metabolic acidosis the critically ill - international ...icnu.ir/slides/day2/b/approach to metabolic...
TRANSCRIPT
Metabolic acidosis in the critically ill
Dr.T.SabaghianAssistant professor of Nephrology,Shahid beheshti university
ICNU,2015


Metabolic acidosis is commonlyassociated with many conditions within critical care.
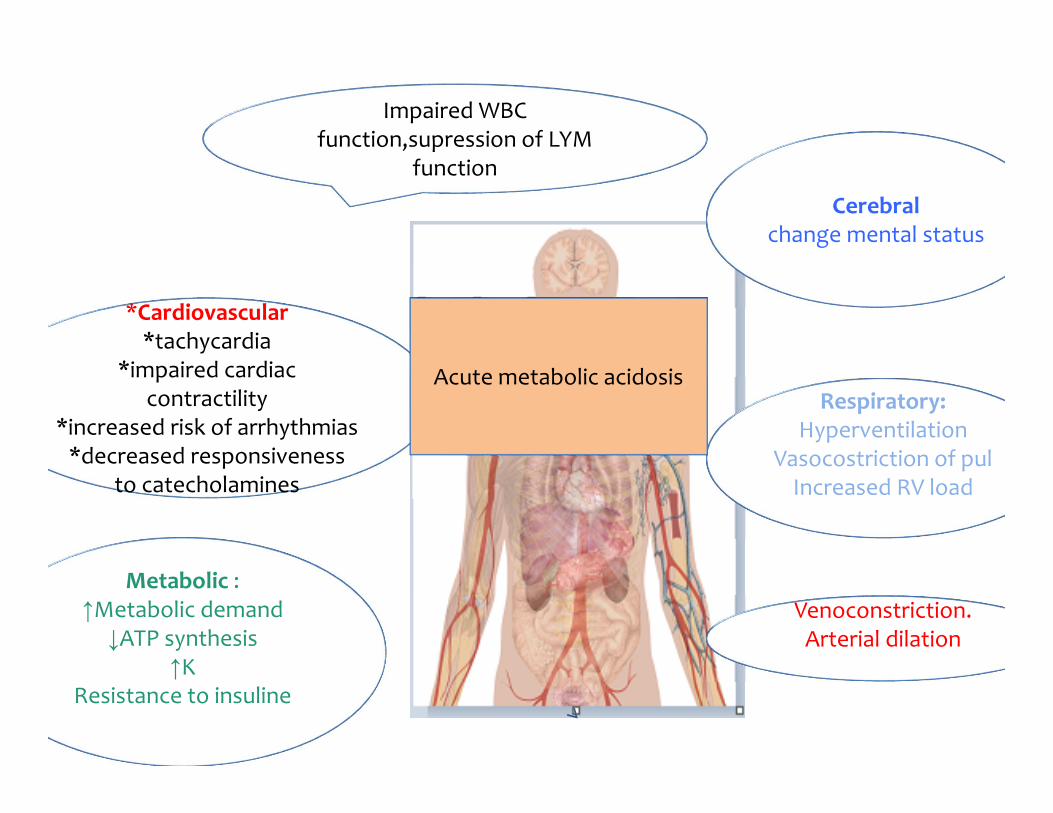
*Cardiovascular*tachycardia
*impaired cardiac contractility
*increased risk of arrhythmias*decreased responsiveness
to catecholamines
Cerebralchange mental status
Metabolic :↑Metabolic demand↓ATP synthesis
↑KResistance to insuline
Impaired WBC function,supression of LYM
function
Venoconstriction. Arterial dilation
Respiratory:Hyperventilation
Vasocostriction of pulIncreased RV load
Acute metabolic acidosis
• observational single‐center cohort analysis over a 3‐year period on ICU patients who had AKI treated with RRT.
• compared patients with SLA at time of initiation of RRT (pH <7.35 or treatment with NaHCO3 to correct acidosis and a serum lactate concentration ≥5 mmol/L) to patients without SLA (serum lactate
concentration ≤5 mmol/L).
The prevalence of SLA at time of initiation of RRT was a common finding in study population(1/3of ICU patients started on RRT had SLA). The association between lactic acidosis and mortality was confirmed in this specific cohort of ICU patients

↑acid production
↓renal acid excretion
Loss of HCO3 or HCO3 precursors
Mechanism of acidosis

