module 5: understanding coagulation transfusion training workshop kkm 2012
TRANSCRIPT

Module 5: Understanding coagulation
Transfusion Training WorkshopKKM 2012

Components of Haemostasis
Vessel wall
Platelets
Coagulation Factors
Fibrinolytic factors
Inhibitors

EC TF vWF
Damage to the vessel wall
vWF - collagen and TF exposedM. Laffan

EC
Primary haemostasis
Platelets adhere to vWF-collagen
TF
platelets
vWF
M. Laffan

VIIaEC TF
PL
Xa
Secondary haemostasis
TF-VIIa triggers Xa productionThrombin generation proceeds on PL (platelet) surface
X
M. Laffan

Stable clot formation
fibrin platelets
Stable fibrin-platelet clot is formed
M. Laffan

After clot formation
Thrombin binds to TM and activates PC and TAFIExcess thrombin is neutralized by ATFibrinolysis is activated by plasmin (P)
tPA
Pgn
P Thrombin
APC
T-AT
TM-
TAFI
-
M. Laffan
No good test for haemostasis
The “coagulation screen”
Clotting
PT
APTT
TT
FibrinogenFBC
platelet count

Coagulation screen
Practical but unphysiological
Has limited sensitivity & specificity
Tests a very limited portion of haemostasis

A good bleeding history is the best screening test

A significant bleeding history
Epistaxis not stopped by 10 mins compression or requiring medical attention
Cutaneous haemorrhage or bruising without apparent trauma (esp. multiple/ large)
Prolonged (>15 mins) bleeding from trivial wounds, or in oral cavity or recurring spontaneously within 7 days
Post-operative bleeding
Menorrhagia (esp. from menarche)
Bleeding in the hospitalised patient Bleeding prolonged, delayed or
recurrent; or more rapid than normal? Single site or several sites? Appropriate to injury? Past h/o bleeding? Medications? Diseases? Family history?

Bleeding
Immediate bleeding Defects in primary haemostasis Vascular abnormality
Delayed bleeding Defects in secondary haemostasis

The “coagulation screen”
Clotting
PT
APTT
TT
FibrinogenFBC
platelet count

IX
II
Fibrinogen Fibrin
PK
HMWK
XI
XII
VIIaTF VIII
XV
CONTACT
PT
APTT
TT IIa

IX
II
Fibrinogen Fibrin
PK
HMWK
XI
XII
VIIaTF VIII
XV
CONTACT
PT 17.3 (9.6-11.6)
APTT 28 (26-32)
TT 16 (15-19)
Prolonged PT

Prolonged PT
Factor VII deficiency

IX
II
Fibrinogen Fibrin
PK
HMWK
XI
XII
VIIaTF VIII
XV
CONTACT
PT 10.6 (9.6-11.6)
APTT 65 (26-32)
TT 16 (15-19)
Prolonged APTT

Prolonged APTT
Deficiency factor VIII, IX, XI, XII and contact factors
Inhibitor Specific (FVIII) Non-specific (LA)

IX
II
Fibrinogen Fibrin
PK
HMWK
XI
XII
VIIaTF VIII
XV
CONTACT
PT 26 (9.6-11.6)
APTT 54 (26-32)
TT 16 (15-19)
Prolonged PT and APTT
Prolonged PT and APTT
Deficiency of X or V
Multiple deficiencies Warfarin Factor V and VIII deficiency

IX
II
Fibrinogen Fibrin
PK
HMWK
XI
XII
VIIaTF VIII
XV
CONTACT
PT 10.6 (9.6-11.6)
APTT 29 (26-32)
TT 23 (15-19)
Prolonged TT
Prolonged TT
Thrombin inhibitor Direct (hirudin) Indirect (UFH, LMWH)
Low fibrinogen (<0.8g/L)
Dysfibrinogenemia Congenital Acquired
Hypoalbuminemia
Elevated FDPs

