my worst case…my best case · 9/15/2016 · day1 – hospital course. day 2 - hospital course...
TRANSCRIPT

My worst case…My best case...
Katarzyna Hryniewcz, MD
Minneapolis Heart Institute® at
Abbott Northwestern Hospital
27th ELSO Annual Conference
September 15, 2016

• I have no disclosures.

My worst case…My best case...

Case 1• 50 years old female, no PMH, started to
feel dizzy while teaching karate class• 911 called, anterior and lateral ST
elevation, in ambulance progressive hypotension, clammy, cardiac arrest while pulling into ambulance bay of ANW
• Manual CPR started, then LUCAS initiated
• Cath lab coronary angiogram …

Case 1
• Spontaneous dissection of the LM extending into LCx and LAD, complicated by LM thrombosis
• Attempted PCI – Unsuccessful due to inability to find true lumen
• Progressive shock • Cool it (therapeutic hypothermia) protocol initiated
Case 1
• Decision to proceed with VA ECMO placement despite on-going CPR with LUCAS, with adequate MAPs
VA ECMO
• Bifemoral approach• 21F LFA, 25 F LFV• 8F 11cm distal perfusion catheter placed
• IABP RFA• 4.8-5.2 l of flow
Case 1CT surgery called – “not a candidate for surgical revascularization due to:
– 1.5h of CPR, and a pH of 6.9 despite being on 5L/min ECMO
– Unsure about her additional comorbidities, and the futility of CABG in a setting of profound shock.
– Spontaneous LM dissection, poor quality of vessels after instrumentation”

Case 1 - Day 1
Drips • Epi at 5mcg/min• Levo at 15mcg/min• Dopa 15 mcg/kg/min• VP at .04u/min

Case 1 - Day 1
Day1 – hospital course• Shock liver(AST/ALT 1439/494)• Acute renal failure creatinine up to 2.0
• Troponin I 946 ng/ml (normal range <0.034)
• ARDS• Rhabdo – CK 10319 31325• ABG FiO2 40% vent/80% ECMO
– pH 7.36 – 39 – 161 – 100%
- Cool left lower extremity with pulses that are not obtainable by Doppler + tense calf
and extended foot; concerning for compartment syndrome.
- Vascular surgery consulted - No occlusion on CT angiogram, rather impaired flow by 8F
arterial sheath, bilateral fasciotomy performed
Day1 – hospital course

Day 2 - Hospital Course
• Waxing and waning pressor requirements
• Lactate and CKs trending down• Creatinine up to 3 with decreasing UOP
• And…

Day 2 - Hospital Course• New L cerebellar infarct per CT head (routine per our protocol)
• EEG - Diffuse slowing of the background record. This is a non specific finding but may be in part secondary to sedating medications. Underlying cerebral dysfunction can not be excluded and clinical correlation is recommended.
Day 2 – Hospital Course
• Neurology called “Repeat head CT to follow cerebellar infarction and rule out mass effect.• Continue current management• Unable to evaluate prognosis at this time.• Continue EEG recording• Will neurologically assess with less sedation. ”

Day 3 – Hospital Course
• Anuric, volume overloaded, creatinine almost 4 CRRT started
• Repeated CT head Repeat CT head yesterday with previously visualized cerebellar stroke (3.5 cm) + two new right parieto-occipital strokes (~1 cm) with associated loss of grey-white interface consistent with cerebral edema

Night 4– Difficult night with hypotension, alternating
afib/SVT/junctional rhythm and sustained VT necessitating defibrillation with 300 joules biphasic + initiation of amiodarone
– Hypotension necessitated brisk volume resuscitation resulting in increased frothy pulmonary secretions + increasing ECMO flow to 6lpm
– Hemodynamics much improved following initiation of paralytic
– Transfused for Hemoglobin 6.2

Case 1
• Multiple multi-disciplinary/family meetings…
• Unclear Advanced directives• Nursing staff uncomfortable with continuation of care