Classification of metabolic acidosis
Anion Gap = Na+ – (Cl– + HCO3–) = 9 ± 3 mEq/L (Each laboratory to determine its own normal range for AG)
S‐Anion Gap = Na+ – (Cl– + HCO3–) = 9 ± 3 mEq/L (Each laboratory to determine its own normal range for AG)
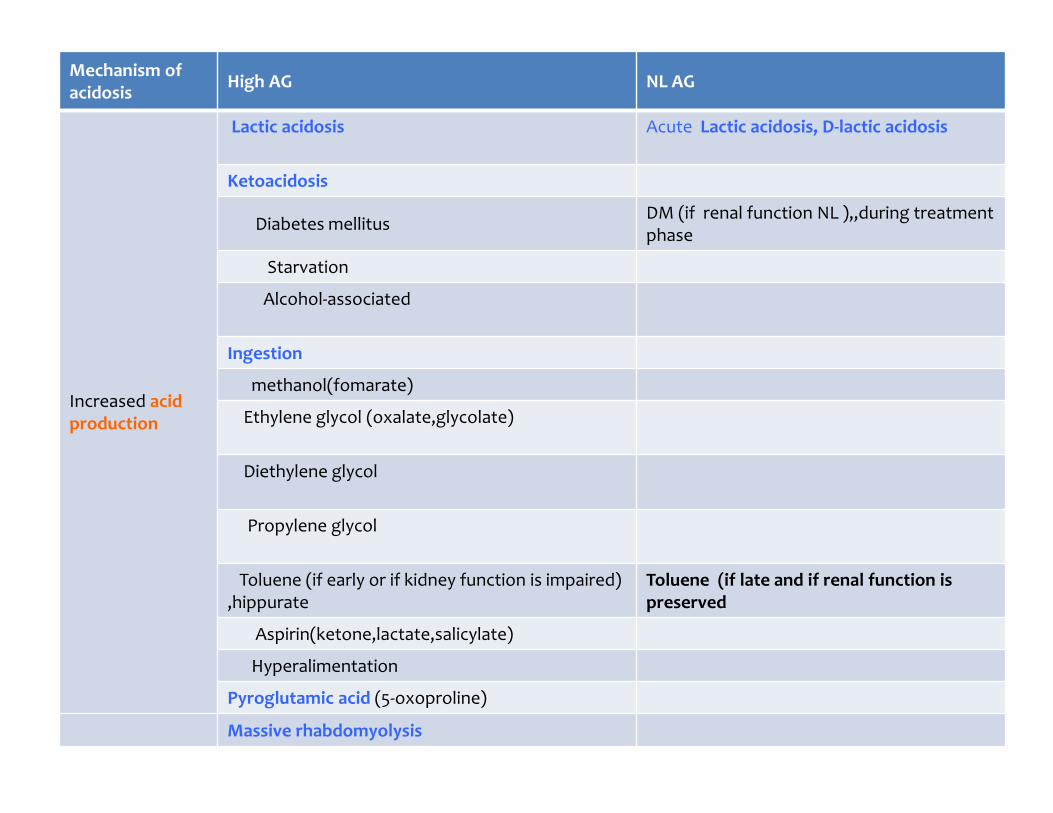
Mechanism of acidosis High AG NL AG
Increased acid production
Lactic acidosis Acute Lactic acidosis, D‐lactic acidosis
Ketoacidosis
Diabetes mellitus DM (if renal function NL ),,during treatmentphase
Starvation
Alcohol‐associated
Ingestion
methanol(fomarate)
Ethylene glycol (oxalate,glycolate)
Diethylene glycol
Propylene glycol
Toluene (if early or if kidney function is impaired) ,hippurate
Toluene (if late and if renal function is preserved
Aspirin(ketone,lactate,salicylate)
Hyperalimentation
Pyroglutamic acid (5‐oxoproline)
Massive rhabdomyolysis

High AG Normal AG
Loss of HCO3 or HCO3 precursors
Diarrhea or other intestinal losses (eg, tube drainage)
proximalRTA
Post treatment of ketoacidosis
Carbonic anhydrase inhibitors
Ureteral diversion (eg, ileal loop)
Decreased renal acid excretion Chronic kidney disease
CKD and tubular dysfunction (but relatively preservedGFR)
Type 1 RTA
Type 4 RTA

The anion gap in critical illness
Two main potential sources of diagnostic error: 1. Iatrogenic hyperchloraemia :due to volume loading in
shock (0.9% saline , colloids are hyperchloraemic).
↑plasma cL, hyperchloraemic acidosis (↓Albumin negative charge➔↓AG)
Masked high anion gap acidosis, e.g. lactate.

