medications and breastfeeding safety done by :mona al saqqa proposed to :dr.mahmoud taleb
TRANSCRIPT
Medications and Breastfeeding Safety
Done by :Mona Al Saqqa
Proposed to :Dr.Mahmoud Taleb
ال�د�ي�ه� : } ب�و� ان� �ن�س� اإل� ي�ن�ا و�و�ص� تعالى قالف�ي �ال�ه و�ف�ص� �و�ه�ن ع�ل�ى! ن$ا و�ه� �ه م%
�أ �ل�ت�ه م� ح� �ير ال�م�ص� �ل�ي� إ ال�د�ي�ك� ل�و� و� ل�ي ك�ر� اش� ن�
أ� ي�ن� ع�ام�لقمان( 14) سورة ]

About Breastfeeding
• Breast milk is recognized as the optimal source of nutrition for infants, with documented benefits not only to infants, but also to mothers, families, and societies.
• Evidence indicates that breast-feeding decreases the incidence or severity of many infectious processes (e.g., otitis media, respiratory infections, urinary tract infections) in infants.
• Its benefits are so important that breastfeeding should only be discontinued if there is strong evidence that a drug taken by the mother will harm the infant and there is no alternative treatment.

Some Benefits for Baby

Breastfeeding and medication
• Many mothers are required to use drugs
during breastfeeding either for chronic or acute use, and almost all drugs transfer into breast milk..
• So:• IS THIS HARMFUL FOR BABY??? and,• SHOUID THE MOTHER STOP
BREASTFEEDING ??

Breastfeeding and medication
• Taking medication does not usually mean that a mother has to stop breastfeeding temporarily or permanently.
• The number of adverse reactions to drugs passing through breast milk is small ..
• In general less than 1% of a drug will pass through breastmilk to the baby.

Factors Influencing Drug Safety
Infants factors-:
Age
Body weight
Health status
Infants factors-:

Pediatric physiologic ch.ch affecting pharmacokinetics
• Thin, permeable skin –increased absorption of topicals
• Immature blood-brain barrier—increased distribution into the CNS until age 2
• Altered protein binding until age 1• Decreased activity of metabolizing enzymes
in infants, increased in children
• Increased percentage of body water• infants have glomerular filtration rates
approximately one-third of adult values after adjusting for difference in body surface area, and premature infants have even more impaired clearance
Pediatric physiologic ch.ch affecting pharmacokinetics

Prematurity concerns
• Less body fat means lipid soluble drugs more likely to deposit in their lipid-rich brain
• Less available plasma protein (albumin) for binding due to their smaller bodies– May also have less protein
from birth complications such as acidosis and hypoxia

Prematurity concerns
• Immature liver less effective at metabolizing drugs, risk of drug building up in their system.
• Bilirubin levels may be increased by the use of some drugs (such as sulfadiazine) which compete with bilirubin for protein binding sites.
• Premature babies also consume less milk

2/Drugs factors

Diffusion / active transport
Plasma level
Lipid solubility
Drug pH
Molecular weight
Protein binding
Half life
Oral bioavailability
Drugs factors
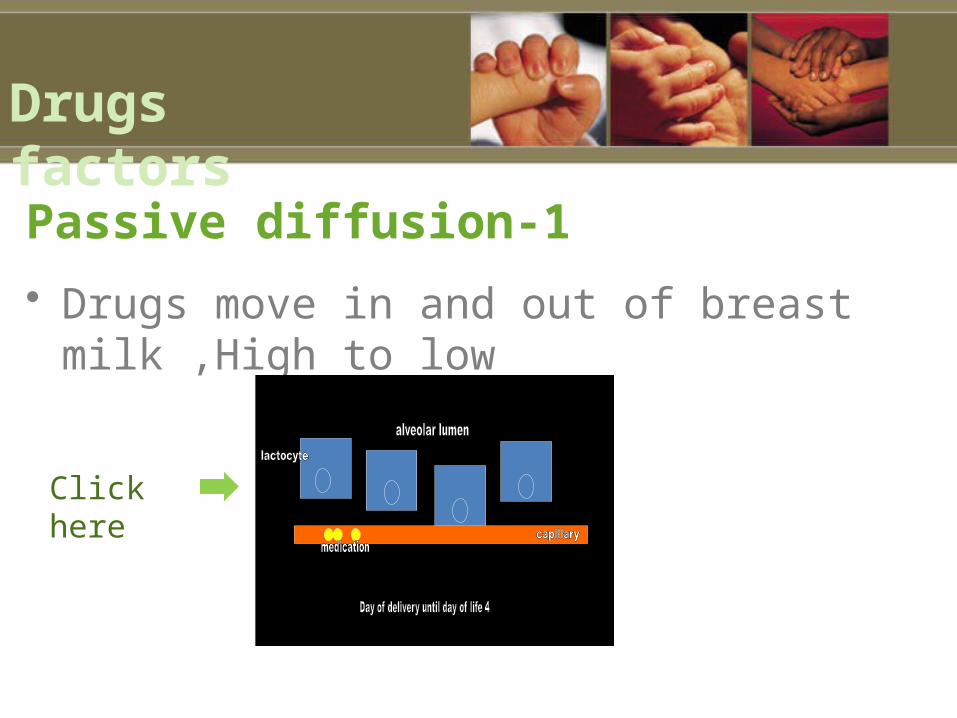
1-Passive diffusion
• Drugs move in and out of breast milk ,High to low
Click here
Drugs factors

