meningitis - bacterial -tuberculosis -viral...
TRANSCRIPT

MENINGITISMENINGITIS- BACTERIAL- TUBERCULOSISTUBERCULOSIS- VIRAL- JAMURJAMUR
ENCEPHALITISDr KIKING RITARWAN MKT SpSDr. KIKING RITARWAN, MKT, SpS
NEUROLOGY DEPARTMENT OF ADAM MALIK GENERAL HOSPITAL/ UNIVERSITY OF SUMATERA UTARA2009

MENINGITISMENINGITIS- Inflamations of the
meningealgcovering of Brainand and spinalcord
- LEPTOMENINGITIS- (arachnoid + pia)- PACHYMENINGITIS- (Duramater)

INFLAMATION OF THE It can be LEPTOMENINGESCAUSED BY BACTERIALINFECTION
It can be categorized into:
a. Spontaneous community acquired meningitisINFECTION
MANY ORG.CAN PRODUCE
acquired meningitisb. Post traumatic meningitis
following neurosur-gery or fx of the skull.
PYOGENIC MENINGITIS ex:Escherichia coli (50%),Strep. Pneumoniae (40%),
c. Device associated meningitis particularly in assoc. With CSF Shunts and drain.
Group B Streptococci (40%),L. monocytogenes (10), etc. Incidence rate are
influenced by country, ethnic group, social class g p,and deprivation, and immunization programmes

AGE Bact. Path. Emp. Th.0-4 weeks E. coli (50%) Amoxycillin + cefo, 0 4 weeks E. coli (50%) Amoxycillin cefo,
Group B. Strep (30%) or amoxycillin+ amino-
L. monocytogenes (10%) glycoside
Klebsiella pneumoniaeKlebsiella pneumoniae
4-12 weeks E. coli, Group B Streptocci, Amox + 3rd gen Ceph
L. monocytogenes, H. infl (cefotaxime or ceftr)
St P i Strep. Pneumoniae,
N. meningitidis
3 mo-18 ys H. influenzae, N. meningitidis, 3rd cephaloporin,
Strep. Pneumoniae Amox.
18-50ys Strep. Pneumoniae (40%), 3rd cephalosporine,
N.meningitidis(30%) Amox
>50ys Strep. Pneumo, N.meningitidis, Amox +
Aerobic gram (-) bacilii, 3rd gen cephalosp.
L. monocytogenes

