hemoglobinemia and hemoglobinuria abnormality (1
TRANSCRIPT

PHYSIOLOGICAL INTRAVASCULAR HEMOLYSIS OF EXERCISE.HEMOGLOBINEMIA AND HEMOGLOBINURIA
FOLLOWING CROSS-COUNTRY RUNS
By D. ROURKE GILLIGAN, M. D. ALTSCHULE, AND E. M. KATERSKY(From the Medical Service and the Medical Research Laboratories, Beth Israel Hospital,
and the Department of Medicine, Harvard Medical School, Boston)
(Received for publication May 19, 1943)
Studies on 3 cases of march hemoglobinuriawere recently reported from this laboratory andthe existing literature concerning this syndromewas reviewed (1). In 1 patient of our series andin some other reported instances, frank hemo-globinuria has been observed following walks ofonly 20 minutes' duration. Such occurrences areobviously unusual and are considered to be due tosome as yet unrecognized and apparently benignabnormality (1). There are, however, other re-ported cases in which hemoglobinuria occurredonly after very long, strenuous walks or after longruns. The question arises whether intravascularhemolysis, giving rise to hemoglobinemia andsometimes hemoglobinuria, occurs with sufficientfrequency in certain types of strenuous exercise oflong duration to be considered physiological. Togain information in this regard, a study was madeof the incidence and degree of intravascular he-molysis in normal individuals performing longstrenuous runs; the results of these studies andof other urinary and blood studies pertinent to theproblem are reported and discussed herein.
MATERIAL AND METHODS
Material. Studies were made in groups of young sub-jects performing runs as follows: (1) 11 men, aged 17 to18 years, after a cross-country run of 2.6 to 2.8 miles, in14 to 18 minutes; (2) 11 men, aged 19 to 21 years, aftera cross-country run of 4.5 to 5.1 miles, in 23 to 31 min-utes; and (3) 26 men, aged 18 to 65 years, after a mara-thon run of 10 to 262 miles. In addition, comparativestudies were made in 1 subject after the 26.2 mile mara-thon run, after a 5-hour period of exercise on the bicycleergometer, after a 262 mile walk with a 52-pound packon his back, and after an additional run of 112 miles in76 minutes and 19 seconds.Methods of study. A blood sample was taken from an
antecubital vein, without stasis, within 15 minutes aftercompletion of exercise. The blood for plasma hemo-globin measurement was drawn as suggested by Ham(2): a sterilized syringe and needle, previously rinsedwith sterile saline solution, were used; 5.0 cc. of blood
were introduced into a tube containing 0.5 cc. of 3.0 percent sodium citrate solution. The tube was stopperedand gently inverted several times to secure mixing. Theplasma specimen was removed from the citrated bloodsamples from one-half to one and one-half hours afterthe blood was drawn. In many instances, 5.0 cc. of ad-ditional blood were placed over oxalate mixture forstudies of hematocrit and of erythrocyte fragility. Asample of urine was collected shortly after blood wastaken. Examination of the abdomen for the presence ofhepatic or splenic enlargement was made at the end ofexercise.
Chemical methods. The chemical methods utilized weredescribed in detail in a previous publication (3). Theconcentration of hemoglobin in the plasma and urine wasmeasured by the benzidine method as described by Bingand Baker (4, 5), with slight modification (3). Testsshowed that no appreciable change in the plasma hemo-globin value occurred when the citrated blood sample re-mained at room temperature for 2 hours before separat-ing the plasma; these tests were made in order to makecertain that the necessary standing of the blood for from30 to 90 minutes, between the time it was drawn at theplace of termination of the exercise and the removal ofthe plasma in the laboratory, resulted in no measurablehemolysis. It was also demonstrated that the amount ofhemoglobin in the plasma was not affected by transport-ing the blood from the field to the laboratory. The plasmahemoglobin values of some 50 normal subjects, who hadnot undertaken any strenuous exercise on the day ofstudy, revealed values usually of 1.0 to 6.0 mgm. per 100cc., with a rare value between 6.0 and 9.0 mgm. per 100cc. and an average value of 4.0 mgm. per cent. We be-lieve that this variability between 1.0 and 6.0 mgm. ofhemoglobin per 100 cc. of plasma is not a true variabilityin the plasma concentration of the circulating blood, but ismore likely occasioned by slight in titro changes. Thisimpression is gained from the fact that 2 blood samples,drawn within a period of a few minutes from a givensubject at rest, not infrequently vary by 2.0 to 4.0 mgm.per 100 cc. Although it is perhaps true that minimalextravascular hemolysis cannot be avoided, no plasmahemoglobin value after exercise has been considered in-creased unless it was higher than the uppermost limitencountered in normal resting individuals, namely, 9.0mgm. per 100 cc.The bilirubin concentration of the plasma was meas-
ured by the method of Malloy and Evelyn (6). The to-
859
D. ROURKE GILLIGAN, M. D. ALTSCHULE, AND E. M. KATERSKY
CaC Ca
oo bO.00,
b
NO
coa4 0CV000-
4 4 .J 4 4
o oeq o o o o
o oou22221.3_
cocc; 000e000
0c 0000000-00
00 00 000000
00 00 0000000Cx
U)
0
'0 e' .00 . - . Cd
4,, Css 4_l >.4- >,0 4° >, (00eq °= = ox S.x ~~~~~~~Ca
3..
0
0o 4 in 4 00 4C4 C02 2 2 00 0 00 04i 4- 4i 4i -W 4-) 4.) 4. 4J
-14 e14 C 0 lq040 0
a4() a-)"
a) a)2 o 2 o~ 2200 0
..3..
U.) ed 4i Cd4i 4- C
0. . 0. 0. Q00000 0
0 (2 000000o 0
'0' 'UV r'''ar 0'a '0 * '0'0 '0'0'V '0
*-u * < t.c* ) C.) C.) C. C.) C. C. C.) C.C)-Ca Cd CaCa CaCaCaCaCaCaCa C Ca Ca Ca Ca Cd cd
NO000 Z- 00 V%0qC4 0V- C4 C4 C4 CN N
00 00 0 0t-C)Cto0ON O toNo -Cl ld
** .*.. *00 ..0
w- v-4 v -4 W-|-
eoo te a)o0o0toommU)0 Q U)%W4c
0 N00 04
*2d4_ld4Ut-UI
'04 V-4 %0' V-U)'00%0 4-4%0
'IO%ONoso NO O %O
eq on 0-0U)U)
u) ++u) 00U)+u)
0000qC 0 50F.00o00o.0
4-. 4)4* *i*) -U -*.*. t. .) U)uuuuu ououesoo
00000 0o0oooo
4~~4.h _~~+4
C.)C.) OC.OC)C.C.C.0000 ZOZOOQO
0cOzCa
Cx:
Cx.
zCx
U)
P.
zV)V
zC
0 t' 00 00 00 in 00 00eq - - eq - -- -
0~0* 0* 0 0
(NUCn-14 %0 000 %00 00ei - Lq-- -M"
CV%4i in %0 CV4cs E)M ,4eqeq..4
0U) N 0 0.o 00toE) OONeq) U)_ C) eq4q_ e " 4
in% 00V4to t LO-V)0 00%OL 0%0%
-~~~~~~~~~~~~~W4-eqe eq eq eqe ~e qeqe
Naw U) ei U)U)UI)U)
eqC)C)~ U) +%Oab000%0'-
in-
Uin-
In t- - ineq4 eqeqC4v4C4V-
a)i4J4- J J4 4 -
U 0 U U U 0i UUZ Z oz
0
a)
Cad
o0 -a..
