medicare wage index project ffy 2015 data ffy 2011 and subsequent years data presenter: dale baker...
TRANSCRIPT

MICHIGAN HEALTH & HOSPITAL ASSOCIATION
Medicare Wage Index ProjectFFY 2015 Data
FFY 2011 and Subsequent Years Data
Presenter:Dale Baker
Baker Healthcare Consulting, Inc.
Dial in Number:1-888-809-4012Access Code: 7038619
Please mute your phone by pressing *6 once you have entered the conference call.
October 9, 2013
2
TOPICS
We will follow the book:
The Basics – Wage Index 2014 Wage Indexes
Hot TopicsSpecial Considerations
Work PlanThe Future of the Wage Index

3
FIRST THE BACKGROUND MATERIALS
Page 1 Wage Index Calculation Flow shows the use of the data
CMS 2552-10 replacing 2552-96 and instructions Also, the Wage Index Instruction Form Occupational
Mix Survey Instructions and background August 19, 2013 Federal Register provisions includes
instructions. 2011 Federal Register provisions for pension cost
finding (not wage index) Finally Data on the “Access Clause” for Contracting
4
THE BASICS
5
COST REPORTING DATA USED FOR WAGE INDEXES BY YEAR
Data for FFY 2011 (cost reporting periods beginning October 1, 2010 through September 29, 2011) will be used for FFY 2015 wage index computation.
For short periods beginning October 1, 2010 through September 29, 2011, CMS uses the longest period, or if two periods are the same length, the most recent period. CMS annualizes short period data.
6
COST REPORTING DATA USED FOR WAGE INDEXES
Wage data includes: Salaries and hours from IPPS hospitals (including paid
lunch hours and hours for military leave and jury duty) Home Office Salaries and hours Certain contract labor: direct patient care, some top
management, pharmacy, lab, physician nonteaching Part A costs, dietary, housekeeping & administrative, and general (includes legal, audit and consulting).
Wage-related costs Certain outpatient services included in OPPS (e.g., ED,
provider-based clinics) Physician Part A (non-teaching)
Wage data excludes: Non-IPPS services, GME, CRNAs, RHC & FQHCs, CAHs, physician Part B and Physician Part A teaching.
7
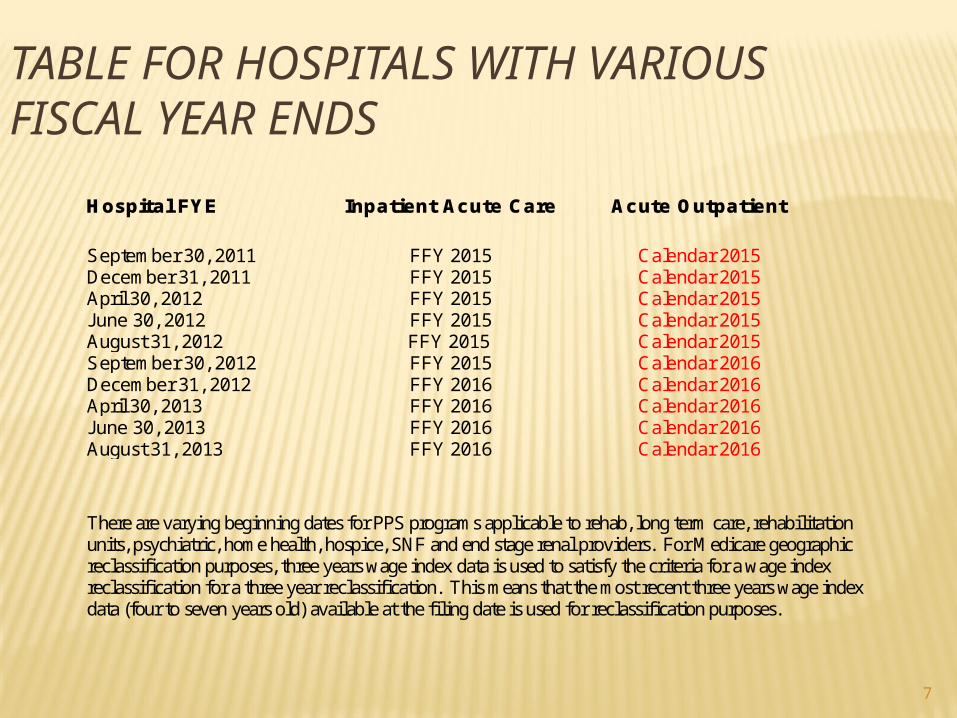
TABLE FOR HOSPITALS WITH VARIOUS FISCAL YEAR ENDS
Hospital FYE Inpatient Acute Care Acute Outpatient
September 30, 2011 FFY 2015 Calendar 2015 December 31, 2011 FFY 2015 Calendar 2015 April 30, 2012 FFY 2015 Calendar 2015 June 30, 2012 FFY 2015 Calendar 2015 August 31, 2012 FFY 2015 Calendar 2015 September 30, 2012 FFY 2015 Calendar 2016 December 31, 2012 FFY 2016 Calendar 2016 April 30, 2013 FFY 2016 Calendar 2016 June 30, 2013 FFY 2016 Calendar 2016 August 31, 2013 FFY 2016 Calendar 2016 There are varying beginning dates for PPS programs applicable to rehab, long term care, rehabilitation units, psychiatric, home health, hospice, SNF and end stage renal providers. For Medicare geographic reclassification purposes, three years wage index data is used to satisfy the criteria for a wage index reclassification for a three year reclassification. This means that the most recent three years wage index data (four to seven years old) available at the filing date is used for reclassification purposes.
8
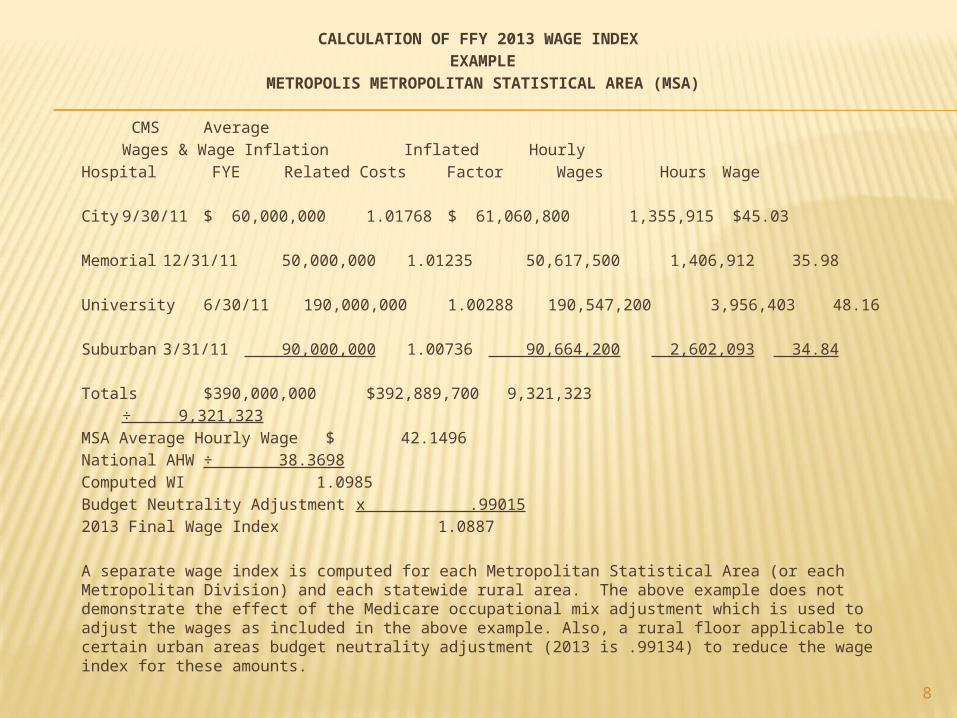
CALCULATION OF FFY 2013 WAGE INDEX EXAMPLE
METROPOLIS METROPOLITAN STATISTICAL AREA (MSA)
CMS AverageWages & Wage Inflation Inflated Hourly
Hospital FYE Related Costs Factor Wages Hours Wage
City 9/30/11 $ 60,000,000 1.01768 $ 61,060,800 1,355,915 $45.03
Memorial 12/31/11 50,000,000 1.01235 50,617,500 1,406,912 35.98
University6/30/11 190,000,000 1.00288 190,547,200 3,956,403 48.16
Suburban 3/31/11 90,000,000 1.00736 90,664,200 2,602,093 34.84
Totals $390,000,000 $392,889,700 9,321,323÷ 9,321,323
MSA Average Hourly Wage $ 42.1496National AHW ÷ 38.3698Computed WI 1.0985Budget Neutrality Adjustment x .990152013 Final Wage Index 1.0887
A separate wage index is computed for each Metropolitan Statistical Area (or each Metropolitan Division) and each statewide rural area. The above example does not demonstrate the effect of the Medicare occupational mix adjustment which is used to adjust the wages as included in the above example. Also, a rural floor applicable to certain urban areas budget neutrality adjustment (2013 is .99134) to reduce the wage index for these amounts.

