy building and living. A booklet de-scribes the work group’s results and outlines rec-ommendations and examples of good practice.2 Aconference was held on the subject in 1997, atwhich the Minister for Spatial Planning, Housingand Environmental Protection commended theresults. As a result of this work, city councilsthroughout the country more frequently requestthis kind of health impact assessment on pro-posed building plans.
Promoting neighbourhood interventionThe Network has long placed a high priority onreducing health inequality through neighbour-hood intervention. Inspired by healthy cities workin the area, the Netherlands Institute for HealthPromotion and Disease Prevention (NIGZ) decided
to establish an office to support this type of workin 1999. The office, called SLAG (SteunpuntLokale Aanpak van Gezondheidsverschillen), co-operates with 15 Network cities. SLAG facilitatesdiscussions among politicians and professionals. Itprovides information on the methods and effectsof health interventions at the neighbourhoodlevel. SLAG also helps cities in securing fundingfor community projects through the NationalHealth Research Fund. Three cities, Arnhem,Eindhoven and Tilburg, are currently implement-ing projects that will soon be evaluated. These areall community-based projects in which experi-ments are taking place on how to involve thepopulation in the whole process of health educa-tion. The results are expected to further under-standing of participatory evaluation methods inhealth promotion.
FutureThe Network aims to influence the developmentof a new government policy for major cities. Thepolicy has economic, infrastructural and social di-mensions affecting approaches to job creation, ur-ban regeneration, social care, health and educa-tion.
The information for this profile was contributed byWilly de Haes, Coordinator of Healthy City Rotterdam([email protected]), before the Network’s newcoordinator, Matthew Commers, was appointed.
For further information, contact:Matt CommersCoordinatorDutch Healthy Cities NetworkAssociation of Dutch MunicipalitiesP.O. Box 30435NL-2500 GK The HagueThe NetherlandsTel.: +31 70 3738623Fax: +31 70 3738438E-mail: [email protected]
Box 5.21. The built environment andhealth in Rotterdam
Low-allergen housingThrough collaboration with the Departmentof Building, 40 low-allergen houses were builtas an experiment in Rotterdam. The buildingswere engineered to make allergic reactionsvirtually impossible. Maintaining theintegrity of this environment requireseducating the inhabitants, who are selectedto live there based on need.
Reducing negative health effects of road trafficIncreased air pollution was measured in anarea of the city where a number of roadsconverge. Children at a nearby school werecorrespondingly found to have more healthproblems, especially lung problems,indicating an overall health risk for thesurrounding neighbourhood. The cityresponded by introducing traffic-calmingregulation, which reduced speed limits from120 km to 80 km and resulted in ameasurable health improvement of 10–15%.
2 Bazuin H, van den Bogaard J, Zoutman R. Buimte voor
gezondheid; gezond bouwen en wonen in nieuwe wijken [Space
for health. Healthy building and living in new neighbourhoods].
The Hague, VNG Uitgeverij, 1997.
NETHERLANDS . 63
31497_National.p65 06-10-2003, 08:0463

64 . NATIONAL HEALTHY CITIES NETWORKS
NorwayCountry factsPopulation: 4.5 millionUrban population: 75%Population living in network cities: 18%
Network factsAccredited: 2000Established: 1994Members: 19Organization: network with statutesWeb site: http://www.poseidon.no/hmnett/index.html
BackgroundThe Norwegian Healthy Cities Network was estab-lished in 1994 based on an understanding that ittakes more than enthusiasts and one-off projectsto make a difference. For this reason, the Networkwas built on the following foundations:• a cooperation agreement with the Ministry of
Health, the Ministry of Environment and theAssociation of Local and Regional Authorities;
• network statutes that ensure political commit-ment; and
• membership criteria.Importantly, the cooperation agreement broughttogether the concepts of health and Agenda 21 – adefining feature of the Network.
Network management – a mix ofpolitical and technical leadershipThe strong participation of politicians in the Net-work has been an important source of strengthand legitimacy. Mayors represent cities in the Net-work’s General Assembly, the highest decision-making body. The Network’s executive board (orsteering committee) consists of three mayors andfour professionals who meet at least four times peryear. The chair of the board, a mayor, acts as thehead of the Network. Both political and technicalrepresentatives are required to attend regular Net-work meetings, which focus on technical priori-ties. Network meetings circulate on a rotating sys-tem between the member cities. Through their ac-tive involvement in the Network, politicians haverecognized the need for a full-time, technical co-ordinator. This post is funded through a govern-ment grant and a portion of the Network’s mem-bership fees.
Supporting nationalpolicy developmentThe Ministry of Health in-vited the NorwegianHealthy Cities Network tocontribute to a white paperon public health in 2002.The Network’s experiencein developing a Norwegian profile (see spotlighton Norway) played an important role in shapingthis paper, which the Storting (parliament)adopted in June 2003. In the future, health will bean obligatory component of municipal develop-ment plans. Government support will be madeavailable to local and regional partnerships thatmake a commitment to long-term, intersectoralmeasures to promote health and prevent disease.This is expected to significantly boost the work ofthe Network and encourage cities to give priorityto health concerns. At the request of the Ministryof Health, the Network will continue to developthe Norwegian profile to support the developmentof the new responsibility for municipal planning.
Networking in the futureThe Network is currently recruiting members. Be-tween two and four cities are expected to join theNetwork in 2003. This will have implications onthe organization and regular activities of the Net-work. If the Network should expand beyond 25members, regional subnetworks are likely to be in-troduced. In the future, the Network also aims topromote closer cooperation between cities by set-ting up work groups on the Network’s priorities(Box 5.22). The main objective of these groups willbe to develop new public health initiatives and rel-evant guidance for cities. The Network will alsostrengthen opportunities for exchange on its website, making information on Network programmesand outcomes available to a wide target group.
Box 5.22. Network priorities in Norway• Nutrition and physical activity• Tobacco and drugs• Safety• Indoor environment• Local Agenda 21
31497_National.p65 06-10-2003, 08:0464
For more information, contact:Richard BrattliNational Network CoordinatorNorwegian Healthy Cities Network
P.O. Box 243, N-8376 LeknesNorwayTel.: +47 76 082184, Fax: +47 76 082006E-mail: [email protected]
Spotlight on Norway
If we want to see results of the work with public health, we must make a joint effort. I will surely do mypart. I believe that the members of the Norwegian Network – the leading municipalities on public health– will be important partners when it is time to put the politics into life in the coming years.Dagfinn Høybråthen, Norwegian Minister for Health(See page 14 for the full text of the statement)
In working with the national authorities, the Network has pointed out the need for an unequivocal na-tional public health policy. The Network has promoted proposals for such a national plan and volun-teered to be a laboratory for trying out new initiatives. We expect to be bestowed such a role in the Gov-ernment’s White Paper on Public Health, due to be presented in January 2004. Thanks to our connectionwith WHO and colleagues in European networks, we expect to be an attractive partner in the nationalpublic health work.Jostein W. Rovik, Mayor of Sandnes (member of the Norwegian Healthy Cities Network)Deputy chair, Norwegian Healthy Cities Network
The Norwegian ProfileThe Norwegian Profile is a population survey onthe state of health and environmental conditionsin the municipalities of the Norwegian HealthyCities Network. Developed in 2000, the Norwe-gian Profile moved away from the traditional ap-proaches, which depend on indicators of mortal-ity and illness. The Profile is based on the popu-lation’s assessment of the state of their ownhealth and the environment.
In each member city, 1200 randomly selectedindividuals aged 15–79 years were sent a ques-tionnaire by post. About half these individuals(9000 total) completed and returned the ques-tionnaire. The estimated cost of the NorwegianProfile 2000 was about EUR 127 000. The mu-nicipalities financed 50% of the survey, and thenational government covered the remainder.
Impact at the local levelThe Norwegian Profile has been important toolfor bridging healthy city and Local Agenda 21work. At the municipal level, the Profile hasfilled an information gap, as there had beenshortage of local data on the well-being of inhab-itants. The Profile also served as a tool for enter-ing into dialogue with inhabitants – one of themost important elements of healthy city and Lo-cal Agenda 21 approaches. The fact that the Pro-file explicitly linked health and environmentaldata provided cities with a stronger basis to dis-cuss comprehensive solutions to local problems.The report has, without doubt, increased the fo-cus on health promotion work in member cities.
The overall findings of the profile have beenused to set the Network’s priorities (Box 5.22).
National partnershipsCarrying out a large scientific project has giventhe Network a professional reputation at the na-tional level and has produced the kind of news-worthy, comparable data the mass media oftendemand. The Ministry of Health, Ministry of theEnvironment and the Association of Local andRegional Authorities supported the project be-cause they consider the Profile an important sup-plement to the existing public statistics. The gov-ernment has shown great interest in the Profileand has invited the Network to present the re-sults at conferences.
International comparisonThe models and questions used in the NorwegianProfile were adapted from surveys carried out inother countries. This not only makes the data in-ternationally comparable but also promotes in-ternational cooperation and exchange. The Net-work considers international cooperation a veryimportant resource. It can result in new ideas andprovide legitimacy to this field of work. The Net-work has therefore invited the other Nordichealthy cities networks to participate in produc-ing a Nordic Health and Environment Profilebased on the Norwegian model. The National In-stitute of Public Health in Denmark will providetechnical support to the joint profile. The surveyis expected to be carried out during 2004–2005.
NORWAY . 65
31497_National.p65 06-10-2003, 08:0465
66 . NATIONAL HEALTHY CITIES NETWORKS
PolandCountry factsPopulation: 38.6 millionUrban population: 65%Population living in network cities: 20%
Network factsAccredited: 2000Established: 1993Members: 45Organization: associationWeb site: http://www.szmp.pl
BackgroundThe number of cities participating in the PolishHealthy Cities Association has increased everyyear since it was established in 1993. Today, 45cities and towns, ranging in population from 5000to 800 000, participate in the network. The mem-bership is diverse, but all these cities and townshave one thing in common – they have made aformal political commitment to work with thehealthy cities approach. The network supports cit-ies in using the approach to determine and act ontheir own needs and priorities.
TrainingThe network attaches great importance to train-ing, as political and staff changes are key factorsinfluencing the progress of healthy cities in Po-land. Training courses are organized for city coor-dinators on evaluation, developing preventionprogrammes, HEALTH21 and the national healthprogramme. The network also provides trainingon issues of national priority. For example, train-ing on the detection of cancer and cardiovasculardisease has been provided for physicians andnurses in network cities, based on scientific re-sources made available by the Medical Academyin Lodz (see spotlight on Poland).
ExchangeAn important function of the network is to trans-late and disseminate foreign-language materials –helping cities to overcome a significant barrier ofaccess to best practices. Cities keep in touch be-tween regular network meetings through a news-letter and the network’s web site. Since 1992, thenetwork has held an annual healthy cities confer-ence, which is open to all cities and professionals
in Poland. The conference is also an opportunityto promote healthy cities at the national level andto demonstrate the network’s potential to respondto national health priorities.
Annual grant competitionsThe network has established a grant competitionas an innovative way to stimulate activities in cit-ies. The network devotes almost 20% of its annualbudget, which is derived from membership fees,to the grant. Member cities consider winning agrant to be a privilege in recognition of a high-quality project. In 2002, 18 cities submitted 65grant applications on the themes of children andyoung people, healthy transport and social exclu-sion. Eight cities received awards: Bielsko-Biala,Inowroclaw, Kalisz, Legnica, Leszno, Lodz, Olsztynand Torun. The theme for the grant competitionin 2003 is healthy environments for children.
Evaluation and impactA survey of 35 of 43 cities undertaken in February2002 highlighted some of the network’s achieve-ments as well as some of the difficulties. The sur-vey included questions related to political sup-port, intersectoral cooperation, programmes andactivities and the position of healthy cities in lo-cal authorities (Box 5.23).Cities reported that the overall benefits of partici-pation in the network included:• increased citizen awareness of health and envi-
ronmental issues;• increased community participation;• easier access to preventive medical examina-
tions; and• better intersectoral cooperation.
31497_National.p65 06-10-2003, 08:0466
Main activitiesThe main activities in cities were the preventionand early detection of cancer; tobacco; addiction;environmental issues; health and environmentaleducation in schools; and campaigns to promotehealthy lifestyles. As a result of their participationin the network, many cities were developing localhealth strategies based on increasing awareness ofhow different sectors affect city life. The cities’links to WHO through the network has been avery strong factor for promoting local health de-velopment.
For more information, contact:Iwona Iwanicka, CoordinatorDepartment of Public HealthPolish Healthy Cities AssociationMunicipal Office of Lodz5 Sienkiewicza St.PL-90 113 LodzTel.: +48 42 6384737Fax: +48 42 6384737E-mail: [email protected]
Spotlight on Poland
Box 5.23. Results of an evaluation of thePolish Healthy Cities Association in 2002• 80% reported stable political support for
healthy city projects• Two thirds of members’ city councils
regularly discuss issues related to healthycities
• 90% involved local communities throughpartnerships with nongovernmentalorganizations
• 80% planned annual healthy city activities• 70% reported on their activities in 2001• 50% had only one staff member assigned
to the healthy city office• 50% involve the private sector in activities,
mainly as a sponsor• 40% implement Local Agenda 21• 30% of coordinators work full time for
healthy city projects• Key problems: limited resources and staffSource: newsletter of the Polish Healthy CitiesAssociation, spring 2002 (Polish)
Research has shown that the broad spectrum of activities implemented in our city have brought a significant in-crease in the citizens’ awareness. As Deputy Mayor, I will definitely continue to promote healthy cities.Zbigniew Fiderewicz, Deputy Mayor of Torun
An integrated and well rounded approach to health-related activities, which embraces the living conditions ofthe population in all aspects, is more effective than work in isolated areas. One of the most effective ways to getthe job done is the WHO Healthy Cities project.Krzysztof Panas, Former Mayor of Lodz
Prevention and early detection of breastcancerFor many years, the early detection and preventionof breast cancer has been a top priority for networkcities in Poland, in accordance with the nationalhealth programme. Research has been carried outon the 21 network cities that implemented breastcancer prevention programmes from 1996 to 2001.Data from a questionnaire provided information onthe effects and cost of these programmes.
Programmes implemented during this period in-cluded organizing screening examinations, activi-ties to popularize regular breast self-examinationand health education for women. Concurrently,training courses were held for health personnel, in-cluding nurses, midwives, primary health care phy-sicians and gynaecologists. The 21 cities involved inthis work covered a total target population of 2.5million women over 18 years of age.
Since 1996, programme activities have reached
456 200 women, of whom 63% were participated ineducational activities connected with training inbreast self-examination and 37% underwent diag-nostic examinations (mammography for womenover 45 years; ultrasonography for women over 35years). In 2001 alone, prevention programmesreached 102 810 women.
In 2001, city budgets provided 90% of the fund-ing, a cost of about EUR 700 000. Local govern-ments in seven cities financed the total cost of theprogrammes, whereas others received external fund-ing from the Ministry of Health, the National Insur-ance Fund, foundations, Project Hope and othersponsors.
Today, the work is continuing and programmesfor the prevention and early detection of breastcancer have become permanent items in city budg-ets. Women’s awareness on the subject has risen,and their participation has demonstrated a socialdemand for these programmes.
POLAND . 67
31497_National.p65 06-10-2003, 08:0467