Cd
ad c)c..o
a.)
*0
a 0
C a
4._
co80 0C a
r)
4.0
COb-.0
co
ad )a)
CO
-,0e
coblo
co
0.
3-.
a)
4J '
O.. a)
Ei
rA
CaC
COCoC
obO
bOCa
;
CaCOa
o._
Ca -
o 0%.cn C)
ac )
CO
a)
860
a)Cd
Cd
a)
10a)10
0
a)
'0
Cl
Cdu
0
-a)0~
.0
la
8 m
.0 -
a.50
a)
Ooe
a)
.0
0S
Ei
a.5Cl
b4
"I)
ZA)
a.
C.)
04'0-
eq
00
~o
CO
U)
Ca
~.
z
C.4
zzCx
crCd
U)go "
eas j%
-
OD0 bo0 A cn.- 0
- 11.>4i 0 r.'V.14 O&..o :3 904 6.
4n
I14. a0 :9v 93E 0w
E-4 !iAr.
c-
vvr.Cd 93-W :3 -a.m W r0
-w W
8.9.0 C:
cn O
Cd

INTRAVASCULAR HEMOLYSIS OF EXERCISE
tal protein concentration of the urine was measured gravi-metrically after precipitation with trichloroacetic acid(3). When the total protein was less than approximately30 mgm. per 100 cc., the concentration was estimated bycomparison of the turbidity of the urine with that ofstandards after the addition of 5.0 per cent solution ofsulfosalicylic acid. Spectrophotometric examination ofplasma and urine specimens were made for us by Dr.0. H. Lowry of the Department of Biochemistry of theHarvard Medical School; a Ko5nig-Martens type ofspectrophotometer was used. The fragility of the redblood cells in hypotonic saline was measured quantita-tively, essentially as described by Hunter (7), with thefollowing modifications: oxalate mixture was used as ananticoagulant, the blood was oxygenated for 3 minutes inair, and after transferring the samples of blood to thesaline solutions, the mixtures were allowed to stand for1 hour. In most instances, a phosphate buffer solution,giving a pH of 7.4, was added to the saline solution, ac-cording to the suggestion of Dr. A. Baird Hastings ofthe Department of Biochemistry of the Harvard MedicalSchool; the final salt concentrations were calculated inosmolar concentration and expressed in equivalent percent of pure sodium chloride solutions.
RESULTS
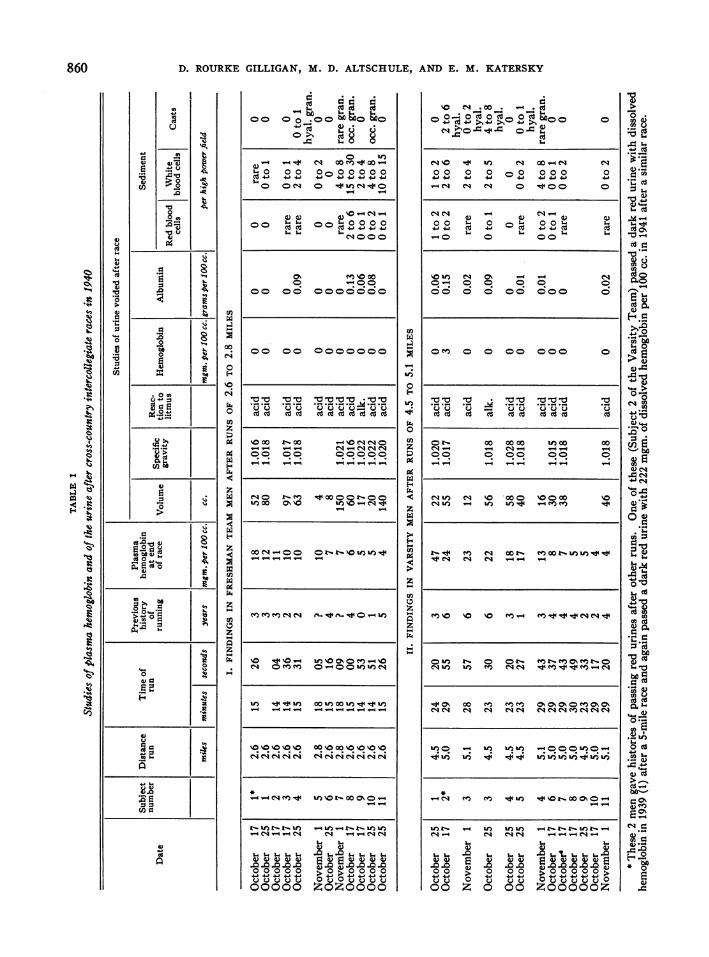
Plasma and urinary hemoglobin findingsCross-country runs. Of 11 Harvard freshmen
who ran 2.6 to 2.8 miles in 14 to 18 minutes, 5had plasma hemoglobins of 10.0 to 18.0 mgm. per100 cc. (i.e., above the upper limit of normal, 9.0mgm. per 100 cc.) at the end of the race (TableI). One of these 5 ran again and had an in-creased plasma hemoglobin on the second run also(Table I). Urines collected in 10 of these sub-jects, following the run, were of normal color andshowed negative benzidine reactions.Of 11 Harvard varsity track men who ran 4.5
to 5.1 miles in 23 to 31 minutes, 5 had definitelyreddish plasma with plasma hemoglobin valueselevated to 17 to 47 mgm. per 100 cc. (Table I).Studies made after another run in 2 of these 5subjects also showed increased plasma hemoglobinconcentration. Urines were collected after theruns in 8 of the 11 subjects, including the subjectwho showed a plasma hemoglobin of 47 mgm. per100 cc.; the urines were all of normal color buthemoglobinuria was detected in one specimen bythe benzidine test.Two of these subjects who showed hemoglobi-
nemia, following these cross-country runs, alsogave histories of having passed red urines on otheroccasions following runs. One of these subjects
