my approach to pnh management - learning is hope pnh management.pdf · 7/17/2017 1 paroxysmal...
TRANSCRIPT

7/17/2017
1
Paroxysmal Nocturnal Hemoglobinuria
David Dingli, MD, PhD, FRCP, FRCPEd, FACP
Professor of Medicine
Mayo Clinic, Rochester, MN
The origin of the name….
PNH – Some history
• First description - J Schmidt (1648)
• Important description - Dr P. Strubing (1882)
• Constant hemosiderinuria – Marchiafava (1911)
• PNH - Ennekin (1925)
• Complement mediated hemolysis – Rosse/Dacie(1964)
• PNH is clonal – Luzzatto (1970)
• GPI biosynthesis – Kinoshita (1993)
• Eculizumab (2004)
Epidemiology
• Rare
• Different test sensitivities
• Different definitions
• Maybe 5-20/million in USA
• Incidence may be higher in other countries
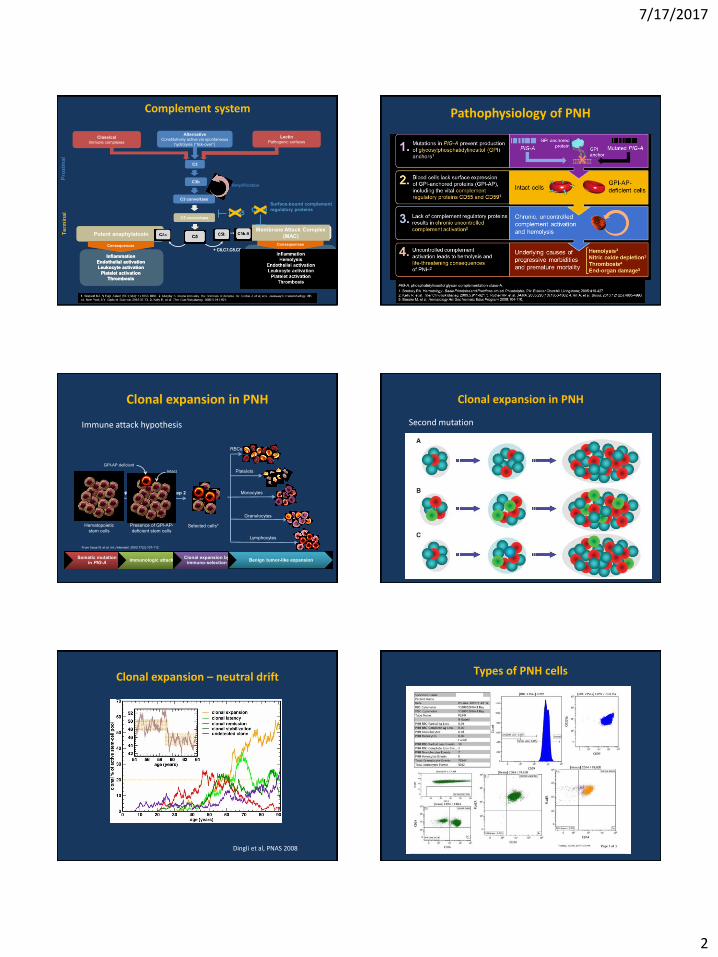
Membrane proteins
7/17/2017
2
LectinPathogenic surfaces
ClassicalImmune complexes
AlternativeConstitutively active via spontaneous
hydrolysis (“tick-over”)