68 . NATIONAL HEALTHY CITIES NETWORKS
PortugalCountry factsPopulation: 10.4 millionUrban population: 66%Population living in network cities:18%
Network factsAccredited: 2001Established: 1992Members: 11Organization: associationWeb site: http://www.redecidadessaudaveis.com
BackgroundThe Portuguese Healthy Cities Network was for-mally established as a association of municipali-ties in April 1998, subsequent to work started in1992. Today, the Network comprises 11 munici-palities at different stages of development. Somemunicipalities have already implemented cityhealth profiles and city health development plans,whereas others are still in the preliminary phases.Although their levels of experience may differ, allthe municipalities are strongly committed to theprinciples of the WHO health for all policy andthe development of local action to promote eq-uity, health and a high quality of life.
Political leadershipMayors are required to represent their cities in theNetwork’s General Assembly, although they maydelegate this task to a city councillor. The GeneralAssembly elects a president and a political boardto manage the Network and carry out the deci-sions of the assembly. This board of mayors andcity councillors meets once a month. The board issupported by a technical group, which is a forumof healthy city coordinators and other local pro-fessionals involved in healthy city projects. Theydiscuss ideas, share best practices and developjoint activities.
Exchange at all levelsThe exchange and sharing of information be-tween municipalities at all levels is one of the keyaims of the Network. The three municipalities des-ignated to the WHO European Healthy Cities Net-work have played an important role by dissemi-nating European-level healthy cities informationin Portugal. The Portuguese Healthy Cities Net-
work publishes a quarterly, thematic newsletter todisseminate good practice. The newsletter alsoraises awareness about healthy cities outside theNetwork and among the public.
Awards for scientists and journalistsTo further promote urban health locally and na-tionally, the Network has established a journalisticand a scientific recognition award. The awards areconferred in alternate years to honour the best in-vestigative journalism and the best scientific re-search in urban health. The awards are expectedto advance the involvement of the scientific com-munity and the mass media in the work of theNetwork. The first journalistic award in October2002 launched the initiative. The theme for thenext journalistic award will correspond to thetheme for World Health Day in 2003 – healthy en-vironments for children.
A strategic plan for NetworkdevelopmentThe Network has adopted a strategic plan (2003–2005) as a tool for reaching the Network’s goalsfor the future (Box 5.24). The aim of the plan is topromote a working dynamic that will double Net-work membership by 2005 and strengthen part-nerships. The plan places special emphasis onmembership criteria, developing city health pro-files and plans and training. The Network aims tostrengthen its links to other networks of munici-palities as well as with national-level bodies, suchas the National Board of Health and the NationalSchool of Public Health.
The futureThe Network sees great opportunities for growth
31497_National.p65 06-10-2003, 08:0468

in the future. The Network is already a strategicpartner for municipalities and national organiza-tions on issues such as poverty and social exclu-
sion, sustainable development, healthy lifestyles,social support and the needs of vulnerable groupsin society. As the Network grows, it will take sig-nificant steps towards building a municipal asso-ciation with the capacity to influence nationalhealth policies.
For more information, contact:Mirieme FerreiraPortuguese Healthy Cities Network CoordinatorRede Portuguesa de Cidades SaudáveisAv. Dr. Arlindo Vicente no. 68 BTorre da Marinha 2840-403 Seixal, PortugalTel.: +351 21 227 62 01Fax: +351 21 227 62 04E-mail: [email protected]
Box 5.24. Strategic goals of the Network• Support municipalities in meeting healthy
city goals• Double the number of member cities by
2005• Maintain high quality standards through
membership criteria• Strengthen the technical group through
training, debate forums and increasedexchange
• Reinforce national and internationalpartnerships
Spotlight on Portugal
We believe that local governments are a strategic partner in health promotion and sustainable development,due to their contributions to economic growth, social cohesion and environmental protection. We considerthe Portuguese Network to provide added value. It supports gains to health, both locally and nationally,through sustained partnership work.Excerpt of a statement signed by politicians of the General Assembly in May 2002A. Monteiro (Mayor) and C. Almeida Loureiro (City Councillor), SeixalJ. Moreira Raposo (Mayor) and M. João Bual (City Councillor), AmadoraC. Encarnação (Mayor) and Nuno Freitas (City Councillor), CoimbraP. Santana Lopes (Mayor) and H. Lopes Costa (City Councillor), LisboaC. Teixeira (Mayor) and A. Barata (City Councillor), LouresM. Amélia Antunes (Mayor) and P. Marques (City Councillor), MontijoM. Porfírio Vargas (Mayor) and N. Santos (City Councillor), OdivelasT. Zambujo (Mayor) and A. Isabel Beça (City Councillor), OeirasA. Vicente (Mayor) and A. Candeias (City Councillor), PalmelaC. Sousa (Mayor) and D. Machado (City Councillor), SetúbalD. Oliveira Moura (Mayor) and R. Barreto (City Councillor), Viana do Castelo
Healthy Sundays in Viana do CasteloIn 2002, World Health Day was dedicated tophysical exercise with the theme being Move forHealth. As this theme was consistent with thegoals of the city health development plan ofViana do Castelo, it decided to join the com-memorations.
Viana do Castelo decided to involve people ofall ages and physical conditions in an event thatwould draw attention to the health benefits ofexercise. On a Sunday morning, activities wereorganized at the city’s Marina Garden, a widegreen space on the seaside, to suit all tastes.These included football, basketball, volleyball,athletics, gymnastics, walking and cycling. Apath with historical and ecological interest wasavailable to those who chose to walk or cycle.Several local sports associations supported theevent. Caps and T-shirts were distributed, andfruit and water was made available.
The event had been promoted in the local andnational press to give visibility to issues sur-rounding physical exercise and to invite allpopulation groups to participate. About 300people of all age groups participated, includingblind people and other disabled people.
The impact of this World Health Day celebra-tion was so positive that the associations andparticipants involved called for the event to berepeated. Responding to this appeal, the HealthyCity Office decided to organize a Healthy Sun-day every second week from April through Sep-tember 2002. The city further incorporated this6-month activity into the 2003 budget plan.This event has gone beyond fulfilling its objec-tives as a one-off activity – it has acted as an im-portant first step towards fulfilling the widergoals of Viana do Castelo’s city health develop-ment plan on promoting healthy lifestyles.
PORTUGAL . 69
31497_National.p65 06-10-2003, 08:0469

