mdg progress report 2015 - wpro | who western pacific · pdf file · 2017-05-18mdg...
TRANSCRIPT

MDGProgressReport2015
ProgressandtransitionofHealth-relatedMDGstoSDGsinLaoPDR

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |1
OverviewAt the beginning of the new millennium, world leaders gathered at the United Nations to developquantified targets for addressing extremepoverty in itsmany dimensions; theMillenniumDevelopmentGoals (MDGs).With thehelpofmanydifferentpartners,everycountry is responsible forachievingeightspecificgoals.Theyear2015marksthefinalimplementationyearfortheMDGsandactsasanintroductionand launchingyearforthenewlydevelopedSustainableDevelopmentGoals (SDGs).ThefollowingreportwillfocusontheprogressofallhealthrelatedMDGsinLaoPDR.
Thehealth sector in LaoPDR is responsible for theachievementof three specificMDGgoals, namely toreducechildmortality(MDG4),toimprovematernalhealth(MDG5),andtocombatHIV/AIDS,malariaandotherdiseases(MDG6).Inaddition,thehealthsectorisalsodirectlyconnectedtoonetargetfromMDG1(to halve the proportion of people suffering from hunger) and one target from MDG 7 (to halve theproportionofpeoplewithoutsustainableaccess tosafedrinkingwaterandbasicsanitation)asaccess tosafewaterandsanitationfallsunderthemandateof theMinistryofHealth inLaoPDRduetothedirectconsequencesthatithasonthehealthrelatedwell-beingofthepopulation.
This report reflects joined efforts by the Government of Lao PDR in collaborationwith awide range ofdevelopment partners. In addition to the Ministry of Health, bilateral development partners,intergovernmental organizations, and international as well as national non-governmental organizations(NGOs)playacrucialroleinreachingouttothenecessarytargetpopulationsinordertoachievetheMDGs.Civil society organizations are amajor force in reaching themost vulnerable population, often living inremote rural areas. This community engagement is also important in reaching out to different ethnicgroups and to develop cultural sensitive approaches on development including health and hygienepromotion. Figure1:OverallhealthrelatedMDGtargetsOverall, Lao PDR has made somesignificant changes and has achieved sixout of the nine health related targets. Asseen in figure 1, Lao PDR successfullyreduced child mortality of under-5-year-olds by two-thirds, reduced maternalmortality by three-quarters, halted andreversed the spread of malaria and TB,halved the proportion of the populationwithout improveddrinkingwater inurbanareas and halved the proportion of thepopulation without sanitation in urbanareas.Asforthetargetofreducinghungerbyhalf,haltingandreversingthespreadofHIV/AIDS, and achieving universal accesstoHIV/AIDStreatmentforthoseinneed,