9
USES OF THE MEDICARE WAGE INDEX
Wage Index <1.0000 Wage Index >1.0000
62% 38% 100% 69.6%* 30.4% 100%Labor Non Labor NonRelated Labor Total Related Labor Total$3,329.67$2,040.71$5,370.28$3,737.71$1,632.57$5,370.28
Example WI x .9831 x 1.0887
Base DRGPayment
Wage $3,273.30 $4,011.15Non-Wage$2,040.71 $1,632.57
Total $5,314.01 $5,643.72
Times to DRG weighing factor
10
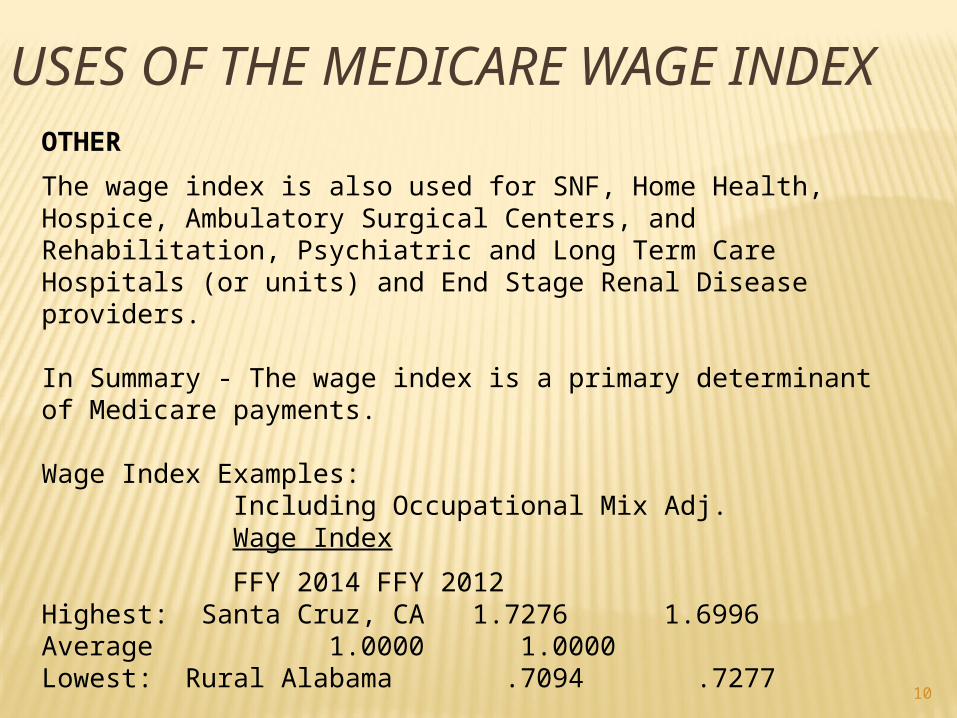
USES OF THE MEDICARE WAGE INDEX
OTHER
The wage index is also used for SNF, Home Health, Hospice, Ambulatory Surgical Centers, and Rehabilitation, Psychiatric and Long Term Care Hospitals (or units) and End Stage Renal Disease providers.
In Summary - The wage index is a primary determinant of Medicare payments.
Wage Index Examples:Including Occupational Mix Adj.Wage Index
FFY 2014 FFY 2012Highest: Santa Cruz, CA 1.7276 1.6996Average 1.0000 1.0000Lowest: Rural Alabama .7094 .7277
11
IMPACT OF 1% INCREASE OF A WAGE INDEX
Hospital with 5,000 Medicare discharges:
Perhaps: $397,000 - $431,000 Plus DSH & IME
12
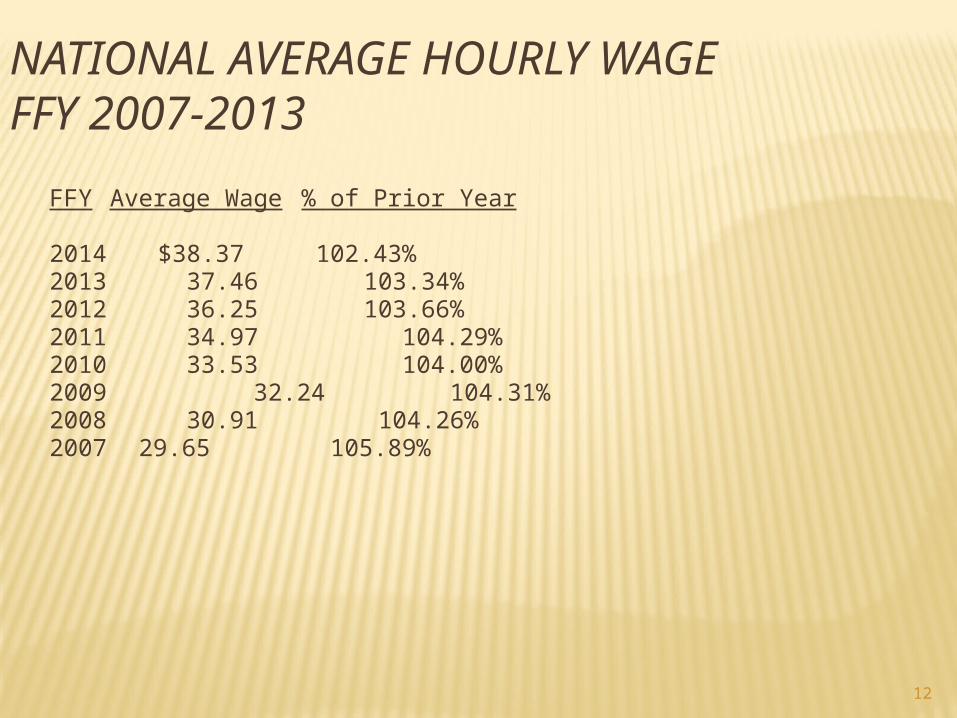
NATIONAL AVERAGE HOURLY WAGEFFY 2007-2013
FFY Average Wage % of Prior Year
2014 $38.37 102.43%2013 37.46 103.34%2012 36.25 103.66%2011 34.97 104.29%2010 33.53 104.00%2009 32.24 104.31%2008 30.91 104.26%2007 29.65 105.89%
13
WAGE INDEX & STATISTICAL TABLES
CMS has discontinued publishing wage index and statistical tables in the Federal Register.
Go to the CMS website to obtain these tables.

14
LOCAL WAGE INDEXES
See Workbook
15
2015 WAGE INDEX TIMETABLE
September 13, 2013 CMS releases public use files
November 21, 2013 Receipt deadline for hospital to submit wage data and hour revisions to intermediary (or
MedicareAdministrative Contractor – MAC). Revisions will be
accepted applicable to wage index data and revisions
of MOMA data hospitals must include “adequate supporting documentation".
February 10, 2014 FI’s complete desk reviews and transmits data to CMS. FI’s notify State hospital
association of non-responsive hospitals.
February 20, 2014 Public Use File released.
March 3, 2014 Hospital deadline to request data correction due to mishandling of data by FI or CMS.
16
2015 WAGE INDEX TIMETABLE (CONT.)
April/May, 2013 Publication of Proposed IPPS Rule.
April 16, 2014 Receipt deadline to appeal Fiscal Intermediary
determination to CMS with a copy to theFiscal Intermediary.
May 2, 2014 Public Use File is published with almost final data.
June 2, 2014 Hospital deadline to request changes due to
Fiscal Intermediary or CMS handling errors.
August 1, 2014 Final IPPS Rule issued.
October 1, 2014 Effective date of Medicare wage indexes.

