mechanistic pain profiling of patients with …
TRANSCRIPT
MECHANISTIC PAIN PROFILING OF PATIENTS WITH OSTEOARTHRITIS
CURRENT KNOWLEDGE AND FUTURE DIRECTIONS
DOCTORAL THESIS (DR.MED.)
KRISTIAN KJÆR PETERSEN


This thesis is dedicated to my close collaborator, mentor, and friend dr.med., Ph.D. Ole Simonsen, who retired as orthopedic surgeon and excellent re-searcher in the summer of 2020. This work and the work of so many oth-er young researcher in Aalborg would not have been possible without Ole Simonsen as a source of inspiration, motivation, and continued support. The pain field and the general research environment around musculoskeletal pain conditions in Aalborg are forever in depth to Ole Simonsen’s work and com-mitment.

Mechanistic Pain Profiling of Patients with Osteoarthritis
4
Kristian Kjær Petersen (KKP)
5
KRISTIAN KJÆR PETERSEN (KKP)KKP is trained as a biomedical engineer, received his M.Sc. de-gree in 2011 and his Ph.D. degree under the supervision of Prof. Lars Arendt-Nielsen in 2014 from Aalborg University, Denmark.
KKP’s long-term mission is to develop the concept: “Personalized Mechanistic Pain Medicine” to provide the correct treatment for the right patient. Specific focuses are on 1) development of pain assessment tools and models, 2) validation and reliability of these models and tools and 3) understanding underlying features of pain mechanisms and predict-ing pain outcomes after treatment.
Through extensive work with Prof. Thomas Graven-Nielsen, Prof. Lars Arendt-Nielsen, and industrial partners, KKP has developed the cuff algometer, which is being used in studies around the world.
KKP has published more than 70 peer-reviewed papers with focus on pain mechanistic profil-ing and understanding the underlying mechanisms for chronic pain. In the period 2017-2020, he was ranked as the 3rd most publishing author and the 2nd most cited authors in the world within the topic of: “Central sensitization in patients with knee osteoarthritis” according to Scopus SciVal.
KKP has years of experience on leading national and international research projects (approx. 35% of papers are published with international partners), has hosted and given lectures at the World Congresses on Pain (IASP) and the Congresses of the European Pain Federation (EFIC), and was appointed as an “Aalborg University Talent” by the Executive Directors at Aalborg University in 2017.


English Summary
7
ENGLISH SUMMARY The Osteoarthritis Research International (OARSI) provides clinical guidelines for the treat-ment of pain in osteoarthritis, and some of the most utilized treatments are Non-Steroidal Anti-Inflammatory Drug (NSAID) plus paracetamol and total joint arthroplasty. Most patients will benefit from these treatments, but some patients are less responsive or showing unwant-ed side effects, and selecting the right patients for the most optimal treatment would further highlight the opportunities of personalize pain medicine. Quantitative sensory testing (QST) of patients with OA includes measures of widespread pressure hyperalgesia (assessed by pres-sure pain thresholds, PPTs), temporal summation of pain (TSP), and conditioned pain modu-lation (CPM). The current dissertation has focus on how assessment of central pain pathways using QST prior to treatment can predict pain and pain reduction after treatment.
The studies presented here found associations between preoperative widespread hyperal-gesia (paper 2), facilitated TSP (paper 1, 3, and 4), and impaired CPM (paper 5) and chron-ic postoperative pain in patients with painful osteoarthritis after total joint arthroplasty. In addition, pre-treatment facilitated TSP was associated with limited analgesic response to 4 weeks of COX-2 inhibitors (paper 6) and 3-weeks of NSAIDs plus paracetamol (paper 7). Finally, impaired CPM was associated to limited analgesic response of 3 weeks of NSAIDs plus par-acetamol (paper 8).
A systematic review on all studies related to QST, chronic postoperative pain, and responses to pharmacological interventions is included in this dissertation (paper 9), which highlights that pressure pain stimuli, TSP, and CPM were the most frequently assessed QST modalities, and TSP (50%) and CPM (approx. 44%) were most frequently associated with chronic postop-erative pain or response to pharmacological treatments.
Conclusively, these studies (paper 1-8) demonstrate that patients with a pro-nociceptive sen-sory profile might respond poorly to the standard OA pain treatment as recommended by OARSI, and the systematic review (paper 9) might indicate that this information is useful in other painful disorders than osteoarthritis.


Dansk resume
9
DANSK RESUME Osteoarthritis Research International (OARSI) er et international forbund, som giver guide-lines til behandling af patienter med slidgigt. Nogle af de meste anvendte behandlinger er Non-Steroidal Anti-Inflammatory Drug (NSAID) plus paracetamol og total led alloplastik (TLA). Det er påvist, at mange patienter vil have god gavn af disse behandlinger Dog vides det, at nogle patienter responderer dårligere og/eller har mange bivirkninger, hvorfor selektion af den rigtige patient til den korrekte behandling vil være fordelagtig og promoverer konceptet ”Personlig Medicin”. Kvantitativ sensorisk testning (QST) kan anvendes til at smerteprofilere patienter med slidgigt, og her benyttes ofte mål for udbredt tryksmerteoverfølsomhed, (som måles ved hjælp af tryksmertetærskler, PPT), temporal summation (TSP) og konditioneren-de smertemodulation (CPM). Denne afhandling beskriver studier, som har anvendt QST før standard-smertebehandling til at forudsige smerter eller smertereduktion efter behandling.
Afhandlingen beskriver, at præoperativt udbredt tryksmerteoverfølsomhed (artikel 2), øget TSP (artikel 1, 3 og 4) og nedsat CPM (artikel 5) er associeret til kroniske postoperative smerter efter TLA. Ligeledes findes det, at øget TSP før behandling er associeret til manglende analge-sisk respons efter 4-ugers behandling med COX-2-hæmmer (artikel 6) og 3-ugers behandling med NSAIDs plus paracetamol (artikel 7). Slutteligt vises det, at nedsat CPM før behandling er associeret med begrænset analgesisk respons af 3-ugers behandling med NSAIDs plus par-acetamol (artikel 8).
Denne afhandling indeholder et systematisk review over alle studier, som anvender QST og undersøger kroniske postoperative smerter eller analgesisk respons til længerevarende farma-kologiske behandlinger (artikel 9), hvori det findes, at PPT, TSP og CPM er meget ofte brugte målemetoder, og TSP (50%) og CPM (ca. 44%) målt før behandlingsstart ofte er associeret til kroniske postoperative smerter eller analgesisk respons af farmakologiske behandlinger.
Denne afhandling konkluderer, at smerteoverfølsomme patienter med slidgigt er fundet as-socieret med dårligere behandlingsrespons til standard slidgigtsbehandling, som er anbefalet af OARSI (artikel 1-8). Det systematisk review kan indikere, at disse fund ikke kun er gældende for patienter med slidgigt, men vil kunne anvendes for andre smertefulde patientgrupper (artikel 9).


11
CONTENTSEnglish Summary 7
Dansk resume 9
Acknowledgement 13
Preface: The Conceptual Frame for this Dissertation 17
List of Papers 19
1. Setting the Scene: Chronic Pain as a Major Clinic Problem 21 1.1 Defining Chronic Pain and Cut-off Points for the Treatment of Pain 21 1.2 The Development of Chronic Pain 21
2. Osteoarthritis is a Major Clinical World-wide Issue 23 2.1 Pain in the Osteoarthritic Joint 23 2.2 Osteoarthritis as a Localized Joint Problem 24 2.3 Osteoarthritis as a Widespread Pain Problem 24 2.4 Osteoarthritis as a Multi-Comorbidity Disease 25 2.5 Recommended Treatments for Painful Osteoarthritis 26 2.6 The Focus of the Current Dissertation 28
3. Personalized Pain Medicine 29 3.1 Predictors for Poor Response to Standard Therapies for 29 Painful Osteoarthritis
4. Profiling Using Quantitative Sensory Testing (QST) 31 4.1 Localized and Widespread Hyperalgesia 31 4.2 Sensitization of Central Pain Mechanisms 32 4.3 Descending Pain Inhibitory Control 33
5. Mechanistic Pain Profiling of Patients with Osteoarthritis 35 5.1 Discussion of the Papers Included in this Dissertation 37
6. General Discussion 43 6.1 The Predictive Value of QST Profiling in Osteoarthritis 43 6.2 “We Only Have Time to Do One Test – Which One Should It Be?” 44 6.3 Methodological Considerations 45
7. Conclusion 47
8. The Future: Development of the Concept “Personalized Mechanistic 49 Pain Medicine”
References 51

Acknowledgement
13
ACKNOWLEDGEMENTWhere to start …?!?
Lars Arendt-Nielsen has been my mentor for the last years. We have discussed research but more importantly, we have discussed strategies for research, how I could position myself in the research arena and how to advance a scientific area. Lars is not only my mentor but also a friend and his continued support and trust in my work has been fundamental for my career.
I have my deepest respect for my co-authors, who have been vital for the many projects presented in this. I am grateful for the strong interdisciplinary collaboration between Center for Sensory-Motor Interaction (SMI), Center for Neuroplasticity and Pain (CNAP) and the Department of Orthopedic Surgery, Aalborg University Hospital. Ole Simonsen and Mogens Berg have been my clinical supervisors within osteoarthritis and their continued motiva-tion, experience and dedication to drive this field forward have been essential for this work. Director and Professor Thomas Graven-Nielsen is head of CNAP and the group for Pain and Motor System Plasticity and have often challenged my views, which is greatly appreciated and have made the work stronger. Professor Anne Estrup Olesen and I have worked together on several project and Anne introduced me to the (somewhat tedious) world of Good Clinical Practice (GCP), which has been fundamental for my research career. Masashi Izumi came to Denmark when I was a young PhD student and together we conducted some interesting studies, learned from each other and had a lot of fun!. Dennis Boye Larsen joined me as a postdoc in 2018 with a mindset to work hard and push forward and together we completed an immense amount of projects, manuscripts and reviews within a very short time (watch out for Dennis in the future!!). Thank you to my co-biomedical engineer Line Lindhardt Egsgaard who conducted the many projects at CCBR and who provided me with written support for this dissertation despite just given birth (much respect and love from Aalborg). Carsten Dahl Mørch was my teacher during my bachelor education, my opponent at my PhD defense and I am now proud to call him my collaborator. I visited Robert R Edwards in Boston in 2015 to understand the impact of pain catastrophizing on pain and later Rob have provided me with help for funding applications, international visits and new project ideas – thank you Rob (I think the next beer is on me). I joined Professor Brigitte Scammell at University of Nottingham in 2016 and together with Lars Arendt-Nielsen and Thomas Graven-Nielsen, we have conduct-ed a lot of studies on patients with osteoarthritis and Brigitte was fundamental for my Talent Management Programme – thank you to Brigitte and the team (Tom Kurien, William Cottam, Sarina Jennifer Iwabuchi and Dorothee Auer) at the Academic Orthopaedics, University of Nottingham. Professor Audun Stubhaug, University of Oslo provided me with much needed support for my research and critical revisions of my funding applications and manuscripts. Professor Andre Wolff, University Medical Center Groningen reached out to us in 2017 and in 2018 I drove through a blizzard in Germany to reach the Netherlands and to set up a new collaboration – the team (Hans Timmerman and Ingrid Schuttert) at University Medical Center Groningen are dedicate hard working people who needs acknowledgement and I look forward to continue our collaboration in the future. In 2013, I witnessed that Professor Olive Wilder-Smith defended his doctoral dissertation at Aalborg University and from that moment I knew that I would committee my life to research on pain mechanisms – I am very humbled that I was allowed to publish a paper with Professor Wilder-Smith before his retirement. To my friend, collaborator and side-kick at countless international bars Associate Professor Henrik Bjarke

Mechanistic Pain Profiling of Patients with Osteoarthritis
14
Vægter, University of Southern Denmark: I think that you were the right kind of company for a visit to a Michelin stared restaurant in Florence.
Projects of the magnitude as presented in this dissertation are not possible without technical personal and I have been fortunate to work with the best! Susanne Nielsen Lundis was head the SMI secretary for years and now runs the Research Administrative Team at the Department of Health Science and Technology. Susanne holds the world record for reading most of my work, since she has tirelessly reviewed and proof-read manuscripts, funding applications and statements for the last 10 years. In addition, Susanne has tremendous knowledge on leader-ship and implementation of a good research structure, which have been vital for me within the last few years when attempting to establish a research group.
Lone Schødt Andersen has provided me with the structure and support needed to conduct multiple large scale projects in parallel. Lone has a keen expertise for writing protocols for the ethical committee, organizing material and keeping a log of all important documents and dates, which I have never found matched in any of my national or international collaborations. The work done by Lone has allowed me to focus on research instead of administration and this has been fundamental for my ability to grow as a researcher.
Project Nurse Ulla Hornum, Project Nurse Gitte Broholm Hansen and Research Secretary Heidi Ladefoged Poulsen have ensured the structure for all of the research conducted at Aalborg University Hospital, Farsø. I am in-depth to your hard work and for taking great care of Masashi Izumi when he conducted his trials with us.
Project Nurse Tina Lyngholm Jensen joined our research team in 2015 and was the main co-ordinator for the studies conducted at Aalborg University Hospital. Working together with Ole Simonsen and myself can be tough and sometimes a little chaotic but Tina always made sure that everything was conducting properly and thereby ensured the completion of many projects.
Section Leader for the Medical Laboratory Technologists Tina Beith Christensen was my first project coordinator when I initiated my studies at the Regional Hospital in Frederikshavn in 2011. Tina is an incredible leader and she managed to organize staff, patients, surgical plan and pain testing in an impressive manner, which ensured the completion of a lot project within a short duration of time. I still refer to Tina as my best project coordinator to date!
I have worked together with Poul Pedersen (formally at Cortex Technology) for nearly a dec-ade and together we have optimized the cuff algometer from an idea to a device, which is now implemented in more than 20 international research projects. Poul has tirelessly implemented and adjusted the machines, so that it fit the needs for many of the studies included in this dis-sertation. The work presented here would never have been possible without Poul Pedersen. I would like to thank the Department of Health Science and Technology and at the Department of Clinical Medicine at Aalborg University for providing an inspiring environment for conduct-ing research. More importantly, I am truly grateful for the interactions with my coworkers and students, which have made this journey exciting and wanted me to go back for more every day.

Acknowledgement
15
The Danish Rheumatism Association, The Bevica foundation, the Danish Advanced Technology Foundation, the Danish Council for Technology and Innovation, Danish Ministry of Higher Education and Science, The Innovation Fund Denmark, Merck (unrestricted grant), The Shionogi Science Program, the TaNeDS Europe grant and The Aalborg University Talent Management Programme are kindly acknowledged for the support needed to complete the work. In addi-tion, Center for Neuroplasticity and Pain (CNAP) is kindly acknowledged for providing me with additional research time to finalize this dissertation.
Thank you to my family Naja, Viktor and Gunilla for allowing me to pursue my dream and for providing me with the much needed support for conducting this work.

Preface: The Conceptual Frame for this Dissertation
17
PREFACE: THE CONCEPTUAL FRAME FOR THIS DISSERTATIONThe aim of this thesis is to explore a basis for “Personalized Mechanistic Pain Profiling” using quantitative sensory testing with the vision of generating new knowledge to be used for fur-ther developing the concept of personalized management of painful osteoarthritis in a vali-dated evidence-based and safe manner.
The hypothesis was that patients with osteoarthritis and a higher level of pain sensitivity might be characterized as a group of patients with more complex pain, and therefore these patients might respond less positively to standard osteoarthritic treatment such as total joint arthroplasty and NSAIDs plus paracetamol.
This dissertation consists of work demonstrating how quantitative sensory testing might act as a predictive “biomarker” for standard pain treatment (pharmacological and surgical inter-ventions) of patients with osteoarthritis. To further pursue the vision, studies must be able to demonstrate that e.g., modulating specific mechanisms or specific preoperative pain pro-files can improve the patients’ outcomes or that certain patients can be selected for more appropriate pain care. The current dissertation will not provide the complete evidence for the fulfilment of the goal to describe the concept for implementation of personalized, mech-anistic pain management of painful osteoarthritis, but highlight novel findings to additionally update the discussion on the further progress of the field of personalized pain management.
Kristian Kjær Petersen18 December 2020, Aalborg
List of Papers
19
LIST OF PAPERSThis dissertation is partly based on the following 9 peer-reviewed papers:
1. Petersen KK, Arendt-Nielsen L, Simonsen O, Wilder-Smith O, Laursen MB. Presurgical assessment of temporal summation of pain predicts the development of chronic post-operative pain 12 months after total knee replacement. Pain. 2015;156(1):55–61
2. Petersen KK, Graven-Nielsen T, Simonsen O, Laursen MB, Arendt-Nielsen L. Preoperative pain mechanisms assessed by cuff algometry are associated with chronic postoperative pain relief after total knee replacement. Pain. 2016;157(7):1400–6.
3. Izumi M, Petersen KK, Laursen MB, Arendt-Nielsen L, Graven-Nielsen T. Facilitated tem-poral summation of pain correlates with clinical pain intensity after hip arthroplasty. Pain. 2017;158(2):323-332.
4. Petersen KK, Simonsen O, Laursen MB, Arendt-Nielsen L. The Role of Preoperative Radiologic Severity, Sensory Testing, and Temporal Summation on Chronic Postoperative Pain Following Total Knee Arthroplasty. Clinical Journal of Pain. 2018;34(3):193–7.
5. Larsen DB, Laursen M, Edwards RR, Simonsen O, Arendt-Nielsen L, Petersen KK. Mechanistic pain profiling and pain catastrophizing are valuable factors for predicting postoperative chronic pain. Pain Medicine, Accepted: October 9 2020.
6. Arendt-Nielsen L, Egsgaard LL, Petersen KK. Evidence for a central mode of action for etoricoxib (COX-2 inhibitor) in patients with painful knee osteoarthritis. Pain. 2016;157(8):1634–44.
7. Petersen KK, Olesen AE, Simonsen O, Arendt-Nielsen L. Mechanistic pain profiling as a tool to predict the efficacy of 3-weeks non-steroidal anti-inflammatory drugs (NSAIDs) plus paracetamol in patients with painful knee osteoarthritis. Pain. 2019;160(2):486-492.
8. Petersen KK, Simonsen O, Olesen AE, Mørch CD, Arendt-Nielsen L. Pain inhibitory mech-anisms and response to weak analgesics in patients with knee osteoarthritis. European Journal of Pain. 2019;23(10):1904-1912.
9. Petersen KK, Vaegter HB, Stubhaug A, Wolff A, Arendt-Nielsen L, Larsen DB. The Predictive Value of Quantitative Sensory Testing – A Systematic Review on Chronic Postoperative Pain and the Analgesic Effect of Pharmaceutical Treatments for Chronic Pain Patients. Pain. 2020, electronic publication ahead of print.

