missionary vision care refractive error assessment missionary vision care - medical missions...
TRANSCRIPT

Missionary Vision Care
Refractive Error Assessment
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Refractive Error AssessmentObjective Methods – limited communication• Retinoscopy• Auto-refractor Subjective Methods – extensive communication• Trail lens set• Foropter (Phoropter)• Focometer • Near-point card for presbyopia
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Refractive Error AssessmentObjective Methods• Retinoscopy equipment and process
• http://eyeontechs.com/new/?p=308 (retinoscopy simulator)
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010
Missionary Vision Care
Refractive Error AssessmentObjective Methods• Retinoscopy assessment– Acquired skill – takes practice!– Limited by cataracts and other conditions– Sphere and astigmatic capable– Complex cases may stump you– May want a subjective confirmation– Little patient cooperation/communication needed
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Refractive Error AssessmentObjective Methods• Auto-refractor equipment and process
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Refractive Error AssessmentObjective Methods• Auto-refractor equipment and process
• http://kendall-optometry-ministry.com/kendall-optometry/Missionary Vision Care - Medical Missions
Interface Conference, June 12, 2010

Missionary Vision CareRefractive Error AssessmentObjective Methods• Auto refractor assessment– Mixed reviews from the field– Requires a large inventory, re-cycled glasses– Requires support staff– Low cost if equipment loaned– Low skill requirement but high information yield– “point
and shoot” high-tech solution.– Requires little patient cooperation/communication
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Refractive Error AssessmentSubjective Methods – all require a much higher
degree of patient cooperation/interaction• Trail lens set• Foropter (Phoropter)• Focometer
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010
Missionary Vision Care
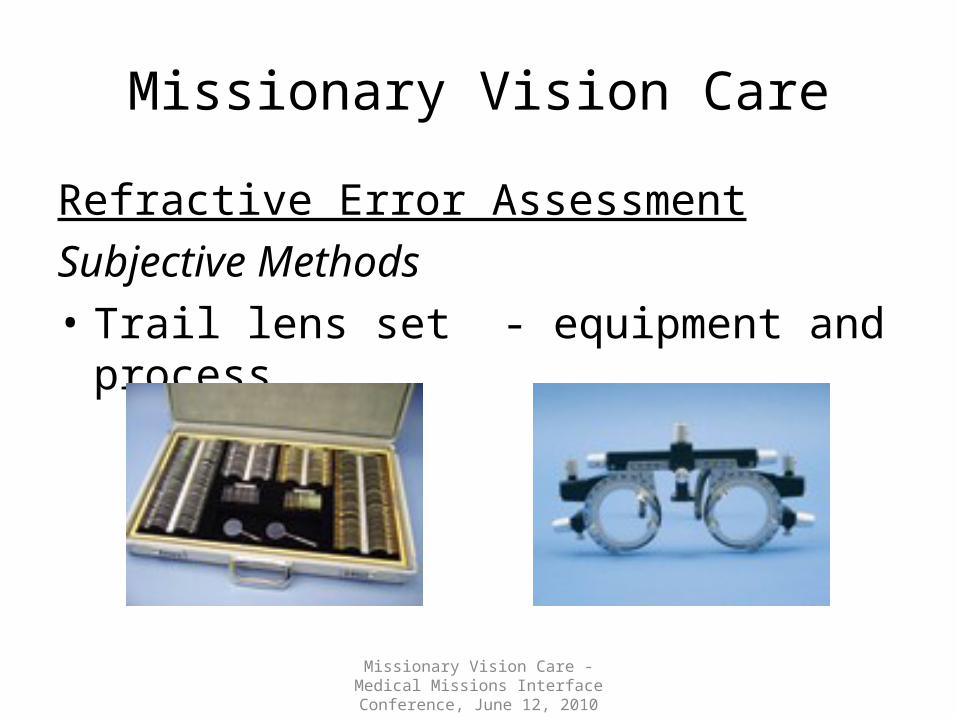
Refractive Error AssessmentSubjective Methods• Trail lens set - equipment and process
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010
Missionary Vision Care
Refractive Error AssessmentSubjective Methods• Trail lens set assessment– Trail and error bracketing process (0.25-0.5 dia)– Sphere and Astigmatic capable– Slower than other methods– Low-tech: no electronics– Requires full patient cooperation/communication
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Refractive Error AssessmentSubjective Methods• Foropter (also spelled Phoropter)
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Refractive Error AssessmentSubjective Methods• Foropter Method #2
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Refractive Error AssessmentSubjective Methods• Foropter methods assessment– Trail and error bracketing process (0.5 diopter)– Sphere and Astigmatic capable– Quicker than trial lenses– Low-tech: no electronics– Requires full patient cooperation/communication
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Refractive Error AssessmentSubjective Methods• Focometer - equipment and process
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Refractive Error AssessmentSubjective Methods• Focometer methods assessment– Continuous RE increments (0.25 diaopter)– Sphere and Astigmatic capable– Quicker than trial len but slower than foropter– Low-tech: no electronics– Requires full patient cooperation/communication
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Presbyopia Assessment (technically not RE)Subjective Methods• Near-point card• Age-guided trial and error method• Mono or biometric approach
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010
Missionary Vision Care
RE Assessment Considerations– Duration of trip– Comfort level with the method– Degree of personal interaction desired– Cost of equipment and supplies– Glasses available to dispense– Support staff available– Experience: start simple and move up
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Vision Clinic End Results• Hugs and smiles!
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Practical Considerations for Primary Vision Care
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Practical considerations for Primary Vision Care• Biometrics vs. monocular exam• Improvement vs. Optimization• Glasses Dispensing• Training and Supply Options
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Practical considerations for Primary Vision Care• Biometrics vs. monocular exam – two schools of thought
• Which one is correct?• Can you do harm?
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010
Eyes are often the same Eyes may be very different
I want to see more patients to help more people
I want to do the best I can on every patient
The time invested only yields incremental improvements
I’m happy to invest time to provide optimal correction
I only have single vision, fixed frame glasses.
I have the ability to build the needed glasses.
Missionary Vision Care
Practical considerations for Primary Vision Care• Biometric blending– Subjective best vision with both eyes
• Disregards astigmatism• Disregards anisometropia (different refracting powers)• Best chance of causing imbalance
– Subjective or Objective assessment with tables• Start with more positive, blend toward more negative• Disregards astigmatism• Avoids imbalance
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Practical considerations for Primary Vision Care
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision CarePractical considerations for Primary Vision Care• Improve vs Optimize – two schools of thought
• Which one is correct?• Can you do harm?• Are you missing opportunities to witness?
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010
Any improvement is a blessing
The Lord’s service requires my very best effort.
I want to see more patients to help more people
I want to do the best I can on every patient
The time invested only yields incremental improvements
I’m happy to invest time to provide optimal correction
I have an abundance of glasses to give away.
I have the ability to build the needed glasses.