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |2
LaoPDRisontrack,yetcomesshorttoachievingthetargets.
Despite thesenotable improvements,major challenges remain including the access to health services inremoteareasandforvulnerablegroups,thequalityofservicesandtheprotectionagainsthealthshocks.AccordingtoWorldBank’ssystematiccountrydiagnosisforLaoPDR,healthshocksconstituteamainfactorforfallingbackintopoverty.Atthesametime,lessthan15%ofthepoorhavehealthinsurance.1Themostcommon problems facing the service delivery system are the excessive patient loads at the central andprovinciallevels,andtheunder-useofdistrictandcommunitylevelfacilities.Asaconsequence,inorderforLao PDR to continue progressing towards amore improved health sector, it is essential to increase theemphasis on policies andmeasures that increase the access of themost vulnerable groups to services,livelihoodsandresources.
It is important tomention that the following summary reportwill draw on statistics and data collectedthroughdifferentchannels,suchasHMIS,LaoSocialIndicatorSurvey(LSIS),UNjointestimates,andotherWHOandUNglobalreports.Assuch,somedatamightvarydependingontheestimatethat itoriginatesfrom.Moreover,anewLSISisintheprocessofbeingplannedandconductedwithinthenextyear,whichwillprovideadditionalandupdatedvaluesforsomeofthecurrentlyestimatedindicators.SUSTAINABLEDEVELOPMENTGOALS(SDGs)
2015markedthetargetyear forachievingtheMDGgoalsandtheSDGsmonitoringwillbe implementedfrom2016onwards.The2030SustainableDevelopmentAgendaisofunprecedentedscopeandambitionand goes well beyond the MDGs. While poverty eradication, health, education, and food security andnutrition remain priorities, the Sustainable Development Goals (SDGs) comprise a broad range ofeconomic, social and environmental objectives, and offer the prospect of more peaceful and inclusivesocieties.
TheSDGsarecomposedof17goalsand169targetsallevolvingaroundasustainabledevelopmentforthepeopleandtheplanet,prosperity,peaceandpartnership.Oneofthe17goals(SDG3)isspecificallyhealthrelatedandsetsouttoensurehealthylivesandpromotewell-beingforallatallages.Its13targetsbuildonprogressmadeontheMDGsandreflectanewfocusonnon-communicablediseasesandtheachievementofuniversalhealthcoverage.ThemajorityofhealthrelatedSDGtargetsandgoalsarereflectedinnationalpoliciessuchasthe8thHSDP.
At the timeof this reportbeingprepared,LaoPDR is still in theprocessofdefining theappropriateSDGindicatorsforthecountry.TheywillbebasedontheMDGindicatorsandattempttocontinuetomaintainthemomentumthatthepreviousdevelopmentindicatorshavehad.Nevertheless,itiscertainthatinorderforLaoPDRtoachievehealthrelatedSDGtargetsfurtheradditional investments inthehealthsectorarerequired.PublicspendingonhealthinLaosremainsverylowandhealthserviceprovisioncontinuestorelyon out of pocket spending and external financing.Without sufficient financial allocations it will not be
1WorldHealthStatistics2015,WHO2015
T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |3
possible to achieve resilienthealth systemsanduniversal health coverageby theproposednational andinternationaldeadlines.
StronghealthsystemswillbethebasisfortheachievementofallhealthrelatedSDGsandwillensurethatpreviousprogressundertheMDGagendaisnotputatrisk.TheintegratedapproachtodevelopmentoftheSDGsrequiresacoordinatedandholisticapproachbygovernmentstoimplementtheagenda.NCDs,roadsafety, and environmental health are emerging challenges which will require strong commitment tomobilize the joint efforts required across government agencies andwithin other sectors to achieve theambitioustargetssetwithintheSDGs.AnactiverolebytheMinistryofHealthtoensurehealthisreflectedinallpoliciesaswellasMoHtakinga leadingroleoncrosssector issueswhichfallunderthemandateoftheMoH such aswater and sanitation,will be important to support Laos’ efforts towardsachieving theSDGs.
SustainableDevelopmentGoals(SDGs)2
2UnitedNations,http://www.un.org/sustainabledevelopment/sustainable-development-goals/
T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |4
COUNTRYCOMPARISON
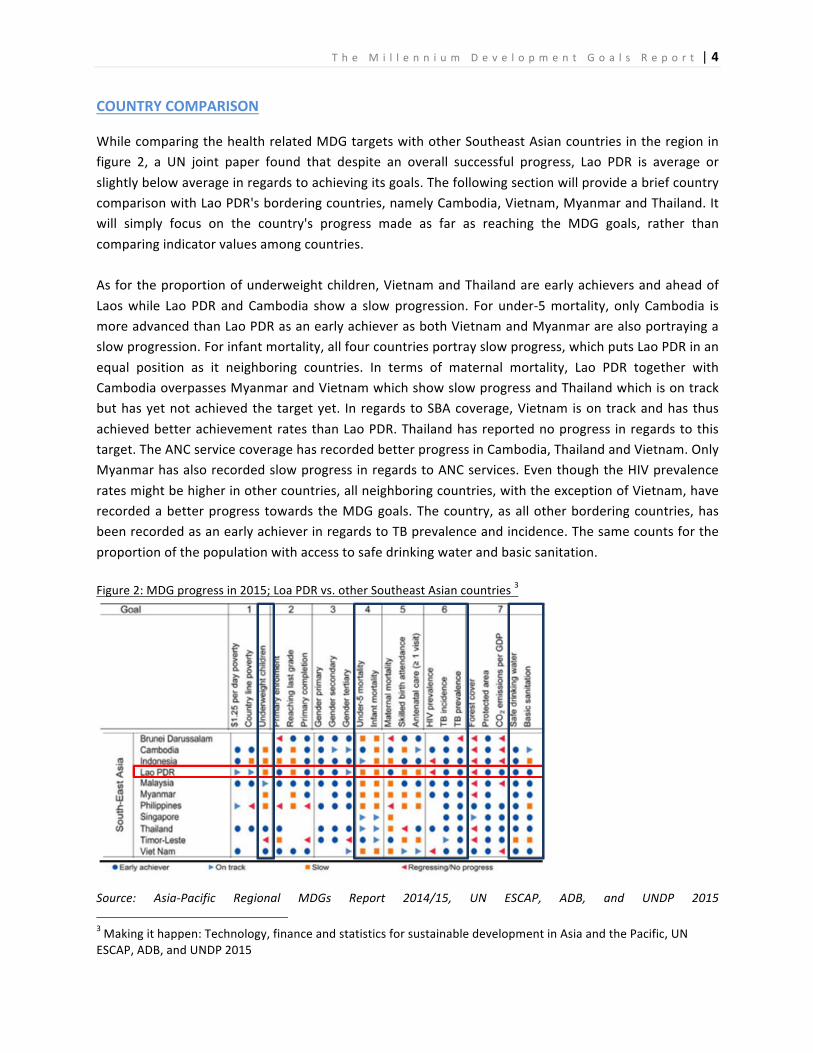
WhilecomparingthehealthrelatedMDGtargetswithotherSoutheastAsiancountriesintheregioninfigure 2, a UN joint paper found that despite an overall successful progress, Lao PDR is average orslightlybelowaverageinregardstoachievingitsgoals.ThefollowingsectionwillprovideabriefcountrycomparisonwithLaoPDR'sborderingcountries,namelyCambodia,Vietnam,MyanmarandThailand.Itwill simply focus on the country's progress made as far as reaching the MDG goals, rather thancomparingindicatorvaluesamongcountries.Asfortheproportionofunderweightchildren,VietnamandThailandareearlyachieversandaheadofLaoswhile Lao PDR andCambodia showa slowprogression. For under-5mortality, only Cambodia ismoreadvancedthanLaoPDRasanearlyachieverasbothVietnamandMyanmararealsoportrayingaslowprogression.Forinfantmortality,allfourcountriesportrayslowprogress,whichputsLaoPDRinanequal position as it neighboring countries. In terms of maternal mortality, Lao PDR together withCambodiaoverpassesMyanmarandVietnamwhichshowslowprogressandThailandwhichisontrackbuthasyetnotachievedthetargetyet. InregardstoSBAcoverage,VietnamisontrackandhasthusachievedbetterachievementratesthanLaoPDR.Thailandhasreportednoprogress inregardstothistarget.TheANCservicecoveragehasrecordedbetterprogressinCambodia,ThailandandVietnam.OnlyMyanmarhasalsorecordedslowprogressinregardstoANCservices.EventhoughtheHIVprevalenceratesmightbehigherinothercountries,allneighboringcountries,withtheexceptionofVietnam,haverecordedabetterprogress towards theMDGgoals.Thecountry,asallotherborderingcountries,hasbeenrecordedasanearlyachieverinregardstoTBprevalenceandincidence.Thesamecountsfortheproportionofthepopulationwithaccesstosafedrinkingwaterandbasicsanitation.Figure2:MDGprogressin2015;LoaPDRvs.otherSoutheastAsiancountries3
Source: Asia-Pacific Regional MDGs Report 2014/15, UN ESCAP, ADB, and UNDP 20153Makingithappen:Technology,financeandstatisticsforsustainabledevelopmentinAsiaandthePacific,UNESCAP,ADB,andUNDP2015