21
1. Setting the Scene: Chronic Pain as a Major Clinic Problem
1. SETTING THE SCENE: CHRONIC PAIN AS A MAJOR CLINIC PROBLEM
Chronic pain is estimated to affect approx. 20% of the world’s population [33,69,83] with low back and neck pain being the most prevalent diseases [227], and generally musculoskeletal disorders are representing 2/3 of all cases of chronic pain .
In the US, the economic consequence of chronic pain, including treatments and low worker productivity, is estimated to be between $560 and $635 billion per year [66]. Surprisingly, the economic burden of chronic pain is higher in the US than other commonly well-known clinical problems such as diabetes, heart diseases, and cancer [66].
1.1 DEFINING CHRONIC PAIN AND CUT-OFF POINTS FOR THE TREATMENT OF PAIN
Acute pain is an essential protective mechanism, which main purpose is to alert the brain about injury and thereby preventing further damage. On the other hand, chronic pain has been defined as being pain, which persists past the normal time of healing [31]. It is important to realize, however, that some injuries do require healing and regrowth before the organism is fully functional [138]. For research purposes, the IASP Task Force on Taxonomy suggested that chronic non-malignant pain should be defined as pain for more than six months, and chronic pain after surgery is defined as pain persisting more than three months after surgery [138].
It is important to evaluate clinical relevant cut-off points when studying the treatment of chronic pain. As an example, it is commonly debated if the clinical cut-off value for an effective pain pharmaceutical treatment is either a 30% or 50% reduction in pain intensities. Another example could be that the common goal of pain treatment is to reduce the pain to a mild in-tensity level (e.g., less than 30 mm on a 100 mm visual analogue scale, VAS), and therefore, effective treatments could be categorized if the patient is reporting less than 30 mm on the VAS by the end of the treatment. Finally, more complicated clinical cut-off points have been established, which rely on a combination of e.g., reduction in pain, improvement in function, and improvement in quality of life [171].Due to this ongoing debate, a range of different cut-off points for the evaluation of pain treatments are being used, and the work carried out in this dissertation is no exception. Multiple cut-off points have been utilized in this work to ex-plore if measures of pain sensitive can predict poor response to the standard pain treatments.
In most pain trials, pain has been selected as the primary outcome parameter. Often trials do not reach the outcome as sometimes the selected pain parameter may not be significantly affected, but the patients’ function and quality of life has been improved suggesting clinical studies in particular on musculoskeletal pain should include measures for function and qual-ity of life.
1.2 THE DEVELOPMENT OF CHRONIC PAINCurrently, it is unknown why some patients develop chronic pain, and one reason for this could be that chronic pain is an umbrella term for multiple different conditions. The IASP Task Force

for Classification of Pain Diseases (ICD-11 development of pain codes) divides chronic pain into seven different disorders [222]: 1) chronic primary pain, 2) chronic cancer pain, 3) chron-ic posttraumatic and postsurgical pain, 4) chronic neuropathic pain, 5) chronic headache and orofacial pain, 6) chronic visceral pain, and 7) chronic musculoskeletal pain.
The studies discussed in this dissertation will focus on the chronic musculoskeletal pain con-dition: “osteoarthritis”, and therefore, the results from these studies may not necessarily be transferable to six other chronic pain disorders. When suited, the author will describe links to other disorders to inform the reader of the similarities and to broaden the perspective of the findings presented here.
The focus of this work has been to describe and provide emerging evidence for the predictive value of central pain mechanisms for standard pain treatment of patients with osteoarthritis (OA).
2. Osteoarthritis is a Major Clinical World-wide Issue
23
2. OSTEOARTHRITIS IS A MAJOR CLINICAL WORLD-WIDE ISSUE
OA is characterized by cartilage degeneration, joint stiffness, and pain. Cartilage degeneration is traditionally assessed using x-ray, and the radiological assessment of OA is often found using the Kellgren & Lawrence scale [101]. The global burden of disease studies estimate the world age-standardized prevalence of OA to be 3,754 per 100,000 capita with North America (prev-alence of 5,924 per 100,000 capita), North Africa and the Middle East (prevalence of 4,610 per 100,000 capita), and Australia (prevalence of 4,595 per 100,000 capita) demonstrating the highest regional prevalence and expected to increase in future [198]. The prevalence of OA increases with age [25], and people in Europe, the United States, and other developed countries tend to live longer [28,61], which could explain part of the reason for the increas-ing prevalence of OA.
Obesity is one of the world leading health care issues [216], and models predict that global level of obesity will continue to rise although many health care systems aim to prevent this [97]. Obesity is linked with development and fast progression of OA in weight- and non-weight-bearing joints [185], and it is assumed that this increase in global obesity will affect the prevalence of OA in future.
Projection studies expect a rise in the prevalence of total joint replacement surgeries [3,116]. Kurtz et al. 2007 [116] predicted a six fold increase in total knee arthroplasties from 2005 to 2030 in the US. A more recent study from Australia concludes that “Australia faces an unsus-tainable joint replacement burden by 2030, with significant healthcare budget and health workforce implications” [3], which emphasizes that OA is as a major clinical issue in the mod-ern world.
2.1 PAIN IN THE OSTEOARTHRITIC JOINT The IASP 2009 Global Year against Musculoskeletal Pain, IASP 2016 Global Year against Pain in the Joints, and the 2017 Global Year against Pain after Surgery highlight the international awareness on musculoskeletal pain, joint pain, and postoperative pain as are also the focus of this thesis.
As OA is characterized as a cartilage degenerative disease, it would be natural to assume that cartilage degeneration is directly associated with pain, but studies finds no or limited associa-tion between the radiological assessment of cartilage degeneration and pain in OA [47,60,85]. This suggests that other factors than cartilage generation are important for OA pain [15]. Multiple factors have been found associated with OA pain, and in general, these can be di-vided into factors directly associated with OA affected joint or other factors. An overview of potential factors associated with OA pain is found in figure 1 [13,16,68,117,162].

Mechanistic Pain Profiling of Patients with Osteoarthritis
24
Figure 1: Factors associated with pain in osteoarthritis (OA) [13,16,68,116,162]. The current thesis mainly focuses on the contribution of sensitization of central pain mechanisms, and it is important to mention that this is one of many factors associated to OA pain.
2.2 OSTEOARTHRITIS AS A LOCALIZED JOINT PROBLEM Nociceptors (pain receptors) produce action potentials when activated, which travel through the nerve system to the brain where it is categorized as pain [136]. The synovium membrane, the Hoffa’s fat pad, and the subchondral bone are highly innervated by nociceptors whereas under normal conditions, cartilage is minimally innervated [60,74], which could explain the lack of association between cartilage degeneration and pain in OA. In addition, nociceptors are found in muscles, tendons, and ligaments surrounding the joint, and these can all give rise to pain [60]. Treatments such as inter-articular injections target a potential inflammation within the joint, and this is successful when used sparely, but not advised to be used often due to further risk of cartilage degeneration [135]. Similar total joint arthroplasty is considered a treatment targeting OA as a localized problem, and this is very effective since up to 80% of patients are satisfied with the procedure [144,168].
2.3 OSTEOARTHRITIS AS A WIDESPREAD PAIN PROBLEM Referred pain to the knee joint is often observed in patients with hip OA, and referred pain does often follow a segmental spread [75]. Experimental pain models can produce referred muscle pain areas where the development of referred muscle pain area is delayed compared with the local painful muscle stimuli [78,118], and the referred muscle pain area decreases as the local painful muscle stimuli are reduced [77]. Therefore, the manifestation of referred
2. Osteoarthritis is a Major ClinicalWorld-wide Issue
25
muscle pain areas has been suggested to be a result of central segmental pain mechanisms [75], and these are often facilitated in patients with OA [15], which could be one of the rea-sons for the widespread pain often observed in OA. Studies have shown that widespread pressure hyperalgesia decreases in patients with hip [113] and knee [81] OA undergoing TJA indicating that referred pain sensitization areas can be normalized if OA is the primary source of pain. Patients with chronic postoperative pain following TJA seem to have a worsening of widespread pressure hyperalgesia [206,207], which might indicate that this specific subgroup of patients does not only have a localized painful joint problem, but it is also complex.
Widespread pressure hyperalgesia is widely reported in patients with severe OA compared with healthy subjects [11,15], and widespread pressure hyperalgesia seems to be associated with increased clinical pain ratings [9,12].
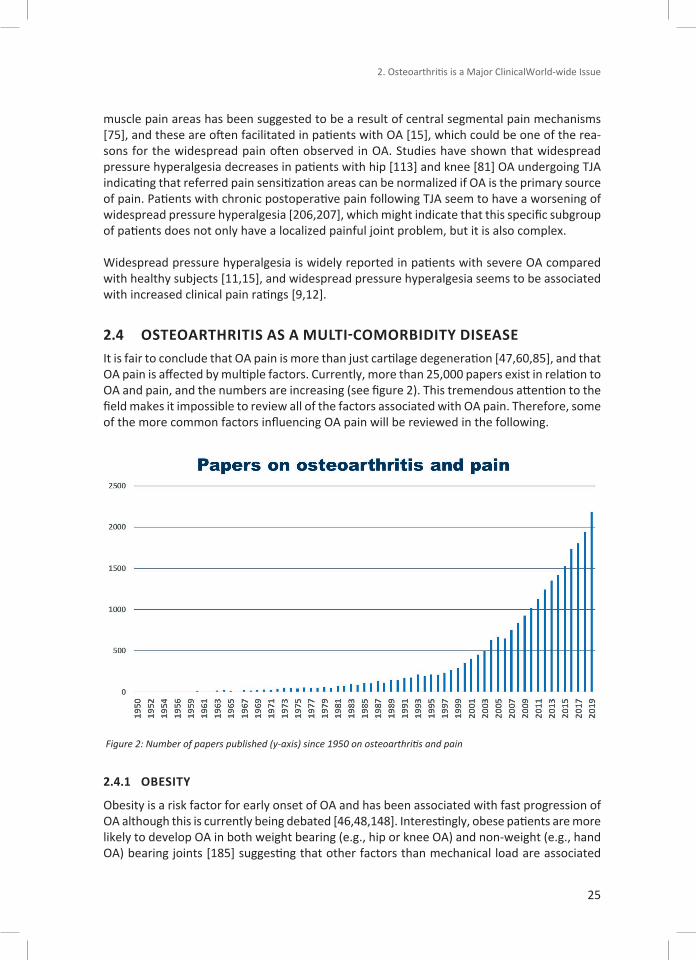
2.4 OSTEOARTHRITIS AS A MULTI-COMORBIDITY DISEASE It is fair to conclude that OA pain is more than just cartilage degeneration [47,60,85], and that OA pain is affected by multiple factors. Currently, more than 25,000 papers exist in relation to OA and pain, and the numbers are increasing (see figure 2). This tremendous attention to the field makes it impossible to review all of the factors associated with OA pain. Therefore, some of the more common factors influencing OA pain will be reviewed in the following.
Figure 2: Number of papers published (y-axis) since 1950 on osteoarthritis and pain
2.4.1 OBESITY
Obesity is a risk factor for early onset of OA and has been associated with fast progression of OA although this is currently being debated [46,48,148]. Interestingly, obese patients are more likely to develop OA in both weight bearing (e.g., hip or knee OA) and non-weight (e.g., hand OA) bearing joints [185] suggesting that other factors than mechanical load are associated
Mechanistic Pain Profiling of Patients with Osteoarthritis
26
with the OA development. A possible explanation is that obesity leads to chronic low-grade inflammation, which has been associated with cartilage degeneration [89,193].
2.4.2 CHRONIC LOW-GRADE INFLAMMATIONTraditionally, OA is considered a non-inflammatory disease when compared with other forms of arthritis (e.g. rheumatoid arthritis). Various subgroups of OA patients can be categorized with different low-grade systemic inflammatory profiles [202]. It is well-known that syno-vitis (inflammation of the synovial membrane) is present in more than 50% of knee OA pa-tients [92], and synovitis is associated with OA pain [59,92]. Preclinical studies have shown that pro-inflammatory cytokines sensitize the peripheral nerves [200]. Pro-inflammatory cy-tokines such as interleukin-1β (IL-1β), IL-6, and tumor necrosis factor alpha (TNF-α) have been found upregulated in synovial fluid in OA patients and associated with increased pain reports [59,65]. Localized pressure hyperalgesia is a common finding in severe OA when compared with healthy subjects [15], and inflammatory processes are most likely one of the reasons for this localized hyperalgesia.
Systemic upregulation of inflammatory markers has been detected in a subgroup of severe knee OA patients [202]. Severe knee OA is associated with widespread hyperalgesia [15], but it is currently unknown if this is due to low-grade systemic inflammation. Epidemiological studies have found that low-grade inflammation is associated with increases pain sensitivity [94,201], and therefore inflammation should be considered as an important factor when as-sessing patients with OA pain.
2.4.3 COGNITIVE FACTORSHigher clinical pain levels in OA have been associated with high levels of pain catastrophizing [30,153,205,212], fear of movement [205], pain self-efficacy [205], anxiety [84,205], and de-pression [84]. Studies focusing on training of pain copying skills have found these effective for managing OA pain [34,211] suggesting that targeting cognitive pain-related beliefs might be an option for non-surgical and non-pharmacological treatment of OA pain. Duloxetine (a ser-otonin and norepinephrine reuptake inhibitor) is approved for the treatment of depression, but studies have shown pain relieving effects when administrated to patients with knee OA [229]. Duloxetine might target a subgroup of OA patients with depression, and alternative-ly, emerging evidence suggests that duloxetine can restore losses in pain inhibitory control [241], which is often impaired in patients with severe OA [15]. This is further supported by the 2019 OARSI guideline, in which duloxetine is conditionally recommended for OA patients with widespread pain and/or depression [21]. Unfortunately, the number needed to treat (NNT) for duloxetine is 7, which could suggest that only a subgroup of patients with knee OA will benefit from duloxetine [40].
2.5 RECOMMENDED TREATMENTS FOR PAINFUL OSTEOARTHRITIS No treatment is currently available to cure OA, and therefore treatment of OA is focused on alleviating pain, improving joint function, and increasing quality of life. “Regenerative medi-cine” has been proposed as a cure for OA focusing on intra articular injections or bone marrow migration of stem cells, aiming to repair the damaged cartilage, but currently no implement-ed treatment has been developed. Being a fascinating area of research, however, the current thesis will not focus on regenerative medicine for OA due to the high risk of bias [160].

2. Osteoarthritis is a Major ClinicalWorld-wide Issue
27
Instead, it will focus on some of the treatments recommended by the Osteoarthritis Research International (OARSI), which can be divided into non-surgical and surgical therapies. They will be briefly reviewed below.
2.5.1 NON-SURGICAL TREATMENT OF OSTEOARTHRITISNon-surgical treatment of OA consists of multiple pharmacological and non-pharmacological options [21,208,228]. The 2019 OARSI guidelines on non-surgical management of knee OA strongly recommend arthritis education, land-based exercise programs, and weight manage-ment if needed [21]. In addition, the 2019 OARSI guidelines strongly endorse the use of topical NSAIDs and conditionally (with high consensus) recommend oral non-selective NSAIDs and COX-2 inhibitors [21]. Intra-articular corticosteroids are conditionally recommended (with low consensus), and this is not included in the current dissertation since recent studies suggest limited pain relief and risk of cartilage damage due to multiple injections of corticosteroids compared with injections of saline [135]. Further, there is ongoing discussion whether the effect is due to hyaluronic acid or the corticosteroids itself [181].
This dissertation will focus on non-surgical treatments with COX-2 inhibitors and non-selective NSIADs as these are very commonly used for OA treatments and considered effective [90,100].
2.5.1.1 SELECTIVE AND NON-SELECTIVE NSAIDSThe analgesic effect of NSAIDs has been widely documented [90,100] even though the mech-anisms of action are not completely understood [71]. It is known that NSAIDs (and paraceta-mol) inhibit the synthesis of prostaglandins through modulation of cyclooxygenase (COX). A preclinical studies have found that non-selective NSAIDs and paracetamol increase the activity of the cannabinoid system [4], and that the effect of NSAIDs and selective COX-2 inhibitors dependents on an intact serotonin system [71]. In addition, human studies suggests that COX-2 inhibitors can modulate widespread hyperalgesia [8,128,183], which further suggests that COX-2 inhibitors act on the central pain pathways.
It is important to highlight that long-term use of NSAID is potentially harmful [128], and there-fore NSAIDs should be used effectively with short duration (weeks). NSAIDs should be ad-ministrated in combination with paracetamol as the combination yields a larger effect in OA than each of the drugs alone [156]. It seems that the most optimal paradigm for OA pain is 1 g paracetamol and 400 mg Ibuprofen three times daily (a total of 3 g paracetamol and 1.2 g ibuprofen daily). This yields an analgesic effect with limited adverse events [49].
2.5.2 SURGICAL TREATMENT OF OSTEOARTHRITISSeveral surgical procedures are performed for OA with the most common ones being arthro-scopic surgery and total joint arthroplasty (TJA) [244]. The current thesis will not focus on arthroscopy surgery as the long-term pain relieving evidence supporting this procedure has been questioned in the last decade when compared with other standard treatments for OA pain [70,104,172,220]. Instead, this thesis will focus on TJA, and the rational will be discussed below.

Mechanistic Pain Profiling of Patients with Osteoarthritis
28
2.5.2.1 TOTAL JOINT ARTHROPLASTYTJA might seem to be the ideal treatment if OA was a purely localized pain disorder as the dam-aged joint is replaced by a prosthesis and thereby eliminates the peripheral pain driver. TJA is a frequently performed procedure [37], and patients ongoing TJA have better improvements in pain, function, and quality of life compared with patients receiving non-surgical treatment [209]. It is problematic, however, that 20% of TKA and 10% of THA patients experience chronic postoperative pain [26]. The primary clinical indication for TKA and THA is OA (94-97% of cas-es) [192]. The number of THA and TKA are increasing worldwide [2,42,105,116,203,204]. The number of Danish TKA and THA seem to have stabilized in the last few years as also stated in the Danish Knee [151] and Hip [157] Arthroplasty Registry yearly reports, but the most recent report seems to indicate an increase in 2018 compared with previous years [152].
2.6 THE FOCUS OF THE CURRENT DISSERTATIONThe focus on this dissertation will be on TJAs and NSAIDs as they are standard treatments which are widely used for OA pain, but it seems evident that some patients respond better to these treatments than others. This dissertation will aim to identify patients who are poor responders to these standard OA treatments.