2) Hypoalbuminaemia: due to pan‐endothelial dysfunction
+↓capillary reflection coefficient (capillary leak syndrome)
raid fall in albumin ⇛↓ anion gap. Corrected AG=SAG +〔2.5×(4.5‐observed serum Alb) 〕 ↓1 mg/dl Alb(4)→↑2.5meq/l AG
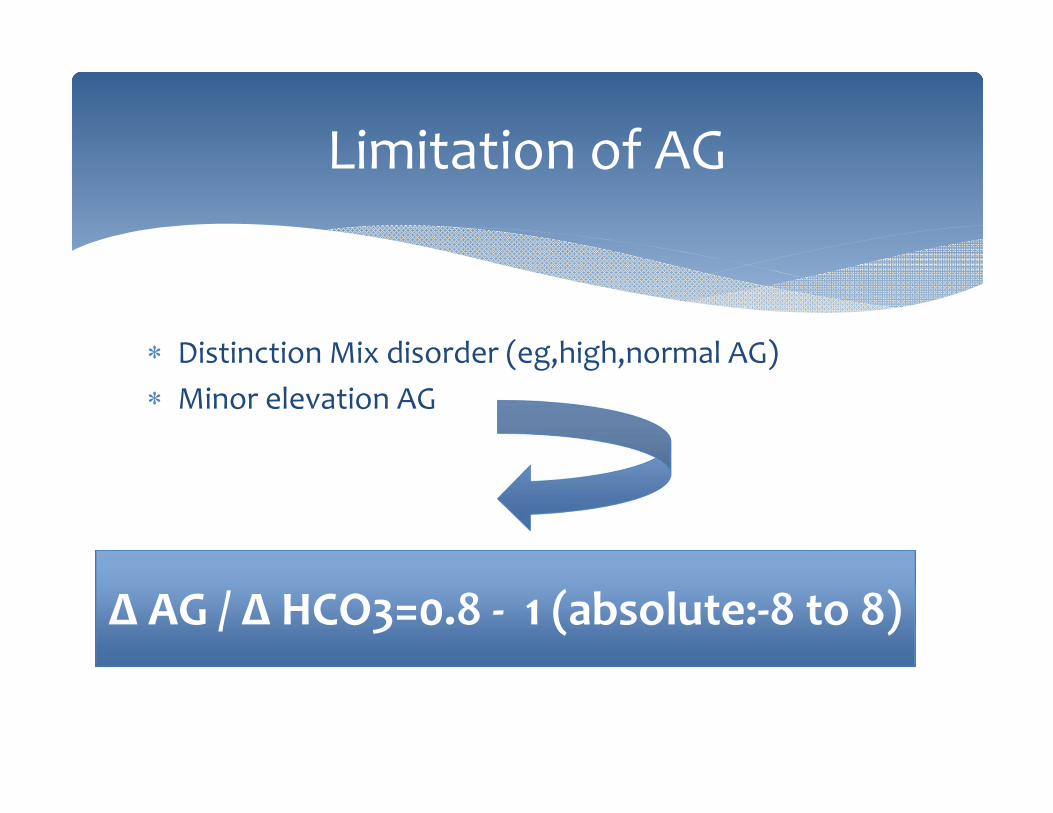
Distinction Mix disorder (eg,high,normal AG) Minor elevation AG
Limitation of AG
Δ AG / Δ HCO3=0.8 ‐ 1 (absolute:‐8 to 8)
Diagnosis
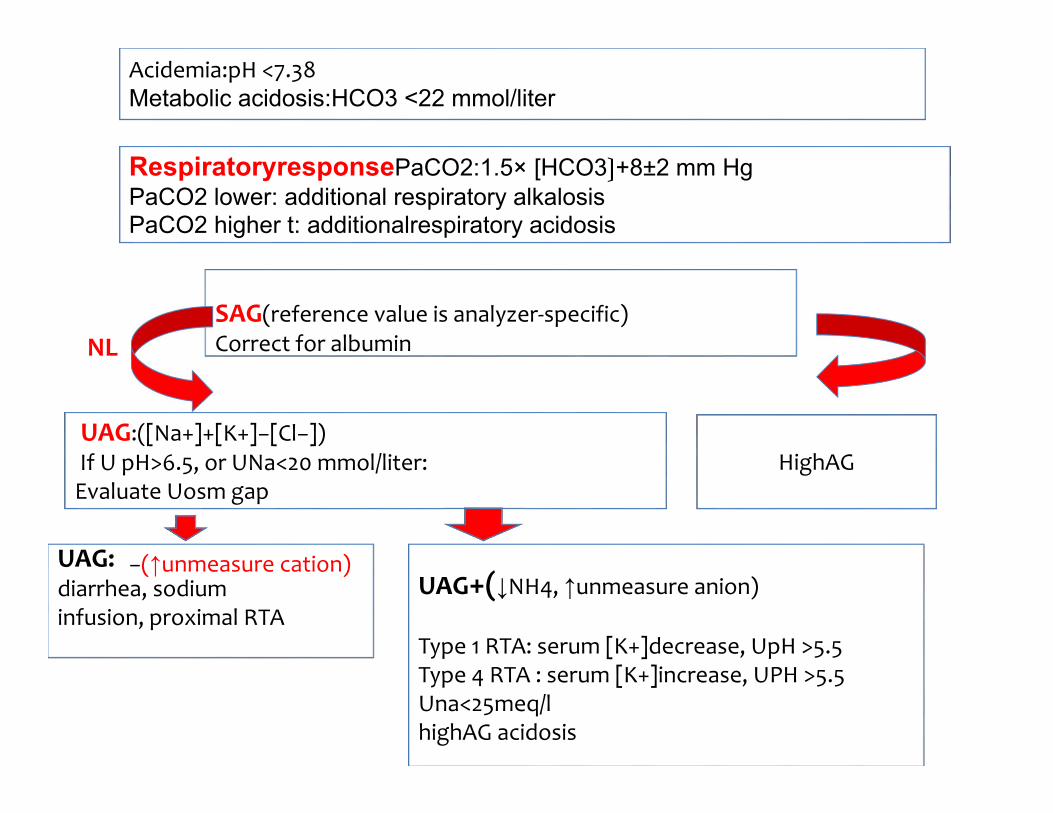
Acidemia:pH <7.38Metabolic acidosis:HCO3 <22 mmol/liter
RespiratoryresponsePaCO2:1.5× [HCO3〕+8±2 mm HgPaCO2 lower: additional respiratory alkalosisPaCO2 higher t: additionalrespiratory acidosis
SAG(reference value is analyzer‐specific)Correct for albumin
HighAGUAG:([Na+]+[K+]−[Cl−])If U pH>6.5, or UNa<20 mmol/liter:Evaluate Uosm gap
UAG:diarrhea, sodiuminfusion, proximal RTA
UAG+(↓NH4, ↑unmeasure anion)
Type 1 RTA: serum [K+]decrease, UpH >5.5Type 4 RTA : serum [K+]increase, UPH >5.5 Una<25meq/lhighAG acidosis
AGNL
−(↑unmeasure cation)
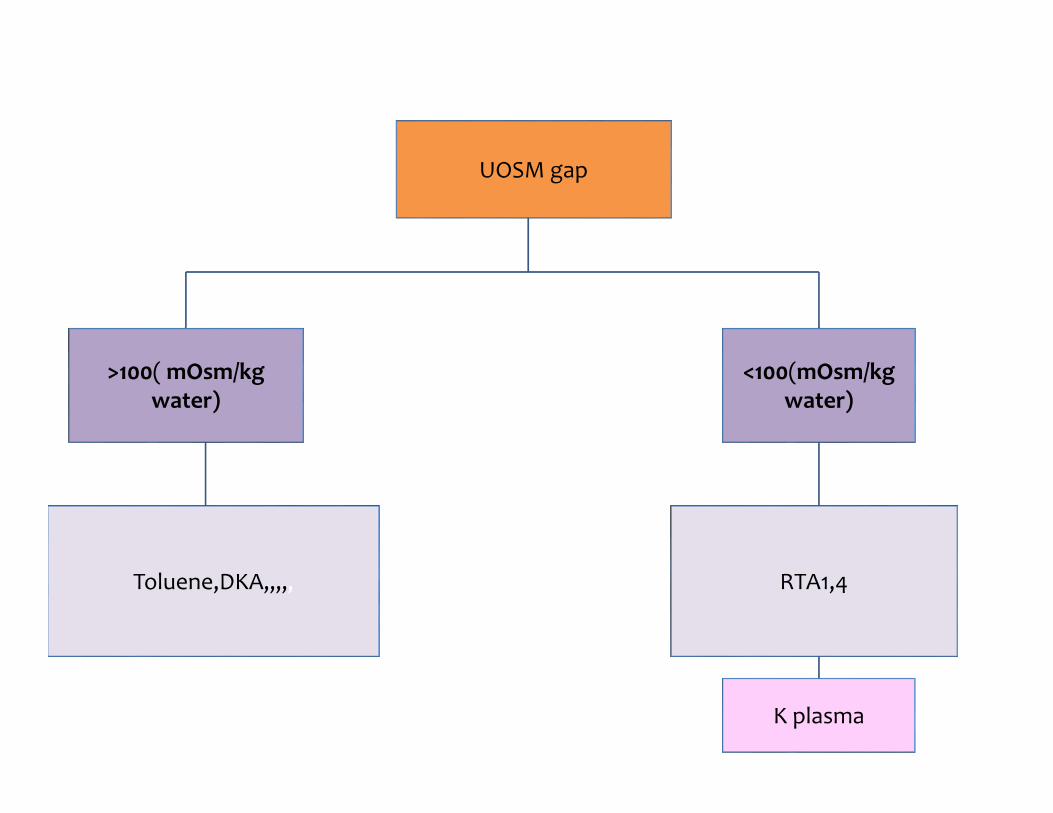
UOSM gap
<100(mOsm/kg water)
>100(mOsm/kg water)
Toluene,DKA,,,,, RTA1,4
K plasma
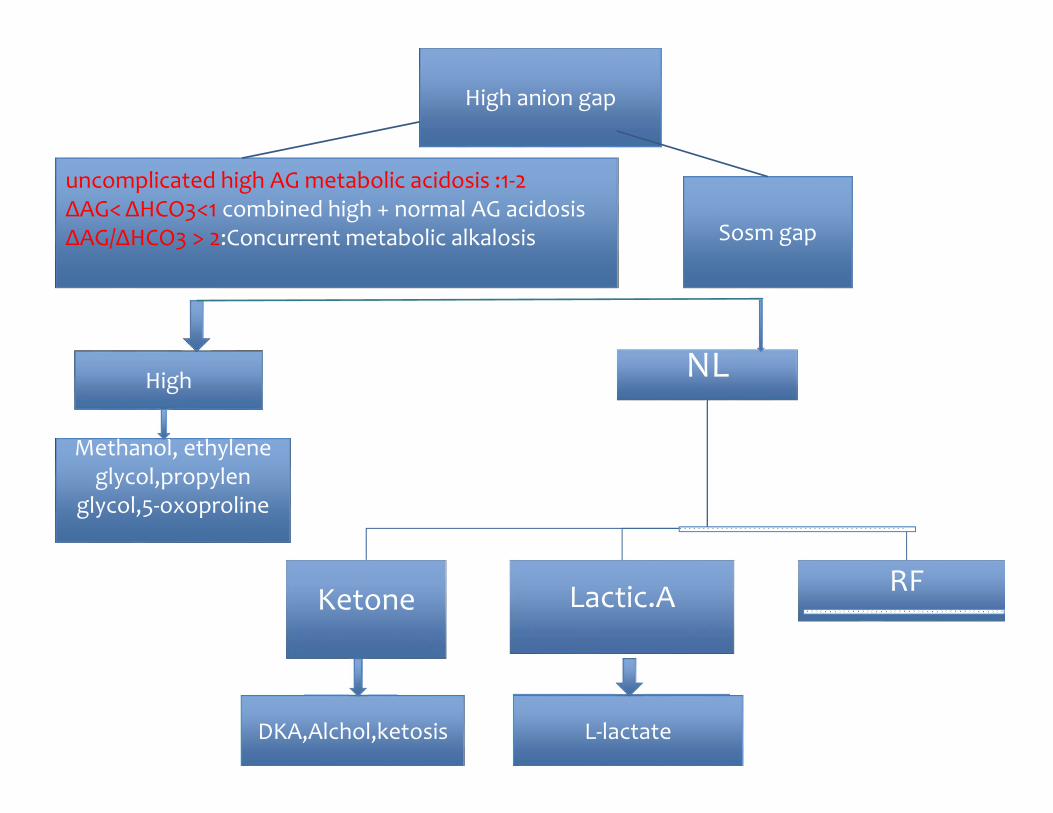
High anion gap
uncomplicated high AG metabolic acidosis :1‐2ΔAG< ΔHCO3<1 combined high + normal AG acidosisΔAG/ΔHCO3 > 2:Concurrent metabolic alkalosis Sosm gap
High NL
Ketone Lactic.A RF
DKA,Alchol,ketosis
Methanol, ethylene glycol,propylen
glycol,5‐oxoproline
L‐lactate