Pro
xim
al
Amplification
C3C3
C3bC3b
C3 convertaseC3 convertase
Te
rmin
al
Inflammation
Endothelial activation
Leukocyte activation
Platelet activation
Thrombosis
Inflammation
Endothelial activation
Leukocyte activation
Platelet activation
Thrombosis
C5aC5aC5C5
C5bC5b C5b-9C5b-9
ConsequencesConsequencesConsequencesConsequences+ C6,C7,C8,C9+ C6,C7,C8,C9
C5 convertaseC5 convertase
Potent anaphylatoxinMembrane Attack Complex
(MAC)
Surface-bound complement
regulatory proteinsCD55
CD59
Complement system Pathophysiology of PNH
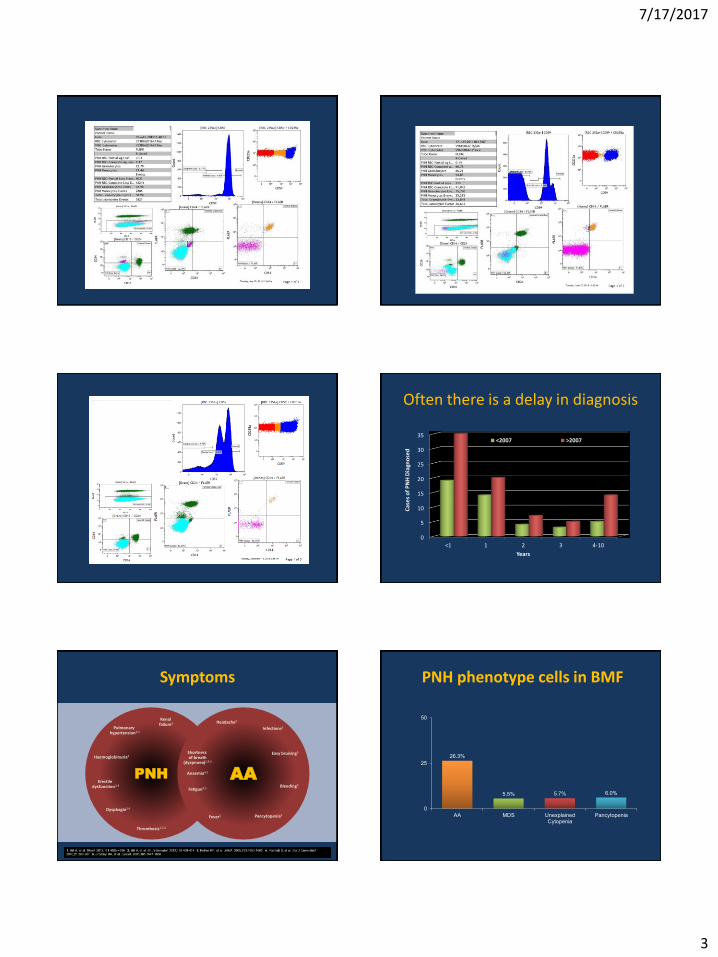
Clonal expansion in PNH
RBCs
Monocytes
Platelets
Granulocytes
Lymphocytes
Step 1 Step 2
Hematopoietic
stem cells
Presence of GPI-AP-
deficient stem cellsSelected cells*
Somatic mutation in PIG-A
Immunologic attackClonal expansion by
immuno-selectionBenign tumor-like expansion
GPI-AP deficient
Intact
From Inoue N, et al. Int J Hematol. 2003;77(2):107-112.