passed a red urine after a race in 1939, i.e., a yearbefore these statistical studies were made, andagain in 1941, a year after these studies. In bothinstances, the urine became normal in color andshowed no hemoglobin or albumin on the morningfollowing the race. There were no symptoms atthe time of the hemoglobinuria.Marathon runs. The plasma hemoglobin values
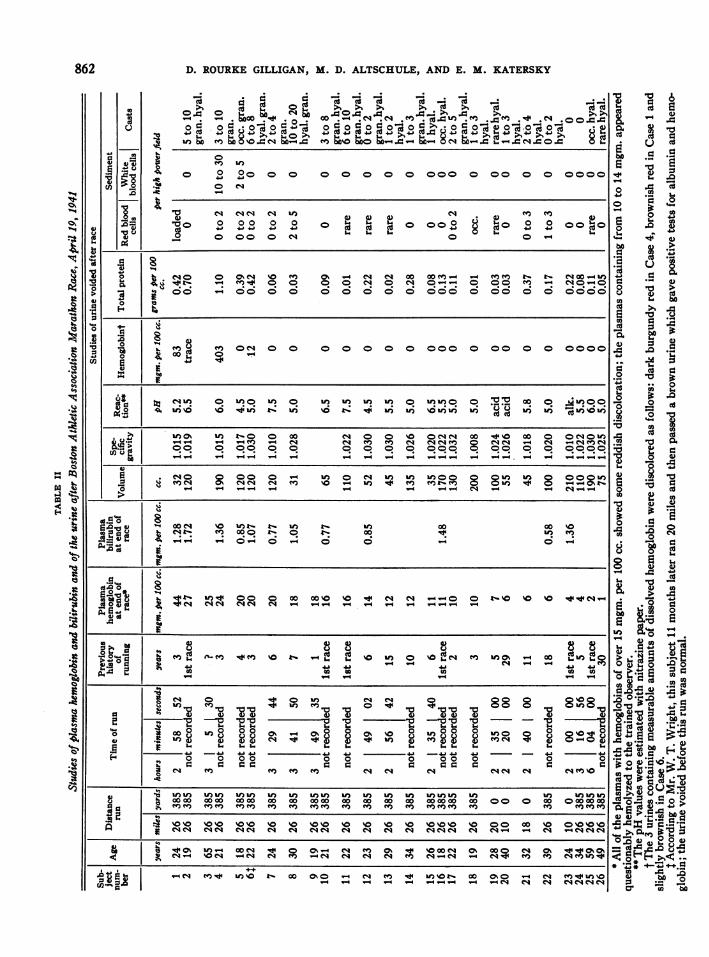
after the marathon run were elevated above theupper limit of normal in 18 of the 22 marathonrunners who ran the entire 26.2 miles (Table II).The plasma hemoglobin values of these 18 sub-jects varied from 10 to 44 mgm. per 100 cc. andaveraged 18 mgm. per 100 cc. In 11 of these 18cases (Cases 1 to 11, inclusive), the plasma hemo-globin was greater than 15 mgm. per 100 cc. Inthese instances, there was a definite reddish dis-coloration of the plasma. Four of these subjectsshowed hemoglobinuria, with concentrations froma trace to as high as 0.4 gram of dissolved hemo-globin per 100 cc. of urine; 3 of these urines werediscolored from light brownish to very dark bur-gundy red. The hemoglobinuria occurred in the4 subjects who showed the higher plasma hemo-globin values at the end of the run (Table II).Two of the subjects who showed hemoglobinuriaat the end of the race were studied for severalhours after the race (Table III). Hemoglobi-nemia and hemoglobinuria disappeared in bothcases within 3 and 4 hours after the end of therace.Four of the marathon runners had histories of
passing red urines on one or more previous occa-sions following long runs; 1 of these subjects(Case 6, Table II) showed hemoglobinuria afterthe race of the present study, and again, 11 monthslater after another long run (Table II).
There was no correlation between the age ofthe runners or the number of years or state oftraining and the occurrence of hemoglobinemia orhemoglobinuria, either in the subjects who ran themarathon (Table II) or in those who ran theshorter races (Table I).
Further observations during various exercises on amarathon runner wtith hemoglobinuria
Further studies on the production of intravas-cular hemolysis during walking, bicycling, andrunning a shorter distance were made in the case
861
D. ROURKE GILLIGAN, M. D. ALTSCHULE, AND E. M. KATERSKY
(4~~~~d Cd( cd
(4 c1 ( cC
.-004 *do.t .oo.0.0
o 0 0 0 0C 0 0 0 0 000 0 0Cd0 0-' 0 00000oa o AS ~~o coHYoA oA oAc Y HS
U, bl m C4 to- Edb NOz=
0 e q
o2202
(4 C4 C4 C4 in (4 .40 ° °4 0 ° ° °0 0 022 ooE0 000 C4 0 C -
0) 08
X o 0 0 ' a o% o. o. e o. 00- o._ o . oo. eq00-ugo B -oo oo oo o o ooo ooo
a)~~~~~~~~~~~~~~~~~~~~~~~~~e
w FI0
01 0 -CE)5 4.1~~~~~~~~~~~~i4. i J4O~~~~~~W la IWO
00 W) W,)o. 0o 0o. Wc 0WW 0.m o. 0s 0m
a)~~~~~~~~~~~~~~~. -
Mo I A~~~~~~~~~C W) m C4 8 t08S Wd-1)% ' ~4tf t'.U) ' 4'. 4'I!1) -- f)l)4i)41 1) i~I)0
'1)0%if) ~~~0 0 00 eq 0 0 0 0ee 00 00 0 OeOf
-- - -v - eq _q i4) (4) eq eqeq(4) 0 eq -4 oq oeq_e
- -oo. o. -o-.-.-.-. ----.oo.o.o. o. -. oooo.
0 - - - eq - -
gA-Q-0 0- 0 -) 0 0 - 0oa.
pO ~ ~ ~ ~ 4 00 0 00 00''0>8a eqeq> -- 0 (''80 '0 §
eq eq eq eq eq - -- - - - -g ---g - 5
q ) 00 'oo' 0o o o o 4o ga a" oa (E) ie(f -X > 44(4> o
704)
a- -
0 .(4-
- a. .0
0
4._ . _.
.bQ0 a) 0
1..U)
Cd
a- 4
%a. .. 4)
8 Ua)
a- b
(4
0.
