musculoskeletal tissues response to diseases and injury
DESCRIPTION
musculoTRANSCRIPT

MUSCULOSKELETAL TISSUES RESPONSE TO DISEASES AND INJURY

INTRODUCTION
BONE EPIPHYSEAL PLATE SYNOVIAL JOINTS SKELETAL MUSCLE

A. BONE
There are just 4 basic ways in which bone can react to abnormal conditions:
1. Local death
2. Alteration of bone deposition
3. Alteration of bone resorption
4. Mechanical failure (fracture)
1. Local Death
When an area of bone is completely deprived of its blood suply, its reaction is local death (avascular necrosis of bone).
the resultan segment of dead bone an abnormal condition in itself and incites further reaction from the surrounding living tissue
Bone that remains alive can react to abnormal condition (an alternation of deposition or resorption, or both)

2. Alternation of bone deposition
A. Generalized Reactions
1. Osteopetrosis (Marble bones)
Bone deposition is normal but bone resorption is defective.
2. Acromegaly
Bone deposition is increase by excessive intramembranous ossification from the periosteum.

Marble Bones
This show an example of a generalized increase in bone. Increased radiographic density in all bones
B. Localized Reactions:
1. Work Hypertrophy
The bone react to the extra stresses and strain of increased function by increased bone
deposition.
Varus deformity of the foot the fifth metatarsal
hypertrophies.
2. Degenerative Osteoarthritis
Subchondral sclerosis
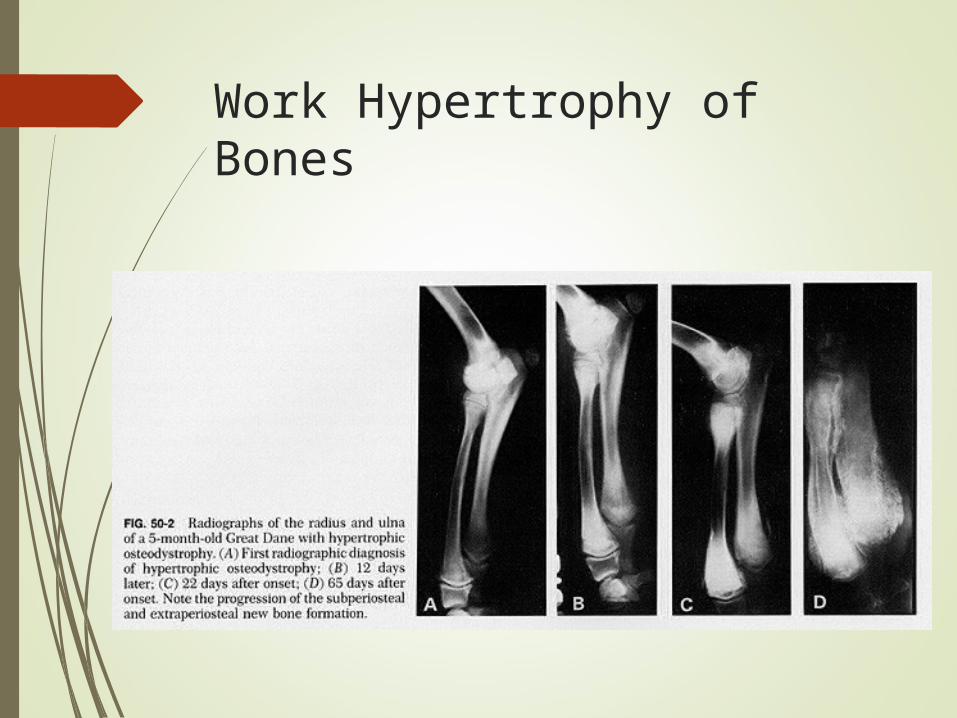
Work Hypertrophy of Bones

3. Fractures
The periosteum and endosteum react to bony injury with localized increased in bone
deposition to form callus.
4. Infection
The periosteum reacts to infection by deposition of new bone.
5. Osteosclerotic Neoplasm
Osteoid osteoma (benign neoplasm)
Osteosarcoma (malignant neoplasm)

