meme phung zhi yuan quek alison wong case d - chronic diabetes
TRANSCRIPT
Meme PhungZhi Yuan Quek
Alison Wong
Case D - Chronic Diabetes
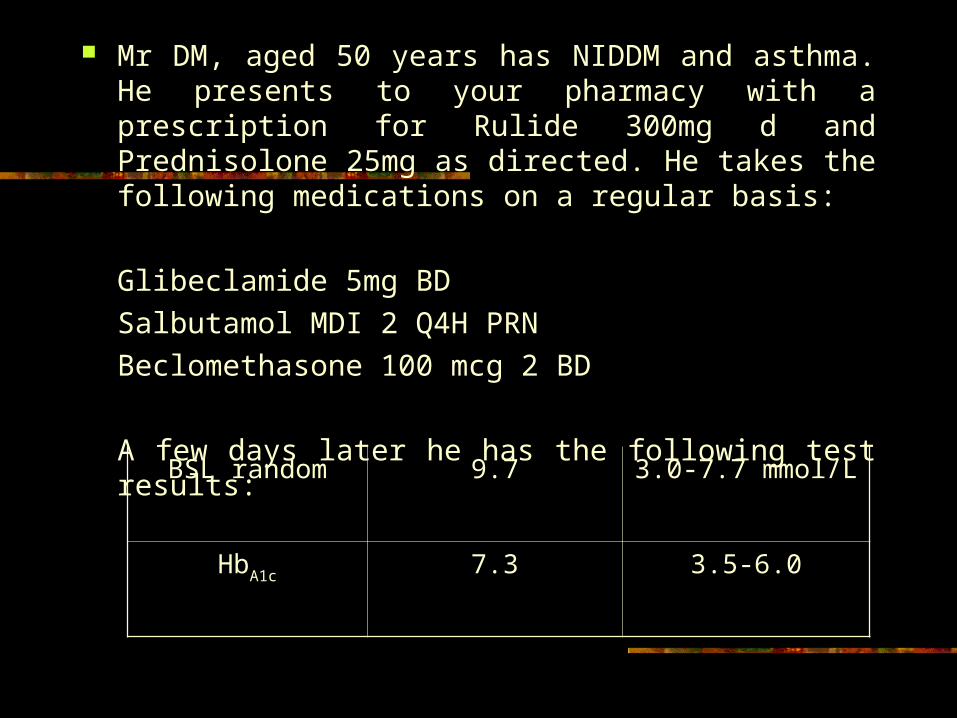
Mr DM, aged 50 years has NIDDM and asthma. He presents to your pharmacy with a prescription for Rulide 300mg d and Prednisolone 25mg as directed. He takes the following medications on a regular basis:
Glibeclamide 5mg BD
Salbutamol MDI 2 Q4H PRN
Beclomethasone 100 mcg 2 BD
A few days later he has the following test results:
BSL random 9.7 3.0-7.7 mmol/L
HbA1c 7.3 3.5-6.0
Glycated Haemaglobin A1c (HbA1c)
Rationale for measuring HbA1c Its use in monitoring the patient
status

What is HbA1c?
Formed by glycosylation of proteins.

Glycosylation of ProteinsHC
HC
CH
O
OH
OH
HC OH
HC
CH2OH
OH
HC
HC
CH
N-Protein
OH
OH
HC OH
HC
CH2OH
OH
Protein-NH2 +
Glucose Aldimine(Schiff base)
HC
HC
CH
O
OH
HC OH
HC
CH2OH
OH
NH Protein
Amadori

A non-enzymatic reaction, Rate of production of the glycosylated product depends largely on the amount of Glucose in the blood.
i.e. The amount of glycated Hb is directly proportional to the average concentration of glucose in the blood.
Linear regression to estimate the Mean Blood Glucose from the HbA1c value:
MEAN BLOOD GLUCOSE estimate = 33.3 (% HbA1c) -86
HbA1c will normally exist throughout the life span of the RBCs in the circulation ~90-120days.
HbA1c reflects the mean plasma glucose concentration for the preceding 6 week-period
Normal person, about 3-6% of Hb is glycated;
Diabetic, the % of HbA1c may double or even triple, depending on the degree of hyperglycaemia.
Why is measuring HbA1c important for managing BSL?
Correlation between HbA1c and glycemic control (Koenig RJ,et al 1976)
Blood glucose test measures glucose in blood at the time of testing
HbA1c shows glycaemic content of haemoglobin in patient’s
blood over time, HbA1c reflects BSL control over the last 4-8 weeks. Reliable reflection of long-term glucose control not affected
by brief fluctuations in glucose levels.
Allows physicians to assess long-term compliance with prescribed medications, diet or exercise.
Can predict risk for diabetic complications. DCCT (Diabetes Control and Complications
Trial) Strong correlation between HbA1c and rate
of progression of diabetic complications (eg. Retinopathy, diabetic nephropathy, etc.) Higher the HbA1c value higher the risk of
developing diabetic complications.
The American Diabetes Association (ADA)
recommends HbA1c testing at least twice a year in
patients with stable glycemic control, and 4 times per year for those whose glycemic
levels are not well controlled, or whose treatment regimen has been modified.
Ideal range for HbA1c is below 7%
DRUG OR DISEASE FACTORS THAT MAY HAVE AFFECTED THE
RESULTS
Mr DM has NIDDM and asthma. He presents with a prescription for Rulide 300 mg d and Prednisolone 25 mg as directed.
Current Medications:
Glibenclamide 5 mg bd
Salbutamol MDI 2 q4h prn
Beclomethasone 100 mcg 2 bd
Drug Factors
1. Corticosteroids
potential for increasing blood glucose levels in diabetics
Mechanism : - by increasing gluconeogenesis
synthesis of glucose from non- hexose substrates
mobilization of amino acids from extrahepatic tissues
stimulation of fat breakdown in adipose tissue
- by decreasing glucose utilization
- by increasing in peripheral resistance to insulin
blood glucose levels may increase by
10% to 20%
may impair glucose tolerance, unmask latent diabetes, or aggravate pre-existing disease
2. Beta 2-agonist
Mechanism of action thought to be mediated via stimulation of cAMP production
triggering a series of intracellular events
raised blood glucose levels
- by stimulation of hepatic glucose
production
- stimulation of glucose release
- stimulation of glycogenolysis and
glycolysis
Standardisation of monitoring glycated
haemoglobin