Production &utilization
Lactic Acidosis

1. ↑production 2. ↓pyruvate conversion to co2,H2O or to glucose 3. An altered redox state within the cell in which
pyruvate is preferentially converted into lactate high metabolic capacity for lactate
component of decreased utilization
Pathophysiology

Glucose
pyruvate
Gluconeogenesis Acetyl coA(TCA) Lactate
P.C
PDH(Aerobic)
LDH(anaerobic)
HCO3
6ATP
C02+H2O
2 ATP
1ATP
liver NADH NAD+H
AA(Alanine)

Co2+H20
20%,PC
80%
PDH

Hyperlactataemia refers to an elevated plasma concentration of lactate anions(greater than 2mmol/l).
lactic acidaemia may be defined as a pH < 7.35 with a lactate concentration > 4meq/l
Lactic acidosis is the most common cause of metabolic acidosis in hospitalized patients.Lactic acidosis is considered to be present if the plasma lactate concentration exceeds 4 to 5 meq/L, even among patients without a systemic acidosis.
Type A (Most cases of lactic acidosis) : due to marked tissue hypoperfusion in shock (due to hypovolemia, cardiac failure, or sepsis) or during a cardiopulmonary arrest
Type B (not Systemic hypoperfusion) mechanisms : toxin‐induced, impairment of cellular metabolism or regional areas of ischemia
Types of lactic acidosis

