medical errors - flagler hospitalphysicians.flaglerhospital.org/documents/cme/medical-errors... ·...
TRANSCRIPT
MEDICAL ERRORS
2
Medical Errors Prevention Release Date: December 16, 2015
Expiration Date: December 15, 2017
Target Audience: Physicians, physicians’ assistants, and advanced registered nurse practitioners
Commercial Support: None
Faculty Financial Interest: None
Investigational Products/Products Not For Use To Be Mentioned In Presentation: None
CME Committee Planners’ relevant financial interest: None
3
Faculty
Michael DiBella, MD
Chief Medical Officer
Flagler Hospital, Inc.
Medical Degree: New Jersey College of Medicine
Contact Number: 904-819-4326
E-mail: [email protected]
Objectives
At the conclusion of this activity, participants will be able to understand and discuss: 1. Root cause analysis, error reduction and prevention and patient safety. 2. The Florida Board of Medicine’s five most misdiagnosed conditions: cancer related issues; neurological related issues; cardiac related issues; timely responding to complications during surgery and post-operatively; urological issues. 3. The Florida Board of Osteopathic Medicine’s commonly misdiagnosed conditions and diversion: inappropriate prescribing of opioids in patients in whom there have been misdiagnosis or failure to diagnose addiction, psychiatric conditions and diversion; failure or delay in diagnosing cancer; retained foreign objects in surgery and wrong site/patient surgery; surgical complications/errors and pre-operative evaluations; prescribing, dispensing, administering, or using non-FDA approved medications and devices.
5
How To Obtain AMA – PRA Category 1
Credit
• Read the power point presentation and be familiar with Flagler Hospital’s Medical Error Policies & Procedures. Estimated time of completion is 2 hours.
• Complete CME test and evaluation form through SurveyMonkey link: https://www.surveymonkey.com/r/MedErrorPrev.
• A passing test grade of 80% along with completed evaluation must be received before CME credits can be reported to CE Broker and certificate sent via e-mail or inter-office mail.
6
Accreditation/Credit Statement
Flagler Hospital is accredited by the Florida
Medical Association to provide continuing
medical education for physicians.
Flagler Hospital designates this educational
activity for maximum of two (2) AMA PRA
Category 1 Credit(s)™. Physicians should
claim only the credit commensurate with
the extent of their participation in the
activity.
7
Disclaimer
This information is provided for general medical education purposes only and is not meant to substitute for the independent medical judgment of a physician relative to diagnostic and treatment options of a specific patient’s medical condition. The viewpoints expressed in this CME activity are those of the authors/faculty. They do not represent an endorsement by Flagler Hospital. In no event will Flagler Hospital be liable for any decision made or action taken in reliance upon the information provided through this CME activity.
Medical Review Case #1
Mid afternoon, A 67 year old male suddenly develops sore throat, chills and nausea.
Later that evening he had a sleepless night with fevers and pain.
That morning family called the physician and who ordered a throat elixir to gargle. Unfortunately, the man aspirated. As the day progressed his condition worsened and he died.
Questions:
1. Should the patient have received a tracheostomy?
2. Antibiotics?
3. Intubation?
8
ANSWER
YES
9
WHO was the Patient?
1. Theodore Roosevelt
2. Harry S Truman
3. George Washington
4. Woodrow Wilson
Hint: “ He was first in War, First in Peace and First in the Heart of his country man.”
10
Answer 11
Medical Review #2
51 YO male is relocated to a near by Island for a short stay. He returned to the main land for 100 days. He develops a heart condition and retires to another near by island.
On this Island he tries less stressful activities such as gardening. He then develops upper gastric pain that is unrelieved by eating and the best medication available is given. Unfortunately, he dies. Autopsy reveals a gastric ulcer.
Who was the patient?
1. Ralph Emerson
2. Ernest Hemingway
3. Napoleon Bonaparte
4. Adolf Schicklguber
12
Answer 13
Constant Change and Improvement
In 1910, when Abraham Flexner researched the state of US medical education, only 16 of the existing 155 medical schools required more than a high school education for admission. Germ theory was still disputed.