3. Alternation of bone resorption
A. Generalized Reactions
1. Osteoporosis
Bone deposition is decreased because of decreased formation of matrix and resorption is increased.
Examples : osteogenesis imperfecta, disuse osteoporosis, steroid induced osteoporosis, postmenopausal osteoporosis.
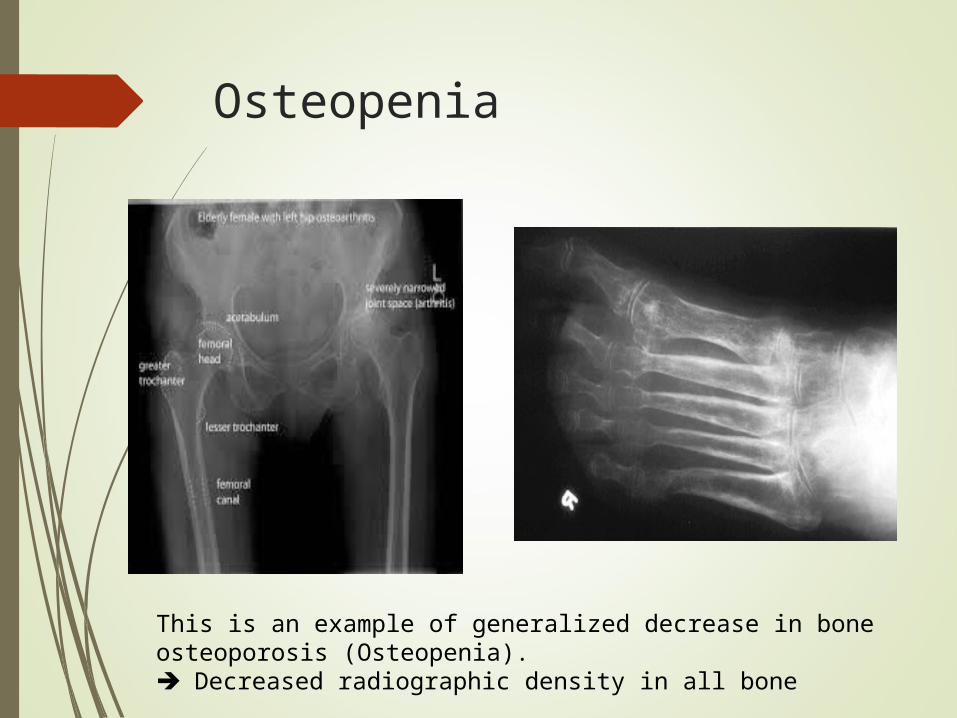
Osteopenia
This is an example of generalized decrease in bone osteoporosis (Osteopenia). Decreased radiographic density in all bone

2. Rickets in Children and Osteomalacia in Adults
Although the osteoblastic formation of matrix is normal, there is decreased calcification (hypocalcification) of the matrix with a resultant
decreased in the amount of calcified bone.

B. Localized Reactions
1. Disuse Atrophy (disuse osteoporosis)
Decreased bone deposition whereas the bone resorption continues unchanged.
2. Rheumatoid Arthritis
The bone reacts to the periarticular soft tissue inflammation of RA by decreased bone
deposition and possibly increased bone resorption.
Decreased in functiondisuse atrophy

4. Mechanical Failure of Bone (Fractures)
The periosteum and endosteum react to bony injury with localized increased in bone deposition to form callus.

II. EPIPHYSEAL PLATES
Normal growth requires:
1.The plate to have an intact structure and a normal blood supply
2. intermittent pressures normal physical activity.
There are just 3 ways in which an epiphyseal plate can react:
1. increased growth
2. decreased growth
3. torsional growth
1. Increased in Growth
A. Generalized
1. Arachnodactyly (Hyperchondroplasia) (Marfan`s Syndrome)
There is excessive cartilaginous growth (hyperchondroplasia) in all epiphyseal plates.
2. Pituitary Gigantism
Excessive growth hormone from an eosinophilic adenoma of the anterior pituitary gland.