Question
Despite the importance of monitoring glycated haemoglobin standardisation of protocols has proved problematic.
Outline the various approaches that have been examined, the problems associated with these approaches and the implications of these analytical problems in interpreting clinical test data.
Limitations
GHb analysis is subject to certain limitations
e.g. haemolysis or significant blood loss will alter the amount of GHb that accumulates
Interassay variability and haemoglobin variants have restricted the use of GHb testing.
Progress in the standardisation of GHb assays and accurate GHb measurement in patients with haemoglobin variants lead to optimism that the problems may be approaching resolution.
BRIEF OVERVIEW
There are >30 different GHb assay methods, which are based on two principles.
1. Separates glycated from non-glycated haemoglobin components based on differences in their charges e.g cation-exchange chromatography and electrophoresis
2. Variations in structure related to the presence of the attached glucose.
Majority are performed by ion-exchange HPLC or immunoassay
These assay measure HbA1C or total GHb (HbA1C and haemoglobin glycated at other sites)
Results reported on the same blood sample can vary substantially, depending on the analyte measured and the method used.
Hb variants >850 Hb variants identified present in up to 1/3 of all diabetic
individuals in the world two recent reports address this concern
.
Problems
Haemoglobinopathies may interfere with GHb analysis
results may be falsely increased or decreased, depending on the particular method and the haemoglobinopathy.
Hb variants that cannot be separated from HbA or HbA1C will produce spuriously increased or decreased results by ion-exchange HPLC.
Most assays routinely used in clinical laboratories for GHb analysis are subject to interference by Hb variants.
Hb variants can be detected by examining the chromatogram
interferences depend on the antibody used and vary among assays.
Hb variants cannot be identified by immunoassays
The problem of assessing glucose control by measurement of GHb in patients with Hb variants has not been completely solved.
However HbA1C can be measured accurately in the presence of most haemoglobinopathies.
However different methods used to analyse GHb have different reference intervals
Standardisation is needed to compare results across all types of methods used.
Problem Resolved
Standardisation of measurements were needed for comparison for the DCCT-based treatment goals
Committees were established independently to standardise GHb assays.
1. AACC
2. IFCC

1. AACC
Reference methods used as the designated
comparison method for GHb
standardisation includes: DCCT (Diabetes Control and Complications
Trial) UKPDS (United Kingdom Prospective
Diabetes Study) NGSP (National Glycohaemoglobin
Standardisation Program) formed to harmonise GHb assays with the DCCT assay.
NGSP (National Glycohaemoglobin Standardisation Program) formed to harmonise GHb assays with the DCCT assay.
This procedure was a pragmatic first step and that formal standardisation required much more work.

NGSP
Uses a network of reference laboratories and interacts with manufacturers of GHb methods to allow them to establish traceability to the CPRL (Central Primary Reference Laboratory)
CPRL analyse HbA1C by HPLC according to the method used in the DCCT
Methods and laboratories can then be certified as traceable to the DCCT
2. IFCC
International Federation of Clinical Chemistry primary reference material: mixture of purified
HbAo and HbA1C reference method: Hb cleaved into peptides by
endoproteinase Glu-C glycated and non-glycated N-terminal
hexapeptides are separated and quantified by HPLC-(ESI-MS) or HPLC-capillary electrophoresis.
HbA1C measured as a ratio between glycated and nonglycated N-terminal hexapeptides.
Method has high specificity which yields lower values than commercial methods.
Approved by IFCC and may provide foundation for global standardisation of GHb measurements.
Standardisation Protocols
Clearly the development of a valid chemical standard is highly desirable.
Parallel line between NGSP values and the IFCC reference method
Important that expression of results remains linked to DCCT/UKPDS values.