70 . NATIONAL HEALTHY CITIES NETWORKS
Russian FederationCountry factsPopulation: 143.8 millionUrban: 77%
Network factsEstablished: 1996Members: 42 (full members and observers)Organization: AssociationWeb site: http://www.hcp.aha.ru
A Support Centre based at the Institute of PublicHealth and Health Care Management of theSechenov Moscow Medical Academy coordinatesthe Russian Healthy Cities Network. The Ministryof Health approved the Support Centre in 1994 topromote the development of healthy cities in thecountry. The Network was founded a year later(Box 5.25). The Ministry of Health funds the
Box 5.25. Milestones in the developmentof the healthy city movement in theRussian Federation2003• Stupino (Moscow region), Tambov (Tambov re-
gion) and Chesma district (Chelyabinsk region)began to develop healthy city projects.
• The Vologda region developed a regional strate-gic health plan based on HEALTH21.
2002• The Network adopted a new constitution to
meet the standards of the WHO action frame-work for European national healthy cities net-works Annexes 2, 3).
• Smolensk launched a healthy city project witha city forum.
• In Kaliningrad, healthy cities was discussed atthe city and regional level, bringing together 28municipalities in collaboration with the BalticRegion Healthy Cities Office.
• Twenty-five communities of the Kurgan,Samara, Chelyabinsk, Tomsk and Sakhalin re-gions became familiar with the healthy com-munities approach through a programme of theAmerican International Health Alliance.
2001• The Vologda city health profile was prepared
using healthy city indicators (see Spotlight).2000• Izhevsk was designated to the WHO European
Healthy Cities Network.
1999• Cities in the Russian Federation joined the ac-
tivities of the European Sustainable Cities &Towns Campaign.
1998• The Izhevsk city health profile was prepared
and presented to the public.• Ten cities developed a set of healthy city indica-
tors (see Spotlight).• Cities in the Russian Federation participated in
the 1998 International Healthy Cities Confer-ence in Athens.
1997• Cities signed the Charter of European Cities
and Towns towards Sustainability (AalborgCharter) at a sustainable development meetingin Stavropol.
• Seventeen more cities became interested inhealthy city projects.
1996• Six more cities initiated healthy city activities
after the first healthy city meeting in Izhevsk.• The Russian Healthy Cities Network was estab-
lished at a meeting in Dolgoprudny.1995• Healthy City Izhevsk was launched.• The Healthy Cities Support Centre in the Rus-
sian Federation was established.1993–1994• Public health researchers in the Russian Federa-
tion learned about the WHO Healthy Citiesproject and information on the project was dis-seminated to cities
Healthy Cities Support Centre in part. Cities arenot required to pay a fee.
Breaking down barriersAn important function of the Healthy Cities Sup-port Centre has been to make international expe-
31497_National.p65 06-10-2003, 08:0470

rience accessible to cities and regions in the Rus-sian Federation. The Support Centre has translatedseveral documents of the WHO European HealthyCities project into Russian, which are available onthe Network’s web site. The Support Centre facili-tates the exchange of experience in the RussianFederation through conferences, meetings andtraining courses.
A path to integrated local developmentCities in the Russian Federation have shown in-creasing interest in healthy cities. This reflects adesire to improve public health conditions andthe quality of life at the local level through inter-nationally recognized approaches to health andsocial policy. The consistent and coherent ap-proach of the WHO Healthy Cities project hasmade it attractive to cities, which are responsiblefor the implementation of a wide range of pro-grammes. These typically include initiatives onhealth promotion, substance abuse, preventingAIDS, environmental health, Local Agenda 21, ur-ban regeneration and transport. However, coordi-nation between these initiatives is often lacking.Many local professionals lack strategic manage-ment skills. The Network creates a supportive en-vironment for local authorities to learn about andmaster new approaches to developing health,based on a social model of health. Cities are opti-mistic that the healthy cities approach will enablethem to coordinate and integrate all activities forhealth development at the local level.
Healthy cities and regionsGiven the vast size of the Russian Federation, theSupport Centre has placed increasing emphasis on
involving the 89 regions in healthy cities initia-tives. Regional authorities are essential partnersfor municipalities as they develop new strategiesand plans. The involvement of regional authori-ties helps to remove barriers to the local imple-mentation of health for all policies. For example,the Vologda region has recently produced a re-gional strategic health plan based on HEALTH21.Now the administration supports the develop-ment of healthy cities in the region.
The futureThe Healthy Cities Support Centre and the Net-work aim to become a strong organization bring-ing together experts and representatives of Net-work cities with interested national and interna-tional organizations. Future plans for the develop-ment of the Network include the further develop-ment of information resources and trainingcourses for cities. The Network also plans to estab-lish an award for journalists on health develop-ment topics.
For more information, contact:Yuliya E. AbrosimovaSupport Centre for Healthy Cities in the RussianFederationPublic Health Policy DepartmentInstitute of Public Health and HealthCare ManagementSechenov Moscow Medical AcademyMinistry of Health37/1, Zubovskiy Boulevard, Moscow 119021Russian FederationTel.: +7 095 2461959E-mail: [email protected]
RUSSIAN FEDERATION . 71
Spotlight on the Russian FederationHealthy city indicatorsIn 1998, researchers from the Support Centreworked in collaboration with the Network cit-ies to develop a set of indicators for cityhealth and sustainable development.The partners began this work by developing adefinition of a healthy and sustainable city.This resulted in a list of seven characteristicsof a healthy and sustainable city, which de-scribe the broad dimensions of city life.These characteristics were then developedinto a set of 29 qualitative and quantitativeindicators, which would allow specialists, de-
cision-makers and citizens to estimate towhat extent a city complied with these char-acteristics. The indicators were discussed incities, and adjusted according to local cir-cumstances a necessary. Cities now use theindicators to prepare city health profiles andto set targets for health and sustainable de-velopment. The focus on sustainable devel-opment has helped to reinforce a holistic ap-proach to health, while the indicators havehelped to translate sustainable developmentfrom an abstract theory into decisions forconcrete local action.
31497_National.p65 06-10-2003, 08:0471

72 . NATIONAL HEALTHY CITIES NETWORKS
SlovakiaCountry factsPopulation: 5.4 millionUrban population: 57%Population living in network cities: 24%
Network factsAccredited: 2001Established: 1994Members: 14Organization: association/nongovernmentalorganizationWeb site: http://www.changenet.sk/azms
BackgroundThe Association of Healthy Cities of Slovakia wasestablished in 1994. The network supports citiesin achieving the objectives and targets ofHEALTH21 and Agenda 21, with the aim of improv-ing the health and the quality of life of theSlovakian population. The network provides re-sources and training to meet these objectives.
Support and exchangeThe network translates and publishes the mostimportant resource documents of the WHO Euro-pean Healthy Cities Network and those of the Eu-ropean Sustainable Cities & Towns Campaign. Thenetwork further coordinates joint activities, ap-plies for grants and provides training for new co-ordinators. Cities exchange experience at regularmeetings.
Active livingThe network currently has one multi-city actionplan (a thematic work group) on the topic of ac-tive living. Important joint activities of the multi-city action plans include organizing nationalevents such as National Days for Health and Car-free Days.
The Active Living multi-city action plan focuseson changing people’s lifestyles. The activities in-clude reducing negative behaviour (excess drink-ing, smoking and drug abuse). Two local work-shops and conferences were organized in BanskaBystrica. The participation of cities is rather lim-ited because resources are few. Mobility issues andphysical exercise are addressed through Car-freeDay and European Mobility Week events. The net-work cities organize various mobility and traffic-
related activities including promoting cycling,calming traffic and developing cycle and pedes-trian paths.
The most successful event remains the NationalDays for Health – week-long activities dealingwith health status and health check-ups.
Tools for health and sustainabledevelopmentNetwork cities in Slovakia have reached highstandards in terms of implementing structures fortackling challenges in health and sustainable de-velopment. Through grants from internationalfoundations and national agencies, the networkhas developed expertise in working with indica-tors and city health profiles and plans. The net-work has also developed an ecological mappingtool for decision-making. By working with thesetools, the network has gained national and inter-national recognition for its expertise.
Ten cities replicated the work on city healthprofiles; the network had financially supportedthe preparation of the first one. The indicatorsproved to be problematic because the status of cit-ies and districts differed and because data werenot always available. The network has very goodrelations with the national statistical office andaccess to the data needed.
The city health plans were developed followingthe case study from Kosice, a former member of theWHO European Healthy Cities Network. Some cit-ies experienced problems related to political accept-ance; others successfully developed needed partner-ships and issued a high-quality city health plan.
National partnershipsThe network works closely with the Ministry ofHealth and Ministry of Environment. It is a vehi-cle for testing and developing tools for the localimplementation of Agenda 21 and Slovakia’s na-tional environment and health action plan. Forexample, network cities have implemented localenvironment and health action plans into theircity health development plans. This experiencewas used to produce a guidebook, with case stud-ies, on how to prepare local environment andhealth action plans. The network’s coordinatorparticipates in several work groups in both minis-tries, and close ties have been established with theNational Health Promotion Centre.
31497_National.p65 06-10-2003, 08:0472
Healthy city community foundationsNetwork cities are working to overcome fundingproblems by setting up healthy city communityfoundations. This is a result of the positive experi-ence of Banska Bystrica, the first city to establishsuch a foundation in Slovakia. The Healthy CityCommunity Foundation was established in 1994by concerned citizens, the Rotary Club and localcouncillors, with a US$ 30 000 grant from the lo-cal government. This enabled the Foundation toget started and raise further funds. The mission ofa community foundation is to improve the qualityof life within its geographical area by empoweringlocal people to build a better future. Further, thefoundations promote partnerships between gov-ernment, businesses and the nonprofit sector. To-day, the Foundation in Banska Bystrica is the mostsuccessful community foundation in Slovakia.
Looking forwardIn the future, the network aims to strengthen itsorganizational structure and increase its statuswithin Slovakia (Box 5.28) to ensure the stabilityof the network. As Slovakia moves closer to Euro-pean Union membership, the network sees itselfas having a greater role in supporting cities, townsand national bodies in reaching health and sus-tainable development objectives.
For more information, contact:Gejza LegenNational Network and Healthy City CoordinatorAssociation of Healthy Cities of SlovakiaZvonarska 21 SK-040 01 Kosice SlovakiaTel.: +421 55 6252493 Fax: +421 55 6252493E-mail: [email protected] [email protected]
Box 5.28. Future plans of the network• Establish a board of healthy cities mayors to
evaluate, to empower and to lobby forhealthy cities
• Set up a for-profit agency for active lifestyletourism to provide the network withsustainable income
• Strengthen the recently established SlovakAssociation of Public Health – a membershiporganization that lobbies for healthpromotion (especially tobacco tax reform)and facilitate exchange and training
• Improve the participation of member citiesthrough strict adherence to network criteria
• Participate in global, European and nationalagendas
Spotlight on SlovakiaNational Days for HealthDays for Health has been one of the most suc-cessful local projects of the network city ofTrnava. The strong political commitment of thecity mayor, combined with strong support fromthe healthy city steering committee, providedthe energy for this annual event. In 1996, theinitiative was presented as a case study to thewhole network. It has since been accepted asuseful tool for health promotion, capacity-build-ing and raising the visibility of healthy cities.Today, many Slovakian cities organize Days forHealth as part of a national event during thefirst week of June.In past years, the Days of Health have includedactivities in five areas.Health care services and disease prevention activi-ties. This involves health check-ups, includingblood pressure, cholesterol, lung capacity, andother factors.Active lifestyle activities (physical exercise and fit-ness). Various competitions for biking, athletics,swimming, trekking and hiking are organized.Healthy diet and elimination of negative habits (ex-
cess drinking and smoking). Healthy food is pre-sented and advisory meetings (such as how toavoid obesity) are held, often sponsored by localproducers of healthy food.Cultural heritage activities (markets, fairs andshows). In many cities the Days of Health are or-ganized in conjunction with local fairs and mar-kets.Cultural events. Music and dance events oftencontribute to other areas such as active living.Successful Days for Health activities include:• a committed and enthusiastic healthy city co-
ordinator with good management skills;• strong political commitment and personal
participation of the mayor (opening, speechesetc.);
• very active participation of local partners attheir own expense;
• good marketing tools for the general public,schools and nongovernmental organizations;and
• planned financial resources in the annual citybudget.
SLOVAKIA . 73
31497_National.p65 06-10-2003, 08:0473