3. Personalized Pain Medicine
29
3. PERSONALIZED PAIN MEDICINE “Personalized medicine” or “precision medicine” aims to provide the correct treatment to the right patient. Currently, personalized medicine is mainly developed within cancer [41,50,121,123], but the concept might also apply to pain medicine.
Management of pain is difficult, and therefore many treatment diagnostic algorithms have been developed to target different chronic pain patient groups. Many of these algorithms are based around a “trial and error”-concept where patients are introduced to many phar-maceutical treatments before the correct one is found. This process is lengthy, potentially harmful due to side effects, costly, and very ineffective. The concept of “Personalized Pain Medicine” revolves around assessing the underlying mechanisms for pain and treating these mechanisms. Advanced treatment options exist today, but assessment of pain is still lacking, and the clinical use is limited.
This dissertation aims to exemplify how sensory profiles using QST may be used to predict re-sponses to standard OA therapies for patients with OA and to investigate if this concept can be used in a different chronic pain population.
3.1 PREDICTORS FOR POOR RESPONSE TO STANDARD THERAPIES FOR PAINFUL OSTEOARTHRITIS
This dissertation is focused on the possible predictive value of sensory profiles for treatment responses to surgery and pharmacological interventions, but it is important to underline that multiple other factors are currently being utilized to predict poor outcome after standard therapies for painful OA. These factors are briefly discussed below.
3.1.1 PAIN CATASTROPHIZINGHigh levels of pain catastrophizing has been suggested to be a predictor for chronic postopera-tive pain following TKA [64,188,190]. Pain catastrophizing can be reduced [187], and therefore studies have aimed to reduce preoperative levels of pain catastrophizing to reduce chronic postoperative pain. Two recent studies were able to reduce preoperative levels of pain cat-astrophizing, but unable to see effects of chronic postoperative pain scores when compared with patients receiving usual care [29,189]. Similar, modulating pain catastrophizing prior to exercise therapy does not improve the pain relieving effect of exercise therapy in patients with hip OA [24]. These findings could suggest that pain catastrophizing might be a predictor of poor outcome after therapy for patients with OA, but that modulating pain catastrophizing might not improve the treatment outcome.
3.1.2 EPIGENETICS Micro and long non-coding RNAs (miRNA and lnRNA, respectively) are, among others tasks, responsible for regulation of the inflammatory cascades [213], and therefore epigenetics is a new and interesting avenue for pain research. A recent proof-of-concept study demonstrated that upregulation of preoperative miRNA-146a-5p combined with high preoperative pain pre-dicted postoperative pain relief following TKA [67]. A previous study [119] found differences in miRNA-146a comparing painless and painful peripheral neuropathies, and multiple other studies have associated miRNAs with pain in patients with e.g., osteoarthritis [27], rheumatoid

Mechanistic Pain Profiling of Patients with Osteoarthritis
30
arthritis [39], or migraine [5]. Combined, this research might indicate that epigenetics could act as predictive biomarkers in the future, but further research is needed to clarify this.
3.1.3 SENSORY PROFILESSensory profiles based on QST have previously been used to predict chronic postoperative pain following e.g., thoracic surgery [240], groin hernia repair surgery [1] and abdominal sur-gery [234] or the analgesic effect of e.g. duloxetine in patients with diabetic neuropathy [241] or migraine [107], pregabalin in patients with painful chronic pancreatitis [154], or to classify patients with peripheral neuropathy as responders to oxcarbazepine [45].
Prior to the work described in this dissertation, three studies were published on the use of QST as predictors in patients with OA with two studies finding that preoperative 1) electrical pain thresholds [124] and 2) widespread pressure hyperalgesia [235] were associated with chronic postoperative pain following TKA. In addition, Martinez et al., 2007 [132] studied pre-operative allodynia, mechanical pain thresholds, heat pain thresholds, and cold pain thresh-olds in 20 patients with knee OA and found no predictive value of these assessment to post-operative pain at four months follow-up. The following sections will address how to assess sensory profiles using QST in OA and the current evidence on profiles in patients compared with healthy subjects.
4. Profiling Using Quantitative Sensory Testing (QST)
31
4. PROFILING USING QUANTITATIVE SENSORY TESTING (QST)
QST is neurological examination of somatosensory function, and multiple standardized pro-tocols exists [52,195,233]. The most comprehensive and most widely used protocol is the German Research Network on Neuropathic Pain (DFNS) protocol for neuropathic pain [195], which includes seven tests focused on thermal and mechanic detection and pain thresholds, allodynia, and wind-up with an assessment time of approx. 60-90 minutes.
While thermal hyperalgesia and hypoesthesia have been reported in OA when compared with healthy subjects [96,106,114,142], it is commonly accepted that deep structures are more affected by pain sensitivity in musculoskeletal pain [62,129], and therefore pressure stimuli are often utilized [15,76]. Severe OA is commonly associated with localized and widespread pressure hyperalgesia, facilitated temporal summation of pain (TSP), and impaired conditioned pain modulation (CPM) [15]. It is important to note, however, that while patients and healthy subjects are different on group levels, some patients are less pain sensitive than others [164], and this variability might be useful in the prediction of pain after standard OA treatments. The following sections will discuss the pain mechanisms and assessment of localized and wide-spread pressure hyperalgesia, TSP, and CPM.
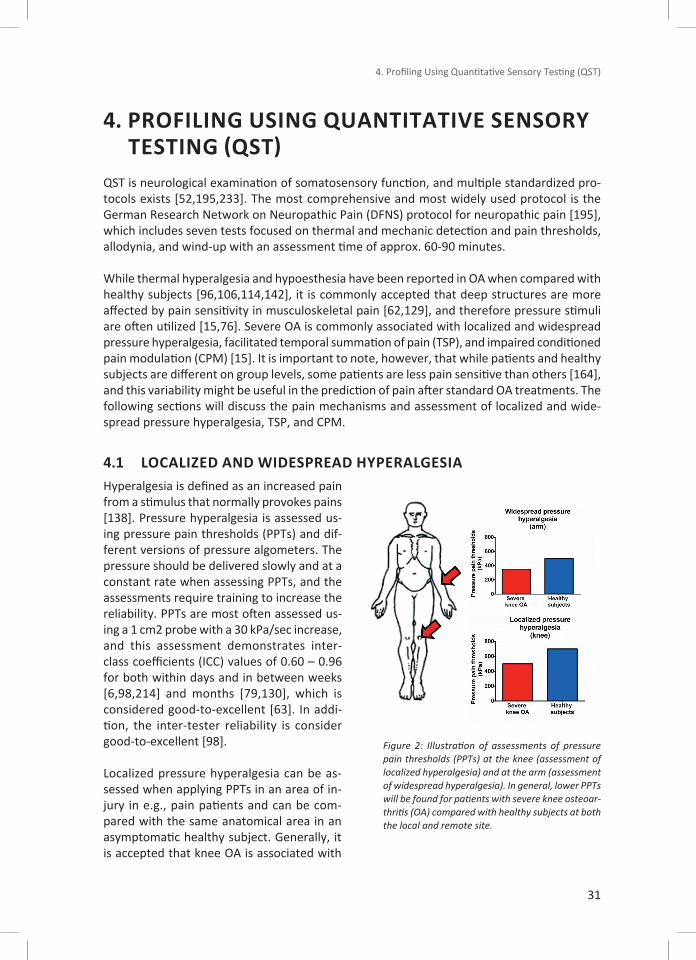
4.1 LOCALIZED AND WIDESPREAD HYPERALGESIAHyperalgesia is defined as an increased pain from a stimulus that normally provokes pains [138]. Pressure hyperalgesia is assessed us-ing pressure pain thresholds (PPTs) and dif-ferent versions of pressure algometers. The pressure should be delivered slowly and at a constant rate when assessing PPTs, and the assessments require training to increase the reliability. PPTs are most often assessed us-ing a 1 cm2 probe with a 30 kPa/sec increase, and this assessment demonstrates inter-class coefficients (ICC) values of 0.60 – 0.96 for both within days and in between weeks [6,98,214] and months [79,130], which is considered good-to-excellent [63]. In addi-tion, the inter-tester reliability is consider good-to-excellent [98].
Localized pressure hyperalgesia can be as-sessed when applying PPTs in an area of in-jury in e.g., pain patients and can be com-pared with the same anatomical area in an asymptomatic healthy subject. Generally, it is accepted that knee OA is associated with
Figure 2: Illustration of assessments of pressure pain thresholds (PPTs) at the knee (assessment of localized hyperalgesia) and at the arm (assessment of widespread hyperalgesia). In general, lower PPTs will be found for patients with severe knee osteoar-thritis (OA) compared with healthy subjects at both the local and remote site.
Mechanistic Pain Profiling of Patients with Osteoarthritis
32
lower PPTs around the knee joint (anatomical markers around patella) compared with age- and gender-match healthy subjects [15,155], which suggests localized pressure hyperalgesia.
Widespread pressure hyperalgesia can be assessed when applying PPTs outside (preferably extra-segmentally) the area of injury in pain patients and comparing this to the same ana-tomical area in an asymptomatic healthy subject. Widespread pressure hyperalgesia is often found in severe knee OA when assessing the PPTs at e.g., the arm compared with age- and gender-match healthy subjects [15]. Widespread hyperalgesia suggests sensation of central pain mechanisms and might be associated with impairment of descending pain inhibitory control systems [76], which is also commonly found in severe knee OA [15] and other painful conditions [11].
Thermal stimuli can be utilized to assess cold and warm detection thresholds (WDT and CDT, respectively) and heat and cold pain thresholds (HPT and CPT, respectively) [194] and can be used to assess localized and widespread hyperalgesia to thermal stimuli. Thermal stimuli are widely used in the DFNS protocols, and Aasvang et al., 2010[1] demonstrated that preopera-tive painful ratings to suprathreshold heat stimuli were associated with chronic postoperative pain following groin hernia repair surgery. In addition, Edwards et al., 2006 [56] have found that pretreatment HPT was associated with the analgesic effect of opioids in patients with postherpetic neuralgia, and Demant et al., 2014 and 2015 utilized the DFNS protocol to clas-sify patients with peripheral neuropathic pain into subgroups defined by irritable nociceptors, which had a lower number needed to treat for oxcarbazepine [45] and lidocaine patches [44] compared with subgroups classified by non-irritable nociceptors.
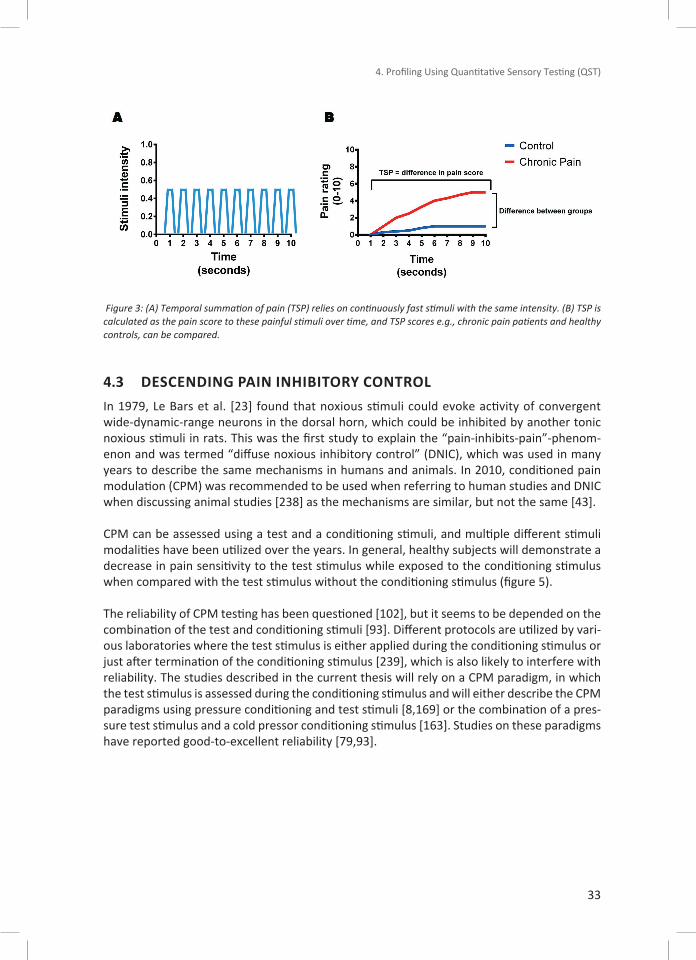
4.2 SENSITIZATION OF CENTRAL PAIN MECHANISMSThe wind-up process of dorsal horn neurons can be assessed in animals [38] and reflects the excitability of dorsal horn neurons [178]. Assessing wind-up requires placement of electrodes into the spinal cord of the animal, which is not feasible in human studies. TSP is the human surrogate model of the wind-up process [10]. TSP can be assessed using painful heat [231], pin-prick [163], electrical [154], or pressure stimuli [164]. In general, the assessment of TSP relies on a train of painful stimuli, which are applied rapidly and with the same intensity [177,184] while the subject is instructed to rate the pain for all of the stimuli or to rate the first and the last stimuli (see figure 4).
Studies have found facilitated TSP in chronic pain conditions such as fibromyalgia [11,80,179,217] and severe osteoarthritis [9,12,36,58,219] compared with healthy subjects, indicating a sensitization central pain mechanisms. Facilitated TSP is believed to be associated with NMDA receptor activation since administrating NMDA-antagonists can decrease TSP [80].
4. Profiling Using Quantitative Sensory Testing (QST)
33
Figure 3: (A) Temporal summation of pain (TSP) relies on continuously fast stimuli with the same intensity. (B) TSP is calculated as the pain score to these painful stimuli over time, and TSP scores e.g., chronic pain patients and healthy controls, can be compared.
4.3 DESCENDING PAIN INHIBITORY CONTROLIn 1979, Le Bars et al. [23] found that noxious stimuli could evoke activity of convergent wide-dynamic-range neurons in the dorsal horn, which could be inhibited by another tonic noxious stimuli in rats. This was the first study to explain the “pain-inhibits-pain”-phenom-enon and was termed “diffuse noxious inhibitory control” (DNIC), which was used in many years to describe the same mechanisms in humans and animals. In 2010, conditioned pain modulation (CPM) was recommended to be used when referring to human studies and DNIC when discussing animal studies [238] as the mechanisms are similar, but not the same [43].
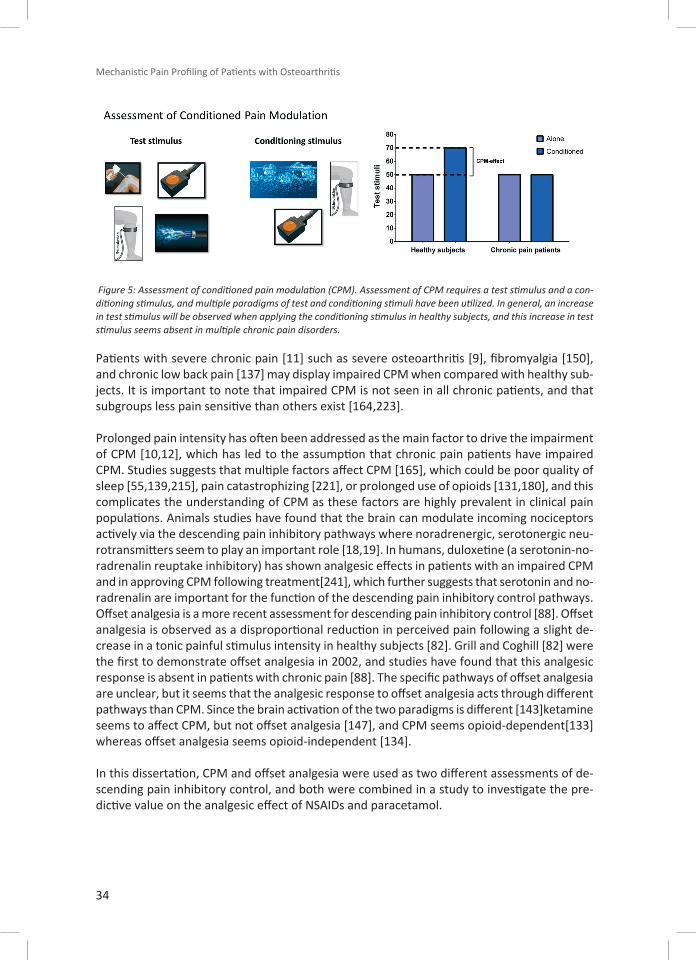
CPM can be assessed using a test and a conditioning stimuli, and multiple different stimuli modalities have been utilized over the years. In general, healthy subjects will demonstrate a decrease in pain sensitivity to the test stimulus while exposed to the conditioning stimulus when compared with the test stimulus without the conditioning stimulus (figure 5).
The reliability of CPM testing has been questioned [102], but it seems to be depended on the combination of the test and conditioning stimuli [93]. Different protocols are utilized by vari-ous laboratories where the test stimulus is either applied during the conditioning stimulus or just after termination of the conditioning stimulus [239], which is also likely to interfere with reliability. The studies described in the current thesis will rely on a CPM paradigm, in which the test stimulus is assessed during the conditioning stimulus and will either describe the CPM paradigms using pressure conditioning and test stimuli [8,169] or the combination of a pres-sure test stimulus and a cold pressor conditioning stimulus [163]. Studies on these paradigms have reported good-to-excellent reliability [79,93].
Mechanistic Pain Profiling of Patients with Osteoarthritis
34
Figure 5: Assessment of conditioned pain modulation (CPM). Assessment of CPM requires a test stimulus and a con-ditioning stimulus, and multiple paradigms of test and conditioning stimuli have been utilized. In general, an increase in test stimulus will be observed when applying the conditioning stimulus in healthy subjects, and this increase in test stimulus seems absent in multiple chronic pain disorders.
Patients with severe chronic pain [11] such as severe osteoarthritis [9], fibromyalgia [150], and chronic low back pain [137] may display impaired CPM when compared with healthy sub-jects. It is important to note that impaired CPM is not seen in all chronic patients, and that subgroups less pain sensitive than others exist [164,223].
Prolonged pain intensity has often been addressed as the main factor to drive the impairment of CPM [10,12], which has led to the assumption that chronic pain patients have impaired CPM. Studies suggests that multiple factors affect CPM [165], which could be poor quality of sleep [55,139,215], pain catastrophizing [221], or prolonged use of opioids [131,180], and this complicates the understanding of CPM as these factors are highly prevalent in clinical pain populations. Animals studies have found that the brain can modulate incoming nociceptors actively via the descending pain inhibitory pathways where noradrenergic, serotonergic neu-rotransmitters seem to play an important role [18,19]. In humans, duloxetine (a serotonin-no-radrenalin reuptake inhibitory) has shown analgesic effects in patients with an impaired CPM and in approving CPM following treatment[241], which further suggests that serotonin and no-radrenalin are important for the function of the descending pain inhibitory control pathways.Offset analgesia is a more recent assessment for descending pain inhibitory control [88]. Offset analgesia is observed as a disproportional reduction in perceived pain following a slight de-crease in a tonic painful stimulus intensity in healthy subjects [82]. Grill and Coghill [82] were the first to demonstrate offset analgesia in 2002, and studies have found that this analgesic response is absent in patients with chronic pain [88]. The specific pathways of offset analgesia are unclear, but it seems that the analgesic response to offset analgesia acts through different pathways than CPM. Since the brain activation of the two paradigms is different [143]ketamine seems to affect CPM, but not offset analgesia [147], and CPM seems opioid-dependent[133] whereas offset analgesia seems opioid-independent [134].
In this dissertation, CPM and offset analgesia were used as two different assessments of de-scending pain inhibitory control, and both were combined in a study to investigate the pre-dictive value on the analgesic effect of NSAIDs and paracetamol.
5. Mechanistic Pain Profiling of Patients with Osteoarthritis
35
5. MECHANISTIC PAIN PROFILING OF PATIENTS WITH OSTEOARTHRITIS
The studies presented here have all utilized longitudinal designs and assessments before and after TKA or treatment with NSAIDs (selective COX-2 inhibitors or non-selective NSAIDs) plus paracetamol.
Prior to the publications of the above papers, two studies on TKA had previously been pub-lished describing an association between preoperative electrical pain thresholds [124] and widespread hyperalgesia [235] and chronic postoperative pain. In addition, Martinez et al., 2007 [132] found no association between preoperative allodynia, mechanical pain thresholds, heat and cold pain thresholds, and chronic postoperative pain. Similar, Noiseux et al., 2014 [149] assessed mechanical pain threshold, heat pain threshold, and pressure pain thresholds assessed around the knee in patients scheduled for TKA and did not find the presence of mod-erate-to-severe postoperative pain at a 6-month follow-up.
The presentation of papers will focus on associations between QST (alone or in combination) and the pain outcomes after standard OA treatments. The coefficient of determination (R2) will be described for both correlations and linear regressions.
The following sections will shortly describe each individual paper, a discussion on how these findings fit into the literature and finalize with an overall discussion and conclusions from the studies. An overview of the eight studies is found in table 1.