The conditions occurs equally in both sexesChild d 6 h 1 h i k dChildren aged 6 month to 1 year are at the greatest risk andchildren under 15 years of age comprise 75% of all cases. Patientsaged 60 and older may be atypical.Symptoms and signsI. early infection: fever, headache, malaise,vomiteII. Higher ICP: vomite, headache, seizure, alteration of
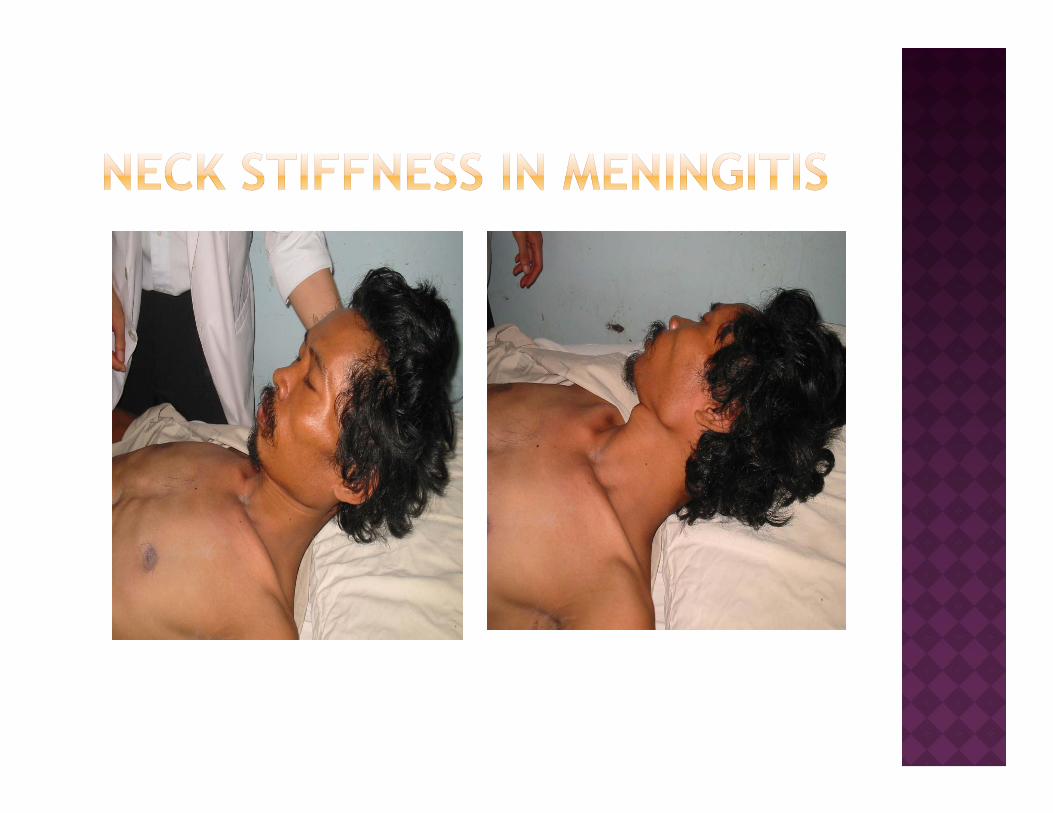
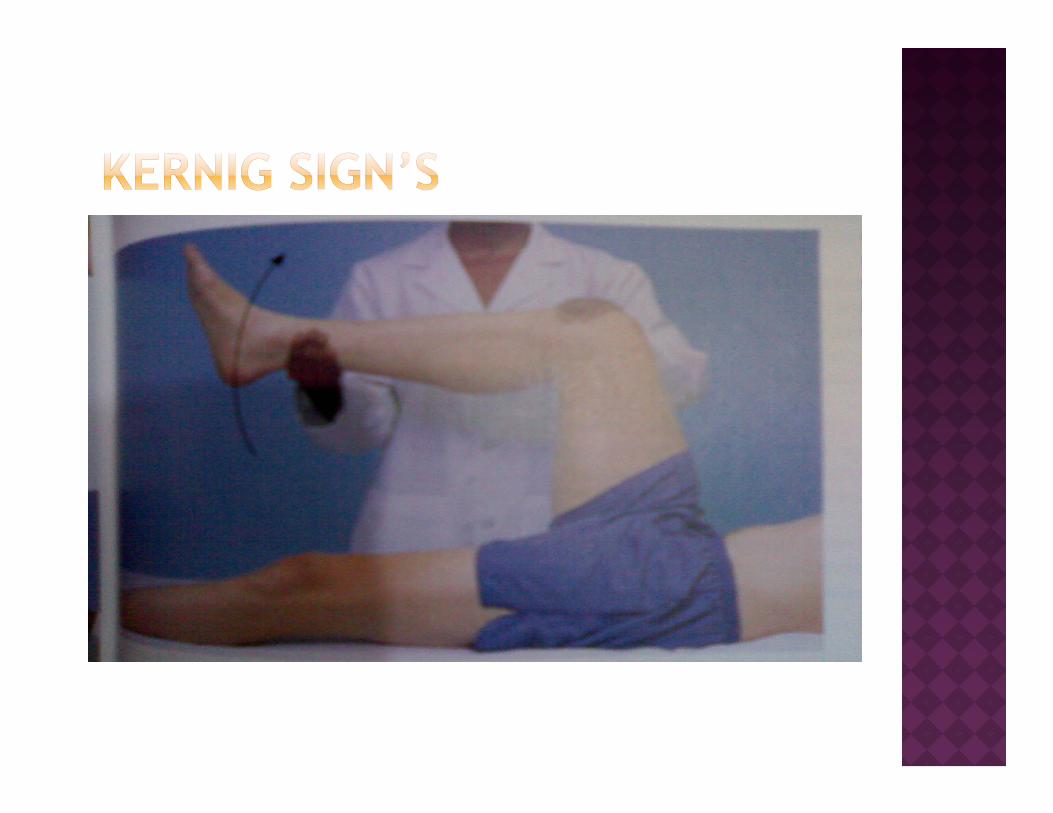
consciousness, papiledemaIII Meningeal irritation: nuchal rigidity Kernig andIII. Meningeal irritation: nuchal rigidity, Kernig and
Brudzinski +IV. CSF:neutrophilic pleocytosis, low glucose level,
elevated protein concentrationelevated protein concentration