Today’s standards of care are now mostly based on scientific evidence. In the past 20 years, courts have held physicians and hospitals to national standards of care rather than accepting local variations in the practice of medicine
14
Case Study: 1
Tom was 12 years old when his appendix burst and he was taken to the local pediatric hospital. 3 days after the appendectomy, he developed another high fever. One week later, the surgeon performed a second procedure and found that a surgical sponge had been left inside.
Postoperative sponge and instrument counts have been routine for decades. There is no single standard, although nursing and surgical organizations have developed best practices for sponge , needle, and instrument counts.
Different ways of counting sponges may be used in the same operating room even during the same case, says the Association of Operating Room Nurses. This Lack of standardized practice creates opportunities for errors
15
Sponges
A Us Department of Health and Human Services study say that this type of mistake occurs in 1:100 to 1:500 persons.
Nursing and surgical groups recommend that each member of the surgical team play an equal role in assuring accuracy of the counts. Recently, manufacturers have made sponges with threads visible on x-rays, radiofrequency identifications systems, and bar coding to alert staff about missing sponges.
16
Case Study: 2
Lillian was 68 years old and weighed 250lb when she underwent surgery to remove her gallbladder. The second day after surgery, she needed help to walk to the bathroom. Lillian’s nurse Millie, wasn’t strong enough to support her and they both fell, breaking Millie's right arm and Lillian’s left leg.
Historically, schools of nursing have taught students to manually lift patients using proper body mechanics, such as lifting with the legs and using correct posture. However, body mechanics are not sufficient to protect nurses from heavy weights, awkward postures, and the repetition involved in manually lifting patients, according to a position paper from the American Nurses Association (ANA)
17
Case Study: 2
The ANA supports policies that eliminate manual patient lifting. Safe patient-handling techniques involve the use of such equipment as full-body slings, stand–assist lifts, lateral transfer devices, and friction-reducing devices.
There is no federal legislation or regulation on safe patient handling, although several states have enacted such legislation, ANA says.
18
Medical Errors
We learn from our most painful mistakes.
Mistakes can injure patients and cause physicians to become engaged in legal and professional trouble.
Studying and learning how to prevent, monitor and respond to them helps to change the standard of care. This in turn, helps to eliminate common medical errors.
By eliminating common medical errors physicians can protect patients, and ultimately themselves from lawsuits.
19
Statistics
Deaths in hospitals (44,000) due to Medical errors exceeded the annual deaths attributable to motor vehicle accidents (43,458) breast cancer (42,297), or Aids (16,516).
In 2011 Florida ACHA reported 125 deaths occurred as a result of hospital error (31% of 405)
Surgical procedures unrelated to the patient’s diagnosis or medical needs (25%)
Surgical procedures to remove a foreign body from a previous surgical procedure (21%)
Surgical repair of injuries or damage resulting from a planned procedure (7%)
Brain damage (7%)
20
Medical Error 21
The Institute of Medicine’s Committee on Quality of Healthcare defines Medical Error as “ The failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim.
The AMA defines a medical error as “an
unintended act or omission, or a flawed system or plan, that harms or has the potential to harm a patient.”
Medical Errors
Medical Errors are not defined as intentional acts of wrong doing; not all medical errors rise to the level of medical malpractice of negligence.
Two types of errors
Either the correct action does not proceed as intended, and “Error of execution”
Or
The original intended action is not correct “Error of planning”
22
Preventable Adverse events or Sentinel events
Medical errors that result in injury are sometimes called preventable adverse events or sentinel events-sentinel because they signal the need for immediate investigation and response.
Preventable adverse events or sentinel events are defined as those events that cause an injury to patients as a result of medical intervention or inaction on the part of the healthcare provider whereby the injury cannot reasonably be said to be related to the patients underlying medical condition.
23
Events that our subject to review by the Joint Commission
The event has resulted in an unanticipated death or major permanent loss of function, not related to the natural course of the patient’s illness or underling condition.
OR
The event is one of the following (even if the outcome was not death or major permanent loss of function unrelated to the natural course of the patient’s illness or underling condition):
24
Joint Commission Reportable Events
1. Suicide of any patient receiving care, treatment, and services in a staffed around-the-clock care setting or within 72 hours of discharge
2. Unanticipated death of a full-term infant
3. Abduction of any patient receiving care, treatment , and services.
4. Discharge of an infant to the wrong family
5. Rape, assault ( leading to death or permanent loss of function), or homicide of any patient receiving care, treatment and services.