74 . NATIONAL HEALTHY CITIES NETWORKS
SloveniaCountry factsPopulation: 2.0 millionUrban population: 50%Population living in network cities: 65%
Network factsEstablished: 1992Members: 23 (8 full members; 15 associatedmembers)Organization: associationWeb site: http://www.zzv-mb.si
BackgroundThe Slovenian Healthy Cities Network was for-mally launched in 1992 by seven cities, buildingon initiatives that had begun in 1989. Today theNetwork is a nationally recognized policy actor indeveloping urban health. The Healthy City Cen-tre, a support centre within the Regional Instituteof Public Health in Maribor, coordinates the Net-work. As of February 2003, the Ministry of Healthfunds the Network’s activities. Cities co-financelocal work. At the end of the Network’s thirdphase (1998–2002), a membership fee was intro-duced. Previously, the City of Maribor and theMinistry of Health had funded the Network.
A standard of excellenceThe Network has achieved a standard of excel-lence by requiring its full members to fulfil a strictset of criteria, similar to the WHO criteria formembers of the WHO European Healthy CitiesNetwork in the third phase. Full members are re-quired to develop and implement city health pro-files and city health development plans, which fo-cus on links between health, social and environ-mental factors. The Network is not, however, anexclusive club. All cities are welcome to join as as-sociate members. This gives cities time to accesssupport to establish the new infrastructure andpolicy approaches needed to meet the Network’scriteria.
Maintaining political commitmentThe Network follows the phases of the WHO Euro-pean Healthy Cities Network, which also coincidewith local election years. At the start of each newphase, the Network holds a General Assembly at-tended by mayors. Each mayor signs a political
declaration in support of the new phase. This dec-laration, which is co-signed by the Minister forHealth, functions as an obligation. The event itselfusually attracts a lot of mass media attention, rais-ing public awareness of healthy cities.
National partnershipsThe Network has maintained steady cooperationwith the Ministry of Health, the Department ofPublic Health of the Faculty of Medicine of theUniversity of Ljubljana, the National Institute forPublic Health and regional institutes of publichealth. In collaboration with these partners, theNetwork will co-found a number of strategic or-ganizations in 2003. These include a school ofpublic health, a foundation to support commonNetwork activities and a WHO Collaborating Cen-tre on Urban Health and Healthy Cities. The Col-laborating Centre will support countries in south-eastern Europe. The Network also cooperates withnational partners and the mass media to organizeWorld Health Day, World No-Tobacco Day, EarthDay, Day of Dance, Disabled Day and World AIDSDay events.
Working with regionsThe government has chosen Healthy City Mariborto coordinate the health and social aspects of theRegional Development Plan of Podravje (2003–2007). The work will also be supported by the Net-work, the corresponding regional institute of pub-lic health and the National Institute of PublicHealth. The results will be disseminated to citiesthrough the Network and used as a basis for thehealth component of regional development plansin the country’s other six regions.
Sustainable development and LocalAgenda 21An important role of the Network is facilitatingsustainable development. The Network hasbrought expertise and resources to Slovenian citiesthrough close cooperation with the European Sus-tainable Cities & Towns Campaign. The Networkis a signatory to the Charter of European Citiesand Towns towards Sustainability (Aalborg Char-ter). From 1999 to 2001, Healthy City Maribor pi-loted a Local Agenda 21 plan for Maribor – thefirst of its kind in the country. The work was sig-nificant for raising awareness among citizens ofhealth and environmental problems in the city.
31497_National.p65 06-10-2003, 08:0474
Maribor is now supporting other cities to imple-ment their own plans. Network cities will be en-couraged to implement Local Agenda 21 plans inthe Network’s fourth phase (2003–2007).
EvaluationThe Network regularly evaluates its activities. TheDepartment of Public Health of the Faculty ofMedicine of the University of Ljubljana carries outan annual external evaluation. The results are pre-sented in the Network’s annual reports, which aresent to the National Institute of Public Health andthe Ministry of Health. Full members of the Net-work produce an annual report, which is pre-sented to the board of the Network as well as tolocal steering committees. The most recent evalua-tion of the Network (2002) yielded conclusionsthat now guide the Network’s criteria and futureplans as described in this profile.
WHO Healthy Cities LibraryOne of the most important functions of the Net-work is the development and maintenance of in-formation on urban health. The Network’s WHOHealthy Cities Library includes WHO literature onhealth and the environment, a number of transla-tions of WHO Healthy Cities publications, na-tional Network publications and city publications.Altogether, the library brings together about 1550titles, representing an important knowledge baseon urban health, health promotion, Local Agenda21 and sustainable development in communities.The WHO Healthy Cities Library is located at the
Healthy City Centre in Maribor and is regularlyused by Network members, municipal administra-tors, researchers, students and other interested in-dividuals. Those unable to visit the library may re-quest photocopies. Basic information is availableon the Network’s web site. The Network alsomaintains a database with information onSlovenian Network cities and WHO European Net-work cities.
For more information, contact:Igor KrampacNational Network and Healthy City CoordinatorInstitute of Public Health MariborHealthy City CentrePrvomajska 1, SLO-2000 Maribor, SloveniaTel.: +386 2 460 02 317, Fax: +386 2 46 22 234E-mail: [email protected]
Spotlight on Slovenia
Box 5.29. Network priorities in Slovenia,2003–2007• Activities to reduce alcohol and tobacco
consumption• Mental health• Preventing injury• Nutrition and physical activity• Safe sex education• Social inequality• Education and training
As Mayor of the University City of Maribor and as President of the Maribor Healthy City Steering Committee, Ican express my delight upon the success of Maribor Healthy City and the Slovenian Healthy Cities Network. Infuture, Maribor intends to prepare short-, medium- and long-term integrated health development plans on aregular basis. The City Council will evaluate the content with regard to the financial possibilities for its imple-mentation. The foreseen fields of cooperation in the fourth phase (2003–2007) with the Slovenian HealthyCities Network will take further the active and fruitful connection with other Slovenian healthy cities and withthe worldwide healthy city family.Boris Sovic, Mayor of Maribor, Slovenia
Rolling out national policyAs of February 2003, healthy cities became a na-tional programme and the accepted model forthe development of urban health in Slovenia.Healthy cities is included in the National PublicHealth Plan 2003–2008 in the chapter on urbanhealth. This chapter is based on proposals theNetwork provided to the Ministry of Healththrough a formal consultation process. The Net-
work will be responsible for organizing the im-plementation of this urban health strategy, withexpert support from the National Institute ofPublic Health. The Network’s priorities are there-fore linked to this responsibility (Box 5.29). TheMinistry of Health will fund national and inter-national healthy city programmes, although cit-ies will co-finance the local action.
SLOVENIA . 75
31497_National.p65 06-10-2003, 08:0475