DM andmetformin1. metformin type B lactic acidosis,2. a moderate degree of lactic acidosis in DKA(may be due
to hypovolemia,altered Redox state and ↑ conversion pyruvate to lactate ).
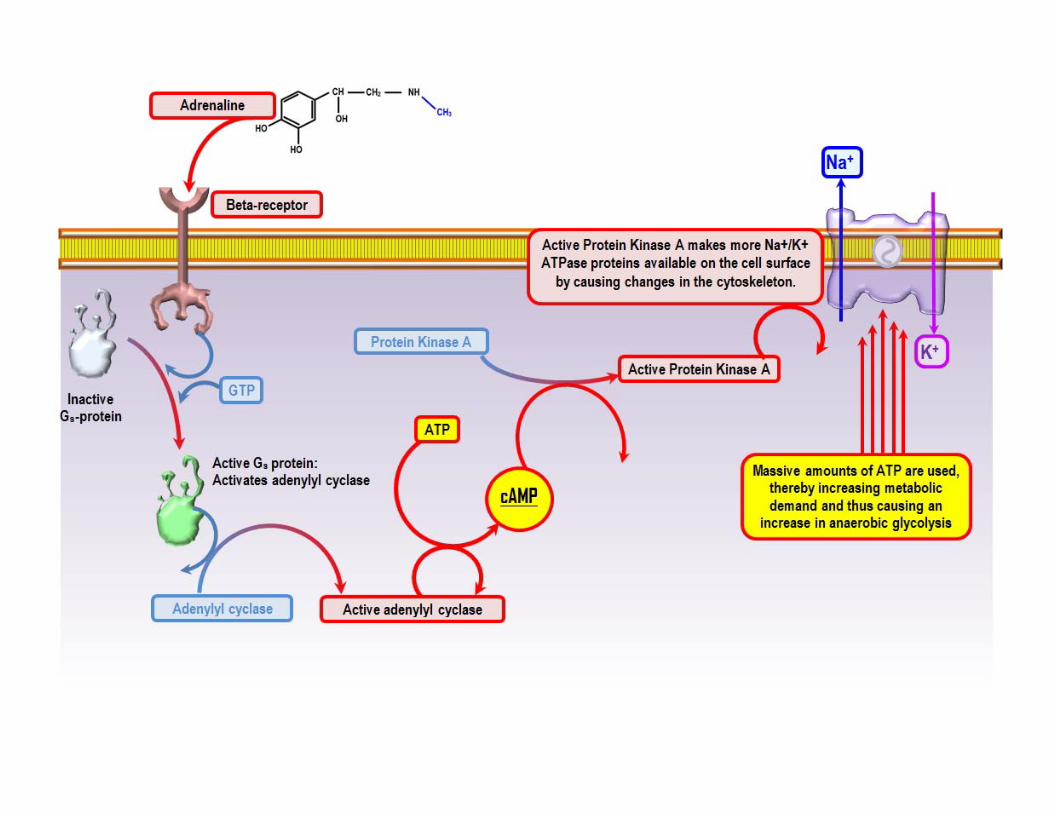
beta agonists(adrenaline, salbutamol and dobutamine),1. stimulate glycolysis and lactate production which may
not be cleared due to inhibited PDH .2. stimulation of Na+ ⁄ K+ ATPase of the muscle cell
membrane enhances cellular glycolysis
Type B
Low risk

A common clinical scenario during resuscitation :volume loading (iatrogenic hyperchloraemia) and adrenaline infusionschloride load and type B lactic acidosis interpreted as ‘shock’ requiring more fluid and morebeta agonis vicious cycle,overresuscitation.

Malignancy — lactic acidosis rarely in leukemia, lymphoma, and solid malignancies .
1. Anaerobic metabolism due to dense clusters of tumor cells
2. Direct lactate production by the neoplastic cells.3. metastatic replacement of the hepatic parenchyma4. Thiamine or riboflavin deficiency
Absolute or functional thiamine deficiency

Carbohydrate metabolism and role of thiamine. The inability to use the Krebs cycle is the major underlying pathophysiological feature of thiamine deficiency. Thiamine
pyrophosphate (TPP), is an essential component of aerobic metabolism. A decrease in its activity may lead to the tissue accumulation of toxic intermediates such as pyruvate and
lactate

major pathophysiology of thiamine deficiency:.Acidosis and the inability to utilize the Krebs cycle.

thiamine deficiency occurs mainly in persons with alcohol abuse severe sepsis‐like syndrome unexplained heart failure lactic acidosis unexplained neurological disorders chronic malnutrition total parenteral nutrition hyperemesis gravidarum following surgery