6. Rape, assault ( leading to death or permanent loss of function), or homicide of any staff member, licensed independent practitioner, visitor, or vendor while on site at the healthcare organization
25
Joint Commission Reportable Events
7. Hemolytic transfusion reaction involving administration of blood or blood products having major blood group incompatibilities (e.g. ABO, Rh other blood groups)
8. Invasive procedure, including surgery, on the wrong patient or wrong site. 9. Unintended retention of foreign object in a patient after surgery or other invasive procedures
10. Severe neonatal hyperbilirubinemia ( Bilirubin >30) 11. Prolonged fluoroscopy with cumulative dose >1500 rads
to a single field or any delivery of radiotherapy to the wrong body region or >25% above the planned radiotherapy dose.
26
Root Cause Analysis
A process for identifying the basic or casual factors that underlie variation in performance, including the occurrence or possible occurrence of a sentinel event.
The Joint Commission requires that healthcare organizations conduct thorough and credible root cause analyses that focus on process and system factors, and documentation of a risk-reduction strategy and internal corrective action plan that includes measurements of effectiveness of process and systems improvements to reduce risk.
27
A thorough Root Cause Analysis must include
1. A determination of the human factors most directly associated with the sentinel event and the processes and systems related to its occurrence
2. Analysis of the underlying systems and processes through a series of “why” questions to determine where redesign might reduce risk
3. Inquiry into all areas appropriate to the specific type of event
4. Identification of risk points and their potential contributions to this type of event
5. A determination of potential improvement in processes or systems that would tend to decrease the likelihood of such events in the future, or a determination, after analysis exists.
28
A credible root cause analysis must include
1. The organization’s leadership and the individuals most closely involved in the process and systems under review must participate in the analysis.
2. The analysis must be internally consistent: that is, it must not contradict itself or leave obvious questions unanswered.
3. The analysis must provide an explanation for all findings of “not applicable” or “no problem”
4. The analysis must include considerations of any relevant literature.
29
Florida Law
Certain Serious adverse incidents are mandated to be reported to Florida's Agency for Health Care Administration (ACHA)
The risk manager must summit incident reports within 3 business days of the incident and depending on the type of incident has to file a full report to ACHA within 15 days.
30
Florida Statute 395.0197
An event over which healthcare personnel could exercise control and which is associated in whole or in part with medical intervention rather than the condition for which such intervention occurred and results in one of the following:
1. Death
2. Brain or spinal damage
3. Permanent disfigurement
4. Fracture or dislocation of bones or joints
5. A resulting limitation of neurological, physical or sensory function which continues after discharge from the facility
6. Any condition that required specialized medical attention or surgical intervention resulting from nonemergency medical intervention, other than an emergency medical condition, to which the patient has not given his or her informed consent
31
Florida Statute 395.0197
7. Any condition that required the transfer of the patient, within or outside the facility, to a unit providing a more acute level of care due to the adverse incident rather than the patient condition prior to the adverse incident.
a. Performance of a surgical procedure on the wrong patient, wrong surgical procedure, wrong site, or a surgical procedure otherwise unrelated to the patient’s diagnosis or medical condition.
b. Surgical repair of damage resulting to a patient from a planned surgical procedure, where the damage was not a recognized specific risk as disclosed to the patient and documented through informed consent process.
c. A procedure to remove unplanned foreign objects remaining from a surgical procedure
32
Florida Board of Medicine 33
Wrong site/wrong procedure surgery continues to be the most common basis for quality of care violations.
The 5 Most Misdiagnosed conditions:
1. Cancer related issues
2. Neurological related issues
3. Cardiac related issues
4. Timely response to complications both during surgery and post-operatively.
5. Urological related issues
Florida Board of Medicine 10/26/2014
Florida Board of Osteopathic Medicine
The 5 Most Misdiagnosed conditions:
1. Inappropriate prescribing of opioids in patients in whom there have been misdiagnosis or failure to diagnose addiction, psychiatric conditions and diversion;