.0 .0
co CO
.0 4J
L r Cd
a)
v-4
'0
'0 a'0 0 4a-~~~~~c
4)A ] =
0 tg-Z tt
z w
.0
I
I4
.9
.C6
cII
UW I! 0 '0 Wm 0 % 0 0 0 0 0 00'0'c '
aa a eqe seq eqe eq e eqe q qeq eq eqqe eqeqn - eq ~eqeq *
"I ~~~~~~~~~~~~~~~~~~~~~~~~~~CIOk tU4 oo 0 eq ( 0% -to %o'0 07% o0 eq. 0 w =%0%
'0eq -eq eIq eq eq e q eqm m
ain, <
+4iU) '0
862
a)
Ci)
.0
~0
t)
44
a)
U-
V"
"4
0-
04
_ eq (44 U)'NO 00 ON - e ) 4 U)'IOt- 00 0%0 - eq- - - - -_- - - e eq eq
I
.4114
-4
i
INTRAVASCULAR IIEMOLYSIS OF EXERCISE
TABLE III
Further observations in 2 subjects showing hemoglobinuria at end of the marathon race
Plasma Urine
Subject number* Time Hemoglobin Bilirubin Volume Hemoglobin Total protein
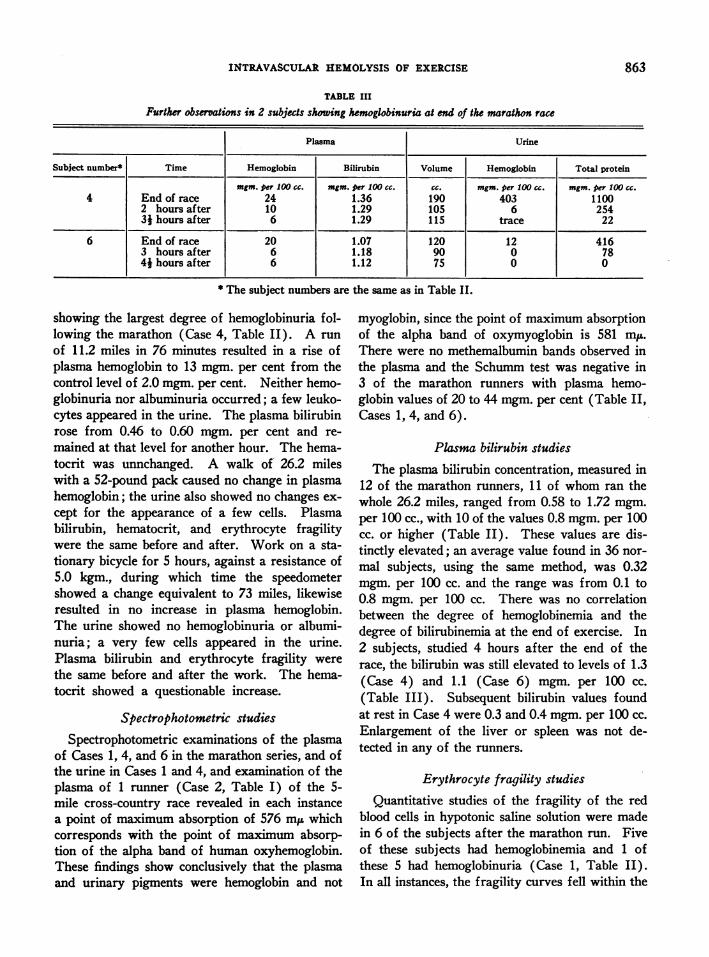
mgm. per 100 cc. mgm. per 100 cc. cc. mgm. per 100 cc. mgm. per 100 cc.4 End of race 24 1.36 190 403 1100
2 hours after 10 1.29 105 6 2543} hours after 6 1.29 115 trace 22
6 End of race 20 1.07 120 12 4163 hours after 6 1.18 90 0 784j hours after 6 1.12 75 0 0
* The subject numbers are the same as in Table II.
showing the largest degree of hemoglobinuria fol-lowing the marathon (Case 4, Table II). A runof 11.2 miles in 76 minutes resulted in a rise ofplasma hemoglobin to 13 mgm. per cent from thecontrol level of 2.0 mgm. per cent. Neither hemo-globinuria nor albuminuria occurred; a few leuko-cytes appeared in the urine. The plasma bilirubinrose from 0.46 to 0.60 mgm. per cent and re-mained at that level for another hour. The hema-tocrit was unnchanged. A walk of 26.2 mileswith a 52-pound pack caused no change in plasmahemoglobin; the urine also showed no changes ex-cept for the appearance of a few cells. Plasmabilirubin, hematocrit, and erythrocyte fragilitywere the same before and after. Work on a sta-tionary bicycle for 5 hours, against a resistance of5.0 kgm., during which time the speedometershowed a change equivalent to 73 miles, likewiseresulted in no increase in plasma hemoglobin.The urine showed no hemoglobinuria or albumi-nuria; a very few cells appeared in the urine.Plasma bilirubin and erythrocyte fragility werethe same before and after the work. The hema-tocrit showed a questionable increase.
Spectrophotometric studies
Spectrophotometric examinations of the plasmaof Cases 1, 4, and 6 in the marathon series, and ofthe urine in Cases 1 and 4, and examination of theplasma of 1 runner (Case 2, Table I) of the 5-mile cross-country race revealed in each instancea point of maximum absorption of 576 mp whichcorresponds with the point of maximum absorp-tion of the alpha band of human oxyhemoglobin.These findings show conclusively that the plasmaand urinary pigments were hemoglobin and not
myoglobin, since the point of maximum absorptionof the alpha band of oxymyoglobin is 581 miu.There were no methemalbumin bands observed inthe plasma and the Schumm test was negative in3 of the marathon runners with plasma hemo-globin values of 20 to 44 mgm. per cent (Table II,Cases 1, 4, and 6).
Plasma bilirubin studiesThe plasma bilirubin concentration, measured in
12 of the marathon runners, 11 of whom ran thewhole 26.2 miles, ranged from 0.58 to 1.72 mgm.per 100 cc., with 10 of the values 0.8 mgm. per 100cc. or higher (Table II). These values are dis-tinctly elevated; an average value found in 36 nor-mal subjects, using the same method, was 0.32mgm. per 100 cc. and the range was from 0.1 to0.8 mgm. per 100 cc. There was no correlationbetween the degree of hemoglobinemia and thedegree of bilirubinemia at the end of exercise. In2 subjects, studied 4 hours after the end of therace, the bilirubin was still elevated to levels of 1.3(Case 4) and 1.1 (Case 6) mgm. per 100 cc.(Table III). Subsequent bilirubin values foundat rest in Case 4 were 0.3 and 0.4 mgm. per 100 cc.Enlargement of the liver or spleen was not de-tected in any of the runners.