4 cases of hospitalized patients without history of alcohol dependencet present with metabolic acidosis and refractory hypotension caused by acute fulminant cardiac beriberi
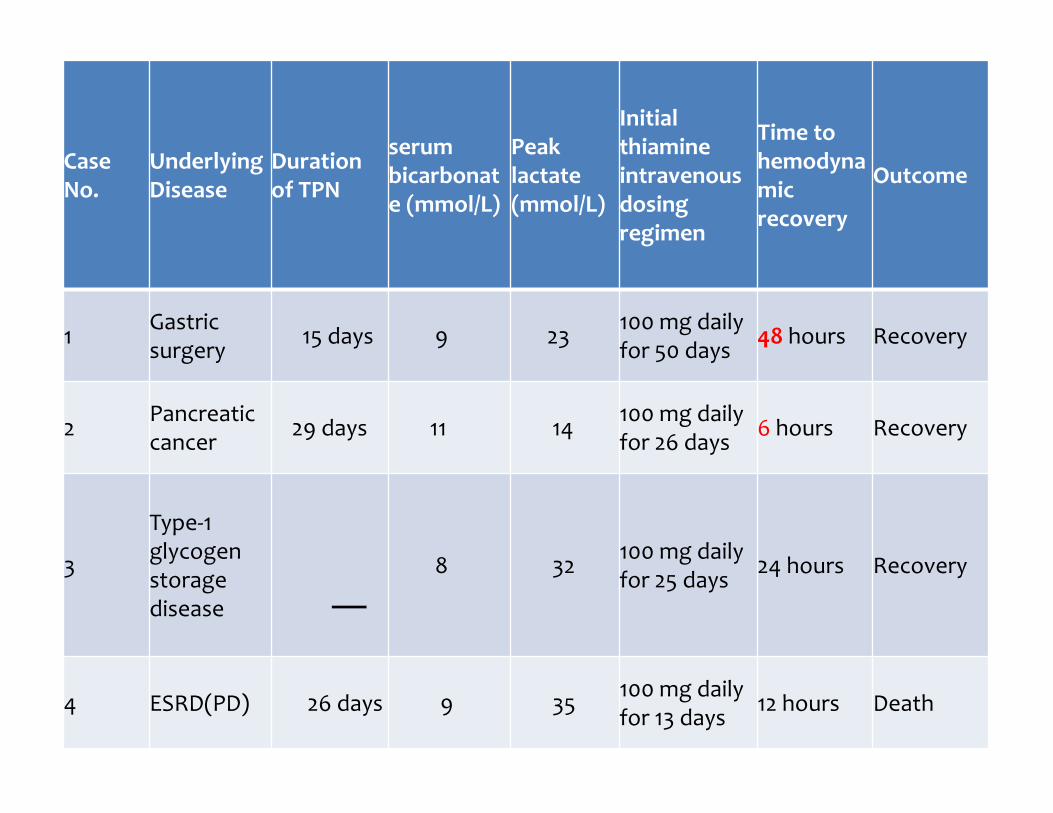
Case No.
Underlying Disease
Duration of TPN
serum bicarbonate (mmol/L)
Peak lactate (mmol/L)
Initial thiamine intravenous dosing regimen
Time to hemodynamic recovery
Outcome
1 Gastric surgery 15 days 9 23 100 mg daily
for 50 days 48 hours Recovery
2 Pancreatic cancer 29 days 11 14 100 mg daily
for 26 days 6 hours Recovery
3
Type‐1 glycogen storage disease
8 32 100 mg daily for 25 days 24 hours Recovery
4 ESRD(PD) 26 days 9 35 100 mg daily for 13 days 12 hours Death

Five out of 14 CLL patients (35.7%) werefound to have a measurable, though subclinical,functional thiamine deficiency

J Crit Care.2010 Dec;25(4):576‐81. doi: 10.1016/j.jcrc.2010.03.003. Epub 2010 Jun 19.Thiamine deficiency in critically ill patients with sepsis.Donnino MW1, Carney E, Cocchi MN, Barbash I, C
indicate critically ill patients may present with TD or develop this deficiency during their acute illness.
potential association between thiamine levels and lactic acidosis in patients without significant liver injury.

Acute fulminant beriberi is not a rare occurrence in the ICU.
symptoms : non specific such as generalized fatigue, loss of appetite, and abdominal pain.
Or with severe biventricular failure, metabolic acidosis, vascular collapse, peripheral cyanosis and eventually death

Diagnosis :difficult due to its protean clinical manifestations, the low index of suspicion, and the lack of readily available emergent blood thiamine measurements

High degree of safety, many authors would strongly recommend a trial of IV thiamine a replacement for cases of impaired cardiac function, impaired neurology, lactic acidosis and other ‘unidentified’ high anion gap acidoses in the critically ill .
An elevated serum anion gap can provide supportiveevidence.
A normal anion gap does not rule out lactic acidosis. In one study, 50% of patients with a serum lactatelevel of 5 to 10 mmol per liter did not have an elevated anion gap.
Lactic acidosis ‐Diagnosis

the ΔAG:ΔHCO3 > 1, in part because the apparent space of distribution of protons exceeds that of lactate; therefore, an increased ratio might not always suggest a coexisting acid–base disorder.
elevated blood lactate level is essential for confirmation of the diagnosis:
1. lower limit : 0.5 mmol/L,2. but upper limit can vary from 1 − 2.2 mmol
/L(differs among laboratories).

Upper limit of normal :increased mortality among seriously ill patients
slightly increased from a previous baseline value(although remaining within the normal range) :poor outcome
A serum osmolal gap of more than 20 mOsm/kg water due to
1. release of osmotically active solute from ischemic tissues.
2. Other disorders with ↑osmolal gap and hyperlactatemia (e.g., exposure to toxic alcohols) should be ruled out.
Supporting the Circulation and Ventilation Restoring tissue perfusion (Vasopressors and inotropic agents). Acidemia blunts the response to catecholamines, thereby increasing the required dose. High doses of catecholamines can aggravate hyperlactatemia by reducing tissue perfusion or overstimulating the β2‐adrenoceptor; therefore, the dose should be adjusted carefully.
Lactic Acidosis ‐Treatment

Comparision safety and effectivity of solutions in lactic acidosis
Published online 30 October 2014 inWiley Online Library
RCTand observational studies that compared outcomes in acutely ill or surgical patients receiving either high‐chloride (cl>111 mmol/l) or lower‐chloride <111 mmol/l ) crystalloids for resuscitation.Endpoints:mortality, kidney function, serum chloride, hyperchloraemia/metabolic acidosis, blood transfusion volume, mechanical ventilation time, and length of hospital and ICU stay
The search identified 21 studies involving 6253 patients. High‐chloride fluids :not affect mortality but associated
with 1. higher risk of AKI(P <0⋅001) and2. hyperchloraemia/metabolic acidosis (P <0⋅001) 3. greater serum chloride (P <0⋅001) 4. ↑blood transfusion volume (P =0⋅014) and 5. mechanical ventilation time (P <0⋅001) Sensitivity analyses excluding heavily weighted studies
resulted in non‐statistically significant effects for AKI and mechanical ventilation time.
A weak but significant association between
higher chloride content fluids and unfavourableoutcomes was found, but mortality was
unaffected by chloride content

Red-cell transfusions :maintain Hb> 7 g/dl. On the basis CVD,some recommendationes are 10g/dl
Improve microvascular perfusion independently of systemic hemodynamics:dobutamine, acetylcholine,and nitroglycerin, have been shown to to reduce hyperlactatemia, and even to improve the outcome.