2. Failure or delay in diagnosing cancer;
3. Retained foreign objects in surgery and wrong site/patient surgery;
4. Surgical complications/errors and pre-operative evaluations; and
5. Prescribing, dispensing, administering, or using non-FDA approved medications and devices.
34
Florida Board of Osteopathic Medicine 08/14/2014
Cancer
12% of Cancer patients are misdiagnosed
Cause of cancer diagnosis may be underdiagnosed based on the different body parts
Lung Cancer –misreading x-ray, lack of follow-up
Breast Cancer-misreading diagnostic exams, poor documentation, importance of biopsy
Prostate Cancer – failure to diagnose (PSA), lack of follow up, treatment misadventures
Colorectal – failure to diagnose, poor documentation
35
Notifying patients of Test Results 36
7.1% rate of apparent failures to inform patients of abnormal test results
These failures were associated with missed cancer diagnoses.
Updated Breast Cancer Screening
The ACS recommends that women with an average risk of breast cancer should undergo regular screening mammography starting at age 45 years (strong recommendation)
45-54 years screened annually (qualified recommendation)
> 55 should transition to biennial screening or have the opportunity to continue screening annually (qualified
recommendation)
40-44 should have the opportunity to begin annual screening (qualified recommendation)
Women should continue screening mammography as long as their overall health is good and they have a life expectancy of 10 years or longer (qualified recommendation)
JAMA.2015;314(15):1599-1614.doi:10.1001/jama.2015.12783
37
Neurological Conditions
Stroke is most commonly missed or delayed diagnosis, which reduces survival rates
Diagnosis of strokes are missed in 14% of patients younger than 50 years of age
Because the time window for tPA is short, suspected stroke or transient ischemic attack should be triaged as if he/she were a serious trauma patient
38
Cardiac Related Issues
Acute Coronary Syndrome (ACS) is most prevalent cause of chest pain presented to emergency departments
Classic symptoms (tightness, sensation of pressure, heaviness, crushing, vise-like, aching pain), but women and older patients present with atypical symptoms, i.e. numbness, tingling, burning, stabbing, prickling
39
Cardiac Related Issues Continued
Atypical chest pain areas include back, between should blades, upper abdomen, shoulder, elbows, axillae, or ears
Other reasons for missed ACS diagnosis include failure to: interpret history, interpret of electrocardiogram, perform EKG, and/or lack proper cardiac enzyme test
Daraswhe, A. et al. (2007) Misdiagnoses ACS. Israeli Journal of Emergency Medicine. 2007;7(3):3-10.
40
Surgical Complications
According to study reported in JAMA October 2015, current estimates show 1 event per 100,000 wrong-site surgery and 1 event per 10,000 procedures for retained surgical items
Follow appropriate time-out procedures and use appropriate sponge-counting systems
Postoperative complications account for up to 22% of preventable deaths among patients.
Thorough assessment of patient both pre-surgery and within post-anesthesia care unit
41
Urological-Related Issues
Difficult to diagnose as presenting symptoms are similar and definitive diagnosis tests are unavailable or underutilized
Nephrolithiasis has similar presentation as abdominal aortic aneurysm, urinary tract infection and other flank pain causes
Delayed diagnosis and treatment of UTI secondary to stone passing through urethra is considered medical liability
42
REMS: Risk Evaluation and Mitigation Strategy
The State of Florida has placed greater emphasis on medical errors, deaths and outcomes related to inappropriate prescribing and usage of controlled substances especially OPIOIDS
43
Prescription Opioid Abuse
According to October 19, 2015 NEJM article people with opioid dependence use both prescription opiates and heroin concurrently
Increased to 42% in 2014 from 24% in 2008
44
NEJM, 2015; 373:1789-1790,doi:10.1056/NEJMc1505541
What is Chronic Pain?
“Pain that persists beyond normal tissue healing time, which is assumed to be three months.” (per International Association for the Study of Pain).