2 -Molecular weight• High molecular weight limits movement
into breast milk• MW >500 daltons does not enter breast
milk• Insulin: MW > 6,000 daltons• Heparin: MW 40,000 daltons• Ethanol: MW 200
Drugs factors

3-Protein binding• Medications circulate in maternal circulation bound
or unbound to albumin • Only unbound drug gets into maternal milk• Definition of good protein binding = > 90%• High protein binding:• Propranolol 90% L2• Diazepam 99% L3
Drugs factors
4-Lipid solubility• Drugs that are very lipid soluble penetrate into
breast milk in higher concentration• Drugs that are active in the CNS are drugs with high
lipid solubility• Phenobarbitone has high lipid/water partition
coefficient of 5.9.• Thiopentone sodium has a chloroform/water
partition coefficient of about 100
Drugs factors
5-Oral bioavailability
Drugs factors
• Maternal GI Tract• Maternal Plasma
Mother body
Summary
Drugs transfer into human milk if they:1 -Attain high conc. in maternal plasma
2 -Are small enough
3 -Are non-protein bound
4 -Are highly lipid soluble
5-Then conc. in breast milk: Are affected by oral bioavailability in baby’s gut
Drugs factors

Before prescribing for any mother and baby pair several factors should be taken into consideration :
Avoid unnecessary drug use and limit use of OTC products
Assess the benefit/risk ratio for both mother and infant
Avoid use of drugs known to cause serious toxicity in adults or children
Drugs licensed for use in infants do not generally pose a hazard
What should mother do ??

Neonates (esp premature infants) are at greater risk from exposure to drugs via breast milk.
Route of administration (minimum amount of drug to the infant.
Avoid long-acting preparations
Monitor Infants exposed to drugs via breast milk for unusual signs/symptoms
Avoid new drugs if possible


In general, baby gets <1% of maternal
dose of drug

Lactation Risk Category

Classification according to WHO
1 .Compatible with breastfeeding
2 .Compatible with breastfeeding. Monitor infant for side-effects
3 .Avoid if possible. Monitor infant for side-effects
4 .Avoid if possible. May inhibit lactation
5 .Avoid

Antibiotics:
• All these are : Compatible with breastfeeding• amoxicillin• ampicillin• benzathine benzylpenicillin• benzylpenicillin• cloxacillin• phenoxymethylpenicillin• procaine benzylpenicillin• amoxicillin+clavulanic acid• ceftazidime• ceftriaxone• imipenem+cilastatin

•chloramphenicol ❏ Avoid if possible, especially if the infant isless than 1 month old. Monitor the infant for side-effects (haemolysisand jaundice).Theoretically, there is a risk of bonemarrowdepression, but this has never been reportedciprofloxacin ❏ Avoid if possible, until more data are availabledoxycycline ❏ Avoid if possible. Possibility of staining the infant’s teeth.Single dose is probably safe• erythromycin Compatible with breastfeeding❏• gentamicin Compatible with breastfeeding. Monitor infant for thrush ❏
and diarrhoea• metronidazole Avoid if possible❏ . Animal data suggest it may be• carcinogenic. If given in single dose of 2 grams,discontinue
breastfeeding for 12 hours.
Antibiotics:

HALE’S L.R.C:
• Dr Thomas W. Hale is a clinical pharmacologist, professor at Texas Tech University School of Medicine, and author of Medications and Mothers' Milk
• He is an expert on the use of medications in breastfeeding women and he has traveled the world lecturing on this topic. He is considered one of the leading experts in the field of human lactation and the use of medication.
• Hale’s Medications and Mothers’ Milk, now in its 14th edition, has become the standard reference for rating the breastfeeding safety of medications. Which is called : Lactation Risk Categoeies (LRC)
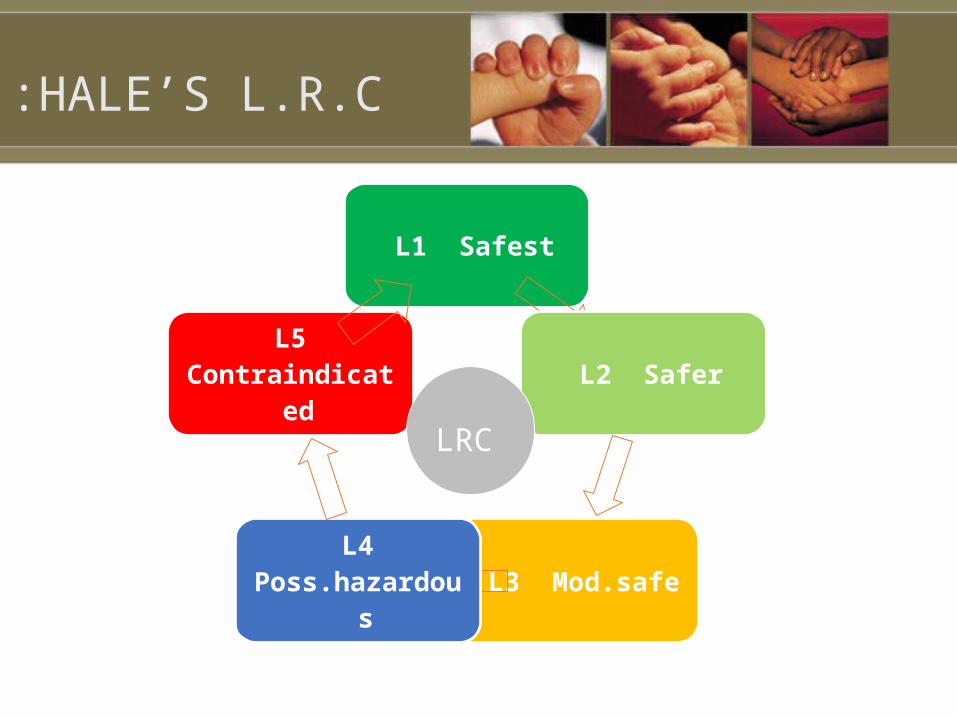
L1 Safest
L2 Safer
L3 Mod.safe L4 Poss.hazardous
L5 Contraindicated
LRC
HALE’S L.R.C:

L1 “Safest
Drug which has been taken by a large number of breastfeeding mothers without any observed increase in adverse effects in the infant.Controlled studies in breastfeeding women fail to demonstrate a risk to the infant and the possibility of harm to the breastfeeding infant is remoteOr the product is not orally bioavailable in an infante.g. vancomycin, dicloxacillin, acetaminophen, cephalexin)

L2 Safer:
Drug which has been studied in a limited number of breastfeeding women without an increase in adverse effects in the infant. And/or, the evidence of a demonstrated risk which is likely to follow use of this medication in a breastfeeding woman is remote.e.g. prednisone, warfarin, ranitidine, phenytoin, Zoloft, Paxil)

L3 Moderate Safe:
There are no controlled studies in breastfeeding women, however the risk of untoward effects to a breastfed infant is possible OR; controlled studies show only minimal non threatening adverse effects. Drugs should be given only if the potential benefit justifies the potential risk to the infante.g. cyclosporine, levofloxacin, morphine, glyburide)

L4 “Hazardous:”
There is positive evidence of risk to a breastfed infant, or to breastmilk production, but the benefits from use in breastfeeding mothers may be acceptable despite the risk to the infant.
e.g. captopril , Demerol, Cafergot)

L5 “Contraindicated:”
Studies in breastfeeding mothers have demonstrated that there is significant and documented risk to the infant based on human experienceOr ; it is a medication that has a high risk of causing significant damage to an infant.The risk of using the drug in breastfeeding women clearly outweighs any possible benefit from breastfeeding.The drug is contraindicated in women who are breastfeeding an infant.e.g. bromocriptine, cocaine, isotretinoin, Taxol,)

