medical management and assessment of respiratory system in ... · respiratory physiology summary...
TRANSCRIPT

Medical management and Medical management and assessment of respiratory system assessment of respiratory system
in neuromuscular diseasein neuromuscular disease
A Respiratory physiology perspective
Andrew MorleyAndrew Morley (BSc Hons, RPSGT),(BSc Hons, RPSGT),
Manager of the Respiratory Physiological services,Manager of the Respiratory Physiological services,
Royal Hospital for Children, Glasgow.Royal Hospital for Children, Glasgow.
Respiratory PhysiologyRespiratory Physiology
PlanPlan•• Why do Lung Function? Why do Lung Function?
•• When to ask for a sleep study ?When to ask for a sleep study ?
•• Which sleep study to ask for ?Which sleep study to ask for ?
•• Positive pressure therapiesPositive pressure therapies
Respiratory PhysiologyRespiratory Physiology

• Inspiratory vital capcity <60% - Predicts sleep disordered breathing
• Inspiratory Vital capacity <40% - predicts Nocturnal hypoventilation
Respiratory PhysiologyRespiratory Physiology
Pulmonary function tests
• MIP & MEP
– (PIPS & PEPS)
• Spirometry
• Lung Volumes
Respiratory PhysiologyRespiratory Physiology
Pulmonary function tests
• MIP & MEP
– (PIPS & PEPS)
• Spirometry
• Lung Volumes
maximum inspiratory pressure (MIP) maximum
expiratory pressure (MEP) measures the strength
of the muscles that are used during normal & forced
breathing in & out
Measuring how much air you can breathe out in one
forced breath.
Measures the volume of air in the lungs, including
the air that remains at the end of a normal breath.
May also include diffusing capacity test this
measures how easily oxygen enters the
bloodstream.
https://www.whatwhychildreninhospital.org.uk/breathing-test
Respiratory PhysiologyRespiratory Physiology

VC / FVC
(Forced) vital
capacity
TV – Tidal Volume
IC
Inspiratory
Capacity
ERV
Expiratory Reserve Volume
RV
Residual volume
TLC
Total Lung capacity
FRC
Functional Residual Capacity
Respiratory PhysiologyRespiratory Physiology
TLC – normal RV - normal
Flow - normal
Normal
Respiratory PhysiologyRespiratory Physiology
TLC – reduced = restriction RV - normal
Flow - > normal
Restriction
Respiratory PhysiologyRespiratory Physiology

• Inspiratory vital capcity
<60% - Predicts sleep
disordered breathing
Respiratory PhysiologyRespiratory Physiology
What is Sleep Disordered Breathing?
“Sleep-disordered breathing is an umbrella term for several chronic conditions in which partial or complete cessation of breathing occurs
many times throughout the night”
• This could be as a result of Obstructive or Central events
Respiratory PhysiologyRespiratory Physiology
How do you assess for Sleep Disordered Breathing?
Respiratory PhysiologyRespiratory Physiology

Sleep Basics
Respiratory PhysiologyRespiratory Physiology
Sleep Basics
•• Sleep stages (REM & NREM)Sleep stages (REM & NREM)
•• Stage N1Stage N1
•• Stage N2: Light sleepStage N2: Light sleep
•• Stage N3: Deep sleepStage N3: Deep sleep
•• REM Rapid eye movementREM Rapid eye movement
Respiratory PhysiologyRespiratory Physiology
Ventilation
REM:
Respiratory PhysiologyRespiratory Physiology
•Muscle atonia
•Breathing more variable, erratic patterns, similar to wakefulness
• Intercostal muscles show virtually no respiratory activity
• Increased abdominal (diaphragm) contribution to ventilation
• � � ventilation
NREM:
• Regular breathing pattern (automatic control)• � ventilation

“I need a sleep study?”
“I need a sleep study?”
• Overnight Oximetry
• Overnight Oximetry & Transcutaneous CO2
• Cardio respiratory study (CRSS or Polygraphy)
• Polysomnogrpahy (PSG)
Respiratory PhysiologyRespiratory Physiology
“I need a sleep study?”
• Overnight Oximetry
• Overnight Oximetry & Transcutaneous CO2
• Cardio respiratory study (CRSS or Polygraphy)
• Polysomnogrpahy (PSG)
Respiratory PhysiologyRespiratory Physiology