Mechanistic Pain Profiling of Patients with Osteoarthritis
36
Pape
r N
umbe
rRe
fere
nce
Year
Type
of
Inte
rven
tion
Num
ber o
f Pa
tient
sQ
ST P
aram
eter
sFo
llow
-up
Tim
eDe
pend
ent
Para
met
erM
odel
s and
Pr
edic
tors
1Pe
ters
en
et a
l. [1
63]
2015
TKA
78PP
Ts, m
TSP,
pCP
M#
12 M
OPa
in in
tens
ityRe
gres
sion:
§m
TSP
and
PreO
P VA
S:
R2 = 0
.13
2Pe
ters
en
et a
l. [1
64]
2016
TKA
103
cPPT
, cPT
T, c
TSP,
cCP
M, P
PTs
12 M
OPa
in re
lief
Regr
essio
n: §
R2 =
0.3
79, u
sing
cPPT
an
d VA
S
3Iz
umi e
t al.
[96]
2017
THA
40cP
PT, c
PTT,
cTS
P, c
CPM
, cSS
, PP
Ts, C
DT, C
PT, W
DT, H
PT, M
PT6
wee
ks
Pain
relie
fCo
rrel
ation
: §R2 =
0.2
70 u
sing
TSP
4Pe
ters
en
et a
l.[16
7]20
18TK
A13
0CD
T, C
PT, W
DT, H
PT, m
TSP
12 M
OPa
in in
tens
ityRe
gres
sion:
§Pr
eOP
mTS
P, W
DT,
HPT
and
KL R
2 = 0
.119
5La
rsen
et a
l.[1
17]
2020
TKA
131
cPPT
, cPT
T, c
CPM
12 M
OPa
in in
tens
ityRe
gres
sion:
R2 = 0
.205
usin
g pr
e-O
P CP
M a
nd P
CS
6Ar
endt
-N
ielse
n et
al.[
8]20
16CO
X-2
in-
hibi
tors
and
pl
aceb
o37
PPT,
pTS
P, p
CPM
ꝉ28
day
s
Chan
ge in
pa
in in
tens
ity
for n
on-r
e-sp
onde
rs
Corr
elati
on:
pTSP
pre
dicti
ng a
no
n-re
spon
se: R
=
0.42
1 - 0
.639
7Pe
ters
en
et a
l. [1
66]
2019
NSA
ID a
nd
para
ceta
mol
132
cPPT
, cPT
T, c
TSP
21 d
ays
Chan
ge in
pa
in in
tens
ity
Regr
essio
n:R2 =
0.2
69 u
sing
VAS
and
cTSP
8Pe
ters
en
et a
l. [1
69]
2019
NSA
ID a
nd
para
ceta
mol
42O
ffset
ana
lges
ia, c
CPM
21 d
ays
Chan
ge in
pa
in in
tens
ity
Corr
elati
on:
R2 = 0
.186
usin
g cC
PM
and
VAS
Tabl
e 1:
Pap
ers
incl
udin
g in
the
diss
erta
tion
usin
g qu
antit
ative
sen
sory
testi
ng (Q
ST) t
o pr
edic
t chr
onic
pos
tope
rativ
e pa
in a
nd a
nalg
esic
effe
cts.
QST
mod
aliti
es: C
DT: C
old
Dete
ction
Thr
esho
ld, C
PT: C
old
Pain
Thr
esho
ld, c
PPT:
Cuff
-indu
ced
Pres
sure
Pai
n Th
resh
old,
cPTT
: Cuff
-indu
ced
Pres
sure
Tol
eran
ce T
hres
hold
, CPM
: Con
ditio
ning
Pai
n M
odul
ation
(c
: cuff
pre
ssur
e te
st a
nd c
ondi
tion
stim
uli,
p: p
ress
ure
test
stim
ulus
, # c
old
pres
sor t
ests
as
cond
ition
stim
ulus
), HP
T: H
eat P
ain
Thre
shol
d, M
PT: M
echa
nica
l Pai
n Th
resh
old,
PP
T: P
ress
ure
Pain
Thr
esho
ld, T
SP: T
empo
ral S
umm
ation
of P
ain
(c: u
sing
cuff
stim
uli,
m: u
sing
mec
hani
cal p
inpr
ick
stim
uli,
p: u
sing
pres
sure
stim
uli),
WDT
: War
m D
etec
tion
Thre
shol
d. O
ther
abb
revi
ation
s: R
: Coe
ffici
ent o
f det
erm
inati
on. §
: Cal
cula
ted
for t
his
diss
erta
tion
only
and
not
pre
sent
ed in
the
orig
inal
pap
er. T
he d
ata
pres
ente
d he
re a
re
mod
ified
from
Pet
erse
n et
al.,
202
0 [1
70].

5. Mechanistic Pain Profiling of Patients with Osteoarthritis
37
5.1 DISCUSSION OF THE PAPERS INCLUDED IN THIS DISSERTATION
Paper 1 [163] aimed to investigate whether assessments of preoperative central pain mech-anisms were associated to chronic postoperative pain after TKA. Paper 1 [163] assessed 78 patients with severe knee OA before, 2 months after, and 12 months after TKA using self-re-ported pain scores (VAS), PPTs, TSP, and CPM. The study was the first to demonstrate that the combination of facilitated preoperative TSP and high preoperative pain intensity predicted high clinical pain 12 months after surgery with a R2 = 13 % using a linear regression model. The R2 was not presented in the original paper, but was calculated for paper 9 [170].
Paper 1 [163] was the first study to demonstrate an association between preoperative TSP and chronic postoperative pain. Previously, assessment of central pain mechanisms had demon-strated that preoperative widespread hyperalgesia was associated to high WOMAC scores 13 months after TKA surgery [235] and that impaired preoperative CPM was associated with chronic postoperative pain intensity after thoracic surgery [240] and major abdominal surgery [234]. The combination of these findings suggested that preoperative assessments of central pain mechanism activity might provide predictive information on chronic postoperative pain.
Paper 2 [164] aimed to identify if preoperative combinations of TSP and CPM profiles could identity a subgroup of patients in higher risk of chronic postoperative pain. This study was mainly a consequence of previously developed “pain sensitivity index” [9], in which subgroups of OA patients reported high clinical pain in combination with facilitated TSP and impaired CPM. Paper 2 [164] assessed 103 patients with severe knee OA before and 12 months after TKA. Self-reported pain scores were assessed before and 12 months after TKA, and pain relief following TKA was calculated as the difference between pre- and postoperative pain scores. In this study, patients were subgrouped based on preoperative CPM and TSP using the aver-age of TSP and CPM from the cohort as cut-off values. Based on this, four groups were de-scribed with 1) facilitated TSP and impaired CPM, 2) facilitated TSP and non-impaired CPM, 3) non-facilitated TSP and impaired CPM, and 4) non-facilitated TSP and non-impaired CPM. Paper 2 [164] found that the group of preoperative, impaired CPM and facilitated TSP had worst pain relief 12 months after TKA compared with patients with impaired CPM alone or facilitated TSP alone. Using a linear regression model, this paper found that the combination of preoperative low cPDT and high preoperative VAS scores was predictive of higher post-operative pain scores (R2 = 38 %). The R2 value was not presented in the original paper, but calculated for paper 9 [170].
Prior to Paper 2 [164], it was established that certain patients with knee OA were more sensi-tive than others and that these patients could be classified by TSP and CPM [9]. Paper 2 [164] supported the previously published data that preoperative, impaired CPM [234,240] and fa-cilitated TSP [163] were risk factors for chronic postoperative pain. Interestingly, a study on patients with chronic pain [223] was published just after paper 2 [164], which supported the idea that CPM and TSP could be utilized to subgroup patients with high clinical pain scores.
The predictive model in paper 2 [164] demonstrated that preoperative widespread pressure hyperalgesia and high preoperative pain was associated with low pain relief after TKA, which supported the study by Wylde et al., 2013 [235]. The group led by Wylde published a large

Mechanistic Pain Profiling of Patients with Osteoarthritis
38
study on THA and TKA in 2015, in which Wylde et al., 2015 [236] found that preoperative widespread pressure hyperalgesia was not associated with 12 months postoperative WOMAC scores for patients undergoing TKA, but predictive for patients undergoing THA. This was in conflict with their previous study [235]. Paper 2 [164] further supported that preoperative assessments of central pain mechanisms are associated to chronic postoperative pain fol-lowing TKA.
Prior to Paper 3 [167], subgroups of patients with OA with facilitated TSP and impaired CPM had been identified based on KL and clinical pain intensity scores [9]. In addition, King et al., 2013 [106] demonstrated that patients with severe knee OA were more sensitive to pain heat stimuli, Aasvang et al., 2010 [1] demonstrated a weak association between preoperative heat pain thresholds and chronic postoperative pain after groin hernia repair surgery, and Lunn et al., 2013 [125] found associations between preoperative heat pain thresholds and acute postoperative following TKA. Paper 3 [167] aimed to assess if preoperative thermal stimuli were predictive of chronic postoperative pain following TKA. Paper 3 [167] was from the same cohort as paper 2 [164] with the overall aim to assess a large range of QST parameter before and after TKA. In total, 200 patients were included in the study, but the cuff algometer (which was described in paper 2 [164]) was added as an amendment after the first 65 patients were included. In paper 3 [167], 70 patients were excluded due to missing data, which was mainly due to technical difficulties using the thermal stimulator. The patients in paper 3 [167] were categorized as patients with chronic postoperative pain if the patients did not yield at least 30% reduction in pain comparing pre- and 12 month postoperative pain scores. Paper 3 [167] utilized a linear regression and found that preoperative WDT, HPT, KL, and TSP all contributed to the predictive value of the model (R2 = 12 %), but TSP was the only significant, independent predictor. The R2 was not presented in the original paper, but was calculated for paper 9 [170].
Paper 3 [167] showed that patients with low KL might be in risk of poor pain alleviation follow-ing TKA, which was supported by Riis et al., 2014 [191]. In addition, paper 3 [167] supported the notion that patients with low KL and high pain might display high pain sensitivity levels argued previously [9], and paper 3 [167] further added that these patients might be in risk of poor pain alleviation following TKA.
Paper 3 [167] did find associations between preoperative WDT and HPT and chronic postop-erative pain intensities, which supported the previous findings on acute [73,125,159,218,230] and chronic [1] postoperative pain.
In paper 4 [117], aimed to advance the predictive models by including QST and other known preoperative risk factors for chronic postoperative pain. Prior to recruitment, no studies found associations between preoperative CPM and chronic postoperative pain following TKA. Previous preoperative CPM had been associated with chronic postoperative pain following thoracic surgery [240] and abdominal surgery [234]. Today, two studies have found preoper-ative CPM associated with chronic postoperative pain following TKA [32,224]. Preoperative pain catastrophizing has been suggested as a strong preoperative predictor for pain 6 [190] and 24 months [64] after TKA surgery, and studies suggest an interaction between CPM and pain catastrophizing [232]. In addition, studies have found widespread pressure hyperalgesia in patients categorized as neuropathic pain-like components compared with patients catego-rized as nociceptive pain-like components according to the PainDetect questionnaire [141],
5. Mechanistic Pain Profiling of Patients with Osteoarthritis
39
and studies have found preoperative widespread hyperalgesia to be associated with chronic postoperative pain after TKA [14,164,235]. Furthermore, preoperative high PainDetect scores have been found associated with high 6 months postoperative pain scores after TKA compared with low preoperative PainDetect scores [115].
Studies indicated that preoperative QST in combination with other known pre- and periop-erative risk factors might improve the predictive models [1,32,124,186,210] (including pa-per 1, 2, and 5 [163,164,167]). Therefore, Paper 4 [117] aimed to assess predictive value of previously established preoperative predictors for chronic postoperative pain after TKA such as pain intensity, CPM, pain catastrophizing, and PainDect scores alone and in combination.
Paper 4 [117] demonstrated statistically significant correlations between chronic postopera-tive pain and preoperative pain intensity (R2 = 18%), CPM (R2 = 3%), pain catastrophizing (R2 = 11%), and PainDetect scores (R2 = 9%). A linear regression model utilizing the four preop-erative predictors could significantly predict chronic postoperative pain (adjusted R2 = 21%).
Paper 4 [117] was the first to combine preoperative pain intensities, CPM, pain catastrophiz-ing, and PainDect scores in one predictive model for chronic postoperative pain following TKA and found that the combination of these factors yielded a better predictive value than each of the elements alone.
Paper 5 aimed to explore if the previous findings from the TKA studies could be utilized for pain after THA. Paper 5 [96] assessed 40 patients with hip OA before and six weeks after THA using the pain intensity scores (VAS) and cold and warm detection and heat and cold pain thresholds, PPTs, TSP, and CPM. The study found that preoperative TSP was associated with postoperative pain (R2 = 19%) and postoperative pain relief (R2 = 27%).
Paper 5 [96] was the first to report that preoperative TSP was associated with postoperative pain and postoperative pain relief after THA. Wylde et al., 2015 [236] found that preoperative widespread hyperalgesia was associated with WOMAC scores 12 months after THA, which was not the case in paper 5 [96] although both studies support the notion that preoperative assessment of central pain mechanisms is associated with postoperative pain after THA.
Paper 5 [96] included data on thermal stimuli as previous studies had demonstrated associa-tions between preoperative thermal stimuli and acute [73,125,159,218,230] and chronic [1] postoperative pain. No association between preoperative thermal stimuli and postoperative pain was reported in paper 5 [96], which could be due to a relatively small sample size or the fact that most previous papers demonstrating a predictive value utilized suprathreshold stim-uli [1,73,125,218,230].
Paper 5 [96] is the only paper in this dissertation reporting on patients with hip OA, and the paper was included to indicate that assessments of central pain mechanisms might be used in other populations than patients with knee OA. Paper 5 [96] is limited by the follow-up as-sessment which was six weeks after surgery, and therefore these findings do not necessarily report chronic postoperative pain.
Mechanistic Pain Profiling of Patients with Osteoarthritis
40
Paper 6 [8] was primarily focused on the modulatory effect of etoricoxib (a COX-2 inhibitor) on clinical pain intensity and PPT, TSP, and CPM. Paper 6 [8] was based on a randomized, dou-ble-blind, placebo-controlled, 2-way crossover study assessing clinical pain intensity, PPTs, TSP, and CPM before and after a 4-week placebo or etoricoxib treatment paradigm in 37 pa-tients with knee OA. Paper 6 [8] is incorporated in this dissertation as a prediction model on the effect of COX-2 inhibitors was included.
Paper 6 [8] demonstrated that four weeks of COX-2 inhibitors decreased clinical pain inten-sities, and it was the first study to demonstrate a decrease in TSP following COX-2 inhibitors when compared with placebo. Furthermore, this paper was the first to demonstrate an asso-ciation between pre-treatment facilitated TSP and poor analgesic response (R2 = 18-41 %) in a subset of patients with knee OA characterized as non-responders.
Paper 6 [8] was the first to demonstrate an association between pre-treatment facilitated TSP and poor analgesic response in patients with knee OA. Edwards et al., 2016 [53] found that pre-treatment impaired CPM was associated with poor analgesic response to topical NSAIDs in patients with knee OA, which supported the finding in paper 6 [8] suggesting that pain sensitive patients with knee OA might not respond well to COX-2 selective and topical non-selective NSAIDs.
NSAIDs and paracetamol are standard treatments for pain in OA [21], and paper 7 [166] fur-ther investigated the association between QST and responses to NSAIDs and paracetamol, which had already been briefly investigated by Edwards et al., 2016 [53] and in paper 6 [8]. Paper 7 [166] assessed 132 patients with knee OA before and after 3 weeks of NSAIDs (400 mg ibuprofen daily) and paracetamol (3000 mg daily) using self-reported pain scores and cPDT, cPTT, and TSP.
Paper 7 [166] was the first to demonstrate that non-responders (either less than 30% or 50% pain relief) to 3 weeks of NSAIDs and paracetamol are categorized by pre-treatment facili-tated TSP. Using a linear regression model, paper 7 [166] found that pre-treatment TSP and pre-treatment clinical pain predicted the analgesic effect of NSAIDs and paracetamol with a R2 = 27%.
Study 7 [166] was the first large-scale study applying QST profiling on pharmaceutical ther-apies in knee OA, and it [166] supported the finding by Edwards et al., 2016 [53] suggesting that pain sensitive OA patients are less likely to benefit from NSAIDs.
Paper 8 [169] elaborated on the findings by Edwards et al., 2016 [53] suggesting that impaired descending pain inhibitory function was associated with poor analgesic response to topical NSAIDs. In a preclinical study, Graham et al., 2013 [71] suggested that an intact serotonin sys-tem was needed for an analgesic response to NSAIDs, and serotonin seemed to be an impor-tant neurotransmitter for the descending pain inhibitory control [19,122]. Therefore, paper 8 [169] assessed if assessment of descending pain inhibitory control could predict the analgesic effect of 3 weeks of NSAIDs and paracetamol.
The study population in Paper 8 [169] was the same as in paper 7 [166]. Clinical pain, CPM, and offset analgesia were assessed before and after 3 weeks of NSAIDs (400 mg ibuprofen

5. Mechanistic Pain Profiling of Patients with Osteoarthritis
41
daily) and paracetamol (3000 mg daily). Using a linear regression model, pre-treatment clini-cal pain and CPM were predictive of the analgesic effect with a R2 = 19%. The data presented in paper 8 [169] were greatly limited by missing data due to the malfunction of the thermal testing device for assessing offset analgesia.
It has been argued that the response of NSAIDs and paracetamol is dependent on an intact serotonin system [71]. Preclinical trials connect the serotonin system to descending pain inhi-bition [19,20,122], the human surrogate model for assessing descending pain inhibition is CPM [237], and impaired CPM can be restored by the administration of serotonin-noradrenaline reuptake inhibitors in patients with painful diabetic neuropathies [241]. Paper 8 [169] demon-strated that impaired CPM was associated with poor response to NSAIDs and paracetamol, which might support the notion that a response to NSAIDs and paracetamol is dependent on an intact serotonin system if CPM is an indirect measure of serotonin activity.
Sangesland et al., 2017 [199] reviewed the literature on preoperative QST and the association with postoperative pain. Sangesland et al., 2017 [199] did not include associations between QST and analgesic effects to pharmacological interventions, and from 2017 to 2020, 10 new studies were published on QST and the association with chronic postoperative pain. Therefore Paper 9 [170] aims to give an up-date on the association between QST and chronic postoper-ative and analgesic effects to pharmacological interventions.
In April 2020, Pubmed and EMBASE were systematically searched for all papers on the predic-tive value of QST in relations to chronic postoperative pain and responses to pharmacological treatments. Inclusion for the surgical papers was prediction models evaluating at least one preoperative QST parameter with an assessment of pain at least three months after surgery. Surgical studies on acute and subacute postoperative pain were excluded since QST seemed to have less predictive value in the early postoperative phase [199]. Pharmacological studies including predictive models which evaluated at least one QST parameter and a pain related outcome after a pharmacological treatment were included. Studies evaluating pain-free sub-jects and studies evaluating the short-term effect of pharmacological interventions (minutes to hours) were excluded.
Paper 9 [170] identified 25 surgical and 11 pharmacological papers with 17 surgical papers and 11 pharmacological papers demonstrating an association between preoperative or pre-treatment QST and chronic postoperative or pain-related response to pharmacological treat-ments. Deep pressure stimuli, TSP, and CPM were the most frequently assessed QST modal-ities, and TSP (50%) and CPM (approx. 44%) were most frequently associated with chronic postoperative pain or response to pharmacological treatment. Paper 9 [170] highlighted that the predictive power of prediction models (both correlations and more advanced prediction models) ranged from 12% to 67%.
Paper 9 [170] is included in this dissertation to give an overview of the field on QST as predic-tors for chronic postoperative pain and responses to pharmacological treatments.
Paper 9 [170] was the first to systematically review all studies on QST as a predictor for surgical and pharmacological outcomes and identified 36 studies with 28 studies (approx. 78%) report-ing a statistically significant association between preoperative or pretreatment QST and chronic

Mechanistic Pain Profiling of Patients with Osteoarthritis
42
postoperative pain or response to pharmacological treatments. The most consistent predictors were TSP (reported in 14 studies and found as predictor in seven studies, 50%) and CPM (report-ed in 17 studies and found as a predictor in seven studies, 41%). Even though multiple studies find QST parameters as predictors for chronic postoperative pain or analgesic effect of phar-macological interventions [1,7,107,115,124,127,154,163,164,166,169,186,8,210,224,234–236,240,241,14,32,44,45,53,56,99], paper 9 [170] questions if these associations are clinical-ly meaningful as the predictive power differs substantially between studies.