76 . NATIONAL HEALTHY CITIES NETWORKS
SpainCountry factsPopulation: 39.9 millionUrban: 78%Population living in network cities: 33%
Network factsAccredited: 2002Established: 1988Members: 62Organization: Spanish Federation of MunicipalitiesWeb site: http://www.femp.es/recs
Objectives of the NetworkThe objective of the Network are:• to promote the exchange of experience;• to promote intermunicipal collaboration in the
field of health and sustainability;• to serve as a focal point for the quality of
healthy city work;• to generate common indicators and other key
tools that make intersectoral collaboration pos-sible; and
• to strengthen partnerships between the SpanishHealthy Cities Network and WHO, interna-tional institutions and regional and nationaladministrations.
Regional networkingThe Network has also has a number of active re-gional networks, including Andalucía, Castilla-LaMancha, Cataluña and one metropolitan networkin Madrid. These networks grew from a strong in-terest in healthy cities in the late 1980s and in re-sponse to the structure of government in Spain,which is divided into 17 autonomous regions. Re-gional networks have provided a forum to discusscommon public health problems and training andto organize joint activities. Over time, however,regional networks have come to have activitiesand objectives that differ from those of the na-tional Network, based on the unique needs of thepopulations in their regions. In addition, somecities that were members of regional networkswere not members of the national Network. Totackle this situation, the Network is making agree-ments with the regional networks. This partner-ship includes a feature that makes member citiesof a regional network members of the Network.
BackgroundSpain has one of the oldest national networks ofhealthy cities in Europe. Healthy cities was firstintroduced to Spain in 1986 at a meeting arrangedby WHO, the Ministry of Health and ConsumerAffairs and the Spanish Federation of Municipali-ties and Provinces. In 1988 the Spanish HealthyCities Network was formally established. The Net-work is a section within the Task Force on HealthIssues of the Spanish Federation of Municipalitiesand Provinces. The Network’s permanent objec-tive is to establish, maintain and adapt the WHOHealthy Cities project in Spain. The Network en-courages and supports cities through research,training, meetings and congresses and throughthe development and maintenance of a web siteand information tools.
Membership and criteriaCities may join the Spanish Healthy Cities Net-work as full or associate members. The criteria formember cities of the Network include:• a political commitment to the principles of
health for all and the Ottawa Charter for HealthPromotion;
• a commitment to produce a city health profileand city health plan;
• the appointment of a political and technicalrepresentative to the Network; and
• acceptance of the Network’s guidelines.A number of institutions have been appointed asassociate members by the Network’s Assembly ofCities. These include the Ministry of Health andConsumer Affairs, regional healthy cities networksand other institutions and organizations dealingwith promoting and protecting health.
31497_National.p65 06-10-2003, 08:0476
These partnerships also create common prioritiesand objectives for all members of a network inSpain. This unification of actions and prioritieswill create a solid group of cities for whichprogress can be monitored on key objectives suchas health planning and community participation.
Common priorities and action areasThe key priorities for the Network are equity, so-cial development and sustainability. The Networkaddresses a broad range of issues related to envi-ronment and health (air and water quality), thebuilt environment, transport, energy and ecology.The Network also strongly emphasizes monitor-ing, evaluation and networking. Regular activitiesof the Network include:• promoting, rebuilding and strengthening the
municipal agreement with healthy citiesthrough council-oriented campaigns;
• encouraging communication, collaborationand exchange of information between cities;
• encouraging and promoting the use of commu-nication technology (e-mail and web site) as ameans of direct communication between cities;
• maintaining an up-to-date documentary data-base;
• promoting interinstitutional partnerships topromote intersectoral action;
• stimulating and encouraging the establishmentof collaboration centres of the Network for thedevelopment of university studies and trainingand research on urban health and sustainabledevelopment;
• supporting member cities in developing healthprofiles and plans;
• developing indicators and evaluation criteria;• conducting public relations and mass media ac-
tivities; and
• developing partnerships with other nationalhealthy cities networks in Europe.
Partnerships and cooperationThe Network already collaborates strongly withthe Ministry of Health and Consumer Affairs. TheNetwork has an agreement with the Ministry:• to produce guidelines for indicators, health pro-
files and health plans for various populationgroups;
• to work on a statistical system for public health;• to establish methods for the evaluation of pub-
lic health programmes;• to develop a web site as a tool for sharing infor-
mation, training, consultation, etc.;• to hold workshops and conferences; and• to translate documents of interest for the devel-
opment of healthy cities in the country.The Network plans to strengthen its partnershipwith the Ministry in the future and has identifieda number of networks, nongovernmental organi-zations, universities and private foundations withwhich it plans to build partnerships.
For further information, contact:Miguel Ángel Bonet GranizoDirector of Area, Spanish Federation of Munici-palities and Provinces (FEMP)Secretary of Section, Spanish Federation of Mu-nicipalities and Provinces, Spanish Healthy CitiesNetwork (RECS)C/ Nuncio 8E-28005 MadridSpainTel.: +34 91 3643700Fax: +34 91 3655482E-mail: [email protected]
SPAIN . 77
31497_National.p65 06-10-2003, 08:0477

78 . NATIONAL HEALTHY CITIES NETWORKS
SwedenCountry factsPopulation: 9.0 millionUrban population: 84%
National healthy cities networking in Sweden isbeing reorganized following an active history ofpublic health networking. A National Network forLocal Public Health Work was established in 1994.The cities of Gothenburg and Stockholm initiatedthe Network to fulfil a criterion for membership ofthe WHO European Healthy Cities Network. Itquickly developed into a major network, involv-ing all Sweden’s regions and counties and onethird of the municipalities. This is the Networkthat has regularly represented healthy cities inSweden. The Network received financial and tech-nical support from the National Institute of PublicHealth. Municipalities made in-kind contribu-tions. It was highly committed to the goals ofhealth for all.
Three parallel networksIn 1995, the National Institute of Public Healthtook the initiative to establish two smaller butclosely associated networks (Fig. 5.1) for large andmedium-sized cities. The Institute aimed to sup-port local public health work and to guarantee aforum for discussion between the national and lo-cal levels. The Institute and municipalities agreedon the aims of these two networks.
A new structure for healthy citiesThe networks were re-established as a PublicHealth Forum in 2001. The Forum is open to allauthorities and organizations active in the field ofpublic health. It is jointly coordinated by the Na-tional Institute of Public Health, the Swedish As-sociation of Local Authorities and the Federationof Swedish County Councils. A separate nationalhealthy cities network will be established during2003. This is in response to an external evaluationcarried out in 2003, which concluded that mem-bers of the network were too loosely associated.The new network will have a set of common goalsand structures based on WHO criteria for nationalnetworks.
Future work – a focus on equity inhealthThe future network members will support the im-plementation of a new government policy calledHealth on Equal Terms – National Goals for PublicHealth. It has one primary goal: the creation of so-cial conditions to ensure good health on equalterms for the entire population. The policy willform the basis for healthy city work in Sweden.
Sustainable welfare developmentFour large cities have formed Partners for Sustain-able Welfare Development, a network that bringstogether municipal councils, municipal housingcompanies, the National Department of Integra-tion, the Swedish Association of Local Authoritiesand the National Institute of Public Health. Thepartnership addresses issues of democracy, envi-ronment, public health, integration and townplanning in local residential areas. The networkpartners have initiated a research study in collabo-ration with Örebro University to evaluate localhousing projects from a healthy city perspective.This network will be closely linked to the nationalhealthy cities network.
Exchange and field visitsMeetings, seminars, conferences, newsletters andspecial training have formed an important basis ofexchange for Sweden’s public health networks.These networking activities have stimulated alearning process in cities, which has given rise tolong-term strategies rather than short-termprojects. The field visit is an important feature ofSweden’s networks. The aim of a field visit is tostudy local public health methods and strategies.Field visits have involved a range of professionalsfrom preschool teachers and school nurses to rec-reation leaders and environmentalists. About 180people have been involved in field visits, whichare well documented in newsletters and reports.
For more information, contact:Elisabeth BengtssonHealthy City Project CoordinatorCity of HelsingborgCity HallS-251 89 HelsingborgSwedenTel.: +46 42 104911Fax: +46 42 106844E-mail: [email protected]
31497_National.p65 06-10-2003, 08:0478
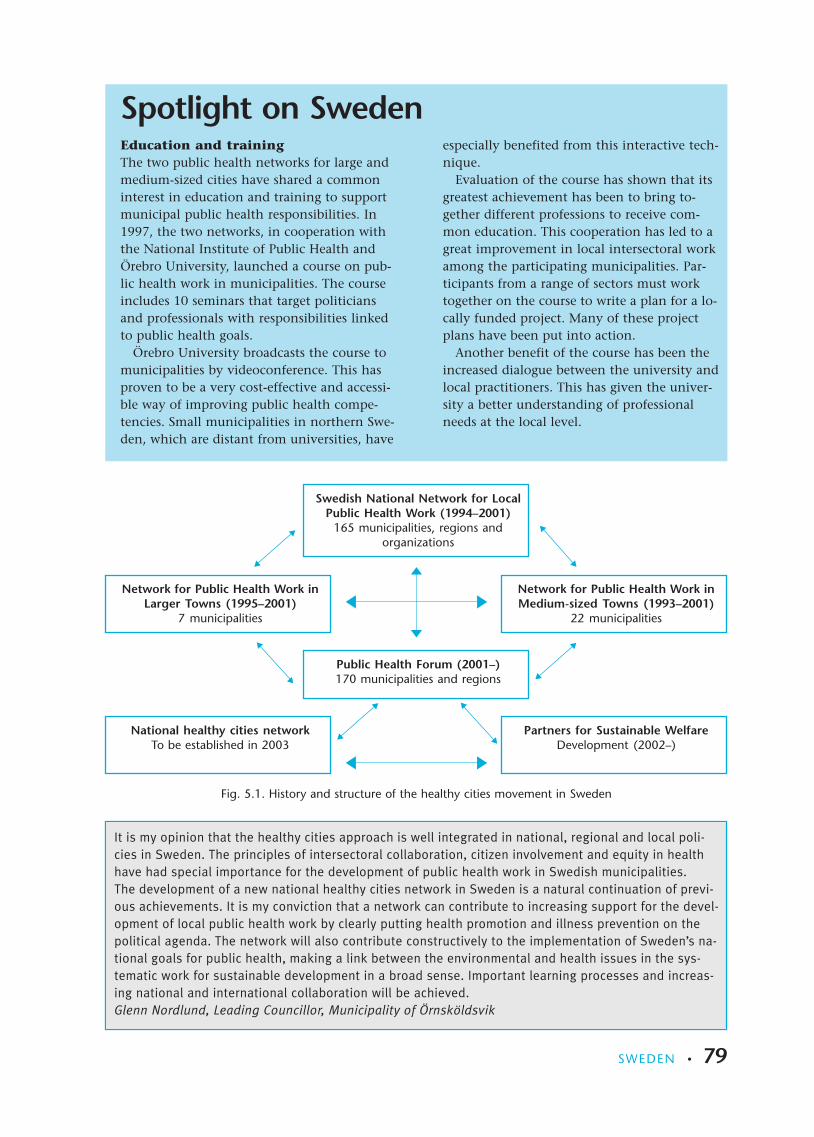
Spotlight on Sweden
It is my opinion that the healthy cities approach is well integrated in national, regional and local poli-cies in Sweden. The principles of intersectoral collaboration, citizen involvement and equity in healthhave had special importance for the development of public health work in Swedish municipalities.The development of a new national healthy cities network in Sweden is a natural continuation of previ-ous achievements. It is my conviction that a network can contribute to increasing support for the devel-opment of local public health work by clearly putting health promotion and illness prevention on thepolitical agenda. The network will also contribute constructively to the implementation of Sweden’s na-tional goals for public health, making a link between the environmental and health issues in the sys-tematic work for sustainable development in a broad sense. Important learning processes and increas-ing national and international collaboration will be achieved.Glenn Nordlund, Leading Councillor, Municipality of Örnsköldsvik
Education and trainingThe two public health networks for large andmedium-sized cities have shared a commoninterest in education and training to supportmunicipal public health responsibilities. In1997, the two networks, in cooperation withthe National Institute of Public Health andÖrebro University, launched a course on pub-lic health work in municipalities. The courseincludes 10 seminars that target politiciansand professionals with responsibilities linkedto public health goals.
Örebro University broadcasts the course tomunicipalities by videoconference. This hasproven to be a very cost-effective and accessi-ble way of improving public health compe-tencies. Small municipalities in northern Swe-den, which are distant from universities, have
especially benefited from this interactive tech-nique.
Evaluation of the course has shown that itsgreatest achievement has been to bring to-gether different professions to receive com-mon education. This cooperation has led to agreat improvement in local intersectoral workamong the participating municipalities. Par-ticipants from a range of sectors must worktogether on the course to write a plan for a lo-cally funded project. Many of these projectplans have been put into action.
Another benefit of the course has been theincreased dialogue between the university andlocal practitioners. This has given the univer-sity a better understanding of professionalneeds at the local level.
Fig. 5.1. History and structure of the healthy cities movement in Sweden
Network for Public Health Work inLarger Towns (1995–2001)
7 municipalities
National healthy cities networkTo be established in 2003
[reverse order]
Swedish National Network for LocalPublic Health Work (1994–2001)
165 municipalities, regions andorganizations
Network for Public Health Work inMedium-sized Towns (1993–2001)
22 municipalities
Public Health Forum (2001–)170 municipalities and regions
Partners for Sustainable WelfareDevelopment (2002–)
SWEDEN . 79
31497_National.p65 06-10-2003, 08:0479