Chronic noncancerous pain
45
Incidence of Chronic Pain
Affects approximately 100 million Americans
According to IOM report Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research costs society $560-$635 billion annually in treatment and lost productivity
46
Characteristics of Chronic- Pain vs. Addicted Patients
CHRONIC- PAIN PATIENT
ADDICTED PATIENT
Medication use is not out of control Medication use is out of control
Follows the practioner-patient agreement for use of the opioid
Does not follow opioid agreement
May have left over medication
Does not have left over medication Loses prescriptions Always has a story about why more drug is needed
47
Poor Medication Outcomes
Patients:
1. Took too much medication or mixed it with
unauthorized substances
2. Were prescribed too much medication by a
physician. Some risk factors include:
• Physician error due to knowledge deficits
• Patient non-adherence to medication regime
• Unanticipated medical and mental health
comorbidities, including substance use disorders
• The presence of additional CNS depressant drugs
48
Risk Factors Associated with Opioids that predispose a patient to serious morbidity and mortality
Advanced age
Impaired renal or hepatic function
Obesity
Cardiopulmonary disorders
Sleep apnea
Mental illness
Patients that combine opioids with respiratory depressants (alcohol, sedative-hypnotics, benzodiazepines, barbiturates)
49
Medication Errors: Patient, Provider, and System-based Factors
Chronic health conditions that predispose an individual to opioid-related adverse event
Failure to adjust opioid dosing in elderly and for hepatic and renal impairment
Multiple doses and routes of administration of opioids
Coadministration of opioids with other sedating medications
Poor patient hand-offs and pharmacy oversight
50
Four key questions to answer when obtaining informed consent in treatment for opioids
1. Does the patient understand various options for treatment?
2. Has the patient been reasonably informed of the potential
benefits and risks associated with each of those options?
3. Is the patient free to choose among those option, free from
coercion by the healthcare professional, family and others?
4. Does the patient have the capacity to communication his/her
preferences – verbally or in other ways (i.e.. deaf/mute)?
51
Signs and Symptoms of Opioid Overdose
Intoxicated behavior – confusion, slurred speech, stumbling
Dizziness or fainting
Unusual snoring, gasping or snorting during sleep
Difficulty waking up from sleep
Acting drowsy or groggy and having trouble staying awake.
52
Universal Precautions
• ANY patient in pain can have a drug misuse
problem.
• Personal or family history of alcohol or drug
abuse
53
CDC Recommendations for Responsible Opioid Prescribing
Use opioid medication for acute and chronic pain only after trying alternative therapies.
Consider urine testing for opioids in patients less than 65 yr. of age with non-cancer pain who is being treated with opioid for more than six weeks
Do not prescribe ER/LA opioids for acute pain
54
Prevention of Medication Errors
Obtain complete medical H&P evaluation prior to treatment and document within medical record
Develop written plan for assessing patient’s risk of aberrant drug related behavior
Provide on-going monitoring of drug-related behavior with drug testing as necessary
Follow FDA Drug Schedule
Use E-Force: www.EFORCSE.com
55
Non-FDA approved medications and devices
Know the law-do not prescribe, dispense or administer, or use non-FDA approved medications and devices
Follow FDA guidelines
Document treatment plan
56
Error Reduction and Prevention
Wrong site/Wrong procedure surgery
It is recommended that a surgeon sign their initials at the correct site of surgery with an indelible pen.
Follow the Universal Protocol
Pre-procedure verification process
Mark the operative/procedure site with an indelible marker
Taking a time-out with all team members immediately before starting the procedure
In 2007, The Joint Commission recommended a Zero tolerance policy for not following the Universal Protocol, this includes the administration of regional anesthetics and radiological interventions.
58
Delays in treatment
According to the Joint Commission, more than half of all reported sentinel event cases of patient death or permanent injury due to delays in treatment were in an emergency department setting.
The most common reason for a delay in treatment is misdiagnosis.
59
Study 60
A systematic review of 53 different series of autopsies reported a median error rate of 23.5 % (range 4.1% to 49.8%) for major errors (clinically missed diagnoses involving a principal underlying disease or primary cause of death) and 9.0 % (range, 0% to 20.7%) for class I errors (the most serious subset of major errors being those likely to have affected patient outcomes).
In essence, approximately 35,000 patients who might have survived to discharge from United States hospitals annually had misdiagnosis not happened.
Potential Causes 61
Patient non-adherence to physician recommendations was present in 44% of patients with missed opportunities.
Diagnosis timing, EX: early identification of sepsis (along with protocols for treatment pathways) has been associated with decreased mortality in surgical intensive care.
Cognitive Factors 62
The cluster of automatic or quasi-automatic decision making processes may be classified as heuristics, or rule-based decision making processes.