Day 5-8• More stable hemodynamically, pressors weaned off
• Remains on dobutamine gtt at 2.5 mcg/kg/min
• ABG adequate but radiographically still in pulmonary edema
• Did not tolerate ECMO wean, LVEF remains < 10%
• Sedation weaned to off on day 8

Day 9, 10, 11, 12• Neurology assessment “Her initial head CT showed subacute infarct in the left cerebellum; repeat head CT showed evolving infarcts in the left cerebellum, as well as the right parietal and right occipital lobes with poor white- gray differentiation suggestive of diffuse anoxic brain injury. Prognosis is poor, but patient may still make some recovery”

Day 13- hospital course
• Nurse notices patient looking around “quite alert”
• Starts following simple and…complex commands!
• But….
Still on CRRT, still in pulmonary edema
Day 13
• Now what?
Ethics consult called by nursing staff
• Improve communication between subspecialties and nurses
• Defer medical decisions to patient’s sister, who was appointed as the POA.
• Sister wants to continue full support and asking about an LVAD/transplant

Now what? • Keep going?
LVAD?
Withdrawal of care?

What’s the data? Not much data…
Some case reports…
E-CPR
- 26 pts with out of hospital arrest
- Average age 40 (+/-15)
- 54% male- Time from cardiac
arrest to initiation of ECMO 77 min (+/-51)
- 4 patients survived to Discharge (15%)

MCS for acute cardiogenic shock

Study design• Retrospective review of adult patients who
required MCS due to CS • The etiology of RCS included
acute MI in 49% acute decompensated HF in 27%.
• VA ECMO was chosen in cases of unknown neurologic status, complete hemodynamic collapse or severe coagulopathy.
Study results• 90 pts received an MCSD for refractory CS (RCS),• 21 (23%) of whom had active CPR. - Mean age was 53±14 years, 71% M, 60% had
IABP- short-term VAD in 49% and VA ECMO in 51%. - Median length of support was 8 days - Survival to hospital discharge was 49%.- Ongoing CPR to be an independent risk factor for
mortality
Study results
• Exchange to implantable VAD in 23 pts
• Survival to hospital discharge was 87% (20/23 pts)
• 1 year survival 86%

Day 15 – hospital course
- Decision to move with permanent LVAD

Day 15-30
- Resolution of pulmonary edema- Return of renal function to normal- Transmetatarsal amputation R foot
Day 30-60
• Rehab, back to work, driving!

1 year later…
• Successful heart transplantation!

Questions?

My best case….my worst case

Case 2• 59 year old F history of active smoking,
hyperlipidemia• Presented to the outside facility with
several weeks of worsening shortness of breath and severe fatigue
• Prior to admission she was treated with antibiotics and steroids, with no relief.

Case 2 – Outside hospital course• On admission
»Hypotensive with SBP in the 80s»Tachycardic»Troponin I 61
• Echocardiogram showed EF less than 10%. • Angiogram 3/8/16 showed normal coronary
arteries. • PCWP 25, no information re other
hemodynamics

Case 2 – Outside hospital course
Quickly progressed to profound cardiogenic shock, VT, acute hypoxic respiratory failure.

Case 2 – Outside hospital course
• An IABP placed • Continued having multiple episodes of VT and was treated with amiodarone gtt.
• Developed complete heart block TPM• IABP removed and Impella 2.5 placed.

Case 2 – Outside hospital course
• Worsening shock despite the above• VA ECMO was initiated and she was transferred to our facility for further management

Case 2 – hospital course
• Arrived intubated, sedated.• Medications on transfer: Levophed infusion at 30
mcg/min, propofol, amiodarone infusion• Labs:
• Cr 0.98, K 3.7, • Troponin I 61.9, • AST 1507, ALT 1722, • Hemoglobin 13.6, white blood count 14• Normal CRP and ESR

Case 2 – hospital courseECG
Underlying rhythm probably complete heart block with accelerated idiopathic ventricular rhythm or slow VT in the high 80s and low 90s.
Very low QRS voltage.