6. General Discussion
43
6. GENERAL DISCUSSION Papers 1-8 [8,96,117,163,164,166,167,169] describe the work on preoperative or pretreat-ment QST as potential predictors for chronic postoperative pain and analgesic effect of NSAIDs and paracetamol in patients with OA. All eight paper find statistically significant associations, but the systematic review (paper 9 [170]) questions if the associations are clinically relevant.
6.1 THE PREDICTIVE VALUE OF QST PROFILING IN OSTEOARTHRITISAs discussed in Paper 9 [170] multiple studies have assessed preoperative [14,32,115,124,132,149,186,224,235,236] and pretreatment [8,53,166,169] QST in patients with OA, and the results are mixed. Paper 9 [170] highlighted that 10 out of 12 surgical (83%) and four out of four pharmacological (100%) studies demonstrate significant QST predictors for chronic post-operative pain or response to pharmacological interventions in patients with OA. In addition, O’leary et al., 2018 [158] found pretreatment facilitated TSP and widespread pressure hyper-algesia to be associated with a limited pain relieving response to physiotherapy in patients with knee OA, which further supports a predictive value for QST in patients with OA. This is supported by a recent study by Hansen et al. [87] demonstrating an association between pre-treatment TSP and pain relief following exercise therapy of patients with knee OA. In 2016, an IASP taskforce suggested “nociplastic” as new pain phenotype [112] to reflect changes in the nociceptive system. The “nociplastic” suggestion did receive some criticism [35,72,140], but it may be suitable for the patients described in this dissertation who are characterized as “centrally sensitized”, and who do not respond well to the standard OA treatment suggested by OARSI [21,243].
It is important to highlight that conflicting literature on the predictive value of QST to OA ther-apy does exist. Arendt-Nielsen et al., 2018 [14] assessed 100 patients with OA and found no association between PPTs at the knee or the lower leg of patients with knee OA and response to exercise therapy. Martinez et al., 2007 [132] investigated 20 patients with OA and found no association between preoperative allodynia or pain thresholds to mechanical, heat and cold stimuli, and chronic postoperative pain after TKA. Finally, Noiseux et al., 2014 assessed 193 patients with OA and found no association between preoperative mechanical heat and pressure pain thresholds and the presence of moderate-to-severe chronic postoperative pain. Conclusively, more studies seem to suggest a statistically significant association between QST and chronic postoperative pain and analgesic effect in OA than studies rejecting this hypothesis.
One could speculate that there could be a publication bias in mainly reporting statistically significant results. A search on Clinical.gov will reveal that approx. 25 studies have been con-ducted using the search terms “osteoarthritis” and “Quantitative Sensory Testing”, and some of these studies have not been published yet, which could indicate a selection bias towards publishing.

Mechanistic Pain Profiling of Patients with Osteoarthritis
44
6.2 “WE ONLY HAVE TIME TO DO ONE TEST – WHICH ONE SHOULD IT BE?”
The above mentioned question is relevant when implementing something as complicated and time consuming as QST into a busy clinical workday, but the answer is not easy. The follow-ing sections will attempt to answer the question by observing it from three different angles, namely 1) the studies based on my research, 2) the studies on osteoarthritis in general, and 3) the studies on different pain populations.
6.2.1.1 STUDIES INCLUDING IN THIS DISSERTATIONThe current dissertation utilized pressure (paper 1[163], 2 [164], 3 [96], 5 [117], 6 [8], 7 [166], and 8 [169]) and thermal pain thresholds (paper 3 [96] and 5 [117]), TSP (paper 1 [163], 2 [164], 3 [96], 4 [167], 6 [8], and 7), and CPM (paper 1 [163], 2 [164], 3 [96], 5 [117], 6 [8], and 8 [169]) in predictive studies on OA. Pressure pain thresholds assessed remotely from the OA affected knee (possible sign of spreading pressure hyperalgesia) were evaluated in four of my surgical studies and found predictive for chronic postoperative in one study (25%) [164] and not predictive of analgesic effect after pharmacological interventions in three studies (0%). TSP was evaluated in four of my surgical studies and predictive of chronic postoperative pain in three (75%) [96,163,167] and assessed in two pharmacological studies and predictive for the analgesic effect in both studies (100%) [8,166]. CPM was assessed in four of my surgical studies and predictive for chronic postoperative pain in one study (25%) [117]. Thermal stimuli were evaluated in two surgical studies and predictive in one study (50%) [167].
Based on this dissertation, TSP is most frequently assessed and most frequently found as predictive, and therefore, TSP could be that “one test”, which should be included in future research.
6.2.1.2 STUDIES ON OSTEOARTHRITIS IN GENERALThe question can also be answered from a more generalized OA perspective including all studies on OA including QST as predictors. Pressure pain thresholds have been assessed in 11 surgical studies and were predictive of chronic postoperative pain in five studies (36%, of note: pressure pain thresholds were predictive for chronic postoperative pain after total hip, but not total knee arthroplasty in Wylde et al., 2015 [236]) [115,164,235,236], and assessed in four pharmacological studies, but not predictive of the analgesic effect (0%). TSP have been evaluated in seven surgical studies and found predictive for chronic postoperative pain in five studies (71%) [96,115,163,167,186] and assessed in three pharmacological studies in which it was found predictive of analgesic effect in two studies (67%) [8,166]. CPM has been assessed in eight surgical studies and found predictive of chronic postoperative pain in three (38%) [32,117,224] and evaluated in three pharmacological studies and predictive of analge-sic effect in two studies (67%) [53,169]. Thermal stimuli have been assessed in four surgical studies and found predictive in one study (25%) [167]. In addition, exercise induced hyperal-gesia was evaluated in on surgical study and predicted chronic postoperative pain [224], and offset analgesia was assessed in one pharmacological study, but did not predict any analge-sic effect [169]. Mechanical pin prick pain has been assessed in two surgical studies, but not found predictive for chronic postoperative pain [132,149]. Finally, allodynia was evaluated in one surgical study, but not found predictive for chronic postoperative pain [132].

6. General Discussion
45
6.2.1.3 STUDIES ON DIFFERENT PAIN POPULATIONS Paper 9 [170] summarized the studies using QST as predictors for chronic postoperative pain and analgesic effects and identified 25 surgical and 11 pharmacological studies. Paper 4 [117] was not included in paper 9 [170] so the current number of surgical papers is now 26. Conclusively, TSP has been assessed in 14 studies and found predictive in seven studies (50%) [8,115,163,166,167,186,210], CPM has been evaluated in 18 studies and found predictive in eight studies (44%) [53,117,169,224,234,240,241], and pressure pain thresholds have been assessed in 18 studies and found predictive in 5 studies (28%) [14,115,164,235,236].Based on these studies, it is concluded that TSP was most frequently assessed and most fre-quently found as a predictor for chronic postoperative pain and analgesic effect.
Based on the studies on OA in general, TSP seems to be most frequently assessed and most frequently found as a predictor for chronic postoperative pain or analgesic effect.
6.2.1.4 CAN WE ANSWER THE QUESTION? Based on the above analysis, TSP seems to be the most consistent predictor for chronic postop-erative pain and analgesic effect. It is important to highlight, however, that a lot (+50%) of the above mentioned studies have been conducted in patients with musculoskeletal pain, which tends to favor pressure stimuli as the QST modality [145]. TSP does not seem to be elevated in patients with e.g., peripheral neuropathic pain [195,226], and therefore TSP might not be predictive of treatment response in these patients. Finally, it is very important to highlight that TSP (or other QST assessment) might be significantly associated with chronic postoperative pain or analgesic effect, but the predictive strength remains low, and therefore, it is advisable to include additional known predictors in future studies.
6.3 METHODOLOGICAL CONSIDERATIONSLinear regression models are often used as the predictive tool in the QST literature, which is also the case for the work presented here. It is worth noticing that linear regression models assume that the dependent factor is linear, which might not be the case for clinical pain inten-sities. Future studies should consider applying more advanced statistical methods to identify if this will improve the predictability of QST.
In this dissertation, the different assessment techniques are self-limiting as multiple different approaches of TSP (pinprick [87,163,167], automated pressure algometer [8] and cuff algom-etry [164,166]) and CPM (conditioning stimulus using the cold pressor test [163], ischemic cuff induced pain [8], and cuff algometry [117,164,169]) have been utilized. As highlighted in paper 9 [170], standardization of QST assessments would increase the comparability between stud-ies, which could push the field forward. On a positive note, the work presented here covers a wide range of different stimuli modalities such as mechanical pin prick, heat and cold stimuli, and deep pressure stimuli and, therefore, substantially adds to the literature discussing which stimuli might be important for predicting treatment outcomes in OA.
QST reliability constitutes an issue in the literature, and CPM has attracted attention recently [102,103]. Reliability studies are conducted either using sessions within days or between days (or weeks). Koo et al., 2016 defines test-retest reliability to “reflect the variation in measure-ments taken by an instrument on the same subject under the same conditions” [111]. In a

Mechanistic Pain Profiling of Patients with Osteoarthritis
46
QST study, this means that reliability studies should aim to establish identical sessions using the same subjects and ensure that the subjects are influenced by the same conditions. The interclass correlation coefficient (ICC) is often reported in QST reliability studies [79,93,225], and this relies on a ranking system in which a better ICC score is obtained if subjects remain within the same rank in between sessions [111]. It is nearly impossible to obtain perfect test-retest reliability of QST parameters due to the fact that everyday factors such as quality of sleep [108,161,215], stress [91,109], or negative affect [54,57] influence QST. Studies sug-gest that these factors might also hold predictive value for pain alleviating response to therapy [126,176,190], and therefore, future studies should focus on understanding the variability of QST parameters and potentially utilizing the variability to strengthen the prediction models.

7. Conclusion
47
7. CONCLUSIONThe current work, demonstrated significant associations between QST poor response to stand-ard surgical and pharmacological treatments in patients with OA indicating that highly pain sensitive patients with OA are less likely to benefit from standard care. In addition, a system-atic review has established that temporal summation of pain is the most consistent predic-tor of chronic postoperative pain and responses to pharmacological treatments. Finally, the predictive strength for quantitative sensory testing remains low and, therefore, encourages a multimodal assessment of patients for future predictive studies.

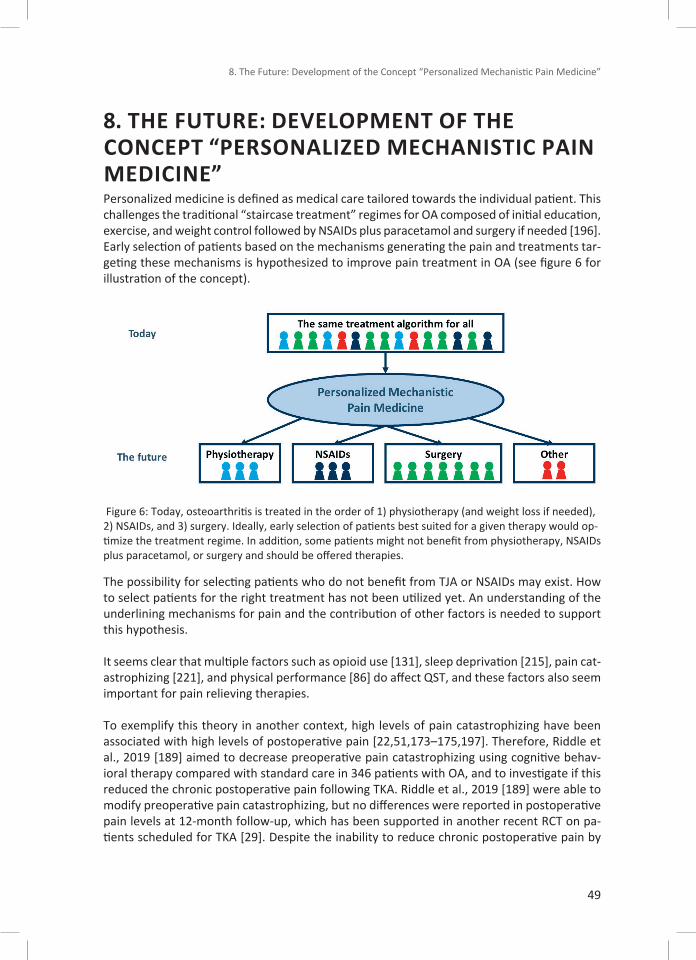
8. The Future: Development of the Concept “Personalized Mechanistic Pain Medicine”
49
8. THE FUTURE: DEVELOPMENT OF THE CONCEPT “PERSONALIZED MECHANISTIC PAIN MEDICINE”Personalized medicine is defined as medical care tailored towards the individual patient. This challenges the traditional “staircase treatment” regimes for OA composed of initial education, exercise, and weight control followed by NSAIDs plus paracetamol and surgery if needed [196]. Early selection of patients based on the mechanisms generating the pain and treatments tar-geting these mechanisms is hypothesized to improve pain treatment in OA (see figure 6 for illustration of the concept).
Figure 6: Today, osteoarthritis is treated in the order of 1) physiotherapy (and weight loss if needed), 2) NSAIDs, and 3) surgery. Ideally, early selection of patients best suited for a given therapy would op-timize the treatment regime. In addition, some patients might not benefit from physiotherapy, NSAIDs plus paracetamol, or surgery and should be offered therapies.
The possibility for selecting patients who do not benefit from TJA or NSAIDs may exist. How to select patients for the right treatment has not been utilized yet. An understanding of the underlining mechanisms for pain and the contribution of other factors is needed to support this hypothesis.
It seems clear that multiple factors such as opioid use [131], sleep deprivation [215], pain cat-astrophizing [221], and physical performance [86] do affect QST, and these factors also seem important for pain relieving therapies.
To exemplify this theory in another context, high levels of pain catastrophizing have been associated with high levels of postoperative pain [22,51,173–175,197]. Therefore, Riddle et al., 2019 [189] aimed to decrease preoperative pain catastrophizing using cognitive behav-ioral therapy compared with standard care in 346 patients with OA, and to investigate if this reduced the chronic postoperative pain following TKA. Riddle et al., 2019 [189] were able to modify preoperative pain catastrophizing, but no differences were reported in postoperative pain levels at 12-month follow-up, which has been supported in another recent RCT on pa-tients scheduled for TKA [29]. Despite the inability to reduce chronic postoperative pain by