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |5
MDG 1: ERADICATE EXTREME POVERTY AND HUNGER
PovertyratesinLaoPDR
Prevalence of underweightchildrenunder5
• By2013,LaoPDRhadalreadyachievedtheMDG1ofhalvingits national poverty rate from 46 % in 1992/93 to 23 % by2012/13i.
• Despite a successful decline in the overall poverty rate,inequalitieshaveincreased,whichcan,amongothers,beseenin the distribution and access to of health services andfinancing.
• FoodinsecurityremainsachallengeinLaoPDR,withone-fifthof the population consuming less than theminimum dietaryenergyrequirementsii.
• Theoverallprevalenceofunderweightandstuntinginchildrenunder five has decreased, yet projections for 2015 have notbeen published and thus uncertainty prevails whether MDGtargets have been reached.
TargetC:Halvetheproportionofpeoplewhosufferfromhunger
Figure3:Prevalenceofstuntedandunderweightchildren
Source:HMIS,LaoPDRMoH2015
As fortarget1C, figure3showsthat there has been a decreasein the prevalence ofunderweight children under-5as well as stunting in childrenunder-5 from 44% and 48% in1995 respectively, to 27% and38% in2010.Nodatahasbeenrecorded or been estimatedfrom 2010 to 2015 yet; thusuncertainty prevails whetherthe national MDG targets of22% and 34% have beenachieved. Both rates remainrelatively high and furtherpolicies should continue to beimplemented in order toachieve additional progress inthe post 2015 agenda.
48
4240
38
4440
37
27
0
10
20
30
40
50
60
1995 2000 2005 2010
Prevalenceofstuntingchildrenunder5
Prevalenceofunderweightchildrenunder5
Linear(Prevalenceofstuntingchildrenunder5)
Linear(Prevalenceofunderweightchildrenunder5)
MDG

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |6
AsmeasuredbytheGlobalHungerIndex,LaoPDRstillsuffersfromconsiderablyhighlevelsofhungerasit hasbeenestimated thatone-fifthof the total population consumes less than theminimumdietaryrequirements4.Especially in regards to child nutrition, strong inequalities exists across regions andgroups,whichcanoftenbeassociatedwithpovertylevelsandthelevelsofeducationamongmothers.Othercausesofchildundernutritionandinadequatefoodandnutrientintakeincludepoorfeedingandcare practices, infectious diseases, poor maternal health and nutrition, adolescent pregnancy, foodinsecurity and poor dietary practices, poor hygiene practices, unsafe water and sanitation, andweaknessesinservicedelivery5.
BylaunchingtheNationalZeroHungerChallengeinMay2015,LaoPDRhasreaffirmeditscommitmentto fight hunger and undernutrition. In order to achieve the Zero Hunger Challenge and increase theoverall health of the population and address the challengesmentioned above, theNationalNutritionStrategyandPlanofAction(NNSPA)wasprolongedforthe2016-2020periodbytheMoH.Thestrategybuilds on the previous nutrition strategy and forms the basis for implementing food security andnutritioninterventionsandistooperateinassociationwiththeNationalSocio-EconomicDevelopmentStrategy (NSEDS) to 2020. It seeks to end hunger, achieve food security and improved nutrition andpromotesustainableagriculture6.
4Thestateoffoodinsecurityintheworld2015,FAO20155LaoPDR:TheMillenniumDevelopmentGoalsandLessonsLearntforthePost-2015Period:ASummaryReview,UN,20156NationalNutritionStrategyandPlanofAction2016-2020,MinistryofHealth2015