Lumbal PunctureBlood should be drawn for blood culture before administration of antibiotic.Bacterial antigenBacterial antigenChest, skull mastoid and paranasal sinus x raysMRI or CT Neuroimaging shoul be performed before LP in the following settings:60 yo or older, Depressed LOC, Focal neurologic signs, papilledema, LOC, Focal neurologic signs, papilledema, Patients is immunocompromised.

CSF Parameter Bacterial meningitisg• WBC Count > 2000/ ul, >60% PMN• Glucose < 40 mg/ dl• Protein > 200 mg/ dl• Gram stain + 80%• Culture + > 90%

1.Antibiotic therapy should be administrated. A minimum of 2 weeks of therapy is recommendedtherapy is recommended.Age Antibiotic0 – 4 mgg Cefotaxim + Ampi4-12 mgg Gen III. Cephalos+ Ampi3 bl 8 h G C h A 3 bln- 18 thn Gen III. Ceph + Ampi atau
Ampi + chloramph.18 thn – 50 thn Gen III. Ceph + Ampi50 thn Gen III. Ceph + ampi.p p
2. When possible etiologies for meningitis include H. Influenza or S Pneumoniae in child, or S Pneumoniae in adults, give dexamethasone 0,15 mg/kg (IV) every 6 hours for 2-4 days in child and 10 mg IV every 6 h f 4 d i d lthours for 4 days in adults.

Cerebral abscessCerebral abscessEmpyema subduralConvulsieShock septicCerebral edemaInfarck serebralHerniation

Mental retardationMental retardationHydrocephalusConvulsie, psikose, pParese, deafness, blind.

TBM:is an infection TB haematogenous TBM:is an infectionof the meningescaused by the acid
spread infection to brain parenchyma or meninges
fast bacillusMycobacteriumt b l i
In the west country,the first make not much diff i b tuberculosis
The first clinicaldescrip Of TBM in
difference again, but lately incident mount drastically in all the world.descrip. Of TBM in
18 century-Sirroberts Whytt,
world.
TBM happened at all of age.roberts Whytt,
even beforeRobert Koch (1882)
of age.Before important HIV factor in prevalens is age

+ 1,7 milyar people ( 1/3 Mycobacterium tuberculosis
worldwide people) Mycobacterium tuberculosa infected.
gol ordo Actinomycetales, famili
Mycobacteriaceae, genus Mycobacterium
Sif t b ( ) til Reported CDC 2002 was 5,36 cases per 100.000 people, but worldwide the
f h
Sifat : aerob, spora (-), motil (-), berkembang biak lambat
Mati dgn pemanasan & sinar UVinfection rate is much
higher.
TB in Indonesian
UV
Bakteri batang tahan asam dgn pewarnaan Ziehl–Neelsen /Auramin leading to
occupy 3rd rank from 22 high
g
nickname “ red snapper”.
burden countries

Meninges tubercle; a central Acid fast of M. TBzone of caseation surrounded by epitheloid cells and some giants cells
Exudate: composed of fibrin
Acid fast of M. TB
Exudate: composed of fibrin, lymphocytes, plasma cells and other monoclear cells, some PMN leucocytes and areas of caseation necrosis.
Arterial become inflamed and occluded, leading to f l b i i f tifocal brain infarction

HIV INF.: 500 TIMES HIGHER CLINICAL FEATURESINCIDENCE OF TBM IN THEGENERAL POPULATION; HIVINFECTION INCREASES THELIFETIME RISK OF
CLINICAL FEATURES- HEADACHE, LETHARGY,
CONFUSION, DROWSINESS, FEVER, STIFF NECK, KERNIG LIFETIME RISK OF
DEVELOPING TB TO ONE INTHREE
ALCOHOL ABUSE,
, ,AND BRUDZINSKI SIGNS,
- FOCAL NEUROLOGIC DEFICIT: DUE TO BRAIN INFARCTION
DIABETES MELLITUS
MALIGNANCY
RECENT CORTICOSTEROID USE
CAUSED BY INFECTIOUS ARTERITIS
- RAISED INTRACRANIAL PRESSURE; DUE TO RECENT CORTICOSTEROID USE
POPULATIONS WITH A HIGHPREVALENCE OF PULMONARYTB
PRESSURE; DUE TO HYDROCEPHALUS


The course of the illness depends:The course of the illness depends:- on the extend of meningeal involvement,- the immune response of the host,p ,- the virulence of the organism,- and the stage at which treatment is g
administered.