This process is also subject to error when attention is pulled away from the task at hand or cognitive capacity is altered for other reasons ( e.g., Lack of sleep)
Malpractice claims attributable to diagnostic
errors 63
Recent study of 91,082 diagnosis-related malpractice claims from 1986 to 2010 estimated payments summing to 38.8 billion dollars
Mean per payout was $386,849
Diagnosis –related claims made up 28.6 % of total claims and accounted for the highest proportion of total payments (35.2%)
In terms of Severity, lethal injuries accounted for 48.4% of total payments.
Tehrani, et al. Quality and Safety in Health Care 2013; 0:1-9 doi:10.1136/bmjqs-2012-001550
Malpractice claims continued…. 64
Study of 350,706 Malpractice claims from the 1986-2010 National practitioner Data Bank found that diagnosis –related reasons accounted for 68.8 % of paid claims from outpatient settings
Inpatient diagnostic errors were more likely to be lethal at 48.4%
Diagnostic reasons were the second most-frequently cited for paid claims in the inpatient setting.
Diagnosis errors 65
The most common missed or delayed diagnosis that physicians recalled were, pulmonary embolism, drug reactions or overdose, various cancers, acute coronary syndrome and stroke.
Diagnostic Error Evaluation and Research (DEER) project tool Found that over 43% were related to clinician assessment
(including failure/delay in considering the diagnosis, placing too much weight on competing /coexisting diagnosis) and 42% to laboratory and radiology testing (including failure to order needed tests, technical errors in processing specimens/tests, erroneous reading of a test)

Possible interventions to reduce diagnostic errors
66
1. Patient factors: Systems may be designed around areas that are more prone to risk (e.g., improved staffing with translators)
2. Human/Clinician Factors: Interventions may aim at errors of planning separately from errors of execution, and may also be designed to address cognitive error, skill-set error, task –based error, and / or personal impairment.
3. Outside care systems, ED access and triage: Consideration of these three framework areas aims to understand patterns of failure and errors that affect patients before their arrival in the ED or initiation of care.
4. Teamwork: Interventions in this area focus on communication, coordination, conflict resolution, personnel assignment practices (considerations of capability workload) and training.
5. Local ED environment, hospital environment, hospital administration and third parties, and community level: systems and resources at each of these four additional levels of the framework have potential for effective interventions to reduce diagnostic errors within the ED and after the patient leaves.
Medication Errors The most common cause of avoidable harm to patients
“Any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the healthcare professional, patient or consumer. “(The National Coordinating
Council for Medication Error Reporting and Prevention)