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |7
MDG4:REDUCECHILDMORTALITY
Under-5 Mortality rate 1995 vs.2015
Vaccinecoverage2010vs2015
• LaoPDRhasreacheditsnationaltargetofreducingunder-5 mortality to 70/1,000 births. In 2015, the under-5mortality rate was 67/1,000 according to the UN JointEstimates.
• The infantmortality rate has decreased to 45/1,000, andthusalsoachievestheprojectedtargetof45/1,000.
• With the exception of DPT-Hep3, Lao PDR has seen anincrease in vaccine coverage over the past five years.Nevertheless,therehavebeenmultiplediseaseoutbreaksover the past years, which in overall requires furthereffortstoensureamoresustainablecoverage.
• Most of the child deaths in Lao PDR are preventable or treatable with high impact cost-effective interventions, but coverage and quality of maternal and child health care services in Lao PDR are still low. iii
Target4A:Reducebytwo-thirdstheunder-5mortalityrate
LaoPDRhasreacheditsnationaltargetofreducingunder-5mortalityto70/1,000births.In2015,under-5mortality reached 67/1,000 (UN Joint Estimates). The infantmortality rate has reached 45/1,000, andthusalsoachievestheprojectedtargetof45/1,000.Sincethedataiscollectedthroughdifferentsurveysanddatasystems,onemustbecarefulwhilecomparingthedataonayeartoyearbasisasitisimpossibletodetermineadefinitetrendbutonlygetsanoverallidea.Despite of reaching the national target, Lao PDR has failed to achieve the international targets ofreducingchildmortalityratestoone-thirdof1990levels,whichwouldbearound57/1,000and38/1,000.Policies have been introduced in 2015 to address this challenge and bring Lao PDR up to achieveinternational targets.

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |8
Figure5:MDG:Under-5andinfantmortalityrates
Source: LSIS 2011, HMIS 2015 & UN Joint Estimates 2015
Figure6:VaccineCoveragefrom2010to2015Reducing child mortality iscorrelated with the proportionof children being immunizedagainst measles. Lao PDR hasseen a significant increase inmeaslescoverageover thepast25yearswhichhasincreasedto79.5% in 2015 (see figure 6).Despite this progress, it fallsshort of reaching the MDGtargetof90%.
Moreover, despite the steadyincrease of vaccination ratesrecordedwithin the past years,data quality still remains anobstacles when breaking downtosub-nationallevel.
As forDPT-Hep3,thevaccinecoveragehas fluctuatedoverthepast fiveyearsandhasnotrecordedaconstantincreaseastheothertwovaccines.DPT-Hep3increasedfrom58.4%in2010to66.8%in2012.FromFY2012to2013,thecoverageremainedconstant(withaveryslightdecreaseof0.1%). In2013-2014,thevaccinecoverageincreasedagainto71.7%beforedecliningbyalmostfivepercentto66.3%in
170
73
67
104
68
45
0
20
40
60
80
100
120
140
160
180
1990 1995 2000 2005 2010 2015 2020
Under-5mortalityrate Infantmortalityrate
Linear(Under-5mortalityrate) Linear(Infantmortalityrate)
MDG
MDG
68.6
79.5
66.3
40
45
50
55
60
65
70
75
80
85
2010 2011 2012 2013 2014 2015
BCGCoverage MeaslesCoverage
DPT-Hep3Coverage

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |9
2014-2015. As for BCG, despite a decline of 4.7% within the past year, BCG coverage has steadilyincreasedwithinthepastfiveyearsfrom57.2%inFY2009/10to68.6%inFY2014/15.
InordertoaddressthechallengesthatLaoPDRfaces inregardstomaternalandchildhealth,in2015theMoHhasapprovedtheNationalStrategyandActionPlanfor IntegratedServicesonReproductive,Maternal andChildHealth2016-2025.Anational steering committeeunder the chairmanshipofViceMinister and 11 technical groups is responsible to coordinate and oversee the mechanism for thetechnicalandimplementationwork.Thestrategyprovidesclearguidanceandidentifiesmajoractivitiestobe implementedover thenext five years that arebeneficial in improvingmaternalhealth.Aswithprevious policies and legal frameworks the main challenge of the strategy will remain itsimplementationatnationalscale,especiallyinremoteareas.
Moreover,TheGovernmentofLaoPDRhasinitiatedHealthEquityFund(HEF)schemesandtherolloutof Free Delivery of Maternal, Neonatal and Child Health Care (Free MNCH). Nevertheless, financialbarriersstill impedeaccesstohealthservices.Improvinghealthsectorfinancingwillrequireincreasingand securing sufficient domestic resources for health, removing financial barriers through nationalprogrammesforHEFschemesandFreeMNCH,andmovingtowardsUniversalHealthCoverage.7
Lastly, the comprehensivemulti-year plan for immunization 2016–2020was introduced in 2015 andaimstoaddressallchallengedinregardstovaccinecoverage.Policiesandactivitiesintheplanattemptto,firstly,eliminateimportantcommunicablediseasessuchaspolio,measles,rubellaand,maternalandneonataltetanus,andsecondlytomobilizecommunitiesforvaccination.
7MinistryofHealthLaoPDR,2013