80 . NATIONAL HEALTHY CITIES NETWORKS
TurkeyCountry factsPopulation: 67.8 millionUrban population: 65%Population living in network cities: 24%
Network factsEstablished: 1993Members: 23Organization: coordinated by the Ministry ofHealth
The Ministry of Health introduced the healthy cit-ies initiative in Turkey in 1993. The Ministry coor-dinates, advises and facilitates the Network. Mu-nicipalities participate in the Network on a volun-tary basis. Cities in the Network are encouraged toestablish healthy city infrastructures as recom-mended by WHO. The Network itself does nothave governing bodies or technical committees.The main role of the Network is to facilitate thelocal implementation of national health policiesand to put healthy cities concepts at the top ofmunicipal agendas. As the Ministry of Health isresponsible for the country’s health policies andservices, healthy cities is well placed to do this.
Facilitating exchangeThe Ministry of Health has organized a number ofmeetings since 1993 to bring together local gov-ernment professionals from a range of sectors. By2000, 21 municipalities reported that they hadadopted healthy cities and Local Agenda 21 poli-cies, and Bursa became the first city in Turkey tobe designated as part of the WHO EuropeanHealthy Cities Network. In 2001, the Ministry ofHealth responded to increasing interest in healthycities by organizing a meeting on the WHOHealthy Cities project that included sharing expe-riences and evaluation. The cities of Bursa andTepesi shared their experiences of the benefits ofhealthy cities and the process of WHO designa-tion. Several cities joined the national Network asa result of this meeting.
Disseminating informationThe Network has produced a number of docu-ments to support the dissemination of healthy cit-ies principles. The Network translated five docu-ments of the WHO European Healthy Cities
project (Box 5.30) to support a training event heldin 2000. The following year, the Network pro-duced a handbook on the Network for cities. Thisbook introduces the concept of healthy cities, de-scribes local activities and outlines targets for thefuture (Box 5.31). Today, five cities have been des-ignated to the WHO European Healthy Cities Net-work.
Box 5.30. Key documents of the WHOEuropean Healthy Cities projectavailable in Turkish• Twenty steps for developing a Healthy Cities
project• Athens Declaration for Healthy Cities• Revised baseline Healthy Cities indicators• City health profiles – how to report on health
in your city• City health planning: the framework• The solid facts: social determinants of health
World Health Day 2002The theme of World Health Day 2002 was Movefor Health. The day was devoted to promotingphysical activity as a means of transport. This in-volved encouraging a habit of physical activityamong people of all ages by breaking down barri-ers to walking and cycling. All members of theNetwork carried out activities in their cities. WHOpresented the Network Coordinator with a certifi-cate, marking the Network’s success.
Healthy environmentsHealthy City activities are a key part of the gov-ernment’s national environment and health ac-tion plan, adopted in January 2001. Two targets
31497_National.p65 06-10-2003, 08:0480

have been set for healthy cities under a section re-lated to healthy settings (Box 5.31). Network citieswill be encouraged to promote healthy environ-ments in a range of settings, including schools,workplaces and homes. The Network will supportcities through training and capacity-building.
PartnershipsThe Network encourages cities to establish localhealth platforms, which bring together key deci-sion-makers who can ensure financial support toprojects and clear lines of responsibility. Healthplatforms typically comprise politicians, directorsof departments and representatives of professionalassociations and universities. The partners vary ac-cording to the agenda. For example, a universityfaculty of medicine may become involved in aproject related to a health profile, whereas theChamber of Architects and Urban Planners wouldjoin a partnership related to urban developmentand services. The Network encourages governors(the heads of provincial state administration), pro-vincial health directorates and other relevant bod-ies to support healthy cities activities.
For more information, contact:Emine Didem EvciHeadProject Coordination UnitGeneral Directorate of Primary Health CareMinistry of HealthTR-Sihhiye, AnkaraTurkeyTel.: +90 312 4356440/1219Fax: +90 312 4350992E-mail: [email protected]
Box 5.31. Plans and strategies forhealthy cities in TurkeyTargets and strategies for healthy citiescorrespond to HEALTH21 and nationalstrategies
Main targetBy 2020, everyone should live in a healthierenvironment at school, in workplaces, athome and everywhere people live.SubtargetBy 2015, 50% of cities should have joined theTurkish Healthy Cities Network.
StrategiesNational regulations should be in accordancewith the principles of healthy cities. WHOcity health indicators, profiles and plans mustbe used as reference for city regulations.Healthy city concepts and subjects should beincluded in the university curriculum.
It is pleasing to realize that our main promise “Liveable Bursa for all, equity in all” coincides, in all as-pects, with the WHO Healthy Cities project.We had promised to improve the living conditions of the people of Bursa to such a point that peoplewould feel satisfied. We emphasized a wish to increase the living standards to an extent where onewould be happy to live in Bursa and be proud of being a Bursa citizen. In other words, we had promisedthem a healthy city in which to live.We had a model to lead us to our goals, which was based on the good communication, common under-standing and creating synergies for solutions. But when we took a closer look at the methods of theWHO Healthy Cities project, we found out that they were quite similar, adaptable and efficiently applica-ble to our planning to enhance equity in living conditions and equity in health.We sincerely believe that one should be able to live in an environment that complies with a person’sphysical, social, psychological, economic and cultural needs and capacities. Governments and local au-thorities should therefore maintain these conditions at the required level by addressing inequities inhealth for the happiness of the citizens.The WHO Healthy Cities project provides Bursa with a very good opportunity to make use of the experi-ences of the member cities. Of course these experiences will reduce the risk of unsuitable applicationsand save us from losing time.I am sure that, in the fourth phase of the WHO European Healthy Cities Network, our city of Bursa willtry its best in exchanging remarkable experiments with other healthy cities.
Erdogan Bilenser, Lord MayorMetropolitan City of Bursa, Turkey
TURKEY . 81
31497_National.p65 06-10-2003, 08:0481
82 . NATIONAL HEALTHY CITIES NETWORKS
UkraineCountry factsPopulation: 48.4 millionUrban population: 67%Population living in network cities: 3%
Network factsAccredited: 2001Established: 1994Members: 5Organization: statutory organizationWeb site: http://www.uiph.kiev.ua
BackgroundThe initiative to develop the Ukrainian HealthyCities Network stemmed from an internationalconference held in 1994 in Slavutych. Followingthis event, the Ministry of Health set up the Na-tional Healthy Cities Coordination Councilwithin the Ukrainian Institute of Public Health.The Council manages the network and has 15members, which includes representatives of theMinistry of Health, Ministry of Energy, Institute ofPublic Health, Academy of Medical Sciences, Na-tional University, Mayor of the City of Slavutychand Head of the Public Health Commission of theCity of Uzhgorod.
Political commitmentThe Network requires its members to demonstratestrong political commitment to implementing thehealthy cities approach. The Network’s charter isbased on WHO’s health for all policy and on na-tional programmes. For a city to join the Network,the mayor must sign a political declaration andthe city council must pass a resolution in supportof membership and the city health plan. The citymust also designate a councillor to be politicallyresponsible for the healthy city project.
Health passportOne of the most important achievements of theNetwork has been the development of a healthycity demonstration model in Slavutych. This in-volved developing a system for collecting andanalysing health data based on a broad and posi-tive definition of health. A computer programcalled Health Passport was developed to incorpo-rate data on lifestyle factors and social well-being.The program’s database has been developed based
on data collected at annual dispensary examina-tions. The program provides a flexible system formonitoring and analysing the health of groups(according to age, gender, socioeconomic status orother parameters) and the overall population. InSlavutych, data from Health Passport were used todevelop a city health plan that gave priority toprimary health care, healthy lifestyles, health in-surance and involving the public in city manage-ment.
Healthy settingsThe Network sees great opportunities for membercities to improve health in all areas of social life,especially in schools, homes and workplaces. Sev-eral cities have begun to work with the EuropeanNetwork of Health Promoting Schools, and thereare plans to implement a project on healthyworkplaces.
Community participationThe Network encourages cities to actively involvethe public in developing city health developmentplans and programmes to improve health. Diverseactivities have been carried out to gain publictrust and to involve local people. For example,public organizations have been established inSlavutych to involve youth and children in thehealthy city project. These include the Youth Cen-tre for Democracy and Solidarity, a centre for eco-logical education called Istochnik and a club formothers and children called Green Sprout. Thecity of Uzhgorod regularly organizes seminars andtraining on ecological improvement for public or-ganizations that participate in the healthy cityprogramme.
31497_National.p65 06-10-2003, 08:0482