Immune attack hypothesis
Clonal expansion in PNH
Second mutation
Clonal expansion – neutral drift
Dingli et al, PNAS 2008
Types of PNH cells
7/17/2017
3
Often there is a delay in diagnosis
0
5
10
15
20
25
30
35
<1 1 2 3 4-10
Cas
es
of
PN
H D
iagn
ose
d
Years
<2007 >2007
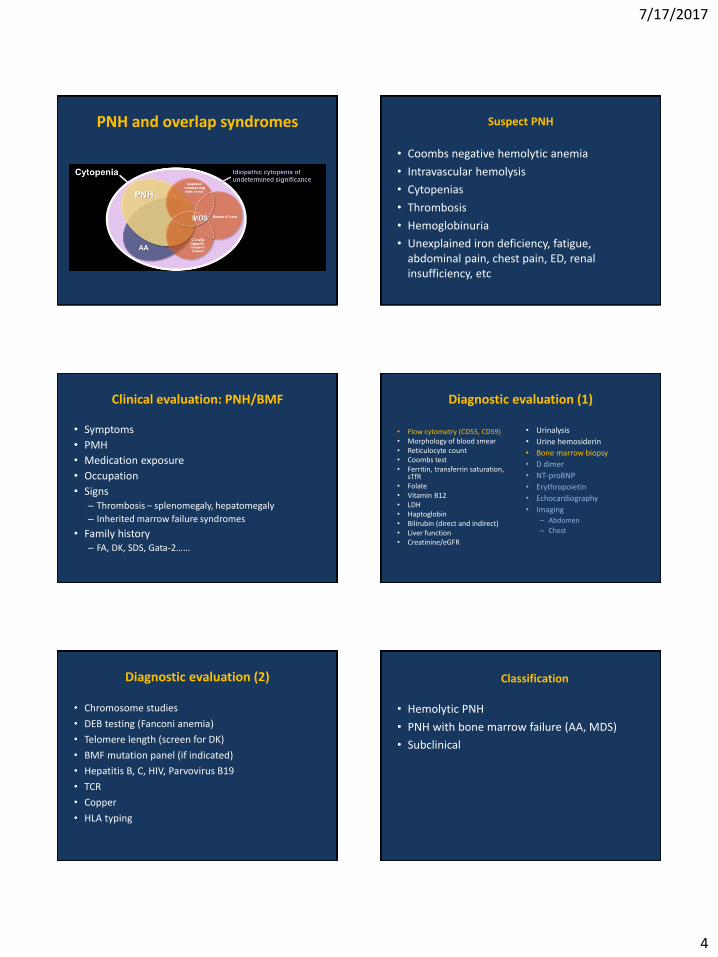
Symptoms
PNH AA
Shortness of breath
(dyspnoea)2,4,5
Anaemia4,5
Fatigue4,5
Renal failure4
Pulmonary hypertension2,4
Haemoglobinuria3
Dysphagia3,4
Erectile dysfunction3,4
Thrombosis1,3,4
Easy bruising5
Bleeding5
Headache5
Fever5
Infections5
Pancytopenia5
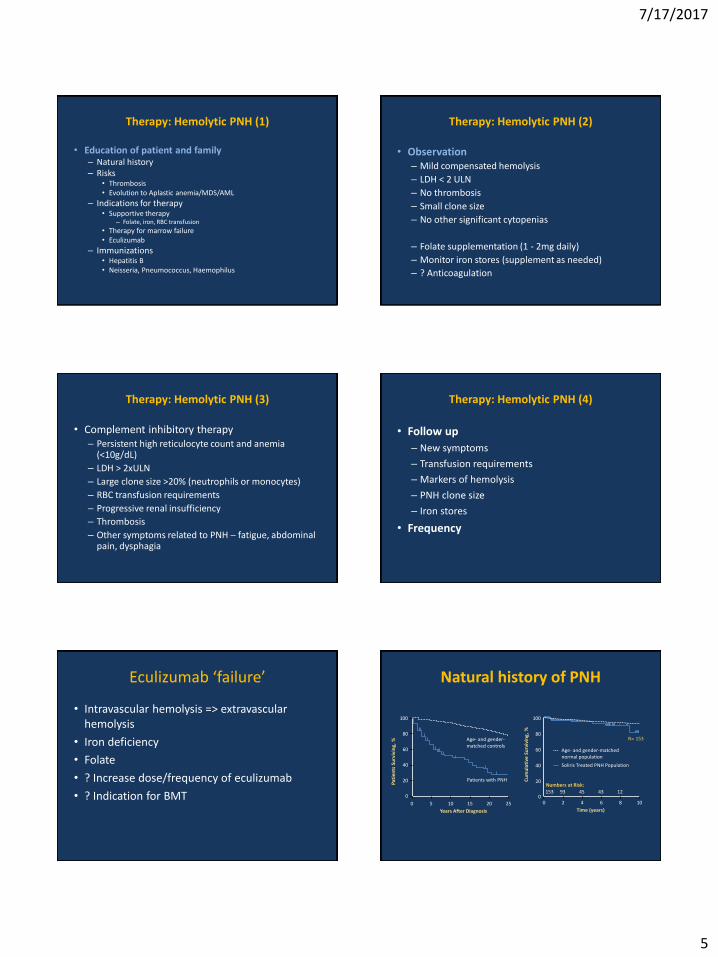
PNH phenotype cells in BMF
26.3%
5.5% 5.7% 6.0%
0
25
50
AA MDS UnexplainedCytopenia
Pancytopenia
7/17/2017
4
PNH and overlap syndromes Suspect PNH
• Coombs negative hemolytic anemia
• Intravascular hemolysis
• Cytopenias
• Thrombosis
• Hemoglobinuria
• Unexplained iron deficiency, fatigue, abdominal pain, chest pain, ED, renal insufficiency, etc
Clinical evaluation: PNH/BMF
• Symptoms
• PMH
• Medication exposure
• Occupation
• Signs– Thrombosis – splenomegaly, hepatomegaly
– Inherited marrow failure syndromes
• Family history– FA, DK, SDS, Gata-2……
Diagnostic evaluation (1)
• Flow cytometry (CD55, CD59)• Morphology of blood smear• Reticulocyte count • Coombs test• Ferritin, transferrin saturation,
sTfR• Folate • Vitamin B12• LDH• Haptoglobin• Bilirubin (direct and indirect)• Liver function• Creatinine/eGFR
• Urinalysis
• Urine hemosiderin
• Bone marrow biopsy
• D dimer
• NT-proBNP
• Erythropoietin
• Echocardiography