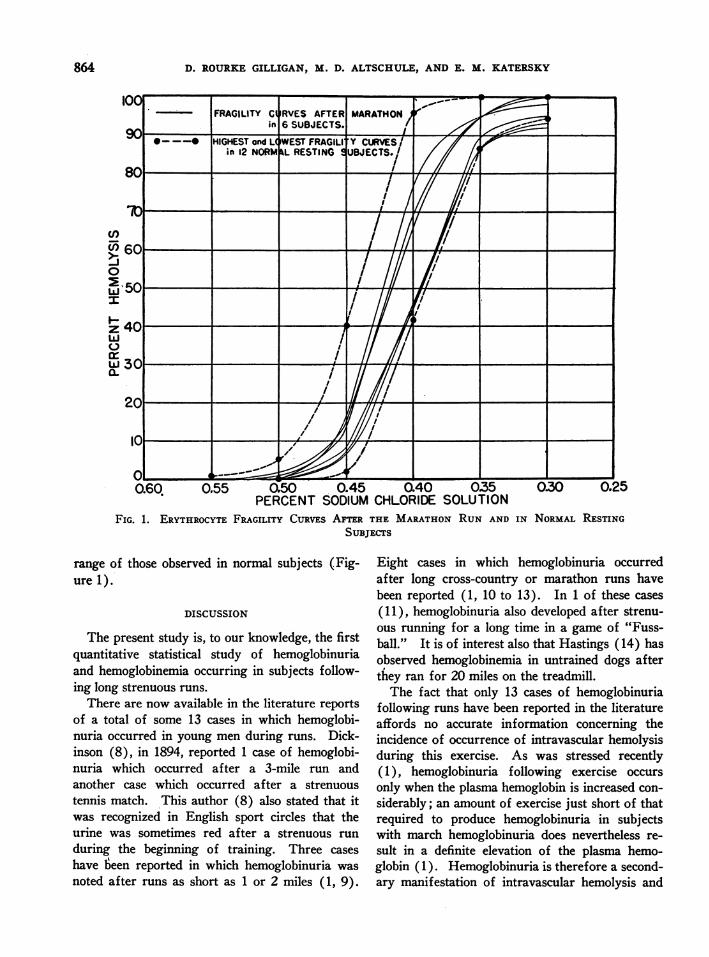
Erythrocyte fragility studiesQuantitative studies of the fragility of the red
blood cells in hypotonic saline solution were madein 6 of the subjects after the marathon run. Fiveof these subjects had hemoglobinemia and 1 ofthese 5 had hemoglobinuria (Case 1, Table II).In all instances, the fragility curves fell within the
863
D. ROURKE GILLIGAN, M. D. ALTSCHULE, AND E. M. KATERSKY
PERCENT SODIUM CHLORIDE SOlUTIONFIG. 1. ERYTHROCYTE FRAGILITY CURVES ATM THE MARATHON RUN AND IN NORMAL RESTING
SUBJECTS
range of those observed in normal subjects (Fig-ure 1).
DISCUSSION
The present study is, to our knowledge, the firstquantitative statistical study of hemoglobinuriaand hemoglobinemia occurring in subjects follow-ing long strenuous runs.
There are now available in the literature reportsof a total of some 13 cases in which hemoglobi-nuria occurred in young men during runs. Dick-inson (8), in 1894, reported 1 case of hemoglobi-nuria which occurred after a 3-mile run andanother case which occurred after a strenuoustennis match. This author (8) also stated that itwas recognized in English sport circles that theurine was sometimes red after a strenuous runduring the beginning of training. Three caseshave teen reported in which hemoglobinuria wasnoted after runs as short as 1 or 2 miles (1, 9).
Eight cases in which hemoglobinuria occurredafter long cross-country or marathon runs havebeen reported (1, 10 to 13). In 1 of these cases(11), hemoglobinuria also developed after strenu-ous running for a long time in a game of "Fuss-ball." It is of interest also that Hastings (14) hasobserved hemoglobinemia in untrained dogs afterthey ran for 20 miles on the treadmill.The fact that only 13 cases of hemoglobinuria
following runs have been reported in the literatureaffords no accurate information concerning theincidence of occurrence of intravascular hemolysisduring this exercise. As was stressed recently(1), hemoglobinuria following exercise occursonly when the plasma hemoglobin is increased con-siderably; an amount of exercise just short of thatrequired to produce hemoglobinuria in subjectswith march hemoglobinuria does nevertheless re-sult in a definite elevation of the plasma hemo-globin ( 1 ). Hemoglobinuria is therefore a second-ary manifestation of intravascular hemolysis and
864

INTRAVASCULAR HEMOLYSIS OF EXERCISE 8
occurs only in instances with the higher concen-trations of plasma hemoglobin.The single most pertinent published observation
concerning the incidence of occurrence of hemo-globinuria during strenuous runs is that of Jun-dell and Fries (13) in 1911. During a statisticalstudy of the albuminuria of exercise, these authorsnoted 4 cases of hemoglobinuria among 39 sub-jects who ran distances of 10,000 meters (6.2miles) to 42,194 meters (26.2 miles). In these 4cases the urine was described as bright red, brown-red, or dark blood-red, and all gave strongly posi-tive guaiac reactions; there were no red cells orvery few in the urinary sediments. The urinesin 2 of these cases were examined spectroscopicallyand showed oxyhemoglobin bands; in 1 instance,the plasma of a blood sample, drawn 1 hour afterthe run, was reddish brown and showed oxyhemo-globin bands on spectroscopic examination. Ex-aminations of the urine for hemoglobin were notmade following runs in any of the 39 competitorsexcept those 4 cases in which the urines wereobviously red, nor were plasma examinationsmade in any but the 1 case noted (13). It is im-portant that the incidence of frank hemoglobinuria,i.e., reddish discoloration of the urine due to dis-solved hemoglobin, after long-distance runs, i
Jundell and Fries' series (13) and in our study(Table II) is quite similar. Jundell and Friesobserved 4 cases of frank hemoglobinuria in aseries of 39 subjects who ran from 6.2 to 26.2miles, while 3 cases of frank hemoglobinuria and1 case in which a trace of hemoglobin was de-tected by chemical analysis were found in ourseries of 26 subjects running from 10.0 to 26.2miles.'