What is pulse oximetry ?
Respiratory PhysiologyRespiratory Physiology
What does Oximetry tell you?
• Oxygen Saturatione.g. Normoxic, Hypoxic,
Supplementary oxygen requirement
3 channels !!!
• Heart rate
• Plethsmography signal
Respiratory PhysiologyRespiratory Physiology
What does Oximetry tell you?
• Oxygen Saturatione.g. Normoxic, Hypoxic,
Supplementary oxygen requirement
3 channels !!!
• Heart rate
• Plethsmography signal
Respiratory PhysiologyRespiratory Physiology

Advantages
• Oximetry provides a Non-invasive marker
• Cheap
• Inpatient or Outpatient - limited supervision
• Easy to administer
• Provides continuous monitoring &
recording of blood oxygenation
• Provides desaturation index ( DI/hr)
• Pre and Post Tx studies – e.g O2, NPA
• Good sensitivity for severe OSA
Respiratory PhysiologyRespiratory Physiology
LTOT : assessment
Respiratory PhysiologyRespiratory Physiology
Clinical question : Can the patient come off Oxygen ?
Air 0.25 L O2 / Min
Respiratory PhysiologyRespiratory Physiology
NPA Out
NPA in situ
Heart rate
NPA OutNPA in situ
Clinical question : Is the NPA working?
- Heart baseline increases, increased WOB?

•• AASM: AASM: Oximetry lacks the specificity and sensitivityOximetry lacks the specificity and sensitivity to be used as anto be used as analternative to PSG or an attended respiratory (type 3) study foralternative to PSG or an attended respiratory (type 3) study for diagnosingdiagnosingsleep related breathing disorders sleep related breathing disorders ((www.aasmnet.org/PracticeParameterswww.aasmnet.org/PracticeParameters))
Limitations
Respiratory PhysiologyRespiratory Physiology
Transcutaneous CO2 monitoringTranscutaneous CO2 monitoring
Respiratory PhysiologyRespiratory Physiology
Why measure Transcutaneous CO2?
• Assess ventilation- Hypercapnic
- Hypocapnic
• Assess stage of condition- Daytime CO2
• Assess effectiveness of ventilator
settings (vent check)
Respiratory PhysiologyRespiratory Physiology

Cardiorespiratory Sleep study
(CRSS / Polygraphy)
http://www.ankitparakh.com/
What is a CRSS?
• Multi channel sleep investigation
• Records breathing patterns and any associated oxygen desaturations
• Provides measurements such as- AHI – Obstruction or central
- DI – Desaturation index
- CO2 trends
Respiratory PhysiologyRespiratory Physiology
Limited PSG:
Cardiorespiratory
Sleep study (CRSS)
Setup– Airflow – (Hypopneas)
– Thermistor – (Apnoeas)
– Respiratory Effort (Tho & Abd)– ECG
– Leg EMG– Snore
– Pulse oximetry
– Video– CO2 (ETCO2 or TransCO2)
Somnomedics
Optional
Respiratory PhysiologyRespiratory Physiology

Respiratory PhysiologyRespiratory Physiology
Respiratory PhysiologyRespiratory Physiology
Obstructive apnoea
• ≥90% reduction in airflow for 2 missed breaths during
baseline breathing
• continued or � respiratory effort
Central Apnoea
Respiratory PhysiologyRespiratory Physiology
• ≥90% reduction in airflow for 2 missed
breaths during baseline breathing
• No respiratory effort/movement

•• DMD patientDMD patient
Duchenne Muscular Dystrophy patient.
Respiratory PhysiologyRespiratory Physiology
• CPAP
• NIV / Bilevel
Picture taken from Resmed website
Respiratory PhysiologyRespiratory Physiology
Continuous Positive Airways Pressure (CPAP)
CPAP can be used to :-
• Splint airways the upper airway opene.g. OSA, Anatomy, Post extubation stridor
• Splint small airways e.g. Bronchiolitis, Asthma- where airways
collapse on expiration
• Improve Lung compliance
• Recruit small airways & alveoli
Sullivan CE. Lancet 1981; 1(8225):862-5
Respiratory PhysiologyRespiratory Physiology

• DMD patient� VT � VT x rate = �MV
Respiratory PhysiologyRespiratory Physiology
Bilevel or BiPAP
Two pressures – Inspiratory (IPAP) & Expiratory (EPAP)
• Bilevel therapy is used when the problem is not just obstructive in origin.
• Bilevel therapy is needed when there are
- Central Apnoeas
- Hypoventilation
- Carbon dioxide retention
- Overlap syndrome : Downs syndrome (Obstructive & Central Apnoeas)
Respiratory PhysiologyRespiratory Physiology
• DMD corrected overnight oxygen saturation tracings
� VT � VT x rate = �MV
�VT �VT x rate = � MV
Respiratory PhysiologyRespiratory Physiology