17
CRITICAL PATH FOR APPEAL RIGHTS FFY 2015
1. Receipt by MACs of adjustments by November 21, 2013 deadline with "supporting documentation”.
2. Obtain written denial from MAC by March 3, 2014.3. Receipt of request for CMS review (copy to MAC) by April 6,
2014 deadline send adequate support.4. CMS responds generally in June/July 2013 timeframe.5. Appeal request must be filed within 180 days of publication
of Final Wage Index – expected publication date in August of 2014.
6. Repeat process for subsequent years.
If in doubt – protect appeal rights.Draft letter in workbook.
Note: Hospitals can also file appeal request within 180 days of receipt of
the Notice of Program Reimbursement.
18
MATERIALITY
An adjustment returns approximately 40% of its value to hospitals in each MSA.
Hours adjustments are powerful and frequent.
Pretend you are the only hospital in your MSA (statewide rural area) in considering materiality.
19
HOT TOPICSOCCUPATIONAL MIX SURVEY
New Survey Calendar 2010:Instructions are very similar to 2007-2008 Survey.Will be used for FFY 2013-2015 wage index.
Data is simple looking data:Paid Paid
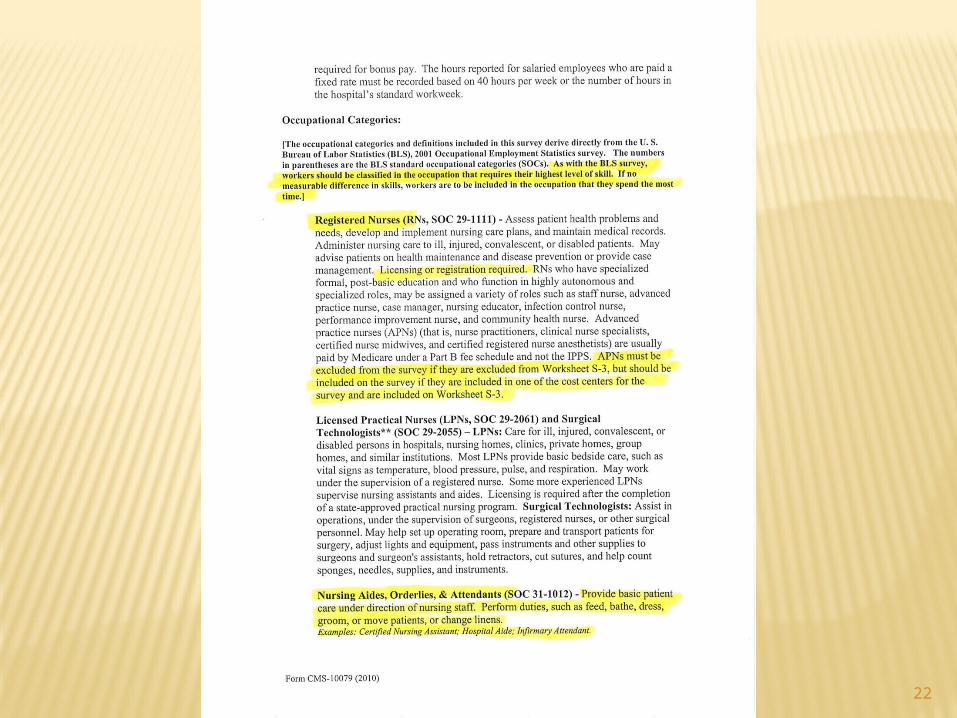
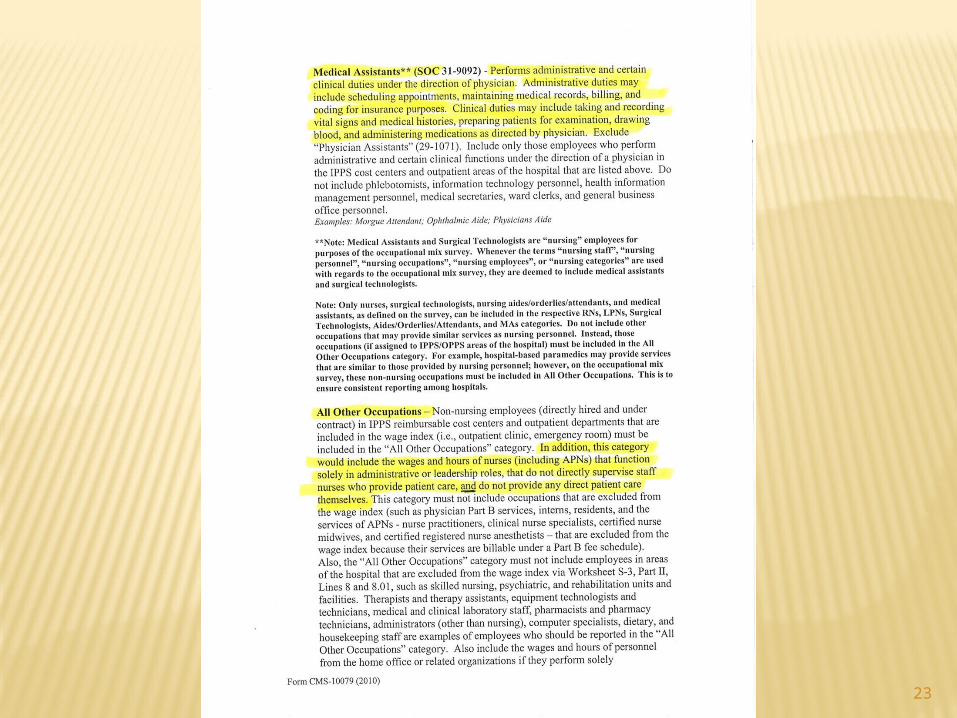
Salaries Hours AHW Nursing occupations
RNsLPNs & Surgical TechnologistsNursing Aides, Orderlies & AttendantsMedical Assistants
Total Nursing All other occupations
Total
TO PROPERLY COMPLETE THIS SURVEY SEEK INPUT FROM NURSING ADMINISTRATION AND--AS APPLICABLE-- OTHER OPERATING PERSONNEL.
CHANGES CAN BE SUBMITTED TO THE MAC BY THE DECEMBER 2012 SCRUBBING DEADLINE.
20
MOMA BASICS
Best to worst line items
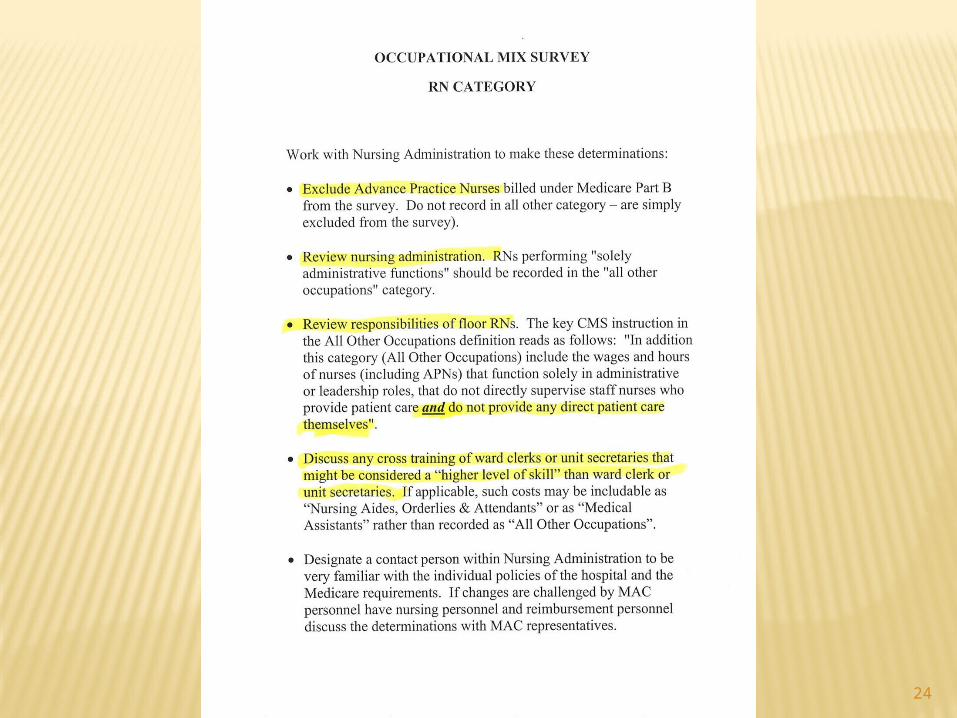
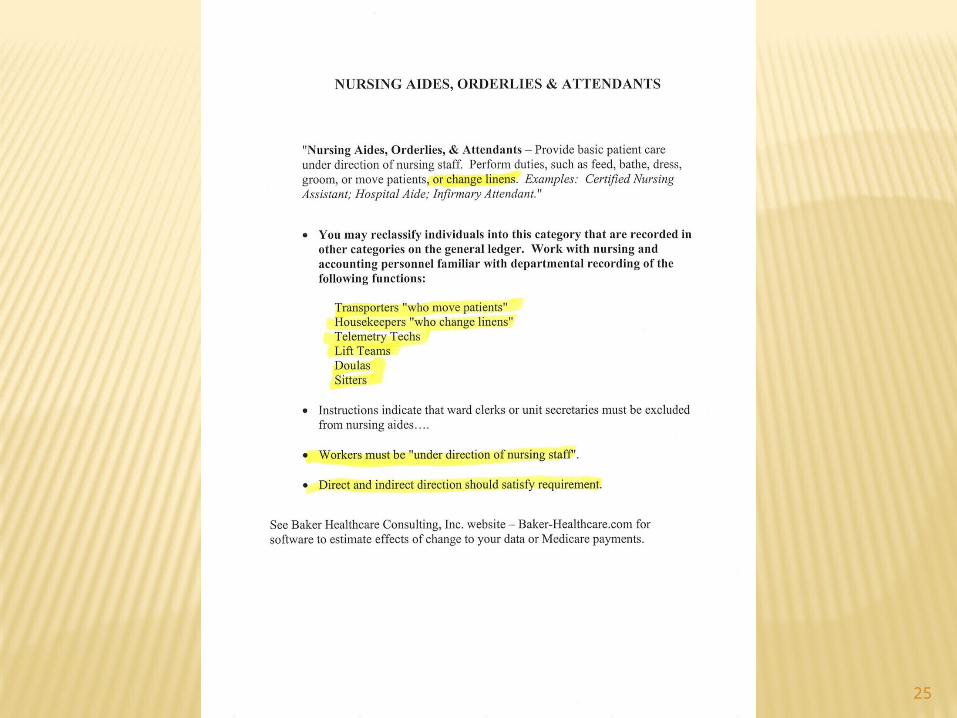
1. Nursing aides, orderlies & assistants2. Medical assistants3. LPNs and surgical technologies4. RNs
“All other” is a neutral but generally desirable
category.
21
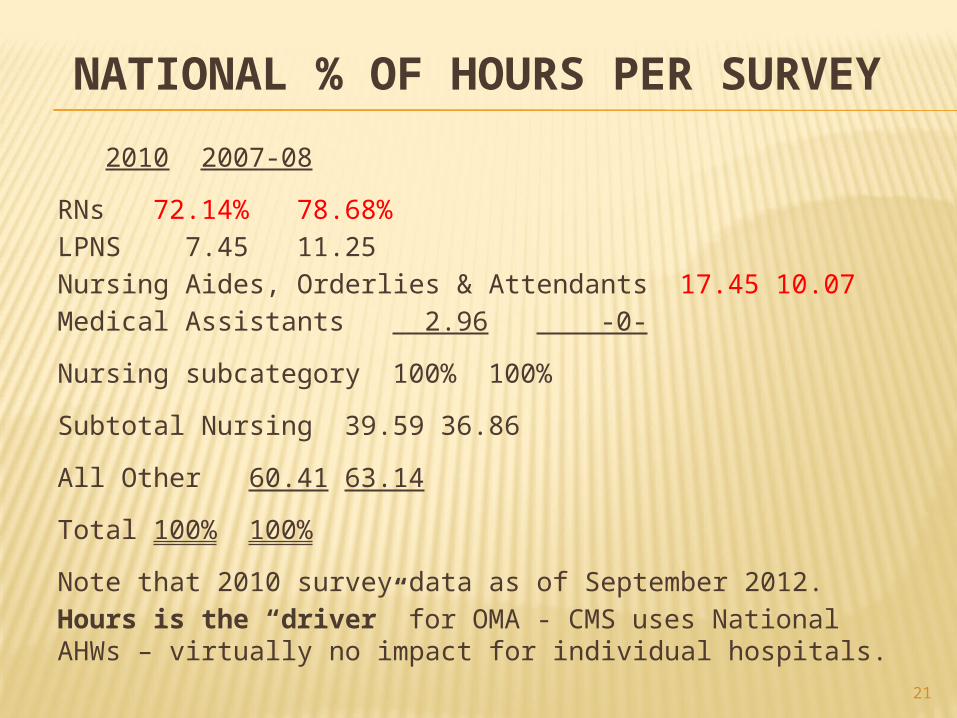
NATIONAL % OF HOURS PER SURVEY
2010 2007-08
RNs 72.14% 78.68%LPNS 7.45 11.25Nursing Aides, Orderlies & Attendants 17.45 10.07Medical Assistants 2.96 -0-
Nursing subcategory 100% 100%
Subtotal Nursing 39.59 36.86
All Other 60.41 63.14
Total 100% 100%
Note that 2010 survey data as of September 2012. Hours is the “driver” for OMA - CMS uses National AHWs – virtually no impact for individual hospitals.
22
23
24
25
26
WHAT IF?
Use the Baker Healthcare Consulting estimator to play “what if games” with your data.
See the Workbook.
BHC website is Baker-healthcare.com
27
OTHER CHANGES
CMS manualizes policy to exclude hours, wage related costs and salaries of capitalized salaries.
Un-accrued PTO hours at year end are to be recognized on the "cash basis" – when paid in the subsequent year.
Some hospitals had excluded these hours in subsequent year.
CMS claims better matching (paid vacation hours of prior year are consistent year to year).
Fully accrued hours should be fine and includable.
But are very rare in hospital systems.
28
HOT TOPICSLEGAL AUDIT & CONSULTING SERVICES
May 2008 CMS releases Revision 18 to PRM formalizing policy.
July 2008 – via private e-mail, CMS clarifies that financial audits are includable.