For more information, contact:Victor PonomarenkoDirectorUkrainian Institute of Public Health5, Dymytrova Str, Building 10-A, 7th floor01601 Kiev, UkraineTel.: +380 44 2168151, Fax: +380 44 2167100E-mail: [email protected]
Spotlight on Ukraine
The WHO Healthy Cities project proposes a new vision of city development for the improvement ofhealth and well-being of the population. The city plays an extremely important role in health provisionand in the survival of the population. The participation of Ukraine in the WHO Healthy Cities projecthelped us to realize that it was impossible to solve the problem of health development within theframework of a purely medical approach. It is necessary to involve different structures of the govern-ment and the population in this activity. The government has adopted a complex intersectoral pro-gramme, Health of the Nation for 2002–2011, based on the WHO health for all strategy, which includesstrategic trends of the WHO Healthy Cities project development. Nearly 30 ministries and departmentsin Ukraine are involved in this programme.Great perspectives for the development of cities participating in the programme lie in its approach,which aims to create health-strengthening possibilities in all areas of social activities, especially inschools, workplaces, residences and among families. The international WHO Health Promoting Schoolsproject is being implemented in a number of cities. Healthy cities will implement the project Health atthe Workplace.The aims of the programme will ultimately be made possible by joining efforts with the United Nationssustainable development programme. At present an agreement has been achieved for a partnership be-tween the WHO Healthy Cities project and the Ukrainian Association of Cities. In this perspective, ahealthy city could become a prototype for a “sociopolis” – a city that advances the evolution of humansettlements.
Olga O. Bobylyova, First State Secretary Deputy, Ministry of Health, Ukraine
Healthy cities as a national goalIn 2002, the Government of Ukraine adoptedan intersectoral programme, Health of the Na-tion for 2002–2011, which is based on theWHO health for all strategy, HEALTH21. In par-ticular, the plan includes projects related toWHO programmes on Healthy Cities, the Eu-ropean Network of Health Promoting Schoolsand Tobacco-free Europe.Health of the Nation includes a number ofcity and district-level plans for the local im-plementation of health for all based on theexperience of the Network. For example, itdraws on the Programme on Social and Eco-nomic Development in the City of Uzhgorodby 2010 (1999) and the Concept on the Sus-tainable Development of Zakarpattya (2002).
The further development of urban health inUkraine is a separate task of the Health of theNation programme. The following main prin-ciples of the healthy city project have beenadopted within the national programme:• an increased role for local authorities in
public health;• policy support for health for all at the city
level;• intersectoral action; and• an increased role for the public in creating
conditions to preserve and improvehealth.
Nearly 30 ministries and departments inUkraine are involved in this national healthprogramme.
UKRAINE . 83
31497_National.p65 06-10-2003, 08:0483
84 . NATIONAL HEALTHY CITIES NETWORKS
United KingdomCountry factsPopulation: 58.8 millionUrban population: 89%Population living in network cities: 14%
Network factsAccredited: 2002Established: 1987Members: 92 (208 including the individuals and organizations in member partnerships)Organization: charitable companyWeb site: http://independent.livjm.ac.uk/healthforall
BackgroundThe United Kingdom does not have a networkthat exclusively supports healthy city projects.This role is assumed by the Health for All Network(UK). It started as an informal network of local au-thorities in 1987; today it involves a much widerrange of members. Membership is open to cities,towns and regions that have adopted the healthycities and health for all philosophy and is alsoopen to other organizations and individuals thatsupport these ideals. Members include representa-tives of cities and towns, national and local-levelcommunity and voluntary organizations, healthservice organizations, academic institutions andothers. They bring a rich range of perspectives onhealth issues, as well as differing expectations, tothe Network. The ability to respond to the needsof a wide range of members has been one of theNetwork’s key accomplishments.
Supporting mainstream policyIn recent years, approaches based on healthy citiesand health for all have become mainstreamed ingovernment policy. Community involvement andpartnership working are key requirements ofmany government programmes, and reducing in-equalities is a stated aim of the government. TheNetwork provides support for its members to in-fluence and deliver a range of government policiesthrough:• national and regional conferences and training
events;• briefing papers on government policy and
plans;• coordinated responses to government consulta-
tions;
• such projects as Hub and Spokespeople, whichhelp people to influence the policies and serv-ices that affect their health;
• publications and resources on health for all,healthy cities and community development;and
• developmental work, including a project thataims to work with local communities to de-velop indicators of health inequality that aremeaningful to them.
Network briefing papersThe Network’s briefing papers summarize govern-ment policy initiatives, outlining the implicationsfor local health for all projects. The Briefing Pa-pers are also used to invite members to participatein joint Network responses to government consul-tations. The Network has published Briefing Pa-pers on the following subjects:• the Children’s Fund• food in schools• health impact assessment• human rights• local strategic partnerships• public health networks• race relations• improvement, expansion and reform – priori-
ties and planning framework 2003–2006• public and patient involvement in health
National recognitionNational players increasingly recognize the Net-work. A Network representative has joined a teamwithin the Home Office Active CommunitiesUnit, which will develop a national strategy forthe voluntary sector. The Commission for Patient
31497_National.p65 06-10-2003, 08:0484

and Public Involvement in Health, an independ-ent national body set up by the government, willuse the structure of the Network to inform the de-velopment of the networks it intends to set up.The annual conference of the Network has be-come an important event on the national scenefor those involved in health policy and practice.
Spotlight on the United Kingdom
The added value of the Network is international recognition of the work locally, better understanding ofthe health agenda, improved European links [and providing] a focus to tackle inequalities.
Barry StockleyEx-Leader of the City CouncilStoke-on-Trent
For more information, contact:Jennie ChapmanNational CoordinatorHealth for All NetworkNew Century House52–56 Tithebarn StreetLiverpool L2 2SRUnited KingdomTel.: +44 151 2314283E-mail: [email protected]
The Health Voice NetworkThe Health Voice Network is one of the coreprojects developed by the Health for All Net-work (UK). It is an Internet-based, self-helpnetwork. Membership of the Health VoiceNetwork is free and open to anyone whowants to help people to have more of a say inplanning and improving services that affecttheir health. Launched in March 2002, over950 health service and local council staff,community groups and individual membersof the public are using the Network to exploreways of coming together to put the healthback into health services.The key idea behind the Network is that com-munication between a wide range of peoplecan benefit all. Just knowing that you are notalone can give you encouragement. Peoplecan also benefit from sharing experiences,ideas and information. It might be informa-tion about methods, campaigns or initiativesor about training or funding resources. TheNetwork enables members to get in touchwith other staff, service users and support or-ganizations quickly and easily.The web site (http://www.healthvoice-uk.net)allows members to:• post information;
• search for others with similar interests;• participate in discussions on a variety of
topics; and• provide input into government policy and
national decisions.Members who are not online can access allthe facilities by phone or by post. Everyonereceives a newsletter each month with detailsof what is going on across the country –events, campaigns, useful books and articles,tips and hints.What members say about the Health VoiceNetwork:“I can only write in [amazed] admiration forthe volume (and precision) of the [informa-tion] I’ve had from you (and directly) as a re-sult of your mailing list.”Worker for a national community development or-ganization, January 2003“... probably the best site of its kind around”Voluntary worker, December 2002.“The response from the list has been excel-lent, and rather better than any other singlecontact I have made during this research.There seems to be a lot of enthusiasm outthere.”Worker for a national community development or-ganization, November 2002
UNITED KINGDOM . 85
31497_National.p65 06-10-2003, 08:0485
86 . NATIONAL HEALTHY CITIES NETWORKS
Annex 1
Resources on healthy citiesSee http://www.euro.who.int/healthy-cities for other online resources.
Getting started on healthy citiesTwenty steps for developing a healthy cities project.3rd ed. Copenhagen, WHO Regional Office forEurope, 1997 (http://www.who.dk/document/E56270.pdf, accessed 17 September 2003).
National networksAction framework & terms of reference (2000–2002) –Network of the European National Healthy Cities Net-works. Copenhagen, WHO Regional Office for Eu-rope, 2000 (http://www.who.dk/eprise/main/who/progs/hcp/Documentation/20011106_1, accessed17 September 2003).
National network fact sheets. Copenhagen, WHORegional Office for Europe, 2002 (http://www.euro.who.int/healthy-cities/CitiesAndNetworks/20020111_5, accessed 17 Sep-tember 2003).
National healthy cities networks in Europe. 3rd ed.Copenhagen, WHO Regional Office for Europe(Centre for Urban Health)/EURONET Association,1997.
City indicators and profilesCity health profiles – a review of progress. Copenha-gen, WHO Regional Office for Europe, 1998(http://www.who.dk/document/e59736.pdf,accessed 17 September 2003).
City health profiles – how to report on health in yourcity. Copenhagen, WHO Regional Office for Eu-rope, 1995 (http://www.who.dk/document/wa38094ci.pdf, accessed 17 September 2003).
Flynn BC. Documenting the urban health situation –tools for healthy cities. Copenhagen, WHO RegionalOffice for Europe, 1995 (http://www.who.dk/healthy-cities/Documentation/20010918_6,accessed 17 September 2003).
Garcia P, McCarthy M. Measuring health – a step inthe development of city health profiles. Copenhagen,WHO Regional Office for Europe, 1996 (http://www.who.dk/healthy-cities/Documentation/20010918_9, accessed 17 September 2003).
Healthy urban planningDuhl LJ, Sanchez AK. Healthy cities and the cityplanning process: a background document on links be-tween health and urban planning. Copenhagen,WHO Regional Office for Europe, 1999 (http://www.euro.who.int/healthy-cities/Documentation/20020514_1, accessed 17 September 2003).
Barton H, Tsourou C. Healthy urban planning – aWHO guide to planning for people. London, E&FNSpon, 2000.
Barton H, Mitcham C, Tsourou C, eds. Healthy ur-ban planning in practice: experience of European cit-ies. Report of the WHO City Action Group on HealthyUrban Planning. Copenhagen, WHO Regional Of-fice for Europe (in press).
Social determinants of healthWilkinson, R. & Marmot, M., ed. Social determi-nants of health. The solid facts. 2nd ed. Copen-hagen, WHO Regional Office for Europe, 2003
European Sustainable Developmentand Health SeriesPrice C, Dubé C. Sustainable development andhealth: concepts, principles and framework for actionfor European cities and towns. Copenhagen, WHORegional Office for Europe, 1997 (http://www.euro.who.int/healthy-cities/Documentation/20010918_11, accessed 17 September 2003). Alsoavailable in French and German.
City planning for health and sustainable development.Copenhagen, WHO Regional Office for Europe,1997 (http://www.euro.who.int/healthy-cities/Documentation/20010918_5, accessed 17 Septem-ber 2003).
31497_National.p65 06-10-2003, 08:0486