Analgesics & NSAIDS
• Codeines - L2 .
• Aspirin - L3 (metabolic acidosis 1 case, at high
dose)
• Indomethacin - L3 (seizure 1 case)
• Cox-2 inhibitors - No available information
• Diclofenac - L2 (non reported via milk)

Antimicrobials (1)
• Ciprofloxacin- L4 ( Arthropathies reported in
animal embryo, no evidence in humans)
• Nalidixic acid - L4 (reported case of hemolysis in
infants with G6PD def.
• Clindamycin - L3 (1 case of pseudomemb.colitis
but rare, observe for diarrhoea, approved by AAP
for use in BF mother

Ciprofloxacin Breastfeeding Warnings
Ciprofloxacin is excreted into human milk. Concentrations found in breast milk have ranged from 85% (at 24 hours post dose) to 214% (at 4 hours post dose) of maternal serum concentration.
In one case report, a 2-month-old girl developed perforated pseudomembranous colitis following ingestion of ciprofloxacin via the mother's milk and subsequently required a bowel resection. In addition, quinolone-induced cartilage erosion and arthropathies that have been observed in juvenile animals render some concern over its possible toxic effects on the developing joints of nursing infants.

Antimicrobials (1)
• Sulfonamides : L2-3 (avoid in sick infants,
prematurity, stress,
hyperbilirubinemia, G6PD def.
• Co-trimozole: L3 (non reported, caution in
hyperbilirubinemia & G6PD def.)
• Metronidazole - L2 (BF should be withheld
until 12-24 hr after 2 g dose)

Antimicrobials (2)
Metronidazole T1/2 = 8.5 hr
In mother receiving 2 g dose
Av. drug conc. 2 hr = 45.8 mg/L
8 hr = 27.9 mg/L
12 hr = 19.1 mg/L
12 -24 hr = 12.6 mg/L
Rx level in infants /children = 7.5-30 mg/L
No report of AE in breastfed infants for 2 g dose or
250 mg X 3 /d X 10 d

Antidepressants (1)
SSRI :
• Fluoxetine -L3 in newborn, L2 in olders [ longer T1/2 --
> relatively greater amount in breastmilk > sertraline
(Zoloft) & paroxetine(Paxil) ]
• Citalopram -L3 (2 cases of excessive somnolence,
(Celexa) decreased feeding, & wt. loss )

Alcohol and Nicotine
• It is advised that women avoid breastfeeding for at least 2 hours after one or two alcoholic drinks, since it passes quickly into the milk
• No need to pump and dump the milk during the 2 hours, as the alcohol will have been reabsorbed into the plasma.
• Women should quit smoking, but for those who cannot, they should be advised to smoke only after nursing so the baby is exposed to the least amount of nicotine possible.
• Women should NEVER smoke around the baby.• Maternal smoking also decreases milk supply, so the growth
of the infant should be monitored carefully.