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |10
MDG5:IMPROVEMATERNALHEALTH
Maternal mortality ratio(deaths per 100,000 livebirths)
Births attended by skilledhealthpersonnel
• LaoPDRhasachievedthefirsttargetofMDG5ofreducingits maternal mortality ratio (MMR) by 75%. In 2015, theMMRwasestimatedat197/100,000.iv
• The percentage of births attended by skilled healthpersonnel has increased to 53.9% in 2015 and thusachievestheMDGtargetof50%.
• Lao PDR reached a relatively highANC1 coverage rate of91%in2015andthusreachedtheprojectedgoalof60%.Nevertheless,ANC4coverageremainslowatonly52.4%.
• Overall, access to reproductive health has improved, yettarget5Bhasnotbeenachievedyet.
Target5A:Reducebythree-quartersthematernalmortalityratio(MMR)
Figure7:Maternalmortalityratiofrom1990to2015Lao PDR has achievedthefirsttargetofMDG5 of reducing itsmaternal mortalityratio(MMR)by75%.AUN joint paper byWHO,UNICEF,UNFPA,WorldBankGroupandthe United NationsPopulation Divisionhas estimated theMMR in 2015 to be197/100,0008.
8TrendsinMaternalMortality:1990to2015,UNjointestimatesbyWHO,UNICEF,UNFPA,WorldBankGroupandtheUnitedNationsPopulationDivision,2015
0
200
400
600
800
1000
1200
1400
1600
1800
1990 1995 2000 2005 2010 2015
MaternalMortalityRatio Expon.(MaternalMortalityRatio)
MDG

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |11
EventhoughtheMDGtargethassuccessfullybeenachieved,itisimportanttomentionthatchallengestoreducethematernalmortalityrateremainastheratioisstillrelativelyhigh.PoliciesintheNationalStrategyandActionPlanforIntegratedServicesonReproductive,MaternalandChildHealth2016-2025willworktowardsreducingthesechallenges.
Figure8:SBACoverage2015
ChallengestoachievealowerMMRincludelowcoverage and inadequate service quality forpregnant women. Only 53.9% of all estimatedbirths in 2015 were assisted by a skilled birthattendant.EventhoughthisexceededtheMDGtargetof50%onanationallevel,themajorityofprovincesstillstruggletoachievethetarget.Wesawthatonlysixprovinces,namelySavanakhet,Vientiane Province, Luangprabang, Bokeo,Xiengkhunag and Luangnamtha achieved theexpected50%.The facilitybaseddelivery is stilllow,at48.5%.Boththeproportionofdeliveriesassisted by a trained health personnel andfacility-based delivery rates are lowest in theruralareaswithout roadaccess,amongwomenwithprimaryornoeducation, fromthepoorestquintilehouseholdsandfromnonLao-Taigroups.
LaoPDRhopestoreduceandeliminatethischallengeasoneofthemainpriorityareasoftheNationalHealth SectorReformby 2020 is thedevelopmentof human resources. By increasing the staff in thequantity as well as the quality especially on a district and health center level, the strategy aims toincrease the number of trained birth attendants aswell as the quality of services provided and thusattemptstoincreasethenumberofSBAdeliveries.Moreover,theintroductionoffreeMCHwillhelptoeliminate some of the existing challenges and will provide more vulnerable women with access tonecessaryservices.
Target5B:Achieveuniversalaccesstoreproductivehealth
As for the second targetof achievinguniversal access to reproductivehealth, LaoPDRhas reachedarelatively high ANC1 coverage rate of 91% in 2015 and thus reached the projected goal of 60%.However,ANC4coverageremainsloweratonly52.4%.Inordertoimprovetheservicequalityofhealthfacilities inLaoPDR, it isessential topromotenotonlytheprovisionofANC1butalsoofANC4.MoreinformationinregardstoANC1andANC4coveragecanbefoundinsection2.1.1oftheNHSR.Norecentdatawasrecordedintermsofthecontraceptiveprevalencerate,adolescentbirthrateandunmetneedfor family planning, which requires further investigation. The Lao social indicator survey planned for2016willprovidedataontheseindicators.