Targeting the cause or causes of lactic acidosis:treatment of sepsis with the appropriate antibiotic agents; management of arrhythmias.
No alkali therapy may be required in lactic or ketoacidosis (where metabolism of the organic anions will regenerate HCO‐
3), some clinicians recommend bicarbonate for severe
acidemia (blood pH, <7.1). But reducing mortality or improving
hemodynamics remains unproven.
Alkali Administration
NHE1 inhibitors : Metabolic Acidosis→↑activation NHE1 →Na,Caoverload in heart→ cellular injury. In experimental models of lactic acidosis due to sepsis, hypoxia, hemorrhagic shock, or cardiac arrest, NHE1 inhibitors attenuated the lactic acidosis and hypotension, improved myocardial performance and tissue oxygen delivery, enabled resuscitation, and reduced mortality.
Inhibitors of LDH are being investigated as promising cancer therapies.

Measure Goal of Therapy Comments
MAP 65‐70mmHg Reflect adequencyofmicrocirculation
HR <100
CVP 8‐12mmHg
PCWP 12‐15mmHg
U/O >0.5cc/Kg/h alone is not an adequate indicator of renal function,also consider changes in Cr
Measures for Monitoring and Goals of Therapy in Patients with Lactic Acidosis

Goals of Therapy in Patients with Lactic Acidosis
Hb >7 g/dl, but can vary on the basis of cardiovascularstatus of patient; some recommendations arefor approximately 10 g/dl
Monitoring of cvO2 saturation requiresinsertion of catheters. A recent study indicated thatthere is no additional value of this measure over the usual hemodynamic measurment
ArterialO2 saturation
≥92%
cvO2 saturation ≥70%
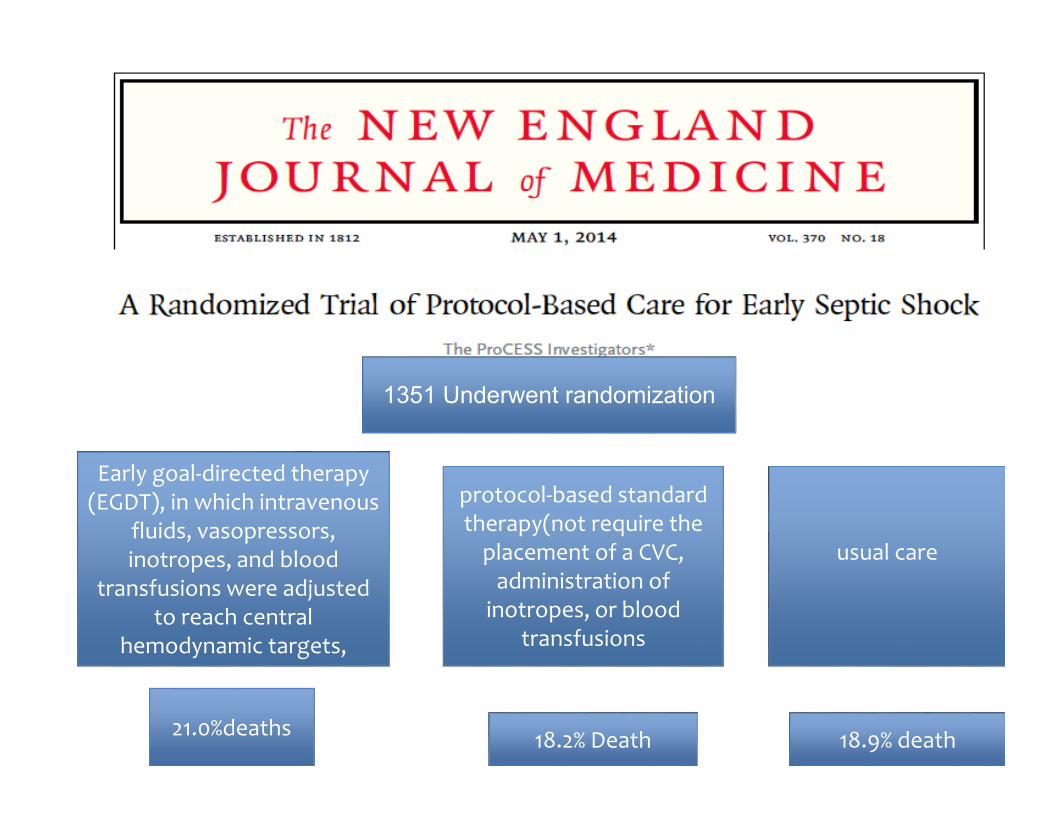
1351 Underwent randomization
Early goal‐directed therapy (EGDT), in which intravenous
fluids, vasopressors, inotropes, and blood
transfusions were adjusted to reach central
hemodynamic targets,
protocol‐based standard therapy(not require the placement of a CVC, administration of inotropes, or blood
transfusions
usual care
21.0%deaths 18.2% Death 18.9% death

The use of central venous blood gases to assess tissue acid–base status has not been established, but measurement should be considered for patients with severe hypoperfusion.
Acid–base measures should be evaluated every few hours

Blood lactate (Peripheral venous and arterial values are interchangeable)is a useful tool for screening, risk stratification, and prognosis.
The initial value has prognostic significance, butserialmeasurements have more value for prognosisand for guiding therapy. Lactate‐guided therapy has been beneficial in some studies.
In one study, reduction of blood lactate by 20% every 2 hr for the first 8 hr was associated with a decrease in morbidity and mortality.
The use of lactate clearance to monitor and guide therapy remains under investigation.
American Journal of Respiratory and Critical Care Medicine
whether lactate monitoring aimed to decreaselevels during initial treatment in critically ill patients improvesoutcome.
In the lactate group hospital mortality was lower (P = 0.006), Organ Failure Assessment scores were lower between 9 and 72 hours, inotropes could be stopped earlier, and patients could be weaned from mechanical ventilation and discharged from the ICU earlier.
In patients with hyperlactatemia on ICU admission, lactate‐guided therapy significantly reduced hospital mortality .This study suggests
that initial lactate monitoring has clinical benefit
Treatment of DKA in dialysis patients
DKA has been increasingly encountered due to rising prevalence of diabetic ESKD.
Average bicarbonate and AG in dialysis‐dependent patients with DKA were 12.0±4.6 mmol/L and 27.2±6.4 mEq/L, respectively.
AG> 20 mEq/L is not typical for ESKD alone➔ search for additional causes such as DKA.
Rarely, metabolic acidosis can be masked by concomitant metabolic alkalosis from exposure to a high bicarbonate dialysate during hemodialysis.