How much is includable? MACs accepted billing hours and amounts
(generally) right off invoices. Obtaining hours from venders is very important. Equipment, travel, overhead is generally
excluded, but for consulting, audit and legal fees right off invoices have been accepted.
29
HOT TOPICSLEGAL AUDIT & CONSULTING SERVICES
What is included?
“Any contract service included on Worksheet A, line 6, column 2. Contract information service, legal services, tax preparation services, and cost report preparation services are examples of contract labor costs includable on line 22.01”.
30
HOT TOPICSLEGAL AUDIT & CONSULTING SERVICES
CMS also clarified that on line 9 Personnel Costs for Contract Management and Administrative Services include such positions as “Director of Pediatrics, Laboratory Services, Administrator, Blood Bank Manager, Administrative Assistant in the Department of Cardiology, SICU Ward Clerk, and Medical Secretary in the Obstetrics Department.”
CMS has broadly defined A & G contract labor what is includable.
31
WHAT TO DOLEGAL AUDIT & CONSULTING SERVICES
Scour "purchased services" for high hourly amounts that are includable.
How about medical record coding engagements?
Charge Master Review Employment agency fees Executive recruiter fees A/R consulting Outsourced department management (lines
9.03 and/or 22.01
Get creative!!
32
HOT TOPICSLEGAL AUDIT & CONSULTING SERVICES
Now – the dark side:
Revision 20 to the PRM (August 2009) in the instructions to line 22.01 (contract A&G).
"Do not include on line 22.01 any costs for contract labor home office personnel (these costs are not currently included in the wage index".
33
HOT TOPICSLEGAL AUDIT & CONSULTING SERVICES (CONT.)
CMS subsequently allowed these costs under the theory that the instructions have been interpreted to prevent a “double dip” inclusion on both the home office and contract service lines.
Aggressive position has prevailedHours and Rates right off the invoices.
Precedent – Agency NursesNot in accordance with CMS' instructions (for
Agency Nurses or for other)
34
MAC DISTRIBUTED WI DESK REVIEW QUESTIONNAIRE
States termination PTO hours need not be included in line 1.
Membership in fitness clubs paid by hospital is not self insurance (not a WRC)
Asks hospitals to provide documentation that self-funded insurance costs do not exceed costs of commercial policy.
Note: Sub regulatory guidance not necessarily uniform across country.
35
WAGE INDEX APPEALS
I. "Bogus" Hours Issues: Self-funded disability “hours”:
Favorable decision at: District Court level in Rochester, NY CMS settled case Court decision vacated as a condition of settlement.New favorable unanimous PRRB decision received
10/11/11 Baylor Plan hours:
DescriptionStatus of issue in Appelate Court in CincinnatiNew favorable unanimous PRRB decision received
10/11/11 Lunch hour
DescriptionChicago Court of Appeals ruled against hospitals
II. “Shared Culpability” Issues: Michael Reese case settled $7 million at Appellate Court in
Chicago. Santa Cruz, CA MSA now before the PRRB a on similar issue.