Arachnodactyly, hyperchondroplasia, Marfan’s Syndrome

B. Localized
1. Chronic Inflammation
The prolonged hyperemia stimulates local growth, such as chronic osteomyelitis and
rheumatoid arthritis.
2. Displaced Fracture of the shaft of a Long Bone
The nutrient artery to the shaft of a long bone is disrupted a temporary compensatory hyperemia at the epiphyseal ends.
3. Congenital Arteriovenous Malformations
The continuing hyperemia stimulation the epipheseal plates.

2. Decreased in Growth
A. Generalized
1. Achondroplasia
There is deficient cartilaginous growth
2. Pituitary Dwarfism (Lorain type)
Deficient growth hormone
3. Rickets
Hypocalcification of the preosseus cartilage of the epiphyseal plate in the zone of calcifying cartilage.

Achondroplasia

B. Localized
1. Disuse Retardation
2. Physical Injury
Fracture local cessation of growth
3. Thermal Injury
Epiphyseal plate is sometimes destroyed either by local cold (frostbite) or by local heat
(burns).
4. Ischemia
5. Infection
Chondrolytic action of pus destroy epiphyseal plate.

3. Torsional Growth
When a growing long bone and its epiphyseal plate are subjected to either continual or intermittent twisting forces, the bone gradually becomes twisted.
The torsional deformity in the long bones occurs through torsional growth in the involved epiphyseal plate and can ussualy be reversed by applying corrective torsional force in the opposite direction.

III. SYNOVIAL JOINTS
In a normal Synovial joint the smooth and reciprocally shaped cartilaginous, painless movement
The joint capsule
stretching
Increased fluid pressure
sensitive

Reaction of articular cartillage
Limited healing
Ro: width/thickness
Change in the intercellular cement substance of the matrix &subsequent uncovering of the collagen fibril

- Rheumatoid arthritis
- Infections
- Ankylosing
- Prolonged immobilization
of synovial joint
- Continous compression
of articular cartillage
- Intra-articular Injections of Hydrocortison
Change in the intercellular cement substance of the matrix &subsequent uncovering of the collagen fibrilPremature aging of cartilage
Previous destruction of cartilage
Incongruity

Possibility of healing and regeneration of articulation
Rest & Motion

Reaction of Synovial Membrane
Nutrition and lubrication
Abnormality 3ways:
• An effusion
• Hypertrophy
• By forming adhesions between itself and the articular cartilage
Joint effusion:
a. Serous: mild sprain
b. Inflammatory exudate: synovitis and RA
c. Grossly purulent: septic arthritis
d. Hemorrhagic: severe injury or hemophilia

Reaction of joint capsule & ligament
Fibrous joint capsule and ligament provide stability and undesired movement
Abnormal conditions:
Undully strecthed and elongated (joint laxity)
Becoming tight and shortened (joint contracture)

IV. SKELETAL MUSCLE
The skeletal muscle reacts to many disorders and injuries in a limited number of ways including:
1. atrophy
2. hypertrophy
3. necrosis
4. contracture
5. regeneration

1. Disuse Atrophy
Skeletal muscle that is not used normally, reacts by becoming weaker and smaller.
Disorders of the anterior horn cell (poliomyelitis), the peripheral nerve fiber (polyneuritis), the myoneural junction (myasthenia gravis)disuse atrophy.

2. Work Hypertrophy
When a given muscle is repeatedly exercised against resistance stronger and larger (work hypertrophy)

3. Ischemic Necrosis
Occlusion of arteries supplying muscle whether by persistent traumatic vascular spasm, thrombosis, embolism, or a compartement syndrome, result in ischemic necrosis of the muscle.

4. Contracture
If muscle remains in a shortened state for a prolonged period persistent shortening (muscle contracture).
Polymyositis, muscular dystrophy, and cerebral palsy.
Muscle fibers of a necrotic muscle are subsequently replaced by dense fibrous scar tissue (fibrous contracture) joint deformities.

5. Regeneration
Injured muscle fibers may regenerate (sarcolemma, muscle cells, satellite cells).
Partial loss of innervation in a skeletal muscle gain a new motor nerve fiber from the remaining intact nerve fibers.

THANK YOU