Missionary Vision Care
Practical considerations for Primary Vision CareJesus’ example? He certainly ministered to large groups, but His
relationship-building touches were 1:1– Matt 8: 14-16 = Healing Peter’s mother-in-law, then minister to ALL
brought – John 3 = Nicodemus – born again; John 4 - Samaritan woman – living
water– Luke 8:43 = Jairus’ daughter, but stopped in the crush, to find the
woman. Her faith had healed her.– Mark 10:46 = Jericho, Blind Bartimaeus - one out of a multitude;
spiritual sight– Luke 19 = Bethany on His way to the cross – Zacchaeus, stopped to be
his guest
Lesson: Jesus wasn’t in a hurry & He didn’t try to heal everyone.Missionary Vision Care - Medical Missions
Interface Conference, June 12, 2010
Missionary Vision Care
Practical considerations for Primary Vision Care• Dispensing Glasses – Objectives– Best available fit : lenses and frames– Function before fashion (mirror?)– PD (pupillary distance) and optical center• Induce prism/distortion• The higher the strength the more important this is
– System of organizing inventory to expedite, simplify and avoid errors.
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Practical considerations for Primary Vision Care• Dispensing Glasses – Option 1– Re-cycled: Lion’s Club with Salvation Army• Assorted lenses and frames of all kinds• Sorting, organizing and matching fit a challenge• Least expensive supply, but large inventory required
and greatest amount of preparation.• Link with an inventory management system (Holland)• Potential for optimal fit – sphere, cylinder and add
power (bifocals)
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Practical considerations for Primary Vision Care• Dispensing Glasses – Option 2– Fixed lens, single-vision plus and minus• Generally of lower quality (imports)• May have the ability to swap out lenses• Biometric blending approach – error potential• Generally 1.0 diopter increments
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Practical considerations for Primary Vision Care• Dispensing Glasses – Option 3– Custom, single-vision plus and minus• Generally of higher quality (imports)• Option of pre-fitted or build your own• Mono-optical approach – reduced error potential• +10 to -10 range, 0.25 to 0.5 diopter increments• Frame and lens style options• Left/right or interchangeable lenses
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Practical considerations for Primary Vision Care• Dispensing Glasses – Option 4– Custom, single-vision +/- with cylinder• Generally of higher quality (imports)• Custom build frames and lenses• Mono-optical approach – reduced error potential• +4 to -4 range, 0.25 to 0.5 diopter increments• Frame and lens style options• Fully interchangeable lenses (reduced inventory)
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010
Missionary Vision Care
Practical considerations for Primary Vision Care• Dispensing Glasses
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Practical considerations for Primary Vision Care• Training Options (handout)– Eye Doc in a Box (Dr. David Curtis)
• Exceptional in basics, optics, foropter emphasis
– InFOCUS/Visual Compassion (Dr. Joey Dollak)• Exceptional in retinoscopy, biometric blending
– Kendall Optometry Minisitry (Holland Kendall)• Exceptional in auto-refractor, integration software to make
use of recycled glasses
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Practical considerations for Primary Vision Care• Material suppliers (handout)– Peachtree Optical (Mr. Jay Biggs)
• Custom missionary field kits, interchangeable +4.0 to -4.0 lenses for multiple frame sizes and styles
– Good-Lite Company (Mr. Joe Villari)• Vast supply of charts, equipment and supplies for missionary
vision care.
– InFOCUS/Visual Compassion (Mrs. Diane Baker)• Retinoscopes, Focometers , lens and frame selections
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Tips for planning and conducting vision clinics
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010

Missionary Vision Care
Tips for planning and conducting vision clinics – Connections on the ground – a must!– Organize/ Communicate, Organize/ Communicate, repeat– KISS approach – stay in your comfort zone– Arrive 2 days ahead of team for set-up– Limit the number of patient records allowed/day– Leave your watch at home– Involve others – you can’t do it all yourself– It will not go the way you plan – that’s OK!– Leave room for God– Pray!
Missionary Vision Care - Medical Missions Interface Conference, June 12, 2010