36
WAGE INDEX APPEALS
VII. Pension & Post Retirement Benefits Historically since 1994 GAAP OIG audits February 2005 OIG memo to CMS May 2005 August 11, 2005 Federal Register – CMS requires
“funding” to include GAAP costs. Retroactive to periods beginning as early as October
1, 2002 Selective implementations by FI Does solution make sense?
ERISA not GAAP includability? California Case appealed June 14, 2011 Hall Render/BHC cases heard at PRRB on April 10,
2012

37
APPEAL ISSUES PENSION
All 5 Campuses of University of California were adjusted.
Reduces payment by approximately $90 million for FFY 2007 for California.
San Diego, Los Angeles (and reclassified into LA) Orange (reclassified into Orange), San Francisco and Sacramento wage indexes
Hooper Lundy & Bookman is coordinatingDale Baker testified for two hours – inconsistency
throughout the U.S.
BHC working with hospitals perhaps $300 million in controversy (approximately 400 hospitals) 2007-2011 April 10, 2012.
PRRB denied – lacks jurisdiction on to DC District Court.
38
HOT TOPICSRURAL FLOOR BNA APPEALS Background:
Balanced Budget Act of 1997
Budget Neutral Rural Floor for Urban Wage Indexes
CMS implemented in a “budget negative manner”.
Approximately 2,200 hospitals appealed this issue 2007-2011
Favorable settlement April 15, 2012
Another 500 hospitals appealing now.
39
OTHER APPEAL ISSUES
2007 SSI ratios now include "Medicare Advantage Days".
Generally decrease SSI % and DSH payments.Regulation CMS says include MA.Statute says only patients "entitled to Part A
benefits.MA are "eligible" for Part A but not "entitled to".Legal Question: Does entitled to = "eligible for“1498R Ruling being implemented by MACsAlso “Dual Eligible”, “Labor and Delivery Days”, and
“Observation Days”

40
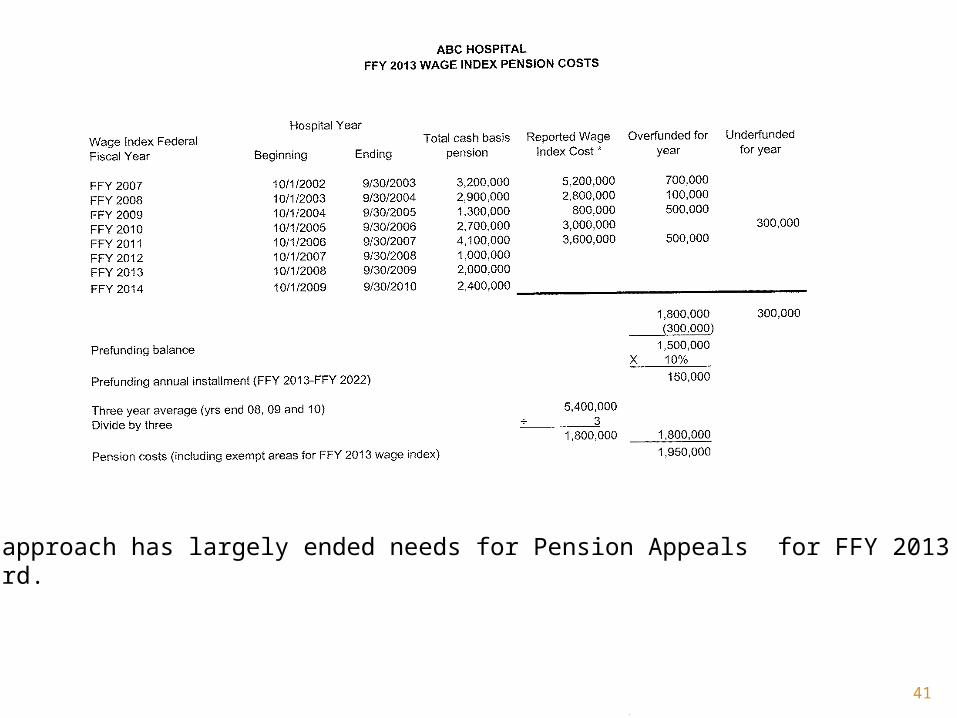
2013 PENSION & POST RETIREMENT BENEFITS
REPORTING NEW RULES:
CMS implemented a three year funding methodology in 2013 that seems reasonable.
We do not contemplate additional pension appeals for 2013 going forward.
41
This approach has largely ended needs for Pension Appeals for FFY 2013 and forward.
42
2015 SPECIAL CONSIDERATIONS
Use of Diagnostic Review Maximizing wage related costs
- Pension audit, legal and consulting- Health insurance – TPA approach- Self-funded health insurance
Allocation of fringes to highly paid physicians and CRNAs
Work plan review
43
WORKBOOK
Focus on workbook

44
QUESTIONS
45
THE FUTURE OF THE WAGE INDEX
46
TAX RELIEF & HEALTH CARE ACT OF 2006
Signed into law December 20, 2006 by
Lame Duck CongressSection 106
Required MedPAC to issue a report by June 30, 2007 including “alternatives the Commission recommends to the method to compute the wage index.
Provides $2 million funding for the study
and
47
TAX RELIEF & HEALTH CARE ACT OF 2006(TRISHA)
Requires the Secretary of HHS to issue for FFY 2009 one or more proposals taking into account the MedPAC report in the IPPS proposed rule due to be published in April 2008. CMS/HHS shall consider:
Problems defining labor markets. Modify/eliminate geographic reclassification. Possibly use BLS data. Minimizing variations between and within MSAs and statewide rural areas. Applying components to other care settings (home health, SNF, etc.) Minimize volatility while maintaining budget neutrality. Regional effects and effects on providers. Implementation phase in. Issues related to occupational mix and effect on quality of care and patient safety.
48
MEDPAC PROPOSED BLS WAGE INDEX, METHODOLOGY
Use Bureau of Labor Statistic data (May & November each year)
Include hospital and non-hospital data: 1.2 million establishments on three year
cycle. By occupation (eliminate need for
Occupational Mix Adjustment (RNs, LPNs, physical therapist, etc))
By county within and outside MSAs Determine wage index for each MSA
(presumably metropolitan division)
49
SMOOTHING WITHIN MSA
High cost county(ies) may be increased up to 105% of MSA average. (Smoothing)
Lower cost counties (generally outlying counties) can be reduced to 95%. (Smoothing)
Maximum “cliff” at county boundary is 10%.
Rural counties (outside Metropolitan Statistical Areas) county by county determination.
10% maximum cliff (smoothing) Eliminate geographic reclassification.

50
WHAT’S WRONG WITH THE MEDPAC PROPOSAL?
Today’s wage index:Mandatory system virtually all IPPS hospitals participate.
Full Year historical hospital data “scrubbed” by hospitals with 100% desk review by FIs (MACs).
MedPAC proposal:Wage indexes subjectively modified by “smoothing”
Cliffs at county boundary could be 8%, 10% or 12%affecting payment by billions of dollars
51
WHAT’S WRONG WITH THE MEDPAC PROPOSAL?
Accuracy Issues
Today’s wage index:
Single data source (S-3) sorted based on Census/OMB designated MSAs (statewide rural areas reconciled to cost reports). Wages, fringes and hours are consistent.
MedPAC proposal:
Sample data (two payroll periods May and November)
Participation by employers is voluntary and confidential.
BLS may secretly impute data for non-responsive employers, CMS would not know.
MedPAC notes that data is not as accurate as current data and that it understates the highest wage indexes (San Francisco Bay Area and NYC, for example).
52
WHAT’S WRONG WITH THE MEDPAC PROPOSAL?
Accuracy Issues (continued) BLS data is reduced to a simple average hourly wage
(excluding fringes). BLS distortion caused by mix of part time/full time employees
(part time x 2,080) What about areas of the county where 7.5 hour workday is
standard rather than 8.0?
Mixing Databases Today’s wage index collects wages, fringes and hours from a
single report, S-3 of cost report. Med PAC proposal – BLS data excludes fringe benefits.
MedPAC “grafted” hospital only fringe benefit data (which ranges up to 47% of salaries) in computing county by county wage indexes.
53
WHAT’S WRONG WITH THE MEDPAC PROPOSAL?
Transparency
Today’s wage index – detailed S-3 data published in Public Use Files in October, February and May. Available earlier on cost report publicly available data. A “final file” is published after release of the Final IPPS rule. Data is very transparent.
MedPAC proposal – Voluntary confidential data no transparency to CMS or the public
Imputed data is secret.
54
LACK OF COMPARABILITY
MedPAC proposal:
Includes CAHs with low wages (distortion of rural wage indexes in counties with both IPPS and CAH hospitals).
BLS does not pick up salaried physician Part A services.
BLS does not pick up contract physician Part A services (required by law in California and possibly Texas).
BLS pick up agency nursing and other contract services in the county where the agency is located rather than the hospital county.
Agency nurses amount paid to nurses, not amounts paid per hour worked by the hospital.
55
ACUMEN, LLCAWARDED A TASK ORDER
Where? Burlingame California (SFO Airport)
Who? Stanford University "Scholars"
Management Team: Thomas MaCurdy – Professor of Economics
Margaret (Peggy) O'Brien-Starn – Gardner Center of Stanford
Jonathan Wilwerding – Research Fellow at
Stanford Institute for Economic PolicyResearch
ACUMEN, LLC
Acumen's Final Findings – We need to study more.Revision of Medicare Wage Index.Final Report: Part II, March 16th, 2010
Acumen recommends further exploration of labor market definitions using a wage area framework based on hospital-specific characteristics, such as the commuting times from hospitals to population centers, to construct a more accurate hospital wage index….
However, it would be naïve on our part to believe that all hospitals would eagerly embrace a wage index that significantly improves the accuracy of the wage index. … Certain hospitals, especially rural hospitals, benefit more from the existing reclassifications and exceptions than they would if their wage index values were more accurate.
Most importantly, Acumen did not endorse MedPAC/BLS wage index proposal.
56