Mechanistic Pain Profiling of Patients with Osteoarthritis
50
Riddle and colleagues, the idea of targeting mechanisms, presumably associated with chronic postoperative pain, is good.
Similar to Riddle et al., 2019 [189], future Personalized Mechanistic Pain Medicine studies must be conducted with the aim to target mechanisms, which presumably generate pain (or contribute to pain) in order to investigate possible new treatment options.
For instance, sleep deprivation leads to up-regulation of IL-6 [95], and IL-6 is known to sen-sitize peripheral free nerve endings, which results in localized and widespread hyperalgesia [200]. High IL-6 is associated with high pain scores in patients with OA [59]. Increased physi-cal activity is associated with better sleep [242], and high intensity exercise interventions can reduce the severity of chronic insomnia [182]. In addition, preclinical trials have reported a shift in macrophages type 1 (pro-inflammatory) to type 2 (anti-inflammatory) after high in-tensity exercise [120], and modulation of micro-RNAs has been observed in healthy subjects following 12 weeks of high intensity exercise [146] indicating an anti-inflammatory response to high intensity exercise. Therefore, exercise therapy might benefit patients with e.g., poor quality of sleep, high inflammation, and widespread hyperalgesia.
Similar, the function of descending pain inhibitory control is believed to rely on serotonin and noradrenaline [17,20]. CPM is assumed to be the human proxy for the assessment of de-scending pain inhibitory control [237]. Duloxetine is a serotonin-noradrenaline reuptake in-hibitory, and duloxetine was recently recommended by the OARSI for OA pain treatment for patients with widespread pain and/or depression [21]. Patients with diabetic neuropathies and impaired patients have been found to respond well to four weeks of duloxetine, and CPM seems to be restored after pain relieving duloxetine treatment [241]. Studies have found that a subset of knee OA patients display impaired CPM compared with healthy subjects [11,15] or other OA patients [164]. A recent RCT [110] administrated pre- and postoperative duloxetine to pain sensitive knee OA patients scheduled for TKA and found this to reduce pain intensities at postoperative week 6 and 12 compared with placebo. This study needs further validation, but could be another example of how a targeted effort towards pain mechanisms might im-prove the treatments in future.
References
51
REFERENCES [1] Aasvang EK, Gmaehle E, Hansen JB, Gmaehle B, Forman JL, Schwarz J, Bittner R,
Kehlet H. Predictive Risk Factors for Persistent Postherniotomy Pain. Anesthesiology 2010;112:957–969.
[2] Ackerman IN, Bohensky MA, de Steiger R, Brand CA, Eskelinen A, Fenstad AM, Furnes O, Garellick G, Graves SE, Haapakoski J, Havelin LI, Mäkelä K, Mehnert F, Pedersen AB, Robertsson O. Substantial rise in the lifetime risk of primary total knee replacement surgery for osteoarthritis from 2003 to 2013: an international, population-level anal-ysis. Osteoarthr Cartil 2017;25:455–461.
[3] Ackerman IN, Bohensky MA, Zomer E, Tacey M, Gorelik A, Brand CA, de Steiger R. The projected burden of primary total knee and hip replacement for osteoarthritis in Australia to the year 2030. BMC Musculoskelet Disord 2019;20:90–99.
[4] Ahn DK, Choi HS, Yeo SP, Woo YW, Lee MK, Yang GY, Jeon HJ, Park JS, Mokha SS. Blockade of central cyclooxygenase (COX) pathways enhances the cannabinoid-in-duced antinociceptive effects on inflammatory temporomandibular joint (TMJ) noci-ception. Pain 2007;132:23–32.
[5] Andersen HH, Duroux M, Gazerani P. Serum MicroRNA Signatures in Migraineurs During Attacks and in Pain-Free Periods. Mol Neurobiol 2016;53:1494–1500.
[6] Andersen HH, Imai Y, Petersen KK, Koenig J, Elberling J, Arendt-Nielsen L. Conditioning pain stimulation does not affect itch induced by intra-epidermal histamine pricks but aggravates neurogenic inflammation in healthy volunteers. Somatosens Mot Res 2016;33:49–60.
[7] Andersen KG, Duriaud HM, Kehlet H, Aasvang EK. The Relationship Between Sensory Loss and Persistent Pain 1 Year After Breast Cancer Surgery. J Pain 2017;18:1129–1138.
[8] Arendt-Nielsen L, Egsgaard LL, Petersen KK. Evidence for a central mode of action for etoricoxib (COX-2 inhibitor) in patients with painful knee osteoarthritis. Pain 2016;157:1634–1644.
[9] Arendt-Nielsen L, Egsgaard LL, Petersen KK, Eskehave TN, Graven- Nielsen T, Hoeck HC, Simonsen O. A mechanism-based pain sensitivity index to characterize knee osteoarthritis patients with different disease stages and pain levels. Eur J Pain 2015;19:1406–1417.
[10] Arendt-Nielsen L, Graven-Nielsen T. Translational musculoskeletal pain research. Best Pract Res Rheumatol 2011;25:209–226.
[11] Arendt-Nielsen L, Morlion B, Perrot S, Dahan A, Dickenson A, Kress HG, Wells C, Bouhassira D, Mohr Drewes A. Assessment and manifestation of central sensitisation across different chronic pain conditions. Eur J Pain 2018;22:216–241.
Mechanistic Pain Profiling of Patients with Osteoarthritis
52
[12] Arendt-Nielsen L, Nie H, Laursen MB, Laursen BS, Madeleine P, Simonsen OH, Graven-Nielsen T. Sensitization in patients with painful knee osteoarthritis. Pain 2010;149:573–581.
[13] Arendt-Nielsen L, Petersen KK. Chapter 8: Assessing Joint Pain Experimentally in Humans. In: Arendt-Nielsen L, Perrot S, editors. Pain in the Joints. IASP press, 2016.
[14] Arendt-Nielsen L, Simonsen O, Laursen MB, Roos EM, Rathleff MS, Rasmussen S, Skou ST. Pain and sensitization after total knee replacement or nonsurgical treatment in patients with knee osteoarthritis: Identifying potential predictors of outcome at 12 months. Eur J Pain 2018;22:1088–1102.
[15] Arendt-Nielsen L, Skou ST, Nielsen TA, Petersen KK. Altered Central Sensitization and Pain Modulation in the CNS in Chronic Joint Pain. Curr Osteoporos Rep 2015;13:225–234.
[16] Arendt-Nielsen L, Perrot S. Pain in the Joints. 1st ed. 2017.
[17] Bannister K, Dickenson AH. The plasticity of descending controls in pain: translational probing. J Physiol 2017;595:4159–4166.
[18] Bannister K, Dickenson AH. What the brain tells the spinal cord. Pain 2016;157:2148–2151.
[19] Bannister K, Lockwood S, Goncalves L, Patel R, Dickenson AH. An investigation into the inhibitory function of serotonin in diffuse noxious inhibitory controls in the neu-ropathic rat. Eur J Pain 2017;21:750–760.
[20] Bannister K, Patel R, Goncalves L, Townson L, Dickenson AH. Diffuse noxious inhibitory controls and nerve injury: restoring an imbalance between descending monoamine inhibitions and facilitations. Pain 2015;156:1803–11.
[21] Bannuru RR, Osani MC, Vaysbrot EE, Arden NK, Bennell K, Bierma-Zeinstra SMA, Kraus VB, Lohmander LS, Abbott JH, Bhandari M, Blanco FJ, Espinosa R, Haugen IK, Lin J, Mandl LA, Moilanen E, Nakamura N, Snyder-Mackler L, Trojian T, Underwood M, McAlindon TE. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr Cartil 2019;27:1578–1589.
[22] Baranoff J, Hanrahan SJ, Connor JP. The roles of acceptance and catastrophizing in rehabilitation following anterior cruciate ligament reconstruction. J Sci Med Sport 2015;18:250–4.
[23] Le Bars D, Dickenson AH, Besson JM. Diffuse noxious inhibitory controls (DNIC). I. Effects on dorsal horn convergent neurones in the rat. Pain 1979;6:283–304.
[24] Bennell KL, Nelligan RK, Rini C, Keefe FJ, Kasza J, French S, Forbes A, Dobson F, Abbott JH, Dalwood A, Harris A, Vicenzino B, Hodges PW, Hinman RS. Effects of internet-based
References
53
pain coping skills training before home exercise for individuals with hip osteoarthritis (HOPE trial): a randomised controlled trial. Pain 2018;159:1833–1842.
[25] Berenbaum F, Wallace IJ, Lieberman DE, Felson DT. Modern-day environmental factors in the pathogenesis of osteoarthritis. Nat Rev Rheumatol 2018;14:674–681.
[26] Beswick AD, Wylde V, Gooberman-Hill R, Blom A, Dieppe P. What proportion of pa-tients report long-term pain after total hip or knee replacement for osteoarthri-tis? A systematic review of prospective studies in unselected patients. BMJ Open 2012;2:e000435–e000435.
[27] Beyer C, Zampetaki A, Lin N-Y, Kleyer A, Perricone C, Iagnocco A, Distler A, Langley SR, Gelse K, Sesselmann S, Lorenzini R, Niemeier A, Swoboda B, Distler JHW, Santer P, Egger G, Willeit J, Mayr M, Schett G, Kiechl S. Signature of circulating microRNAs in osteoarthritis. Ann Rheum Dis 2015;74:e18–e18.
[28] Bijlsma JWJ, Berenbaum F, Lafeber FPJG. Osteoarthritis: an update with relevance for clinical practice. Lancet (London, England) 2011;377:2115–26.
[29] Birch S, Stilling M, Mechlenburg I, Hansen TB. No effect of cognitive behavioral patient education for patients with pain catastrophizing before total knee arthroplasty: a ran-domized controlled trial. Acta Orthop 2020;91:98–103.
[30] Birch S, Stilling M, Mechlenburg I, Reinholdt MB, Hansen TB. Association between pain catastrophizing, physical function and pain at first visit in the outpatient knee clinic. Knee 2019:8–13.
[31] Bonica JJ. The Management of Pain. Philadelphia: Lea & Febiger, 1953.
[32] Bossmann T, Brauner T, Wearing S, Horstmann T. Predictors of chronic pain follow-ing total knee replacement in females and males: an exploratory study. Pain Manag 2017;7:391–403.
[33] Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur J Pain 2006;10:287–333.
[34] Broderick JE, Keefe FJ, Bruckenthal P, Junghaenel DU, Schneider S, Schwartz JE, Kaell AT, Caldwell DS, McKee D, Reed S, Gould E. Nurse practitioners can effectively deliver pain coping skills training to osteoarthritis patients with chronic pain: A randomized, controlled trial. Pain 2014;155:1743–54.
[35] Brummett C, Clauw D, Harris R, Harte S, Hassett A, Williams D. We agree with the need for a new term but disagree with the proposed terms. Pain 2016;157:2876.
[36] Campbell CM, Buenaver LF, Finan P, Bounds SC, Redding M, McCauley L, Robinson M, Edwards RR, Smith MT. Sleep, Pain Catastrophizing, and Central Sensitization in
Mechanistic Pain Profiling of Patients with Osteoarthritis
54
Knee Osteoarthritis Patients With and Without Insomnia. Arthritis Care Res (Hoboken) 2015;67:1387–1396.
[37] Carr AJ, Robertsson O, Graves S, Price AJ, Arden NK, Judge A, Beard DJ. Knee replace-ment. Lancet (London, England) 2012;379:1331–40.
[38] Chapman V, Dickenson AH. The combination of NMDA antagonism and morphine pro-duces profound antinociception in the rat dorsal horn. Brain Res 1992;573:321–3.
[39] Churov A V., Oleinik EK, Knip M. MicroRNAs in rheumatoid arthritis: Altered expression and diagnostic potential. Autoimmun Rev 2015;14:1029–1037.
[40] Citrome L, Weiss–Citrome A. A Systematic Review of Duloxetine for Osteoarthritic Pain: What is the Number Needed to Treat, Number Needed to Harm, and Likelihood to be Helped or Harmed? Postgrad Med 2012;124:83–93.
[41] Crea F, Watahiki A, Quagliata L, Xue H, Pikor L, Parolia A, Wang YY, Lin D, Lam WL, Farrar WL, Isogai T, Morant R, Castori-Eppenberger S, Chi KN, Wang YY, Helgason CD. Identification of a long non-coding RNA as a novel biomarker and potential therapeu-tic target for metastatic prostate cancer. Oncotarget 2014;5:764–74.
[42] Culliford DJ, Maskell J, Beard DJ, Murray DW, Price AJ, Arden NK. Temporal trends in hip and knee replacement in the United Kingdom: 1991 to 2006. J Bone Joint Surg Br 2010;92:130–5.
[43] Cummins TM, Kucharczyk M, Graven-Nielsen T, Bannister K. Activation of the descend-ing pain modulatory system using cuff pressure algometry: Back translation from man to rat. Eur J Pain 2020;24:1330–1338.
[44] Demant DT, Lund K, Finnerup NB, Vollert J, Maier C, Segerdahl MS, Jensen TS, Sindrup SH. Pain relief with lidocaine 5% patch in localized peripheral neuropathic pain in re-lation to pain phenotype: a randomised, double-blind, and placebo-controlled, phe-notype panel study. Pain 2015;156:2234–44.
[45] Demant DT, Lund K, Vollert J, Maier C, Segerdahl M, Finnerup NB, Jensen TS, Sindrup SH. The effect of oxcarbazepine in peripheral neuropathic pain depends on pain phe-notype: A randomised, double-blind, placebo-controlled phenotype-stratified study. Pain 2014;155:2263–2273.
[46] Dieppe P, Cushnaghan J, Tucker M, Browning S, Shepstone L. The Bristol ‘OA500 study’: progression and impact of the disease after 8 years. Osteoarthr Cartil 2000;8:63–68.
[47] Dieppe P, Lohmander L. Pathogenesis and management of pain in osteoarthritis. Lancet 2005;365:965–973.
[48] Dieppe PA, Cushnaghan J, Shepstone L. The Bristol ‘OA500’ Study: progression of
References
55
osteoarthritis (OA) over 3 years and the relationship between clinical and radiographic changes at the knee joint. Osteoarthr Cartil 1997;5:87–97.
[49] Doherty M, Hawkey C, Goulder M, Gibb I, Hill N, Aspley S, Reader S. A randomised con-trolled trial of ibuprofen, paracetamol or a combination tablet of ibuprofen/ paraceta-mol in community-derived people with knee pain. Ann Rheum Dis 2011;70:1534–1541.
[50] Duan W, Du L, Jiang X, Wang R, Yan S, Xie Y, Yan K, Wang Q, Wang L, Zhang X, Pan H, Yang Y, Wang C. Identification of a serum circulating lncRNA panel for the diagnosis and recurrence prediction of bladder cancer. Oncotarget 2016;7:78850–78858.
[51] Dworkin RH, Peirce-Sandner S, Turk DC, McDermott MP, Gibofsky A, Simon LS, Farrar JT, Katz NP. Outcome measures in placebo-controlled trials of osteoarthritis: responsive-ness to treatment effects in the REPORT database. Osteoarthr Cartil 2011;19:483–92.
[52] Dyck PJ, Zimmerman I, Gillen DA, Johnson D, Karnes JL, O’Brien PC. Cool, warm, and heat-pain detection thresholds: testing methods and inferences about anatomic dis-tribution of receptors. Neurology 1993;43:1500–8.
[53] Edwards RR, Dolman AJ, Martel MO, Finan PH, Lazaridou A, Cornelius M, Wasan AD. Variability in conditioned pain modulation predicts response to NSAID treatment in patients with knee osteoarthritis. BMC Musculoskelet Disord 2016;17:284–292.
[54] Edwards RR, Dolman AJ, Michna E, Katz JN, Nedeljkovic SS, Janfaza D, Isaac Z, Martel MO, Jamison RN, Wasan AD. Changes in pain sensitivity and pain modulation dur-ing oral opioid treatment: The impact of negative affect. Pain Med (United States) 2016;17:1882–1891.
[55] Edwards RR, Grace E, Peterson S, Klick B, Haythornthwaite JA, Smith MT. Sleep con-tinuity and architecture: Associations with pain-inhibitory processes in patients with temporomandibular joint disorder. Eur J Pain 2009;13:1043–1047.
[56] Edwards RR, Haythornthwaite J a, Tella P, Max MB, Raja S. Basal heat pain thresh-olds predict opioid analgesia in patients with postherpetic neuralgia. Anesthesiology 2006;104:1243–8.
[57] Edwards RR, Wasan AD, Michna E, Greenbaum S, Ross E, Jamison RN. Elevated pain sensitivity in chronic pain patients at risk for opioid misuse. J Pain 2011;12:953–963.
[58] Egsgaard LL indhardt, Eskehave TN avndrup, Bay-Jensen AC, Hoeck HC hristian, Arendt-Nielsen L. Identifying specific profiles in patients with different degrees of painful knee osteoarthritis based on serological biochemical and mechanistic pain biomarkers: a diagnostic approach based on cluster analysis. Pain 2015;156:96–107.
[59] Eitner A, Pester J, Vogel F, Marintschev I, Lehmann T, Hofmann GO, Schaible H-G. Pain sensation in human osteoarthritic knee joints is strongly enhanced by diabetes melli-tus. Pain 2017;158:1743–1753.
Mechanistic Pain Profiling of Patients with Osteoarthritis
56
[60] Felson DT. The sources of pain in knee osteoarthritis. Curr Opin Rheumatol 2005;17:624–628.
[61] Felson DT, Lawrence RC, Dieppe PA, Hirsch R, Helmick CG, Jordan JM, Kington RS, Lane NE, Nevitt MC, Zhang Y, Sowers M, McAlindon T, Spector TD, Poole AR, Yanovski SZ, Ateshian G, Sharma L, Buckwalter JA, Brandt KD, Fries JF. Osteoarthritis: New insights - Part 1: The disease and its risk factors. Ann Intern Med 2000;133:635–646.
[62] Finocchietti S, Nielsen M, Mørch CD, Arendt-Nielsen L, Graven-Nielsen T. Pressure-induced muscle pain and tissue biomechanics: A computational and experimental study. Eur J Pain 2011;15:36–44.
[63] Fleiss JL. Reliability of measurement. Des Anal Clin Exp 1986:1–32.
[64] Forsythe ME, Dunbar MJ, Hennigar AW, Sullivan MJL, Gross M. Prospective relation between catastrophizing and residual pain following knee arthroplasty: two-year fol-low-up. Pain Res Manag 2008;13:335–41.
[65] Gandhi R, Santone D, Takahashi M, Dessouki O, Mahomed NN. Inflammatory predictors of ongoing pain 2 years following knee replacement surgery. Knee 2013;20:316–318.
[66] Gaskin DJ, Richard P. The Economic Costs of Pain in the United States. J Pain 2012;13:715–724.
[67] Giordano R, Petersen KK, Andersen HH, Lichota J, Simonsen OH, Arendt-Nielsen L. MicroRNAs expression as circulating genomic biomarkers in patients with chronic postoperative pain after total knee replacement. MicroRNAs expression as circulat-ing genomic biomarkers in patients with chronic postoperative pain after total knee replacement. 17th World Congress on Pain, IASP 2018 - Boston, MA, USA, 2018.
[68] Giordano R, Petersen KK, Andersen HH, Lichota J, Valeriani M, Simonsen O, Arendt-Nielsen L. Preoperative serum circulating microRNAs as potential biomarkers for chronic postoperative pain after total knee replacement. Mol Pain 2020;16:174480692096292.
[69] Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health 2011;11:770–774.
[70] van de Graaf VA, Noorduyn JCA, Willigenburg NW, Butter IK, de Gast A, Mol BW, Saris DBF, Twisk JWR, Poolman RW, ESCAPE Research Group. Effect of Early Surgery vs Physical Therapy on Knee Function Among Patients With Nonobstructive Meniscal Tears: The ESCAPE Randomized Clinical Trial. JAMA 2018;320:1328–1337.
[71] Graham GG, Davies MJ, Day RO, Mohamudally A, Scott KF. The modern pharmacology of paracetamol: Therapeutic actions, mechanism of action, metabolism, toxicity and recent pharmacological findings. Inflammopharmacology 2013;21:201–232.
References
57
[72] Granan L-P. We do not need a third mechanistic descriptor for chronic pain states! Not yet. Pain 2017;158:179.
[73] Granot M, Lowenstein L, Yarnitsky D, Tamir A, Zimmer EZ. Postcesarean Section Pain Prediction by Preoperative Experimental Pain Assessment. Anesthesiology 2003;98:1422–1426.
[74] Grässel S. The role of peripheral nerve fibers and their neurotransmitters in cartilage and bone physiology and pathophysiology. Arthritis Res Ther 2014;16:485–497.
[75] Graven-Nielsen T. Fundamentals of muscle pain, referred pain, and deep tissue hyper-algesia. Scand J Rheumatol Suppl 2006;122:1–43.
[76] Graven-Nielsen T, Arendt-Nielsen L. Assessment of mechanisms in localized and wide-spread musculoskeletal pain. Nat Rev Rheumatol 2010;6:599–606.
[77] Graven-Nielsen T, Arendt-Nielsen L, Svensson P, Jensen TS. Stimulus-response func-tions in areas with experimentally induced referred muscle pain--a psychophysical study. Brain Res 1997;744:121–8.
[78] Graven-Nielsen T, Babenko V, Svensson P, Arendt-Nielsen L. Experimentally induced muscle pain induces hypoalgesia in heterotopic deep tissues, but not in homotopic deep tissues. Brain Res 1998;787:203–10.
[79] Graven-Nielsen T, Izumi M, Petersen KK, Arendt-Nielsen L. User-independent as-sessment of conditioning pain modulation by cuff pressure algometry. Eur J Pain 2017;21:552–561.
[80] Graven-Nielsen T, Kendall SA, Henriksson KG, Bengtsson M, Sörensen J, Johnson A, Gerdle B, Arendt-Nielsen L. Ketamine reduces muscle pain, temporal summation, and referred pain in fibromyalgia patients. Pain 2000;85:483–491.
[81] Graven-Nielsen T, Wodehouse T, Langford RM, Arendt-Nielsen L, Kidd BL. Normalization of widespread hyperesthesia and facilitated spatial summation of deep-tissue pain in knee osteoarthritis patients after knee replacement. Arthritis Rheum 2012;64:2907–2916.
[82] Grill JD, Coghill RC. Transient analgesia evoked by noxious stimulus offset. J Neurophysiol 2002;87:2205–8.
[83] Gureje O, Von Korff M, Kola L, Demyttenaere K, He Y, Posada-Villa J, Lepine JP, Angermeyer MC, Levinson D, de Girolamo G, Iwata N, Karam A, Borges GLG, de Graaf R, Browne MO, Stein DJ, Haro JM, Bromet EJ, Kessler RC, Alonso J. The relation be-tween multiple pains and mental disorders: Results from the World Mental Health Surveys. Pain 2008;135:82–91.
[84] Hadlandsmyth K, Sabic E, Zimmerman MB, Sluka KA, Herr KA, Clark CR, Noiseux NO,
Mechanistic Pain Profiling of Patients with Osteoarthritis
58
Callaghan JJ, Geasland KM, Embree JL, Rakel BA. Relationships among pain intensity, pain-related distress, and psychological distress in pre-surgical total knee arthroplasty patients: a secondary analysis. Psychol Health Med 2017;22:552–563.
[85] Hannan MT, Felson DT, Pincus T. Analysis of the discordance between radiographic changes and knee pain in osteoarthritis of the knee. J Rheumatol 2000;27:1513–1517.
[86] Hansen S, Dalgaard RC, Mikkelsen PS, Sørensen MB, Petersen KK. Modulation of Exercise-Induced Hypoalgesia Following an Exercise Intervention in Healthy Subjects. Pain Med 2020;Ahead of p.
[87] Hansen S, Vaegter HB, Petersen KK. Pretreatment Exercise-induced Hypoalgesia is Associated With Change in Pain and Function After Standardized Exercise Therapy in Painful Knee Osteoarthritis. Clin J Pain 2020;36:16–24.
[88] Hermans L, Calders P, Van Oosterwijck J, Verschelde E, Bertel E, Meeus M. An Overview of Offset Analgesia and the Comparison with Conditioned Pain Modulation: A Systematic Literature Review. Pain Physician 2016;19:307–26.
[89] Hill CL, Hunter DJ, Niu J, Clancy M, Guermazi A, Genant H, Gale D, Grainger A, Conaghan P, Felson DT. Synovitis detected on magnetic resonance imaging and its relation to pain and cartilage loss in knee osteoarthritis. AnnRheum Dis 2007;66:1599–1603.
[90] Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, McGowan J, Towheed T, Welch V, Wells G, Tugwell P. American College of Rheumatology 2012 recommenda-tions for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res 2012;64:465–474.
[91] Van Den Houte M, Van Oudenhove L, Bogaerts K, Van Diest I, Van den Bergh O. Endogenous Pain Modulation: Association with Resting Heart Rate Variability and Negative Affectivity. Pain Med 2018;19:1587–1596.
[92] Hunter DJ, Guermazi A, Roemer F, Zhang Y, Neogi T. Structural correlates of pain in joints with osteoarthritis. Osteoarthr Cartil 2013;21:1170–1178.
[93] Imai Y, Petersen KK, Mørch CD, Arendt Nielsen L. Comparing test–retest reliability and magnitude of conditioned pain modulation using different combinations of test and conditioning stimuli. Somatosens Mot Res 2016;33:169–177.
[94] Iordanova Schistad E, Kong XY, Furberg A-S, Bäckryd E, Grimnes G, Emaus N, Rosseland LA, Gordh T, Stubhaug A, Engdahl B, Halvorsen B, Nielsen CS. A population-based study of inflammatory mechanisms and pain sensitivity. Pain 2020;161:338–350.
[95] Irwin MR, Olmstead R, Carroll JE. Sleep Disturbance, Sleep Duration, and Inflammation: A Systematic Review and Meta-Analysis of Cohort Studies and Experimental Sleep Deprivation. Biol Psychiatry 2016;80:40–52.