IX
II
Fibrinogen Fibrin
PK
HMWK
XI
XII
VIIaTF VIII
XV
CONTACT
PT 25 (9.6-11.6)
APTT 38 (26-32)
TT 23 (15-19)
All prolonged
All tests prolonged
Inhibitor of thrombin- heparins
DIC
Synthetic failure - liver

Bleeding disorders not detected by routine coagulation screen Mild factor deficiencies von Willebrand disease Factor XIII deficiency Platelet disorders Excessive fibrinolysis Vessel wall disorders Metabolic disorders (e.g. uraemia)

Pre-operative coagulation screening tests BCSH guideline 2008
PPV of abnormal tests 0.03-0.23 No significant increase in bleeding
associated with abnormal tests
Routine pre-op screening is NOT RECOMMENDED
Chee, BCSH guideline 2008

A good bleeding history is still the best screening test

Case 1
En KZ, 45 year-old man
Admitted for ureteric colic
US: Large R ureteric stone with hydronephrosis
Planned for stenting
PT, APTT sent

Case 1 – cont’d
APTT 98 sec PT 12s
Procedure cancelled
Referred to hematologist
APTT mix with normal plasma corrected
FXII assay: 15%

Case 1
FXII deficiency is not associated with bleeding or clotting (no clinical significance)
Required for contact activation for in-vitro laboratory testing
A laboratory nuisance
Waste of time and money investigating a prolonged APTT
Routine pre-op PT, APTT screening is not recommended
A good bleeding history is the best screening test

Case 2
1o year old boy with chronic tonsillitis Planned for tonsillectomy FBC, PT, APTT sent Mother c/o that son has easy bruising
and recurrent epistaxis and she herself has menorrhagia
Hb 12 Plt 243 PT 12.5s (12- 16s) APTT 38s (30- 42s)

Case 2 – cont’d
Since platelet count and PT, APTT all normal
Mother reassured and proceeded with tonsillectomy
During surgery, excessive bleeding noted but controlled with local measures
2 hours post-op, further significant bleeding

Case 2 – cont’d
Returned to OT, cauterization done
2 Packed RBC and 2 FFP transfused; bleeding controlled
Repeat PT, APTT the following day – normal
Refer hematologist

Case 2 – cont’d
Further bleeding history taken
Mother’s blood sample sent
FBC normal PT 13s (12-16) APTT 40s (30- 42)
FVIII 34% (40-150) vWF 30% (50-150)
Son’s results similar to mum’s (on f/u)
Diagnosis: von Willebrand disease type 1

Limited investigation of a patient with a bleeding history
is as inappropriate as Extensive investigation of a patient with no bleeding history

This has led to unnecessary transfusion of blood and blood components
Just think if this was your own child

Normal screening tests results in a false sense of security
Limitations of PT, APTT
Lack sensitivity and specificity
Tests a very limited portion of haemostasis
Can only detect factor levels below 30%

Bleeding disorders not detected by routine coagulation screen Mild factor deficiencies von Willebrand disease Factor XIII deficiency Platelet disorders Excessive fibrinolysis Vessel wall disorders Metabolic disorders (e.g. uraemia)

Case 3
En AP, 58 year-old man
Admitted for CCF
Noted LA thrombus on ECHO
PT 35s INR 2.5 APTT 30s
PT repeated 5x still prolonged
Diagnosis: liver disease or patient on warfarin

Case 3 – cont’d
Anticoagulation not started in view of prolonged PT hence ‘auto-anticoagulated’
Patient had a cardiac arrest and died
Sample sent over to haemostasis laboratory
FVII 5%
Diagnosis: mild FVII deficiency

