meckel’s diverticulum. general data i.s. 6 mos old female filipino roman catholic pandacan, manila
TRANSCRIPT
Meckel’s Diverticulum
General DataI.S.6 mos oldFemaleFilipinoRoman CatholicPandacan, Manila
Bloody stools
History of Present Illness4days PTC fever (T38.8C),Paracetamol drops
no fever, cough, colds, vomitinggood appetite and activityno consult
2 days PTC persistence prompted consult with AMD, Dx: acute viral illness
1 day PTC lysis of fever 2 episode of dark stools, irrritable,
decrease in appetiteER : SFA ileus; no recurrence of
stoolsDx : AVI, resolving; t/c Milk Allergy
History of Present IllnessFew hrs PTC 2 episode of voluminous
maroon colored stoolsAdmitted
Review of SystemGeneral: (-) weight loss, anorexia, easy
fatigabilityHEENT: no trauma, no ear infection, Neck: (-) limitation of motion, mass,
adenopathy Respiratory: (-) shortness of breath, easy
fatigability, wheezing Cardiology: (-) palpitation or cyanosisMusculoskeletal: (-) swelling, deformities
Past Medical HistoryNo bronchial asthma no Primary Tuberculosis infectionno known allergiesThis is the patient’s first admission
Family History(+) Diabetes: maternal grandparents(+) Hypothyroid : motherNo history of cancer
Birth and Nutritional HistoryBorn to a 34 year old G3P2, non-smoker,
non-alcoholic beverage drinker, with regular prenatal check up
Denied illness during pregnancyBorn Full term via Repeat Ceasarian section
at Cardinal Santos Medical CenterNo fetomaternal complicationsNo history of BreastfeedingEnfapro 6oz/bottle x 12 bottles/dayComplimentary feeding (Cerelac): 6 mos old
ImmunizationBCG 1 DOSE
HEPA B 2 DOSES
DPT 2 DOSES
OPV 2 DOSES
Developmental HistoryPresently, sits with support
Upon arrival ERS>(+) maroon
colored stoolO>pale looking,
irritableHR 106 RR28 clear breath soundssoft abdomen, non tendergood pulses
A>Lower GI bleed t/c Meckel’s Diverticulum
P>lab work up PRBC 10cc/kgpost transfusion Hgb 10.6
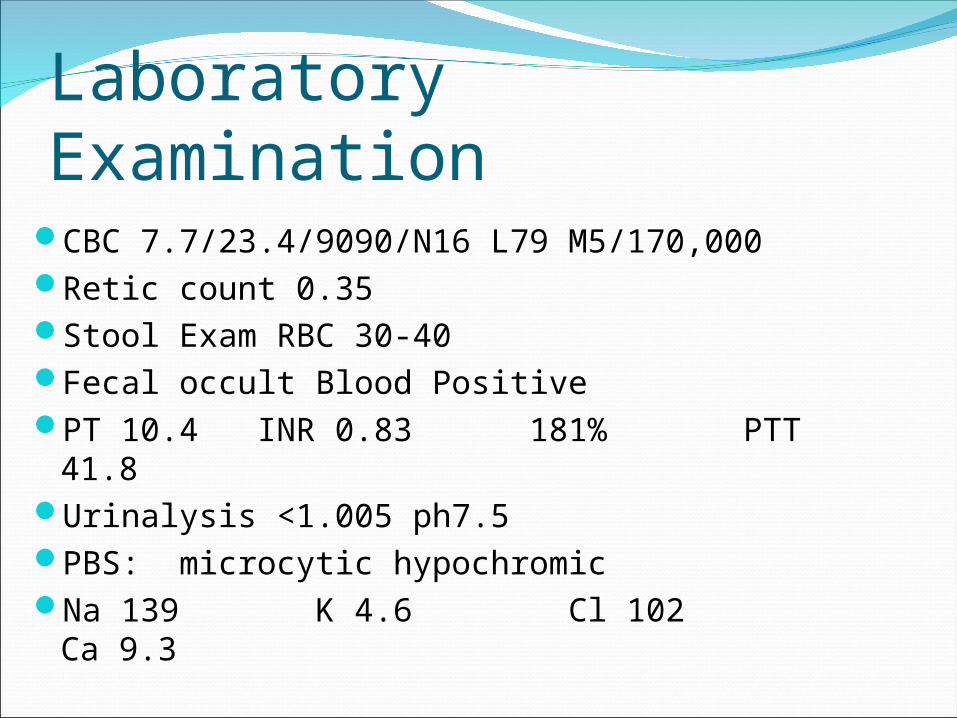