• Imaging– Abdomen
– Chest
Diagnostic evaluation (2)
• Chromosome studies
• DEB testing (Fanconi anemia)
• Telomere length (screen for DK)
• BMF mutation panel (if indicated)
• Hepatitis B, C, HIV, Parvovirus B19
• TCR
• Copper
• HLA typing
Classification
• Hemolytic PNH
• PNH with bone marrow failure (AA, MDS)
• Subclinical
7/17/2017
5
Therapy: Hemolytic PNH (1)
• Education of patient and family– Natural history– Risks
• Thrombosis• Evolution to Aplastic anemia/MDS/AML
– Indications for therapy• Supportive therapy
– Folate, iron, RBC transfusion
• Therapy for marrow failure• Eculizumab
– Immunizations• Hepatitis B• Neisseria, Pneumococcus, Haemophilus
Therapy: Hemolytic PNH (2)
• Observation– Mild compensated hemolysis
– LDH < 2 ULN
– No thrombosis
– Small clone size
– No other significant cytopenias
– Folate supplementation (1 - 2mg daily)
– Monitor iron stores (supplement as needed)
– ? Anticoagulation
Therapy: Hemolytic PNH (3)
• Complement inhibitory therapy– Persistent high reticulocyte count and anemia
(<10g/dL)
– LDH > 2xULN
– Large clone size >20% (neutrophils or monocytes)
– RBC transfusion requirements
– Progressive renal insufficiency
– Thrombosis
– Other symptoms related to PNH – fatigue, abdominal pain, dysphagia
Therapy: Hemolytic PNH (4)
• Follow up
– New symptoms
– Transfusion requirements
– Markers of hemolysis
– PNH clone size
– Iron stores
• Frequency
Eculizumab ‘failure’
• Intravascular hemolysis => extravascular hemolysis
• Iron deficiency
• Folate
• ? Increase dose/frequency of eculizumab