Isolated prolonged PT
Can only be FVII deficiency

Case 4
En LK, 49 year-old man Known alcoholic liver disease Admitted for chronic cough CXR: RUL cavities and R pleural effusion Planned for pleural tap and biopsy PT 19s (INR 1.5) APTT 45s Request for 2 FFP
Liver disease
PT, APTT only measures the pro-coagulant function
In liver disease, there is parallel reduction in both pro-coagulant factors and anti-coagulant proteins
PT, APTT is not a reliable test to assess bleeding risk in patients with liver disease
Tripodi A, NEJM 2011
INR (International Normalised Ratio)
Was devised and validated to standardise across laboratories the PTs in patients receiving warfarin
Should only be used for monitoring warfarin therapy
Cannot be used for patients with chronic liver disease (unless a different calibration based on plasma from patients with liver disease is developed)
Idem. The INR, J Thromb Haemost 2008

Case 4 – cont’d
Patient underwent pleural tap and biopsy without FFP cover
Outcome: no bleeding complications

Case 5
PL, 35 year-old lady
Known case of APLS with h/o stroke and L DVT
Admitted for elective ovarian cyst removal
Warfarin stopped x 5 days
Switched to LMWH
APTT 79s PT 12.5s (as requested by anaesthetist)

Case 5 – cont’d
Seen by haematologist Explained that APTT prolongation is due
to the lupus anticoagulant (inhibitor) Despite this, 2 units FFP was transfused Patient developed urticaria Repeat APTT 98s Op cancelled

Isolated prolonged APTT
FVIII deficiency or severe vWD
FIX deficiency
FXI deficiency
FXII deficiency (nuisance)
Lupus anticoagulant
Inhibitors to FVIII

Inappropriate transfusion of blood/ blood components must be discouraged

The next time you decide to transfuse
Stop, think and ask yourself …
Is it really necessary?

Be aware of the risks of transfusion and the morbidity/ mortality associated with it! Febrile/ non-febrile transfusion reactions
Wrong blood
Bacteremia
Transfusion-related acute lung injury (TRALI)
Transfusion-transmitted infections (TTI)

Almost the end

Thrombophilia testing
Tests the phenotype
Will not identify or exclude a thrombophilic genetic defect completely
Finding a low level of the natural anticoagulant is not diagnostic of a deficiency
A normal result does not exclude a deficiency

Thrombophilia testing
There may be many other genetic factors that have not been identified
Negative tests cause a false sense of security
Positive tests cause unnecessary anxiety
Prolonging anticoagulation increases risk of haemorrhage

So why do clinicians request for thrombophilia testing?
To predict VTE recurrence
To determine duration of anticoagulation
To prevent/ reduce thrombosis
The ‘in-thing’ to do

Predicting recurrence
Long-term prospective cohort outcome studies have shown that finding a heritable thrombophilia does not typically predict recurrence
Baglin et al, 2003; Christiansen et al, 2005

Risk of Recurrence
In patients with deficiency of a natural anticoagulant (AT, PC, PS) the risk of recurrence is uncertain
Relative risks of recurrence appear to be <2.0 in patients who are not selected from thrombosis-prone families
Baglin et al, 2003; Christiansen et al, 2005; De Stefano et al, 2006

Case 6
28 year-old female nurse
No medical illness
Weight 110 kg
c/o Fever and RIF pain x 3 days

Case 6 – cont’d
Diagnosis: acute appendicitis
Appendicectomy performed
Findings: perforated appendix
Discharged POD6

Case 6 – cont’d
Returned evening of same day
Acute SOB with reduced O2 sat
Ventilated
CT pulmonary angiogram confirmed pulmonary embolism

CTPA – Pulmonary embolism

Case 6 – cont’d
Initial LMWH, then warfarin x 6 months
Thrombophilia test sent PS activity 30%
Referral: ? to continue long-term ac

Indications for thrombophilia testing
NICE guidelines 2012
1.