Medication errors stem from a variety of causes, including miscommunication between prescribers and pharmacists in the form of misunderstood and/ or illegible abbreviations.
67

Official “Due Not Use” List 68
Do Not Use Potential Problem Use instead
U, u (unit) Mistaken for “O” ( zero, the number “4” ( four) or “cc”
Write “Unit”
IU (International Unit) Mistaken for IV (intravenous) or the number (ten)
Write “International Unit”
Q.D., QD, q.d., qd(daily) Q.O.D., QOD, q.o.d., qod (every other day)
Mistaken for each other Period after the Q mistaken for “I” and the “O” mistaken for “I”
Write “Daily” Write “Every other day”
Tailing Zero ( x.0 mg)* Lack of Leading Zero (.x mg)
Decimal Point is missed Write X Write 0.x
MS MSO4 and MgSO4
Can mean morphine sulfate or magnesium sulfate Confused for one another
Write “morphine sulfate” Write “magnesium sulfate”
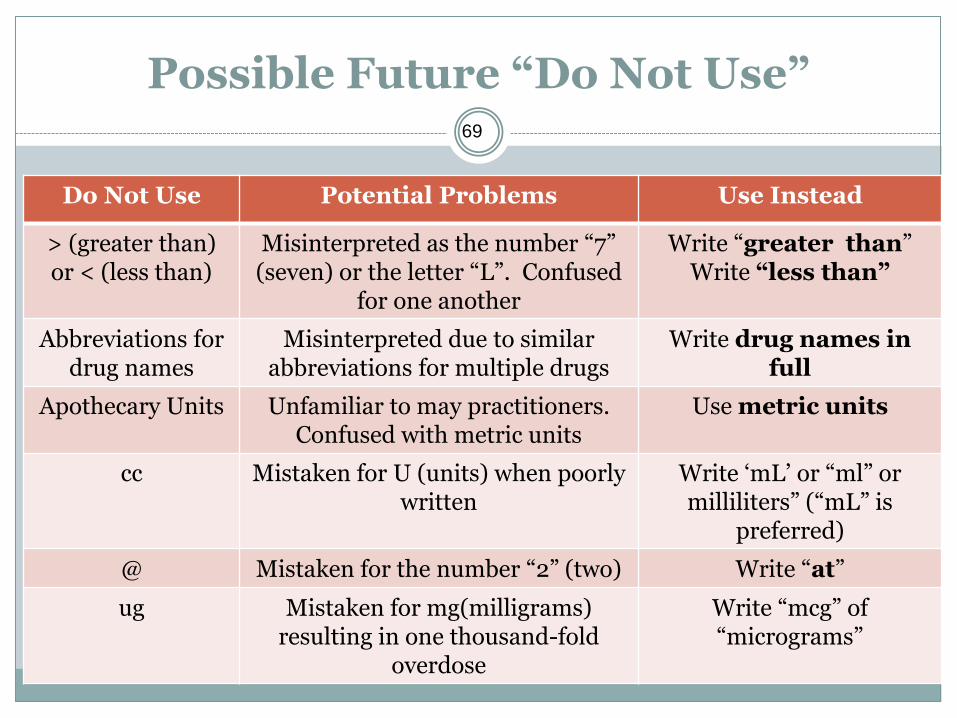
Possible Future “Do Not Use” 69
Do Not Use Potential Problems Use Instead
> (greater than) or < (less than)
Misinterpreted as the number “7” (seven) or the letter “L”. Confused
for one another
Write “greater than” Write “less than”
Abbreviations for drug names
Misinterpreted due to similar abbreviations for multiple drugs
Write drug names in full
Apothecary Units Unfamiliar to may practitioners. Confused with metric units
Use metric units
cc Mistaken for U (units) when poorly written
Write ‘mL’ or “ml” or milliliters” (“mL” is
preferred)
@ Mistaken for the number “2” (two) Write “at”
ug Mistaken for mg(milligrams) resulting in one thousand-fold
overdose
Write “mcg” of “micrograms”
Abbreviation Error “Fun” Facts 70
Most errors (81%) occur during prescribing
Between 2004 and 2006 a total of 29,974 medication errors out of 643,151 (4.7%) reported to the MEDMARX program were associated with abbreviations.
43% were due to using the term “QD”
Electronic Prescribing 71
Eliminates illegible handwriting
Clinical decision support may be configured to prompt providers to avoid abbreviations and /or to auto –correct or translate abbreviations to preferred terms.
System-Related Interventions 72
The 6 interventions that address the organizational vulnerabilities to diagnostic research
1. Technique – ( introduction of novel technologies for testing, adaptations of testing equipment, or changed in medical interventions potentially affecting diagnostic performance)
2. Additional Review Methods - ( introduction of additional steps from the interpretation through reporting of test results)
3. Personnel Changes - ( introduction of additional health care members and/or replacing certain professionals with others
4. Educational Interventions – ( Implementation of Educational Strategies)
5. Structured Process Changes – ( Implementation of feedback systems or additional stages in the diagnostic pathway)
6. Technology– based Systems – ( Implementation of technology-based tools at the system level-computer assistive diagnostic aids, decision support algorithms, text message alerting, pager alerts, etc.)