• ? Indication for BMT
Natural history of PNH
100
80
60
40
20
0
0 5 10 15 20 25
Years After Diagnosis
Pat
ien
ts S
urv
ivin
g, % Age- and gender-
matched controls
Patients with PNH
2 4 6 8 10
20
40
60
80
100
Time (years)
Cu
mu
lati
ve S
urv
ivin
g, %
00
N= 153
Age- and gender-matched normal population
Numbers at Risk:153 93 45 43 12
Soliris Treated PNH Population
7/17/2017
6
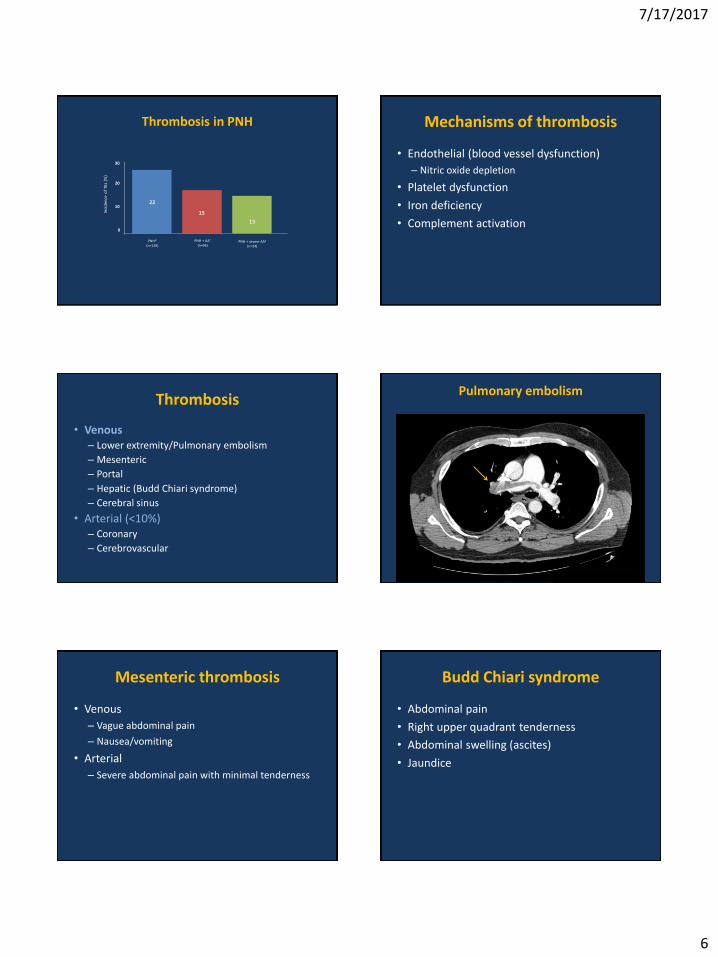
Thrombosis in PNH
PNH*(n=126)
PNH + severe AA‡
(n=24)
PNH + AA†
(n=96)
22
15
13
30
20
10
0
Inci
den
ce o
f TE
s (%
)
Mechanisms of thrombosis
• Endothelial (blood vessel dysfunction)
– Nitric oxide depletion
• Platelet dysfunction
• Iron deficiency
• Complement activation
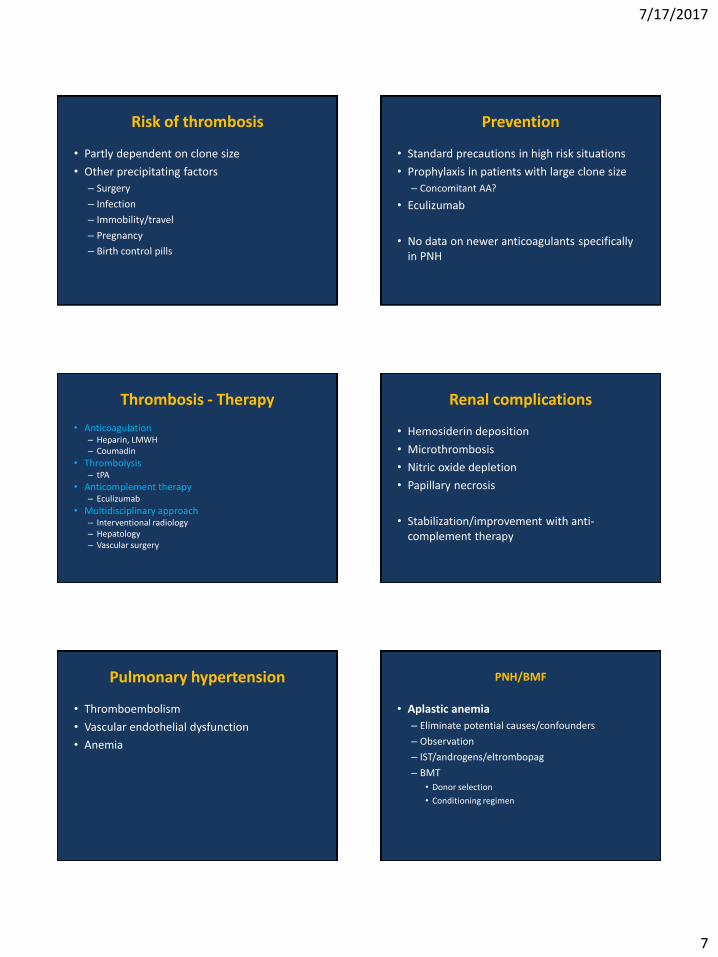
Thrombosis
• Venous– Lower extremity/Pulmonary embolism
– Mesenteric
– Portal
– Hepatic (Budd Chiari syndrome)
– Cerebral sinus
• Arterial (<10%)– Coronary
– Cerebrovascular
Pulmonary embolism
Mesenteric thrombosis
• Venous
– Vague abdominal pain
– Nausea/vomiting
• Arterial
– Severe abdominal pain with minimal tenderness
Budd Chiari syndrome
• Abdominal pain
• Right upper quadrant tenderness
• Abdominal swelling (ascites)
• Jaundice
7/17/2017
7
Risk of thrombosis
• Partly dependent on clone size
• Other precipitating factors
– Surgery
– Infection
– Immobility/travel
– Pregnancy
– Birth control pills
Prevention
• Standard precautions in high risk situations
• Prophylaxis in patients with large clone size
– Concomitant AA?
• Eculizumab
• No data on newer anticoagulants specifically in PNH