Case 6 – Duration of AC
Provoked
Precipitating factor- major: surgery
Predisposing factor: obesity
No family history of VTE
Duration of AC: 3 months (9th ACCP 2012)
Repeat PS act 76% (as pt was anxious & a staff nurse)

Inaccuracy of thrombophilia testing
BJH guidelines 2010

Case 7
28 year old lady doctor
c/o recurrent hemoptysis x 1 month
Investigated for PTB and started empirically on anti-TB Rx
Noted bilateral leg swelling

Case 7 – cont’d
Doppler US confirmed bilateral DVT
CT pulmonary angiogram confirmed pulmonary embolism
Anti-TB Rx stopped

Case 7- cont’d
Unprovoked or idiopathic
Duration of AC: at least 3 months or long term
(9th ACCP 2012)

Case 7 – cont’d
After 6 months ac
PC 86%
PS 55%
AT 90%
Referred whether to continue AC

Extending anticoagulation
BJH Guidelines 2010

Case 7 – LA screen sent
LA normalised ratio: 3.1
ACL antibody: positive
Anti-β2 GP1: positive
Diagnosis: Primary APLS
Duration of AC: long-term

Indications for thrombophilia testing
NICE guidelines 2012
2.
3.

Case 8
28 year-old man Spontaneous R LL
swelling Doppler US:
thrombosis R common femoral vein
Father also had unprovoked DVT on long-term ac
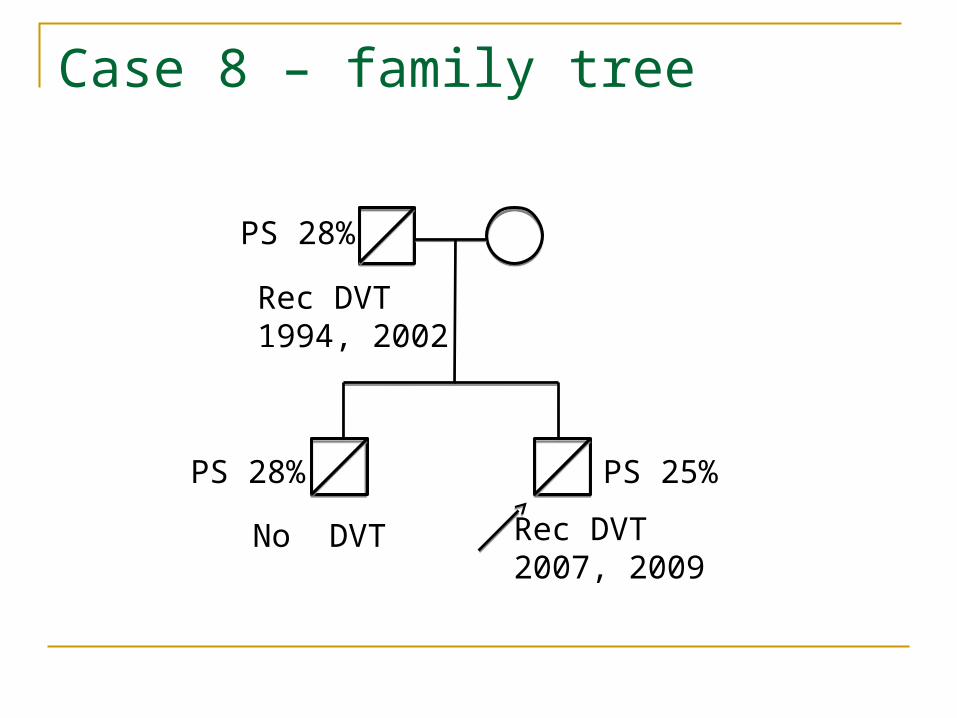
Rec DVT2007, 2009
No DVT
PS 25%PS 28%
PS 28%
Rec DVT1994, 2002
Case 8 – family tree
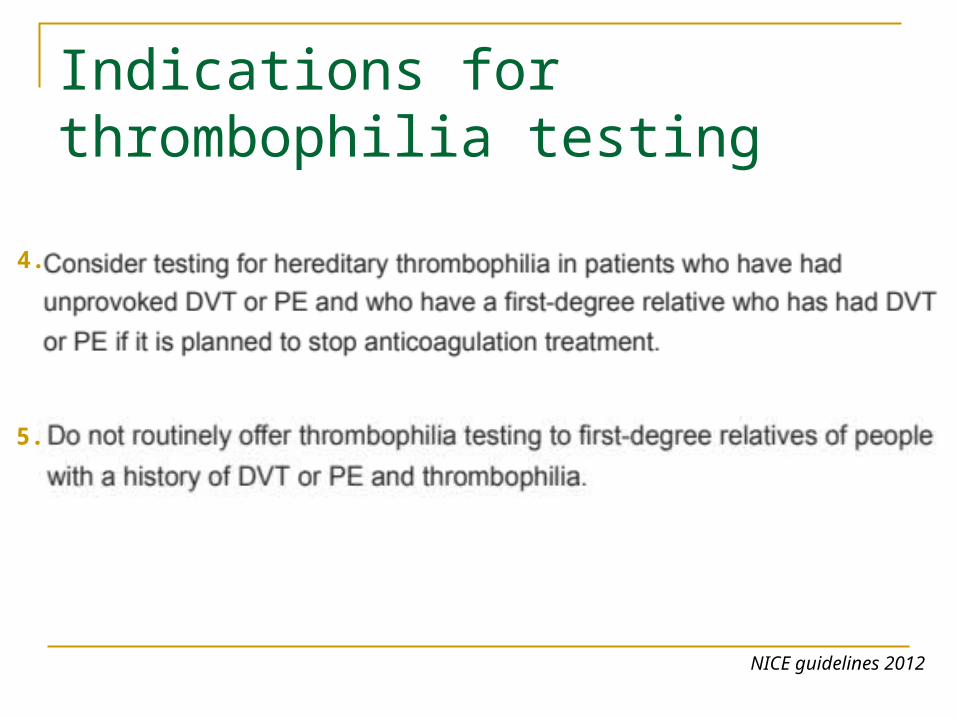
Indications for thrombophilia testing
NICE guidelines 2012
4.
5.