57
INDUSTRY SUPPORT FOR MEDPAC PROPOSAL
Opposed by AHA
Opposed by FAH
Opposed by most state and regional associations.
AFFORDABLE CARE ACTPublic Law 111-148
Enacted March 23, 2010
By December 31, 2011, the Secretary of HHS shall submit to Congress a plan to reform the Medicare Hospital Wage Index System including the goals set forth in the June 2007 MedPAC Report that: Use Bureau of Labor Statistics (BLS) data or other data or methodologies.
This was drafted in 2009, before Acumen released their final report 3/16/20. BLS could be outdated.
Minimize wage index adjustments between and within metropolitan statistical areas and statewide rural areas.
58

AFFORDABLE CARE ACT
Minimize volatility, on a budget neutral basis.
Consider implementation and redistribution of payment issues.
Address occupational mix and consider patient quality and safety.
Provide a transition.
59
PROVISIONS IN ACA
Renewal of Section 508 reclassifications for FFY 2010
Eliminates state by state rural floor budget neutrality
Reinstates historical thresholds for geographic reclassification – rural and RRC 82% of target, urban (non-RRC) 84%, countywide 85%, which could sunset for FY 2014 or 2015.
Includes provisions to study certain post acute wage indexes.
60
61
ACUMEN REPORT, APRIL 2011 MAJOR PROVISIONS
Replace Metropolitan Statistical Areas as “building blocks” for wage index with zip codes or Census Tracts.
Determine an Average Hourly Wage (AHW) for each zip code.
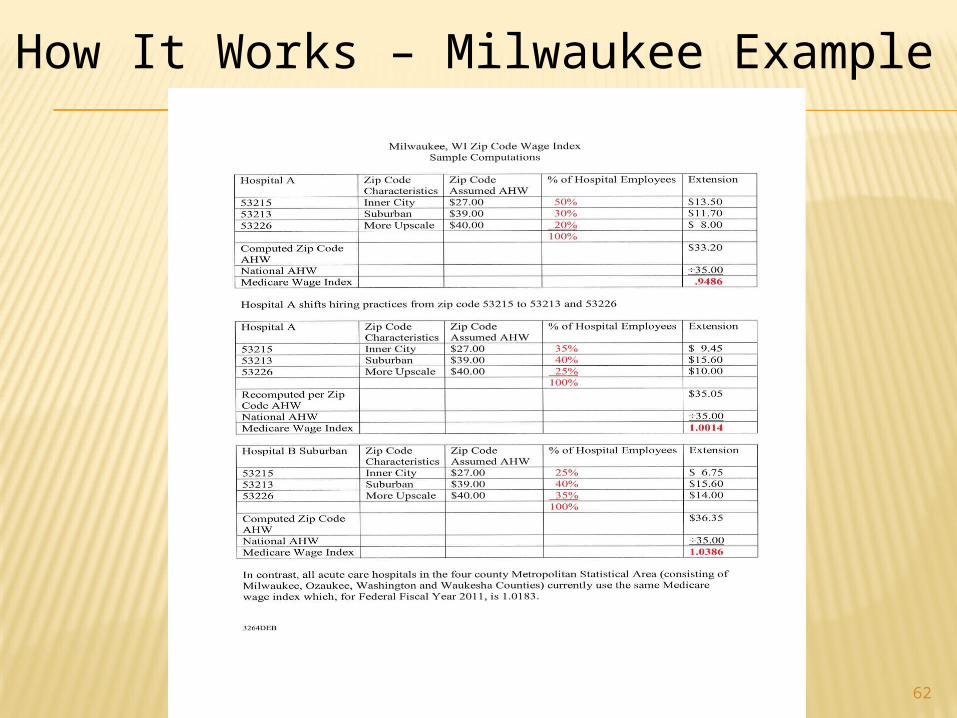
Identify hospital employees by zip code multiply by % of hospital employees in each zip code and “build” a hospital specific wage index.
Use either old Census data or massive hospital database to determine zip code.
Probably do away with geographic reclassification.
62
How It Works – Milwaukee Example
63
IMPLICATIONS
Punishes inner city hospitals (safety net hospitals) that can not cost shift to other payors.
Punish large rural hospitals (referral centers) in many areas “the backbone” of the rural health system.
Provide disincentive to hire workers in the inner city, when unemployment and the need for jobs is greatest.
DOA per former CMS official Institute of Medicine did not even
acknowledge Acumen Proposal in their June 1, 2011 report.

64
INSTITUTE OF MEDICINE (IOM)
Non-profit think tank (academics from all over USA).
Engaged by CMS in August 2010 No direct linkage to Congress Paid by CMS Public meetings: September 2010,
January 2011, June 1, 2011, July 17, 2012
65
JUNE 1, 2011 PRESS CONFERENCE & RELEASE OF PRELIMINARY REPORT
Continue using MSAs as building blocks (perhaps breakdown statewide rural)
Eliminate geographic reclassification Use Bureau of Labor Statistics Data Increase Transparency (between government
agencies) Silent as to transparency with the public Make border adjustments based on
commuting patterns between neighboring wage index areas.
No discussion of two way commuting patterns
66
WHAT’S NEXT?
All meetings have been completed IOM tentative recommendations are
the final IOM recommendations IOM Webinars scheduled for October
10th and 17th, 2012 One additional webinar to be
scheduled on telemedicine

67
68
2011 MA CONTROVERSY 2012 WI
Nantucket Cottage Hospital – 19 Beds Formerly a Critical Access Hospital Affiliated with a major health care system, returned to IPPS
hospital Establishes a rural floor in Mass for FY 2012 of 1.3452
compared to Boston wage index of 1.2263 for FY 2011. Every hospital in Mass gets rural floor based solely on
Nantucket. AHA and others express concern Reduces wage indexes by .62% outside of Massachusetts. Hospital Coalition, of approximately 20 hospital associations,
asks President to “fix” Massachusetts Rural Floor issue. Hospital coalition estimates $367 million budget neutral shift to
Massachusetts from other states. CMS has taken no action in FFY 2013 Final Rule
69
POSSIBLE FUTURE ACTIONS
In the July 18, 2011 Outpatient Proposed PPS Rule:
CMS expresses concern over manipulation of Rural Floor CMS notes that urban hospitals can request rural status --
under current policies the rural wage index (the floor) can increase.
Options to CMS: Do not apply Rural Floor to OPPS when it is set by small
number of hospitals and benefits the whole stateor
State by state budget neutralityor
Something else Also CMS contemplates only truly rural hospitals in computing
the rural wage index (floor). CMS did not finalize these proposals.
70
URBAN HOSPITALS RECLASSIFYING TO RURAL STATUS
Regulation 42 CFR 412.103:Urban hospitals can become rural if they meet the requirements to be either a Sole Community Hospital (SCH) or a Rural Referral Center (RRC) if they were in a rural area.
At least 5,000 discharges (3,000 in certain osteopathic hospitals)
Case Mix Index equal to a greater than CMS Regional Average Non-Teaching Case Mix (published in F.R.).
At least 50% of medical staff is Board eligible or Board certified.