Laboratory ExaminationCBC 7.7/23.4/9090/N16 L79 M5/170,000Retic count 0.35Stool Exam RBC 30-40Fecal occult Blood PositivePT 10.4 INR 0.83 181% PTT 41.8Urinalysis <1.005 ph7.5PBS: microcytic hypochromicNa 139 K 4.6 Cl 102 Ca 9.3
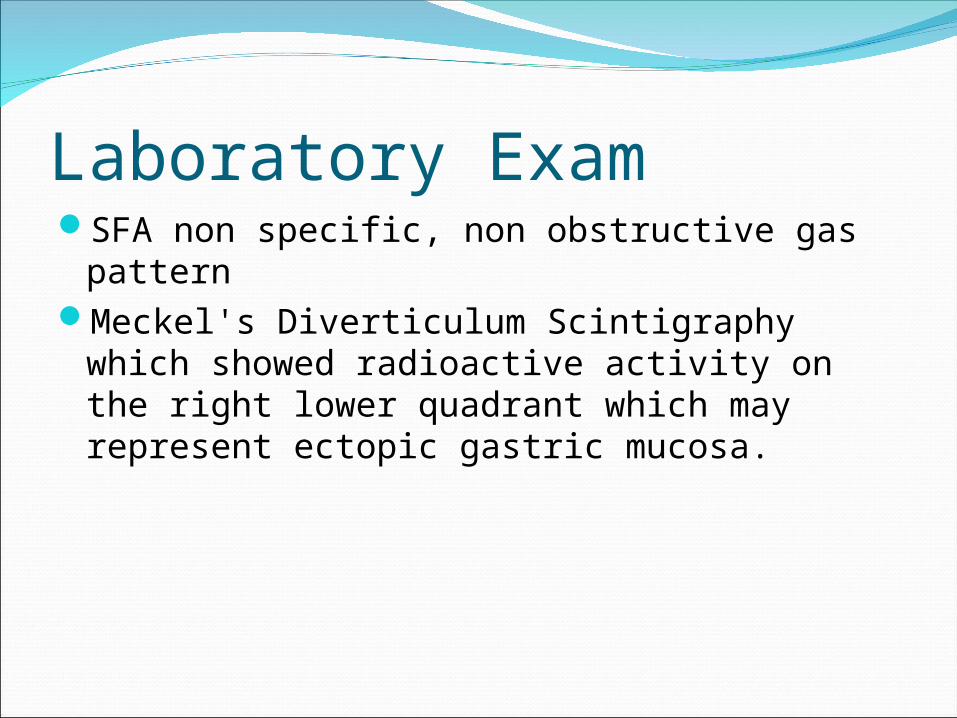
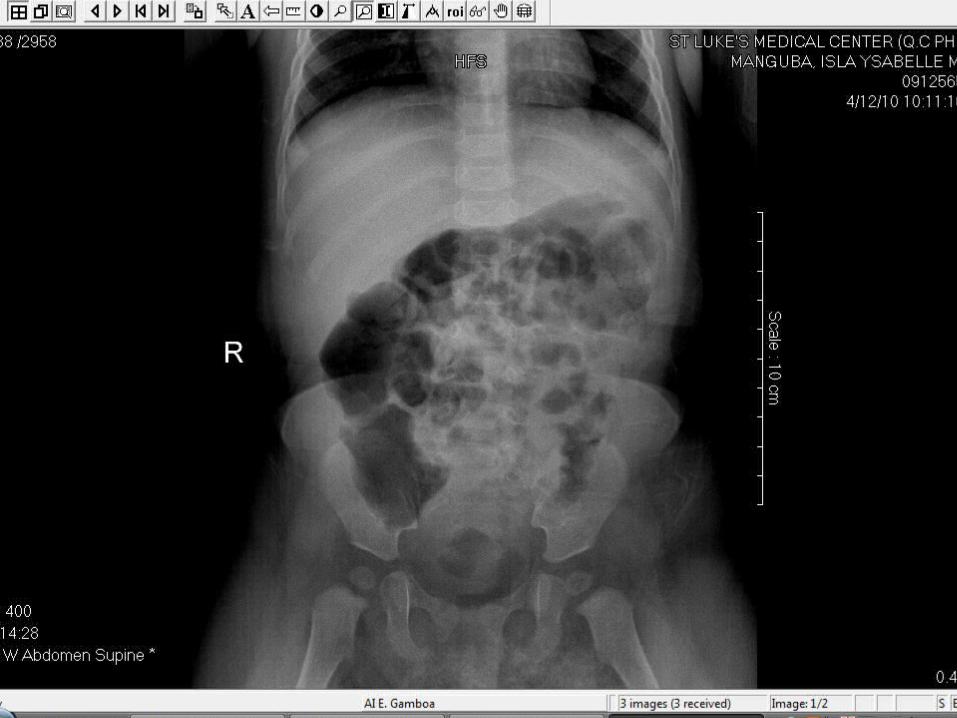
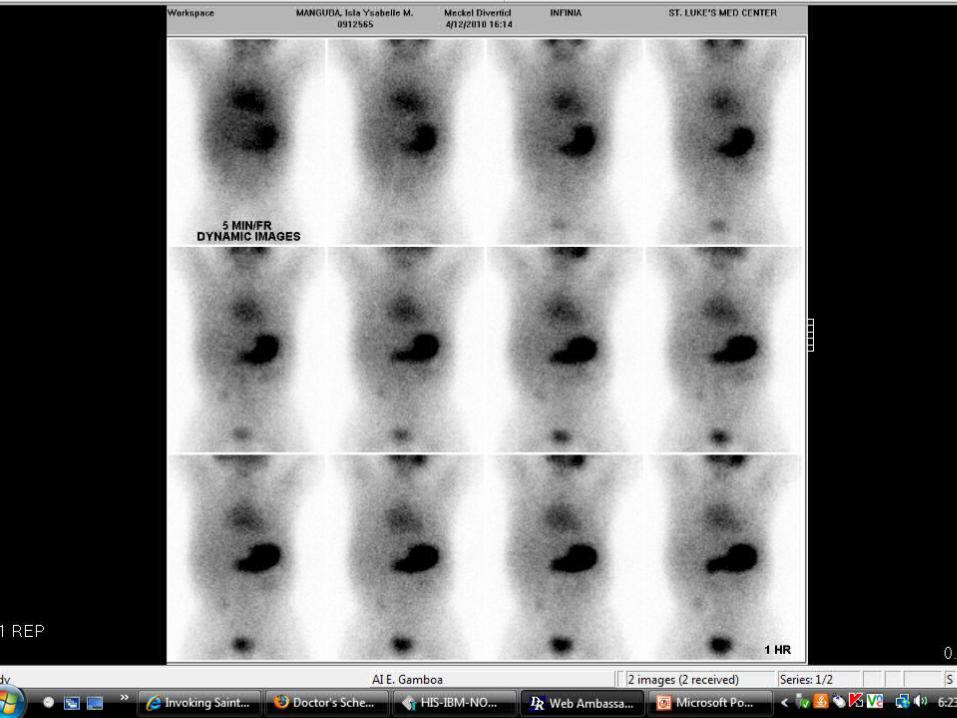
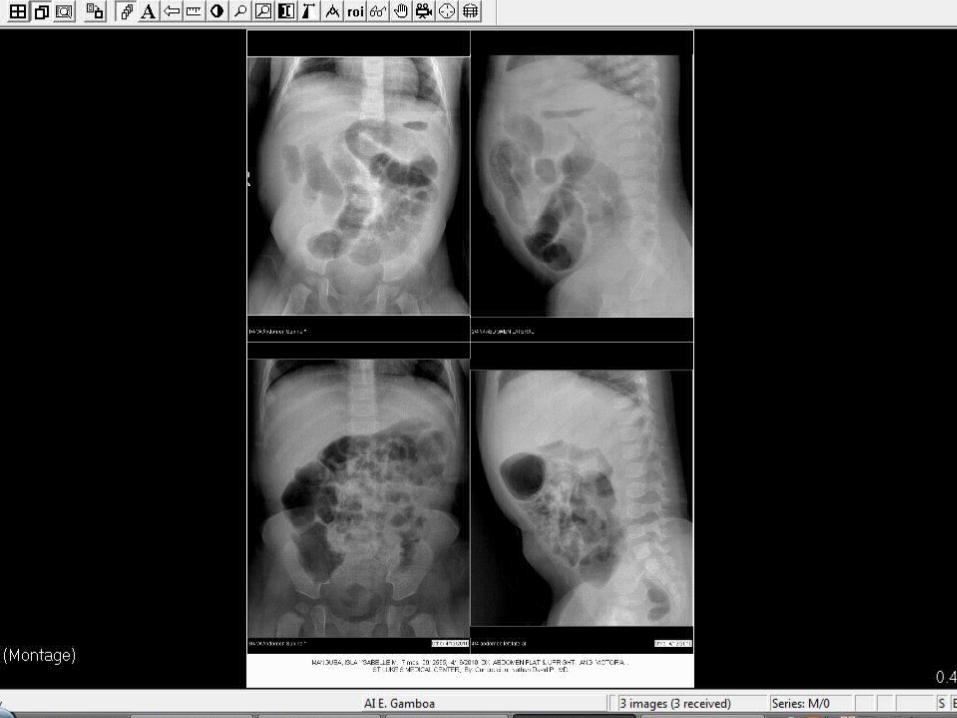
Laboratory ExamSFA non specific, non obstructive gas patternMeckel's Diverticulum Scintigraphy which
showed radioactive activity on the right lower quadrant which may represent ectopic gastric mucosa.

Upon arrival at PICUs/p Explore
Laparotomy, Resection of Meckel’s diverticulum with end to end anastomosis
OR findings: 1.5cm Meckel’s Diverticulum approx 25cm from appendix
Estimated Blood Loss <20cc
s/p 160 PRBC (20cc/kg)
P> NPOD5NR x 40cc/hrCefazolin 250mg/IV
(125mkd)Ranitidine 10mg/IV q8Nubain 2mg q6Ketorolac 10mg q6
Second PICU DayS> no bleedingO>BP 90/60,
afebrile Stable VSCBC
13.7/39/11680/N50 L40 M8 B1/268K
P> transfer to regular room
Meckel’s Diverticulumremnant of the embryonic yolk sacEmbyonal stage: omphalomesenteric duct
connects the yolk sac to the gut, nutrition5th and 7th wk AOG: duct separates from the
intestineYolk sac + lining epith similar to stomachPartial or complete failure of involution of the
omphalomesenteric duct results in various residual structures.
FrequencyOccurs in 2–3% of all infantsa 3–6 cm outpouching of the ileum along the
antimesenteric border 50–75 cm from the ileocecal valve
1st 2 years of life, 2.5yo
ManifestationsIntermittent painless rectal bleeding Stool: brick colored or currant jelly colored. Bleeding: self-limited, contraction of the
splanchnic vesselsr/o acute appendicitisDiverticulitis can lead to perforation and
peritonitis
DiagnosisMeckel radionuclide scan: IV infusion of
technetium-99m pertechnetate: mucus secreting ectopic gastric mucosa : visualization of the Meckel diverticulum
sensitivity enhanced scan : 85%specificity : 95%. Other methods of detection: abdominal
ultrasound, superior mesenteric angiography, abdominal CT scan, and exploratory laparoscopy.