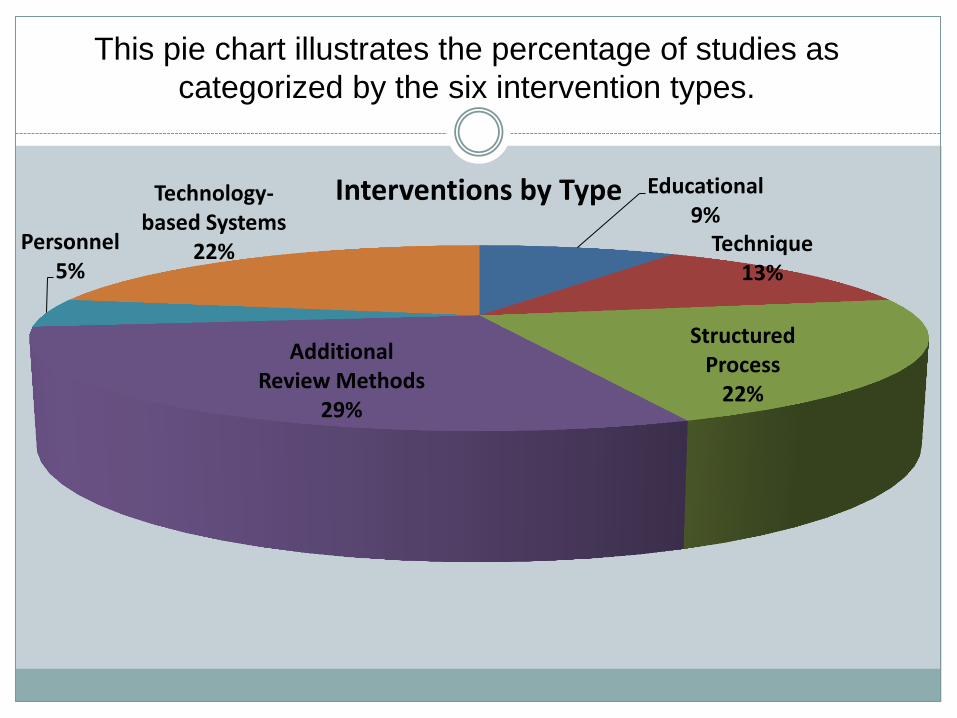
Educational 9%
Technique 13%
Structured Process
22%
Additional Review Methods
29%
Personnel 5%
Technology-based Systems
22%
Interventions by Type
This pie chart illustrates the percentage of studies as
categorized by the six intervention types.
Patient Safety Practices 74
1. Preoperative checklists and anesthesia checklists to prevent operative and post –operative events
2. Bundles that include checklists to prevent central line-associated bloodstream infections
3. Interventions to reduce urinary catheter use, including catheter reminders, stop orders, or nurse initiated removal protocols
4. Bundles that include head of bed elevation, sedation vacations, oral care with chlorhexidine, and subglottic-suctioning endotracheal tubes to prevent ventilator-associated pneumonia
5. Hand Hygiene
6. “Do not use” list
7. Multicomponent interventions to reduce pressure ulcers
8. Barrier precautions to prevent healthcare-associated infections
9. Use of real-time Ultrasound for central line placement
10. Interventions to improve prophylaxis for venous thromboembolisms
Encouraged Patient Safety Practices 75
1. Multicomponent interventions to reduce falls
2. Use of clinical pharmacists to reduce adverse drug events
3. Documentation of patient preferences for life-sustaining treatment
4. Obtaining informed consent to improve patients understanding of the potential risks of procedures
5. Team training
6. Medication reconciliation
7. Practices to reduce radiation exposure from fluoroscopy and computed tomography scans
8. Use of surgical outcome measurements and report cards like the American College of Surgeons
9. National Surgical Quality improvement program
10. Rapid response systems
11. Utilization of complementary methods for detecting adverse events/medical errors to monitor for patient safety problems
12. Computerized provider order entry
13. Use of simulation exercises in patient safety efforts
Pay for Performance
Many payers, including the Centers for Medicare & Medicaid Services, have embedded patient safety into pay-for-performance and “no pay for errors” initiatives.
76
Pearl of Wisdom
If a patient decides to leave against medical advice (AMA), the physician needs to document in the medical record by a written progress note:
1. His discussion with the patient of why he needs to stay and
2. the consequences of not staying in the hospital.
In the event the patient decompensates at home, the physician has the documentation to protect him from liability
77
Conclusion
US has one of the top 40 healthcare systems in the world ….Why are the numbers of Medical Errors so High?
Physicians should actively participate in the root cause analysis process, understanding the goal is not to blame but rather make process improvements.
78

Resources
Daraswhe, A. et al. (2007) Misdiagnoses ACS. Israeli Journal of Emergency Medicine. 2007;7(3):3-10
JAMA.2015;314(15):1599-1614.doi:10.1001/jama.2015.12783
NEJM, 2015; 373:1789-1790,doi:10.1056/NEJMc1505541
Tehrani, et al. Quality and Safety in Health Care 2013; 0:1-9 doi:10.1136/bmjqs-2012-001550
79