Towards a new planning process. A guide toreorienting urban planning towards Local Agenda 21.Copenhagen, WHO Regional Office for Europe,1999 (http://www.euro.who.int/healthy-cities/Documentation/20020517_1, accessed 17 Septem-ber 2003).
Community participation in local health and sustain-able development: approaches and techniques. Copen-hagen, WHO Regional Office for Europe, 2002(http://www.euro.who.int/healthy-cities/Docu-mentation/20030401_1, accessed 17 September2003).
ANNEX 1 . 87
31497_National.p65 06-10-2003, 08:0487

88 . NATIONAL HEALTHY CITIES NETWORKS
Annex 2
WHO criteria for accrediting nationalhealthy cities networks
• Endorsement of principlesand strategies, whereby thehead of the national networksigns a formal agreement tofulfil the responsibilities of thenetwork
Minimum criteria Ideal criteria (includingthe minimum criteria)
• Demonstrate the formal sup-port of a range of partnersthat might include ministries,WHO liaison officers and na-tional associations of local au-thorities
• Challenge politicians to advo-cate for additional resourcesfor the WHO Centre for Ur-ban Health so that it canstrengthen its work for na-tional networks
Endorsement of principles andstrategies
• Identify a coordinator or focalpoint with technical and ad-ministrative resources
• Formal organization of thenetwork under statutes or aconstitution
• A steering committee
• Clear membership criteria forcities that include a politicaldeclaration (Annex 3)
• Full-time coordinator
• Political representative
• Steering committee compris-ing city coordinators, politi-cians and nationalstakeholders
• Clear membership criteriabased on the four action ele-ments of a healthy city (en-dorsing principles and strate-gies, establishing infrastruc-ture, making a commitmentto products and outcomes,and networking), a politicaldeclaration and signing theAthens Declaration forHealthy Cities
• Technical and administrativesupport including an officewith a budget for activitiessuch as training and commu-nication
Infrastructure
31497_National.p65 06-10-2003, 08:0488
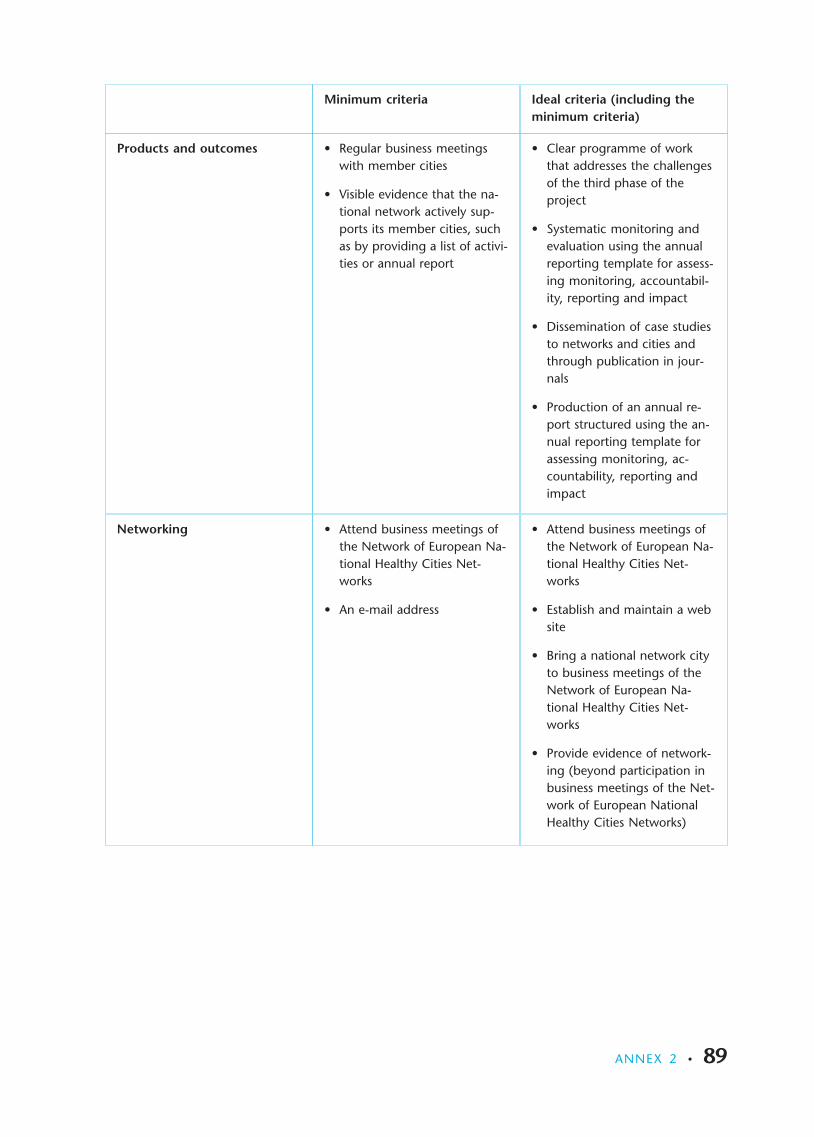
• Regular business meetingswith member cities
• Visible evidence that the na-tional network actively sup-ports its member cities, suchas by providing a list of activi-ties or annual report
Minimum criteria Ideal criteria (including theminimum criteria)
• Clear programme of workthat addresses the challengesof the third phase of theproject
• Systematic monitoring andevaluation using the annualreporting template for assess-ing monitoring, accountabil-ity, reporting and impact
• Dissemination of case studiesto networks and cities andthrough publication in jour-nals
• Production of an annual re-port structured using the an-nual reporting template forassessing monitoring, ac-countability, reporting andimpact
Products and outcomes
• Attend business meetings ofthe Network of European Na-tional Healthy Cities Net-works
• An e-mail address
• Attend business meetings ofthe Network of European Na-tional Healthy Cities Net-works
• Establish and maintain a website
• Bring a national network cityto business meetings of theNetwork of European Na-tional Healthy Cities Net-works
• Provide evidence of network-ing (beyond participation inbusiness meetings of the Net-work of European NationalHealthy Cities Networks)
Networking
ANNEX 2 . 89
31497_National.p65 06-10-2003, 08:0489
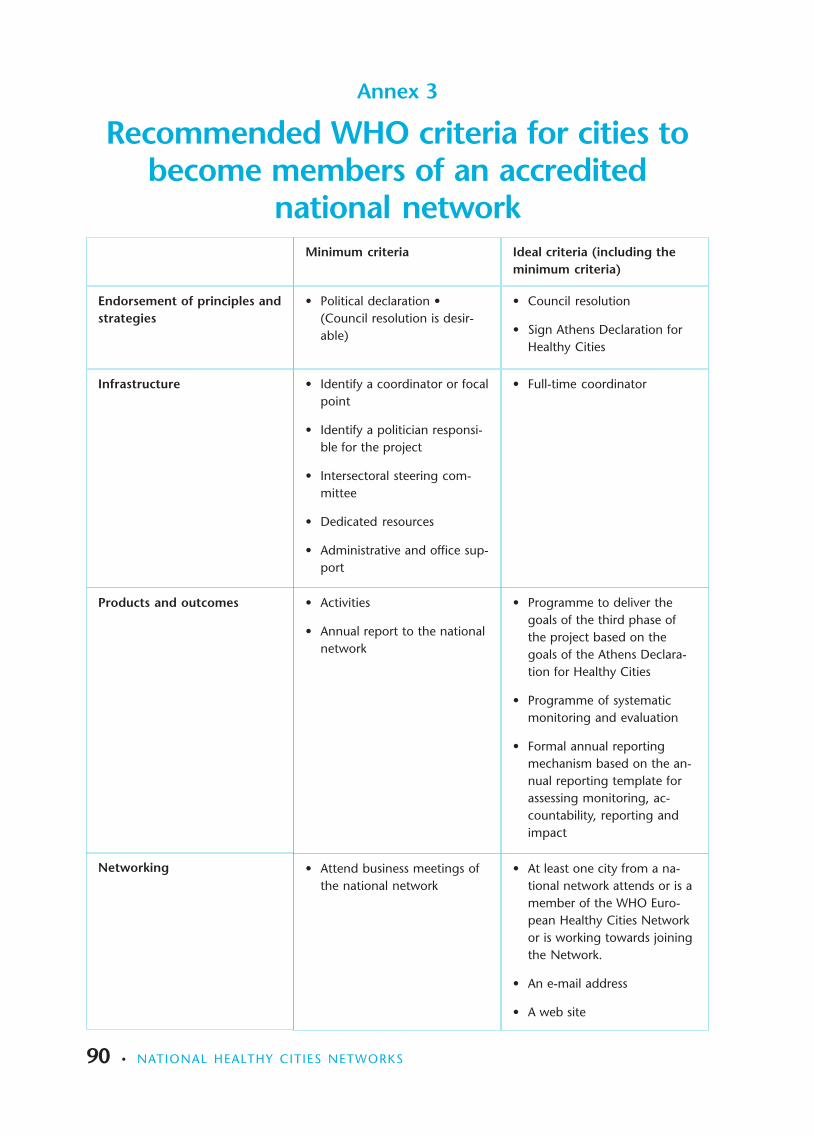
90 . NATIONAL HEALTHY CITIES NETWORKS
• Activities
• Annual report to the nationalnetwork
• Programme to deliver thegoals of the third phase ofthe project based on thegoals of the Athens Declara-tion for Healthy Cities
• Programme of systematicmonitoring and evaluation
• Formal annual reportingmechanism based on the an-nual reporting template forassessing monitoring, ac-countability, reporting andimpact
Products and outcomes
• Attend business meetings ofthe national network
• At least one city from a na-tional network attends or is amember of the WHO Euro-pean Healthy Cities Networkor is working towards joiningthe Network.
• An e-mail address
• A web site
Networking
Annex 3
Recommended WHO criteria for cities tobecome members of an accredited
national network
• Political declaration •(Council resolution is desir-able)
Minimum criteria Ideal criteria (including theminimum criteria)
• Council resolution
• Sign Athens Declaration forHealthy Cities
Endorsement of principles andstrategies
• Identify a coordinator or focalpoint
• Identify a politician responsi-ble for the project
• Intersectoral steering com-mittee
• Dedicated resources
• Administrative and office sup-port
• Full-time coordinatorInfrastructure
31497_National.p65 06-10-2003, 08:0490