Case 2 – hospital course
• In/out incessant VT/VF, but maintaining ECMO flows and MAPs
• On amiodarone gtt with multiple boluses
• Temporary pacemaker not sensing.

Case 2 – hospital course
Clinical picture consistent with acute, fulminant myocarditis
Case 2 – hospital course Day 2
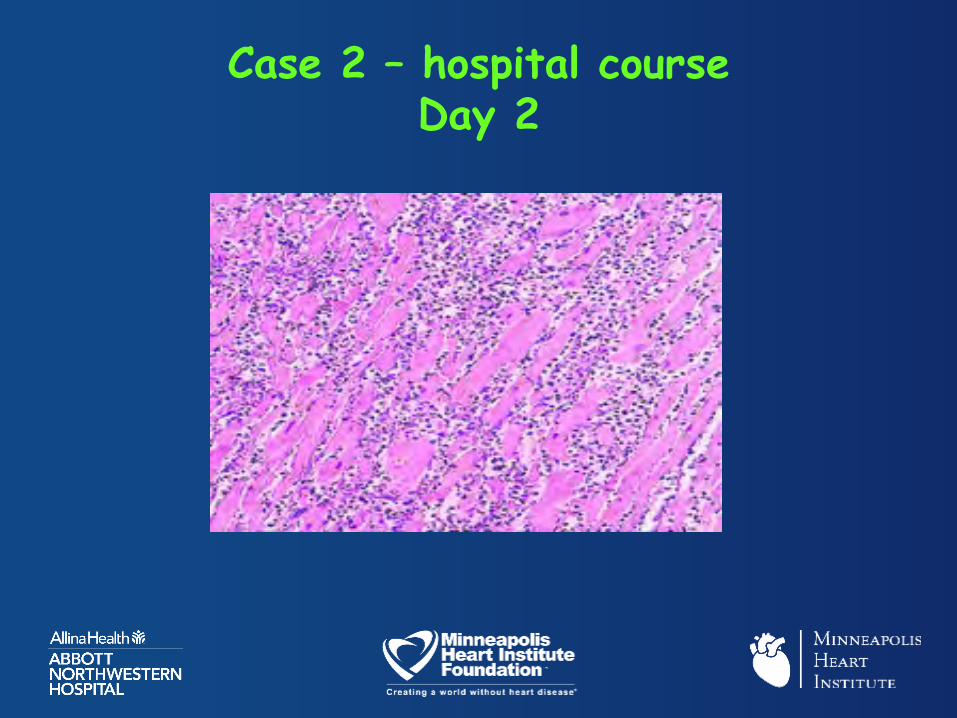
• Another TPP placed• Endomyocardial biopsy performed• Pathologists calls at 7 pm ….
Spectacular case of lymphocytic myocarditis with myocardial necrosis
Case 2 – hospital course Day 2

Case 2 – hospital course Day 2
• Stable VA ECMO parameters– Pump flow LPM: 4.84– FiO2 ECMO: 90– Sweep flow LPM: 3
• Severely volume overloaded• Started CRRT• Started on Solu-Medrol 1g IV x 3 doses

Case 2 – hospital course Day 3
– Overall more stable, VF x 2, shocked successfully
– PA sat > 70%, continue DBA at 4 mcg/kg/min, IABP
– Vasopressor: off NE, low dose VP– Echo with some recovery of LVEF in the 25% range, large, hypokinetic RV
– Lactate down to 2.2

Case 2 – hospital course Day 4
• Tolerated wean to 1.5 l with good CO, LVEF of 30-35%, still severely enlarged RV
• Continues to have runs of VT• Sedation off, seems to be waking up• Plan to repeat endomyocardial biopsy before consideration of ECMO decannulation