Initiating NIV can be difficult
Respiratory PhysiologyRespiratory Physiology
Initiating NIV can be difficult
• Patients do not always find this an easy therapy to use.
“It was like an endurance test every night”
• Medical/Health care professionals often underestimate patient concerns.
• Patient / Parent can be very anxious
(NIV is often associated with milestones in a condition)
Respiratory PhysiologyRespiratory Physiology
Sensation:
“CPAP is like trying to breath while having
your head stuck out the car window”
Respiratory PhysiologyRespiratory Physiology
• Uncomfortable
• Claustrophobic
• Communication - Talking difficult
Physical:-
• Growth defects
Respiratory PhysiologyRespiratory Physiology
Physical:-
• Pressure Sores
Respiratory PhysiologyRespiratory Physiology
Respiratory PhysiologyRespiratory Physiology
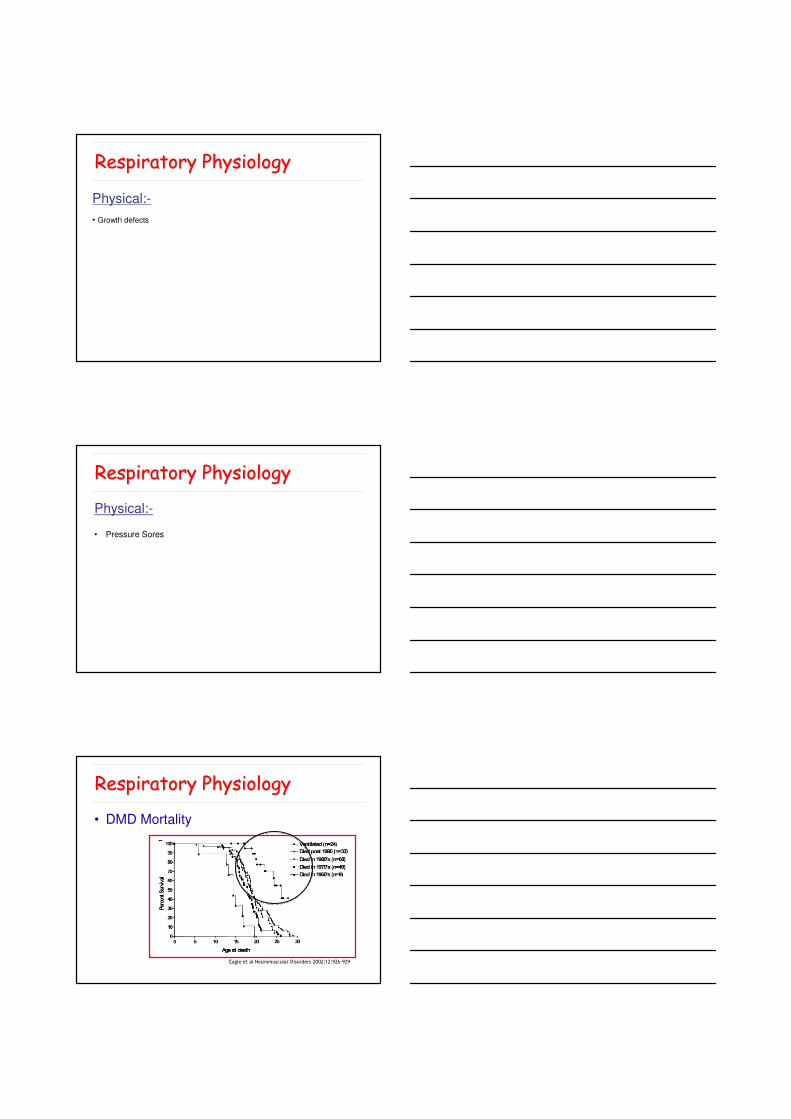
• DMD Mortality
Eagle et al Neuromuscular Disorders 2002;12:926-929

• Never be too pleased with yourself
Respiratory PhysiologyRespiratory Physiology
Case Study
•15 year old Prader-Willi Syndrome
• SBD? , Snores, Tiredness
• CRSS
CRSS
• AHI = 20.7/hr
(Central Apnoeas =18.1/hr)
• Desat. Index = 21.3/hr
NIV establishment(Inpatient admission – 3 nights)
Respiratory PhysiologyRespiratory Physiology
SUMMARY
Respiratory physiology have an important role to play in the
assessment and management of Neuromuscular patients.
NIV therapy is a very successful treatment, however the
level of skill, time & effort required to make this an effective
treatment should not be underestimated.