Summary of distribution of drugs into breast milk


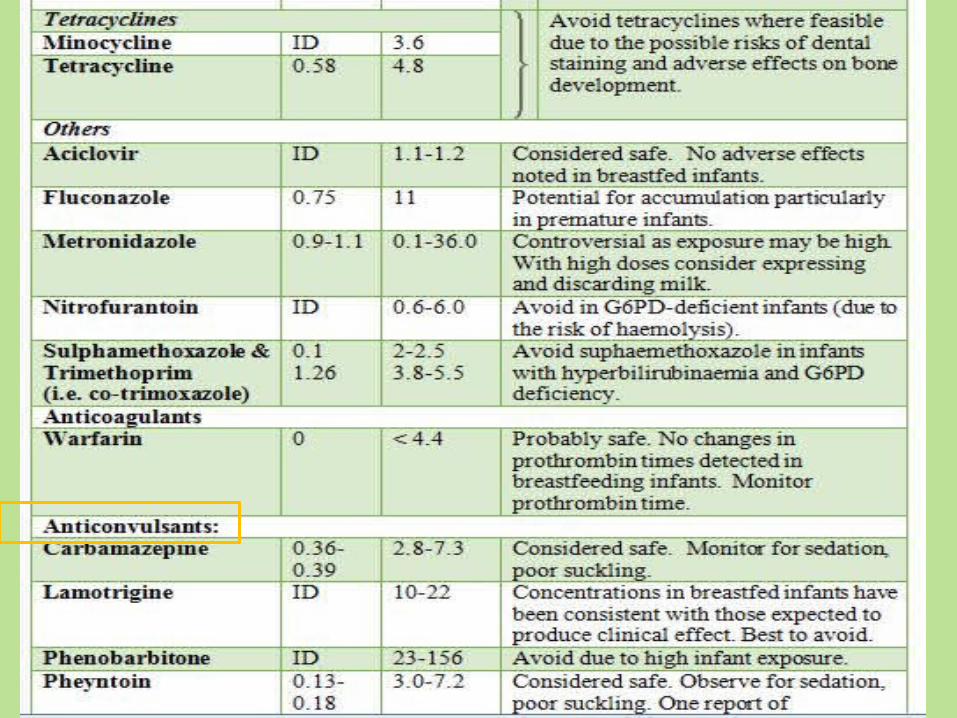



http://www.medsafe.govt.nz/profs/puarticles/lactation.htm

Drugs commonly prescribed in Specific
Conditions
Drugs commonly prescribed in Specific
Conditions

Drugs commonly prescribed (1)
Caution Alternative Recommended Condition
/ 1-Cetrizine 2-Loratadine
3-Sedatingantihist
4-Decongestants5-Cromolyn
1-Beclomethasone“(Beconase)
2-Fluticasone(Flonase)
Allerg.rhinitis
1-Atenolol ((Tenormin
2-Soralol Diltiazem
1-Nifedipine2-Hydralazine
(Apresoline)4-Captopril
5-Enalapril
1-Hydrochlothiazide2-Metoprolol tartrate
(Lopressor)3-Propanolol
4-Labetalol
CVS

Caution Alternative Recommended Condition
Fluoxetine NortriptylineDesipramine
SertralineParoxetine
Depression
Metformin Thiazolinediones
AcarboseInsulinGlyburide Glipizide Tolbutamide
DM
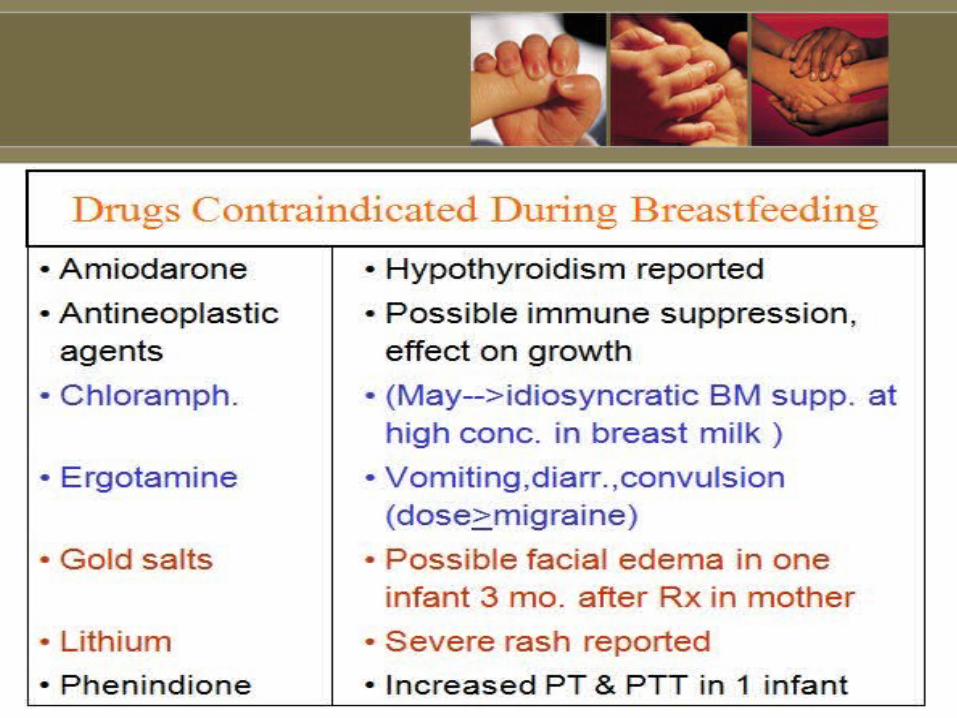
Contraindication drugs:




الله بحمد تم ، للمتابعة شكرا