Thrombosis - Therapy
• Anticoagulation– Heparin, LMWH– Coumadin
• Thrombolysis– tPA
• Anticomplement therapy– Eculizumab
• Multidisciplinary approach– Interventional radiology– Hepatology– Vascular surgery
Renal complications
• Hemosiderin deposition
• Microthrombosis
• Nitric oxide depletion
• Papillary necrosis
• Stabilization/improvement with anti-complement therapy
Pulmonary hypertension
• Thromboembolism
• Vascular endothelial dysfunction
• Anemia
PNH/BMF
• Aplastic anemia
– Eliminate potential causes/confounders
– Observation
– IST/androgens/eltrombopag
– BMT
• Donor selection
• Conditioning regimen

7/17/2017
8
Therapy of PNH/BMF
• CsA/ATG/Prednisone
• Eculizumab
• BMT
– If AA is predominant problem
– Transfusion dependence/ongoing hemolysis
– Evolution to MDS/AML
– Recurrent, severe thrombosis
Eculizimab
• Often effective– ~ 70% transfusion independent
• Will not improve WBC and PLT
• Does not alter risk of evolution
• Generally well tolerated
• Dose may be adjusted in some patients
• Look for other causes of fatigue– Iron deficiency
LT complications
• ATG/CsA– Immunosuppression
– Renal toxicity, hypertension
– Risk of tumors
• BMT– Immunosuppression
– CsA toxicity
– GVHD
– Tumors
Special considerations
• Pregnancy
– High risk of thrombosis
– Eculizumab
• Surgery
– Prophylaxis
– Eculizumab
• Air travel
– Prophylaxis
In development
• Other C5 inhibitors
– Mab, Si-RNA, Aptamers
• C3 inhibitors
• C3 convertase inhibitors
• AP inhibitors
– Si-RNA, Aptamers, FH based proteins
Thank you