Definite- bila kultur positi- otopsi positip, atau keduanyaProbable - likuor pleiositosis (>5/mm3), kultur bak-teri dan jamur negatip + salah satu:1 test tuberkulin positip1. test tuberkulin positip2. TB diluar SSP atau TB aktip sebelumnya3. glukosa likuor < 40 mg/dl4 protein likuor > 60 mg/dl4. protein likuor > 60 mg/dl

Arteritis thrombosis of a major arteryArteritis thrombosis of a major arterycerebral infarction.HydrocephalusSeizuresFocal motor deficits and impaired cognitiveHypopituitarism in childhood
Viral encephalitisViral encephalitisPartially treated pyogenic meningitisFungal infectiongOther inflammatory disordersThe presence of active TB elsewhere, and p ,the results of CSF examination are usually sufficient to establish the dx.

1. Lumbal Puncture1. Lumbal PunctureCSF Parameter TB meningitis
• WBC Count < 500/ ul, MN,• Gluco moderate or marked decrease• Protein marke increse• Gram stain + +.-• CSF lactic acid > 35 mg/dl.

2. Laju endap Darahj p3. Radiologic
3a. Chest x ray: detect pulmonary involvementinvolvement
3b. CT scan8 enhancement of the basal cistern.
3b. MRI are more sensitive than CT sans in detecting basal meningitis i f ti i t t iti h d h l infarction owing to arteritis hydrocephalus and parenchymal tuberculomas often in combination in AIDS patient.combination in AIDS patient.
4. Arteriografi

file 1: Contrast-enhanced computed tomography (CT) scan in a patient with tuberculous patient with tuberculous meningitis demonstrating marked enhancement in the basal cistern and meninges basal cistern and meninges, with dilatation of the ventricles.

file 2: Petechial file 2: Petechial hemorrhages in the subcortical white matter of th b i lt f the brain as a result of tuberculous meningitis–associated vasculitis.associated vasculitis.

file 3: Extensive file 3: Extensive infarcts of the right basal ganglia and internal capsule after the appearance of
liti i th vasculitis in the thalamoperforating arteries in a child arteries in a child treated for tuberculous meningitis.g

1. Combination of antituberculous drugTherapy WHO GILROY ATS- Initial INH+R+PZA+E INH+R+PZA INH+R+PZA atau S
atau R+ PZA+S
-2MO - 2 MO - 2 MO- Continued INH+R INH+R INH+R
-7 MO - 9 MO - 9 MO7 MO 9 MO 9 MOPyridoxine 50 mg/ hr
2. Spinal arachnoiditis and arteritis may show improvement when terated with corticosteroidimprovement when terated with corticosteroid.3. Seizure anticonvulsant4. ventriculoperitoneal shunt.

Mortality 10 & 20%yThe prognosis is poor in infants, the elderly, when treatment is delayed, and in patients with poor nutrition or in patients with poor nutrition or debilation from HIV infection or other chronic disease.Th t i l l i t d ith The outcome is clearly associated with the stage of the disease at dx and the introduction of early treatment. Those
h i d i h who are conscious and without neurological deficits have a good prognosis; those in coma at the beginning p g ; g gof treatment have 20% mortality and only 20 oercent make complete recovery.

Viral meningitis shares clinical features Viral meningitis shares clinical features with bacterial meningitis, but patients appear less ill and the disease follows a more benign course.Headache, often meningismus and photophobia, is often the presenting symptoms.Th h i l d h The most pathogens include herpes simplex-1 (HSV1), mumps, enterovirus, herpes zoster adenoviruses and Epstein herpes zoster, adenoviruses and Epstein barr virus.