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |12
MDG6:COMBATHIV/AIDSANDOTHERDISEASES
ARV among adult andchildrenfrom2005to2015
Malaria death rate (per100,000)1990to2015
• LaoPDRhasmanaged tokeepHIVprevalenceat0.29%andthustobewithinthetarget limit forMDG6,which isbelow0.5%forthegeneralpopulation.
• Target 6B, the % of adults and children with advanced HIVinfection receiving ARV treatment, remains far from beingreached. Despite an overall increase in ARV coverage from2005to2015,LaoPDRhasseenadecreaseinaccesstoARVdrugswithinthelastyear.
• Despite an increase in 2014, the overall malaria death ratehas significantly decreased from 9 per 100,000 in 1990 to0.03 in 2015. Especially the southern provinces are at highriskofmalariainLaoPDR.
• TB incidence per 100,000 as well as TB prevalence per100,000, Lao PDR had reached theMDG target of 240 and750 respectively by 2010 and 2005 respectively. The TBtreatmentsuccessratewashigh(87%)in2015,leadingtotheachievementoftheMDGtargetof85%.
Target6A:Havehaltedby2015andbeguntoreversethespreadofHIV/AIDS
Figure9:HIVprevalenceamonggeneralpopulationandamongtargetpopulations
LaoPDRhasmanagedtokeepHIVprevalence at 0.29% and thus tobewithinthetargetlimitforMDG6, which is below 0.5% for thegeneral population. However, aslight increase in the estimatedHIVprevalenceamongthegeneralpopulation in the last five yearswas recorded from0.25% in2010to0.29%in2015.
1.4 1.4 1.4
2.1
1.6 1.6
0.25 0.29 0.29
0
0.5
1
1.5
2
2.5
2010 2014 2015
HIVamongFSW
HivamongMSM
HIVamonggeneralpopulation
Source:MOH,CentreforHIV,AIDSandSTIs.2015

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |13
Moreover,LaoPDR'sincreasedintegrationintheregionaleconomyofSoutheastAsialeadtoahigherHIVinfectionrateof1.6%in2015inthetargetpopulations(femalesexworkersandmenwhohavesexwithmen).HIVtestingaswell as treatment services remains limited to the central level and major urban areas. Stigmatization and lowawareness amongnon-specializedhealth personnel further complicate the enrolment of patients into treatment.Thus,closersurveillanceandbiggereffortsarerequiredinordertoeffectivelyreduceHIVratesamongallpopulationgroups.
Target6B:AchieveuniversalaccesstotreatmentforHIV/AIDSforallwhoneedit
Figure10:ARVamongadultandchildrenIn the past ten years, the number ofchildrenandadultsinadvancedstageof HIV infection registered on ARVtreatmenthasslightlybeenincreased.The most significant increase wasrecorded from 2005 to 2010 whentherateincreasedby10%.From2010to2014,therateincreasedbyalmostanother10%,yetitfellwithinthelastyearfrom60.6%to54.8%.
Asaconsequence,theMDGtargetof90% is far from being reached andfurther progress is required in the
post2015agenda.Thecalculationofthecurrentcoveragerateisbasedonthe2012globaldefinitionwhichidentifiesHIVpatientsinneedofARVtreatmentalreadyataslightlyearlierstageoftheirinfection(CD4countat350comparedto CD4 count at 250 previously). This means that the total number of persons considered to require treatmentincreased in2012.Howeverdespite this increase thehealthauthoritiesmanaged to further increase the coverageratecomparedtopreviousyears.
InordertocombatHIVandaddressthesechallenges,LaoPDRhasendorsedthe90–90–90fasttrackinitiativetoachieve, by 2020, 90% of people living with HIV knowing their status, 90% of people living with HIV accessingantiretroviral treatment and 90% of patients receiving antiretroviral treatment having viral suppression9. Specialemphasisneedstobegiventoreachingthekeypopulationsatrisk,whichwillrequireanexpansionofnetworksofpeereducators.Inordertodoso,muchhigherallocationsfromthenationalbudgetarerequiredforHIVresponse,sincecurrentlymostoftheHIVinterventionsarefundedfromexternalsources.10
Target6C:Havehaltedby2015andbeguntoreversetheincidenceofmalariaandothermajordiseases
Malaria
Malaria is endemic throughoutmost of LaoPDRbutmost of the transmissions are associatedwithhilly forestedareasinthesouthernpartofthecountrywhichaccountforabout97%ofreportedcases.Figure11belowshowsa9LaoPDRcountryprogressreport,GlobalAIDSResponseProgressCountryReport,CHAS201510LaoPDR:TheMillenniumDevelopmentGoalsandLessonsLearntforthePost-2015Period:ASummaryReview,UN,2015
MDG
40.8
50.855.4 58.2 60.6
54.8
0
10
20
30
40
50
60
70
80
90
2005 2010 2012 2013 2014 2015%ofadultsandchildrenwithadvancedHIVinfectionreceivingARV(%)
MDG