References
59
[96] Izumi M, Petersen KK, Laursen MB, Arendt-Nielsen L, Graven-Nielsen T. Facilitated temporal summation of pain correlates with clinical pain intensity after hip arthro-plasty. Pain 2017;158:323–332.
[97] Jaacks LM, Vandevijvere S, Pan A, McGowan CJ, Wallace C, Imamura F, Mozaffarian D, Swinburn B, Ezzati M. The obesity transition: stages of the global epidemic. Lancet Diabetes Endocrinol 2019;7:231–240.
[98] Jakorinne P, Haanpää M, Arokoski J. Reliability of pressure pain, vibration detection, and tactile detection threshold measurements in lower extremities in subjects with knee osteoarthritis and healthy controls. Scand J Rheumatol 2018;47:491–500.
[99] Jarrell J, Ross S, Robert M, Wood S, Tang S, Stephanson K, Giamberardino MA. Prediction of postoperative pain after gynecologic laparoscopy for nonacute pelvic pain. Am J Obstet Gynecol 2014;211:360.e1-360.e8.
[100] Jordan KM, Arden NK, Doherty M, Bannwarth B, Bijlsma JWJ, Dieppe P, Gunther K, Hauselmann H, Herrero-Beaumont G, Kaklamanis P, Lohmander S, Leeb B, Lequesne M, Mazieres B, Martin-Mola E, Pavelka K, Pendleton A, Punzi L, Serni U, Swoboda B, Verbruggen G, Zimmerman-Gorska I, Dougados M. EULAR Recommendations 2003: An evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis 2003;62:1145–1155.
[101] Kellgren JH, Lawrence JS. Radiological Assessment of Osteo-Arthrosis. Ann Rheum Dis 1957;16:494–502.
[102] Kennedy DL, Kemp HI, Ridout D, Yarnitsky D, Rice AS. Reliability of conditioned pain modulation. Pain 2016;157:2410–2419.
[103] Kennedy DL, Kemp HI, Wu C, Ridout DA, Rice ASC. Determining Real Change in Conditioned Pain Modulation: A Repeated Measures Study in Healthy Volunteers. J Pain 2020;21:708–721.
[104] Khan M, Evaniew N, Bedi A, Ayeni OR, Bhandari M. Arthroscopic surgery for degener-ative tears of the meniscus: a systematic review and meta-analysis. Can Med Assoc J 2014;186:1057–64.
[105] Kim H-A, Kim S, Seo YI, Choi HJ, Seong S-C, Song YW, Hunter D, Zhang Y. The epidemi-ology of total knee replacement in South Korea: national registry data. Rheumatology 2008;47:88–91.
[106] King CD, Sibille KT, Goodin BR, Cruz-Almeida Y, Glover TL, Bartley E, Riley JL, Herbert MS, Sotolongo A, Schmidt J, Fessler BJ, Redden DT, Staud R, Bradley LA, Fillingim RB. Experimental pain sensitivity differs as a function of clinical pain severity in sympto-matic knee osteoarthritis. Osteoarthritis Cartilage 2013;21:1243–52.
Mechanistic Pain Profiling of Patients with Osteoarthritis
60
[107] Kisler LB, Weissman-Fogel I, Coghill RC, Sprecher E, Yarnitsky D, Granovsky Y. Individualization of Migraine Prevention. Clin J Pain 2019;35:753–765.
[108] Klyne DM, Moseley GL, Sterling M, Barbe MF, Hodges PW. Individual Variation in Pain Sensitivity and Conditioned Pain Modulation in Acute Low Back Pain: Effect of Stimulus Type, Sleep, and Psychological and Lifestyle Factors. J Pain 2018;19:942.e1-942.e18.
[109] Koenig J, Jarczok MN, Ellis RJ, Hillecke TK, Thayer JF. Heart rate variability and experi-mentally induced pain in healthy adults: A systematic review. Eur J Pain 2013;18:1–14.
[110] Koh IJ, Kim MS, Sohn S, Song KY, Choi NY, In Y. Duloxetine Reduces Pain and Improves Quality of Recovery Following Total Knee Arthroplasty in Centrally Sensitized Patients. J Bone Jt Surg 2019;101:64–73.
[111] Koo TK, Li MY. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J Chiropr Med 2016;15:155–163.
[112] Kosek E, Cohen M, Baron R, Gebhart GF, Mico JA, Rice ASC, Rief W, Sluka AK. Do we need a third mechanistic descriptor for chronic pain states? Pain 2016;157:1382–1386.
[113] Kosek E, Ordeberg G. Lack of pressure pain modulation by heterotopic noxious con-ditioning stimulation in patients with painful osteoarthritis before, but not following, surgical pain relief. Pain 2000;88:69–78.
[114] Kuni B, Wang H, Rickert M, Ewerbeck V, Schiltenwolf M. Pain threshold correlates with functional scores in osteoarthritis patients. Acta Orthop 2014;86:1–5.
[115] Kurien T, Arendt-Nielsen L, Petersen KK, Graven-Nielsen T, Scammell BE. Preoperative Neuropathic Pain-like Symptoms and Central Pain Mechanisms in Knee Osteoarthritis Predicts Poor Outcome 6 Months After Total Knee Replacement Surgery. J Pain 2018;19:1329–1341.
[116] Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J bone Jt Surg 2007;89:780–5.
[117] Larsen DB, Mogens L, Edwards RR, Simonsen OH, Lars A-N, Petersen KK. The com-bination of preoperative pain, conditioned pain modulation, and pain catastrophiz-ing predicts postoperative pain 12 months after total knee arthroplasty. Pain Med 2020;Accepted.
[118] Laursen RJ, Graven-Nielsen T, Jensen TS, Arendt-Nielsen L. Quantification of local and referred pain in humans induced by intramuscular electrical stimulation. Eur J Pain 1997;1:105–13.
[119] Leinders M, Üçeyler N, Thomann A, Sommer C. Aberrant microRNA expression in pa-tients with painful peripheral neuropathies. J Neurol Sci 2017;380:242–249.