1 Mr. William T. Wright of the John Hancock LifeInsurance Company recognized an additional instance ina marathon runner, during the course of a study on theurine of runners in the North Medford Road Race (20miles) on March 14, 1942. A sample of urine was ob-tained from J. M. which gave positive tests for albuminand hemoglobin, although it contained no erythrocytes;his urine was normal immediately before the race andagain 24 hours after it. Through the cooperation of Mr.Wright, we were able to study J. M. after the B. A. A.Marathon of 1942 and obtained the following data: J. M.ran the 26 miles and 385 yards in 3 hours, 3 minutes, and40 seconds. Thirty minutes later he voided 37 cc. ofdark amber urine with a specific gravity of 1.032 andcontaining a large amount of albumin, a few leukocytes
If the urine alone had been studied after therace in the 11 freshmen running races of 2.6 to2.8 miles in approximately 15 minutes (TableI), no evidence of any intravascular hemolysiswould have been detected; however, the plasmahemoglobin studies revealed slight but definite in-travascular hemolysis in 5 of the 11 men. Simi-larly, during the 4.5 to 5.1 mile runs, performedby the varsity team in approximately 23 to 31minutes, hemoglobinuria occurred in only 1 of the11 subjects, whereas a considerable amount ofhemoglobinemia, at times sufficient to give a defi-nite reddish tinge to the plasma and to be detect-able with the Zeiss hand spectroscope, was presentin 5 of the 11 subjects at the end of the race. Theincidence of detectable hemoglobinuria after the2.6 to 5.1 mile runs in college men, namely, 1 casein 22 subjects, would certainly be too low to dem-onstrate the benign physiological nature of the in-travascular hemolysis of exercise; however, theincidence of hemoglobinemia, namely, 10 cases in22 subjects, is sufficiently high to suggest thatintravascular hemolysis during such exercises isquite normal.A quantitative study of plasma hemoglobin re-
vealed a strikingly high incidence of increased in-travascular hemolysis in those subjects who ran26.2 miles in the marathon race; 18 of the 22 menstudied had suspiciously reddish to definitely red-dish plasmas and quantitative hemoglobin meas-urements revealed plasma hemoglobin values dis-tinctly above normal (Table II). Four of thesubjects running in the marathon showed freehemoglobin in the urine; these 4 were the subjectswith the highest plasma hemoglobin values, namely,20 mgm. to 44 mgm. per 100 cc. at the end of therace (Table II).Although hemoglobinuria in exercise occurs
only in the cases with higher plasma hemoglobinvalues, the plasma level at which hemoglobinuria
and granular casts, and rare erythrocytes. This urinecontained 15 mgm. of hemoglobin per 100 cc. An hourand one-half later his urine still contained a small amountof albumin but no hemoglobin. He was a 32-year-oldwhite mechanic who had noted the occurrence of "black"urine 5 years ago, when he began to run distances over 5miles. There were no associated symptoms of any sort;hemoglobinuria did not occur after exposure to cold.Physical examination was entirely normal; the bloodHinton and Kahn reactions were negative.
865
D. ROURKE GILLIGAN, M. D. ALTSCHULE, AND E. M. KATERSKY
occurs following exercise appears to be consider-ably lower than the level required to producehemoglobinuria in normal man when hemoglobin isinjected intravenously (3, 15). In the marathonrunners, a somewhat higher level of plasma hemo-globin than that found at the end of the race mayhave obtained earlier in the run, for work is per-formed most rapidly earlier in the race, especiallyin those subjects who take some 4 or more hoursto finish the course of 26.2 miles. Whereashemoglobinuria was observed in 4 of 5 urines fromsubjects with plasma hemoglobin levels of 20 to44 mgm. per cent at the end of the 26 mile mara-thon race, hemoglobinuria was detected in only 1of the 4 urines from subjects with plasma hemo-globin levels of 22 to 47 mgm. per cent after the5-mile cross-country race. The plasma hemo-globin values were probably at their highest pointat the end of these shorter cross-country races.
There are not available sufficient statistical datato demonstrate to what extent exercises other thanrunning lead to physiological intravascular hemol-ysis. However, there are reports indicating thatvery strenuous marching may lead to hemoglobi-nemia and hemoglobinuria in normal individuals.Albu and Caspari (16) reported the occurrence ofreddish yellow and dark red urines, showing oxy-hemoglobin bands by spectroscopic analysis, in 2of 3 subjects after a most strenuous march of 202kilometers (125 miles) in an endurance walkingcontest. Feigl (17) examined the plasma spec-troscopically and the urine by the qualitative benzi-dine test for hemoglobin in 27 men after an armypack march of 35 kilometers (21.7 miles); he re-ported finding oxyhemoglobin in the serum of 6and a positive benzidine test in the urine of 19 ofthe 27 cases after the march. Of the urines con-taining no erythrocytes which showed a positivebenzidine test, some were voided in cases in whichthere was no oxyhemoglobin or hematin detectedin the serum. Because of the qualitative nature ofthe study, these findings are difficult to interpret,especially since there is no mention of any reddishdiscoloration of the serum or urine in any of thecases. Further statistical studies of the incidenceof intravascular hemolysis in normal individualsduring marching would be of interest. In thepresent study, the marathon runner (Case 4, TableII) with the most marked hemoglobinuria showed
no evidence of intravascular hemolysis after a 26-mile walk with a 52-pound pack.
It has been questioned by several authors (18to 20) whether the red pigment of the urine inmarch hemoglobinuria is not the muscle pigmentmyoglobin rather than hemoglobin. Our ownstudies in 3 previously reported cases of marchhemoglobinuria (1), and a similar spectrophoto-metric observation by Witts (21) in his case,showed, however, that the plasma and urinary pig-ments in these cases were hemoglobin and notmyoglobin. Similarly, in several of the cases ofthe present study, the red pigment of the plasmaand urine was identified spectrophotometrically ashemoglobin and not myoglobin.The mechanism of the intravascular hemolysis
of exercise is obscure (1). Its occurrence hasbeen recorded in man only following the exerciseof walking or running, and in dogs, only after run-ning. Equal or more strenuous exercise of othertypes in man does not cause it (1). There arereported in the literature 3 cases of hemoglobinuriafollowing walks in the usual upright position, inwhich cases hemoglobinuria did not occur follow-ing similar or longer walks in a slightly kyphoticposition (1, 22 to 24). Most subjects with marchhemoglobinuria show no lordosis of the lumbarspine (1), and in the present study, there appearedto be no correlation between body build or stand-ing posture and the occurrence of intravascularhemolysis during runs.Although these evidences of hemolysis, namely,
the appearance of red plasma and less frequentlyred urine, occur after strenuous runs, the totalamount of blood destroyed intravascularly is un-doubtedly very small. It may be calculated thatthe hemoglobin from less than 10 cc. of normalblood is sufficient when released into the plasmato cause a hemoglobinemia of approximately 50mgm. per 100 cc. of plasma in a subject with ablood volume of 5 liters and a normal hematocrit.The findings of a previous study (3), in whichhemoglobin in solution was injected intravenouslyin normal subjects, accord with this statement.These injection studies also demonstrated that theplasma hemoglobin level does not become normalagain for about 5 hours after the injection of suffi-cient hemoglobin to cause a plasma level of 50mgm. per 100 cc. Since the plasma hemoglobin
866

INTRAVASCULAR HEMOLYSIS OF EXERCISE
level was not greater than 50 mgm. per 100 cc.after the runs in any of the subjects of the presentreport, and since increased levels were not main-tained long, it must be concluded that the hemo-globin of not more than approximately 10 cc. ofblood was destroyed. This is approximately trueeven when there was some hemoglobinuria. Thegreatest urinary hemoglobin output occurred inCase 4 after the marathon; the first urinary speci-men voided after the race contained a total of0.77 gram hemoglobin and the following 2 speci-mens contained a total of less than 0.01 gram.The total hemoglobin excreted in the urine there-fore would be contained in about 5.0 cc. of normalblood. These findings are in marked contrast tothose in dogs in which anemia, reticulocytosis,and increased excretion of bilirubin may occurafter long runs every day for several days (25 to28). Whether there was blood destruction in oursubjects other than that which occurred intra-vascularly cannot be answered by the data of thispaper. Addition of erythrocytes to the circulatingblood during prolonged exercise has been re-ported (29 to 31). The hematocrits following ex-ercise in our subjects after the marathon wereentirely normal; no control values were obtainedbefore the run.The increased concentrations of bilirubin in the
plasma after the marathon race may have been dueto decreased liver function consequent to hepaticischemia during the exercise. The fact that thehyperbilirubinemia occurred in the absence as wellas in the presence of hemoglobinemia demonstratesthat it did not result from intravascular hemolysis;the degree and duration of hemoglobinemia werein no instance sufficient to give rise to such highlevels of bilirubinemia (3). Although we have notbeen able to find reference in the literature tohyperbilirubinemia after exhausting exercise, thereare reports of hyperbilirubinemia in man duringanoxia at high altitudes (32) and of impairedbilirubin excretion in dogs during anoxia from lowoxygen tensions (33).