Insulin administration is only treatment required for DKA management in dialysis patients.
initial rate of IV insulin :similar to non‐dialysis individuals, bolus to 0.1 U/kg followed by continuous insulin infusion at 0.05 U/kg/h.
recommended serum glucose decline: 100–125 mg/dL/h (Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy 2014:7)

No signs of volume depletion (lack of osmotic diuresis )➔ not require IV fluids
If intravascular volume depletion→ boluses of normal saline (250 mL) with close monitoring
pulmonary edema in severe DKA (due to hyperglycemia‐associated interstitial hypertonicity) responds to insulin alone; in severe cases, acute dialysis may be required.

hyperkalemia : ↓GFR, insulinopenia, and hypertonicity result in positive potassium balance, placing ESKD patients with DKA at high risk for hyperkalemia➔routine K replacement is not indicated unless plasma potassium level is below 3.3 mmol/L.
Insulin is typically the only treatment necessary for hyperkalemia in dialysis‐dependent patients with DKA.

Role of hemodialysis in the treatment of DKA is controversial .
Main indications for acute hemodialysis in DKA:Severe pulmonary edema and hyperkalemia.

Normal anion gap acidoses

prospective, observational trial in a medical ICU. 100 critically ill patients at the age ≥18, expected to stay in the ICU for ≥24 h, with the clinical necessity for aurinary catheter and the absence of anuria were included.Base excess (BE) subset calculation based on a physical‐chemical approach on the first 7 days after ICU admission.Calculation U osmolal gap (UOG) as an approximate measure ≃urine NH4 → Determination renal and extrarenal HCO3 loss in hyperchloremic acidosis.

Results: During the first week of ICU stay %43 of the patients presented with hyperchloremic acidosis
RTA is highly prevalent in critically ill patients with hyperchloremic acidosis, whereas it is often neutralized by the simultaneous occurrence of other acid‐base disturbances.


During the 3‐year study period, 454 patients with AKI were treatedwith RRT. On the day of initiation of RRT, 148 patients (32.6%) werediagnosed with SLA. nonsurvivors were more acidotic, lactate concentrationat initiation of RRT was not able to discriminate betweensurvivors and nonsurvivors in the cohort of patients with SLA at timeof initiation of RRT. In AKI patients with SLA, lactate concentration atinitiation of RRT may, therefore, not be a useful parameter forselecting those who will benefit of treatment with RRT.

Type 1 RTA Type 2 RTA Type 4 RTA
Primary defect Impaired distal acidification
Reduced proximal bicarbonate reabsorption
Decreased aldosterone secretion or effect
Plasma bicarbonate
Variable, may be below 10 meq/L
Usually 12 to 20 meq/L
Greater than 17 meq/L
Urine pH Greater than 5.3
Variable, greater than 5.3 if above bicarbonate reabsorptive threshold
Usually less than 5.3
Plasma potassium
Usually reduced but hyperkalemic forms exist; hypokalemia largely corrects with alkali therapy
Reduced, made worse by bicarbonaturia induced by alkali therapy
Increased
Characteristics of the different types of renal tubular acidosis
1. Rapid administration of chloride‐rich solutions (essentially colloids and normal 0.9% saline containing Cl– 154 mEq.l)1 ) Balanced lactate solutions ( contain chloride at a concentration of 110 mEq.l) .
2. Alkaline gastrointestinal losses , especially lower loss(gastric outlet obstruction, fistulae ).
3. RTA4. Ureteric diversion.
pathophysiologiy

RTA: group of disorders in which, despite a relatively well‐preservedGFR , metabolic acidosis develops because of defects in renal tubules to perform normal functions required to maintain acid‐base balance.


Total H+ turnover :150 000 milli moles/d.
The excretion of acid load : in three categories(different rates of production and elimination)
1. Class 1: Volatile, i.e. CO2: production:15 000 mmol/d co2 from metabolism of carbohydrate and fats excretion : lungs.
Pathogenesis of metabolic acidosis

2) Class 2 :Organic acids: i.e lactate and ketones. 3) Class 3: Inorganic acids:i.e Sulphate and phosphate production nonvolatile:50‐100meq/d from dietary protein and amino acid metabolism. (Sulphur‐containing amino acids methionine and cysteine). excretion nonvolatile: urine

uncomplicated high AG metabolic acidosis :1‐2 ΔAG/ ΔHCO3<1(↓Hco3 greater than expected)1. In ketoacidosis, D‐lactic acidosis, or toluene
intoxication(excretion organic acid anions by kidney ),AG may be NL
2. Early‐stageCKD: Preserved GFR but severe tubular damage(Reduced NH4 synthesis and excretion)
3. combined high and normal AG acidosis ΔAG/ΔHCO3 > 2(↓Hco3 less than expected) 1. Concurrent metabolic alkalosis2. preexisting chronic respiratory acidosis.
ΔAG /ΔHCO3

adverse effect HCO3 therapy: 1. intracellular acidification (due to the
accumulation of carbon dioxide after bicarbonate infusion) → ↓cardiac contractility
2. Metabolic alkalosis: ↑protein binding →↓ ionized calcium→↓cardiac contractility.
3. lactic acid production4. Volume overload