71
URBAN HOSPITALS RECLASSIFYING TO RURAL STATUS
Present Policy:
If urban hospital AHW is higher than Rural AHW it is added into the rural data before computing a wage index.
72
SO BHC TESTED POSSIBLE IMPACTS AS FOLLOWS:
Our data guy (Jack) selected two large urban hospitals in several states that likely meet all criteria for RRC status.
He did not disclose which hospitals he chose.
He recomputed the FFY 2012 Rural Floor wage index including the two large hospitals in each state.
73
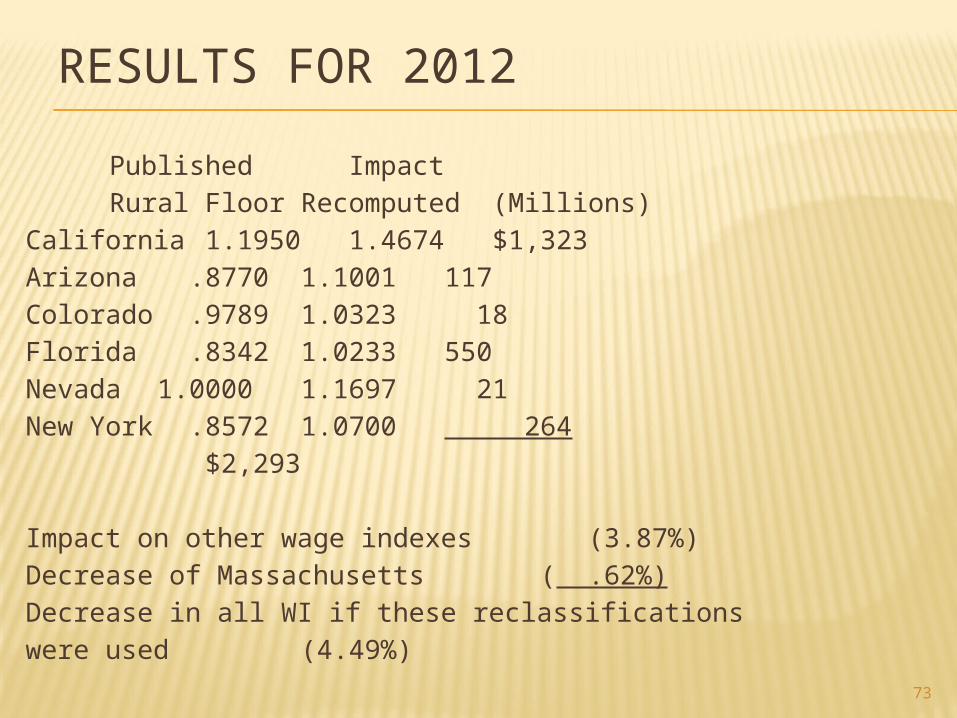
RESULTS FOR 2012
Published ImpactRural Floor Recomputed (Millions)
California 1.19501.4674$1,323 Arizona .87701.1001117Colorado .97891.0323 18Florida .83421.0233550Nevada 1.00001.1697 21New York .85721.0700 264
$2,293
Impact on other wage indexes (3.87%)Decrease of Massachusetts ( .62%)Decrease in all WI if these reclassifications were used (4.49%)
74
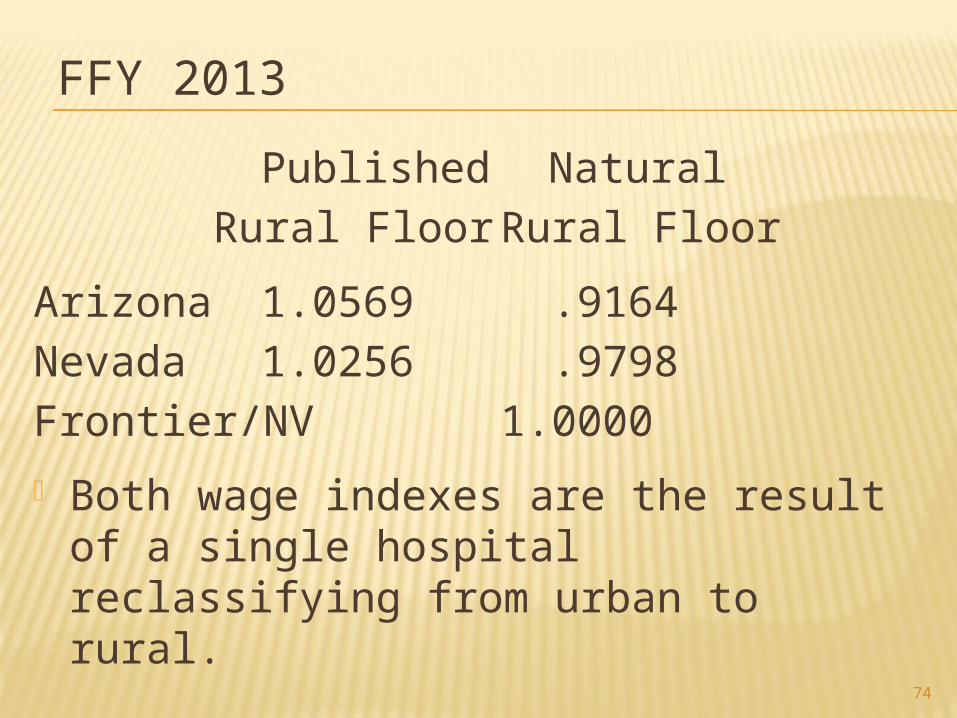
FFY 2013
Published NaturalRural Floor Rural Floor
Arizona 1.0569 .9164Nevada 1.0256 .9798Frontier/NV 1.0000
Both wage indexes are the result of a single hospital reclassifying from urban to rural.

75
CONCLUSION
CMSHAS NOT ACTED TO
AVOID THIS TRAIN WRECK
76
IOM STILL USES BUREAU OF LABOR STATISTICS DATA Area wide data lumps physician office practice RNs with hospital
RNs & Advance Practice Nurses. An RN is a RN is a RN! Assumption we make is that hospital RNs are paid substantially
more per hour and have higher fringe benefits than “office practice” RNs.
24/7 nursing care California Nurses Association (National Nurses United)
One primary goal of the ACA (and whatever form that future healthcare reform takes) is to reduce costs.
To do so means changing the site of care to reduce costs whenever it is appropriate.
If BLS data is statistically sound as the site of care changes, more lower paid office practice RNs will be included in a computed wage index.
Perverse incentive – Penalize hospitals with a lower wage index for shifting the site of care and RNs from hospital to office practice.

77
IOM PROPOSAL HAS ANTI-WESTERN STATE BIAS
Patient Days National Avg. % StatePer Thousand Patient Days Less ThanPopulation Per Thousand National
Alaska 483.8 613.5 21%Arizona 483.3 613.5 23%California 468.1 613.5 24%Colorado 438.6 613.5 29%Idaho 403.2 613.5 34%Nevada 488.5 613.5 30%New Mexico 408.8 613.5 32%New Hampshire 471.8 613.5 34%Oregon 359.8 613.5 41%Utah 346.2 613.5 44%Vermont 490.5 613.5 20%Washington 391.2 613.5 36%Per 2012 Edition AHA Hospital StatisticsIf BLS data is statistically accurate a BLS wage index would be substantially biased against the Western states, that incur fewest patient days per thousand population.Based on the 2012 Occupational Mix Adjustments 37% of all hospital salaries (nationally) are for services of RNs.
78
WHAT’S NEXT?
AHA Medicare Area Wage Index Task Force: 19 members 4 health system CEOs 2 hospital CEOs 10 hospital association CEOs
Final recommendations due in October AHA – Regional Policy Boards will act on
Task Force Recommendations late 2012.
Per CMS, final recommendations in early 2013.
79
2012 LAME DUCK SESSION
AHA annual meeting, May 2012: Trent Lott, former Republican Senate
Majority Leader predicted: If Obama is re-elected and if Senate
stays Democratic a wild lame duck session, including tax, health care, and other issues that Congress has been unable to agree upon all legislated in December 2012
2% Sequestration possibly repealed??
A COMPREHENSIVE MEDICARE WI REFORM (CMWI) PROPOSAL COMPILED BY BHC
GOALS: Continue the existing wage
index/geographic reclassification process but modify them to meet Congressional and Industry needs.
Focus on acute care hospitals. Also modify post acute care PPS
80

A PROPOSED COMPREHENSIVE MEDICARE WI REFORM (CMWI)
GOALS FOR CMWI PROPOSAL: Develop a CMWI proposal that includes:
Changes in LawChanges in RegulationsChanges in PolicyChanges in the manner in which wage index decision making is made.
Goal – make the changes very cost effective
Continue today’s transparent system Minimize redistributive effect. 81
A PROPOSED COMPREHENSIVE MEDICARE WI REFORM (CMWI)
Consists of:Legislative proposalsAdministrative fixes
Congress needs to pass legislation Members of Congress could sign a
letter to Secretary Sebelius requesting:Administrative fixes (not requiring legislation)
82