References
61
[120] Leung A, Gregory NS, Allen L-AH, Sluka K. Regular physical activity prevents chronic pain by altering resident muscle macrophage phenotype and increasing interleukin-10 in mice. Pain 2016;157:70–9.
[121] Li Q, Shao Y, Zhang X, Zheng T, Miao M, Qin L, Wang B, Ye G, Xiao B, Guo J. Plasma long noncoding RNA protected by exosomes as a potential stable biomarker for gastric cancer. Tumor Biol 2015;36:2007–2012.
[122] Lockwood SM, Bannister K, Dickenson AH. An investigation into the noradrenergic and serotonergic contributions of diffuse noxious inhibitory controls in a monoiodoacetate model of osteoarthritis. J Neurophysiol 2019;121:96–104.
[123] Longo DL. Personalized Medicine for Primary Treatment of Serous Ovarian Cancer. N Engl J Med 2019;381:2471–2474.
[124] Lundblad H, Kreicbergs A, Jansson K. Prediction of persistent pain after total knee re-placement for osteoarthritis. J Bone Jt Surg 2008;90-B:166–171.
[125] Lunn TH, Gaarn-Larsen L, Kehlet H. Prediction of postoperative pain by preoperative pain response to heat stimulation in total knee arthroplasty. Pain 2013;154:1878–85.
[126] Luo Z-Y, Li L-L, Wang D, Wang H-Y, Pei F-X, Zhou Z-K. Preoperative sleep quality affects postoperative pain and function after total joint arthroplasty: a prospective cohort study. J Orthop Surg Res 2019;14:378–387.
[127] Mainka T, Malewicz NM, Baron R, Enax-Krumova EK, Treede R-D, Maier C. Presence of hyperalgesia predicts analgesic efficacy of topically applied capsaicin 8% in patients with peripheral neuropathic pain. Eur J Pain 2016;20:116–129.
[128] Malfait A-M, Schnitzer TJ. Towards a mechanism-based approach to pain management in osteoarthritis. Nat Rev Rheumatol 2013;9:654–64.
[129] Manafi Khanian B, Arendt-Nielsen L, Kjær Petersen K, Samani A, Graven-Nielsen T. Interface Pressure Behavior During Painful Cuff Algometry. Pain Med 2016;17:915–23.
[130] Marcuzzi A, Wrigley PJ, Dean CM, Adams R, Hush JM. The long-term reliabili-ty of static and dynamic quantitative sensory testing in healthy individuals. Pain 2017;158:1217–1223.
[131] Martel MO, Petersen K, Cornelius M, Arendt-Nielsen L, Edwards R. Endogenous Pain Modulation Profiles Among Individuals With Chronic Pain: Relation to Opioid Use. J Pain 2019;20:462–471.
[132] Martinez V, Fletcher D, Bouhassira D, Sessler DI, Chauvin M. The evolution of primary hyperalgesia in orthopedic surgery: quantitative sensory testing and clinical evaluation before and after total knee arthroplasty. Anesth Analg 2007;105:815–21.
Mechanistic Pain Profiling of Patients with Osteoarthritis
62
[133] Martini C, van Velzen M, Drewes A, Aarts L, Dahan A, Niesters M. A Randomized Controlled Trial on the Effect of Tapentadol and Morphine on Conditioned Pain Modulation in Healthy Volunteers. PLoS One 2015;10:e0128997.
[134] Martucci KT, Eisenach JC, Tong C, Coghill RC. Opioid-independent mechanisms sup-porting offset analgesia and temporal sharpening of nociceptive information. Pain 2012;153:1232–1243.
[135] McAlindon TE, LaValley MP, Harvey WF, Price LL, Driban JB, Zhang M, Ward RJ. Effect of intra-articular triamcinolone vs saline on knee cartilage volume and pain in patients with knee osteoarthritis a randomized clinical trial. JAMA 2017;317:1967–1975.
[136] McMahon SB, Koltzenburg M. Textbook of Pain. Fifth edit. 2006.
[137] McPhee ME, Vaegter HB, Graven-Nielsen T. Alterations in pronociceptive and antino-ciceptive mechanisms in patients with low back pain: a systematic review with me-ta-analysis. Pain 2020;161:464–475.
[138] Merskey H, Bogduk N. Classification of Chronic Pain—Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms. 1995.
[139] Michael T. Smith, Robert R. Edwards, Una D. McCann JAH. The Effects of Sleep Deprivation on Pain Inhibition and Spontaneous Pain in Women. 2007;30:494–505.
[140] Moloney N, Rabey M, Nijs J, Hush J, Slater H. Support for extended classification of pain states. Pain 2017;158:1395.
[141] Moss P, Benson HAE, Will R, Wright A. Patients With Knee Osteoarthritis Who Score Highly on the PainDETECT Questionnaire Present With Multimodality Hyperalgesia, Increased Pain, and Impaired Physical Function. Clin J Pain 2018;34:15–21.
[142] Moss P, Knight E, Wright A. Subjects with Knee Osteoarthritis Exhibit Widespread Hyperalgesia to Pressure and Cold. PLoS One 2016;11:e0147526.
[143] Nahman-Averbuch H, Martucci KT, Granovsky Y, Weissman-Fogel I, Yarnitsky D, Coghill RC. Distinct brain mechanisms support spatial vs temporal filtering of nociceptive in-formation. Pain 2014;155:2491–2501.
[144] Nakano N, Shoman H, Olavarria F, Matsumoto T, Kuroda R, Khanduja V. Why are pa-tients dissatisfied following a total knee replacement? A systematic review. Int Orthop 2020;44:1971–2007.
[145] Neziri AY, Limacher A, Jüni P, Radanov BP, Andersen OK, Arendt-Nielsen L, Curatolo M. Ranking of Tests for Pain Hypersensitivity According to Their Discriminative Ability in Chronic Neck Pain. Reg Anesth Pain Med 2013;38:308–320.
[146] Nielsen S, Åkerström T, Rinnov A, Yfanti C, Scheele C, Pedersen BK, Laye MJ. The miRNA
References
63
Plasma Signature in Response to Acute Aerobic Exercise and Endurance Training. PLoS One 2014;9:e87308.
[147] Niesters M, Dahan A, Swartjes M, Noppers I, Fillingim RB, Aarts L, Sarton EY. Effect of ket-amine on endogenous pain modulation in healthy volunteers. Pain 2011;152:656–63.
[148] Niu J, Zhang YQ, Torner J, Nevitt M, Lewis CE, Aliabadi P, Sack B, Clancy M, Sharma L, Felson DT. Is obesity a risk factor for progressive radiographic knee osteoarthritis? Arthritis Rheum 2009;61:329–335.
[149] Noiseux NO, Callaghan JJ, Clark CR, Zimmerman MB, Sluka KA, Rakel BA. Preoperative Predictors of Pain Following Total Knee Arthroplasty. J Arthroplasty 2014;29:1383–1387.
[150] O’Brien AT, Deitos A, Triñanes Pego Y, Fregni F, Carrillo-de-la-Peña MT. Defective Endogenous Pain Modulation in Fibromyalgia: A Meta-Analysis of Temporal Summation and Conditioned Pain Modulation Paradigms. J Pain 2018;19:819–836.
[151] Odgaard A. The Danish Knee Arthroplasty Register (DHR), National Annual Report. 2018.
[152] Odgaard A. The Danish Knee Arthroplasty Register 2019 Report. 2019.
[153] Odole A, Ekediegwu E, Ekechukwu END, Uchenwoke C. Correlates and predictors of pain intensity and physical function among individuals with chronic knee osteoarthritis in Nigeria. Musculoskelet Sci Pract 2019;39:150–156.
[154] Olesen SS, Graversen C, Bouwense SAW, van Goor H, Wilder-Smith OHG, Drewes AM. Quantitative Sensory Testing Predicts Pregabalin Efficacy in Painful Chronic Pancreatitis. PLoS One 2013;8:e57963.
[155] De Oliveira Silva D, Rathleff MS, Petersen K, Azevedo FM de, Barton CJ. Manifestations of Pain Sensitization Across Different Painful Knee Disorders: A Systematic Review Including Meta-analysis and Metaregression. Pain Med 2019;20:335–358.
[156] Ong CKS, Seymour RA, Lirk P, Merry AF. Combining Paracetamol (Acetaminophen) with Nonsteroidal Antiinflammatory Drugs: A Qualitative Systematic Review of Analgesic Efficacy for Acute Postoperative Pain. Anesth Analg 2010;110:1170–9.
[157] Overgaard S. The Danish Hip Arthroplasty Register (DHR), National Annual Report. 2018.
[158] OʼLeary H, Smart KM, Moloney NA, Blake C, Doody CM. Pain sensitization associat-ed with nonresponse after physiotherapy in people with knee osteoarthritis. Pain 2018;159:1877–1886.
[159] Pan PH, Coghill R, Houle TT, Seid MH, Lindel WM, Parker RL, Washburn SA, Harris L,
Mechanistic Pain Profiling of Patients with Osteoarthritis
64
Eisenach JC. Multifactorial Preoperative Predictors for Postcesarean Section Pain and Analgesic Requirement. Anesthesiology 2006;104:417–425.
[160] Pas HI, Winters M, Haisma HJ, Koenis MJ, Tol JL, Moen MH. Stem cell injec-tions in knee osteoarthritis: a systematic review of the literature. Br J Sports Med 2017;51:1125–1133.
[161] Paul-Savoie E, Marchand S, Morin M, Bourgault P, Brissette N, Rattanavong V, Cloutier C, Bissonnette A, Potvin S. Is the deficit in pain inhibition in fibromyalgia influenced by sleep impairments? Open Rheumatol J 2012;6:296–302.
[162] Petersen KK, Arendt-Nielsen L. Chronic postoperative pain after joint replacement. Pain Clin Updat 2016;24.
[163] Petersen KK, Arendt-Nielsen L, Simonsen O, Wilder-Smith O, Laursen MB. Presurgical assessment of temporal summation of pain predicts the development of chronic post-operative pain 12 months after total knee replacement. Pain 2015;156:55–61.
[164] Petersen KK, Graven-Nielsen T, Simonsen O, Laursen MB, Arendt-Nielsen L. Preoperative pain mechanisms assessed by cuff algometry are associated with chronic postoperative pain relief after total knee replacement. Pain 2016;157:1400–1406.
[165] Petersen KK, McPhee ME, Hoegh MS, Graven-Nielsen T. Assessment of conditioned pain modulation in healthy participants and patients with chronic pain: manifestations and implications for pain progression. Curr Opin Support Palliat Care 2019;13:99–106.
[166] Petersen KK, Olesen AE, Simonsen O, Arendt-Nielsen L. Mechanistic pain profiling as a tool to predict the efficacy of 3-week nonsteroidal anti-inflammatory drugs plus par-acetamol in patients with painful knee osteoarthritis. Pain 2019;160:486–492.
[167] Petersen KK, Simonsen O, Laursen MB, Arendt-Nielsen L. The Role of Preoperative Radiologic Severity, Sensory Testing, and Temporal Summation on Chronic Postoperative Pain Following Total Knee Arthroplasty. Clin J Pain 2018;34:193–197.
[168] Petersen KK, Simonsen O, Laursen MB, Nielsen TA, Rasmussen S, Arendt-Nielsen L. Chronic Postoperative Pain After Primary and Revision Total Knee Arthroplasty. Clin J Pain 2015;31:1–6.
[169] Petersen KK, Simonsen O, Olesen AE, Mørch CD, Arendt-Nielsen L. Pain inhibitory mechanisms and response to weak analgesics in patients with knee osteoarthritis. Eur J Pain 2019;23:1904–1912.
[170] Petersen KK, Vaegter HB, Stubhaug A, Wolff A, Scammell BE, Arendt-Nielsen L, Larsen DB. The predictive value of quantitative sensory testing. Pain 2020;Publish Ahead of Print.
[171] Pham T, van der Heijde D, Altman RD, Anderson JJ, Bellamy N, Hochberg M, Simon
References
65
L, Strand V, Woodworth T, Dougados M. OMERACT-OARSI initiative: Osteoarthritis Research Society International set of responder criteria for osteoarthritis clinical trials revisited. Osteoarthr Cartil 2004;12:389–99.
[172] Pihl K, Ensor J, Peat G, Englund M, Lohmander S, Jørgensen U, Nissen N, Fristed JV, Thorlund JB. Wild goose chase - no predictable patient subgroups benefit from me-niscal surgery: patient-reported outcomes of 641 patients 1 year after surgery. Br J Sports Med 2020;54:13–22.
[173] Pinto P, McIntyre T, Araujo-Soares V, Ferro R, Almeida A. The role of pain catastro-phizing in the provision of rescue analgesia by health care providers following major joint arthroplasty. Pain Physician n.d.;17:515–24.
[174] Pinto PR, McIntyre T, Araújo-Soares V, Almeida A, Costa P. Psychological factors pre-dict an unfavorable pain trajectory after hysterectomy. Pain 2018;159:956–967.
[175] Pinto PR, McIntyre T, Araújo-Soares V, Costa P, Almeida A. Differential predictors of acute post-surgical pain intensity after abdominal hysterectomy and major joint ar-throplasty. Ann Behav Med 2015;49:384–97.
[176] Powezka K, Adjei T, von Rosenberg W, Normahani P, Goverdovsky V, Standfield NJ, Mandic DP, Jaffer U. A pilot study of preoperative heart rate variability predicting pain during local anesthetic varicose vein surgery. J Vasc Surg Venous Lymphat Disord 2019;7:382–386.
[177] Price DD, Hu JW, Dubner R, Gracely RH. Peripheral suppression of first pain and central summation of second pain evoked by noxious heat pulses. Pain 1977;3:57–68.
[178] Price DD, Mao J, Frenk H, Mayer DJ. The N-methyl-D-aspartate receptor antagonist dextromethorphan selectively reduces temporal summation of second pain in man. Pain 1994;59:165–174.
[179] Price DD, Staud R, Robinson ME, Mauderli AP, Cannon R, Vierck CJ. Enhanced temporal summation of second pain and its central modulation in fibromyalgia patients. Pain 2002;99:49–59.
[180] Ram KC, Eisenberg E, Haddad M, Pud D. Oral opioid use alters DNIC but not cold pain perception in patients with chronic pain - New perspective of opioid-induced hyper-algesia. Pain 2008;139:431–438.
[181] Ran J, Yang X, Ren Z, Wang J, Dong H. Comparison of intra-articular hyaluronic acid and methylprednisolone for pain management in knee osteoarthritis: A meta-analysis of randomized controlled trials. Int J Surg 2018;53:103–110.
[182] Reid KJ, Baron KG, Lu B, Naylor E, Wolfe L, Zee PC. Aerobic exercise improves self-report-ed sleep and quality of life in older adults with insomnia. Sleep Med 2010;11:934–940.
Mechanistic Pain Profiling of Patients with Osteoarthritis
66
[183] Reinold H, Ahmadi S, Depner UB, Layh B, Heindl C, Hamza M, Pahl A, Brune K, Narumiya S, M??ller U, Zeilhofer HU. Spinal inflammatory hyperalgesia is mediated by prosta-glandin E receptors of the EP2 subtype. J Clin Invest 2005;115:673–679.
[184] Ren K. Wind-up and the NMDA receptor: from animal studies to humans. Pain 1994;59:157–158.
[185] Reyes C, Leyland KM, Peat G, Cooper C, Arden NK, Prieto-Alhambra D. Association Between Overweight and Obesity and Risk of Clinically Diagnosed Knee, Hip, and Hand Osteoarthritis: A Population-Based Cohort Study. Arthritis Rheumatol 2016;68:1869–1875.
[186] Rice DA, Kluger MT, McNair PJ, Lewis GN, Somogyi AA, Borotkanics R, Barratt DT, Walker M. Persistent postoperative pain after total knee arthroplasty: a prospective cohort study of potential risk factors. Br J Anaesth 2018;121:804–812.
[187] Riddle D, Keefe F, Nay W, McKee D, Attarian D, Jensen M. Pain Coping Skills Training for Patients with Elevated Pain Catastrophizing who are Scheduled for knee Artroplasty: A Quasi-experimental Study. Natl Inst Heal 2011;92:859–865.
[188] Riddle DL, Keefe FJ, Ang D, J K, Dumenci L, Jensen MP, Bair MJ, Reed SD, Kroenke K. A phase III randomized three-arm trial of physical therapist delivered pain coping skills training for patients with total knee arthroplasty: the KASTPain protocol. BMC Musculoskelet Disord 2012;20:149–159.
[189] Riddle DL, Keefe FJ, Ang DC, Slover J, Jensen MP, Bair MJ, Kroenke K, Perera RA, Reed SD, McKee D, Dumenci L. Pain Coping Skills Training for Patients Who Catastrophize About Pain Prior to Knee Arthroplasty: A Multisite Randomized Clinical Trial. J Bone Joint Surg Am 2019;101:218–227.
[190] Riddle DL, Wade JB, Jiranek WA, Kong X. Preoperative pain catastrophizing predicts pain outcome after knee arthroplasty. Clin Orthop Relat Res 2010;468:798–806.
[191] Riis A, Rathleff MS, Jensen MB, Simonsen O. Low grading of the severity of knee oste-oarthritis pre-operatively is associated with a lower functional level after total knee replacement: a prospective cohort study with 12 months’ follow-up. Bone Joint J 2014;96-B:1498–502.
[192] Robertsson O, Bizjajeva S, Fenstad AM, Furnes O, Lidgren L, Mehnert F, Odgaard A, Pedersen AB, Havelin LI. Knee arthroplasty in Denmark, Norway and Sweden. Acta Orthop 2010;81:82–89.
[193] Robinson WH, Lepus CM, Wang Q, Raghu H, Mao R, Lindstrom TM, Sokolove J. Low-grade inflammation as a key mediator of the pathogenesis of osteoarthritis. Nat Rev Rheumatol 2016;12:580–592.
[194] Rolke R, Baron R, Maier C, Tolle TR, Treede RD, Beyer A, Binder A, Birbaumer N,
References
67
Birklein F, Botefur IC, Braune S, Flor H, Huge V, Klug R, Landwehrmeyer GB, Magerl W, Maihofner C, Rolko C, Schaub C, Scherens A, Sprenger T, Valet M, Wasserka B. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): standardized protocol and reference values.[Erratum appears in Pain. 2006 Nov;125(1-2):197]. Pain 2006;123:231–243.
[195] Rolke R, Magerl W, Campbell KA, Schalber C, Caspari S, Birklein F, Treede RD. Quantitative sensory testing: A comprehensive protocol for clinical trials. Eur J Pain 2006;10:77–88.
[196] Roos EM, Juhl CB. Osteoarthritis 2012 year in review: Rehabilitation and outcomes. Osteoarthr Cartil 2012;20:1477–1483.
[197] Ruscheweyh R, Viehoff A, Tio J, Pogatzki-Zahn EM. Psychophysical and psychological predictors of acute pain after breast surgery differ in patients with and without pre-ex-isting chronic pain. Pain 2017;158:1030–1038.
[198] Safiri S, Kolahi A-A, Smith E, Hill C, Bettampadi D, Mansournia MA, Hoy D, Ashrafi-Asgarabad A, Sepidarkish M, Almasi-Hashiani A, Collins G, Kaufman J, Qorbani M, Moradi-Lakeh M, Woolf AD, Guillemin F, March L, Cross M. Global, regional and na-tional burden of osteoarthritis 1990-2017: a systematic analysis of the Global Burden of Disease Study 2017. Ann Rheum Dis 2020;79:819–828.
[199] Sangesland A, Støren C, Vaegter HB. Are preoperative experimental pain assessments correlated with clinical pain outcomes after surgery? A systematic review. Scand J Pain 2017;15:44–52.
[200] Schaible H-G. Nociceptive neurons detect cytokines in arthritis. Arthritis Res Ther 2014;16:470–478.
[201] Schistad EI, Stubhaug A, Furberg AS, Engdahl BL, Nielsen CS. C-reactive protein and cold-pressor tolerance in the general population: The Tromsø Study. Pain 2017;158:1280–1288.
[202] Siebuhr AS, Petersen KK, Arendt-Nielsen L, Egsgaard LL, Eskehave T, Christiansen C, Simonsen O, Hoeck HC, Karsdal MA, Bay-Jensen AC. Identification and characterisation of osteoarthritis patients with inflammation derived tissue turnover. Osteoarthr Cartil 2014;22:44–50.
[203] Singh JA. Epidemiology of knee and hip arthroplasty: a systematic review. Open Orthop J 2011;5:80–5.
[204] Singh JA, Vessely MB, Harmsen WS, Schleck CD, Melton LJ, Kurland RL, Berry DJ. A population-based study of trends in the use of total hip and total knee arthroplasty, 1969-2008. Mayo Clin Proc 2010;85:898–904.
[205] Sinikallio SH, Helminen E-E, Valjakka AL, Väisänen-Rouvali RH, Arokoski JP. Multiple
Mechanistic Pain Profiling of Patients with Osteoarthritis
68
Psychological Factors Are Associated With Poorer Functioning in a Sample of Community-Dwelling Knee Osteoarthritis Patients. JCR J Clin Rheumatol 2014;20:261–267.
[206] Skou ST, Graven-Nielsen T, Rasmussen S, Simonsen OH, Laursen MB, Arendt-Nielsen L. Facilitation of pain sensitization in knee osteoarthritis and persistent post-operative pain: A cross-sectional study. Eur J Pain 2014;18:1024–1031.
[207] Skou ST, Graven-Nielsen T, Rasmussen S, Simonsen OH, Laursen MB, Arendt-Nielsen L. Widespread sensitization in patients with chronic pain after revision total knee ar-throplasty. Pain 2013;154:1588–1594.
[208] Skou ST, Roos EM. Physical therapy for patients with knee and hip osteoarthritis: su-pervised, active treatment is current best practice. Clin Exp Rheumatol n.d.;37 Suppl 1:112–117.
[209] Skou ST, Roos EM, Laursen MB, Rathleff MS, Arendt-Nielsen L, Simonsen O. A Randomized, Controlled Trial of Total Knee Replacement. N Engl J Med 2015;373:1597–1606.
[210] Sng BL, Ching YY, Han NLR, Ithnin FB, Sultana R, Assam PN, Sia ATH. Incidence and association factors for the development of chronic post-hysterectomy pain at 4- and 6-month follow-up: A prospective cohort study. J Pain Res 2018;11:629–636.
[211] Somers TJ, Blumenthal JA, Guilak F, Kraus VB, Schmitt DO, Babyak MA, Craighead LW, Caldwell DS, Rice JR, McKee DC, Shelby RA, Campbell LC, Pells JJ, Sims EL, Queen R, Carson JW, Connelly M, Dixon KE, Lacaille LJ, Huebner JL, Rejeski WJ, Keefe FJ. Pain coping skills training and lifestyle behavioral weight management in patients with knee osteoarthritis: a randomized controlled study. Pain 2012;153:1199–209.
[212] Somers TJ, Keefe FJ, Pells JJ, Dixon KE, Waters SJ, Riordan PA, Blumenthal JA, McKee DC, LaCaille L, Tucker JM, Schmitt D, Caldwell DS, Kraus VB, Sims EL, Shelby RA, Rice JR. Pain catastrophizing and pain-related fear in osteoarthritis patients: relationships to pain and disability. J Pain Symptom Manage 2009;37:863–72.
[213] Sommer C, Leinders M, Üçeyler N. Inflammation in the pathophysiology of neuropathic pain. Pain 2018;159:595–602.
[214] Srimurugan Pratheep N, Madeleine P, Arendt-Nielsen L. Relative and absolute test-re-test reliabilities of pressure pain threshold in patients with knee osteoarthritis. Scand J pain 2018;18:229–236.
[215] Staffe AT, Bech MW, Clemmensen SLK, Nielsen HT, Larsen DB, Petersen KK. Total sleep deprivation increases pain sensitivity, impairs conditioned pain modulation and facili-tates temporal summation of pain in healthy participants. PLoS One 2019;14:e0225849.
[216] Stanaway JD et al. Global, regional, and national comparative risk assessment of 84 be-havioural, environmental and occupational, and metabolic risks or clusters of risks for
References
69
195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Stu. Lancet 2018;392:1923–1994.
[217] Staud R, Cannon RC, Mauderli AP, Robinson ME, Price DD, Vierck Jr. CJ. Temporal sum-mation of pain from mechanical stimulation of muscle tissue in normal controls and subjects with fibromyalgia syndrome. Pain 2003;102:87–95.
[218] Strulov L, Zimmer EZ, Granot M, Tamir A, Jakobi P, Lowenstein L. Pain catastrophiz-ing, response to experimental heat stimuli, and post-cesarean section pain. J Pain 2007;8:273–9.
[219] Suokas A, Walsh D, McWilliams D, Condon L, Moreton B, Wylde V, Arendt-Nielsen L, Zhang W. Quantitative sensory testing in painful osteoarthritis: a systematic review and meta-analysis (Structured abstract). Osteoarthr Cartil 2012;20:1075–1085.
[220] Thorlund JB, Juhl CB, Roos EM, Lohmander LS. Arthroscopic surgery for degen-erative knee: systematic review and meta-analysis of benefits and harms. BMJ 2015;350:h2747–h2747.
[221] Traxler J, Hanssen MM, Lautenbacher S, Ottawa F, Peters ML. General versus pain-specific cognitions: Pain catastrophizing but not optimism influences conditioned pain modulation. Eur J Pain 2019;23:150–159.
[222] Treede R-D, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, Cohen M, Evers S, Finnerup NB, First MB, Giamberardino MA, Kaasa S, Kosek E, Lavandʼhomme P, Nicholas M, Perrot S, Scholz J, Schug S, Smith BH, Svensson P, Vlaeyen JWS, Wang S-J. A classifica-tion of chronic pain for ICD-11. Pain 2015;156:1003–7.
[223] Vaegter HB, Graven-Nielsen T. Pain modulatory phenotypes differentiate subgroups with different clinical and experimental pain sensitivity. Pain 2016;157:1480–1488.
[224] Vaegter HB, Handberg G, Emmeluth C, Graven-Nielsen T. Preoperative Hypoalgesia After Cold Pressor Test and Aerobic Exercise is Associated With Pain Relief 6 Months After Total Knee Replacement. Clin J Pain 2017;33:475–484.
[225] Vaegter HB, Lyng KD, Yttereng FW, Christensen MH, Sørensen MB, Graven-Nielsen T. Exercise-Induced Hypoalgesia After Isometric Wall Squat Exercise: A Test-Retest Reliabilty Study. Pain Med 2019;20:129–137.
[226] Vollert J, Attal N, Baron R, Freynhagen R, Haanpää M, Hansson P, Jensen TS, Rice ASC, Segerdahl M, Serra J, Sindrup SH, Tölle TR, Treede R-D, Maier C. Quantitative sensory testing using DFNS protocol in Europe: an evaluation of heterogeneity across multi-ple centers in patients with peripheral neuropathic pain and healthy subjects. Pain 2016;157:750–8.
[227] Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, Carter A, Casey DC, Charlson
Mechanistic Pain Profiling of Patients with Osteoarthritis
70
FJ, Chen AZ, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388:1545–1602.
[228] Wallis JA, Taylor NF. Pre-operative interventions (non-surgical and non-pharmacolog-ical) for patients with hip or knee osteoarthritis awaiting joint replacement surgery--a systematic review and meta-analysis. Osteoarthr Cartil 2011;19:1381–95.
[229] Wang G, Bi L, Li X, Li Z, Zhao D, Chen J, He D, Wang C-N, Wu T, Dueñas H, Skljarevski V, Yue L. Maintenance of effect of duloxetine in Chinese patients with pain due to osteoarthritis: 13-week open-label extension data. BMC Musculoskelet Disord 2019;20:174–182.
[230] Weissman-Fogel I, Granovsky Y, Crispel Y, Ben-Nun A, Best LA, Yarnitsky D, Granot M. Enhanced presurgical pain temporal summation response predicts post-thoracotomy pain intensity during the acute postoperative phase. J Pain 2009;10:628–636.
[231] Weissman-Fogel I, Sprecher E, Granovsky Y, Yarnitsky D. Repeated noxious stimula-tion of the skin enhances cutaneous pain perception of migraine patients in-between attacks: clinical evidence for continuous sub-threshold increase in membrane excita-bility of central trigeminovascular neurons. Pain 2003;104:693–700.
[232] Weissman-Fogel I, Sprecher E, Pud D. Effects of catastrophizing on pain perception and pain modulation. Exp Brain Res 2008;186:79–85.
[233] Wilder-Smith OH. A paradigm-shift in pain medicine. Aalborg: Center for Sensory-Motor Interaction (SMI), Department of Health Science and Technology, Aalborg University, 2013.
[234] Wilder-Smith OH, Schreyer T, Scheffer GJ, Arendt-Nielsen L. Patients with chron-ic pain after abdominal surgery show less preoperative endogenous pain inhibition and more postoperative hyperalgesia: a pilot study. J Pain Palliat Care Pharmacother 2010;24:119–28.
[235] Wylde V, Palmer S, Learmonth ID, Dieppe P. The association between pre-operative pain sensitisation and chronic pain after knee replacement: An exploratory study. Osteoarthr Cartil 2013;21:1253–1256.
[236] Wylde V, Sayers A, Lenguerrand E, Gooberman-Hill R, Pyke M, Beswick AD, Dieppe P, Blom AW. Preoperative widespread pain sensitization and chronic pain after hip and knee replacement. Pain 2015;156:47–54.
[237] Yarnitsky D. Conditioned pain modulation (the diffuse noxious inhibitory control-like effect): its relevance for acute and chronic pain states. Curr Opin Anaesthesiol 2010;23:611–615.
References
71
[238] Yarnitsky D, Arendt-Nielsen L, Bouhassira D, Edwards RR, Fillingim RB, Granot M, Hansson P, Lautenbacher S, Marchand S, Wilder-Smith O. Recommendations on ter-minology and practice of psychophysical DNIC testing. Eur J Pain 2010;14:339–339.
[239] Yarnitsky D, Bouhassira D, Drewes AM, Fillingim RB, Granot M, Hansson P, Landau R, Marchand S, Matre D, Nilsen KB, Stubhaug A, Treede RD, Wilder-Smith OHG. Recommendations on practice of conditioned pain modulation (CPM) testing. Eur J Pain 2015;19:805–806.
[240] Yarnitsky D, Crispel Y, Eisenberg E, Granovsky Y, Ben-Nun A, Sprecher E, Best LA, Granot M. Prediction of chronic post-operative pain: Pre-operative DNIC testing identifies pa-tients at risk. Pain 2008;138:22–28.
[241] Yarnitsky D, Granot M, Nahman-Averbuch H, Khamaisi M, Granovsky Y. Conditioned pain modulation predicts duloxetine efficacy in painful diabetic neuropathy. Pain 2012;153:1193–1198.
[242] Youngstedt SD, Kline CE. Epidemiology of exercise and sleep. Sleep Biol Rhythms 2006;4:215–221.
[243] Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, Bierma-Zeinstra S, Brandt KD, Croft P, Doherty M, Dougados M, Hochberg M, Hunter DJ, Kwoh K, Lohmander LS, Tugwell P. OARSI recommendations for the management of hip and knee osteoarthritis, Part I: Critical appraisal of existing treatment guidelines and sys-tematic review of current research evidence. Osteoarthr Cartil 2007;15:981–1000.
[244] Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, Bierma-Zeinstra S, Brandt KD, Croft P, Doherty M, Dougados M, Hochberg M, Hunter DJ, Kwoh K, Lohmander LS, Tugwell P. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthr Cartil 2008;16:137–162.