Lumbal PunctureLumbal PunctureCells Glucose Protein Smear CSF lactic < 500 Normal Mild incr No org < 35 mg/dlg gMN /mm3PCRMRI predominant temporal lobe and insular changes in HSE-1 and basal ganglia lesion in japanese encephalitis.
TREATMENT:ACICLOVIR 10 mg/ kg iv every 8 hours for 10-14 days.

ETIOLOGYFungi invade of CNS producing meningitis in a small
fraction of patients with systemic fungal infection (mycoses)(mycoses)
The most pathogens are Cryptococcus neoformans, C idi d i iti C did lbi A ill H Coccidiodes immitis, Candida albicans, Aspergillus, H. Capsulatum, Blastomyces, and Mucor
Mucormycosis and aspergillosis usually spreads to the CNS from infected sinuses and generally cause local inflamation and necrosis rather than a diffuse inflamation and necrosis rather than a diffuse meningitis

Fungi can cause infection in patients with:1. Cancer2. Receiving corticosteroids3 Other immunosuppressive drugs3. Other immunosuppressive drugs
(Diabetes, malignancy, immunosuppressive th., or AIDS)
4 IV d b4. IV drug abuse.
Route of entryA. Haematogenous: from the heart, lung, GIT
and skinB. Direct: from the orbit and paranasal sinuses.

Symptoms progress over days, sometimes weeks, with Symptoms progress over days, sometimes weeks, with headache, nausea, vomiting and mild encephalopathy.Neurologic examination:1. meningeal irritation (+) 5, Visual loss2. papilledema 6. Confusional state 3. Cranial nerve palsies 7. Focal paralysis4. Ptosis

Lab investigations:Lab investigations:1. Blood culture2. Serum glucose g3.Arterial blood gases4. Electrolyte5. Liver function test6. UrinalysisCSF Examinations:Imaging

CSF Exam:- Pressure: Increased- Appearance: varies with organism
Whit Bl d ll 50 10 000 ( i d - White Blood cells: 50 – 10.000 (mixed or lymphocytic).
- Glucose :NormalGlucose :Normal- Protein: increased- Cryptoccal antigen is more sensitiveyp g- Fungal culture of CSF(+)

Chest X-ray : Hilar lymphadenopathy, Chest X ray : Hilar lymphadenopathy, cavitation, effusion.CT or MRI: mass lesion (Cryptococcus)
Amphotericin BAmphotericin B- Protocol, starting with 1 mg/ day- doubling the dose daily until reaching 16 g y g
mg per day, than increasing at increments of 10 mg until reaching full therapeutic g g pdose of 0,5 to 1,5 mg/ kg per day IV.

Dr. Kiking Ritarwan MKT, SpSEmail: kritarwan@ yahoo.com

Virus Representative virus for Neurologic DiseaseDNA- Herpesviruses HSV,VZV,CMV,EBV- Papovavirus PML
Posvirus Vaccinia- Posvirus Vaccinia- Adenovirus Adenovirus serotypeRNA- Enterovirus ( Picornavirus) Poliovirus, coxsackivirus, echovirus, enterovirus 70-( ) , , ,71, Hepatitis A- Togavirus, alphavirus ( arbovirus) Equine encephalitis- Flavivirus (arbovirus) St louis enceph, Japanese and Tic Borne encephenceph- Orbovirus (Arbovirus) Colorado Tick fever- Bunyavirus (arbovirus) California enceph- Togavirus, rubivirus Rubella- Orthomyxovirus Influenza- Rhabdovirus Rabies- Retrovirus HIV, HTLV

RUTE INFEKSI:Saluran pernafasan
HIV AND BRAIN (1)Saluran pernafasan : parotitis, varicella, morbilli
MeningitisHIV itselfTB morbilli
Saluran makanan : polio, enterovirus
TB CryptococcalSyphiliticp ,
Mukosa kelamin : Herpes simpleks
yp
Space occupying l iInokulasi : spt
gigitan binatang
lesionsToxoplasmosisTuberculomas
(rabies a nyamuk)Placenta : CMV + R b ll
TuberculomasLymphoma
Rubella

Encephalitis HIV AND SPINAL CORDHIV dementiaProgressive multifocal leukoencephalopathy
Vacuolar myelopathySyphilis