83
WHAT DOES THIS COMPREHENSIVE PROPOSAL DO?
Reduces volatility by using a two year “rolling” wage index (50/50).
Clears out the Halls of Congress – puts in a “stop loss” for wage index decreases of over 1% of total Medicare payment (1.5% of wage index).
Modernizes payment for Post Acute Care improving comparability to local acute care wage indexes actually paid.
Provides a new money fix for low wage index areas of the country while maintaining current incentives to “scrub data”.
Recompute outmigration adjustment annually, it is wrong two of every three years since it is only computed once every three years.
Make regulatory “mini fixes’ to eliminate obvious inequities.
TWO YEAR WI PROPOSAL (1) Use two years data to reduce volatility of
annual wage index changes. ½ year FFY 2011 ½ year FFY 2012 for example Legislative.
Budget neutral over two year period. Reduces volatility by 50%. Can be implemented immediately. Data
would be accumulated under the current system from the S-3, Part II. Cost of implementation zero. No new data required.
Change cutoff dates from FFY to calendar year data to improve the timeliness of data.
84
TWO YEAR ROLLING WAGE INDEX
This reduces volatility by 50%. Results in identical payments to each wage
index area over a two year period (i.e. no redistributive effect).
Calculations would be based on current year configuration of wage index areas (urban and rural) using ½ year data from prior year.
Reclassified wage indexes would be based on current year reclassifications so as not to distort wage indexes because of changes in reclassification (or wage index areas from census changes).
85
.015 ANNUAL STOP LOSS FLOOR (2)
Implement a hospital specific 1½% annual stop loss floor, eliminating catastrophic decreases in wage indexes.
86
.015 ANNUAL STOP LOSS FLOOR
Redistributive effect for FFY 2010 is $57 million (.0005 of IPPS payments).
FFY 2009 was approximately $35 million.
Conclusion:The impact is very minor and redistributive effect is de minims.
87

POST ACUTE PARITY (3)
Modernize post acute care geographic payment parity by applying actual average IPPS wage indexes in each geographic area throughout the country.
88
POST ACUTE CARE PAYMENT EQUITY (PAPE)
CMS, using existing data computes the average wage index actually paid within each CBSA or statewide rural area. Based on most recent CMS data on number of discharges, case mix index using the actual wage indexes (reclassified, unreclassified or rural floor) by each hospital in a geographic area.
There is some redistribution. Could be one time budget neutral
adjustment. Needed for bundling of payment under
health reform. 89
9090
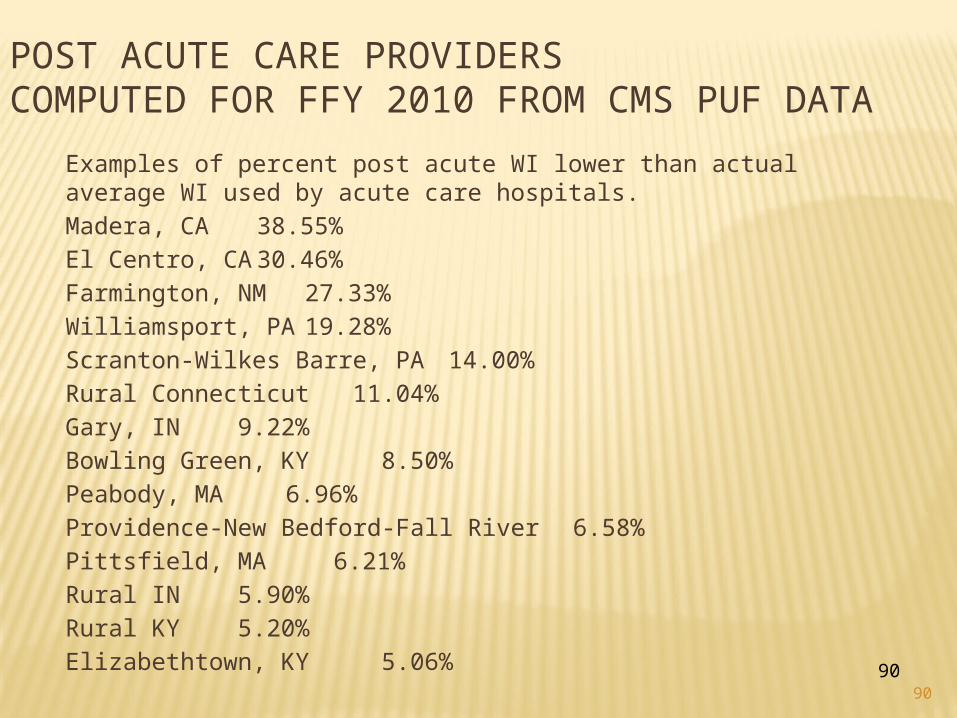
POST ACUTE CARE PROVIDERSCOMPUTED FOR FFY 2010 FROM CMS PUF DATA
Examples of percent post acute WI lower than actual average WI used by acute care hospitals.Madera, CA 38.55%El Centro, CA 30.46%Farmington, NM27.33%Williamsport, PA 19.28%Scranton-Wilkes Barre, PA 14.00%Rural Connecticut 11.04%Gary, IN 9.22%Bowling Green, KY 8.50%Peabody, MA 6.96%Providence-New Bedford-Fall River 6.58%Pittsfield, MA 6.21%Rural IN 5.90%Rural KY 5.20%Elizabethtown, KY 5.06%
GEO ADJUSTMENT FACTOR FOR WAGE INDEXES LESS THAN 1.000 (4)
Implement a new money methodology to increase all wage indexes under 1.0000, preserving incentives to "scrub" data (legislative).
91
GEO ADJUSTMENT FACTOR FOR WAGE INDEXES LESS THAN 1.000
MedPAC report criticized current wage index system because of "circularity".
The rich get richer – they $eldom complain.
The poor get poorer – they always complain
$olution – Congress can create a new money fix for hospitals with wage indexes lower than 1.0000.
Let the rich get richer.92
GEO ADJUSTMENT FACTOR FOR WAGE INDEXES LESS THAN 1.000
CMS implements using a GAF methodology which would include the following.
Lowest wage indexes increase the most. As wage indexes get closer to 1.0000 the amount of the increase decreases.
This maintains all hospitals in the same rank and order as current wages and preserves the incentive to "scrub" wage index data. This is essential!
93
GEO ADJUSTMENT FACTOR FOR WAGE INDEXES LESS THAN 1.000
Alternatives such as a “floor” (of 1.0000 for example) changes wage index incentives and can result in the opposite from what is intended.
Frontier states (MT, NV, WY, ND & SD) given wage indexes of minimum of 1.0000 in the ACA.
Approx $500 million annually would raise all low indexes appropriately (Congress’s call).
Phase in? Modification possible for “low cost counties”
and other Congressionally mandated adjustments.
94
OUTMIGRATION ADJUSTMENT (5)
Recompute the outmigration adjustment annually rather than every third year (legislative).
95
OUR CMWI PROPOSALS
Originally we proposed to eliminate occupational mix but we dropped this provision as too re-distributional.
Moves monies from East Coast and Midwest to California (with mandated minimum staffing ratios).
Even our California clients realize the level of opposition to eliminating the OMA.
96
ADMINISTRATIVE FIXES
Letter to Secretary Sebelius signed by Members of Congress requesting:1. Allow hospitals to file for repetitive
reclassification annually rather than once every three years.
2. Allow two campus hospitals in different counties to each participate in countywide reclassification to different targets.
3. All hospitals in an MSA should have the same wage index (statewide rural floor distorts this basic principle in MSAs that are low wage areas in more than one state).
97
ADMINISTRATIVE FIXES4. Allow a hospital to reclassify to a “higher
wage” MSA based on the most recent single years data rather than only based on three year data.
5. Include pension costs in wage index based on GAAP – not ERISA funded amounts.
6. CMS should give six years prospective notice in changes in 82%, 84%, 85%, 106% & 108% (Same as age of data used in reclassification criteria).
7. Reinstitute an industry Medicare Technical Advisory Group(M-TAC) for wage index issues.
98

ADMINISTRATIVE FIXES
8. Longstanding urban RRCs should have the same proximity requirements as rural RRCs.
9. Measure proximity to nearest MSA county line with an IPPS hospital in it (affects one hospital in Bemiji, Minnesota).
10.New provider in a county should receive countywide reclassification when opened – currently there is up to a three year wait.
11. Take steps to improve consistency between the MACs and FIs in implementing wage index adjustments.
12. Eliminate bizarre interpretations that urban RRCs must obtain rural status every third year to reclass to a wage index area over 15 miles away99
100
QUESTIONS?