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |14
significant decline in both malaria incidence and deaths from 1995 to present, with an exception of a 3 foldsincrease in incidence of malaria in 2014 compared to the 2012 incidence rate, which was caused by malariaoutbreaksinthesouthofthecountry,includingdrug-resistantmalaria.Nevertheless,theratefellagaindramaticallyfrom7.1 in2014 to4.92 in2015.Despite thedecline in thepastyears, LaoPDR refrains fromreaching theMDGtargetofanincidencerateof0.6.
Asforthemalariadeathrate,datashowsasimilartrendasthemalariaincidence,withanoveralldecline,yetapeakin2014.In2015,thedeathratereached0.03andthustheMDGtargetof0.2hasbeenachieved.Itisalsoobservedthatinthelastfiveyears,moreeffortshavebeenmadeincollectingmalariarelatedinformationonaregularbasis.
Figure11:TrendsofMalariaincidenceanddeaths1990-2015
Source:MOH,CentreforMalaria,ParasitologyandEntomology.2015
The increase in malaria cases is likely related to economic activities, particularly in forest areas and large-scaledevelopment projects, which have attracted workers and families from less endemic areas of Lao PDR orneighboring countries,wherepeopleare less familiarwith the threatofmalaria andmaybemore susceptible toseveremalariaordeathduetolackofimmunity.Challengesinregardtoeliminatingmalariaonanational,provincialaswellascentrallevelareaddressedintheNationalStrategicPlanforMalariaControlandElimination(2016-2020).Theplanlaysoutthegoals,objectives,strategies,partiesresponsibleandcoordinationmechanisms,andcoststosuccessfullyreducetheburdenofmalariaintheLaoPDRoverthenextfiveyearstopreparethecountryfornationaleliminationby2030.
Tuberculosis(TB)
TBprevalence,althoughdeclining,ismuchhigherthanpreviouslyestimated.Figure12showsthatinregardsofTBincidenceper100,000aswellasTBprevalenceper100,000,LaoPDRhadreachedtheMDGtargetof240and750respectivelyby2010and2005respectively.Nevertheless,theTBburdenremainshighwithanestimatedincidencerateof180per100000populationandarateofco-infectionwithHIVof7.4per100000.ItisimportanttomentionthattheWHOTBestimatesarecurrentlyonlyavailableuntil2014astheWHOprojectedestimatesof2015willbereleasedbymid-2016.TBburdenestimateswillmostprobablyfollowthesamedecliningtrendasinpreviousyearswithprojectedprevalence441/100,000andincidence180/100,000.
10
12
9.1
3.5
2.8 3.5
2.7
7.1
4.92
9
14
7.1
3.5
1.4
0.4
0.3 0.6
0.03
0
2
4
6
8
10
12
14
16
1990
1995
2000
2005
2009
2010
2012
2014
2015
MDG- MalariaIncidence(per1,000) MDGMalariaDeathrate(per100,000)

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |15
Figure12:TBsituationinLaoPDR2005-2015per100,000
Figure13:TBdetectedandTBcured1995–2015The TB treatment success rate washigh (87%) in 2015, contributing tothe achievement of the MDG targetof85%.ThereportsfromthenationalTBCenter, surveys as well as the WHOglobal report show a decline in bothincidenceandprevalenceofTBinthepasttenyear.Theyears2012to2014have recorded a decline in thenumberofTBcasesdetectedthroughtheDOTSprogramme.
Itisimportanttomentionthatsincethedataiscollectedthroughdifferentsurveys,reportsanddatasystems.Datain proportion of TB case detected are givenwith different estimates of the denominator (incidence) at differentperiods.Afterthefirstprevalencesurveyin2010,WHOhasentirelyre-modeledtheTBburdenestimatestrendsince1990.Basedonthisnewmodel,theproportionofcasedetectedvs.theestimatedincidence(casedetectionrate)hasincreasedregularlyfrom13%in2000to35%in2014andprojected37%in2015.
Based on previous achievements in improving quality, availability and access to treatment, the national programnow focuseson increasing thedetection ratewhich still remains lowatanestimated34% in2015.11TheNationalTuberculosisStrategicPlan2015-2019isinlinewiththevisionofLaoPDRfreeoftuberculosis–zerodeaths,diseaseand suffering due to tuberculosis and aims at reducing the burden of TB.With its focus on improving access totreatmentandtesting,strengtheningTB-HIVcollaborativeactivities,managementofdrugresistanttuberculosisandstrengtheningthemanagementofTBservices, itwill contributetoreachingthetargetsofWHOPost-2015GlobalTuberculosisStrategy.
11GlobalTuberculosisReport2015,WHO,2015
270213 197 190
700
540488 462
0
100
200
300
400
500
600
700
800
2005 2010 2013 2014IncidenceofTB PrevalenceofTB
37
87
0
20
40
60
80
100
1990 1995 2000 2005 2010 2015 2020
ProportionTBcasesdetected ProportionTBcasescuredDOTs
MDG