Risk
Age
Thrombotic threshold
Risk from “ageing”
Genetic risk 2
Genetic risk 1
Thrombosis is Multi-Causal Arising from Interacting Genetic and Acquired Risk Factors
Cumulative riskAcquired risk
Laffan M, 2007

Virchow’s triad
1. Blood
2. Vessel
3. Flow

No evidence that thrombophilic trait is associated with an increase risk for arterial thrombosis or recurrent miscarriagesExcept for lupus anticoagulant (LA)
NICE guidelines 2011

Guidelines for thrombophilia testing
BJH Guidelines 2010

Thrombophilia testing- has little clinical utility
Except for Lupus Anticoagulant (LA)

VTE CPG 2013

Case 9
70 yrs old man; known DM/ HT
Skidded and fell from motorbike
Fell on L side
c/o pain L hip
Unable to walk
Admitted to ward

Case 9 – cont’d
In pain
Small haematoma L temple
GCS 15 BP 193/93 PR 94 O2 sat 97%
Rxed with analgesics
Hb 13.0 TW 8.5 Plt 235

Case 9 – Fracture L pubic rami

Case 9 – D5 post-MVA
c/o chest tightness & SOB
O2 sat 90%
ECG: sinus tachy
CXR: haziness both bases
? Pulmonary embolism
Referred to medical

Case 9 – D5 post-MVA
Seen by medical
D-Dimer sent
If D-Dimer high >> CTPA
D-Dimer 3.6 ug/mL (0 - 0.5)

Causes of a high D-Dimer
DVT
Cellulitis/ infection
Haematoma or bleeding
DIC
Pregnancy
Inflammation/ Fracture

D-dimer & DVT in hospitalised patients
Brotman DJ, Am J Med 2003

D-dimer assays lack standardisation
Legnani C, Hematologica 2008

D-dimer: cut-off values?
Outpatient vs. hospitalised patients Pregnant vs. non-pregnant Old vs. young Cancer vs. non-cancer
Legnani C, Hematologica 2008

The end
Thank you