It has been repeatedly demonstrated that normalindividuals excrete albumin and formed elementsin the urine after strenuous exercise (13, 34 to38). The incidence of occurrence of albuminuria,and the excretion of formed elements in the urinefollowing the runs reported here, accord with thefindings of Jundell and Fries (13). As observed
in Tables I and II, the urinary findings afterstrenuous exercise may be quite the same as ob-served in nephritis; in subjects with normal kid-neys, however, albuminuria disappears and theurinary sediment becomes normal in one to a fewhours after the cessation of the exercise. In cer-tain instances, the specific gravity of a urine col-lected following strenuous exercise may be suffi-ciently high to allow differentiation of this urinefrom the urine in chronic glomerular nephritis.Sometimes, however, the specific gravities follow-ing exercise may be within the range usually ob-served in advanced chronic glomerular nephritis.In 2 of the cases reported above (Table III) whichwere studied for some hours following the end ofexercise, the urine became completely normal 3hours after the termination of runs which pro-duced albuminuria, hemoglobinuria, and the ex-cretion of formed elements.The frequent occurrence' of these temporary
renal changes manifested by albuminuria and theappearance of abnormal elements in the urinarysediment, and by decreased glomerular filtration(38) during repeated strenuous exercise overmany years, has never been shown to result in anypermanent kidney damage. Similarly, the re-peated occurrence of the relatively mild hemoglo-binemia and hemoglobinuria following exercisehas never been known to result in damage to thekidneys.2The importance of differentiating the physiolog-
ical intravascular hemolysis of exercise frompathological conditions leading to the passage ofred urine is obvious. The benign nature of thealbuminuria of exercise has been recognized fora long time. That the passage of a red urine fol-lowing strenuous runs or walks may be equally asbenign has not been generally recognized, how-ever. The findings of this study are of particularimportance at this time, when large numbers ofyoung men in the armed forces are accomplishingextremely strenuous physical feats.
SUMMARY AND CONCLUSIONS
1. Studies of intravascular hemolysis, as meas-ured by the appearance of hemoglobinemia and
2As suggested previously (1), alkalinization of theurine during the period of hemoglobinuria provides a pre-cautionary measure against precipitation of hemoglobinin the renal tubules.
867

D. ROURKE GILLIGAN, M. D. ALTSCHULE, AND E. M. KATERSKY
hemoglobinuria, have been made in groups ofathletes following 2.6 to 26.2-mile cross-countryruns. The plasma bilirubin, the red cell fragility,the hematocrit, and the urinary albumin and sedi-ment were also studied.
2. Hemoglobinemia was observed in 5 of 11young athletes who ran 2.6 to 2.8 miles, in 5 of 11athletes who ran 4.5 to 5.1 miles, and in 18 of 22men who ran 26.2 miles.
3. Hemoglobinuria was observed in 1 of theseathletes on 3 occasions after 5-mile runs. Hemo-globinuria occurred in 4 of the 22 men who ran26.2 miles; these urines were brownish to verydark burgundy red. Observations on 1 of these 4athletes showed the occurrence of hemoglobinuriaagain after a 20-mile run.
4. The occurrence of intravascular hemolysisappeared to be unrelated to the age, body build, orstanding position of the runners, or to the numberof years or state of their training.
5. Hemoglobinemia and hemoglobinuria disap-peared in a few hours after the end of the run. Ithas been calculated that the amount of blood de-stroyed intravascularly is very small.
6. The plasma bilirubin was distinctly elevatedafter the marathon run. The significance of thishyperbilirubinemia is discussed.
7. Quantitative studies revealed normal erythro-cyte fragility after the marathon runs.
8. Transient albuminuria was observed fre-quently after the 2.6 to 5.1-mile runs and in everyinstance after the marathon run. Transient uri-nary excretion of formed elements occurred fre-quently after the shorter runs and in almost everyinstance after the marathon runs.
9. Hemoglobinemia sometimes accompanied byhemoglobinuria occurs in man with sufficient fre-quency after strenuous runs to be consideredphysiological under these conditions. This in-travascular hemolysis after strenuous runs iscomparable in its apparently benign nature to thealbuminuria of exercise. The importance of dif-ferentiating this condition from pathological statesleading to the passage of red urine is obvious.
We wish to acknowledge the cooperation of Dr. An-drew W. Contratto of the Department of Hygiene,Harvard University, Mr. Jaakko J. Mikkola, TrackCoach, Harvard University, Mr. Thomas J. Kanaly ofthe Boston Athletic Association, and Mr. William T.
Wright, in arranging for the collection of the materialof study, and the assistance in the field and laboratory ofDrs. Howard A. Frank, Paul M. Zoll, and NormanZamcheck.
BIBLIOGRAPHY
1. Gilligan, D. R., and Blumgart, H. L., March hemo-globinuria. Studies of the clinical characteristics,blood metabolism and mechanism; with observa-tions on three new cases and review of the litera-ture. Medicine, 1941, 20, 341.