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |16
MDG7:ENSUREENVIRONMENTALSUSTAINABILITY
• Thepercentageofpeopleusinganimprovedwatersourcehas increased to 76% in 2015, yet falling short theMDGtargetof80%.
• The proportion of the population using an improvedsanitation facility has reached 71%, thus achieving theMDG target of 60%.
TargetC:Halvethepopulationwithoutsustainableaccesstosafewaterandbasicsanitation
Overthepasttenyears,LaoPDRhasseensignificantchangesinboththeproportionofpopulationusinganimproveddrinkingwatersourceaswellastheproportionofpopulationusinganimprovedsanitationfacility. In termsof theproportionof thepopulationusingan improvedsanitation facility, ithasbeenestimatedthattheratehasincreasedto71%in2015,thusreachingtheMDGtargetof60%.
Fortheproportionofthepopulationusinganimproveddrinkingwatersource,theratefellfrom84.7%in 2014 to 76% in 2015. Thus, even though the number of persons having access to safewater andimprovedsanitationhasthree-foldedsincethe1990s,theMDGtargetof80%ofthepopulationusinganimproveddrinkingwatersourcehasnotbeenreached.Therural-urbangaphasnarrowedregardingtheaccess to improvedwater sourcesbutdisparities remain significantacrosswealthquintiles. Inequitiesareevengreaterinsanitationthaninwatercoverage.
Figure14:Proportionofpopulationusingimprovedwatersourceandsanitationfacilities
Source:NCEHWS2007&HMIS2015
Inorder to improve the challenges related to improveddrinkingwater and sanitation,drinkingwaterquality standardswereadopted in2014, aiming tomakewater safetyplansmandatoryand includingdetailed surveillance and reporting requirements. However capacity of the National Center forEnvironmentalHealthandWaterremainsinsufficienttosupportthedevelopmentandimplementationoftheseplansatalllevels,especiallyinreachingouttothevillages.Auditingofthewatersafetyplansin
57
70
84.776
4959
67.9 71
0
10
20
30
40
50
60
70
80
90
2005 2010 2014 2015
Proportionofpopulationusinganimproveddrinkingwatersource
Proportionofpopulationusinganimprovedsanitationfacility

T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |17
urban and rural water supply systems and water quality surveillance, which should be led by theDepartmentforHygieneandHealthPromotionundertheMoHalsoneedsfurtherstrengthening.
Moreover, the National Environmental Health Strategic Action Plan for 2016-2020 has been draftedunder the leadership of the MoH in consultation with representatives from the environment,infrastructure development and water sectors. Continuation of this multi-sectoral coordination andengagementisofcriticalimportancetoensureoperationalplanning,effectiveimplementationandjointmonitoring.
T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |18
References:
CHAS (2015). Lao PDR Country progress report, Global AIDS Response Progress Country Report. Available fromhttp://www.aidsdatahub.org/sites/default/files/publication/Lao_PDR_narrative_report_2015.pdf.
FoodandAgricultureOrganizationoftheUnitedNations(2015).Thestateoffoodinsecurityintheworld.Availablefromhttp://www.fao.org/3/a-i4646e.pdf.
Ministry of Health (2015). National Nutrition Strategy and Plan of Action 2016-2020. Available fromhttp://swgard.maf.gov.la/download/other_important_resource_and_documents/2016-National-Nutrition-Strategy-and-Plan-of-Action-ENG.pdf.
United Nations (2015). , The Millennium Development Goals Report 2015. Available fromhttp://www.un.org/millenniumgoals/2015_MDG_Report/pdf/MDG%202015%20rev%20(July%201).pdf.
UnitedNations(2015).LaoPDR:TheMillenniumDevelopmentGoalsandLessonsLearntforthePost-2015Period:A Summary Review. Available from http://rtm.org.la/wp-content/uploads/formidable/LaoPDR_MDG_-Review_2015.pdf.
UN ESCAP, ADB, and UNDP (2015). Making it happen: Technology, finance and statistics for sustainabledevelopment in Asia and the Pacific. Available fromhttp://www.adb.org/sites/default/files/publication/159951/asia-pacific-regional-mdg-report-2014-15.pdf.
World Health Organization (2015). World Health Statistics 2015 Report. Available fromhttp://www.who.int/gho/publications/world_health_statistics/2015/en/.
World Health Organization (2015). Global Tuberculosis Report 2015. Available fromhttp://apps.who.int/iris/bitstream/10665/191102/1/9789241565059_eng.pdf.
WHO,UNICEF,UNFPA,WB,&UnitedNations(2015).TrendsinMaternalMortality:1990to2015.Availablefromhttp://apps.who.int/iris/bitstream/10665/194254/1/9789241565141_eng.pdf.
iLaoStatisticsBureauandtheWorldBank,2014iiThestateoffoodinsecurityintheworld2015,FAO2015iiiLSIS,2011/2012ivTrendsinMaternalMortality:1990to2015,UNjointestimatesbyWHO,UNICEF,UNFPA,WorldBankGroupandtheUnitedNationsPopulationDivision,2015
T h e M i l l e n n i u m D e v e l o p m e n t G o a l s R e p o r t |19