Case 2 – hospital course Day 5
• Incessant VT overnight on Day 5, then quiet after addition of ranolazineand lidocaine
• Endomyocardial bx still showing dense myocarditis.
• Unable to wean VA ECMO due to hypotension
• Remains on CRRT
Case 2 – hospital course Day 6-10
• Discussed at multidisciplinary meeting. • Unclear if/when recovery will occur but
clear is that it will not occur in a time frame amenable to support with ECMO
• In this setting appropriate to look towards alternative modalities of support.
• Plan for conversion to temporary BiVADsupport (RA-PA and LV-Ao), placed the following day

Case 2 – hospital course Day 11-45
• Woke up• Trached, weaned of the ventilator, able to
communicate• Recovery of renal function, off RRT• Progressing well with PT/OT, sitting in a
chair, standing with assist• Plan to give another 3-4 weeks and list for
heart transplantation
Case 2 – hospital course day 46• On call MD called by a nurse that patient
vomiting and unresponsive with• Blood glucose 256 mg/dL, MAP 72 mmHg,
SpO2 99%.• Physical examination:
• Cheyne-Stokes respiration• GCS 3/15, PEARL 4 • Decerebrate posturing• Bilateral extensor plantars
• Concern for neurological event

Case 2 – hospital course day 46
• Placed back on mechanical ventilator.• Heparin infusion stopped• (APTT 54 seconds, INR 1.2).• STAT CT head
Case 2 – hospital course day 46
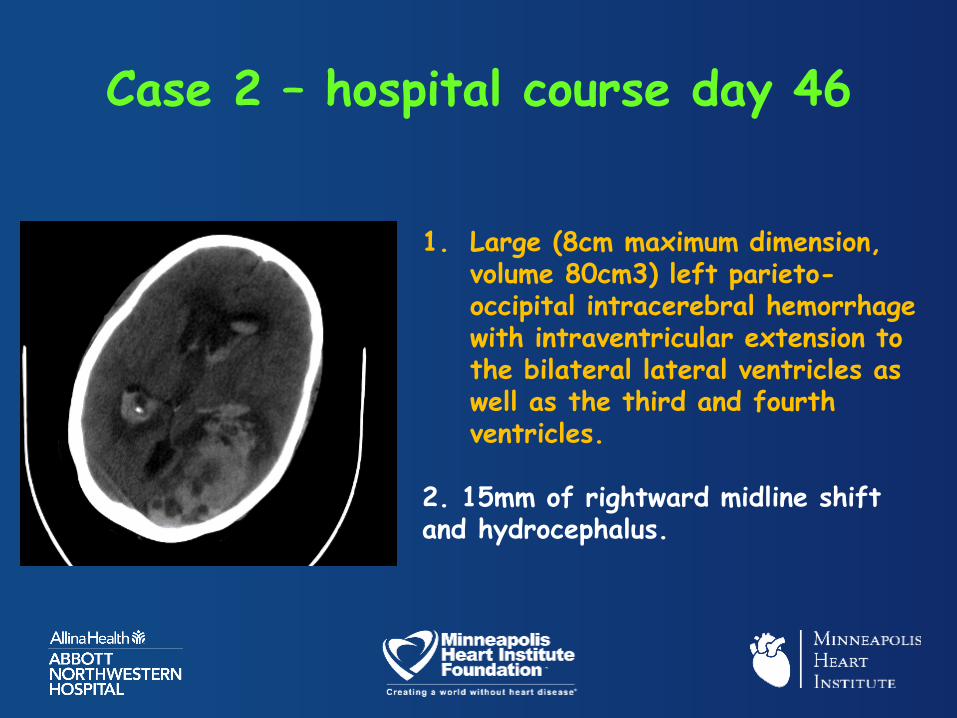
1. Large (8cm maximum dimension, volume 80cm3) left parieto-occipital intracerebral hemorrhage with intraventricular extension to the bilateral lateral ventricles as well as the third and fourth ventricles.
2. 15mm of rightward midline shift and hydrocephalus.
Case 2 – hospital course day 46
• Family meeting and decision to withdraw care

Questions?