2. Ham, T. H., Studies on destruction of red blood cells.I. Chronic hemolytic anemia with paroxysmal noc-turnal hemoglobinuria: An investigation of themechanism of hemolysis, with observations on fivecases. Arch. Int. Med., 1939, 64, 1271.
3. Gilligan, D. R., Altschule, M. D., and Katersky,E. M., Studies of hemoglobinemia and hemo-globinuria produced in man by intravenous injec-tion of hemoglobin solutions. J. Clin. Invest.,1941, 20, 177.
4. Bing, F. C., and Baker, R. W., Determination ofhemoglobin in minute amounts of blood by Wu'smethod. J. Biol. Chem., 1931, 92, 589.
5. Bing, F. C., Purification of benzidine, and an im-proved reagent, for estimating hemoglobin in blood.J. Biol. Chem., 1932, 95, 387.
6. Malloy, H. T., and Evelyn, K. A., The determinationof bilirubin with the photoelectric colorimeter. J.Biol. Chem., 1937, 119, 481.
7. Hunter, F. T,, A photoelectric method for quantita-tive determination of erythrocyte fragility. J.Clin. Invest., 1940, 19, 691.
8. Dickinson, L., Haemoglobinuria from muscular ex-ertion. Tr. Clin. Soc. London, 1894, 27, 230.
9. Attlee, W. H. W., Haemoglobinuria following exer-tion. Lancet, 1937, 1, 1400.
10. Finny, C. M., Functional hemoglobinuria. Brit. M. J.,1926, 2, 685.
11. Hantzschel, K., Ein Fall von echter Marschhimo-globinurie. Med. Klin., 1939, 35, 976.
12. Fisher, A. M., and Bernstein, A., March hemoglobin-uria. A case report. Bull. Johns Hopkins Hosp.,1940, 67, 457.
13. Jundell, I., and Fries, K. A. E., Die Anstrengungs-albuminurie. Eine Studie iiber die Einwirkungmaximaler Korperanstrengungen (des Sports unddes Trainings) auf die Nieren. Nord. med. Arkiv.,1911, 44, Afd. II. N:r 2, 1.
14. Hastings, A. B., The physiology of fatigue. Physico-chemical manifestations of fatigue in the blood.Public Health Bull., 117, 1921.
15. Ottenberg, R., and Fox, C. L., Jr., The rate of re-moval of hemoglobin from the circulation and itsrenal threshold in human beings. Am. J. Physiol.,1938, 123, 516.
16. Albu, A., and Caspari, W., Bericht fiber die Unter-suchungen an den Dauergehern beim Distanzmarsch
868

INTRAVASCULAR HEMOLYSIS OF EXERCISE
Dresden-Berlin am 18/19 Mai 1902. Deutsche med.Wchnschr., 1903, 29, 252.
17. Feigl, J., Chemische Blutuntersuchungen an derTeilnehmern eines Armee-Gepackmarsches. I.tJber Umsatz und Ausscheidung von Blutfarbstoff.Hamoglobinamie, Hamatinamie und Hamoglobin-urie. Biochem. Ztschr., 1916, 76, 88.
18. Foerster, A., Ueber Marschhamoglobinurie. Miinchen.med. Wchnschr., 1919, 66, 554.
19. Watson, E. M., and Fischer, L. C., Paroxysmal"march" hemoglobinuria. With a report of a case.Am. J. Clin. Path., 1935, 5, 151.
20. Hamburger, L. P., and Bernstein, A., Chronic he-molytic anemia with paroxysmal nocturnal hemo-globinuria. Am. J. M. Sc., 1936, 192, 301.
21. Witts, L. J., The paroxysmal haemoglobinurias.Lancet, 1936, 2, 115.
22. Porges, O., and Strisower, R., Offizielles Protokollder k.k. Gesellschaft Aerzte in Wien. Ein Fallvon Marschhamoglobinurie. Wien. klin. Wchnschr.,1913, 26, 193.
23. Porges, O., and Strisower, R., tVber Marschhamo-globinurie. Deutsches Arch. f. klin. Med., 1914,117, 13.
24. Schellong, F., Untersuchungen uiber Marschhamoglo-binurie; ihre Beziehung zur Kaltehamoglobinurieund orthostatischen Albuminurie. Ztschr. f. d. ges.exper. Med., 1923, 34, 82.
25. Broun, G. O., Blood destruction during exercise. II.Demonstration of blood destruction in animals ex-ercised after prolonged confinement. J. Exper.Med., 1923, 37, 113.
26. Broun, G. O., Blood destruction during exercise. III.Exercise as a bone marrow stimulus. J. Exper.Med., 1923, 37, 187.
27. Broun, G. O., Blood destruction during exercise. IV.The development of equilibrium between blood de-
struction and regeneration after a period of train-ing. J. Exper. Med., 1923, 37, 207.
28. McMaster, P. D., Broun, G. O., and Rous, P., Studieson the total bile. I. The effect of operation, exer-cise, hot weather, relief of obstruction, intercur-rent disease and other normal and pathological in-fluences. J. Exper. Med., 1923, 37, 395.
29. Chang, H. C., and Harrop, G. A., Jr., The deter-mination of the circulating blood volume with car-bon monoxide. J. Clin. Invest., 1928, 5, 393.
30. Keys, A., and Taylor, H., The behavior of the plasmacolloids in recovery from brief severe work andthe question as to the permeability of the capil-laries to proteins. J. Biol. Chem., 1935, 109, 55.
31. Kaltreider, N. L., and Meneely, G. R., The effect ofexercise on the volume of the blood. J. Clin.Invest., 1940, 19, 627.
32. Hurtado, A., Studies at high altitude. Blood ob-servations on the Indian natives of the PeruvianAndes. Am. J. Physiol., 1932, 100, 487.
33. Barron, E. S. G., Bilirubinemia. Medicine, 1931, 10,77.
34. Leube, W., Ueber die Aussheidung von Eiweiss imHarn des gesunden Menschen. Arch. f. path. Anat.u. Physiol. u. f. klin. Med., 1878, 72, 145.
35. McFarlane, A., The presence of albumin and casts inthe urine of football players. M. Rec., 1894, 46,769.
36. Frenkel-Tissot, H. C., Zur Frage der sportlichenAlbuminurie, besonders bei Skifahrern. Ztschr. f.klin. Med., 1921, 90, 54.
37. Edwards, H. T., Richards, T. K., and Dill, D. B.,Blood sugar, urine sugar and urine protein in ex-ercise. Am. J. Physiol., 1931, 98, 352.
38. Covian, F. G., and Rehberg, P. B., Uber die Nieren-funktion wahrend schwerer Muskelarbeit. Skan-dinav. Arch. f. Physiol., 1936, 75, 21.
869